
Abstract
Background
Previous research showed acute psychedelic effects were associated with decreases in racial trauma (RT) symptoms among black, indigenous, and people of color (BIPOC). Among samples comprised primarily of white participants, positive outcomes of psychedelic experiences have been mediated by increases in psychological flexibility. Therefore, we examined whether changes in psychological flexibility from before to after a psychedelic experience mediated the relationship between acute psychedelic effects and changes in RT symptoms among BIPOC.
Methods
This cross-sectional online survey study included 313 BIPOC (mean age = 33.1; SD = 11.2; female = 57%). A multiple linear regression analysis was used to examine the association between acute psychedelic effects and decreases in RT symptoms in a nonclinical setting; a path analysis was used to explore whether changes in psychological flexibility mediated this relationship.
Results
Acute insight and challenging effects were significantly (p < .001) associated with decreases in RT symptoms following a psychedelic experience. Increases in psychological flexibility partially mediated relationships between greater intensity of psychological insight and less intensity of challenging experiences and decreases in RT symptoms (ps<.001).
Conclusion
This research suggests psychedelics confer potential benefits in decreasing RT symptoms among BIPOC and psychological flexibility may be an important mediator of these effects. Future research should test this hypothesis in a longitudinal clinical trial among BIPOC.
Introduction
Trauma and stressor-related disorders are a common mental health consequence following a traumatic event. 1 One form of trauma underrepresented in empirical investigations is racial trauma,2,3 defined as traumatization due to distressing experiences that can include physical or psychological threats to oneself or witnessing such threats to another based on race or ethnicity. 3 According to the US Department of Justice, many people of color (POC) have experienced some form of racial trauma in their lifetime. 4 The public health burden of trauma includes trauma symptoms that are significantly predicted by overt and subtle racial discrimination, 5 and the development of posttraumatic stress disorder (PTSD) symptoms or a PTSD diagnosis due to the cumulative effects of ongoing racial discrimination.6–8 Although several efficacious treatments exist for PTSD (eg, prolonged exposure 9 and cognitive processing therapy 10 ) existing treatment studies largely do not address the role of race or ethnicity. 11 Furthermore, evidence shows that treatment dropout rates are high among POC.12,13 Thus, the development of treatments for racial trauma is sorely lacking.
One emerging research area has examined the psychotherapeutic action of psychedelic compounds (eg, psilocybin and lysergic acid diethylamide [LSD]). These substances have been administered in clinical trials14–17 and used in naturalistic settings18–20 as potential treatments for mental health problems. These substances act primarily as serotonin receptor (eg, 5-HT1A/2A/C) agonists, often producing profound changes in sensory perceptions, cognitions, behavior, and mood. 21 For example, recent clinical studies examining psychedelics administered with psychological support have demonstrated efficacy in decreasing symptoms of anxiety and depression,15,17,22–25 and several survey and observational studies have reported decreases in depression and anxiety occur following psychedelic use in ceremonial and recreational contexts.19,20,26,27 Although more research is needed, the beneficial effects of psychedelics appear to be associated with the intensity of acute subjective effects. For example, several published studies have shown the importance of the acute mystical-type (measured with the Mystical Experience Questionnaire [MEQ])28,29 and acute insight (measured with the Psychological Insight Questionnaire [PIQ] 30 ) in both healthy19,28,31,32 and clinical24,25,30,33,34 populations.
Although recent clinical trials have found positive effects of psychedelic-assisted therapy on mental health outcomes, samples are small and have lacked inclusion of POC. For example, out of 18 published randomized controlled trials on psychedelic-assisted therapy, the large majority of participants were non-Hispanic White (82%) with low percentages of POC (eg, 3% black; 2% Latina; 2% Asian; 5% Indigenous; 5% mixed race). 35 Although the lack of representation in these studies may have been related to lack of cultural inclusivity in the research community, stigma about mental health issues, or study recruitment methods, and the lack of POC in these studies substantially limits generalizability of findings. Because POC may also use licit and illicit substances to cope with the sequelae of racial trauma symptoms,36,37 they may seek out novel substances, including psychedelics, if they do not have access to empirically supported treatments or when those treatments have not been effective. Highlighting this phenomenon, a recent online survey study 21 examined how the use of psychedelics in the natural ecology affected subsequent psychopathology among a sample comprised solely of POC. Results showed significant and large reductions in the intensity of traumatic stress, depression, and anxiety symptoms from the 30 days before to the 30 days after a referent psychedelic experience. Additionally, there was a significant canonical correlation (Rc = 0.52, p < .001) between a dimension of the acute mystical-type and insight effects as well as acute challenging experiences (measured with the Challenging Experiences Questionnaire [CEQ] 38 ) and decreases in subsequent psychopathology.
