
Abstract
Introduction
Lesser tuberosity osteotomy (LTO) during anatomic total shoulder arthroplasty has a 13% nonunion rate. Treatment for LTO nonunion is controversial and poorly described in the literature. The purpose of this study was to compare the surgical and nonsurgical treatment outcomes of LTO nonunion.
Methods
A retrospective case series of 9 consecutive patients with LTO nonunion after primary anatomic shoulder arthroplasty at 1 institution from 2010 to 2016 were studied. Outcomes measured were radiographic evaluation of LTO on axillary X-ray, clinical range of motion (ROM), subscapularis strength, and pain at the time of LTO nonunion diagnosis and after either conservative care or surgical repair of the LTO nonunion.
Results
LTO nonunion was treated surgically in 4 and conservatively in 5 patients with average follow-up of 30 and 22 months, respectively. There were no significant differences in age, sex, or smoking status between groups. Treatment decision was a shared model of surgeon and patient. Displaced LTO nonunion was treated surgically in 2 and conservatively in 3 patients. There were no differences in LTO union rate of 50% in the surgical versus 60% in the conservative group. Abdominal compression test was abnormal in 50% of surgical versus 40% of conservative groups. At follow-up, ROM was lower in the surgical group with 128° forward elevation (FE) and 33° external rotation (ER) compared to 148° FE and 62° ER. Only 1 patient with LTO nonunion required conversion to reverse replacement.
Conclusion
LTO nonunion after shoulder arthroplasty is rare. Surgical repair of LTO nonunion does not significantly improve clinical or radiographic outcomes compared to conservative care.
Introduction
Anatomic shoulder arthroplasty reliably improves symptoms of end-stage osteoarthritis.1–3 During total shoulder arthroplasty (TSA), multiple techniques have been employed to manage the subscapularis tendon including tenotomy, peel, and lesser tuberosity osteotomy (LTO). Purported benefits of the LTO include maintenance of the tendon bone junction, stronger initial fixation strength,4,5 bone-to-bone healing, increased glenohumeral joint exposure,2,6–9 and clinical effectiveness.7,9–13 Unfortunately, failure of LTO healing may occur at a rate of approximately 13%, with nearly 7% of these LTO nonunions displacing and jeopardizing the function of the subscapularis.14,15 Surgical treatment of LTO nonunion has been described in 5 patients with good results, but no description of the outcomes of conservative care has been described.14,15 The purpose of this study was to compare outcomes of patients with LTO nonunion after anatomic shoulder arthroplasty treated either surgically or conservatively.
Methods
Study Design
This study was a single-center retrospective review of 69 adult patients who underwent shoulder arthroplasty from 2010 to 2016. After the approval of institutional review board, patients who underwent LTO were identified in a departmental database using current procedural terminology codes. Data were subsequently extracted from institutional electronic medical records for patients who met criteria. Patients lost to follow-up, or without at least 6 months follow-up from LTO nonunion treatment, were excluded from this study. Shoulder radiographs, including axillary, outlet lateral, and anteroposterior (AP) views, were obtained at each time point. Patients were subsequently subdivided into groups of postoperative union or nonunion at 6 months following the index procedure based on radiographic evidence of osseous bridging of the lesser tuberosity on axillary and/or AP views. In the cases with a 100% displaced LTO, fragment nonunion may have been diagnosed earlier than 6 months at the time of this radiographic finding. The postoperative nonunion group was then divided into surgically treated versus conservatively managed groups.
Data Collection
Data were collected through chart review by researchers who were not directly involved in the care of the patients in the study. The extracted records included demographic information, indications for surgery, types of prosthesis implanted, radiographic evidence of healing or healing failure, presence of postoperative injury or shoulder trauma, and clinical outcomes following treatment, including range of motion (ROM), subscapularis strength by abdominal compression testing, and pain by Visual Analog Scale (VAS). Radiographic evaluation of LTO healing was performed by at least 2 fellowship trained shoulder and elbow surgeons for each case who agreed on the diagnosis of union, nonunion, and nonunion displaced or nondisplaced. Each case was assessed with standardized AP, scapular-Y outlet, and axillary views of the shoulder by radiograph at routine visits. Preoperative and postoperative radiographs were available for all 9 cases. All patients had preoperative computed tomography or magnetic resonance imaging to evaluate the integrity of the lesser tuberosity and to assess for secondary degenerative changes of the glenoid. All radiographs and imaging studies were evaluated for quality prior to be included in this research. Patients with poor quality radiographs were excluded from the study.
