
Abstract
Background
The Grammont-style reverse shoulder arthroplasty (RSA) has demonstrated complications intrinsic to its design such as tuberosity fracture and scapular notching. A new short-stem press-fit humeral component with an onlay tray has been devised to avert these issues. We hypothesize that the clinical outcomes and rates of humeral complications of this new stem will be comparable to those of the traditional Grammont design and the lateralization obtained from the stem’s lower neck-shaft angle will decrease the rate of notching without creating instability.
Methods
We retrospectively evaluated 100 patients who underwent RSA with an onlay short-stem humeral component with a minimum follow-up of 2 years. Clinical outcomes as well as standard radiological examinations were documented pre- and postoperatively. Several correlations were analyzed.
Results
At mean 32.6-month follow-up, the cohort demonstrated a significant improvement in several outcomes: Constant score increased from 25.5 to 69.7 points, mean anterior elevation increased from 82.1° to 141.9°, external rotation from 5.6° to 25.1°, and internal rotation from sacrum to the L3 vertebral level. There was a 30% rate of stem malalignment and 37% rate of scapular notching, not associated with any adverse clinical outcomes. The overall rate of complications was 15%, of which scapular fractures were most common (5%).
Conclusion
Our short-term results suggest that the clinical outcomes and rates of humeral complications are similar to those reported for the Grammont RSA, demonstrating less scapular notching, but increased scapular stress fractures and potential subsidence of the prosthesis due to the metaphyseal press-fit require further investigations.
Keywords
Introduction
Reverse total shoulder arthroplasty (RSA) is a clinically proven treatment option for several different pathologies about the shoulder, but complications can occur secondary to the inherent alteration to the joint biomechanics created by the prosthesis. Studies have shown that bone lysis, component loosening, and overall complications occur more frequently on the humeral side (1.5%–10%), and this is especially true for revision arthroplasty.1–8 The design of the inlay Grammont stem creates the potential for several of these humeral complications. For example, implantation involves reaming the metaphysis, which can damage the tuberosities. 6 In addition, the 155° neck-shaft angle causes impingement between the humeral polyethylene (PE) insert and the scapula pillar, which leads to scapular notching and PE wear debris.9,10 The difference between the neck-shaft angles of anatomic and reverse prostheses is also an obstacle to easy conversion of an anatomic arthroplasty, as the Grammont RSA required implantation of a new stem.11,12 This last point is particularly relevant as the revision of an anatomic prosthesis for secondary rotator cuff tear or glenoid loosening represents around 20% of the indications for reverse prosthesis.3,12–14
A short-stem press-fit humeral component with an onlay tray that is convertible from an anatomic to a RSA has recently been designed to avoid these aforementioned complications. The design aims to preserve proximal bone stock and the integrity of tuberosities and also has a decreased neck-shaft angle that provides lateralization and reduces impingement.
The aim of our study is to report the early clinical and radiographic results of RSA performed using the short-stem press-fit humeral component with an onlay tray with a minimum of 2-year follow-up. Our first hypothesis is that this new stem design will demonstrate clinical and radiographic results comparable to those of the traditional long-stemmed designs. Our second hypothesis is that the reduced neck-shaft angle of 145° will decrease the rate of scapular notching without creating instability.
Materials and Methods
Institutional review board approval was obtained to conduct a retrospective analysis of patients who underwent RSA at our institution. Between November 2012 and June 2014, a consecutive series of 120 RSAs were implanted by 3 senior experienced shoulder surgeons (GW, AG and LN) in 119 patients. All arthroplasties were performed using the Ascend Flex prosthesis (Tornier Inc, Bloomington, MN). The results were retrospectively collected from a prospectively gathered database.
Surgical Technique
A deltopectoral approach was used in all cases. A subscapularis (SSC) tendon tenotomy was performed for access to the joint. When possible, the tenotomy was repaired with transosseous sutures (12% had no SSC repair). The long head of the biceps was tenodesed to the pectoralis major when present.
The Ascend Flex stem (Tornier Inc) is short (66 mm to 94 mm long) and has proximal titanium plasma spray coating for metaphyseal press-fit fixation (Figure 1). Long and short stems with a polished surface finish were available for cementation, if press-fit rotational stability could not be achieved. Three different neck-shaft angles were available: 127.5°, 132.5°, and 137.5°. The Ascend Flex stem has an onlay design and can accommodate a reversed tray with low or high offset. The 132.5° neck-shaft angle was used with a 12.5° PE insert to reach a final 145° neck-shaft inclination for all cases.
