
Abstract
Background
Child maltreatment negatively affects the formation of internal schemata of self and other during development, leading to negative adaptations in self-concept and social cognition. Clinical reports suggest the efficacy of psychedelics in treating the psychopathological sequelae of child maltreatment. Altering maladaptive schemata of self and other implicated in negative self-concept and impaired social cognition may be a central mechanism for reducing posttraumatic stress symptoms.
Aims
This study aims to assess whether psychedelic use moderates the relationships between child maltreatment and self-concept, social cognition, and posttraumatic stress symptoms.
Method
An online survey was completed by 166 participants and included measures of maltreatment exposure and severity, history of intentional therapeutic psychedelic use, posttraumatic stress symptoms, internalized shame, and facial emotion recognition.
Results
Child maltreatment significantly correlated with posttraumatic stress symptoms (r = .26 and r = .20, p < .01) and internalized shame (r = .18, p < .05). Of all maltreatment subtypes, emotional abuse and neglect most strongly correlated with complex trauma symptoms (r = .32, p < .001) and internalized shame (r = .31, p < .001). Participants with a history of intentional therapeutic psychedelic use reported significantly lower complex trauma symptoms (d = 0.33, p < .05) and internalized shame (d = 0.35, p < .05) despite similar histories of maltreatment. Differences in complex trauma symptoms (d = 0.66, p < .01) and internalized shame (d = 0.80, p < .001) were largest for participants with a history of more than 5 occasions of intentional therapeutic psychedelic use. A history of more than 5 occasions of intentional therapeutic psychedelic use significantly moderated the relationship between emotional abuse and neglect and complex trauma symptoms (p < .01). No associations were found between maltreatment or psychedelic use and facial emotion recognition.
Conclusion
These findings demonstrate that using psychedelic drugs with therapeutic intent is associated with lower levels of complex trauma symptoms and internalized shame in individuals with histories of child maltreatment. Psychedelic use may have therapeutic benefit in treating the posttraumatic sequelae of child maltreatment.
Keywords
Introduction
Child maltreatment (CM), including physical abuse and neglect, emotional abuse and neglect, and sexual abuse, is extremely common worldwide and is implicated in the etiology of myriad mental and physical disorders.1–5 CM is often referred to as developmental trauma in order to signal the lasting and global effects of prolonged exposure to trauma on the child’s cognitive, affective, social, and biological development.6–10 Emerging clinical data are verifying longstanding anecdotal reports that psychedelic substances are singularly effective in treating the psychopathological sequelae of CM.11–14 Psychological and neurobiological mechanisms of therapeutic action, however, have yet to be robustly elucidated.15–21 A proposed mechanism of action is the capacity of psychedelic drugs to acutely disintegrate and post-acutely reshape maladaptive schemata of self and other formed in reaction to developmentally traumatic experiences. 17 , 18
Schemata of self and other form in early relationships and play a central role in organizing social cognition, self-concept, affect regulation, and relational behavior throughout the lifespan.22–24 When these schemata develop within and functionally adapt to an interpersonally traumatic environment in childhood, they are likely to prove maladaptive in adulthood and contribute to symptoms of psychopathology, such as negative or unstable self-concept, pervasive affect dysregulation, and social dysfunction. 9 , 23 , 25 , 26 Treatment may aim to adjust or “update” maladaptive schemata in order to more accurately and adaptively represent current reality.
CM has consistently been associated with negative self-concept. Multiple cross-sectional and longitudinal studies have found that child maltreatment predicts internalized shame and low self-esteem.27–35 Multiple studies have also found distorted and impaired facial emotion recognition (FER) in children and adults with histories of CM, though the nature of these alterations remain inconclusive. A systematic review from 2014 found decreased global accuracy in FER, greater reactivity to negative emotions, and greater response bias toward negative emotions. 36 A number of other studies have reported increased amygdala reactivity to negative faces.37,38
As described above, theoretical models suggest that disturbances in self-concept are etiologically related to impairments in social cognition, each the result of maladaptive schemata of self and other that develop from disturbed interpersonal experiences in infancy and childhood. 22 , 23 , 39 In adulthood, low self-worth, high internalized shame, and impaired capacity to recognize and interpret others’ emotions may produce pervasive difficulties in social interactions, leading to problematic and unstable relationships and a worsening of posttraumatic stress symptoms (PTSS) over time.40–43 Adaptively altering the schemata that underlie these phenomena, then, may be an important target in the treatment of CM. 39 , 44 , 45
Psychedelic drugs may prove valuable agents in catalyzing this kind of therapeutic transformation of maladaptive schemata. Models of the acute neurological activity of psychedelics suggest that they decrease within-network functional connectivity and increase between-network, global connectivity, thereby disrupting reified neural patterns of cognition and behavior and facilitating new learning. 17 , 46 A recent theoretical model of the psychological action of psychedelics argues that they “relax” cognitive predictive models and representations, temporarily increasing their pliability, enhancing their sensitivity to current information, and allowing for their positive transformation and revision. 17
Psychedelics have robustly been shown to profoundly compromise the normal subjective sense of self and, in high doses, occasion “mystical” states of selflessness, self-transcendence, or “ego dissolution,” frequently leading to enduring positive changes in mood, personality, and self-concept.47–51 Furthermore, in many studies of psychedelics with both psychiatric and healthy samples, the degree or strength of loss of self directly correlated with positive outcomes.52–56 Psychological insight, an important mechanism of change in psychotherapy, has also been shown to mediate positive outcomes associated with psychedelic use in clinical and naturalistic settings.57–62 Adaptive alterations and updates to dysfunctional self-schemata, therefore, may be a salient psychological mechanism underlying the curative effects of psychedelic use in people with histories of CM.