Because the evidence presented above suggests that psychedelics can lead to beneficial outcomes when administered in clinical and naturalistic settings, and emerging evidence shows that psychedelic use is related to reductions in race-based trauma symptoms among POC, potential mediators of psychedelic effects on therapeutic outcomes could help increase understanding the mechanism underlying such effects. Previous studies suggest changes in the entropy of brain network connectivity, 39 the experience of awe/ego dissolution,40,41 and changes in psychological flexibility30,42–46 may mediate therapeutic outcomes following a psychedelic experience.
Psychological flexibility (measured by the Acceptance and Action Questionnaire-II [AAQ-II]47,48) is described as a set of psychological processes that help people manage stressors and engage in adaptive behaviors promoting value-driven action. 49 Thus, psychological flexibility is a transdiagnostic construct wherein people are believed to have the capacity to recognize and adapt to various contextual demands, shift their mindset or behaviors during individual and social experiences, maintain balance across important life domains, and learn to be open to, aware of, and committed to behaviors congruent with their values. 50 According to the model, well-being would be supported when an individual fully contacts the present moment as a conscious human, and changes or persists in value-driven behavior, despite negative feelings that may be present for them in each moment. 51 Conversely, dysfunctions in psychological functioning, including mental health problems such as race-based PTSD,6–8 could be theorized as the result of reduced psychological flexibility (or psychological inflexibility), in which individuals may struggle to maintain value congruent behavior in the face of challenging emotional responses related to past racial trauma. Importantly, psychological flexibility is a broad term that includes aspects of experiential avoidance, which is theoretically related to maladaptive responses to trauma through avoidance of thoughts and feelings related to the trauma. 1 Indeed, several PTSD symptom clusters (reexperiencing, avoidance, and physiological hyperarousal) have also been associated with higher AAQ-II scores (eg, Hosseini Ramaghani et al, 52 Meyer et al, 53 and Tull and Roemer 54 ), and thus, one could expect that symptoms of racial trauma and psychological flexibility might also be correlated.
To date, no study has yet looked at the relationship between psychological flexibility and the experience of race-based trauma. However, a recent investigation 30 explored whether psychological flexibility mediated the outcomes of psychedelics on depression and anxiety symptoms among a large primarily White sample of 985 online survey respondents who used psychedelics. Results indicated that the intensity of acute drug effects (ie, mystical-type and insightful effects) was significantly associated with decreases in depression/anxiety following the psychedelic experience, and a path analysis showed that increases in psychological flexibility fully mediated the effect of mystical-type and insightful experiences on decreases in depression and anxiety. Furthermore, a recent prospective study 55 found that psychological flexibility (measured with the AAQ-II47,48) improved from pre- to postpsychedelic experience and that these changes were correlated with decreases in depressive symptoms. Results also showed that the acute psychedelic effects (mystical experience and emotional breakthrough) were associated with greater improvements in psychological flexibility. 55 Another report 56 showed that psychological insight (measured with the PIQ 30 ) was significantly correlated with retrospectively reported increases in psychological flexibility that occurred from pre- to postpsychedelic experience. Although emerging evidence suggests that acute insight experiences may be highly correlated with therapeutic outcomes,23,30 it is important to consider that these effects usually occur in the context of a mystical-type experience and prior studies that have modeled this relationship have controlled for the moderate to large correlation between these variables. 30
Taken together, these findings suggest that psychological flexibility may be an important mediator of the acute effects of psychedelic drugs on therapeutic outcomes. Therefore, this study sought to examine psychological flexibility as a mediator of the relationship between acute psychedelic effects and changes in racial trauma symptoms among POC. Because prior research showed that acute psychedelic effects (mystical type, insight, and challenging) are associated with reductions in trauma symptoms in this population, 21 that psychedelic effects are associated with changes in psychological flexibility, 30 and that increases in psychological flexibility are associated with positive mental health outcomes.30,57 Firstly, we hypothesize (Hypothesis 1 [H1]) that a multiple linear regression model will show that acute psychedelic effects (mystical-type, challenging, and insight effects) will be associated with changes in racial trauma symptoms following a psychedelic experience. Secondly, we hypothesize that a path analysis model will show that acute psychedelic effects will be directly related to changes in psychological flexibility (H2), that changes in psychological flexibility will be directly related to changes in racial trauma symptoms (H3), and that psychological flexibility will mediate the relationships between acute psychedelic effects and changes in racial trauma symptoms (H4).