(a) Ascend Flex Humeral convertible short stem. (b) Postoperative X-ray at 33 months after a BIO-RSA. Graft osteolysis type 2.
The humeral canal was sized and then compacted until rotational stability of the trials was achieved. A surface planer was then used to ensure adequate contact between the tray and humeral cut. A cemented stem was required in 20 RSAs, secondary to poor bone stock and/or insufficient rotational stability (Figure 2).
(a) Cemented short stem with a polished surface. (b) Postoperative X-ray at 29 months. Graft osteolysis type 3.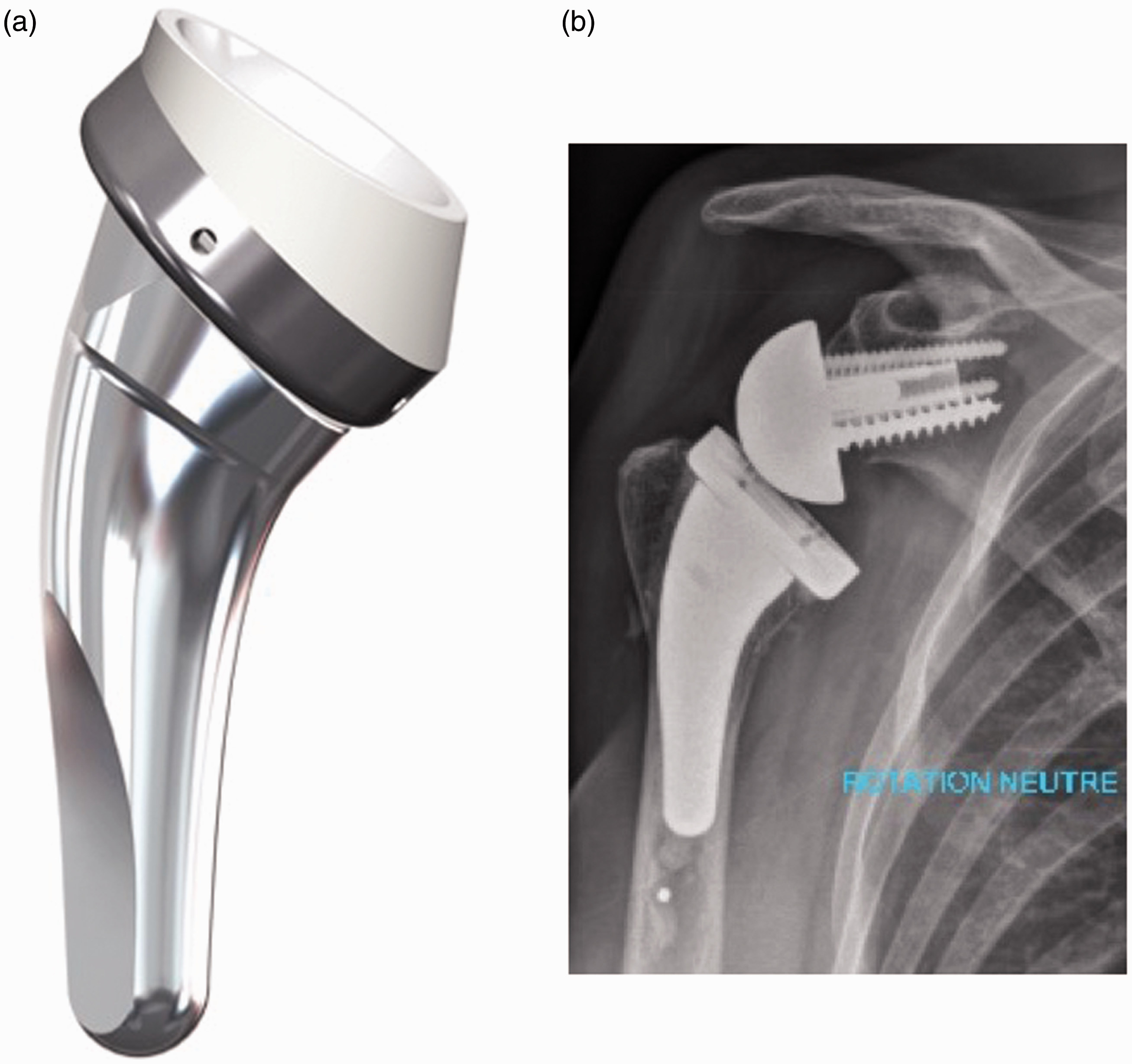
The glenoid was reamed to accept the RSA baseplate, which was then impacted and fixed with 4 screws. The Bony-Increased-Offset (BIO-RSA) 15 technique was used at the surgeon’s discretion in 53 cases for glenoid lateralization or excessive glenoid retroversion and/or superior inclination correction as well as standard or inferior offset glenospheres. The glenosphere diameters were 36 mm for females and 42 mm for males.