Psychedelics have also been shown to alter the recognition of negative faces and reduce amygdala reactivity to negative faces, with a number of studies finding associations between acute and post-acute attenuations of amygdala reactivity to negative faces and post-acute increases in positive mood and well-being.63–66 Another study, however, found that increased amygdala responses compared to baseline for fearful and happy faces 1 day after psilocybin correlated with decreases in depressive symptoms. 67 In contrast to these prior results, a recent study found no acute or post-acute effects of ayahuasca on FER compared to placebo. 68 The nature of psychedelic-induced alterations to FER as well as their relationship to positive outcomes thus remains unclear.
Though most research on the use of psychedelics to treat mental disorders has been conducted in controlled, clinical settings, preliminary survey-based research suggests the therapeutic benefit of naturalistic psychedelic use as well. 60 , 61 , 69 Multiple studies have shown that the explicit intentions and expectations that the user assigns to the experience beforehand critically affect both the experience itself and its outcomes.70–73 Using psychedelics with the deliberate intention of deriving therapeutic benefit and reduction of symptoms associated with psychopathology, therefore, may be as important as the formal setting in which the use occurs (i.e., naturalistic or clinical). 74
The present study aims to examine
H1 (replication). Child maltreatment exposure and severity will a) positively correlate with posttraumatic stress symptoms, b) positively correlate with internalized shame, and c) negatively correlate with global accuracy in identifying facial emotions.
H2 (primary hypothesis). Compared to individuals without a history of intentional therapeutic psychedelic use, individuals with a history of intentional therapeutic psychedelic use will a) report less posttraumatic stress symptoms, b) report less internalized shame, and c) show higher global accuracy in identifying facial emotions.
the impact of intentional therapeutic psychedelic use (ITPU), in either naturalistic or clinical settings, on maladaptive schemata of self and other among adults with histories of CM. This study operationalizes schemata of the self in a measure of internalized shame and schemata of others in an FER task. Our main hypotheses are:
Method
Participants
Volunteer participants were recruited online via the social networking websites Reddit and Facebook as well as by word of mouth. Inclusion criteria were that participants be 18 years or older, fluent in English, and endorse a history of CM. No compensation was provided to participants.
Materials
Demographics Questionnaire
Items in this survey assessed age, gender, race, sexual orientation, marital status, socioeconomic status of childhood home, education, psychiatric diagnoses, and lifetime substance use history.
History of ITPU
History of ITPU was assessed with the following question: “Have you ever used a psychedelic/entheogenic/hallucinogenic substance (including, but not limited to: psilocybin “magic” mushrooms or truffles, LSD/“acid”, ayahuasca/yagé, mescaline/peyote/San Pedro, DMT, MDMA/ecstasy, ketamine, or 2 C-B) with the intention of healing or processing childhood trauma?” For participants who endorsed a history of ITPU, follow-up questions assessed which substances had been used, number of occasions of use, timeframe of most recent occasion of use, settings of use, and impact of use, which included an optional open-ended text entry item.
Childhood Trauma Questionnaire
The Childhood Trauma Questionnaire (CTQ) is a 28-item retrospective self-report scale that assesses exposure to and severity of childhood maltreatment across five subscales. 75 Items are answered using a Likert scale of 1 (“Never true”) to 5 (“Very often true”); total scores for each subscale range from 5-25, and total overall score ranges from 25 (low) to 125 (severe). Internal consistency for the maltreatment type subscales in the present sample were as follows: physical abuse, α = .83; emotional abuse, α = .80; sexual abuse, α = .95; physical neglect, α = .74; emotional neglect, α = .83.
