
Abstract
Purpose:
To demonstrate the differences between outcomes and complications after reverse total shoulder arthroplasty (rTSA), according to the types of lateralized prosthesis designs: glenoid-based lateralization (LG) and humerus-based lateralization (LH).
Methods:
PubMed, Embase, and the Cochrane Library databases were systematically searched for studies published before 1 April 2021, using the PRISMA guidelines. A network meta-analysis was applied for indirect comparison, incorporating studies including medialized or conventional Grammont prosthesis and each lateralized prosthesis (LG vs control and LH vs control). Out of 1,989 screened studies, 11 studies were included to compare functional scores, range of motion (ROM), radiologic outcomes, and revision rates. In addition, six articles from the included studies, which had repaired subscapularis after rTSA were analyzed to exclude the potential influence of subscapularis repair on the outcomes. The data were pooled using a random-effects model. The pooled estimates of the mean differences (MDs) and 95% confidence intervals (CIs) were calculated for continuous data, while dichotomous data were analyzed using the pooled relative risk (RR) and their 95% CIs.
Results:
The ROM, complications, and functional scores were similar between the two groups. In subgroup analysis of 6 studies involving concomitant subscapularis repair, the LH group showed higher American Shoulder and Elbow Surgeons (ASES) scores and Constant scores than the control group. Regarding the ROM, LH group showed better forward elevation than the LG group (LH vs LG: MD 10.07, 95% CI −9.05–29.19).
Conclusion:
Overall, the outcomes and occurrence of complications were not significantly different between the two lateralized prosthesis groups. However, when the subscapularis was repaired, LH prosthesis seems to be more suitable to obtain a better ASES score and ROM.
Level of Evidence:
Level III, network meta-analysis.
Keywords
Introduction
Reverse total shoulder arthroplasty (rTSA) has been used as an effective treatment option for rotator cuff arthropathy and massive irreparable rotator cuff tears. 1 However, despite the favorable clinical outcomes of the traditional rTSA prosthesis, the Grammont design has high rates of scapular notching and subsequent polyethylene wear in long-term follow-up. 2 The medialization of the center of rotation and the 155° neck shaft angle of the Grammont style rTSA can also lead to several additional limitations, including decreased range of motion (ROM) without impingement, decreased tension of the intact cuff (associated with potential instability and weakness in external rotation), and altered anatomic contour of the shoulder. 3
Therefore, there have been efforts to decrease the scapular notching and improve biomechanics in rTSA, including modification of the implant position or design, such as lateralization. 4 Several studies have investigated the effects of lateralization, and a recent systematic review showed decreased scapular notching and increased external rotation with these recent lateral offset prostheses.4,5 However, there has been significant limitations arise from a variety of products and types of the lateralized prosthesis used. And it makes difficult to draw clear conclusions when demonstrating the effectiveness of the lateralized prosthesis over the conventional Grammont design. 6 Furthermore, a direct comparison has not yet been performed between the glenoid lateralization and humeral lateralization.
As lateralization can be achieved on the glenoid side, humeral side, or both, understanding the benefits or disadvantages of each mode of lateralization may be important for choosing the proper implant based on the patient’s individual anatomy. 2 Therefore, we reviewed the published literatures to demonstrate differences in outcomes and complications after rTSA between the glenoid-based lateralization group (LG group) and the humerus-based lateralization group (LH group). We hypothesized that both LG- and LH-designed rTSA systems were not significantly different in terms of functional, radiological, and revision rates.
Materials and methods
Search strategy and study selection
This systematic review was performed on the outcomes and complications after rTSA using a lateralized center of rotation (COR) prosthesis and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines and Cochrane Reviews.7,8 A comprehensive literature search was performed in PubMed, Scopus, and the Cochrane Library from January 2005 to April 2021. The search identified articles published until 1 April 2021, using an a priori search strategy.
