
Abstract
Background
Suicidal thoughts and behaviors are an acute public health issue, particularly among US Veterans. The interpersonal-psychological theory of suicide posits that unmet interpersonal needs, specifically thwarted belongingness (TB) and perceived burdensomeness (PB) contribute to desire for death by suicide and increased suicidal ideation (SI). However, little is known about the neurochemical correlates of TB and PB. Prior research using proton magnetic resonance spectroscopy (1H-MRS) has implicated glutamate (Glu) and glutamine (Gln), as well as gamma-aminobutyric acid (GABA), in SI and related psychiatric disorders. The current study sought to examine the relationship between thwarted belongingness and perceived burdensomeness and concentrations of Gln, Glu, and GABA in US Veterans with and without a history of SI.
Methods
In this preliminary exploratory study, 25 US Veterans underwent a two-dimensional J-resolved 1H-MRS exam to measure in vivo concentrations of Gln, Glu, and GABA in the anterior cingulate cortex. Veterans also completed the Columbia Suicide Severity Rating Scale to characterize lifetime history of suicidal thoughts and behaviors and the Interpersonal Needs Questionnaire to measure TB and PB.
Results
Reduced Gln/water was associated with increased TB and PB scores. Reduced Gln/Glu was associated with increased TB scores. Veterans with a lifetime history of SI also exhibited reduced Gln/water and Gln/Glu. Follow-up regression models showed that neither TB, PB, nor SI history were uniquely associated with Gln, but TB was uniquely associated with Gln/Glu.
Conclusion
Results provide preliminary evidence that TB and PB may be linked to abnormalities in Gln. This work further integrates biological and psychosocial perspectives on SI.
Keywords
Suicide is an increasingly urgent public health concern in the United States and around the world. The problem is particularly acute among veterans in the United States. Recent estimates found that 6407 US veterans died by suicide in 2022. 1 Twenty-four percent of male veterans and 28.8% of female veterans report a lifetime history of suicidal ideation (SI). 2 Additional research suggests that veterans may be at increased risk for SI compared to nonveteran adults. 3 Thus, identifying mechanisms that might inform novel approaches to SI treatment may be particularly beneficial to veteran populations. The interpersonal-psychological theory of suicide (IPTS4,5), one prominent psychosocial model of suicide, posits that social isolation or thwarted belongingness and feeling like a burden to others—perceived burdensomeness—increase desire for death by suicide. Parallel research exploring neurobiological mechanisms underlying SI and related conditions has implicated glutamate-glutamine and gamma-aminobutyric acid systems. 6 However, the relationships of TB and PB to these neurochemicals have not yet been explored. As an initial effort to address this gap in the literature, we conducted a preliminary exploratory investigation using proton magnetic resonance spectroscopy to evaluate the relationship between concentrations of glutamate, glutamine and gamma-aminobutyric acid with thwarted belongingness and perceived burdensomeness in a sample of US Veterans.
The IPTS asserts that for an individual to die by suicide there must first be a desire for death. This desire arises from feelings of thwarted belongingness (TB) and perceived burdensomeness (PB). TB refers to an individual's unfulfilled sense of belonging and comprises both feelings of loneliness and the relative absence of mutually caring relationships. PB reflects a belief that the individual is a liability to others and that their death may provide greater benefit than their life. There is substantial empirical evidence that both TB and PB are robustly associated with suicidal ideation (SI). Chu et al 7 conducted a meta-analysis using 122 distinct samples and thousands of participants. They concluded that TB and PB were associated with increased risk for SI. Similar findings have also been reported in samples comprised exclusively of service members and/or Veterans, highlighting their relevance to this population.8,9
While there is strong support for TB and PB as risk factors for SI, less is known about their neurobiological correlates. A deeper understanding of these correlates would help integrate psychosocial and brain-based approaches to characterizing suicidal thoughts and behaviors. 10 In recent years, research has implicated glutamatergic and GABA-ergic systems in suicide and related conditions such as major depression. Glutamate (Glu) is an amino acid that operates as the primary excitatory neurotransmitter in the central nervous system. 11 Glu is primarily synthesized from glutamine (Gln) transported from glial cells. Glu is synthesized from Gln in the presynaptic terminal by the mitochondrial enzyme glutaminase. 12 Zhao and colleagues found that expression for genes regulating Glu-Gln cycling was increased in the anterior cingulate cortex (ACC) in postmortem analyses of suicide decedents with major depression compared to decedents with major depression who did not die by suicide. 13 Other research has found altered expression of Glu receptors to be linked to suicidal behavior. 14 Consistent with genomic and postmortem research, studies using proton magnetic resonance spectroscopy (1H-MRS) to measure combined Glu and Gln (Glx) concentrations in vivo have found evidence for alterations of Glx in depression. Reduced prefrontal concentrations of Glx in patients with major depressive disorder have been observed across multiple brain regions.15,16 This idea is further supported by recent 1H-MRS investigations of Glx changes following ketamine administration. Ketamine is known to increase glutamatergic activity and work as a rapid-acting anti-depressant that reduces SI.17–20 Though few 1H-MRS studies of SI and related conditions have examined Glu and Gln separately, there is some evidence that doing so may clarify the relationship between these conditions and the glutamate-glutamine cycle. For instance, one study by Shirayama et al 21 in drug-naïve patients experiencing their first major depressive episode observed reductions of Gln in the medial prefrontal cortex, amygdala, and hippocampus. Another study examining Glx/Glu ratio (as a proxy for Gln/Glu) in the prefrontal cortex found that lower Glx/Glu was predictive of greater improvement in depressive symptoms following ketamine administration. This suggests that the relative balance of Gln to Glu may also be a marker of SI-related conditions. 22
