
Abstract
Introduction
Reverse total shoulder arthroplasty (RTSA) procedures are becoming increasingly more common. While the main complications are known, the management of clavicle fractures in patients with an ipsilateral RTSA is not well described. There are three case studies that document clavicular stress fractures following RTSA with an atraumatic etiology, and to our knowledge, no studies have described a traumatic clavicular fracture following RTSA.
Case
We describe the case of a 75-year-old woman with a traumatic clavicle fracture five years after RTSA for rotator cuff tear arthropathy. With minimal pain and subjective symptoms initially, the patient wished to pursue non-operative treatment. However, she eventually developed a painful non-union and pseudoparalysis of the shoulder with serial radiographs demonstrating progressive superior scapular tilting and scapular notching. Subsequent open reduction internal fixation of her clavicle fracture significantly improved her pain and function.
Conclusion
We report a traumatic clavicle fracture in the setting of RTSA that not only failed to heal but also resulted in scapular notching and shoulder pseudoparalysis that was improved with surgical stabilization of the fracture. It is possible that the setting of a semi-constrained RTSA, the resulting biomechanical imbalance may predispose to impaired fracture healing and non-union of the clavicle fracture.
Introduction
Over the past decade, reverse total shoulder arthroplasty (RTSA) is becoming increasingly more common.1,2 This has led to a corresponding rise in complication rates including scapular notching, infection, instability, glenoid component failure and less frequently fractures of the shoulder girdle (such as the acromion, scapular spine and clavicle).3,4
Grammont et al. 5 introduced the design for the RTSA in 1980s, which medialized the center of rotation by approximately 10 mm to increase the deltoid moment by 20%. Specifically, the deltoid fibers that were once lateral to the center of rotation, became more medial, and in turn produced abductor and/or elevator moments. This decreased the muscle forces necessary for shoulder abduction and elevation which was particularly useful in the treatment of pseudoparalysis associated with rotator cuff arthropathy.6,7 The RTSA design lengthens the deltoid and the arm is distalized by approximately 2.5 cm.3,8,9 The resulting tension at the deltoid attachment increases the risk of insufficiency/stress fractures to the acromion, scapular spine and clavicle. 4 , 9