Methods
Procedure
The present study includes data from a larger cross-sectional, observational study among POC. 21 Eligibility criteria included being at least 18 years old, able to read and understand English, having used a psychedelic that produced psychoactive effects, experienced relief from racial discrimination after taking the psychedelic, and currently reside in Canada or the United States. During September of 2019, potential participants clicked an electronic advertisement sent directly from Qualtrics. Potential participants were recruited by the Qualtrics team as they were all members of their research panels. 21 They were then presented with the informed consent document and led to a secure online survey to complete their questionnaire. Eligible participants were asked to report their past racial trauma experiences, experience of psychedelic use and its acute and enduring effects, and mental health symptoms. After data cleaning (ie, “poor responder” detection, “bot” detection, and duplicate responses), we have included 313 participants as the final sample. There was no missing data because participants were required to respond to every item in order to continue in the survey. Qualtrics provided an incentive to their research participant panels for their time completing the survey. See the published primary outcomes paper for more details. 21
Measures
Demographics
Items queried participants to report their age, gender, race, ethnicity, nationality, income, level of education, and marital status.
General Ethnic Discrimination Scale
Seventeen multipart questions from the General Ethnic Discrimination Scale 58 examined the frequency and severity of discrimination that participants experienced in education, employment, legal, health care, or community settings due to one's race/ethnicity. Frequency of discrimination experiences were rated on a 6-point scale (from 1 = “Never” to 6 = “Almost all the time”). Instructions were modified to orient participants to report the frequency of racial discrimination before the psychedelic experience. Internal consistency was excellent (Cronbach's alpha = 0.95).
Psychedelic Experience Questionnaire
This 8-item questionnaire assessed the type of psychedelic used, the age of having the psychedelic experience, memory of the experiences, and self-reported dose and length of the psychedelic experience.
Psychological Insight Questionnaire
The 23-item PIQ30,56 was included and participants were oriented to think back on their psychedelic experience and then to rate their insights on a 6-point scale (from 0 = “No; not at all” to 5 = “Extremely/More than ever before in my life”). For this study, we used a total scale mean score and internal consistency reliability was excellent (Cronbach's alpha = 0.95).
Mystical Experience Questionnaire
The 30-item MEQ28,29 was included, and participants were oriented to think back their psychedelic experience and then to rate their mystical-type experience on a 6-point scale (from 0 = “None; not at all” to 5 = “Extremely/More than ever before in my life”). For this study, we used a total scale mean score, and internal consistency reliability was excellent (Cronbach's alpha = 0.96).
Challenging Experience Questionnaire
The 26-item CEQ 38 was included, and participants were oriented to think back to their psychedelic experience and then to rate their feelings of grief, fear, insanity, death, isolation, physical distress, or paranoia on a 6-point scale (from 0 = “No; not at all” to 5 = “Extremely/More than ever before in my life”). For this study, we used a total scale mean score and internal consistency reliability was excellent (Cronbach's alpha = 0.97).
Acceptance and Action Questionnaire-II
The 7-item AAQ-II47,48 was included as a measure of psychological flexibility to evaluate avoidance, emotional states, and perceptions of oneself on a 7-point scale (from 1 = “Never true” to 7 = “Always true”). For this study, we calculated the mean psychological flexibility change score from “before the psychedelic experience” to “after the psychedelic experience.” The sign of these scores was then reversed to aid in the interpretability of the findings (eg, + was changed to − such that a decrease in score would be interpreted as an increase in psychological flexibility). Internal consistency reliability was good (“before” measure: Cronbach's alpha = 0.89; “after” measure: Cronbach's alpha = 0.89).