In addition to findings for the role of Glu and Gln in suicide, research suggests that gamma-aminobutyric acid (GABA), the primary inhibitory central nervous system neurotransmitter, is related to suicide and related conditions. A meta-analysis of 1H-MRS studies found reduced GABA concentrations across different cortical regions, including the ACC, in depressed patients compared to healthy controls. 23 One 1H-MRS study by Prescot et al 24 found evidence for reduced concentrations of GABA in the ACC within a sample of female veterans with a history of suicidal thoughts and behaviors compared to those without. Another 1H-MRS study of veterans with a history of chronic pain found a positive relationship between the Glu/GABA ratio in the ACC and depression and anxiety symptoms, suggesting a possible role of excitatory-inhibitory imbalance in SI-related conditions. 25
Overall, the 1H-MRS literature suggests that Glu, Gln, and GABA metabolites are related to SI and related conditions. We sought to extend this research by exploring the associations of these metabolite concentrations with TB and PB. We conducted an exploratory preliminary single-voxel 1H-MRS study in US Veterans. We selected to evaluate metabolite concentrations in the ACC due to its central role in cognitive and emotional processing 26 as well as prior research identifying metabolite differences in the ACC associated with SI and related conditions.11,20 We expected to observe negative correlations of Glu, Gln, and GABA concentrations with higher levels of TB and PB. We also expected to observe an association between reduced metabolite concentrations and SI history. Moreover, we expected that these associations would remain after accounting for the overlap between IPTS constructs and SI history in regression analyses.
Method
Participants
The sample for the current study comprised 25 US Veterans (8 female; 15 White/Non-Hispanic) recruited from the Salt Lake City area. The average age in the sample was 38.93 years (SD = 8.97). Participants were recruited via online advertisements distributed through the local Department of Veterans Affairs (VA) medical center. To be eligible for the study, participants must have been between the ages of 18 and 55, have no reported history of major sensorimotor handicap, history of autism, psychosis, claustrophobia, or electroconvulsive therapy. Due to ethical considerations, participants were not asked to stop taking current medications.
Procedure
All participants completed a brief clinical interview and self-report protocol that included the Interpersonal Needs Questionnaire to measure TB and PB. Suicidal thoughts and behaviors were assessed using the Columbia Suicide Severity Rating Scale (C-SSRS). Symptoms of depression, anxiety, and PTSD along with alcohol and substance misuse were also assessed via self-report questionnaires. These scores were used to characterize the current mental health symptom severity in the current sample and to identify potential covariates. The C-SSRS along with all self-report measures were completed in the Research Electronic Data Capture (REDCap) platform. Lastly, participants also underwent a 1H-MRS exam to measure Glu, Gln, GABA, and other metabolite concentrations in the brain.
Clinical and Self-Report Measures
Interpersonal Needs Questionnaire (INQ-15). TB and PB were assessed using the INQ-15. The INQ-15 is a well validated instrument comprising two distinct scale scores for TB and PB. 27 The TB scale comprises 9 items (6 reverse coded). The PB scale consists of 6 items. All items were rated on a 1 to 7 Likert-type scale. After reverse coding, TB and PB are computed as sum totals for each item (One participant did not respond to one item of the PB scale. A weighted sum score was computed for this participant using the completed 5 items for this scale.). In the current sample, both TB and PB scales exhibited acceptable reliability with Cronbach's alphas of .89 and .77 respectively.
Columbia Suicide Severity Rating Scale (C-SSRS). The C-SSRS is a clinician administered assessment of suicidal ideation and behavior over the lifespan. The C-SSRS captures both lifetime suicidal thoughts and attempts as well as suicidal thoughts over the past month and suicide attempts and gestures over the past three months. Intensity of suicidal thoughts on the C-SSRS can be classified along a continuum of 1 (wish to be dead) to 5 (active suicidal ideation with specific plan and intent). For the current study, lifetime SI was operationalized as any non-zero score on the C-SSRS. We also operationalized lifetime active SI as a score of 2 or greater.
Patient Reported Outcomes Measurement Information Symptoms (PROMIS) - Depression and Anxiety Scales. Past week depression and anxiety symptoms were measured using the depression and anxiety scales of the Patient Reported Outcomes Measurement Information System (PROMIS) Adult Profile. 28 The PROMIS is a widely used instrument for assessing self-report health outcome measures across the general population and clinical populations. Participants rated each item, and totals were summed and normed automatically using REDCap software and reported as T-scores as recommended by the PROMIS developers.