Two authors independently screened titles and abstracts by the literature search. Texts of potentially relevant studies were included based on eligibility criteria. If the title and abstract did not provide adequate information to determine whether the eligibility criteria were met, the study was included for full text review. Then, the same two authors independently assessed the full-text studies according to the inclusion and exclusion criteria. If no consensus was reached, the senior shoulder expert as the third reviewer decided as the final authority after discussion. The following search terms were used: “rTSA” OR “reverse TSA” OR “reverse arthroplasty” OR “reverse shoulder arthroplasty” OR “reverse total shoulder arthroplasty” OR “reverse shoulder replacement” AND “arthritis” OR “osteoarthritis” OR “rotator cuff tear” OR “cuff tear” OR “rotator cuff tears” OR “cuff tears” OR “cuff tear arthropathy” OR “rotator cuff tear arthropathy” OR “massive cuff tear” OR “massive rotator cuff tear” OR “massive cuff tears” OR “massive rotator cuff tears” OR “proximal humerus fracture” OR “humerus fracture”. There were no restrictions on language or publication year. After the initial electronic search, relevant articles and their bibliographies were manually searched (Figure 1). Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram for the identification and selection of studies included in the meta-analysis.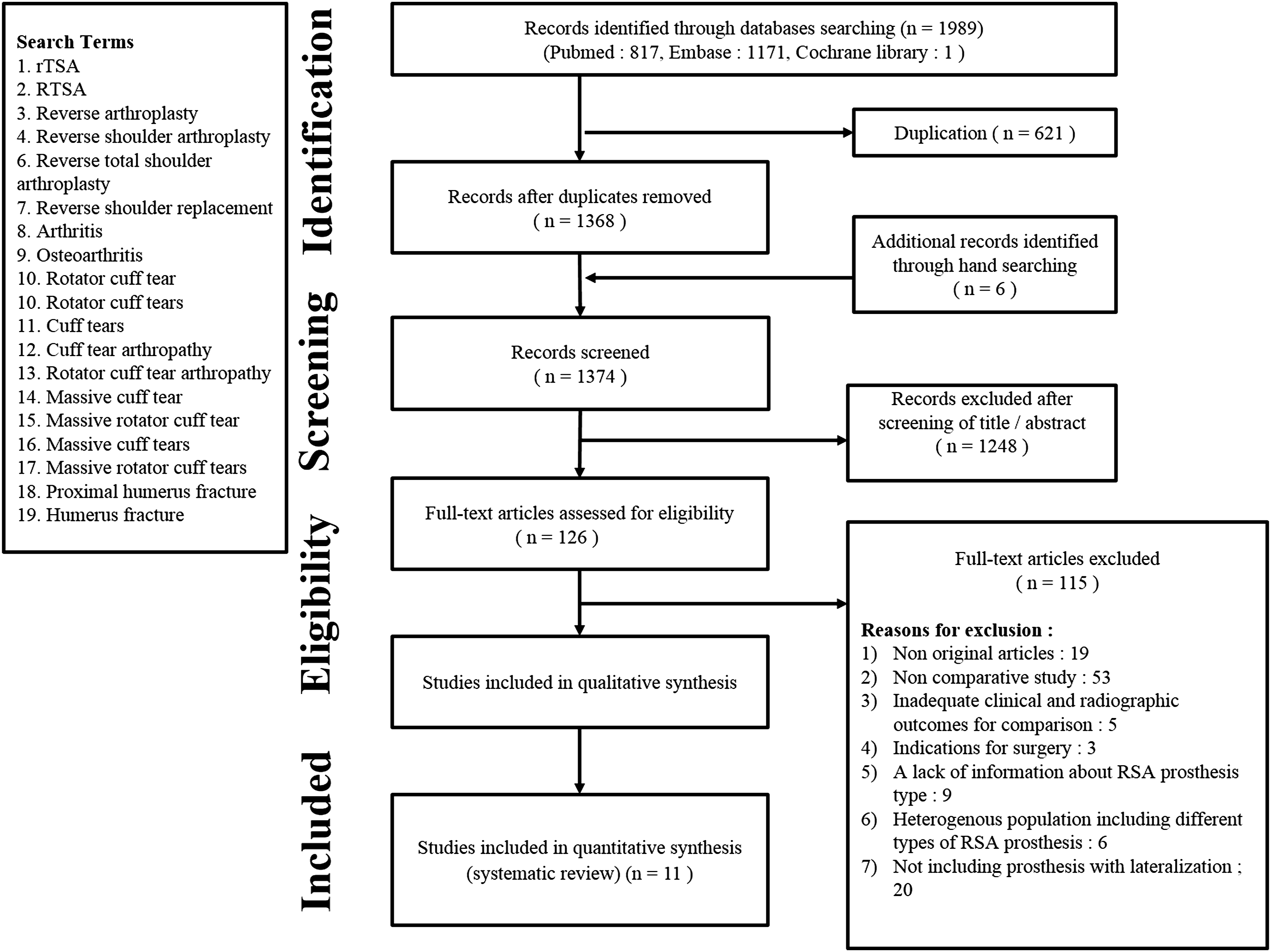
At each stage of the study selection, the κ-value was calculated to determine the inter-reviewer agreement regarding the study selection. Agreement between the reviewers was correlated a priori using the following κ-values: κ = 1 corresponded to “perfect” agreement; 1.0 > κ ≥ 0.8 to “almost perfect” agreement; 0.8 > κ ≥ 0.6 to “substantial” agreement; 0.6 > κ ≥ 0.4 to “moderate” agreement; 0.4 > κ ≥ 0.2 to “fair” agreement; and κ < 0.2 to “slight” agreement. Disagreements at each stage were resolved by consensus between the two investigators or by discussion with a third investigator, a board-certified orthopedic surgeon.
Given the lack of comparative studies published with high-quality evidence, we decided to perform a network meta-analysis with indirect comparisons, by selecting the literature, comparing the medialized prosthesis and the type of lateralized prosthesis (LG and LH).