Trauma Symptoms of Discrimination Scale
The 21-item Trauma Symptoms of Discrimination Scale 5 was included in this study to examine participants’ discriminatory distress about symptoms of trauma (ie, uncontrollable arousal, feelings of alienation, worries about future negative events, and perceiving others as dangerous) in the 30 days before and 30 days after the psychedelic experience. The participants were oriented to think back to their psychedelic experience and to rate the frequency of their experience of discriminatory distress regarding trauma on a 4-point scale (from 0 = “Never” to 3 = “Often”). For this study, we used a total scale score and calculated the average change in trauma symptoms from “30 days before the psychedelic experience” to “30 days after the psychedelic experience.” Internal consistency reliability for the total scale score was excellent (“before” measure: Cronbach's alpha = 0.96; “after” measure, Cronbach's alpha = 0.95).
Analytic Plan
Firstly, descriptive statistics for demographic and background characteristics for all study variables were calculated. Normality for all primary study variables was checked and no values for skewness or kurtosis fell outside an acceptable range. Pearson and point biserial correlation coefficients were calculated to examine the relationships among all primary study variables (age, sex, acute insight, mystical-type, and challenging effects, trauma symptom change score, and psychological flexibility change score; race groups). Next, a regression analysis was used to test (H1): acute mystical-type, challenging, and insight experiences will be associated with trauma symptom change scores. A path analysis was then used to test hypothesized direct effects (H2-H3: Intensity of psychological insight, challenging, and mystical-type effects have a direct effect on changes in psychological flexibility, and changes in psychological flexibility have a direct effect on changes in trauma symptoms) and mediation effects (H4): Intensity of psychological insight, challenging, and mystical-type effects are indirectly related to changes in trauma symptoms via changes in psychological flexibility. The sum of ethnic discrimination events was included as a control variable in the regression and path analyses. Although race was considered as a control variable, it was uncorrelated with all other variables and thus was excluded from analyses. Analyses were conducted in SPSS v 27 59 and MPlus version 8.0 using maximum likelihood estimators. 60
Results
Respondent Characteristics
The sample for this study was recruited intentionally for diversity, with about one-half of the participants currently living in Canada, and the other half in the United States. Most participants reported their race as black or African heritage (32%), East Asian, South Asian, Asian American/Canadian (29%), with smaller proportions reporting their race was Native American or Indigenous Canadian (18%), or Native Hawaiian, Pacific Islander, other (21%). Most other demographic characteristics have been reported in the primary manuscript from this study. 21 Briefly, the average age in the sample was 33.1 (SD = 11.2), approximately one-half were female (57%), living with a partner or married (51%), and three-quarters reported annual household income equal to or greater than $35 000 (73%). Approximately equal proportions of participants reported they consumed LSD (36%), psilocybin/mushrooms (37%), or 3,4-methylenedioxymethamphetamine (MDMA; 27%) during their psychedelic experience, and about one-half (∼56%) reported that they consumed a moderately high or high dose (see the published manuscript 21 for further demographic data).
Associations Between Acute Psychedelic Effects and Changes in Psychological Flexibility and Changes in Trauma Symptoms
A series of point-biserial correlations (Table 1) revealed that race subgroup was weakly related (range: −0.17 to 0.13) to the intensity of acute psychedelic effects (acute challenging, insight, and mystical-type effects), trauma symptom change scores, and psychological flexibility change scores. As Table 1 also shows, Pearson correlations revealed that the intensity of mystical-type and insight effects was strongly positively correlated with each other, and insight was weakly positively correlated with the intensity of challenging effects. Greater intensity of acute insight and mystical-type experiences was moderately positively correlated with changes in psychological flexibility and negatively correlated with decreases in trauma symptoms. Additionally, greater changes in psychological flexibility were associated with greater changes in trauma symptoms. A series of Pearson correlations also revealed that psychological flexibility was negatively correlated with number of trauma symptoms prior to the psychedelic experience (R = −0.66, p < .001), and after the psychedelic experience (R = −0.61, p < .001).