International Trauma Questionnaire
The International Trauma Questionnaire (ITQ) is a 12-item measure designed to assess PTSD and complex PTSD (CPTSD) symptomatology as described in the 11th revision of the International Classification of Diseases (ICD-11). 76 PTSD comprises three symptom clusters (reexperiencing in the here and now, avoidance of traumatic reminders, and a sense of threat), and CPTSD comprises these three core symptom clusters plus three additional symptom clusters that collectively represent “Disturbances in Self-Organization” (DSO; affective dysregulation, negative self-concept, and disturbances in relationships). A recent psychometric study of two trauma-exposed samples found two broad symptom clusters corresponding to PTSD and DSO, supporting the structural validity of the disorders. 77 The scale showed good internal consistency in the present sample (α = .87).
Reading the Mind in the Eyes Test
The reading the mind in the eyes test (RMET) is a widely used and reliable measure of FER. 78 The test comprises 36 grey-scale photographs of the eye region of actors and actresses accompanied by four complex emotional mental-state descriptions. Participants are instructed to select the word that best matches what emotion the person in the picture is expressing; only one of the four items is deemed correct. Stimuli were coded by emotional valence (positive, neutral, or negative) based on categorization previously established. 79
Internalized Shame Scale
The Internalized Shame Scale (ISS) is a 30-item self-report measure comprising 24 negatively worded items to assess internalized (trait) shame and 6 positively worded items to counteract a negative response set. 80 Items are answered using a Likert scale of 1 (“Never”) to 5 (“Almost always”). The scale showed good internal consistency in the present sample (α = .86).
Procedure
Participants completed the study online via Qualtrics. No portion of the study had time constraints. After granting informed consent on the initial page of the survey, participants completed a demographics questionnaire and reported their history of ITPU. Participants then completed the CTQ to assess CM exposure and severity and the ITQ to assess current PTSS. The RMET followed, with a link to a glossary of terms provided on the first page and each photograph subsequently presented on its own webpage; after selecting a response, the survey automatically continued to the next photograph. Time spent on each page (i.e., before clicking a response) was recorded to collect reaction time data. Participants then completed the ISS. The final page of the survey thanked the participants for volunteering to participate and provided the contact information of the study principal investigator and their supervisor as well as information for referrals to mental health providers. The study was deemed exempt from review or oversight by the Institutional Review Board of The New School.
Data Analysis
Descriptive statistics were calculated for all variables. Independent-samples t-tests, chi-square tests, and one-way analysis of variance (ANOVA) tests were used to assess associations between demographic variables and primary study variables. Data were manually inspected for outliers, and outliers representing invalid data points were removed as necessary and appropriate. Data were also inspected for duplicate responses and invalid responding and removed as necessary and appropriate. Only the data of those participants who completed the entire survey were included in analyses.
Bivariate correlation analyses were used to assess the relationship of CM exposure and severity (CTQ scores) to PTSS (ITQ PTSD and DSO scores; H1a), internalized shame (ISS scores; H1b), and FER accuracy (RMET scores; H1c). Bivariate correlation analyses were also used to assess the relationships of CM subtypes to outcome variables.
Independent-samples t-tests were used to assess differences between the ITPU and non-ITPU groups in ITQ PTSD and DSO scores and subscores (H2a), ISS scores (H2b), and RMET scores (H2c). One-way ANOVA tests were used to assess whether differential relationships with outcome variables were found among ITPU factors (number of occasions of ITPU, timeframe of most recent ITPU occasion, and impact of ITPU); Tukey post hoc tests and further independent-samples t-tests were used to assess these differential relationships
Finally, linear regression analyses including manually coded interaction variables (i.e., CTQxITPU) were used to assess whether ITPU moderated any of the H1 relationships between CM and outcome variables in which ITPU showed significant associations with the dependent variable in H2 analyses.
Results
Participant Characteristics
Recruitment of participants took place from October 15–24, 2019 during which time 283 people began the survey and 167 completed it entirely. One participant was excluded for entering a birth date indicating they were less than 18 years of age, and so the final sample comprised 166 participants. Median completion time for the survey was 20 min 32 s (interquartile range: 16 min 58 s to 29 min 34 s).