Life Events Checklist (LEC-5) and PTSD Checklist for DSM-5 (PCL-5). Exposure to traumatic life events and PTSD symptoms were assessed using the LEC-5 and PCL-5 respectively. The LEC-5 contains 17 items covering potentially traumatic life events. 29 The PCL-5 is 20 item self-report inventory that corresponds to DSM-5 symptoms of PTSD. Both the LEC-5 and PCL-5 scores for the current sample were presented in another study. Please see Yancey et al 30 for a detailed discussion of the LEC-5. In brief, all participants experienced at least one traumatic life event. PCL-5 scores are reported here to provide additional detail on mental health symptoms in the current sample.
Alcohol Use Identification Test (AUDIT). Hazardous drinking was measured using the AUDIT. 31 The AUDIT comprises 10 items. The first 8 items are scored on a 0–4 scale; the last 2 items are rated as either 0, 2, or 4. A score of 8 or more is indicative of harmful or hazardous drinking.
Drug Abuse Screening Test (DAST-10). Substance abuse was indexed using the DAST-10. 32 The DAST-10 comprised 10 yes/no items that screen for substance abuse and dependence symptoms within the past 12 months.
Proton (1H) Magnetic Resonance Spectroscopy (MRS) Imaging Acquisition
Participants completed a structural magnetic resonance imaging and 1H-MRS scan on a 3.0 Tesla Siemens (Erlanagen, Germany) PrismaTM whole-body MRI scanner. High resolution, three-dimensional T1-weighted magnetization-prepared, rapid gradient echo (MP-RAGE) MR images (TR/TE/TI = 2500/2.80/1060 ms; FOV = 256 × 256; 1 mm isotropic resolution) were obtained to facilitate the position of the MRS voxel (25 × 25 × 30 mm3) within mostly gray matter of the anterior cingulate cortex (ACC). The voxel was placed along the midline to primarily cover the dorsal ACC based on midsagittal T1-weighted images with the voxel's ventral anterior edge aligned with the centroid genu of the corpus callosum. The voxel was oriented along the sagittal plane with its smallest dimension oriented in the superior-inferior dimension. Placement of the voxel is depicted in Figure 1. Within-voxel B0 shimming was completed using FAST(EST)MAP33,34 in conjunction with interactive manual shimming procedure until a full-width half-maximum (FWHM) of < 11 Hz was observed for the real component of the unsuppressed water signal. A Point Resolved Spectroscopy (PRESS) sequence was then used to acquire two-dimensional (2D) J-resolved 1H MRS spectra measurements modified to enable TE stepping; TR/TE range = 2400/31–229 ms; signal averages per TE = 4; delta TE = 2 ms; 3-pulse WET water suppression. The spectral data were recorded using a maximum-echo sampling scheme whereby the analogue-to-digital converter (ADC) on time was fixed for all 100 TE steps. 35 Outer-volume suppression (OVS) was achieved using six saturation bands positioned at least 1.0 cm away from the voxel faces. Hyperbolic secant adiabatic full passage RF pulses were used to achieve band saturation. A three-pulse water elimination through T1-effects scheme (WET) 36 was interleaved with the OVS module for global water suppression. In addition, an unsuppressed water 2D J-resolved 1H-MRS dataset was recorded from each voxel with 2 signal averages recorded for each TE step.
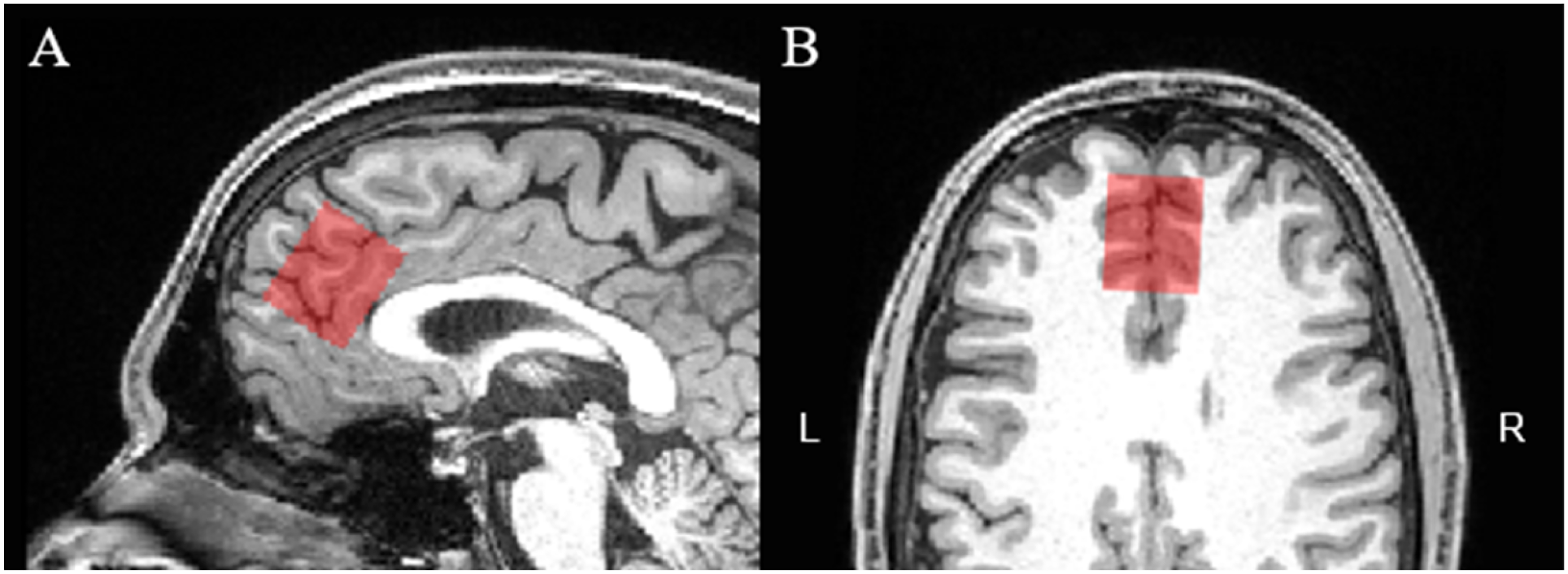
Representative Voxel Position in the Anterior Cingulate cortex Overlaid in (A) Sagittal and (B) Axial Planes by the Orange box. L = Left; R = Right.
