
Abstract
Background
Digital therapeutics such as cognitive–emotional training have begun to show promise for the treatment of major depressive disorder. Available clinical trial data suggest that monotherapy with cognitive–emotional training using the Emotional Faces Memory Task is beneficial in reducing depressive symptoms in patients with major depressive disorder. The aim of this study was to investigate whether Emotional Faces Memory Task training for major depressive disorder is associated with changes in brain connectivity and whether changes in connectivity parameters are related to symptomatic improvement.
Methods
Fourteen major depressive disorder patients received Emotional Faces Memory Task training as monotherapy over a six-week period. Patients were scanned at baseline and posttreatment to identify changes in resting-state functional connectivity and effective connectivity during emotional working memory processing.
Results
Compared to baseline, patients showed posttreatment reduced connectivity within resting-state networks involved in self-referential and salience processing and greater integration across the functional connectome at rest. Moreover, we observed a posttreatment increase in the Emotional Faces Memory Task-induced modulation of connectivity between cortical control and limbic brain regions, which was associated with clinical improvement.
Discussion
These findings provide initial evidence that cognitive–emotional training may be associated with changes in short-term plasticity of brain networks implicated in major depressive disorder.
Conclusion
Our findings pave the way for the principled design of large clinical and neuroimaging studies.
Keywords
Introduction
Major depressive disorder (MDD) is among the leading causes of disability worldwide and is associated with both significant functional impairment and reduced quality of life. 1 MDD is a highly prevalent mental illness, affecting approximately 17% of the population across the lifespan and frequently following a recurrent and chronic course. 2 Despite the availability of established treatments, it is estimated that only about one-third of patients with MDD achieve remission.3,4 Novel interventions are therefore urgently needed. To address this knowledge gap and accelerate discovery, the National Institute of Mental Health is implementing an “experimental medicine” model of which an immediate goal is to determine if interventions “act on a target and affect a biological process or endpoint related to a clinical disorder.” 5
Numerous studies have shown that patients with MDD exhibit persistent deficits in cognitive control (the capacity to maintain and manipulate information) in the presence of emotionally salient stimuli and that such deficits are associated with illness severity.6,7 Functional magnetic resonance imaging (fMRI) studies in MDD have shown that dorsal cortical regions known to underlie cognitive control are hypoactive, whereas regions involved in emotion processing, particularly the amygdala (AMG), are hyperactive.8,9 These abnormalities have been observed across multiple tasks but have been most commonly studied using working memory 10 and facial affect processing paradigms.11,12 These abnormalities in local brain activation extend to functional connectivity of dorsal cortical regions and the AMG, characterized by reduced “top-down” regulatory input from cortical regions to the AMG. 13 MDD is also associated with alterations in resting-state functional connectivity, particularly in networks associated with cognitive control (central executive network; CEN), salience (salience network; SAL), and self-referential processing (default mode network; DMN). 14 Compared to healthy individuals, patients with MDD show hypoconnectivity within regions of the CEN and hyperconnectivity between medial brain regions that form part of the dorsal DMN (dDMN). 14 These changes in the internal network cohesion appear to occur in the context of reduced functional integration between resting-state networks. 14 Collectively, these task and resting-state abnormalities in brain functional connectivity represent the network-level correlates of the emotional dysregulation commonly observed in MDD populations.
Digital therapeutics such as cognitive–emotional training offer significant promise as treatment interventions for MDD because of the theoretical potential to target and ameliorate the neural network abnormalities observed in MDD. With this in mind, the Emotional Faces Memory Task (EFMT) was developed and evaluated as a digital therapeutic cognitive–emotional training exercise that aims to enhance cognitive control for emotional information processing (and accordingly, improve emotion regulation) in MDD by targeting the activation of both cognitive control and emotional processing networks. 15 We have previously shown in two trials using a double-blind, randomized, sham-controlled clinical trial design that EFMT training is beneficial in reducing depressive symptoms in patients with MDD.16,17 In this study, we explored the potential neural mechanisms underlying this clinical effect. Specifically, we acquired resting-state and emotional working memory task-related fMRI data from 14 patients with MDD who underwent the same scanning protocol prior to and after six weeks of EFMT training. We then examined whether EFMT training was associated with changes in functional connectivity in resting-state networks and effective connectivity within the emotion processing and working memory networks. We hypothesized that EFMT training would enhance the functional integration of resting-state networks and the effective connectivity from cortical control brain regions to regions involved in emotional responses.