Patients were evaluated before the index shoulder arthroplasty with LTO, at a minimum of 6 months postoperatively, and at least 6 months following diagnosis of LTO nonunion. Nonunion cause was classified as traumatic or atraumatic. Nonunion was defined as a lesser tuberosity without bony apposition and lack of osseous bridging between the affixed surfaces by 6 months postoperatively. LTO nonunions were described as displaced if the LTO bone fragment was displaced 100% on axillary and/or AP radiographs. The indications for revision surgery were evidence of clinical subscapularis dysfunction preventing active forward elevation (FE), anterior instability, pain, and radiographic nonunion and with a shared decision between the surgeon and patient. Revision surgery for LTO nonunion was not randomized.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistical software, and results were expressed using percentages, means, and standard deviations. Differences in numerical parameters between groups were assessed using unpaired t tests. The level of significance for each test was set at 5% (P<.05).
Results
Patient Population
A total of 69 patients with LTO were identified by the electronic database query who met inclusion criteria, of which 60 patients (87%) had radiographic evidence of LTO bony healing and 9 patients (13%) had radiographic evidence of nonunion of the LTO. There were 36 men and 33 women, average age was 69 years, and surgical indication for the majority of patients (N = 63, 91%) was end-stage osteoarthritis of the glenohumeral joint, with a minority of cases indicated for inflammatory arthritis (Table 1).
Analysis of All Included Patients Who Underwent Shoulder Anatomic Arthroplasty With LTO for Glenohumeral Joint Access, With Comparison Between Patients Who Experienced Nonunion and Those Who Experienced Successful Bony LTO Healing.

Abbreviations: BF, Bigliani–Flatow; deg, degrees; TM, Trabecular Metal; VAS, Visual Analog Scale. Bold face values represents the statistically significant values p<0.05.
Of the 9 patients who experienced LTO nonunion, 5 were men (56%) and 4 were women (44%). The average age was 64 years (range: 52–75). Patients had an average body mass index (BMI) of 33.5 kg/m2 (range: 26.5–48.6), 22% were smokers, and no patients had preexisting diabetes mellitus. All cases were primary anatomic shoulder arthroplasties treated with an LTO for subscapularis management during exposure.
LTO Union Versus Nonunion
The 69 patients were divided into 2 groups based on radiographic evidence of healing or nonunion of the LTO. The nonunion group was significantly younger (64 vs 70, P < .05) than the group that healed. Preoperative strength training and postoperative strength training were significantly different between groups—patients who successfully healed the LTO were more likely to exhibit negative abdominal compression tests preoperatively (100% vs 88%, P < .05) and postoperatively (100% vs 63%, P < .05). There was no significant difference in preoperative patient reported pain by means of VAS (P > .05), but postoperatively the patients who experienced nonunion reported significantly greater pain (0.3 vs 3.6, P < .05). There were no significant differences in preoperative or postoperative ROM (P > .05) between groups, nor were there significant differences in surgical prostheses used between groups (P > .05, Table 1).
Nonunion Treatment Outcomes
The 9 patients were divided into 2 cohorts based on treatment of the nonunion, either surgical (N = 4) or conservative (N = 5). The average follow-up was 30 and 22 months in the LTO nonunion surgery group and conservative care group, respectively. Time to nonunion diagnosis was on average 5 months after shoulder arthroplasty as 100% displaced nonunions were diagnosed earlier than 6 months postoperatively, and reoperation on LTO nonunion occurred on average 41.5 days (range: 11–63 days) after the LTO nonunion diagnosis was made. No significant differences in age (60.4 vs 67.2 years), sex (75% vs 40% men), smoking status (25% vs 20% smokers), comorbid diabetes (0% vs 0% diabetics), and BMI (31.1 vs 35.1 kg/m2) were found between surgical and conservative groups, respectively (P > .05).