Demographics
The mean age of participants was 30.49 (SD = 9.52) years, and the majority of participants identified as White (90.4%), cisgender (90.4%), woman (60.2%), and heterosexual (50.0%). A large proportion of the sample was LGBTQ, with 9.6% identifying as transgender and 49.7% identifying as non-heterosexual. The majority of participants endorsed at least one self-reported psychiatric condition, most commonly anxiety (84.9%) and/or depression (82.5%), and only 5.4% endorsed no psychiatric condition. All participants endorsed some lifetime history of substance use, most commonly caffeine (91.0%), alcohol (89.2%), and cannabis (75.3%). Full demographic information is reported in Table 1.
Demographic Characteristics (N = 166).
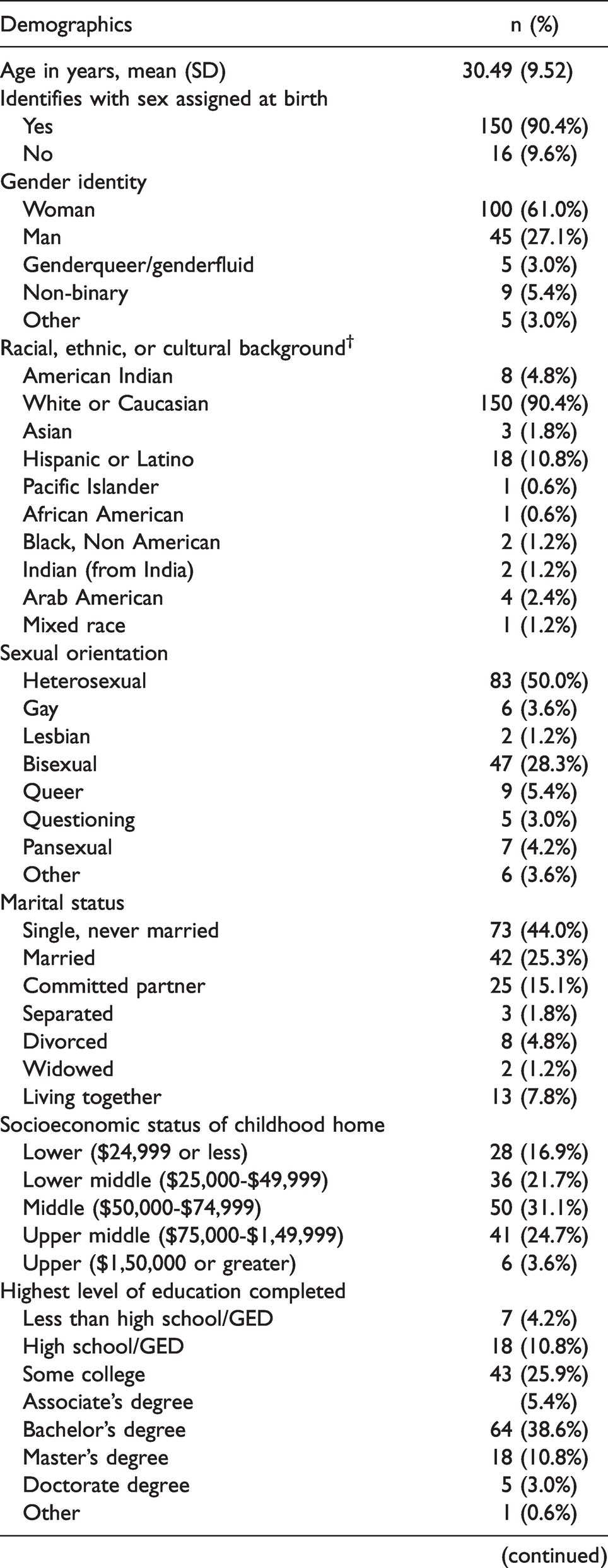
GED: General Educational Development (equivalent to US high school diploma).
†Participants could select multiple responses for this question.
History of ITPU
Approximately one third of the sample (31.3%) endorsed a history of ITPU, among whom 40.4% had used psychedelics with therapeutic intent more than 5 times and 73.1% had used within the past 6 months; three quarters (75.0%) rated their experiences as exclusively healing/helpful/positive change, while only 1 participant (1.9%) rated them as exclusively harmful/damaging/negative change. The ITPU group did not significantly differ from the non-ITPU group in any demographic variable. Full information on ITPU is reported in Table 2.
Characteristics of ITPU Experiences (N = 52).

LSD: lysergic acid diethylamide; DMT: N,N-dimethyltryptamine; MDMA: 3,4-methylenedioxy-methamphetamine; 2 C-B: 2,5-dimethoxy-4-bromophenethylamine.
†Multiple responses could be selected for this question.