Clinical and Radiographic Evaluation
All patients had at least 2-year follow-up and were assessed for range of motion (ROM), Constant-Murley Score (CS), and the subjective shoulder value (SSV) score. Perioperative data (cemented or uncemented stems, implant sizes, and intraoperative complications) and postoperative complications were collected. The clinical postoperative evaluation was performed by an independent examiner not involved with the surgery (FA).
Standardized pre- and postoperative radiographic films, including a true anterior–posterior (AP) view with 3 different rotations of the arm (internal, external, and neutral) and the scapular Y-view, were obtained, according to Lévigne et al.’s
9
protocol to detect scapular notching. Three independent observers (FA, GB and PD) analyzed the radiographic data. When disagreement between observers occurred, a discussion was held to obtain an agreement. All radiographs were analyzed for alignment of the stem in neutral rotation as described by Schnetzke et al.,
16
radiolucent lines (RLL) around the stem or glenoid, loosening of either the humeral or the glenoid component, subsidence/migration, disassembly, osteolysis, fracture, glenohumeral ossifications, scapular spurs, and scapular notching using the Sirveaux-Nerot classification10,17 and/or graft resorption in cases of BIO-RSA. Graft status was analyzed on the AP plain X-rays with the arm in neutral rotation, as with notch grading.10,17 We defined the graft as “intact” when it still appeared flush to the inferior aspect of scapular pillar, and “stage 1, 2, or 3” of resorption when there was osteolysis including one-third, two-thirds, or three-thirds of the space between scapular pillar and baseplate post, respectively (Figure 3).
Graft resorption staging in Bio-RSA.
Statistical Analysis
The statistical analysis was performed using the Social Science Statistics collaborative website (http://www.socscistatistics.com). The Student’s t test for paired data was used to compare differences between preoperative and final follow-up data; the Fisher test or the Chi-square test was used to find the relationships between variables. A P value less than .05 was considered significant.
Results
Patient Demographics, Shoulder Status, and Indications for Surgery.

CTA, cuff tear arthropathy; MRCT, massive rotator cuff tear; OA, osteoarthritis; RA, rheumatoid arthritis; RCR, rotator cuff repair.
Clinical Evaluation
Preoperative and Postoperative Clinical Outcomes.

AFE, active forward elevation; CS, Constant score; ER1, external rotation with the arm at side; IR1, active internal rotation (thumb at vertebra level in points 0–10); SD, standard deviation; SSV, subjective shoulder value.
Radiographic Evaluation
Nonprogressive (<2 mm) RLL were present in 4 cases around a cemented stem and in 2 cases around the glenoid component and screws, but we did not observe any cases of humeral stem loosening or subsidence. Alignment was assessed as valgus in 19 cases, varus in 11, and neutral in 70 (Figure 4).
Evaluation of stem alignment. (a) Neutral stem position, (b) Valgus stem position and (c) Varus stem position.
Scapular notching was observed in 37% of cases, with 8% of notching grade 2 or higher (Figure 5). An inferior scapular spur was found in 26% of cases, and glenohumeral ossification occurred in 22% of cases. In the 53 cases of BIO-RSA, 39 (73.6%) had some degree of graft resorption. Of these, 20 were stage 1, 14 were stage 2, and 5 were stage 3.
Last follow-up image of a patient with preoperative acromial insufficiency, treated with the BIO-RSA technique. Stage 2 graft resorption and scapular notching stage 1 is present.