Methods
Subjects
Between December 2014 and April 2017, 25 unmedicated MDD participants in a current major depressive episode (MDE) were recruited to participate in this study protocol, which involved undergoing an fMRI scan before and after completing six weeks of EFMT or sham-control training (CT) as part of a parent clinical trial protocol (NCT01934491). Participants were recruited online and through advertisements in local newspapers for depression research studies. All participants were between the ages of 18 and 55 and were evaluated by trained clinicians using the Structured Clinical Interview for DSM-IV-TR Axis I Disorders (SCID). 18 Other Axis I comorbid diagnoses (excluding psychotic disorders, bipolar disorders, substance abuse, or dependence within the past six months) were permitted as long as the participants’ MDD diagnosis was considered to be primary. MDD severity, as measured by the Hamilton Depression Rating Scale—17-item version (Ham-D), 19 had to be at least “moderate” (Ham-D ≥16). Participants with very severe MDD (Ham-D ≥27) were excluded and referred for treatment. Participants who reported taking any antidepressant medications during their current MDE as well as those with a history of treatment nonresponse (2+ failures of an adequate trial of a standard antidepressant medication) were excluded from participation. Cognitive–behavioral therapy attendance in the six weeks prior to, or at any time during, the study was also exclusionary as per the protocol, and participants were asked to refrain from any cognitive-enhancing activities (e.g., mindfulness training programs, memory exercises, etc.) during the study. Participants with unstable medical illnesses were excluded from the study; however, stable illnesses were allowed and participants could take medication for those as needed during the study (e.g., hypertension). Participants with visual or motor impairments who were thought to interfere with performance on the EFMT training were also excluded, as were participants with a history of head trauma with loss of consciousness.
The protocol and study procedures were approved by the Program for the Protection of Human Subjects at the Icahn School of Medicine at Mount Sinai (ISMMS) and were conducted in accordance with the Declaration of Helsinki. After an initial prescreening interview, potentially eligible participants were informed about the study procedures and signed informed consent to complete screening and baseline procedures. Participants who were eligible for and enrolled in the parent clinical trial investigating EFMT efficacy were subsequently offered enrollment in the fMRI study protocol and provided informed consent if they elected to participate. Participants were reimbursed for each study session completed to compensate for time and travel expenses.
Procedures
The study intervention (EFMT) was administered over 20 separate research visits. At the first visit, the SCID and Ham-D were administered to confirm MDD diagnosis and determine symptom severity. A subsequent baseline evaluation was conducted, which included the pretreatment fMRI scan. Participants were randomly assigned to the EFMT or CT groups by a research coordinator using a predetermined randomization sequence for group assignment. Participants were assigned to complete 18 training sessions over six weeks (an approximate duration of 20–35 min each, three times per week). Participants who failed to complete at least two training sessions in any week or who missed more than three training sessions during the course of the study were discontinued as per the clinical trial protocol. Weekly depression severity (Ham-D) assessments were conducted by PhD- or MD-level clinicians who were blind to group assignment. Ham-D raters were extensively trained to administer the assessment and demonstrated an intraclass correlation coefficient (ICC) >0.8 on two separate training interviews. An outcome evaluation was conducted within one week of completing the training sessions, at which time baseline assessments and the fMRI scanning procedures were repeated.
