
Abstract
Background
Although venous thromboembolic (VTE) events are known to develop after lower extremity surgery, there is little research on the risk of VTE after upper extremity surgery. The aim of this study is to identify the risk factors for VTE in patients undergoing open shoulder surgery.
Methods
We used International Classification of Diseases, 9th Revision, Clinical Modification procedure codes to identify patients in the Nationwide Inpatient Sample (NIS) from 1998 to 2011 who underwent open shoulder surgery. Patients were tracked to determine the incidence of VTE after surgery and stratified by demographics, comorbidities, and hospital characteristics. Risk factors were analyzed using multivariate analysis.
Results
A total of 315 423 open shoulder procedures were identified in the NIS from 1998 to 2011, of which 1420 (0.45%) carried a diagnosis of VTE, with 873 (0.27%) cases of pulmonary embolism, and 976 (0.31%) cases of deep vein thrombosis. The VTE incidence was similar in common shoulder surgeries, including total shoulder replacement (0.28%), partial shoulder replacement (0.51%), open reduction internal fixation of humerus (0.73%), and open rotator cuff repair (0.28%). Patients with VTE were older, male, African-American, and had a longer hospital stay (14.0 days compared with 3.2 days for patients without VTE). Comorbidities associated with higher risk of VTE included hypercoagulability (odds ratio [OR]: 5.62, P < .001), cancer (OR: 2.51, P < .001), congestive heart failure (OR: 2.01, P < .001), electrolyte abnormalities (OR: 2.1, P < .001), and obesity (OR: 1.46, P < .001).
Conclusions
There is a low overall risk of VTE after open shoulder surgery. Risk factors for VTE in this population should be used in conjunction with current guidelines to update recommendations for postoperative prophylactic treatment.
Introduction
Venous thromboembolic (VTE) events are known to develop postoperatively after major lower extremity orthopedic surgeries. Routine prophylaxis using antiplatelet agents, anticoagulants, or pneumatic compression of the leg has reduced the incidence of VTE after hip and knee surgery.1–4 However, indications for VTE prophylaxis for shoulder surgery are widely varied across different practices as some surgeons do not prescribe anticoagulation postoperatively while others routinely give oral or subcutaneous anticoagulation. Therefore, a thorough investigation of the incidence and identification of risk factors for VTE after inpatient shoulder surgery is needed to guide the use of routine postoperative prophylaxis or screening.
Previous studies evaluating the incidence of VTE after shoulder surgery have been limited to state databases as well as registries in Europe.5–9 These studies have shown a low rate of VTE ranging from 0.0018% to 0.734% in their respective cohorts.10,11 There have not been any studies investigating a large national population across the United States. Having data from a large cohort would allow for a thorough analysis on the incidence and risk factors for VTE after open shoulder surgery.
The purpose of this study was to determine the incidence and risk factors for VTE occurrence among patients undergoing inpatient open procedures of the shoulder using data collected from the Nationwide Inpatient Sample (NIS) database. We hypothesize that open reduction internal fixation (ORIF) of the humerus will have increased the incidence of VTE in the setting of trauma, but expect other risk factors for VTE to be similar to those identified in the general population.
Materials and Methods
Data Source
A retrospective cross-sectional analysis of patients who underwent shoulder surgeries was performed using data from the NIS and the Healthcare Cost and Utilization Project (HCUP), sponsored by the Agency for Healthcare Research and Quality. The NIS is the largest national database of all-payer inpatient discharge information, sampling approximately 20% of all nonfederal US hospitals and including approximately 9 million hospital admissions each year. Each NIS entry includes ICD-9-CM (International Classification of Diseases, 9th Revision, Clinical Modification) diagnosis and procedure codes of activity during the patient’s hospitalization at the time of discharge, as well as patient demographics, hospital characteristics, and duration of stay. More information about the NIS can be found at: http://www.hcup-us.ahrq.gov/nisoverview.jsp.
Data Extraction
All available NIS data from 1998 to 2011 were queried. Patients who underwent open shoulder surgeries were identified using ICD-9-CM procedure codes (online Appendix II). Within this cohort, patients with a diagnosis of pulmonary embolism (PE) or deep vein thrombosis (DVT) after surgery were identified using ICD-9-CM diagnosis codes (online Appendix I). The incidence of VTE was stratified according to age, sex, diagnosis, census region, primary payer class, and hospital characteristics (including size, location [e.g., urban or rural], and teaching status). Hospital size (small, medium, or large) is defined by the HCUP according to the number of short-term acute-care beds in a hospital, and it varies according to census region, location (urban or rural), and teaching status. In an urban teaching center, bed size less than 300 is small, less than 500 is medium, and over 500 is large. Data on indication for shoulder surgery were identified using primary diagnosis for admission while comorbidities were identified using ICD-9-CM coding similar to other analyses5,12 (online Appendix I).