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) original studies; (2) reverse shoulder arthroplasty for cuff tear arthropathy, massive rotator cuff tear, osteoarthritis, or fractures; (3) comparative studies including rTSA prosthesis with lateralization; and (4) studies with a follow-up period of >1 year. The exclusion criteria were as follows: (1) non-original studies (case report, surgical technical report, and in situ/cadaveric/biomechanical studies); (2) papers which had fewer than 10 participants; (3) papers which had no clinical and radiographic outcomes; (4) indications for surgery included revision shoulder arthroplasty, chronic dislocation, rheumatoid arthritis, and severe bone loss; (5) studies that included concomitant tendon transfer; (6) inclusion of only one type of rTSA prosthesis; (7) a lack of information about the rTSA prosthesis type or manufacturer; and (8) heterogeneous population including different types of rTSA prostheses, which make classification for comparison difficult.
Quality appraisal and risk of bias
Three reviewers independently reviewed each included article and decided whether to include or exclude any study based on discussion and consensus. The level of evidence of each study was determined according to the criteria stipulated by the Oxford Centre for Evidence-Based Medicine. 9 The Methodological Index for Nonrandomized Studies (MINORS) was used to assess the risk of bias of each study. 10 As there is no consensus regarding the cutoff point for MINORS assessment, a score >60% of the total score with the MINORS evaluation tool (14 of 24 points) was considered high quality.
Data extraction
The recorded data elements included the following: the study design, number of shoulders treated with rTSA, mean age, prosthesis brand, type, mean duration of follow-up, ROM, and radiological outcomes. The functional scores, including constant score and American Shoulder and Elbow Surgeons Score (ASES), were scrutinized. Any disagreements in data extraction were resolved by group discussion.
Additionally, we performed a subgroup analysis for six articles, that involved subscapularis repair after reverse arthroplasty.11-16 There has been a controversy on the role of concomitant subscapularis repair onto outcomes following shoulder arthroplasty. Therefore, we attempted to compare the outcomes of the LH- and LG-designed prostheses (functional, ROM, radiologic outcomes, and revision rates) when combined with subscapularis repair. The remaining studies from the 11 final articles were not included in this evaluation because they did not describe whether they performed subscapularis repair or not.