Five of the 9 LTO nonunions were radiographically classified as displaced. Two of these were surgically treated, and 3 were treated conservatively. Displaced nonunion was seen in 2 of the 4 surgically treated patients, and both were in patients who experienced a traumatic fall onto an outstretched hand. Among those with conservatively treated nonunion, only 1 patient experienced a traumatic fall onto an outstretched hand (Figure 1). One patient treated conservatively reported noncompliance with postoperative restrictions with premature return to strenuous activity.
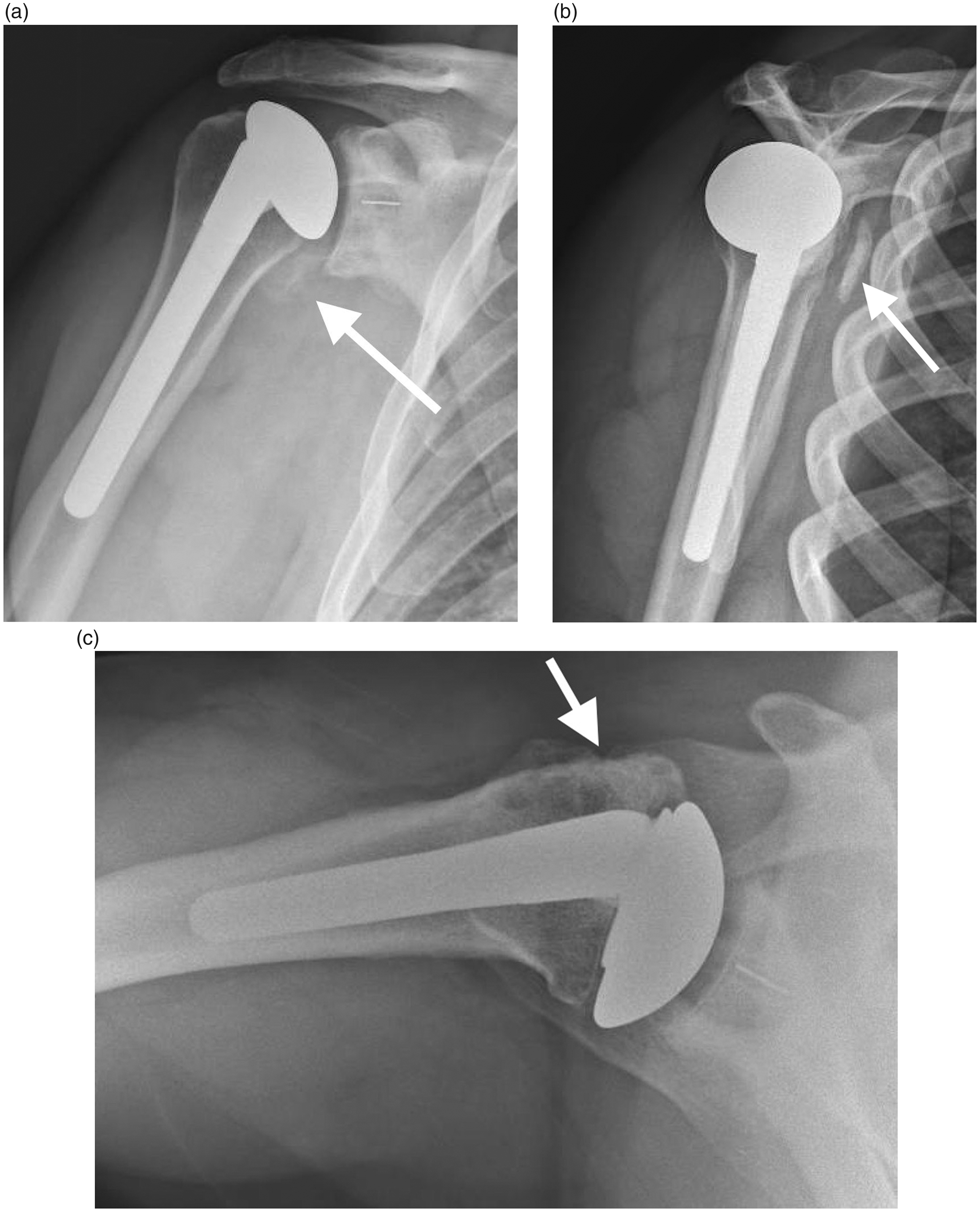
Displaced Nonunion of LTO After Shoulder Replacement. Radiographic images of a patient with pain after a fall onto an outstretched hand 4 months after total shoulder arthroplasty. The patient presented with radiographic evidence of a displaced LTO nonunion: (a) anteroposterior radiograph demonstrating a medialized LTO fragment (arrow), (b) outlet view showing an LTO nonunion (arrow), and (c) axillary lateral X-ray showing LTO healing and union 6 months after surgical treatment.