Means, Standard Deviations, and Correlations Among Variables (ie, Mystical-Type Experiences Score, Challenging Experiences Score, Psychological Insight Score, Trauma Symptom Change Score, Psychological Flexibility Change Score; Sum of Ethnic Discrimination Events, Race Groups; N = 313).
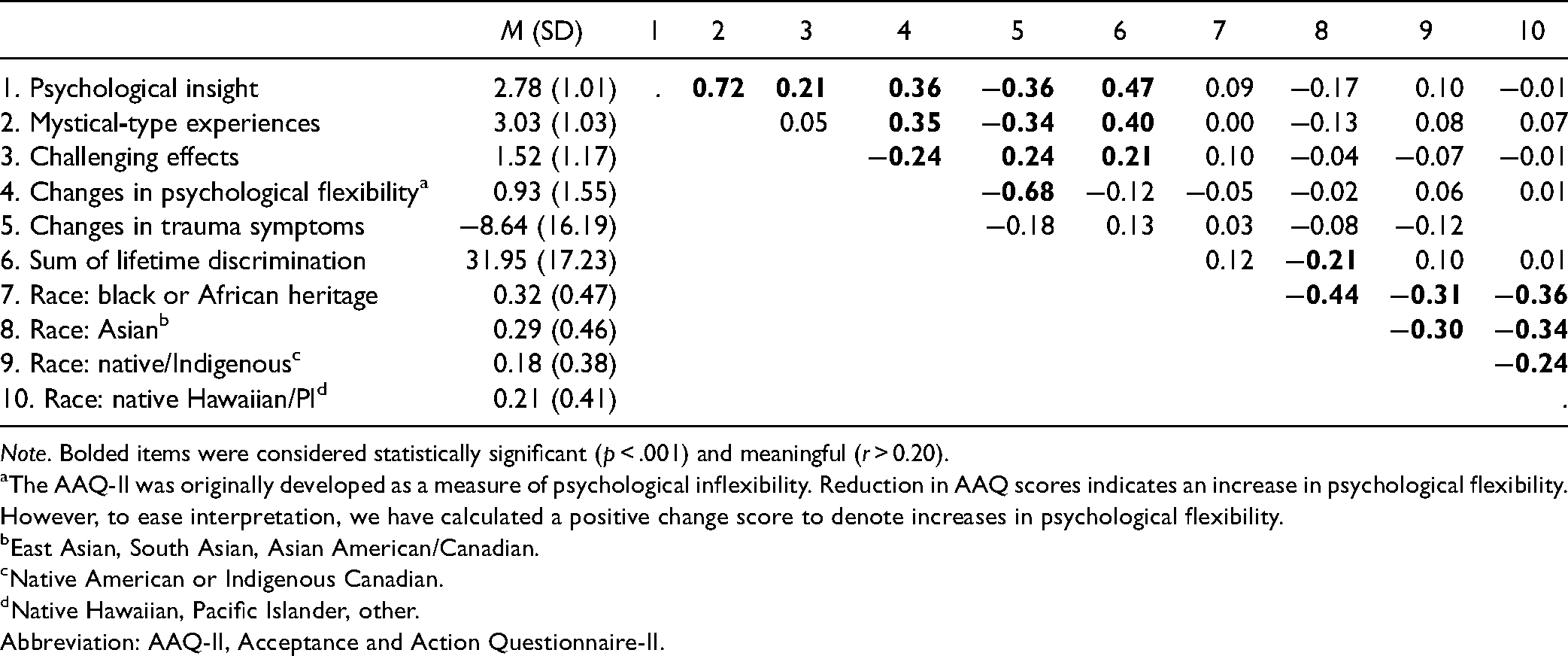
Note. Bolded items were considered statistically significant (p < .001) and meaningful (r > 0.20).
The AAQ-II was originally developed as a measure of psychological inflexibility. Reduction in AAQ scores indicates an increase in psychological flexibility. However, to ease interpretation, we have calculated a positive change score to denote increases in psychological flexibility.
East Asian, South Asian, Asian American/Canadian.
Native American or Indigenous Canadian.
Native Hawaiian, Pacific Islander, other.
Abbreviation: AAQ-II, Acceptance and Action Questionnaire-II.
