
Abstract
The deltopectoral exposure has earned the reputation as the “workhorse” approach to the shoulder. Due to the reproducible anatomy and its extensile nature, there is little debate when considering exposure in total shoulder arthroplasty (TSA). Despite this consensus, there is still significant variability in management of the subscapularis. Several repair techniques including a subscapularis tenotomy, peel, and lesser tuberosity osteotomy (LTO) have been developed to ensure healing and optimize function. This article focuses on performing a LTO in anatomic TSA. We will review the surgical technique and advantages in exposure in addition to biomechanical and clinical outcomes.
Keywords
Background
Initial techniques in anatomic total shoulder arthroplasty (TSA) exposed the glenohumeral joint by subscapularis tenotomy or peel. In 1997, Torchia published his technique using bone-on-bone fixation with a lesser tuberosity osteotomy (LTO). 1 The technique was then refined by Ponce and Gerber in 2005 and 2006, respectively.2,3 The size of the osteotomy can be variable from a complete osteotomy or “fleck,” but the primary advantage of the technique is potentially more consistent bone-to-bone healing compared with subscapularis tenotomy or peel techniques. Osteotomy also theoretically avoids iatrogenic tendon damage. In addition, confirmation of subscapularis integrity can be inferred by plain radiographs without the need for advanced imaging.
A variety of LTO techniques have been described. The initial LTO described by Ponce had dimensions of 2.5 cm2 × 4- to 5-mm thick. 2 Krishnan et al. later reported outcomes with a smaller “fleck” osteotomy. 4 With a fleck osteotomy, the LTO is repaired with previously described methods, but the thickness of the osteotomy is 50% or less of the tuberosity. A thinner osteotomy preserves proximal bone stock but limits glenoid exposure and decreases surface area of bone-to-bone healing. 5
Management of the subscapularis continues to be refined because of its importance in TSA. Preserving its integrity is critical for preserving anterior stability and optimizing function following anatomic shoulder arthroplasty. The goals of this article are to review the surgical technique and outcomes with a LTO. We will discuss technical pearls in addition to intraoperative advantages of the LTO technique. Biomechanical testing and clinical outcomes after an LTO will also be compared.
Biomechanical Comparisons
Debate over subscapularis management has led to biomechanical studies in an effort to establish the strongest and most durable repair constructs. These studies do not account for response to healing as they represent a time zero analysis but still provide important information on initial strength and effects of cyclic stress on subscapularis repair.
Subscapularis Tenotomy Versus LTO
Ponce’s initial biomechanical testing showed decreased displacement with cyclic loading and an increased load to failure of the LTO technique compared to subscapularis peel with transosseous repair and soft tissue repair via tenotomy. 2 Giuseffi et al. evaluated a traditional subscapularis tenotomy versus LTO. 6 Ten Cadavers underwent tenotomy (1 cm medial to insertion) and a contralateral LTO (2.5 cm2 by 4- to 5-mm thick, repaired with 2 parallel rows, and 4 drill holes). There was less cyclic displacement with tenotomy (0.8 mm) compared to osteotomy (1.8 mm). No difference was found in maximum load to failure.
Schrock et al. performed a meta-analysis on 12 cadaveric studies from 2005 to 2014. 7 They found that an LTO had a higher load to failure than a tenotomy, 443 N versus 350 N, respectively. There were, however, no differences in cyclic displacement. When comparing subscapularis tenotomy to a lesser tuberosity fleck osteotomy, the fleck osteotomy had a higher load to failure. 4 Krishnan et al. showed that single- and dual-row fleck osteotomy repairs had a 430 N and 466 N load to failure, respectively, while standard tenotomy repair demonstrated a load to failure at 252 N. There was no statistically significant difference between the single- and dual-row repair load to failure. Schmidt et al. compared thin versus thick LTO fragment repairs and showed no difference in initial displacement if a tensioned repair was utilized. 8
Recent data suggest that a subscapularis peel with a stem-based repair has similar strength and durability to LTO. 9 No differences were found in cyclic displacement or load to failure when comparing the 2 techniques.