Digital Therapeutic Interventions
EFMT has been fully described in previous publications.15,16 EFMT is a digital therapeutic cognitive–emotional training exercise designed to enhance cognitive control for emotional information processing and improve emotion regulation by targeting the activation of both cognitive control and emotional processing networks. The EFMT intervention combines cognitive tasks known to elicit activity specifically in the dorsolateral prefrontal cortex (DPFC) and AMG: working memory and emotion identification, respectively.20,21 Indeed, a version of this task demonstrated simultaneous activation of the DPFC and AMG in a sample of healthy volunteers.
22
To do so, EFMT prompts participants to remember the emotions observed on a series of faces, displayed one at a time on a computer screen. For each face observed, the participant must indicate whether the emotion on the face matches the emotion shown N (number) of faces prior. The task difficulty level (N) is modulated depending on the participant’s performance to ensure a consistent challenge and engagement of the targeted neural networks. Thus, the EFMT task involves exerting cognitive control over emotional information processing and is hypothesized to induce simultaneous activation of AMG and DPFC. Figure 1 depicts an example trial sequence in the EFMT task. The sham cognitive training (CT condition) was administered in identical fashion to the EFMT condition. Both training regimens were delivered via desktop computer in a private room in the lab setting, three times per week as scheduled by the participant. The CT condition involved a working memory training exercise which utilized the same N-back paradigm as EFMT, but included neutral shapes as stimuli instead of emotional faces so no emotion processing or limbic activation was expected. For each shape observed, the participant must indicate whether the shape is the same as the one shown N (number) of shapes prior, with task difficulty level (N) modulated across blocks depending on the participant’s performance to ensure a consistent challenge. A session of EFMT or CT can take approximately 15 to 25 min to complete, and the study regimen involved completing 18 sessions of EFMT or CT over a six-week period (three sessions per week for six weeks).