Imaging data acquired for all participants were exported from the scanner to a secure lab server in the following formats - structural imaging data were exported as DICOMs whereas the raw 1H-MRS data were saved and transferred as TWIX data.
1H-MRS Data Processing and Quantification
All metabolite concentrations for 2D J-resolved 1H-MRS were quantified using the prior knowledge fitting (ProFit) algorithm as implemented in MATLAB (Version R2018a) without additional line broadening applied to prior spectral fitting.35,37 Before the 2D fast Fourier transformation (FFT), the raw 2D matrix was zero-filled to 200 points along the indirectly detected J dimension. The ProFit algorithm fits spectra for a total of nineteen metabolites to the raw 2D spectral surface without considering spatial localization effects including Glu, Gln, and GABA.35,37 Representative spectra extracted from ProFit are displayed in Figure 2. Raw metabolite concentrations were quantified as a ratio of metabolite/water ratios. Metabolite/water (H2O) ratios are expressed as institutional units (Iu). The reliability of measuring Glu, Gln, and GABA at 3 Tesla using 2D J-resolved 1H-MRS and ProFit has been previously established.38,39

(Top Panel) Raw 2D J-Resolved spectrum Recorded from a Single Subject and (Bottom Panel) Spectral fit Analyzed Using Prior Knowledge Fitting (ProFit). the 2D Data are Characterized by the Chemical Shift (0.2–4.2 ppm) Dimension Plotted Against the J-Resolved Axis (± 40 Hz). Signal Assignments for the Dominant Metabolite Resonances are Provided on the Bottom Panel. the Colored Horizontal Bars Indicate Approximate Primary Spectral Locations Where the Glu and Gln Protons Resonate. the Color Bars to the Right Indicate the Contour Levels (Arbitrary Units). Glu, Glutamate; Gln, Glutamine; Cr, Creatine; Cho, Choline; NAA, N-Acetyl Aspartate.
Voxel co-registration and segmentation using the T1-weighted images to determine gray matter (GM), white matter (WM) and cerebrospinal fluid (CSF) tissue composition within the MRS voxel was derived using SPM12 integrated with the Gannet software (Statistical Parametric Mapping toolbox version 3.1.5.12 (SPM12).40,41 Descriptive statistics for voxel tissue composition and cerebrospinal fluid (CSF)-corrected metabolite concentrations relative to water ratios along with Cramer-Rao Lower Bound (CRLB) values are displayed in Table 1.
Mean Tissue Composition, Metabolite/Water Ratios & CRLB Values.
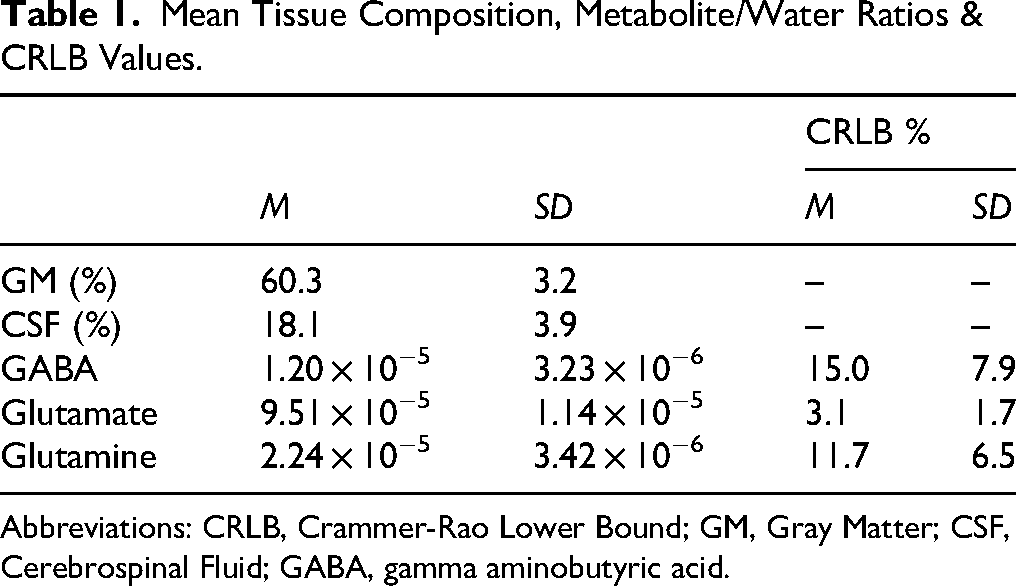
Abbreviations: CRLB, Crammer-Rao Lower Bound; GM, Gray Matter; CSF, Cerebrospinal Fluid; GABA, gamma aminobutyric acid.