Statistical Analysis
NIS data from the 13 years in the study period were pooled for analysis. Summary statistics were calculated for demographics, comorbidities, type of shoulder procedure, and primary diagnosis in VTE and non-VTE groups. The Pearson χ2 test or Student’s t test was used to analyze differences between various subgroups within the study cohort. Multivariate logistic regression model was estimated for the outcome of VTE adjusted for type or procedure, age group, surgical indication, gender, race, hospital demographics, length of stay, study years divided evenly, and comorbidities were used to investigate potential influences on rates of VTE. The joint significance of each group was tested with standard Wald tests. All analyses were performed using Python 2.7 (Python Software Foundation, www.python.org) and R 2.13 (R Foundation, www.r-project.org).
Results
We identified 315 423 cases of shoulder surgery between 1998 and 2011, of which 1420 (0.45%) had a diagnosis of either a PE or a DVT event (Figure 1). Of these patients, 873 (0.27%) had a PE event, 976 (0.31%) had a DVT event and 429 (0.13%) had both PE and DVT events. The mortality rate was increased in patients with VTE (0.51%) compared to those without VTE (0.03%). The incidence of VTE also increased from 0.26% in 2003 to 0.75% in 2009.
Rate of venous thromboembolic events occurring by year, 1998–2011 stratified by isolated DVT, isolated PE, either DVT or PE or both DVT and PE. VTE rate is defined as number of inpatient admissions with diagnosis DVT, PE, either DVT or PE, and both PE and DVT divided by the total number of inpatient admissions occurring in 1-year period, expressed as percentage. DVT, deep vein thrombosis; PE, pulmonary embolism; VTE, venous thromboembolism.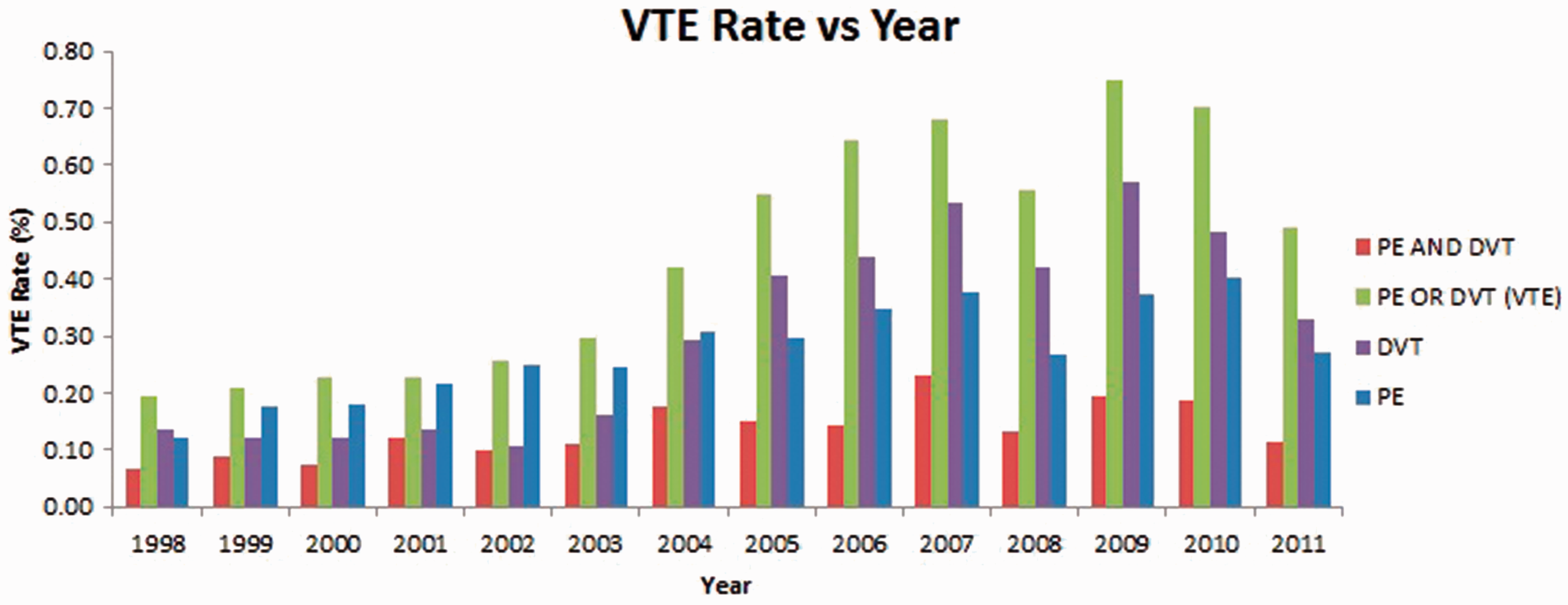
Patient Demographics
VTE Incidence According to Sex, Race, and Hospital Characteristics.