We compared the amount of lateralization of each offset (glenoid offset, humeral offset, and global offset) based on which of the Delta III (DePuy, WarTSAw, IN). 2 In this study, we classified into two groups (LG group and LH group) based on the lateral offset measurements and the classification described by Werthel et al. 2 Missing data (such as confidence interval and standard deviation) were requested by contacting the corresponding author.
Data analysis
We calculated the pooled estimates of the mean differences (MDs) and 95% confidence intervals (CIs) for continuous outcomes, as well as the pooled relative risk (RR) and their 95% CIs for dichotomous outcomes. The dichotomous outcomes that were not reported in the included article for complication in both design systems were not included in network meta-analysis. The estimate of the treatment effect was determined between the LG and LH by synthesizing the pooled treatment effect estimate of each treatment compared to the common comparator indirectly in the network meta-analysis. 17
Statistical heterogeneity and inconsistency were assessed with p-values and I2 statistics. A random-effect model was performed based on the result of heterogeneity and inconsistency analysis. Potential publication bias was assessed through visual inspection of funnel plots and Begg and Mazumdar’s test for rank correlation. Statistical analyses were performed using STATA version 13 (StataCorp, College Station, Texas, USA) and “netmata” package in R version 4.0.4 software (http://www.r-project.org).
Results
Study identification
The details of the study identification and selection are summarized in Figure 1. The initial electronic literature search yielded 1,989 articles; after removing 621 duplicates, 1,368 studies were screened. Additional records were included through manual searching (n = 6); of these, 1,248 were excluded after screening the titles and abstracts, and 115 were excluded after full-text review. Thus, eleven studies were eligible for qualitative and quantitative data analysis.11-16,18-22 The agreement between the two reviewers regarding the study selection was “substantial” at the title review stage (κ = 0.728), “almost perfect” at the abstract review stage (κ = 0.829), and “perfect” at the full-text review stage (κ = 1.0).
Study characteristics
Studies included in the network meta-analysis.

MINORS: Methodological index for non-randomized studies, BIO: Bony increased offset, COR: Center of rotation.
Methodological quality assessment
The MINORS score for methodological quality assessment was 19.1/24 (range, 16–22) (Table 1). Regarding the eight main evaluation parameters, 10 studies lost a point for their retrospective study design and for not clearly describing the assessments (bias) of their endpoint; one study lost a point for inappropriate descriptions about the reason for patient exclusion; three studies lost a point for an insufficient follow-up period to assess the main endpoint or possible adverse effects; eight studies lost a point due to a lost-to-follow-up rate of >5% of the initial patients, or inadequate explanation about the lost-to-follow-up rate; and eight studies lost a point as they had no or inadequate information of the size of the detectable difference of interest, calculating 95% confidence interval.
Quantitative data synthesis
Range of motion
The pooled analysis showed no significant difference in the degree of forward elevation (FE) between the two arthroplasty systems (LG12, 18-20 vs LH13-15) (mean difference [MD] = 1.03, 95% CI: Forest plot showing the difference in the range of motion: (a) FE and (b) ER. FE, forward elevation; ER, external rotation.
Functional scores
The evaluated functional scores, including the ASES and Constant score, were pooled and analyzed to compare the two systems. No significant differences were observed in ASES (Figure 3(a)), while, the LG and LH groups showed higher Constant scores than the control group (LG vs control: MD = 2.30, 95% CI: Forest plot showing the difference in the functional scores: (a) ASES score and (b) Constant score. ASES, American Shoulder and Elbow Surgeons.