Descriptive Statistics of Sample Demographic and Clinical Variables.

Abbreviations: M, mean; SD, standard deviation; CSSRS, Columbia Suicide Severity Rating Scale; PROMIS-DEP, PROMIS Depression Scale; PROMIS-ANX, PROMIS Anxiety Scale; PCL-5, PTSD Checklist for DSM-5; AUDIT, Alcohol Use Identification Test; DAST, Drug Abuse Screening Test.
Statistical Analyses
All statistical analyses were conducted in SPSS (Version 30.0). All scored and processed self-report and 1H-MRS data were evaluated for outliers using a threshold of the mean ±3 standard deviations. No outlying values were detected. Pearson correlations were used to evaluate bivariate relationships of TB, PB and SI history variables with metabolites of interest. Partial correlations were used to control for age, sex, and psychiatric medication use for significant zero-order associations with 1H-MRS metabolites. Additional correlational analyses were conducted to assess possible associations between mental health symptoms and metabolite concentrations that could account for associations of TB and PB with metabolites. Lastly, if TB and PB shared metabolite correlates with SI history and mental health symptoms, follow-up linear regressions were used to evaluate shared versus overlapping relationships of IPTS constructs and clinical variables. This study was designed as an initial exploratory analysis of possible metabolite correlates of TB and PB. Statistical significance was set at an alpha of .05. Given the preliminary nature of the current study, we report uncorrected p-values.
Results
Demographic and Clinical Characteristics of the Sample
Demographic information for the whole sample is presented in Table 2. In brief, the sample was mostly male (n = 17; 68%). The average age of the sample was 38.9 years (SD = 9.0). Sixty percent identified as White/European American; three (12%) Asian American/Pacific Islander, one person identified as more than one race. Six veterans (24%) identified as Hispanic/Latino. Sixteen participants (64%) reported taking some type of medication regularly. Six participants (24%) reported taking psychotropic medications. Additional details regarding medication use in this sample are presented in Supplemental Material A.
Descriptive statistics for clinical symptom measures are also summarized in Table 2. On the CSSRS, 44% of the sample (n = 11) denied a history of any SI. 56% (n = 14) acknowledged a lifetime history of any SI including passive ideation. Of those veterans, 6 reported wishing to be dead, 1 reported non-specific active suicidal thoughts, 3 reported SI with some intent to act and 4 Veterans reported active SI with specific plan and intent. Two veterans (8%) reported SI during the month prior to their study visit—one reported a wish to be dead, and another reported non-specific active SI. Regarding lifetime history of suicidal behaviors, four Veterans (16%) reported a lifetime history of suicidal behaviors; three Veterans reported at least one lifetime attempt and 1 reporting an aborted attempt. Zero participants reported any suicidal behavior within the past three months of their study visit. Regarding self-report symptom measures of depression, anxiety, and PTSD, participants, on average, reported mild to moderate symptoms of these conditions. Scores on the AUDIT and DAST also indicated low levels of problematic alcohol and substance use across the sample.
Correlations of TB and PB with lifetime history of SI and clinical variables are presented in Table 3. TB exhibited a positive significant correlation with lifetime SI history, r = .459, p = .021, and was positively correlated with lifetime history of active SI, albeit the correlation was not significant, r (25) = .364, p = .073. PB exhibited a positive but not statistically significant association with lifetime SI history, r (25) = .378, p = .063. However, PB was significantly correlated with lifetime history of active SI, r (25) = .532, p = .006. Both TB and PB exhibited medium to large correlations with measures of depression, anxiety, and PTSD symptoms, r's ranging from .336 to .770. Both TB and PB showed medium-small, though non-significant, positive correlations with DAST scores, r (25) = .307 and r (25) = .313 respectively, and both TB and PB exhibited very small correlations with AUDIT total scores. In the current sample, TB and PB were moderately correlated with one another, r (25) = .516, p = .008.
Pearson Correlations of TB and PB with SI History, Clinical, and Demographic Measures.

Notes: CSSRS variables dummy coded as 0 = absent/1 = present; Sex dummy coded 0 = woman/1 = man; Psychotropic Medications dummy coded as 0 = no use/1 = medication use.
Pearson Correlations of TB, PB, SI History, age, and Sex with 1H-MRS Metabolites.