Regression Analysis
Table 2 shows data from the multiple linear regression controlling for the sum of ethnic discrimination events (M = 31.95; SD = 17.23; range: 0-85) and including acute mystical-type (M = 3.03; SD = 1.03; range: 0.37-5), challenging (M = 1.52; SD = 1.17; range: 0-5), and insight effects (M = 2.78; SD = 1.01; range: 0.17-5.0) as correlates of decreases in trauma symptoms from before to after the psychedelic experience (M = −8.64; SD = 16.19; range: −62 to 63). After controlling for the sum of ethnic discrimination events, the overall model was significant (p < .001), accounting for 23% of the variance in trauma symptom change scores (H1). Although accounting for a small amount of variance in this model, greater intensity of insight effects and less intensity of challenging effects were significantly associated with decreases in trauma symptoms (see Table 2).
Summary of Multiple Linear Regression Showing Significant Predictors of Changes in Trauma Symptoms From Before to After a Psychedelic Experience (N = 313).

Note. The overall model was significant, F(4, 312) = 23.93, p < .001.
Path Analysis
As shown in Figure 1, the path analysis controlling for the sum of ethnic discrimination events prior to the psychedelic experience revealed that greater mean intensity of acute insight effects and less intensity of challenging effects were directly related (insight: β = 0.34, p < .001; challenging: β = −0.32, p < .001) to mean increases in psychological flexibility (Mincrease = 0.93; SD = 1.55; range: −5.14 to 6; supporting H2), and mean changes in psychological flexibility were directly related (β = −0.58, p < .001) to mean changes in racial trauma symptoms (supporting H3). Findings also revealed indirect effects wherein changes in psychological flexibility mediated the relationships between the intensity of acute insight (β = 0.20, SE = 0.04, p < .001), and challenging (β = −0.18, SE = 0.03, p < .001) effects and mean changes in racial trauma symptoms (supporting H4). Model fit was excellent: χ2 = 1.865 (p = .394); root mean square error of approximation = 0.000 (90% CI: .00, .11); comparative fit index = 1.00; standardized root-mean-square residual = 0.008.

Path analysis showing that changes in psychological flexibility mediate the relationship between acute psychedelic effects and changes in trauma symptoms among individual exposed to racial trauma (N = 313). ns = not significant, *p < .05, **p < .01, ***p < .001.
Discussion
Several hypotheses were tested to examine the relationship between psychological flexibility and racial trauma symptoms in this sample of POC. Firstly, a multiple linear regression model found that acute psychedelic effects, specifically greater intensity of acute insight and lower intensity of challenging experience, were significant correlates of change in racial trauma symptoms (H1). Interestingly, mystical-type effects were not significantly related to the change in racial trauma symptoms, suggesting these may be less important for therapeutic benefits in POC or possibly less relevant specifically to racial trauma symptoms. It could also be related to the fact that approximately one-quarter of the sample reported using MDMA which is known to produce less intense mystical-type effects, 61 thus possibly attenuating this relationship in the sample.
Secondly, greater intensity of acute insight effects and lower intensity of challenging effects were directly related to changes in psychological flexibility, supporting the hypothesis that acute psychedelic effects directly impact changes in psychological flexibility (H2). These findings add to a growing literature indicating a central role for acute subjective effects of psychedelics in influencing subsequent mental health outcomes,24,25,33,62,63 and suggest that psychological flexibility may be an important factor related to those outcomes.30,45 Interestingly, there is also a small, but statistically significant, correlation between the intensity of challenging and insight effects in this sample. This relationship could be due to increases in negative emotional and physiological arousal that may accompany novel insights into one's past traumatic experiences. However, data from this study does not allow for causal inferences, and therefore, this hypothesis awaits further testing in clinical trials.
Thirdly, there was a direct relationship between psychological flexibility and changes in racial trauma symptoms, such that changes in psychological flexibility were related to changes in racial trauma symptoms (H3). These results suggest that consistent with other research,64,65 psychological flexibility may be a substantial factor contributing to mental health per se, apart from psychedelic use, and comprises an area for further study in its own right.