Radiologic outcomes and revision rates
Scapular notching, acromial stress fracture, and glenoid loosening were reported in the included studies. In six of the studies comparing the LG with the control group,12,16,18-20,21 scapular notching was lower in the LG-type prosthesis than the control group, with a pooled relative risk (RR) of 0.40 (95% CI: 0.22–0.73, Figure 4(a)). There was no significant difference in other comparisons (LH vs control, and LH vs LG; Figure 4(a)). Four studies reported postoperative acromial stress fracture in each comparison: LG versus control,11,16 LH versus control.13,14 In comparison analysis, there was no significant difference (Figure 4(b)). Regarding the report of glenoid base plate loosening, two studies13,14 were included, and both described that LH had lower loosening than the control design prosthesis (RR: 0.29, 95% CI: 0.12–0.73; Figure 4(c)). Forest plot showing the relative risk of complications: (a) scapular notching, (b) acromion stress fracture, (c) loosening, and (d) revision.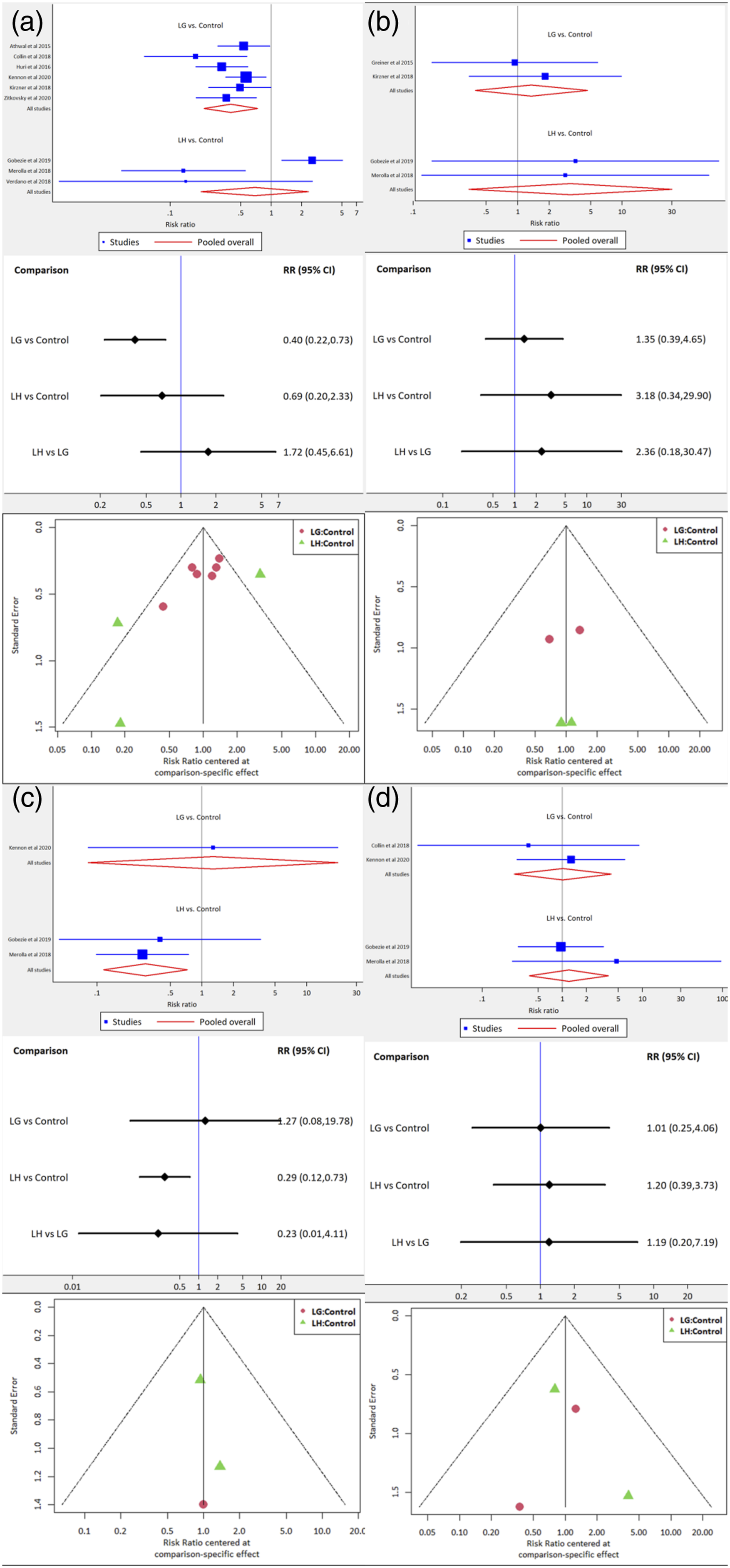
Five of the included studies reported revision11,12,16,18,19 for LG versus control, and two studies13,14 reported revision for LH versus control. Among the 255 patients in the control design prosthesis group, 9 patients (3.5%) underwent revision surgery for the following reasons: dislocation (2), periprosthetic fracture (2), acromial fracture (1), persistent instability (2), baseplate loosening (1), and infection (1). In the LG prosthesis group (159 patients), 3 patients (1.9%) underwent revision surgery for recurred dislocation (1) and infection (2). In the LH prosthesis group (69 patients), 6 patients (8.7%) had revision surgery for dislocation (3), infection (2), and broken baseplate screw (1). The overall revision rate was not significantly different between each system (Figure 4(d)).