There are three case studies that document clavicular stress fractures following RTSA with an atraumatic etiology,10–12 and to our knowledge, no studies have described a traumatic clavicular fracture following RTSA. In this case study, we present a patient with a traumatic clavicular fracture following a RTSA and discuss the management and outcomes. The patient was informed that information regarding her case would be submitted for publication, and she provided written informed consented.
Case Report
A 69-year-old female presented to our clinic with a longstanding history of symptomatic right shoulder rotator cuff tear arthropathy. She exhausted non-operative management including activity modification, oral anti-inflammatories, physiotherapy and multiple corticosteroid injections (Figure 1). Her physical exam demonstrated significantly limited pre-operative active range of motion: 40 degrees of forward elevation, 20 degrees of abduction, 0 degrees of external rotation (with arm adducted to the side) and internal rotation to the buttock. X-ray and CT scan imaging studies demonstrated superior migration of the humeral head, an acromiohumeral interval <6 mm and acetabularization of the acromion, consistent with grade 3 Hamada rotator cuff tear arthropathy. Due to persistent pain and dysfunction negatively impacting on her quality of life, it was recommended that her most reliable surgical option would be a RTSA. After a thorough discussion regarding the risk and benefits, she elected to move forward with the procedure.
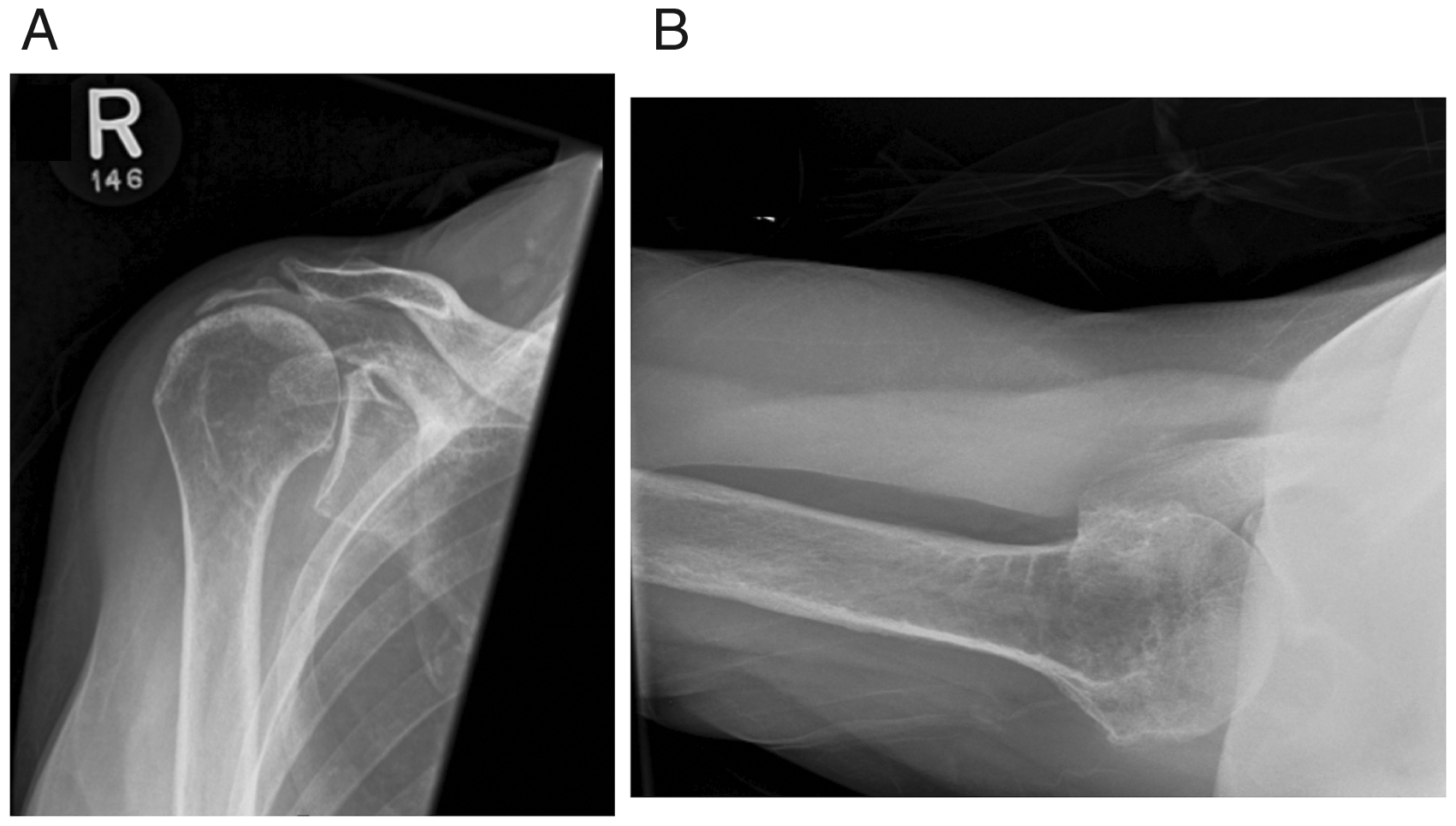
Pre-operative radiographs of right shoulder showing Hamada 3 rotator cuff tear arthropathy. A, Grashey (Glenoid AP) view. B, Axillary view.
In October 2013, a RTSA procedure was completed (Biomet Comprehensive Reverse Shoulder prosthesis (Biomet Inc, Warsaw, Indiana, USA) with a 6-mm mini cemented stem, 28-mm glenoid baseplate, 36-mm standard glenosphere (Versa-Dial between position B and C providing a 2 mm inferior offset) and a standard 44-mm humeral tray with a 36-mm polyethylene humeral cup was implanted (Figure 2). The procedure was uncomplicated. She was provided a routine rehabilitation protocol that consisted of an abduction sling and non-weightbearing in the right upper extremity for 6 weeks followed by active physiotherapy treatment to increase range of motion and gradual strengthening.