Example EFMT trial. Participants observe an expression of facial affect shown on screen for 1 s and identify the emotion expressed. Participants then compare the observed emotion to the emotion observed N faces prior, in this case N = 2 faces prior.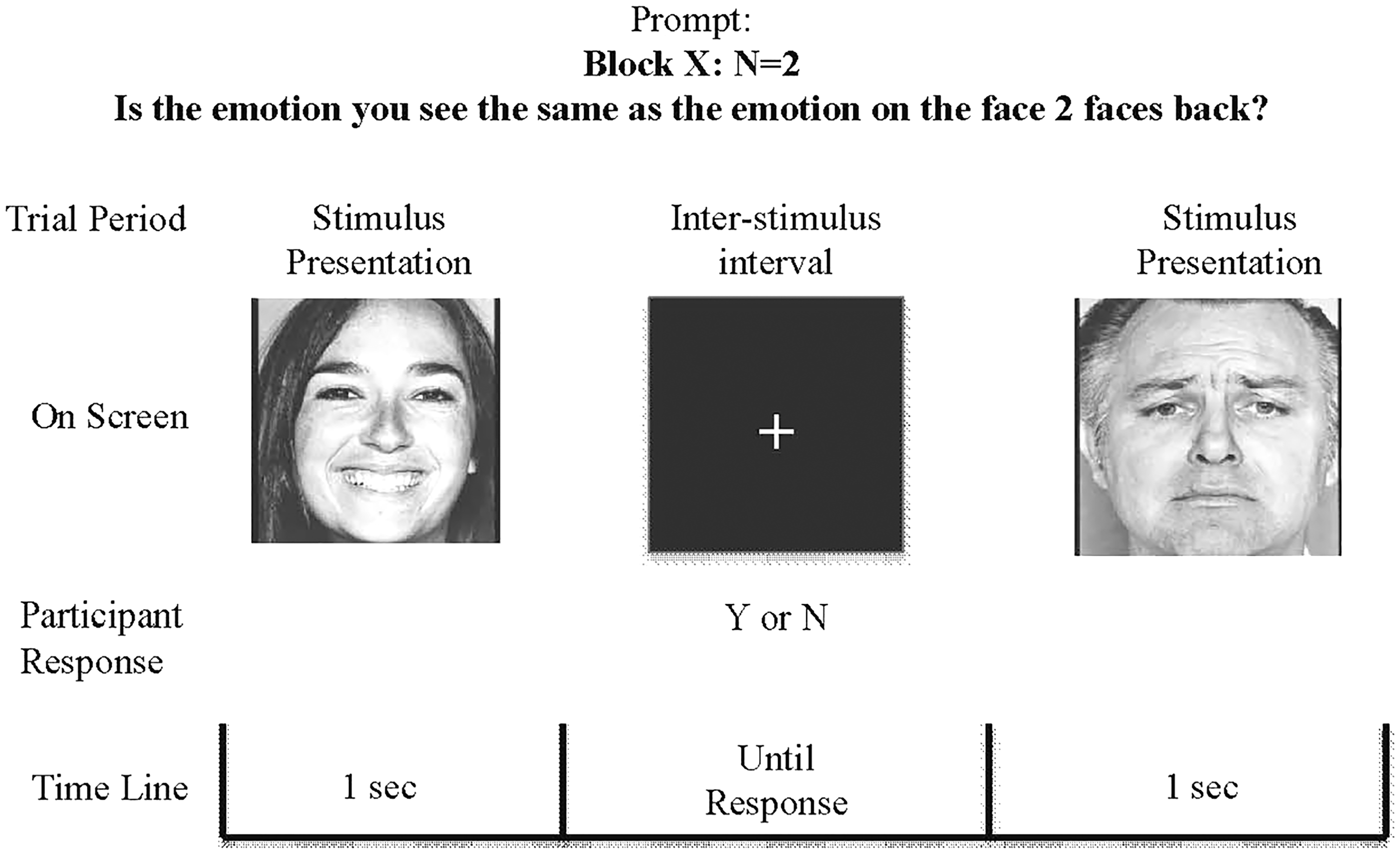
Neuroimaging Data Acquisition
Imaging data were acquired at ISMMS on a 3 T Skyra scanner (Siemens, Erlangen, Germany) with a 32-channel receiver coil. Participants were scanned at study enrollment (baseline) and within one week after completing six weeks of EFMT training. Anatomical as well as resting-state and task-based FMRI data were acquired. The task consisted of an abridged and modified version of an EFMT session. Twelve blocks of 10 trials began with a 2.5 s cue identifying the target type (0-back, 1-back, or 2-back). In 0-back trials, subjects viewed a target image (a face depicting an emotion) and indicated if each subsequent stimulus was exactly the same image as the target image. In the 1-back and 2-back trials, participants indicated whether each face depicted the same emotion as the face that was presented either “1-back” or “2-back” (respectively). The anatomical, resting-state, and task acquisitions were identical at baseline and posttreatment for all participants.
The resting-state and task-fMRI data were acquired using a T2* single-shot echo-planar gradient echo imaging sequence with the following parameters: time to echo/repetition time (TE/TR) = 35/1000 ms, 2.1 mm isotropic resolution, 70 contiguous axial slices for whole brain coverage, field of view (FOV): 206 × 181 × 147 mm3, matrix size: 96 × 84, 60° flip angle, multiband factor 7, blipped CAIPIRINHA (Controlled Aliasing in Parallel Imaging Results in Higher Acceleration) phase-encoding shift = FOV/3, ∼2 kHz/pixel bandwidth with ramp sampling, echo spacing: 0.68 ms, and echo train length: 57.1 ms. The duration of the resting-state acquisition was 10 min and the duration of the WM task was 7 min 34 s. Structural images were acquired using a T1-weighted, 3D magnetization-prepared rapid gradient-echo sequence (FOV: 256 × 256 × 179 mm3, matrix size: 320 × 320, 0.8 mm isotropic resolution, TE/TR = 2.07/2400 ms, inversion time = 1000 ms, 8° flip angle with binomial (1,−1) fat saturation, bandwidth 240 Hz/pixel, echo spacing 7.6 ms, in-plane acceleration (GeneRalized Autocalibrating Partial Parallel Acquisition) factor 2, and total acquisition time of 7 min.
