
Abstract
Background
Substantial proximal humeral bone loss may compromise reverse shoulder arthroplasty secondary to limited implant support, insufficient soft tissue tension due to shortening, lack of attachment sites for the posterosuperior cuff when present, and lack of lateral offset of the deltoid. In these circumstances, use of a proximal humeral replacement may be considered.
Patients/Methods
Between 2012 and 2014, 34 consecutive reverse shoulder arthroplasties were performed using a proximal humeral replacement system. The indications were failed shoulder arthroplasty (15), oncology reconstruction (9), humeral malunion/nonunion (7), prior resection arthroplasty (2), and intraoperative fracture (1). All patients were included in the survival analysis. Twenty-two patients with minimum 2-year follow-up were included in analysis of clinical results.
Results
Among the cohort of 34 patients, there were 8 additional reoperations: humeral loosening (3), periprosthetic fracture (2), irrigation and debridement (2), and glenoid loosening (1). Humeral component loosening occurred exclusively in patients undergoing revision shoulder arthroplasty. The 4 patients had an average 3.75 prior procedures before the proximal humeral replacement. Two of the revisions were from cemented to uncemented stems. Among the 23 patients with minimum 2-year follow-up, there was significant improvement in pain scores (4.1 vs 0.6), forward elevation (31 vs 109) degrees, and 81% were satisfied.
Conclusion
Use of a proximal humeral replacement when performing a reverse shoulder arthroplasty in the complex setting of substantial proximal humerus bone loss provides good clinical results and a particularly low dislocation rate. However, the rate of loosening of the humeral component in the revision setting suggests that proximal humeral replacement components should be cemented when revising a previously cemented stem.
IRB
16-006966.
Keywords
Introduction
Reverse shoulder arthroplasty (RSA) continues to evolve as a reliable treatment option for many conditions of the shoulder. Although its use was traditionally indicated for patients with arthropathy related to massive rotator cuff tears, promising results have been reported in the setting of inflammatory arthritis, posttraumatic arthritis, proximal humerus malunions, in the revision setting, and in cases of substantial glenoid deformity. As a result, use of the RSA continues to increase.1–5
Proximal humeral bone loss continues to represent a major challenge when performing RSA. This scenario can be encountered in a range of circumstances, including tumor resection, periprosthetic infection, nonunions or failed fixation attempts (ie, malunion), periprosthetic fractures, 6 and revision arthroplasty. Without metaphyseal support, stem fixation is dependent on diaphyseal fixation, which can often be tenuous. In addition, there is often inadequate lateral tensioning of the deltoid, combined with difficulty reattaching the posterior or anterior rotator cuff. It can be challenging to restore humeral length as well, which may further compound the issues related to soft tissue tensioning. These factors may lead to an increased risk of stem loosening, dislocation, weakness and potentially worse function.7,8
The effect of glenoid abnormalities and glenoid bone deficiency in the setting of reverse arthroplasty has been studied to some extent. However, there is relatively little in the literature relating to proximal humeral bone loss in RSA. Reported management options include the use of osteoarticular allografts, allograft-prosthetic composites (APCs), and reconstruction proximal humerus-replacing implants.6–12 The use of an APC is a potentially attractive option, though graft incorporation, nonunion, and resorption are of concern. Reconstruction of missing bone with metal has become the standard treatment in hip and knee arthroplasty due limited availability of appropriately sized and prepared allografts, the time-consuming nature of the allograft procedures and challenges associated with soft tissue reattachment to grafts.
There are few reports on the outcomes of shoulder reconstruction with an RSA in the setting of substantial proximal humeral bone loss. The use of a tumor endoprosthesis has been reported.8,12–17 though these studies largely focus on patients having undergone tumor resection. The purpose of this study was to evaluate the outcomes of RSA using a segmental reconstruction prosthesis to address significant proximal humeral bone loss following nonmalignant conditions (ie, malunions, nonunions, or failed arthroplasty) as well as after tumor resection.