Post-operative right shoulder x-ray demonstrating reverse total shoulder arthroplasty.
She did not return for additional assessments after the 6-week clinical and radiographic check as she lived a significant distance from our hospital. Thus, her preference was to follow-up on an as needed basis and objective measures of motion and strength subsequently were not available. However, she stated she did well during this time returning to all her normal activities of daily living of self-care and house-hold tasks both at and above shoulder level maintaining independent function.
In November 2018, she sustained a mechanical fall onto her right shoulder. Repeat radiographs demonstrated an isolated mid-to-distal one-third clavicle shaft fracture without any evidence of prosthetic loosening or change in position of her RTSA implants (Figure 3). Her initial physical exam demonstrated no significant clinical deformity consisting of an ipsilateral shoulder droop, significant clavicular shortening, or an anterior rotational deformity with shoulder ptosis and/or scapular winging. Radiographically, the clavicle fracture had minimal shortening of <1cm and mild angulation. Therefore, non-operative treatment was recommended and a sling was applied for comfort with therapy to be initiated after 2 weeks to maintain motion.

Right clavicle demonstrating a displaced mid-to-distal third shaft fracture AP view at 1 week post fall.
On serial reassessments, the fracture failed to demonstrate healing on standard clinical and radiographic examinations and she subsequently developed a chronic symptomatic non-union of her right clavicle fracture (Figure 4). She had no history of bone metabolic abnormalities. At 6 months post-injury, she continued to have pain localized to the right clavicle, motion at the fracture site, as well as significantly reduced active range of motion. Her forward elevation was 60 degrees, abduction was 50 degrees, external rotation was 0 degrees, and internal rotation was limited to the greater trochanter. X-rays revealed an oligotrophic non-union of the clavicle fracture. The scapula had a notable increase in superior tilt, as demonstrated with increasing upward rotation angle with scapular measurements taken according to Endo et al. 21 and shoulder AP radiographs (Figure 5), in addition to scapular notching and exposure of the inferior base plate screw compared to her initial postoperative imaging (Figure 6). While the glenoid base plate was still noted to be stable on CT imaging, given the potential of further notching and impingement leading to progressive glenoid loosening and persistent symptoms, the decision was made to proceed with operative fixation of her clavicle fracture.

Failure of non-operative management. Right clavicle x-ray demonstrating fracture non-union AP view at 6 months post fall.

Superior scapular tilt with an increase in upward rotation angle of the scapula. A, One week post fall with scapular tilt 16.6 degrees. B, One-month post fall with scapular tilt 24.8 degrees. C, Post clavicle ORIF with scapular tilt 19.3 degrees. Scapular measurements were taken according to Endo et al. 21 using a shoulder AP radiograph. Two landmarks were used create the scapular spine line and included 1) the interface between the upper border of the scapular spine and the acromio-clavicular joint and 2) the most medial aspect scapular spine. The angle between the scapular spine line and the horizontal (reference line that is parallel to the floor) represented the upward rotation angle.

Right shoulder AP x-ray and CT scan coronal views at 5 months following clavicle fracture demonstrating scapular notching + superior scapular tilt.
In May 2019, the patient underwent open reduction and internal fixation of her clavicle fracture. Her pseudoarthrosis was excised and a 3.5-mm precontoured clavicular lateral locking plate (DePuy Synthes, West Chester, PA) was used to anatomically reduce and stabilize the clavicle fracture with local autograft. Her surgery was uncomplicated.

Post-operative right clavicle x-rays at 4 months after anatomic reduction and internal fixation. A, AP view. B, Lateral scapular (Y view). C, Axillary view.