Complications and Revisions
Fifteen complications with a mean delay of 11 months (0–36 months) were observed. Five implants required revision, and 5 operations were performed involving only soft tissues. One acromion and 4 spine fractures were reported (Figure 6). There were no postoperative humeral fractures and no loosening, migration, or subsidence of the stem was observed. Complications and surgical revisions/reoperations are summarized in Table 3.
Scapular spine fracture observed at 3 months postoperatively. Complications, Reinterventions, and Revisions. ORIF, open reduction internal fixation.

Correlations
We did not identify any correlation between the above findings and any clinical outcomes. Scapular notching did not have any implication on clinical outcomes. Possible risk factors for cemented stem implantation were studied, and the patients requiring cemented stems were older (78.2 vs 72 years) and had more often previously undergone shoulder surgery (45% vs 22%), but this did not reach statistical significance. Surgical indications other than osteoarthritis were a statistically significant (P < .0001) risk factor for cementation as 6 of 8 patients with fracture sequelae and 2 of 2 patients with rheumatoid arthritis required a cemented stem.
Scapular fractures after surgery occurred in 4 of the BIO-RSA group and in 1 in the classic RSA group. The complication rate was higher in the BIO-RSA group, but this did not achieve significance. Moreover, the control group scored significantly better than the scapular spine fracture group for Constant Score and forward flexion (P < .0001), any treatment has been practiced.
A significantly lower percentage of scapular notching was observed in the BIO-RSA group (24.5% vs 51.1%) and inferior offset glenosphere (P < .05).
Discussion
The design of the traditional Grammont prosthesis may affect the stability of the humeral component and can lead to loosening, migration, or fractures as well as challenging revision scenarios.1–6,8,12,13,18 Short-stem, press-fit humeral components have been introduced to preserve humeral bone stock, to decrease the neck-shaft angle, and to provide easier and faster revision options. 19 Concerns exist though that malalignment of the component (related to stem recent design and consequently to surgeons’ experience) could potentially produce bone adaption phenomena or suboptimal ingrowth of bone.16,20 This stem is widely used in anatomic total shoulder arthroplasty with encouraging results and excellent mid-term survival reports,16,20,21 but its use in RSA is still not well studied. Our results suggest that the concept is encouraging, and this stem can be safely used in RSA as well. No humeral stem-related problems and/or reinterventions were reported in our series (fractures, loosening/migration, and disassembly), in spite of what literature attributes to the component complications (1.5%–10%) and reinterventions (12%–27%).1–8
In this series, 20% of patients required cementation for stem stability. This was attributed to both poor metaphyseal bone stock causing insufficient intraoperative rotational stability, as well as to the surgeons’ learning curve of a new concept stem. Two etiologies—posttraumatic sequelae and rheumatoid arthritis—had a significantly greater number of cemented stems. In these situations, diaphyseal stability stems or cemented stems may be a more reasonable choice than metaphyseal fixation stems.
Apart from these situations, the new convertible platform uncemented humeral stem can be a good option for several reasons: (1) long-lasting biologic fixation of the prosthesis with preservation of the bone stock and (2) easy convertibility that allows for a less demanding and time-consuming revision surgery with reduced costs. 19 By leaving the diaphysis relatively untouched, it also potentially reduces complications associated with the removal of components. 22
The results reported here confirm that the short-term clinical outcomes at an average 3 years of follow-up is comparable with those obtained with the Grammont design.5,6,9,10,12,15,17–19,22–27 This stem still requires longer term follow-up to confirm these initial findings. Interestingly, internal rotation appears improved with the short-stem press-fit component compared to the Grammont design. Patients reported an average internal rotation (IR) score of 6 points out of 10 (thumb at L3 vertebra), and 42% had active IR corresponding to the level of T12 or higher, that is the most meaningful clinical improvement compared to older RSAs.12,24,25,27 The external rotation also improved by 19.5° at the final follow-up compared to preoperative scores, despite the high rate of preoperative infraspinatus and teres minor fatty infiltration and atrophy. These are probably due to the lateralized design of the implant and the neck-shaft inclination angle of 145°, which can provide a larger impingement-free range of rotation.24,25,28,29
The scapular notching rate is reported to be greater than 50% in most series.1,3,4,7–9,12,17,23,28,30 Our results demonstrated scapular notching in 37% of cases, and only 8% were Grade 2 or 3 at short term, detected with the X-ray–specific protocol 9 ; these data confirm a recent systematic review 28 that demonstrated a reduction in notching incidence with a lower neck-shaft angle compared to Grammont RSA cited series, whereas other literature reports of 135° stems 28 proved even better results (but some series had shorter follow-up and/or not standardized notching investigation X-rays). Furthermore, when BIO-RSA and an inferior offset glenosphere were used,15,26,30 the scapular notching rate was even lower (Figure 5).