Neuroimaging Preprocessing and Quality Assurance
Task and resting-state fMRI (rs-fMRI) data acquired at baseline and posttreatment were preprocessed separately using identical methods. All analyses were implemented using the Statistical Parametric Mapping software, version 12 (SPM12; www.fil.ion.ucl.ac.uk/spm/software/spm12/) and the Data Processing and Analysis for Brain Imaging Toolbox. 23 Each fMRI dataset was motion corrected to the first volume with rigid-body alignment; coregistration between the functional scans and the anatomical T1 scan; spatial normalization of the functional images into Montreal Neurological Institute stereotaxic standard space; spatial smoothing within functional mask with a 6 mm at full width at half-maximum Gaussian kernel. Resting-state data were additionally preprocessed to correct for head motion using the following steps: wavelet despiking (removing signal transients related to small amplitude (<1 mm) head movements), 24 detrending, and multiple regression of motion parameters and their derivatives (24-parameter model) 25 as well as white matter (WM), cerebrospinal fluid (CSF) time series, and their linear trends. The WM and CSF signals were computed using a component-based noise reduction method (CompCor, five principal components). 26 Finally, a bandpass filtering was applied (0.01–0.1 Hz). Individual task- and rs-fMRI datasets were excluded if volume-to-volume head motion was above 3 mm or 1°. No significant differences were present in maximal or mean head motion between baseline and follow-up scans (all p > 0.2).
Resting-State Network Connectivity Analysis
rs-fMRI data acquired at baseline and posttreatment were analyzed separately using identical methods as described below. We focused on the resting-state networks that are most relevant to MDD. Specifically, we examined connectivity of the ventral (vDMN) and dDMN, the left CEN (LCEN) and right CEN (RCEN), and the SAL. To ensure the reproducibility of the analyses, these networks were defined using validated and freely available templates provided by the Functional Imaging in Neuropsychiatry Disorders Lab, Stanford University (http://findlab.stanford.edu/functional_ROIs.html; Figure 2(a)).
27
In each participant, we calculated the within- and between-network functional connectivity of each network that respectively reflect functional cohesiveness and segregation. For the within-network functional connectivity, we computed the average voxelwise time series within each network region and then calculated and averaged the pairwise Pearson’s correlations between network regions. For the between-network functional connectivity, we first calculated an average time series within each network (averaging all the time series of the voxels part of the network) and then computed the Pearson’s correlation between each pair of networks’ time series. Both within- and between-network measures were further Fisher Z-transformed.
Resting-state functional connectivity. (a) Spatial distribution of the resting-state networks examined. (b) Effect size of posttreatment changes in within-network and between-network functional connectivity; only those with effect size > 0.3 are shown. dDMN: dorsal default mode network; vDMN: ventral default mode network; SAL: salience network; LCEN: left central executive network; RCEN: right central executive network.
Task-Based fMRI (Connectivity) Analysis
Posttreatment change in task-related brain activation.

Note: Coordinates are shown in MNI space; x = axial; y = coronal; z = sagittal. We used cluster-level inference to identify spatially contiguous voxels at a threshold of p < 0.001, without correction, and then applied a familywise error-corrected cluster-extent threshold of p < 0.05 to infer statistical significance.
Statistical Analysis Strategy
Effect sizes for repeated measures based on Cohen’s d were computed to estimate the posttreatment changes of any given functional measure using the formula:
Results
Study Sample and Clinical Characteristics
Demographic and clinical characteristics of the sample.

Note: Values represent mean (SD) or n. MDD: major depressive disorder.
In the parent clinical trial from which participants in this study were derived, EFMT was observed to result in significantly superior MDD symptom reduction from baseline to study outcome compared to CT. 17 The 14 participants in the present sample also demonstrated, on average, a clinical response to the EFMT intervention (Ham-D improvement from a mean score of 19.14 (SD = 2.6) at baseline to a mean score of 11.43 (SD = 5.12) at study outcome; t(13) = 6.88, p < 0.001).