‡These response choices are drawn from Garcia-Romeu et al. 61
Trauma Exposure and Symptoms
The sample reported high levels of CM and PTSS. Mean CTQ score was 69.58 (SD = 16.03). In the entire sample, 92.8% of participants scored in the severe range on at least one of the maltreatment type subscales. Based on ITQ scores, 61.4% of the sample met diagnostic criteria for PTSD and 45.8% for CPTSD. Non-heterosexual participants had significantly higher CTQ scores (t(164) = 2.340, MDiff = 5.95, 95% CI[1.11, 10.79], p = .016) and ITQ PTSD scores (t(164) = 2.427, MDiff = 1.89, 95% CI[0.30, 3.49], p = .020) and were significantly more likely to meet diagnostic criteria for PTSD (X2(1,166) = 4.984, p = .026) and CPTSD (X2(1,166) = 6.213, p = .013). Mean CTQ scores were not significantly different between ITPU and non-ITPU groups (t(164) = 0.395, MDiff = 1.06, 95% CI[-4.25, 6.37], p = .693).
Hypotheses
Our first hypothesis was partially confirmed. Parts (a) and (b) were confirmed: CTQ scores showed weak, positive correlations with ITQ PTSD scores (r(164) = .26, p = .001), ITQ DSO scores (r(164) = .20, p = .009), and ISS scores (r(164) = .18, p = .020). Bivariate correlation analyses of CTQ subtype scores with PTSD, DSO, and ISS sores are presented in Table 3.
Matrix of Correlations Between CTQ Subscale Scores and ITQ PTSD Scores, ITQ DSO Scores, and ISS Scores.

*Correlation is significant at the .05 level (2-tailed).
**Correlation is significant at the .01 level (2-tailed).
***Correlation is significant at the .001 level (2-tailed).
Part (c) was not confirmed: no significant relationship was found between CTQ scores and RMET scores (r(163) = .23, p = .093), and no CTQ subtype scores significantly correlated with RMET scores. Exploratory analyses found that CTQ scores also did not significantly correlate with RMET accuracy within any emotion valence (positive, neutral, or negative).
Our second hypothesis was also partially confirmed. Part (a) was partially confirmed: ITQ PTSD scores were not significantly different between ITPU and non-ITPU groups (t(164) = −0.430, MDiff = −0.38, 95% CI[−2.13, 1.37], p = .668). ITQ DSO scores, however, were significantly lower in the ITPU group with a small effect size (t(164) = −2.010, MDiff = −1.63, 95% CI[−3.22, −0.03], p = .046, d = 0.33). A multiple regression analysis, however, found no significant effect of the interaction between CTQ and ITPU on DSO scores (ΔR 2 = .010, F(1,162) = 1.797, p = .182),
A one-way ANOVA of the effect of number of occasions of ITPU on DSO scores was trending toward significance (F(2,49) = 2.536, p = .090), and a Tukey post hoc test showed lower DSO scores in participants endorsing more than 5 occasions of ITPU (ITPU5) than in participants endorsing 2 to 5 occasions or in participants endorsing 1 occasion, though these differences were not significant. When comparing the ITPU5 group to the rest of the sample (i.e., not just to the participants who endorsed 1-5 occasions of ITPU), ITPU5 reported significantly lower significantly lower DSO scores with a medium to large effect size (t(164) = −3.178, MDiff = −3.52, 95% CI[−5.71, −1.33], p = .002, d = 0.66; Figure 1(a)). There was no significant effect of timeframe of most recent ITPU occasion or impact of ITPU on DSO scores.

The differences in mean DSO scores (a) and mean ISS scores (b) between ITPU5 and non-ITPU5 groups.
ISS scores were also significantly lower in the ITPU group with a small effect size (t(164) = −2.104, MDiff = −5.72, 95% CI[−11.08, −0.35], p = .037, d = 0.35). A multiple regression analysis, however, found no significant effect of the interaction between CTQ and ITPU on ISS scores (ΔR 2 = .001, F(1,162) = 0.255, p = .614).
A one-way ANOVA showed a significant effect of number of occasions of ITPU on ISS scores (F(2,49) = 4.240, p = .020). A Tukey post hoc test revealed that ISS scores in the ITPU5 group were significantly lower than those of participants endorsing 2 to 5 occasions of ITPU (MDiff = −12.64, 95% CI [−24.37, −090], p = .032) and were also lower than participants endorsing 1 occasion at the trend level (MDiff = −14.68, 95% CI [−30.84, 1.47], p = .082). When comparing the ITPU5 group to the rest of the sample, ITPU5 reported significantly lower ISS scores with a large effect size (t(164) = −3.648, MDiff = −13.48, 95% CI [−20.77, −6.18], p < .001, d = 0.80; Figure 1(b)). There was no effect of timeframe of most recent ITPU occasion or impact of ITPU on ISS scores.