Methods
Between 2012 and 2014, 34 consecutive reverse shoulder arthroplasties were performed using a proximal humeral replacement system (Segmental Revision System [SRS]; Zimmer-Biomet, Warsaw, IN, USA). All of the procedures were performed by 1 of 3 fellowship-trained shoulder surgeons. The indication was failed shoulder arthroplasty (15), oncology reconstruction (9), humeral malunion/nonunion (7), prior resection arthroplasty (2), and intraoperative fracture (1). There were 9 males and 25 females, with a mean age of 66 (range: 40–94) years. There were 16 right shoulders and 18 left shoulders. All patients were included in the survival analysis. Twenty-three patients with minimum 2-year follow-up, or until the time of revision surgery, were included in analysis of clinical results (mean: 2.4 years). Of the remaining 11 patients, 6 had died prior to the 2-year postoperative time interval (5 of these 6 had a malignancy) (Figure 1) and the other 6 were lost to follow-up. Of those 6, 2 had severe medical comorbidities and were unable to sufficiently communicate or provide follow-up information.
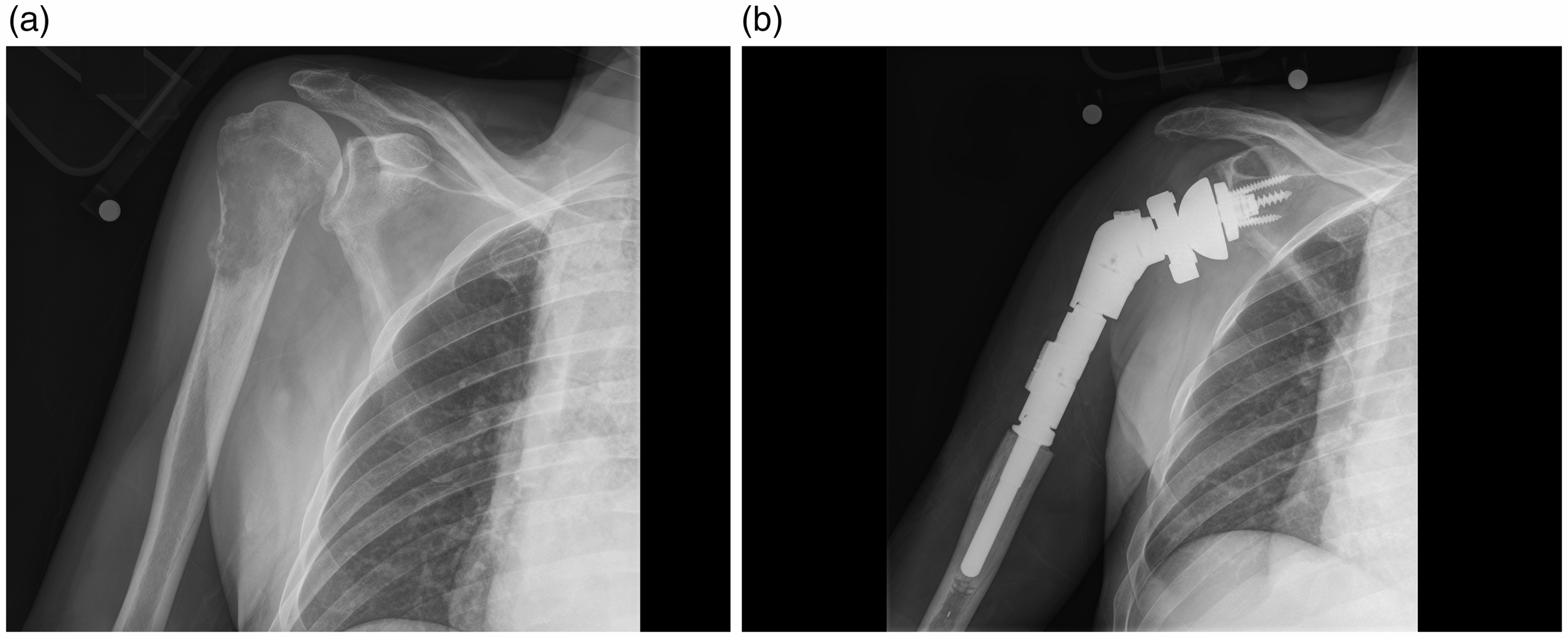
(a) Preoperative and (b) postoperative radiographs of the SRS used for primary proximal humerus reconstruction following resection of a pathologic lesion.
In addition to patient demographic information, other pertinent factors were recorded, including the presence of any neurological injury (ie, brachial plexus pathology), history of prior trauma or infection, the numbers and types of any prior surgeries, the presence of cement preoperatively and cement use intraoperatively, and whether complications had occurred.