Fourthly, psychological flexibility mediated the relationships between acute psychedelic effects (ie, insight and challenging effects) and changes in racial trauma symptoms (H4). This finding supports models of psychedelics’ therapeutic efficacy being linked to increases in psychological flexibility and presents intriguing opportunities for incorporating psychological flexibility as a therapeutic target in psychedelic-assisted therapies.30,42,43 Although a number of neurobiological and psychological mechanisms of psychedelics’ therapeutic efficacy have been posited in the literature, there is as yet no consensus on how observed benefits of psychedelics can persist for months or years after the acute effects have subsided. The present results add to the emerging literature suggesting psychological flexibility could be an important mediator of psychedelics’ benefits that necessitates additional focused research. Furthermore, it adds to our understanding specifically of how psychological flexibility may be beneficial to POC in overcoming racial trauma.
Notable study limitations include potential recall bias in participants’ ability to accurately remember symptoms and psychedelic experiences that occurred months or sometimes years in the past. As the study was conducted using a cross-sectional online survey design, participant responses cannot be conclusively verified. Similarly, participant self-selection and computer literacy and availability may have impacted the accessibility of this research study. Additionally, because participants were purposively sampled to collect data from individuals reporting benefits in racial trauma symptoms after psychedelic use, we cannot determine the relative prevalence of such positive outcomes or characterize cases in which POC who used psychedelics may have experienced negative mental health outcomes. Furthermore, this study lacks multiple prospective assessments to measure changes in psychological flexibility or mental health symptoms over time, which is needed to make strong interpretations of mediational analyses. However, to partially overcome this limitation, we employed a quasiexperimental 1-group pretest/posttest design using “then-test” items to assess symptoms 1 month prior to and 1 month after the psychedelic experience. This type of design allows for cautious interpretation of temporality, although these data should be replicated in a prospective study. It is also possible that other confounding factors, such as halo effects and expectancies were related to outcomes reported in this study.
In addition to the limitations above, several concerns have been raised about the AAQ-II as a measure of psychological flexibility. Recent studies have explored the convergent and discriminant validity of the AAQ-II compared to other measures of psychological flexibility and experiential avoidance,66–68 suggesting the AAQ-II may be more strongly related to negative affect and personality constructs, than to features theorized as the core aspects of psychological flexibility. Secondly, there may be questionable face validity of the items included on the AAQ-II, such that they may be more related to psychopathology rather than psychological flexibility. Nevertheless, the AAQ-II remains a predominant measure of psychological flexibility, but further investigation of the validity of this assessment tool is warranted. Lastly, it is possible that the subjective indicators of the acute psychedelic state as measured by the MEQ, PIQ, and CEQ, are correlated with objective neurobiological changes that underlie shifts in psychological flexibility. These relationships should be explored in laboratory-based studies.
Conclusion and Implications
POC face substantial health disparities, including unique and often undertreated mental health challenges.69,70 Among these, trauma and racial trauma are particularly debilitating and difficult to treat.71–73 Psychedelic studies have also lacked inclusion of POC and little is known about the unique ways in which psychological processes may underlie the potential therapeutic effects of psychedelics in this population. Thus, despite the limitations noted above, the present study and related research on psychedelic benefits in POC 21 represent a promising path ahead for developing novel, tailored interventions for POC that incorporate the current wave of research and clinical interest in psychedelic-assisted therapies. Although psychedelic-assisted interventions may not directly impact systemic factors such as poverty, unemployment, and criminal justice inequity that greatly contribute to current mental health disparities,74,75 they do comprise a critical potential avenue for improving mental health outcomes in POC, which is urgently needed. This work also highlights a much-needed expansion of research efforts to include racial/ethnic and other minoritized populations in assessing psychedelics’ therapeutic potentials for underserved communities.
Footnotes
Declaration of Conflicting Interests
Drs Williams and Davis are board members of Source Research Foundation. This organization was not involved in the design/execution of this study or the interpretation or communication of findings.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the study was provided by the University of Ottawa and the Canada Research Chairs Program (MTW). by the Effort for AKD, AGR, and NDS was provided from support from Tim Ferriss, Matt Mullenweg, Craig Nerenberg, Blake Mycoskie, and the Stevenand Alexandra Cohen Foundation. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Ethical Approval
This study (2019E0717) was deemed exempt from review by the Ohio State University human research protection program.