Part (c) was not confirmed: RMET scores were not significantly different between ITPU and non-ITPU groups (t(163) = 0.540, MDiff = 0.36, 95% CI [−0.95, 1.67], p = .590).
Post Hoc Analyses
Moderation Analyses
Due to the stronger relationships of emotional abuse and emotion neglect with primary outcome variables than other CTQ subscale scores (Table 3), a composite score of emotional abuse and neglect (EAN) was used in post hoc analyses. EAN scores showed stronger correlations than individual CTQ subscale scores or total CTQ scores with DSO scores (r(164) = .32, p < .001) and ISS scores (r(164) = .31, p < .001) .
Based on these findings and the prior finding that ITPU5 was most strongly associated with outcome variables among ITPU factors, regression analyses were conducted to examine any moderating effects of ITPU5 on the relationship between EAN and outcome variables.
A multiple regression analysis including ITPU5 and EAN in the first step of the model and the interaction term between the two variables in the next step found no significant effect of the interaction on variance in ISS scores (ΔR 2 = .011, F(1,162) = 2.171, p = .143). When DSO was used as the dependent variable in the model, however, the interaction between EAN and ITPU5 accounted for a significant amount of variance in DSO scores (ΔR 2 = .036, F(1,162) = 7.323, p = .008), indicating that ITPU5 significantly moderates the relationship between EAN and DSO scores. Bivariate correlation analyses found that in the non-ITPU5 group, EAN scores showed a moderate, positive correlation with DSO scores (r(143) = .42, p < .001), while in the ITPU5 group, there was no significant relationship between the two scores (r(19) = −.18, p = .434; Figure 2).
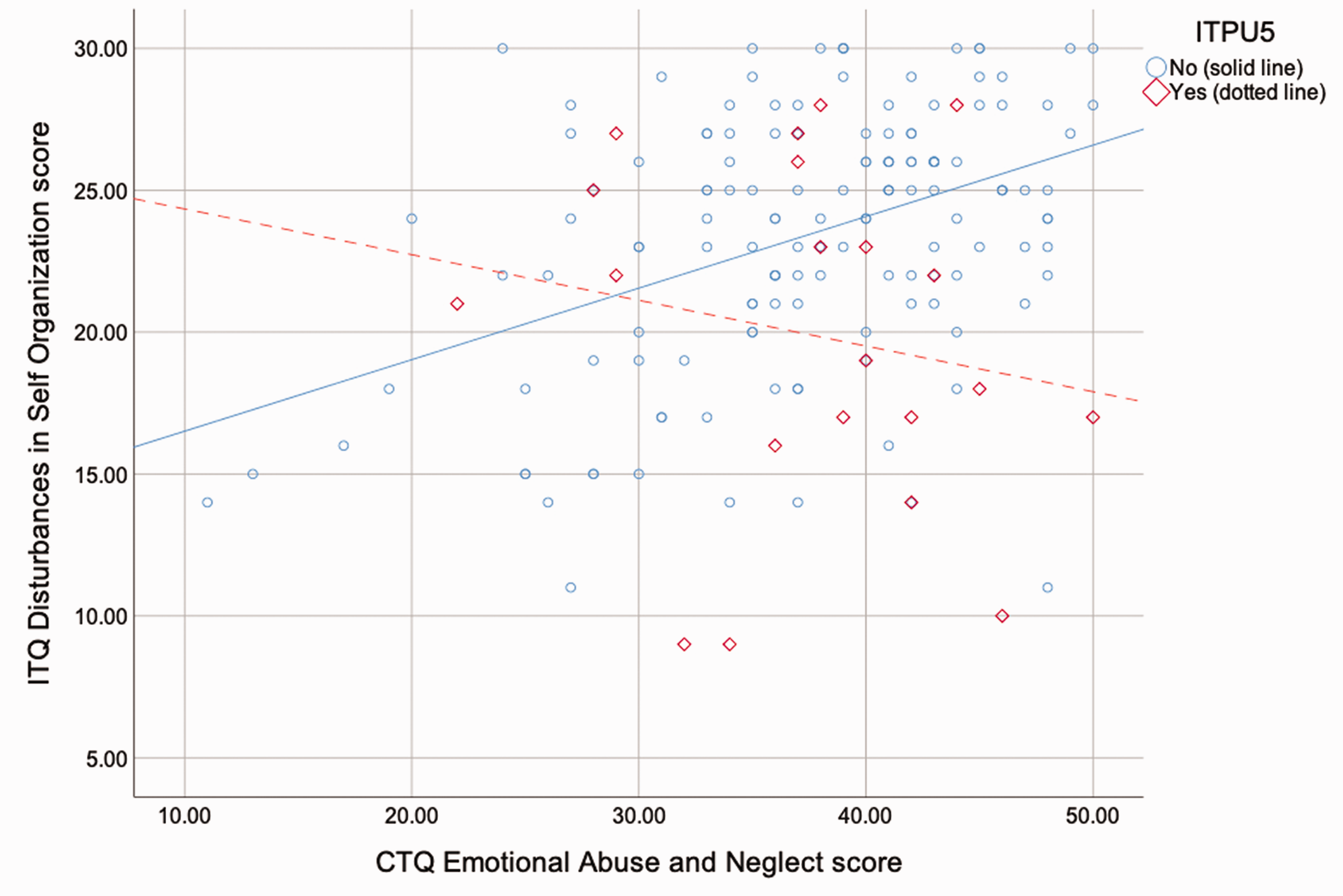
The moderating effect of ITPU5 on the relationship between EAN scores and DSO scores.