All surgeries were performed through a deltopectoral approach. Glenosphere sizes implanted were 36 mm in 16 shoulders and 41 mm in 18 shoulders. The average length of the humeral stem was 85 mm. There were twenty five 75-mm stems, seven 100-mm stems, and two 150-mm stems. Cement fixation was used in 21 shoulders (Figure 2); use of cement was based on surgeons’ preference. The average length of the proximal body was 47 mm (range: 42–62 mm). Soft tissue (ie, rotator cuff) was reattached in 12 cases, 2 of which involved reattachment of the deltoid (Figure 3).
(a) A narrow stem can be cemented in the canal. (b) Intraoperative image showing the implant in-vivo. (a) AP radiograph showing a metastatic squamous-cell carcinoma of the proximal humerus. Intraoperative photo (b) demonstrates the manner by which the soft tissue can be attached the prosthesis. (c) Postoperative AP radiograph.
Radiographic parameters were assessed by 2 consultant surgeons (JWS and JSS) and separately by 3 independent reviewers. The parameters assessed were the presence of scapular notching and grading when present, as well as radiographic signs of humeral or glenoid loosening. Immediate postoperative radiographs were compared to those obtained at most recent follow-up.
Statistical Analysis
Univariate analyses were performed to evaluate clinical outcomes. The Student’s t test was used to compare continuous variables, and correlation was assessed using Pearson’s correlation coefficient where applicable. In addition, the relative risk and odds ratios were calculated for selected variables. Statistical significance was set at a P value <0.05.
Results
Clinical and Radiographic Outcomes
RSA using this proximal humeral replacement system resulted in significant improvements in pain, motion, satisfaction, and function. Among the 23 patients with adequate follow-up, the mean pain score improved from 4.1 preoperatively to 0.6 postoperatively (scale of 5 severe pain to 0 no pain) (P < .0001). Forward elevation significantly improved postoperatively from 31° to 109° (P < .0001). Although clinical improvements were observed in external rotation (17° to 37°) and in mean strength from a grade of 3 preoperatively to 4 postoperatively, these values were not statistically different. There was an 81% satisfaction rate (17 of the 21 patients who responded to the question). Two of the 4 dissatisfied patients had suffered a complication. Nineteen of the 20 (91%) patients felt that they had improved as a result of the surgery.
Of the 23 patients with adequate follow-up, it was noted that there was sufficient soft tissue (ie, rotator cuff) that could be repaired to the implant in 9 cases. There was no correlation between the ability to repair part of the rotator cuff and whether or not a complication occurred.
Scapular notching was noted in 3 of the 23 patients: grade 2 in 2 patients and grade 3 in 1 patient. Glenoid loosening was evident in one patient who had undergone structural grafting at the time of the index procedure, though this shoulder did not undergo revision surgery.
Complications
Among the entire cohort of 34 patients, there were 8 (24%) reoperations. The indications for reoperation were humeral loosening (3 shoulders), periprosthetic fracture (2 shoulders), irrigation and debridement (I&D) for infection (2 shoulders), and dislocation (1 shoulder). One additional humeral component was considered loose but has not been revised at the time of most recent follow-up. All humeral loosenings complicated revision shoulder arthroplasty. Two of the loose implants were cemented and 2 were uncemented. These 4 patients had undergone a mean of 3.8 procedures (range 2–6) prior to proximal humeral replacement. Although the results did not achieve statistical significance, there was a calculated relative risk of 7.5 (95% CI: 0.5–123; P = .16) of humeral loosening if the patient had 2 or more prior procedures, and an odds ratio of 11.4 of humeral loosening in that group (95% CI: 0.5–247; P = .12).
The one patient with a dislocation underwent replacement with an SRS at our institution following multiple failed procedures, including having had an infected failed APC after tumor resection, and multiple I&D procedures. At the time of revision, the length of the proximal body was increased to increase the soft tissue tension and the patient has remained stable. Among the 2 patients with a periprosthetic fracture, 1 was revised for a periprosthetic fracture 3.6 years following implantation of the SRS and was treated with an APC. This patient had 3 prior surgeries prior to the SRS: a Bankart procedure, a hemiarthroplasty, and an anatomic shoulder arthroplasty. The other patient had a history of Parkinson’s disease with falls in the past and suffered a periprosthetic fracture after falling at home 1 year following implantation with the SRS. He had a history of failed ORIF of the proximal humerus as well as a failed hemiarthroplasty prior to implantation of the SRS.
There was 1 patient with the history of Parkinson’s disease and Alzheimer’s dementia who sustained a minimally displaced impacted periprosthetic fracture that did not require reoperation and healed uneventfully.