Surgical Technique
Lesser Tuberosity Osteotomy
Following superficial deltopectoral exposure, the subscapularis presents itself deep to the clavipectoral fascia and lateral to the conjoint tendon. Exposing the boundaries of the tendon is the first step in precise dissection and mobilization, regardless of take-down technique. The lateral footprint of the subscapularis is trapezoidal with a 25 mm superior to inferior dimension and a 17 mm medial to lateral dimension. 10 It passes deep to the conjoint tendon, and the superior two-thirds of the muscle forms a flattened tendon that inserts onto the greater tuberosity, bicipital groove, and lesser tuberosity. Superior fibers interdigitate with the supraspinatus, coracohumeral ligament, and superior glenohumeral ligament. 10 The inferior third has a muscular attachment on the inferior lesser tuberosity and the anterior aspect of the humeral metaphysis through a membranous structure. 11
The most critical tendinous insertion is directly to the lesser tuberosity. To preserve these fibers, the long head of the biceps tendon is an excellent landmark, as it lies just lateral to the lesser tuberosity and is easily identifiable. Incising the transverse humeral ligament exposes the tendon. The long head of the biceps can then be longitudinally followed to its insertion on the superior labrum. This allows release of the rotator interval while protecting the supraspinatus and upper rolled border of the subscapularis. The long head of the biceps tendon can be tenotomized or tenodesed at this point. While the long head of biceps is a useful landmark, it may not be present in cases of presurgical rupture. In this situation, palpating the bicipital groove is helpful. Inferiorly, the ascending humeral circumflex artery and vein are excellent landmarks to expose the subscapularis. These vessels may be ligated or coagulated to maintain hemostasis and in turn demarcate the inferior border of the subscapularis dissection.
By exposing the bicipital groove, the upper rolled border of the subscapularis, and the inferior border by way of the ascending humeral circumflex vessels, a bracket now outlines the subscapularis tendon insertion (Figure 1). This dissection clearly identifies the tendon to perform a precise LTO.

Outlining subscapularis tendon footprint. The lateral, superior, and inferior borders of the subscapularis are outlined using the bicipital groove, the upper rolled border of the subscapularis, and ascending humeral circumflex vessels, respectively. This forms a bracket around the subscapularis tendon.
Variability exists in the size of bone that can be mobilized with the LTO. One advantage of a large tuberosity fragment is improved glenoid exposure due to less humeral head crowding when translating the humerus with posterior glenoid retractors. When less force is required for posterior translation, there is also, theoretically, less traction on the axillary nerve, which can be easily palpated between the conjoint tendon and subscapularis. A large LTO also provides increased surface area for direct bone healing and can in turn lead to a more reliable repair. However, depending on the ultimate mode of humeral stem fixation, a large LTO can breach metaphyseal bone required for stem stability. This is especially important in metaphyseal press-fit implants or stemless implants. A small or “fleck” LTO may be more appropriate in these circumstances despite disadvantages with glenoid exposure and surface area for bone healing. The initial technique was described by Krishnan et al. with approximate dimensions of the fleck measuring 2 cm in length, 1 cm in width, and 3 to 4 mm in thickness. 4
After deciding the desired size for the LTO fragment, an osteotome or sagittal saw may be used to perform the osteotomy (Figure 2). We find that using a microsagittal saw allows for excellent precision when initiating the vertical osteotomy in the bicipital groove. If a larger LTO is performed, the osteotomy may extend into the proximal humeral shaft. In order to prevent continued distal extension, a 45° counter cut can be made so that the osteotomy exits anteriorly. The osteotomy is subsequently completed with a curved osteotome to separate the fragment from the distal bed. The osteotome can also be used to lever the lesser tuberosity fragment off the humeral head and complete dissection of any remaining soft tissue (Figure 3). An additional technique to protect and identify the subscapularis tendon includes placing a Lane or Freer elevator vertically through the dissected rotator interval. This helps delineate the upper border of the tendon and also helps retract the posterior surface of the subscapularis. By placing this retractor, you can confidently identify the trajectory of the tendon and its deep insertion to help tailor the size of the osteotomy. The elevator also indirectly protects the glenoid from the saw or osteotome.