VTE, venous thromboembolism.
Indications for Surgery
VTE Incidence According to Surgical Indication.
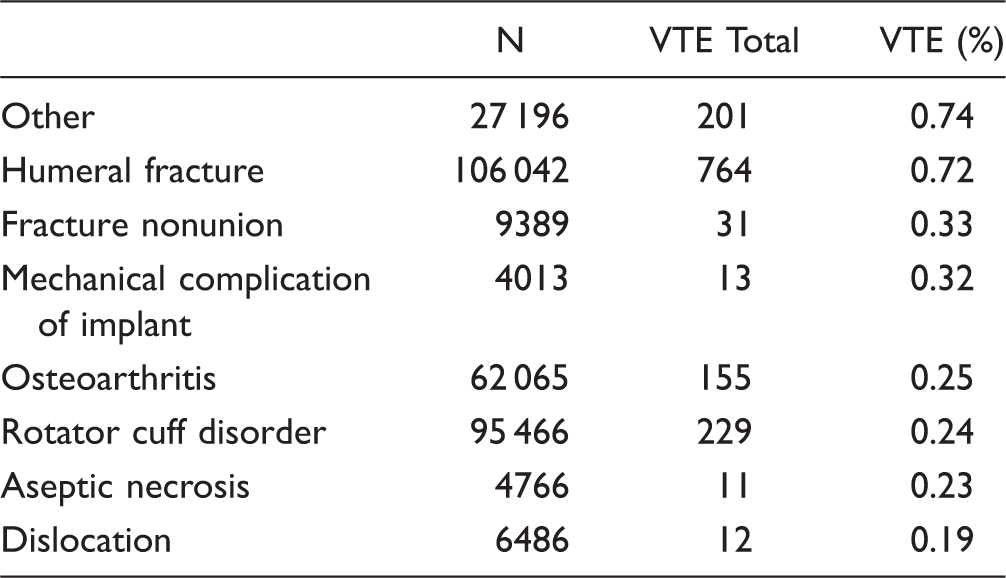
VTE, venous thromboembolism.
VTE Incidence According to Procedure Type.

VTE, venous thromboembolism.
Comorbidities
VTE Prevalence According to Medical Comorbidities.

VTE, venous thromboembolism.
Surgical Procedures
A total of 92 640 (29.4%) underwent ORIF of the humerus, of which 51 856 (16.4%) underwent rotator cuff repair, 49 686 (15.7%) underwent total shoulder replacement, and 38 676 (12.3%) underwent more than 1 shoulder surgery (Table 4). Of these patients, higher rates of VTE were found in patients undergoing disarticulation of the shoulder (3.15%), ORIF of the humerus (0.73%), and removal of shoulder prosthesis (0.70%). The VTE incidence was similar in common shoulder surgeries, including total shoulder replacement (0.28%), partial shoulder replacement (0.51%), and open rotator cuff repair (0.28%).
Risk Factors
VTE Risk Factors.

IQR, interquartile range; VTE, venous thromboembolism.
Patients with a surgical indication of humeral fracture were more likely to develop VTE compared to other surgical indications (OR: 2.37, P = .01). Age group of >75 years had higher risk of VTE (OR: 1.36, P = .005), and age group of < 25 years was less likely to have VTE (OR: 0.49, P < .001). Several comorbidities were found to be associated with higher risk of VTE, including hypercoagulability (OR: 5.62, P < .001), cancer (OR: 2.51, P < .001), congestive heart failure (OR: 2.01, P < .001), electrolyte abnormalities (OR: 2.1, P < .001), and obesity (OR: 1.46, P < .001). Factors not associated with a higher risk of VTE included chronic kidney disease (OR: 0.64, P = .017) and diabetes (OR: 0.81, P < .013). Type of shoulder surgery and medical insurance status did not impact likelihood of developing VTE.
Discussion
The incidence of postoperative VTE in 315 423 patients undergoing open shoulder surgery was 0.45%. The main risk factors identified were male sex, age greater than 75 years, African-American race, surgical indication of humeral fracture, and comorbidities of hypercoagulability, cancer, congestive heart failure, electrolyte abnormalities, and obesity. Several smaller cohort studies report varied rates of VTE associated with shoulder arthroplasty ranging from 0.0018% to 0.734% based on clinical diagnosis, and as high as 13% including subclinical VTE diagnosed via Doppler ultrasound.10,11,13 Our findings are consistent with previously reported analysis that patients undergoing open shoulder surgery are at much lower risk of VTE compared to patients undergoing lower limb orthopedic procedures.