Discussion
The results of our study seem to indicate that proximal humeral replacement is a reliable option for the management of proximal humeral bone loss following both malignant and nonmalignant conditions. The most profound clinical improvements were noted in forward elevation and in the reduction of pain. This remains a very challenging problem, and given that the majority of patients without an associated malignancy had undergone prior procedures, there was a very acceptable satisfaction rate of 81% with 91% of patients having felt that they had improved as a result of the surgery.
We did not find that the ability to repair any remaining posterior or anterior rotator cuff tissue was correlated either positively or negatively with function or the rate of complications, particularly humeral loosening. In addition, we did not observe a problematic rate of scapular notching.
As the indications of RSA continue to expand, research has focused on strategies to maximize implant longevity. Glenoid-sided failures have traditionally been viewed as more frequently occurring and more problematic than humeral-sided failures. As a result, there is relatively little in the literature on humeral bone loss and its management at the time of RSA. Several authors have reported that bone loss at the time of reverse arthroplasty is associated with greater rates of poor function, prosthetic dislocation, and failure.7,8,18 This can be partially attributed to the lack of deltoid tensioning, soft tissue attachment sites, and the degree of unsupported metadiaphyseal implant. The inability to restore humeral length and achieve deltoid wrapping may particularly increase the risk of dislocation. Only 1 of 34 (3%) patients dislocated in our cohort. This represents an improvement over reported dislocation rates of 8% 1 and 34% 18 in patients with proximal humeral bone loss or deformity (ie, malunion).
Early use of anatomic-style endoprostheses for proximal humeral bone loss were associated with moderate rates of proximal migration, instability, and more limited range of motion, though the goal of preserving hand and elbow function was often met.8,13,14,16,17 Bos et al. noted a 56% instability rate (subluxation or dislocation) and 67% revision rate following anatomic-style replacements for proximal humeral tumors and nonunions. 13 Cannon et al. observed a 29% proximal migration rate with a mean active forward elevation of 42°. 14 Given the success of the RSA in patients with deficient rotator cuff tissue and proximal humeral deformity, a reverse style of implant has been used in these situations, though minimally reported.
To our knowledge, the clinical outcomes of a reverse-style proximal humerus replacing implant to address bone loss have not been reported. However, authors have reported heterogeneous results after implantation of a standard RSA in the setting of some bone loss.19,20 De Wilde et al. published one of the earliest reports of RSA following tumor resection in 2003 and reported the restoration of a stable, painless articulation. 20 Stephens et al. reported the results of standard RSA following failed hemiarthroplasty in 32 patients. The authors observed proximal humeral bone loss in 16 patients, of which 3/16 (19%) ultimately had humeral loosening, which is slightly higher than our observed rate of 13%, although direct comparisons cannot be made.
Another potential option for addressing significant bone loss is an APC, though concerns for graft nonhealing and instability remain. Chacon 6 reported the outcomes of 25 patients following APC reconstruction with an RSA, and noted an 8% dislocation rate, 17% rate of graft resorption or fragmentation, and 21% of incomplete graft-host union.
There are several important insights to be gained from this study. Firstly, we recommend cementing the humeral stem if cement was ever used in the humeral canal in a prior procedure. Of the 4 cases of humeral loosening, 2 of the patients had an uncemented SRS implanted following the removal of a cemented stem. Although the number of cases with humeral loosening was too limited to make statistical conclusions, we believe that a larger number of cases might result in a statistically significant finding. Secondly, a larger number of cases might also demonstrate a strong correlation between humeral loosening and an increasing number of prior arthroplasties.
The data from this study suggest that the use of a proximal humeral replacement when performing an RSA in the complex setting of substantial proximal humerus bone loss results in improved pain outcomes with a low dislocation rate. Humeral loosening remains a concern, especially when these implants are used in the setting of revision shoulder arthroplasty. The data from the study also suggest that when proximal humeral replacement implants are used, revision humeral components should be cemented in the setting of a previously cemented stem.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: John W. Sperling, MD: Royalties: Zimmer-Biomet, DJO, Wright Medical Technology; Paid Consultant: Exactech; Journal of Shoulder and Elbow Surgery and SLACK: Editorial or Governing Board.
Joaquin Sanchez-Sotelo, MD: Royalties: Journal of Shoulder and Elbow Surgery, Elsevier; Paid presenter or speaker: Stryker, Merck; Editorial or Governing Board: Journal of Shoulder and Elbow Surgery.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
All studies were performed in accordance with the ethical standards in the 1964 Declaration of Helsinki.