Performing the lesser osteotomy. A microsagittal saw allows for excellent precision when initiating the vertical osteotomy in the bicipital groove. This may be completed with an osteotome. A Darrach retractor is protecting the axillary nerve medially.

Mobilizing the subscapularis. Once the LTO is completed, residual soft tissues of the rotator interval and lower muscular subscapularis are released to mobilize the fragment.
Tendon Mobilization
Once the osteotomy is complete, focus shifts to releasing capsular tissue around the subscapularis and mobilizing the tendon. The tendon is often contracted in a degenerative setting but even more so in the presence of glenoid retroversion or in revision cases. Care must be taken to appropriately release the tendon to restore function and excursion while protecting the nearby neurovascular structures. The 360° release begins superiorly due to ease of exposure (Figure 4). The rolled upper border of the tendon is identified, and all superior attachments to the base of the coracoid are released (the rotator interval, coracohumeral, and superior glenohumeral ligaments). The lateral edge of the subscapularis tendon can be tagged with a suture to help control these releases. The middle glenohumeral ligament (MGHL) is then dissected off the deep surface of the tendon. To protect the subscapularis tendon, the MGHL should be released close to the glenoid origin. Next, the inferior capsule is separated from the subscapularis muscle and divided from anterior to posterior while protecting the axillary nerve (2.5 cm inferior to the tendon edge). 12 This will free the entire deep subscapularis from the anterior glenoid. If necessary, the superficial aspect of the subscapularis should be released from the conjoint tendon. The subscapular nerves can be present 15 mm medial to the conjoint or anterior glenoid rim, so maintaining this “safe zone” is crucial along the anterior surface of the tendon. 13 Adhesions in this area are especially common in revision surgery.

Subscapularis release and mobilization. A circumferential release of the subscapularis is performed. The rotator interval, middle glenohumeral ligament, and inferior capsular are released while protecting the axillary nerve and surrounding neurovascular structures.
LTO Repair