Additional Post-Hoc Analyses
Additional post-hoc analyses regarding RMET reaction times, non-intentional psychedelic use, substance type in ITPU, and naturalistic ITPU are presented in the Supplemental Materials. Qualitative results regarding the impact of ITPU are also presented in full in the Supplemental Materials.
Discussion
This study aimed to assess whether ITPU may have a moderating influence on the relationships between CM exposure and severity, posttraumatic symptomatology, and schemata of self and other. Our hypotheses were: 1) CM would be associated with higher PTSS, higher internalized shame, and impaired FER; and 2) ITPU would be associated with lower PTSS, lower internalized shame, and better FER compared to non-ITPU.
Our first hypothesis was partially confirmed: CM positively correlated with internalized shame and PTSS but showed no significant association with FER accuracy. Our second hypothesis was also partially confirmed: complex (but not simple) PTSS and internalized shame were significantly lower in the ITPU group, but FER accuracy did not differ between the ITPU and non-ITPU groups.
Endorsing more than 5 instances of ITPU significantly moderated the relationship between levels of exposure to and severity of emotional abuse and neglect and CPTSD symptoms such that among participants who had not used psychedelics with therapeutic intentions more than 5 times, there was a positive, linear correlation between emotional abuse and neglect and CPTSD symptoms, while among participants who had, there was a non-significantly negative correlation.
The partial confirmation of H2a and confirmation of H2b lend themselves to multiple interpretations. Though ITPU was associated with lower internalized shame and complex trauma symptoms, these findings do not conclusively indicate causal or chronological relationships among the variables. The significant moderation analysis described above, however, may be suggestive of a beneficial influence of repeated occasions of ITPU on the relationship between CM and posttraumatic sequelae. Replications and clarifications of moderation findings as well as longitudinal studies of the effects of ITPU in people with histories of CM would provide further evidence of a causal relationship.
The failure to confirm H1c or H2c may be due to a number of factors at a number of levels of interpretation. A confounding factor may be alexithymia, a condition marked by difficulties with identifying and labeling emotional experiences, which has been shown consistently to be associated with childhood trauma.81–83 A recent study found that RMET scores were significantly lower in alexithymic participants than non-alexithymic participants. 84 RMET scores in the present study were comparable to those of the alexithymic group in Oakley et al. and lower than the norm among healthy participants reported by Baron-Cohen et al. in the development study of the test. 78 , 84 The high levels of CM exposure and severity across the entire sample may be associated with sample-wide impairments in performance that may or may not be related to alexithymia; a restricted range effect, therefore, may be impacting the capacity to detect an association between RMET scores and CTQ scores or ITPU.
Limitations, Implications, and Future Directions
This study has some limitations, including its cross-sectional design, its reliance on retrospective reporting, its predominantly White sample, the potential for volunteer bias among participants, and the potential role of social desirability in participant responses, all of which may have affected the validity and generalizability of the findings. Another limitation is that past and/or current psychiatric treatment, such as psychotherapy or pharmacological treatment, was not assessed, and any confounding effects of such treatment, therefore, cannot be accounted for in the findings. An important future direction is the aforementioned longitudinal design to assess changes in internalized shame, social cognition, posttraumatic symptomatology, and other areas following ITPU in people with histories of CM. Such future studies ought to attempt to recruit a sample higher in racial diversity.