A, Initial 2 week post-operative RTSA x-ray pre-injury. B, Scapular notching with serial Grashey views in a RTSA after clavicle fracture. C, Six weeks post-operative ORIF. D, Ten months post-operative ORIF with restoration of scapular tilt comparable to pre-injury x-ray.
At her 4 month post-operative follow-up, her fracture had healed, both clinically and radiographically (Figure 7). There was no further progression of her superior scapular tilt or scapular notching (Figure 8). Her active range of motion improved, such that she was able to forward elevate and abduct to 100 degrees, externally rotate to 20 degrees and internally rotate to the sacrum.
Discussion
To our knowledge this is the first study to report on a traumatic clavicle fracture in a patient with an ipsilateral RTSA and its subsequent sequalae. However, there have been three case reports of atraumatic clavicle stress fractures in the setting of RTSA previously reported in the literature.10–12 These patients typically had an indolent course of clavicle pain and were diagnosed with insufficiency fractures of the clavicle between 6 and 40 weeks post-operatively. Interestingly, all patients, including the one in this case report, had a fracture in the mid-to-distal one third of clavicle. This may be attributed to the origin of the anterior deltoid at the lateral one-third of the clavicle. 13 In addition, it has previously been hypothesized that a RTSA can increase deltoid tension and forces at the deltoid attachments through the combined distalization and lateralization of current 3rd generation reverse prosthetic designs. 9 , 12 In our patient, this likely resulted in an imbalance of deforming forces with deltoid activation that led to excessive motion at the fracture site and her resultant non-union.
The management of clavicle fractures in patients with an ipsilateral RTSA is not well described. In the aforementioned case studies, all patients were initially managed non-operatively with immobilization. One patient went on to heal with a successful union at 8 months (Kim et al 2016), however it is important to note that this fracture was the least displaced among all cases (<100%). The remaining cases went on to non-union with one patient undergoing operative fixation 10 and the other electing for continued non-operative management. 12 In our case, the patient also failed non-operative management after 6 months and underwent open reduction internal fixation. She had successful union at her 4 month post-operative visit.
Traumatic displaced clavicle fractures in a non-arthroplasty setting is known to alter the biomechanics of the shoulder. 14 In the context of RTSA, a displaced clavicle fracture can also have important implications on implant loading and positioning. The clavicle is the only anatomical connection joining the shoulder to the axial skeleton and plays a key role in the overall alignment and stability of the forequarter. In the case report presented, we found that the scapula demonstrated superior tilting after the clavicle fracture (Figure 5). This is not surprising as the reverse prosthesis and its semi-constrained design results in significantly higher contact force loads compared to native unconstrained shoulders.15,16 The superior tilt of the scapula may disrupt normal mechanical loading, causing redistribution of contact forces such that there is a greater upward shear force of the glenoid component by the humerus, and less compressive forces in the lateral to medial direction. This can be problematic as greater upward shear forces can predispose to scapular notching and lower compressive forces can affect stability. Our patient demonstrated radiographic signs of progressive scapular notching and remodeling after sustaining the clavicle fracture with exposure of the inferior base plate screw (Figure 6). It is not clear whether this was a result of the altered scapular mechanics due to the fracture or the natural course of the arthroplasty. However, the patient had a lateralized onlay type prosthesis with a decreased neck shaft angle which have increasingly shown to reduce scapular notching. 17 Although the management of scapular notching remains controversial, there is increasing evidence that scapular notching may affect functional outcomes and result in clinical failure, such as glenoid loosening. 6 ,18–20 Thus, concern of progressive scapular notching, in addition to the patient’s symptomatic pseudoarthrosis, was one of our primary indications to treat the clavicle non-union surgically. This is an important consideration that has not previously been discussed in the three case reports on ipsilateral clavicle fractures in patients with a RTSA.10–12 More research is needed to better understand how to best manage clavicle fractures in patients with an ipsilateral RTSA and its impact on potential complications such as non-union, glenoid impingement and scapular notching, thus, decreasing the duration of disability and optimizing function.
There are limitations to this study. The patient did not follow up between 6 weeks and 5 years after her RTSA given the significant distance to travel from her remote location and patient preference for follow-up only on an as needed basis. Therefore, we could not comment on any objective measures of motion, strength or radiographic outcomes. However, during his time, she was able to return to her normal activities of daily living and there were no subjective reports of pain or dysfunction. As well, at the time of reassessment following her clavicle fracture, there was no evidence of hardware failure of her RTSA on imaging. While we observed progressive superior tilting after the clavicle fracture and hypothesized that this could be related to the disruption of the normal mechanical loads and predispose to scapular notching, the biomechanical effects of an ipsilateral clavicle fracture after RTSA on scapular notching still requires further studies. Thus, this report is not meant to draw any conclusions or recommendations but to report the case observation and potential rationale of the treatment.
Conclusion
The patient in this case report had impaired healing of an acute distal third clavicular shaft fracture treated non-operatively. This was in the setting of a prior ipsilateral RTSA that demonstrated progressive superior tilting of the scapula, scapular notching that was not present before the injury and resultant pseudoparalysis of the shoulder which was improved with surgical stabilization and healing of the clavicle fracture. While a single case report does not constitute the basis for any definitive conclusions, the biomechanical alterations in this clinical context may be important to consider and warrant further study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.