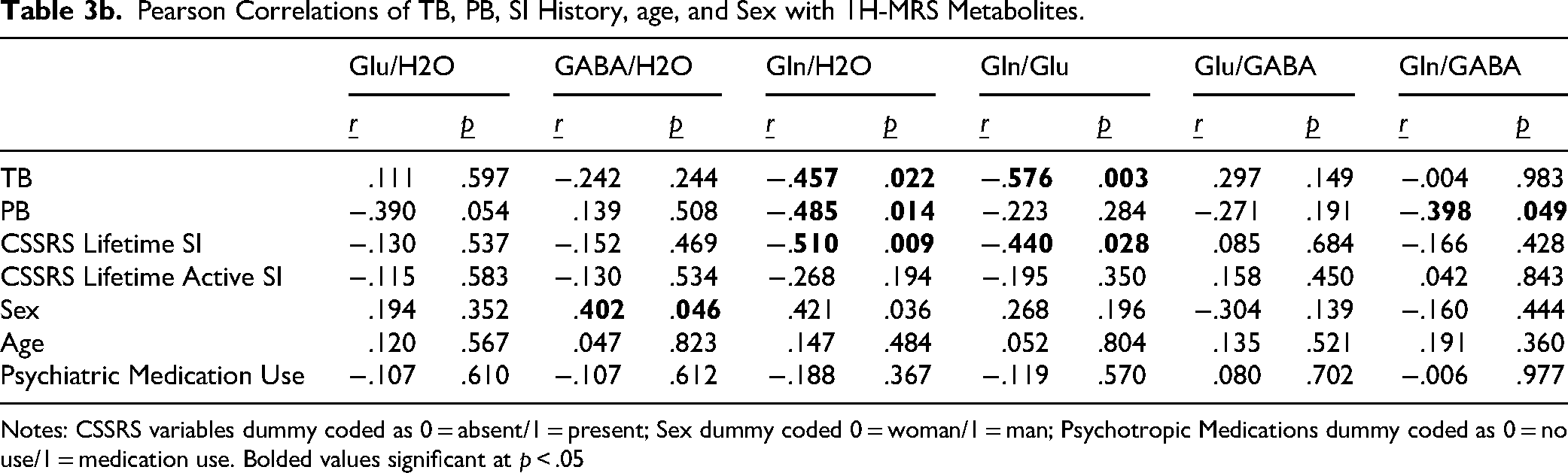
Notes: CSSRS variables dummy coded as 0 = absent/1 = present; Sex dummy coded 0 = woman/1 = man; Psychotropic Medications dummy coded as 0 = no use/1 = medication use. Bolded values significant at p < .05
Associations with TB and PB
Pearson correlation coefficients quantifying the relationships of TB and PB to metabolites of interest are presented in the first two rows of Table 4. There was a significant association between TB scores and reduced Gln/H2O, r (25) = −.457, p = .022. This relationship remained significant after adjusting for age, sex, and psychiatric medication status, rpartial (20) = −.459, p = .032. There was also a significant association between TB scores and reduced Gln/Glu ratios, r (25) = −.576, p = .003, which remained significant after controlling for age, sex, and psychiatric medication status, rpartial (20) = −.573, p = .032. Scatterplots depicting the correlations of TB with these metabolite ratios are presented in panels A and C of Figure 3. There were no other significant associations between TB scores and 1H MRS metabolites.
Regression Model Predicting Gln/H2O.

Notes: Bolded values are significant at p < .05; VIF = Variance Inflation Factor.

Scatterplots Depicting Significant Zero-Order Associations Between INQ Subscales and 1H MRS Metabolites. Red Points Represent Individuals who Scored Greater Than Zero on Lifetime CSSRS (SI+). Blue Points Represent Individuals who Scored Zero on Lifetime CSSRS (SI-). A) Association Between TB and Gln/H2O. B) Association Between PB and Gln/H2O. C) Association Between TB and Gln/Glu. D) Association Between PB and Gln/GABA.
For PB scores, there was a significant negative correlation with Gln/H2O, r (25) = −.485, p = .022, which remained after controlling for age, sex, and psychiatric medications rpartial (20) = −.534, p = .011. PB scores were also significantly associated with Gln/GABA ratio, r (25) = −.398, p = .049. However, this relationship did not remain significant after adjusting for age, sex, and psychiatric medication status, rpartial (20) = −.393, p = .071. Scatterplots depicting the zero-order relationships are presented in panels D and B of Figure 3. There were no other significant correlations between metabolite concentrations and PB scores.
Associations Between 1H-MRS Metabolites and SI History
Pearson correlations with SI history assessed via the CSSRS and metabolites of interest are also presented in Table 4. For lifetime SI history wishing to be dead (ie, a non-zero CSSRS score), there was a significant association between SI history and Gln/H2O, r (25) = −.510, p = .022. This relationship remained significant after controlling for age, sex, and psychiatric medication use, rpartial (20) = −.456, p = .033. There was also a significant association with Gln/Glu ratio, rpartial (20) = −.440, p = .028. However, this relationship fell below statistical significance after controlling for age, sex, and psychiatric medication use, rpartial (20) = −.418, p = .053. There were no other significant associations between SI history and metabolite ratios. There were also no significant associations of lifetime history of active SI with 1H-MRS metabolites.