Despite these limitations, the present findings are significant in their implications for psychedelic-assisted treatments. Clinical trials of psychedelic-assisted psychotherapy for PTSD have thus far focused exclusively on MDMA, and none has yet used a “classic” psychedelic (e.g., psilocybin, LSD, or ayahuasca/yagé). 13 , 85 In this study, however, psilocybin and LSD were the two most commonly used psychedelics in the ITPU group, suggesting, in line with findings from prior survey studies of naturalistic psychedelic use in traumatized populations, that classic psychedelics also have therapeutic utility in the treatment of PTSD, particularly complex PTSD associated with CM. 19 , 86 , 87 Furthermore, of all the substances endorsed as being utilized in ITPU, ayahuasca/yagé was the only unique predictor of reductions in complex PTSS (see Supplemental Materials). Some literature has discussed the potential of ayahausca/yagé as a pharmacologic intervention for PTSD, though no clinical or observational studies have yet been conducted examining the question. 88 , 89 The present findings add to these prior discussions in situating ayahuasca/yagé as a viable candidate drug for use in psychedelic therapy for complex PTSD. Finally, despite the limited racial diversity of the present sample, nearly half of the participants were non-heterosexual, suggesting that psychedelics may have similar therapeutic potential for LGBT people as for heterosexual and cisgender people.
Our results also show that therapeutic benefit is derived from intentional psychedelic use in naturalistic settings (see Supplemental Materials), indicating that this benefit is not limited to formal, clinical settings where a psychiatric professional administers the drug and oversees the experience. These findings add to those of prior studies that reported therapeutic outcomes for alcohol use disorder, tobacco dependence, and cannabis, opioid, and stimulant misuse associated with naturalistic psychedelic use. 60 , 61 , 69 Future models of psychedelic treatment may incorporate more informal and independent use of psychedelics following adequate preparation in addition to structured psychedelic-assisted psychotherapy.
Finally, though ITPU, and especially ITPU5, was associated with decreased complex PTSS (i.e., disturbances in self organization; DSO), it was not associated with decreased “simple” PTSS, i.e., the symptoms of “simple” PTSD (versus complex PTSD). Emotional abuse and neglect showed the strongest associations with DSO, while physical and sexual abuse were not significantly associated with DSO. These results have significant implications both for the diagnosis and treatment of the variety of presentations of PTSD and for the development and conduct of psychedelic-assisted psychotherapy. Distinct patterns and types of CM result in differential profiles of posttraumatic symptomatology; the symptoms that comprise DSO – the profile of symptoms most strongly associated with emotional abuse and neglect and most effectively relieved by psychedelics in the present study – centrally relate to the self. The pervasive and disturbed patterns of interpersonal relating that define emotional abuse and neglect have a lasting, negative impact on the developmental process of forming, or becoming, a self. Psychedelics, which catalyze a profound alteration in the subjective sense of self, often effecting a total loss of self and subsequent re-forming of the self, may then, as the present findings suggest, be particularly well-suited as therapeutic agents in psychiatric disorders involving disturbances of the self, most notably complex PTSD. Representative qualitative reports from participants in the present study regarding their experiences with ITPU (see Supplemental Materials) may illustrate this process of coming to embody a more adaptive self-schema that psychedelics can catalyze: “It showed me who I am and that I like myself”; “Made me feel real for the first time in probably a decade”; “I also realized that my true essential Self is that which is consistent between all states of being and consciousness, which has helped me leave the darkness of trauma induced dissociation”; “That trip was a gut wound to my ego and the best thing to move towards a healing and authentic life”; “I was exactly who I was supposed to be”; “It has freed me from the ego that I’ve spent my whole life creating.” These findings contribute to elucidating the mechanisms of therapeutic action of psychedelics with implications for the development and conduct of psychedelic-assisted psychotherapy.
Conclusion
The findings of the present study demonstrate that using psychedelic drugs with therapeutic intent is associated with lower levels of complex posttraumatic stress symptoms and internalized shame in individuals with histories of child maltreatment. Psychedelics may prove valuable clinical agents in the treatment of a variety of mental disorders in which child maltreatment is etiologically implicated.
Supplemental Material
sj-pdf-1-css-10.1177_24705470211029881 - Supplemental material for Using Psychedelics With Therapeutic Intent Is Associated With Lower Shame and Complex Trauma Symptoms in Adults With Histories of Child Maltreatment
Supplemental material, sj-pdf-1-css-10.1177_24705470211029881 for Using Psychedelics With Therapeutic Intent Is Associated With Lower Shame and Complex Trauma Symptoms in Adults With Histories of Child Maltreatment by C. J. Healy, Kellie Ann Lee and Wendy D’Andrea in Chronic Stress
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.