At the time of LTO nonunion diagnosis, the average ROM was 158° FE and 60° external rotation (ER) in the group that underwent surgical LTO revision, and 132° FE and 61° ER in the group that underwent conservative management (Table 2). Abdominal compression testing was positive at the time of nonunion diagnosis in 3 patients in the surgical group (75%) and 2 patients in the conservative group (40%).
Analysis of Patients Who Experienced Nonunion After Shoulder Arthroplasty With LTO for Glenohumeral Joint Access, With Comparison Between Patients Treated With Surgical Intervention Versus Conservative Management Addressing the Nonunion.
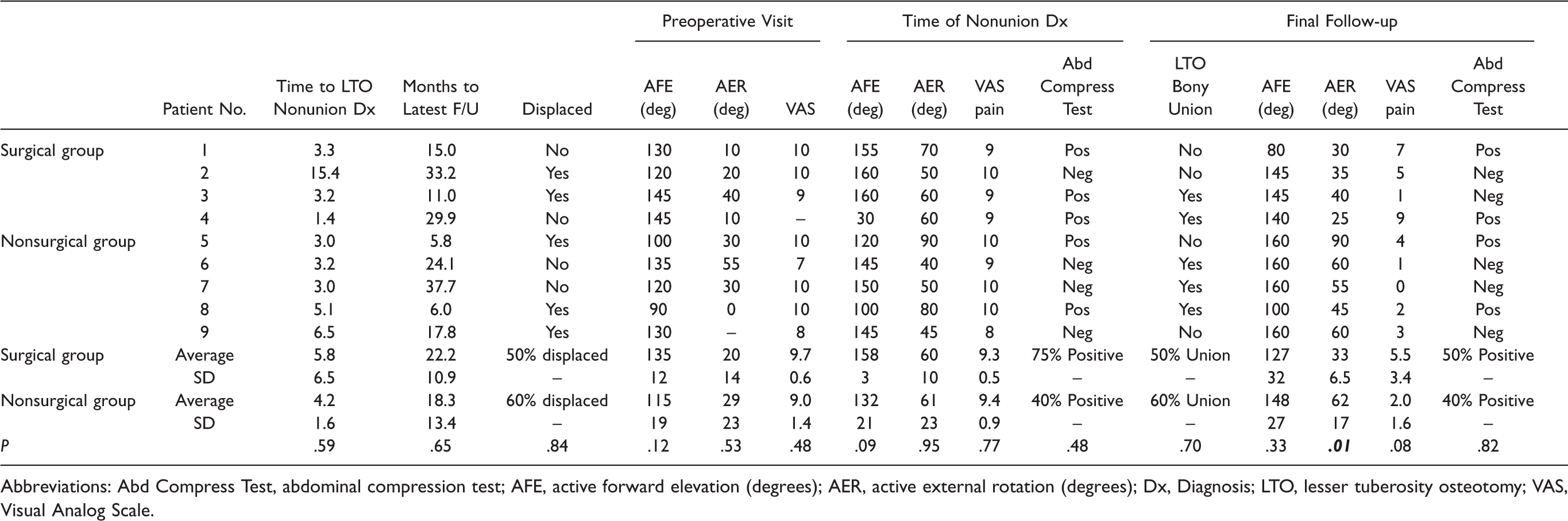
Abbreviations: Abd Compress Test, abdominal compression test; AFE, active forward elevation (degrees); AER, active external rotation (degrees); Dx, Diagnosis; LTO, lesser tuberosity osteotomy; VAS, Visual Analog Scale.