Associations with Mental Health and Substance use Measures
Additional correlational analyses of mental health and substance use variables with metabolites of interest were conducted to evaluate if these variables shared 1H-MRS metabolite correlates with TB, PB and CSSRS variables. A table displaying correlation coefficients of all mental health symptoms measured with metabolites of interest is available in Supplemental Table B. In brief, PROMIS Depression scores were significantly associated with reduced Gln/Glu ratios, r (25) = −.433, p = .030. AUDIT scores were related to reduced Glu/H2O, r (25) = −.453, p = .023 and increased Gln/Glu, r (25) = .496, p = .012. No other correlations were significant.
Regression Analyses
Given that Gln/H2O was associated with TB, PB, and SI history at the zero-order level, a follow-up regression model was conducted to evaluate if any of these clinical or self-report measures were uniquely related to Gln/H2O concentrations. Results are displayed in Table 4. While the overall model was statistically significant, R2 = .492, p = .037, neither beta weights for TB, PB, nor SI history were statistically significant, suggesting that the co-variance among these three variables was most associated with Gln/H2O concentrations.
Similarly, another regression model was computed to evaluate the unique relationships of TB, Lifetime SI, PROMIS depression and AUDIT scores to Gln/Glu concentrations. Results are displayed in Table 5. The overall model was statistically significant, R2 = .610, p = .011. TB scores were uniquely associated with reduced Gln/Glu ratios, β = −.778, p = .011, whereas neither lifetime SI history nor depression scores were significant. The beta weight for AUDIT scores was also significant and positively associated with the Gln/Glu ratio, β = .487, p = .010.
Regression Model Predicting Gln/Glu.

Notes: Bolded values are significant at p < .05; VIF = Variance Inflation Factor.
Discussion
The current study utilized 1H-MRS to identify brain metabolite correlates of the IPTS constructs thwarted belongingness (TB) and perceived burdensomeness (PB)—two psychosocial risk factors for suicidal ideation—in a sample of US Veterans recruited from the community. Based on prior literature implicating glutamatergic and GABAergic systems in suicidal ideation, we focused our analyses on Glu, GABA and their precursor Gln. Our results indicated that TB scores were associated with reduced Gln/H2O and Gln/Glu. PB scores were also associated with reduced Gln/H2O, but not Gln/Glu. PB was also associated with Gln/GABA at the zero-order, but this association did not remain significant after adjusting for sex, age, and medication use. Lifetime history of SI was also associated with reduced Gln/H2O and Gln/Glu. Depression symptoms were associated with reduced Gln/Glu, and alcohol misuse was associated with increased Gln/Glu. This was driven largely by a positive association between AUDIT scores and Glu/H2O. Post-hoc regressions indicated that neither TB, PB or SI history was uniquely related to Gln/H2O; however, only TB was uniquely associated with Gln/Glu. Overall, these findings provide preliminary evidence for a relationship between Gln and Gln/Glu and psychosocial risk factors for SI. Though highly preliminary, replicate and extend the extant literature in several important ways.
Results from this study are also the first to our knowledge that identify a link between reduced Gln and the interpersonal-psychological theory constructs of TB and PB. The IPTS is a widely used framework for researchers and clinicians to understand the psychosocial processes that contribute to SI. Our findings provide initial evidence for overlap between these constructs and findings implicating deficits in glutamatergic systems in SI and related conditions.15–18 Moreover, study results dovetail with preclinical models showing reductions in Gln and Glu in the hippocampus of rodents raised in social isolation. 42 Another study by Yokoyama et al 43 has shown that R-ketamine administration facilitated social cognition in mice reared in isolation, suggesting that agents which alter glutamatergic systems may help facilitate social connection. In conjunction with the broader literature, our findings tentatively suggest that alterations in Gln and Gln/Glu may in part reflect a neural signature of impaired social connection that is measured by the TB and PB scales. We also detected an association between lifetime history of SI, inclusive of passive ideation, and Gln/H2O and Gln/Glu. This finding aligns with those reporting alteration in genes regulating Gln-Glu cycling in the ACC among suicide decedents. 13 It is informative that we observed differences in Gln and Gln/Glu even among those with a lifetime history of SI but little active SI. This could indicate that neurochemical markers reflect in part a more trait-like risk factor for SI that also encompasses individual differences in IPTS constructs.
A major strength of our study was the ability to examine Gln and Glu separately, using a 2D J-resolved 1H -MRS data that was analyzed using ProFit which has previously been shown to provide a reliable separation of Glu and Gln signals. 38 Prior 1H-MRS research into SI and related conditions largely relied on Glx (Glu + Gln). Our findings indicated that Gln/H2O, but not Glu/H2O, was associated with TB and PB as well as to lifetime history of SI. Gln is primarily synthesized in astrocytes and serves as a chemical precursor to both Glu and GABA. 44 The associations between reduced Gln and both TB and PB could implicate astrocyte (dys)function as a possible neural mechanism explaining these 1H-MRS findings, raising an important question for future research. We also observed more selectivity in the association of Gln/Glu with TB (ie, no association with PB). This could suggest that TB may be uniquely related to the relative balance of Gln to Glu. If replicated in larger samples, it could suggest that TB may be correlated with the glutamate-glutamine cycle.