Posttreatment Changes in Resting-State Functional Connectivity
We observed posttreatment reductions in within-network connectivity in the dDMN (d = −0.38) and SAL (d = −0.36) (Figure 2(b)). By contrast, connectivity was increased between the LCEN and RCEN (d = 0.30), between the vDMN and dDMN (d = 0.32), and between the LCEN and both vDMN (d = 0.45) and SAL (d = 0.53; Figure 2(b)). None of these findings reached statistical significance. The correlations between changes in resting-state connectivity and symptomatic change posttreatment were generally low and did not reach statistical significance.
Effective Connectivity
We observed bilateral posttreatment reductions in the effective connectivity from the dACC to the AMG (left: d = −0.44; right: d = −0.32) and right-sided increase in the top-down connectivity from the DPFC to the AMG (d = 0.33; Figure 3). The posttreatment change in effective connectivity from both DPFC and DACC to the AMG correlated with a reduction in depressive symptoms as measured with the total score of the HAM-D, with the latter significant at an uncorrected threshold (r = 0.51, p = 0.05).
Effective connectivity during the EFMT task. (a) Schematic representation of the change pre- to posteffective connectivity between dACC, DPFC, and AMG during the EFMT. Solid arrow indicates enhanced connectivity; dashed arrow indicates reduced connectivity. (b) Bars represent changes in effective connectivity during EFMT task completion from pre to post-EFMT treatment. AMG: amygdala; dACC: dorsal anterior cingulate cortex; DPFC: dorsolateral prefrontal cortex.
Discussion
We present initial data on the potential neural mechanisms associated with the beneficial effect of a digital therapeutic intervention for depressive symptoms in patients with MDD. The main finding was that, post-EMFT, the working memory-induced connectivity from cognitive control regions (the right DPFC and bilateral dACC) to the right AMG was modulated, and this modulation was associated with symptomatic improvement. Effective connectivity from the right DPFC to AMG was increased and, at the same time, effective connectivity from the dACC to the AMG was reduced posttreatment, both of which correlated with MDD symptomatic improvement. We also observed posttreatment reduction in the functional connectivity of the dDMN and SAL and increased integration between the cognitive control network and networks involved in self-referential and salience processing.
Effective connectivity can be considered an index of short-term neural network level plasticity.36–38 This short-term plasticity represents a fundamental mechanism by which the brain alters or contextualizes its connectivity and functions in response to external or internal cues. 39 There is emerging yet compelling evidence that cognitive training induces plastic changes in the resting-state architecture of the brain40–42 and in the cognitive control network.43,44 The data presented here suggest that EFMT training is also likely to induce neuroplastic changes in patients with MDD. Previous studies have suggested a degree of lateralization in prefrontal dysfunction in MDD, with abnormalities in right DPFC being primarily associated with reduced voluntary control of emotional processing. 45 It is therefore noteworthy that the effective connectivity changes observed posttreatment were more pronounced for the right DPFC. A further posttreatment change concerned the weakening of the functional coupling between the dACC and AMG. It has been suggested that the dACC shows maladaptive inflexibility in MDD 46 because its connectivity does not show the expected variation across different tasks. 47 We observed a weakening of the connectivity from the dACC to the AMG after the EFMT intervention, and this was associated with symptomatic improvement. It is therefore possible that the reduction in the effective connectivity of the dACC following EFMT training may reflect a shift toward improved dACC functioning in MDD. These results are consistent with the notion that depressive symptoms in MDD may arise or persist through reduced regulatory control of limbic regions. 48 The symptom improvement observed in this study appears to be associated with restoration of the regulatory control of limbic regions as indicated by increased DPFC and decreased dACC connectivity with AMG. This is also consistent with the hypothesized target and mechanism of action for EFMT-modulating the imbalance in activation patterns between cortical and limbic brain regions involved in cognitive control and emotion processing, respectively. 15