At latest follow-up after treatment, there were radiographic LTO union rates of 50% in the surgically treated patients versus 60% in the conservatively managed group. Abdominal compression testing was normal in 50% of patients who underwent surgical repair of their nonunion and 40% of patients who had their nonunion treated conservatively (P > .05). The average VAS pain score was greater in the surgery group (5.5) than in the conservative group (2.0, P = .08). The average FE and ER at final follow-up was 140° and 35° in the surgery group and 153°(P > .05) and 73° (P < .05) in the conservative group (Table 2). Only 1 of the 9 patients with LTO nonunion required conversion to reverse shoulder replacement (Figure 2).

Failed Surgical Treatment of Displaced Nonunion of LTO after Shoulder Replacement. Images depict the surgical radiographic outcome revision of LTO nonunion 6 months after index TSA. (a) Anteroposterior radiograph showing continued medial LTO displacement (arrow) and (b) axillary radiograph illustrating continued displaced medial LTO nonunion (arrow) despite surgical repair 3 months prior. The patient eventually went on to conversion to reverse replacement for continued pseudoparalysis.
Discussion
The treatment of LTO nonunion after shoulder arthroplasty is controversial and has rarely been described in the literature.14,15 Surgical indications for LTO nonunion are uncertain, with most shoulder surgeons considering surgical repair of a displaced LTO nonunion if there is subscapularis dysfunction that prevents active shoulder FE or is associated with prosthetic anterior instability. The treatment of nondisplaced LTO nonunion when found 6 months after TSA without prosthetic instability or loss of active motion is controversial, as many patients continue to experience pain symptoms. It is unknown if waiting longer to allow the LTO nonunion to heal or become asymptomatic is beneficial, compared to attempted surgical repair of the nonunion. The purpose of this study was to compare outcomes of patients with LTO nonunion after TSA treated both surgically and conservatively to help understand the expected outcomes from these difficult treatment decisions.
LTO during shoulder arthroplasty is associated with successful outcomes in the majority of patients, but there exists a significant incidence of healing failure and nonunion. As proposed by Shi et al., 14 our study suggests that LTO nonunion is uncommon, as we reported a nonunion rate of roughly 13%. Shi et al. found risks for nonunion to include active smoking or tobacco use, younger age <50 years, and male gender, likely due to increased subscapularis muscle bulk or premature return to activities. The use of an LTO during TSA is preferred by some surgeons due to initial mechanical robustness, bone-to-bone healing, and the ability to radiographically measure subscapularis healing and failure with simple X-rays. Several studies suggest that functional and clinical outcomes favor the LTO, with better abdominal compression testing, lift-off testing, and ability to tuck a shirt into one’s beltline.6–8 Other studies have demonstrated that LTOs can sustain greater force loads than tenotomy repairs and that LTOs exhibit higher clinical scores and lower rates of subscapularis tears than the tenotomy counterparts.8,9 Furthermore, several studies demonstrate greater initial repair strength in LTOs compared to tenotomy repairs, as well as greater combinations of subscapularis strength and length, and less gapping postrepair than other subscapularis management strategies.1–3
In contrast to LTO superiority studies, there exist studies supporting other subscapularis management strategies. Giuseffi found no differences in postrepair strength between LTO, tenotomy, or subscapularis peel techniques. 4 Van Thiel et al. also noted that there was no difference in ultimate failure strength or stiffness between techniques. 5 In addition, some studies favor the notion that LTO failure occurs more commonly than it is reported, leaving the patient debilitated and the surgeon with few options for treatment. 14 Most notable was the randomized controlled trial data published by Lapner et al. suggesting no significant differences in subscapularis muscle strength and clinical outcome scores between LTO and subscapularis peel. 12 Discrepancies in the published studies make it difficult for surgeons to interpret the results.