Consistent with previous 1H-MRS studies of SI and depression45,46 in clinical populations, we found evidence for alterations of glutamatergic systems. However, these findings should be interpreted with caution given the relatively small sample size, with limited representation of active SI (n = 8). This small sample size may explain the failure to detect significant metabolite differences between individuals with lifetime active SI compared to those with no SI or a wish to be dead. Notably, we observed these associations in a community Veteran sample, which complements much of observational and clinical research in patient populations. According to the 2024 National Veteran Suicide Report, almost 40% of US Veterans who utilized VA healthcare and died by suicide did not have a documented mental health or substance use diagnosis. 1 Understanding neurobiological factors for SI outside of clinical populations may help address knowledge gaps in this population.
Limitations and Future Directions
While the current study has several notable strengths, there are also substantial limitations that should be addressed through future research. First, this study was a preliminary exploratory investigation of metabolite correlates of TB and PB. As such, the sample size is relatively small and is likely underpowered to detect small to medium effects after controlling for variables such as age, sex and psychiatric medication status. Relatedly, the small sample size limited power to detect possible interactions between TB and PB in predicting metabolite concentrations as well as moderating effects of SI history on the associations between TB and PB and 1H-MRS metabolites. Future studies in larger samples will be needed to confirm and extend these preliminary findings. Additionally, we were unable to collect comprehensive diagnostic interview data on participants’ mental health history to complement self-report data on recent mental health symptoms. Future studies in larger samples will want to test for moderating or mediating effects of mental health history on metabolite correlations with TB and PB.
Another important limitation is that the study was limited in representation of participants with SI within the past month, and there were no participants who reported a suicide attempt in the past three months. Therefore, our findings regarding differences in Gln and Glu among Veterans with SI history may best be conceptualized as reflecting biological signatures of chronic as opposed to acute risk factors. Future work examining differences in metabolites among individuals with recent SI and attempts compared to those with remote histories would be informative as there is increasing recognition of the heterogeneity among individuals with suicidal thoughts and behaviors with respect to frequency, intensity and impulsivity of these experiences. It is very likely that this heterogeneity is also reflected in unique neurobiological subtypes. 47
Lastly, due to time constraints on the MR scanner, we were only able to conduct MRS using the single voxel at the ACC. Thus, we are limited in terms of understanding the regional specificity of metabolite findings. Future studies should examine associations between TB, PB and metabolites using a single-voxel approach at multiple regions or using multivoxel techniques such as chemical shift imaging.
Conclusions
In summary, the current study represents an important preliminary step in understanding the neurochemistry of TB and PB and risk for suicidal ideation. Mapping the IPTS constructs onto neurobiological markers of increased SI risk could serve to clarify how psychosocial factors affect brain health and contribute to suicidal thoughts and behaviors. This work may refine existing interventions and support the development of novel approaches to reducing the societal burden of suicide.
Supplemental Material
sj-docx-1-css-10.1177_24705470251385745 - Supplemental material for Glutamine Metabolite Ratios are Related to Thwarted Belongingness and Perceived Burdensomeness: Preliminary Evidence from a Veteran Sample with and Without History of Suicidal Ideation
Supplemental material, sj-docx-1-css-10.1177_24705470251385745 for Glutamine Metabolite Ratios are Related to Thwarted Belongingness and Perceived Burdensomeness: Preliminary Evidence from a Veteran Sample with and Without History of Suicidal Ideation by James R. Yancey, PhD, Punitha Subramaniam, PhD, Jiyoung Ma, PhD, Chelsea N. Carson, PhD, Keenan E. Roberts, MS, Erin C. McGlade, PhD, Perry F. Renshaw, MD, PhD and Deborah A. Yurgelun-Todd, PhD in Chronic Stress
Footnotes
CRediT Author Statement
James R. Yancey: Conceptualization, Methodology, Formal analysis, Investigation, Writing-Original Draft, Project administration. Punitha Subramaniam: Software, Methodology, Investigation, Data Curation, Writing Review & Editing. Jiyoung Ma: Data Curation, Software, Formal analysis Writing-Review & Editing. Chelsea N. Carson: Data curation, Formal analysis, Writing-Review & Editing. Keenan E. Roberts: Data curation, Writing-Review & Editing, Project administration. Erin C. McGlade: Conceptualization, Writing-Review & Editing, Supervision, Funding acquisition. Deborah A. Yurgelun-Todd: Conceptualization, Writing-Review & Editing, Supervision, Funding acquisition. Perry F. Renshaw: Conceptualization, Methodology, Writing-Review & Editing, Supervision, Funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding support was provided by the Rocky Mountain Mental Illness Research, Education and Clinical Center for Suicide Prevention. The content is solely the responsibility of the authors and does not represent the official views of the VA or the U.S. Government.
Additional support was provided by the Rocky Mountain Mental Illness Research, Education and Clinical Center for Suicide Prevention. Support for author CC was also provided by the Department of Veterans Affairs Advanced Fellowship in Mental Illness Research and Treatment Program. The content is solely the responsibility of the authors and does not represent the official views of the VA or the U.S. Government.
Research Electronic Data Capture (REDCap) resources used for the research presented in this publication were supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UM1TR004409. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.