To our knowledge, there are only limited reports in the literature on the use of short RSA stems.31,32 Giuseffi et al. 31 assessed the outcomes of 44 short, uncemented stems for RSA with a mean follow-up of 27 months. Clinical outcomes were similar to our results, with a mean AFE of 142°, ER1 of 45°, and Neer modified scores that rated excellent in 61.4%. They reported a 6.8% rate of scapular notching and no radiographic evidence of loosening in any patient. As in our study, they used the deltopectoral approach in all cases, which may make easier inferior glenosphere placement that protects against scapular notching. Our rate of notching was higher, which we attribute to our longer follow-up time. Levy et al. 32 also demonstrated their mid-term (average of 50 months) results of a metaphyseal stability short-stem RSA in 98 patients that similarly had good final outcomes. In this series, the average SSV was 85%, the scapular notching rate was 21.4%, and scapula fractures occurred in only 2% of patients (which was lower than our results of 5%).
We did not observe more overall complications or reoperations than is reported,1–4,6,8 with the exceptions of acromion and spine fractures. In our series, the rate of scapular fractures after RSA (Figure 4(B) and (C)) was 5%, which is a higher percentage compared to the classic reverse designs reported in the literature1,3,4,8,12 and negatively affected outcomes (Constant Score and forward flexion) in our series, whichever treatment has been adopted. This increased number of postoperative stress fractures could be secondary to the greater lateralization and forces induced by the curved offset humeral stem.33,34 Importantly, the same higher rate of scapular fracture has also been reported with the other equivalent onlay platform (Equinoxe System, Exactech Inc, Gainesville, FL). 35 Further studies to assess this finding are necessary, since worse results are expected.
Our study has several limitations. First, this study has the shortcomings inherent to a nonrandomized and retrospective study, but our clinical and radiological assessments were standardized. The 2-year follow-up remains insufficient to assess long-term clinical and radiographic outcomes; longer follow-up is necessary to evaluate these results and to study the stem convertibility and the press-fit concept. Although the patients underwent surgery by 3 different experienced high-volume surgeons, the surgeries were performed at the same shoulder center using similar clinical indications, surgical technique, and the same implants. The study includes a consecutive series of RSA in different etiologies and, therefore, several configurations of glenoid bone loss, treated or not by BIO-RSA technique; it could be a limitation for new stem analysis, but it allows a homogeneous population of patients. Furthermore, the series includes early uses of the prosthesis, and thus the surgeons’ learning curve with the use of the short new stem was a factor in the outcomes as well. Our numbers may also be insufficient in detecting the clinical correlations of the radiographic findings described in this study. Lastly, our results suggest that this short-stem press-fit humeral component can be used to treat several etiologies, but the results cannot be extrapolated to use in cases of acute fracture, fracture nonunion, or revision.
Conclusion
Our results suggest that the use of a short-stem press-fit humeral component in RSA is encouraging and comparable to the traditional Grammont design in the short term. With 3 years of mean follow-up, the outcomes are comparable to the literature, and we did not observe a higher risk of complications or mechanical problems. We did find improvements in internal and external rotations as well as a lower scapular notching rate, which we attribute to the decreased humeral neck-shaft angle (in addition to the BIO-RSA technique and to the use of an inferior offset glenosphere), without invalidating implant stability. Mid- and long-term results are necessary to compare with the Grammont design and to ensure that similar outcomes will continue. The increased number of postoperative stress fractures of the scapula in this series, however, requires careful investigation.
Footnotes
Authors' Note
We confirmed good short-term results for this new concept stem in Reverse Arthroplasty, with the only remark of higher scapular fractures.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Lionel Neyton receives royalties and fees for consulting from Wright-Tornier and fees for consulting from Arthrex. Arnaud Godeneche receives royalties and fees for consulting from Wright-Tornier and FH societies and fees for consulting from Arthrex and Conmed societies. Gilles Walch receives royalties from Wright-Tornier company and equity from Imascap.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.