Nonunion of the LTO repair may have significant effect on shoulder TSA outcomes due to subscapularis dysfunction. Postsurgical surveillance with routine X-rays has been recommended by some authors to diagnose LTO nonunion earlier and expedite treatment. Shi et al. identified a cohort of patients who are at higher risk for LTO failure, namely, young patients of age ∼50 years, male patients with muscular builds. 14 It is hypothesized that this group of patients is at greater risk of failure due to early return to active ROM beyond the rehabilitation regimen recommended following surgery. For these patients, they recommend augmentation with a transosseous suture repair of the LTO with a tension band construct using a suture button. 14 The association between active smoking and poor bony LTO healing is also well known. 16 Evaluation of smoking cessation on postsurgical complications found that patients who quit smoking 4 to 8 weeks prior to surgery experience the greatest benefit, and those who quit smoking within 4 weeks of surgery experienced no benefit in postoperative morbidity. 17
There is no consensus on the recommended treatment of an LTO nonunion after TSA. This retrospective study found that patients who failed primary shoulder arthroplasty with LTO were middle-aged, heterogeneous in sex, and often suffered a minor traumatic event within the first 6 months postoperatively. Patients treated surgically demonstrated no improvement in clinical or functional outcomes including abdominal compression and ROM testing than those treated conservatively. In this study, treatment of LTO nonunion differs in the mechanism of nonunion, which was mostly traumatic in those who elected for surgical management, in contrast to mostly atraumatic nonunions in those who elected to be managed conservatively. Those managed surgically also reported significantly greater pain levels on VAS at their latest follow-up visit.
Ultimately, this study highlights the shared clinical decision-making between surgeon and patients when an LTO nonunion is diagnosed. The senior authors made treatment decisions based on the nature of the injury, the patient’s clinical shoulder strength on examination, but not based on the degree of displacement of the LTO nonunion. Even with operative repair of nonunion, there were only marginal improvements in clinical outcomes, specifically ROM, pain, and strength. Decision-making in these situations of displaced LTO nonunion will continue to evolve as more registry data are analyzed; however, this study highlights that clinical decisions in such circumstances are difficult and attempted surgical repair may not yield the excellent outcomes that the patient and surgeon desire.
Limitations of this study are inherent to this study design as a retrospective case control study. Due to the relatively small incidence within a limited population, and the varied presentation and treatment plans, we were able to identify only 9 patients with nonunion. In the future, multicenter studies or registry studies may increase study size and improve the power of statistical comparisons. There is also likely selection bias in treatment modality. Patients with less symptomatic LTO nonunions or significant medical comorbidities may have been unwilling to pursue surgical care. Despite this, our study represents the only study elucidating the natural history of LTO nonunions and represents an initial report of the available data in the literature.
Conclusion
The treatment of LTO nonunion after shoulder arthroplasty is controversial and has rarely been described in the literature. This retrospective study suggests that surgical repair of LTO nonunion has similar radiographic and clinical outcomes to conservative management with only 50% of LTO nonunion repairs attaining union after revision. The surgical indications for LTO nonunion repair are evolving and likely related the acuity, mechanism of injury, degree of subscapularis dysfunction, and patient symptoms.
Footnotes
Ethical Approval
This study was approved by Columbia University Institutional Review Board (IRB)—IRB-AAAL7810.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Charles M Jobin has received consultant payments from Acumed, Wright-Tornier, and Zimmer-Biomet, which is not directly related to the subject of this work. Dr Jobin receives grant support from American Shoulder and Elbow Surgeons not related to the subject of this work and grant funding from Orthopaedic Scientific Research Foundation this is directly related to this research. Dr Jobin is on the editorial board of Journal of American Academy of Orthopedic Surgeons (JAAOS). William N Levine is an unpaid consultant for Zimmer-Biomet and receives research grant financial support from Smith and Nephew not directly related to the subject of this work and is on the editorial/governing board of the JAAOS. The other authors have nothing to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: grant funding from Orthopaedic Scientific Research Foundation to perform this research.