During repair, transosseous drill holes are created in the humerus. This can be performed in parallel rows on either side of the osteotomy or a single column just lateral to the osteotomy site (Figure 5). For the single-column technique, we prefer to place the tunnels on the anterior aspect of the greater tuberosity exiting into the humeral canal. Heavy sutures (#5 caliber) are placed through the bone tunnels, and the stem is inserted into the humerus with the inferior sutures around stem.
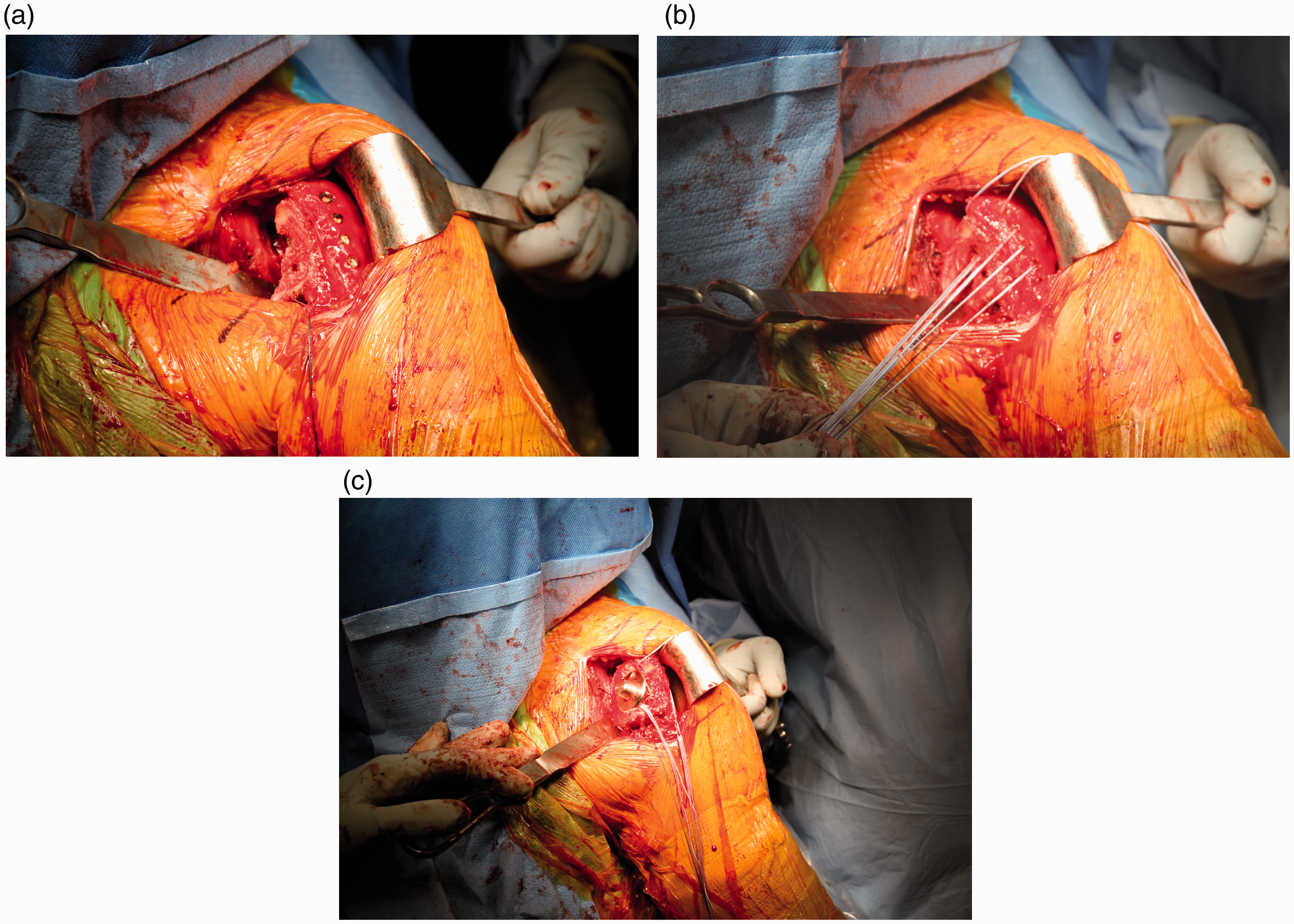
Placement of sutures for lesser tuberosity repair. (a) Drill tunnels are placed in the anterior aspect of the greater tuberosity exiting into the cut surface of the humerus. (b) Heavy sutures are placed through the bone tunnels. (c) The stem is inserted into the humerus with the inferior sutures placed around the humeral stem.
The reduction in the LTO fragment should then be evaluated. Depending on the proximal stem anatomy or size of the LTO, it may malreduce. The deep contour of the osteotomy may need to be tapered with a rongeur for the fragment to key into place. For larger LTO fragments, a portion of the humeral head may need to be removed to allow the LTO fragment to key back into proper alignment (Figure 6). However, some advocate preservation of the anatomic neck osteophyte on the LTO fragment is a key for reduction during repair. The subscapularis sutures are then passed through the tendon at the tendon bone junction (Figure 7). Reduction in the LTO is facilitated with slight internal rotation of the arm. Secure fixation of the sutures is mandatory and is facilitated by using techniques that obtain good loop security with sutures that do not slide. Suture can also be tunneled through the great tuberosity and passed through a button plate. This “Backpack Technique” theoretically reduces potential suture cutout. 3 Closure of the rotator interval by approximating the anterior supraspinatus and the upper subscapularis reinforces the osteotomy repair while augmenting stability of the shoulder. 14

Debulking the lesser tuberosity fragment. For larger LTO fragments, a portion of the humeral head must be removed to allow proper reduction in the fragment to the native bone bed.

Lesser tuberosity osteotomy (LTO) repair. (a) The subscapularis repair sutures are passed through the subscapularis at the tendon-bone junction. (b) Secure fixation of the LTO fragment. The rotator interval has been closed with a heavy suture superiorly reinforcing the repair.