Subgroup analysis for subscapularis repair after rTSA
In subgroup analysis of 6 studies involving concomitant subscapularis repair, the lateralized prosthesis showed similar radiologic complications and revision rates compared to the medialized system. Moreover, the LH group showed better ASES score12,14-16 and Constant score11,13,15 than control group. Compared to the LG group, the LH had a tendency to achieve higher scores than the LG group, although with no significant difference (Figure 5(a) and (b)). Regarding the ROM, the LH group showed better forward elevation than the LG group12-15 (LH vs LG: MD: 26.08, 95% CI: 8.50–43.65; Figure 5(c)). In terms of external rotation, there was no significant difference between the two groups11-15 (Figure 5(d)). Forest plot showing the difference in the functional scores and ROM: (a) ASES score, (b) Constant score, (c) FE, and (d) ER. ASES, American Shoulder and Elbow Surgeons; FE, forward elevation; ER, external rotation.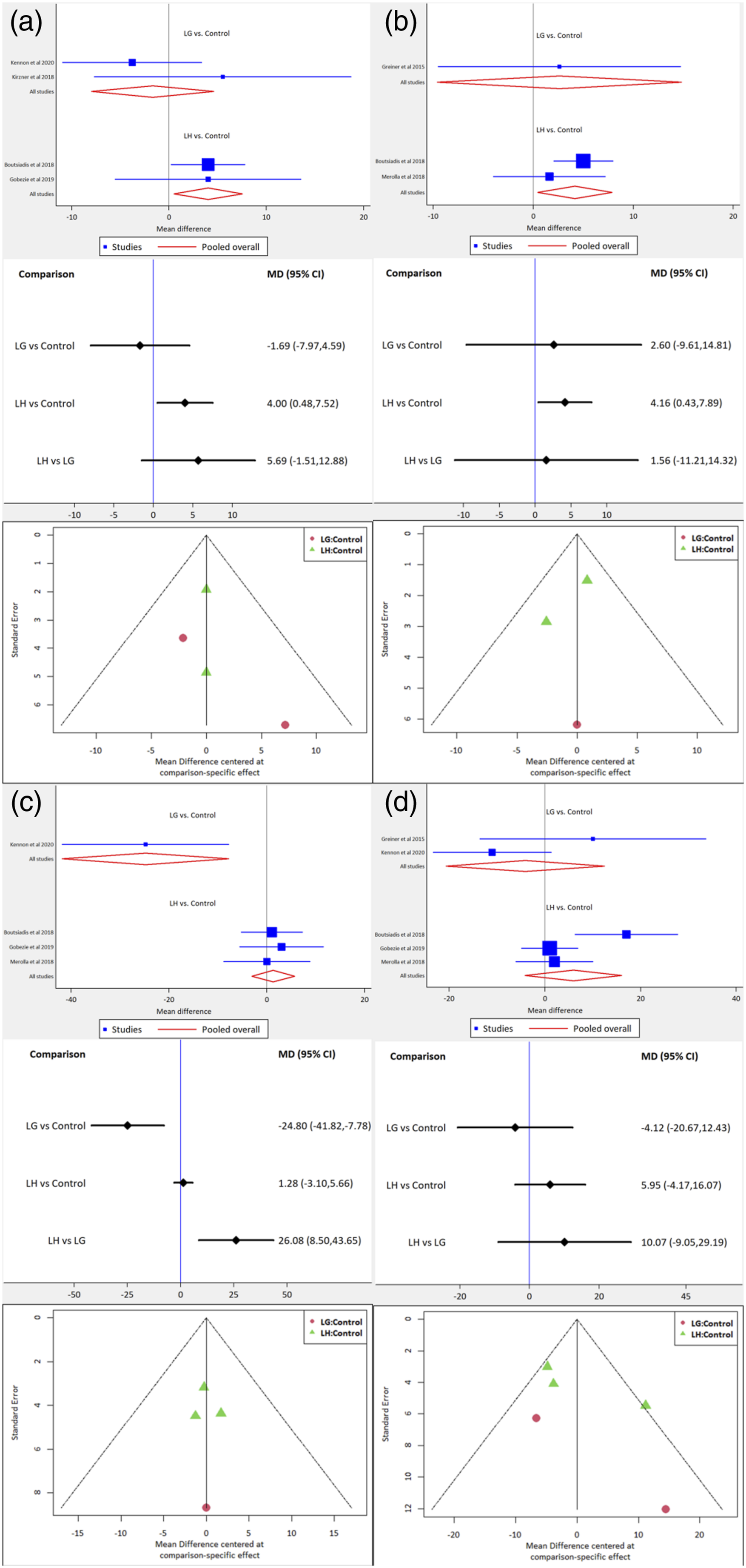
Discussion
The main findings of this study were that the LG-designed prosthesis had a lower rate of scapular notching complications than the medialized design, and the LH-designed prosthesis had less loosening than the medialized design. Both lateralized prostheses tended to achieve better Constant scores than the medialized design. In the network meta-analysis, two lateralized prostheses of reverse total shoulder arthroplasty showed similar outcomes in terms of function, ROM, radiological outcomes, and revision rates. However, if reverse arthroplasty was performed in combination with subscapularis repair, the LH-designed prosthesis had better functional scores and ROM than the LG prosthesis.
First, the constant score showed a tendency for increased scores in the LG- and LH-designed prosthesis groups than the control design group. As a result, although we expected that the difference would be significant clinically, we found no significant difference. Moreover, we were unable to demonstrate statistically significant differences in terms of ROM and clinical scores because of the heterogeneity of the available data. We assumed that the non-anatomical circumstance from reverse arthroplasty makes latissimus dorsi, and teres major tendons’ role different as internal rotators.