The results of this study demonstrated that patients were almost as likely to have PE events (0.27%) as DVT events (0.31%). Of the 873 patients with PE, 49% also had DVT, consistent with literature citing that 40% to 70% of patients developing PEs also have DVT. 14 Of the 976 patients with DVT, 429 (43.9%) developed PE, which was similar to a one-third conversion rate cited in the literature.14–16
The contribution of age to risk of VTE is well described, rarely occurring in children without strong predisposing factors17,18 and increasing in risk with age following multiple different surgical procedures.16,19–21 In addition, in our analysis, male gender was a significant risk factor for VTE with OR = 1.22. This was consistent with other studies that have described males to have a mild predilection for VTE compared with women in several VTE epidemiologic studies.8,12,21
An increasing incidence in VTE from 2003 to 2009 (Figure 1) may indicate improved diagnosis of VTE since the increasing popularity of computed tomography scan pulmonary angiography in 2001. 22 Alternatively, as shoulder procedures became more common, (21 000 shoulder surgeries in 1998 vs 26 000 shoulder surgeries in 2011) surgeons may have become more comfortable operating on sicker patients. The decreasing incidence from 2009 to 2011 may indicate improved efforts to increase adherence to in-hospital prophylaxis protocol, with the advent of automated alerts for VTE prophylaxis in high-risk patients as well as implementation of programs in hospitals to assess need for VTE prophylaxis in late 2008.23,24 The incidence of having both DVT and PE remained relatively unchanged throughout the study time period, suggesting adequate treatment and diagnosis of DVT to prevent secondary PE.
The increased risk of African-Americans with VTE demonstrated in our study may be explainable by comorbidities. In the Genetic Attributes and Thrombosis Epidemiology study, compared to Caucasians who had VTE, African-Americans with VTE had higher frequencies of diabetes, hypertension, renal disease, and chronic disease. 25 Furthermore, despite having a comparable prevalence of family history of VTE between African-Americans and Caucasians, African-Americans had increased risk of VTE. This finding is likely influenced by genetic risk factors not yet identified.26,27
In the general population, strong risk factors for VTE (OR > 10) include lower extremity fracture, hip/knee replacement, major trauma, and spinal cord injury. Moderate risk factors (OR = 2–9) include congestive heart or respiratory failure, malignancy, hyperestrogenism, previous VTE, and thrombophilia. Weak risk factors (OR < 2) include older age, immobility, obesity, and laparoscopic surgery. 28 Our findings demonstrate that these risk factors are also applicable to patients undergoing open shoulder surgery. Our multivariate regression analysis found that chronic kidney disease and diabetes were not found to be risk factors for VTE when adjusting for other comorbidities. Diabetes has been reported to have increased age-adjusted incidence rates for VTE, but no clear mechanism has been identified, and no adjustments were made to account for comorbidities. 29 Patients with severe stages 3 to 4 chronic kidney disease, on dialysis, or with kidney transplant are at increased risk of VTE, but mechanisms are also unclear. 30
Finally, humeral fractures were a risk factor for DVT, and this is most likely attributable to the fact that trauma patients are more likely to be immobilized and are thought to be in an injury-related systemic hypercoagulable state. 31 In addition, patients with trauma-related humeral fractures that also had concomitant fractures were at particularly high risk of VTE (Appendix III). Although we could determine the location of the accessory fracture, it is possible that concomitant lower extremity fractures would be most likely to attribute to the increase in VTE. 32
Our study has several limitations. Large administrative databases lack data such as the use of mechanical or chemical prophylaxis, or family history of VTE. Prophylactic methods are thus a potential confounder as VTE prevention protocols vary between practices; a hospital instituting more aggressive postoperative VTE prophylaxis would result in underestimation of risk among their patients. Future studies analyzing prophylaxis measures would help further define at-risk populations. Because the NIS data set only documents events during admission, postdischarge occurrence of VTE is not accounted for and VTE incidence is thus likely underestimated in this sample. Cross-sectional retrospective data also cannot identify important temporal risk factors. VTEs occurring before shoulder surgery during the same admission are not discerned from postoperative VTE. A prospective study with proper postoperative outcomes follow-up would contribute more insight on true VTE incidence and risk factors albeit with limited study power. We are also unable to discern whether a longer length of stay resulted in higher rates of VTEs or if the occurrence of a VTE lead to a longer stay.
Conclusion
Analysis of a national database over 10 years identified a number of independent risk factors for VTE such as male sex, age greater than 75 years, African-American race, surgical indication of humeral fracture, and comorbidities of hypercoagulability, cancer, congestive heart failure, electrolyte abnormalities, and obesity. These results can be used to identify appropriate candidates for targeted VTE prophylaxis or the use of postoperative screening with Doppler ultrasound.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.