Hypoconnectivity and reduced integration of frontoparietal resting-state networks have been identified as a reliable correlate of MDD. 14 It is therefore interesting that most of the posttreatment changes in between-network resting-state functional connectivity resulting from EFMT concern the CEN, which is considered a key network for cognitive control. 49 The CEN was more integrated across the left and right hemispheres, and with the DMN and SAL, after EFMT. This increase in the integration between networks for cognitive control, self-referential, and salience processing has the potential to facilitate a more coherent and coordinated response to emotional stimuli in patients with MDD. Moreover, there was also evidence for posttreatment reduction in the functional connectivity of the dDMN, which has also been observed following successful treatment with antidepressants. 50
It is important to consider a number of methodological issues. The anatomical model used in the DCM analysis does include brain regions that could be engaged by the task. However, dynamic causal network models are not intended to reproduce all known aspects of the functional neuroanatomy of working memory. This is because overly complex models will start fitting noise (overfitting) and will therefore be less generalizable. In DCM, the network of interest is best modeled using the simplest possible circuit diagram that can account for the observed data.33,34 Importantly, the interpretation of the study results is limited by the small sample size and the lack of a placebo control group in the analyses. The effect size of posttreatment changes in resting-state and in task-related connectivity suggests that larger samples are necessary for appropriately powered future studies. The lack of a placebo control group makes it difficult to discern treatment effects from nonspecific effects associated with symptomatic improvement and the greater familiarity of participants with the scanning set-up during the follow-up scan. Nonetheless, the results reported here provide encouraging preliminary support for the potential neural mechanisms associated with the beneficial effect of a digital therapeutic intervention for depressive symptoms in patients with MDD.
Conclusion
In summary, the findings presented here provide first insights into the possible effect of cognitive–emotional training at the neural network level, which appear to implicate mechanisms of short-term plasticity of interregional brain connections. Our findings further suggest that EFMT may provide a promising new intervention for the treatment of MDD that could be further evaluated in larger studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Authors Hoch, Doucet, Moser, Lee, Huryk, DeWilde, Fleysher, and Frangou declare that they have no competing interests. Dr Iacoviello is an adjunct faculty member of the Icahn School of Medicine at Mount Sinai (ISMMS) and is employed full time as the Head of Discovery and Translational Research at Click Therapeutics. Prior to joining Click Therapeutics, Dr Iacoviello (in his role as a full time faculty member at ISMMS) and Dr Charney (Dean of the Icahn School of Medicine at Mount Sinai) codeveloped EFMT as a computer-based brain training exercise for the treatment of depression. Drs Iacoviello and Charney are named coinventors on a patent filed by ISMMS to develop this therapeutic approach as a mobile/remote program (app). There is a licensing agreement between Mount Sinai and Click Therapeutics to develop this technology; if a commercial product is developed, Mount Sinai, Dr Iacoviello, and Dr Charney would benefit financially. Dr Iacoviello has served as a consultant to Fortress Biotech, Inc. and reports grant funding from the National Institutes of Health and the Brain and Behavior Research Foundation. In the past three years, Dr Murrough has provided consultation services to Allergan, Fortress Biotech, Novartis, Janssen Research and Development, Genentech, ProPhase, and Global Medical Education and has received research support from Avanir Pharmaceuticals. In the past five years, Dr Iosifescu has consulted for Avanir, Axome, CNS Response, INSYS Therapeutics, Lundbeck, Otsuka, Servier, and Sunovion, and he has received grant/research support through the Icahn School of Medicine at Mount Sinai from Alkermes, Astra Zeneca, Brainsway, Euthymics, Litecure, Neosync, Roche, and Shire.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health grant 5K23MH099223 and the Brain and Behavior Research Foundation (awarding NARSAD Grants) Young Investigator grant #24100, both to B.M.I.