Second, when compared to the medialized prosthesis, both lateralized prostheses showed a decreased prevalence of scapular notching, especially the LG-designed prosthesis. The concept of lateralization for reducing the complication of scapular notching was realized. Our integrated data analysis also demonstrated that the lateralization functioned to reduce notching. Based on the previous study, which scapula notching could affect to reduce the Constant score, the tendency of increased Constant score in lateralized prosthesis could be explainable. 23
The occurrence of acromial fracture in the LG group was similar to the medialized prosthesis and the LH group. Previous biomechanical studies have highlighted concerns about the risk of acromial stress fracture with the glenoid-lateralized prosthesis, which is associated with a decrease in the deltoid moment arm and an increase in deltoid force required for abduction. 24 As the LG-designed prosthesis was developed to reduce the risk of scapular notching, it would be an optimal rTSA prosthesis while the risk of the acromion stress fracture is equivalent to either of the traditional medialized prosthesis or the LH-designed prosthesis.
Third, through our subgroup analysis, the lateralized prosthesis showed similar radiologic complications and revision rates to the medialized system. There is some controversy regarding whether the subscapularis should be repaired or not in rTSA. Some previous studies have reported that subscapularis repair in the lateralized prosthesis did not contribute to the stability of the joint. 25 In addition, there are concerns regarding whether scapular notching or osteolysis may occur because of the increased joint contact pressure, hence why we performed subgroup analysis of the articles conducting subscapularis repair. 24 However, in our study, the anticipated complications (scapula notching, loosening, and revision rates) from increased contact pressure were not increased in the lateralized prosthesis compared to the medialized prosthesis.