Technical Considerations
Disadvantages of the LTO include variable reproducibility. With implants that require more proximal fixation, a smaller LTO would be advised, while cases with difficult glenoid exposure, (posterior glenoid erosion) a larger LTO is helpful. There is a learning curve for trainees and lesser experienced surgeons to overcome to perform an appropriately sized osteotomy. An aggressive LTO resection can alter the surgical plan.
With the advent of stemless implants, increased attention is required when performing an LTO. In implants that require more peripheral fixation, a “fleck” osteotomy can be performed in order to avoid significant breach to the anterior cortex. If the surgeon feels that they are unable to reproduce an osteotomy that breaches the cortical rim outside the LTO bed, this technique should be avoided when implanting stemless implants.
In osteoporotic patients, the area of the lesser tuberosity bed may be impacted by posterior glenoid retractors. If there is significant concern, a humeral head cut protector can be placed or a trial stem may be used to protect the osteotomy bed. When a defect does occur, we prefer to impact cancellous bone into the defect covering any exposed metal from the humeral implant. We have not found this to negatively impact tuberosity healing.
Clinical Outcomes
Biomechanical data are helpful to quantify strength and durability in an experimental setting, but the ultimate outcome is a patient’s clinical function. These data are perhaps more difficult to standardize but provide the most relevant argument for the optimal subscapularis management technique. Although there was no control, Ponce’s data showed that clinically 93% of patients had intact subscapularis function at 15 months (5 patients had dysfunction and 1 patient ruptured). 2 Radiographic evaluation demonstrated union of the osteotomy in all 76 patients; however, 1 patient had a delayed clinical failure.
Subscapularis Tenotomy Versus LTO
Some retrospective reviews have shown better subscapularis function with an LTO compared to an intrasubstance tenotomy; however, the level of evidence is low. Osteotomy of the lesser tuberosity demonstrated better functional outcomes than those who had a subscapularis tenotomy as assessed by the graded belly-press test. 15 Scalise et al. showed greater improvements in Penn Shoulder Scores with LTO compared to tenotomy. 16 In this study, sonographic evaluation showed 40% of shoulder had attenuation of the subscapularis with tenotomy compared to 10% with LTO. Furthermore, abnormalities on ultrasound correlated with worse Penn Shoulder Scores. However, a recent systematic review comparing the 2 techniques showed forward elevation improvements were significantly greater for the tenotomy group (mean 50.9°) than for the LTO group (mean 31.3°) at final follow-up. 17
Subscapularis Peel Versus LTO
Level I evidence has suggested no difference in clinical or radiographic outcomes between LTO and a subscapularis peel repair. 18 In this study, the subscapularis peel repair was augmented at the suture to bone interface with a plate to prevent suture cutout through bone. The authors found no difference in subscapularis strength at 24 months. No differences were seen in Western Ontario Osteoarthritis of the Shoulder Index or American Shoulder and Elbow Surgeons scores at any time point up to 24 months between groups. In addition, there were no differences in healing rates or progression of muscular fatty infiltration. 19 Both LTO and peel groups advanced approximately one-half grade of fatty infiltration based on the Goutallier classification.
Recent retrospective cohort studies have demonstrated that 90% of shoulders have a normal lift-off test after LTO compared to 70% after subscapularis peel with transosseous repair; however, the peel group demonstrated better final external rotation motion (69° vs 60°).20,21 Abnormal subscapularis tendons on ultrasonography correlated with poorer outcome scores. Otherwise, most clinical data show similar outcomes.
Conclusion
Although debate still exists in subscapularis management, the LTO has proven to be an effective and reliable technique. There are several intraoperative benefits including improved glenoid exposure and decreased axillary nerve traction. Subscapularis integrity and healing can also be followed on postoperative radiographs. Most importantly results are reproducible with excellent biomechanical and clinical outcomes. Like any method of subscapularis management during shoulder arthroplasty, the principles of complete tendon mobilization and secure repair are paramount to preserved subscapularis function long term.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.