Moreover, the LH-designed prosthesis was the appropriate treatment choice for achieving a better functional score and ROM than the LG-designed prosthesis when conducting subscapularis repair with arthroplasty. Recently, the role of the concomitant subscapularis repair following the rTSA has been on controversy in particularly for using lateralized prosthesis, and there was no significant difference of outcomes rates between the repairing and not repairing groups.26,27 However, the previous reports were based on the analysis mixing the two different subtypes of the lateralized prosthesis (LG and LH).26,27 In the present study, we found that in contrast to the LG prosthesis, subscapularis repair seemed to play some role in the LH group in terms of improving the function and FE. We suggest some reasons based on previously published studies. First, subscapularis repair with rTSA creates a biomechanically unfavorable condition during arm elevation, owing to an increase in the force required by the deltoid and the generally weak posterior rotator cuff. 27 Since the center of rotation of the joint ends closer to the deltoid line of pull in the LG prosthesis, the deltoid’s efficiency could be decreased, even the moment arm of the deltoid could be maintained because of the lateralization at the glenoid side. 2 On the contrary, the LH prosthesis is believed to have a better deltoid’s efficiency associated with the lateralization of greater tuberosity and the increased lever arm of posterior deltoid leading to external rotation moment arm, compared with the LG prosthesis.2,24 Finally, we concluded that the concomitant subscapularis repair with the LH prosthesis may lead to increased joint stability and the effectiveness of arm elevation with well-balanced reaction forces (equal counteract of external rotation force against the internal rotation forces of the repaired subscapularis), which was not with the LG prosthesis. Therefore, along with those expectations, we thought that FE and ASES score was improved better in the LH prosthesis in our subgroup analysis.
In addition, here were no significant differences in the occurrence of complications between the LG-designed prosthesis and the LH prosthesis at an average follow-up >12 months, especially for evaluating the occurrence of implant loosening. Recent meta-analysis of humeral stem loosening after rTSA, including 75 studies, demonstrated that the prevalence of aseptic loosening was significantly higher in the group with a mean follow-up period ≥5 years compared to the group with a mean follow-up period <5 years. 28 Thus, it might be difficult to assess the occurrence of implant loosening due to the relatively short-term follow-ups and the heterogeneity of the glenoid lateralized groups.
This study is the first meta-analysis comparing the two different subtypes of lateralized prosthesis (LG and LH). Moreover, we suggested that the concomitant subscapularis repair may affect the outcomes along with the different types of lateralization. And it has not been demonstrated clinically in previous studies.
There were some limitations. First, although the number of studies investigated in our study was sufficient for analysis, there were few randomized control trials. Second, as the included studies have heterogeneity, including different study designs and indications of surgery, various implants, despite being classified as the same group, different reasons for rTSA by each case (not the same disease), and other unknown factors affecting the results of each study, this meta-analysis might have some risks of bias. Third, we assessed the outcomes comparing the groups classified according to the measurement of rTSA prosthesis offset described by Werthel et al. 2 In addition, as we classified the groups by focusing on the offset measurement of the prosthesis only, and not on the individual relative offset of each shoulder, which might be vary according to the patient characteristics, the real offset and biomechanics of the shoulder after surgery may not be reflected. Finally, the included literatures have relatively short follow-up periods for assessing the loosening of the humeral or glenosphere baseplate.
Conclusion
The outcomes and occurrence of complications were not significantly different between the two lateralized rTSA prosthesis groups. However, when subscapularis repair was performed after rTSA, LH prosthesis is likely to be more suitable to obtain a better ASES score and ROM.
Footnotes
Acknowledgements
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number : HI21C0196).
Authors’ contributions
Co-First authors: HJK and SBM
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number : HI21C0196).
Availability of data and material
The datasets used and/or analyzed during the present study are available from the corresponding author on reasonable request.
Study conceptualization
IHJ, JHS, WJY, and EK.
Data acquisition
HJK, SBM
Data interpretation
HJK, SBM, JHS, WJY, and EK
Drafting of the manuscript
HJK, and SBM
Revision and final approval of the manuscript
KHK, and KWL