
Abstract
Background
Although childhood endangerment often precedes adult posttraumatic stress disorder (PTSD), the mechanism from danger to disorder is unclear. We proposed a developmental process in which unprotected and uncomforted danger in childhood would be associated with “shortcuts” in information processing that, in adulthood, could result in PTSD if the adult experienced additional exposure to danger. Information processing was defined as the basic associative, dissociative, and integrative processes used by all humans. Individual differences in parents’ (or primary caregivers’) protective and comforting behavior were expected to force unprotected children to use psychological shortcuts that linked early trauma to later vulnerability for PTSD.
Method
We compared 22 adults with chronic PTSD to (a) 22 adults with other psychiatric diagnoses and (b) 22 normative adults without any diagnosis, in terms of information processing around childhood danger. The Adult Attachment Interview was used to derive information processing variables, including self-protective strategies, childhood traumas, and depression.
Results
The two patient groups differed from the normative group on all variables. Adults with chronic PTSD differed from other psychiatric patients in having more childhood traumas and using more transformations of associative and dissociative processes. Within the PTSD group, there were three psychologically different subgroups.
Conclusion
Our findings suggest that (1) prediction of risk for adult PTSD may be possible, (2) treatment might be facilitated by provision of a protective and supportive therapist, (3) who included a focus on correction of information processing errors and use of more adaptive strategies, and (4) subgroups of adults with PTSD may require different forms of treatment.
Keywords
Introduction
Up to now, the roots of posttraumatic stress disorder (PTSD) have not been well understood. We wondered if that was partly attributable to considering it a disorder, rather than an adaptive process gone awry. In this study, we explored the notion that PTSD may be a distressing by-product of the human mind’s evolved ability to learn from experience. Specifically, we propose that the psychological processes associated with PTSD may serve self-protective functions, and we suggest conditions under which they might become maladaptive. We then test our hypothesis on a set of adults with chronic PTSD as compared to archival data on adults with other psychiatric disorders and without any disorder. We defined chronic PTSD as having the diagnosis for six or more months.
Information Processing and Danger
Early exposure to danger influences how individuals respond to future danger by changing the way they process information about danger. 1 Two crucial learned processes are the perceptual processes of inattention or attention and the cortical processes of keeping information apart (dissociation) or connecting it (association). These processes are central to adaptation, but require judicious application such that one attends to and connects relevant information while avoiding attention to and dismissing irrelevant information. These processes correspond to the Diagnostic and Statistical Manual of Mental Disorders (DSM, APA) 2 and International Statistical Classification of Diseases and Related Health Problems (ICD), 3 diagnostic criteria for PTSD of “avoiding/dismissing” the traumatizing event, and feelings associated with it, alternating with a “preoccupying” focus upon the event and a heightening of feelings associated with it. 4 In PTSD, the processes may be misapplied, resulting in omission (dismissing) of relevant protective information and preoccupation with irrelevant information.
Because danger is not the same for everyone, nor for all time, recognizing danger and generating self-protective strategies requires learning and, sometimes, conscious reflection. Moreover, the signs of impending danger are often complex, ambiguous, or inconsistently predictive. Although the brain is evolved to give preferential attention to signs of danger, 5 the long period of childhood is needed for children to learn to recognize the signs of danger and to organize self-protective strategies. This developmental process shapes how the brain organizes and functions in the future.6,7 Early capabilities are reflexively simple and fast, whereas maturation enables more complex, but slower, cortical processing that yields more accurate prediction and more nuanced responses.
Information Processing and PTSD
When parents (or other primary caregivers) are protective and comforting, children are kept safe while they learn to recognize and respond to danger. This promotes gradual adaptation and brain development which is the basis of resilience in the face of threat.
When parents themselves are the source of threat
8
or when they fail to provide comfort, children may rely on psychological “shortcuts” and reflexive responses. Shortcuts simplify complex conditions by omitting or transforming information (see the transformations of cognitive and affective information in Figure 1). The most frequent shortcuts are over-generalization of instances such that they are treated as universally present and reductionist assignment of blame exclusively to one party in a dispute. For example, instead of recognizing that the mother is often violent, but sometimes caring, the adult recalls the mother only as “violent.” Similarly, instead of recognizing that, when the mother belittled the father, the father slapped the mother, the adult recalls that the mother was victimized by the abusive father. In the first example, making the danger of the mother absolute bypasses the more complex process of understanding the conditions under which she is likely to be dangerous. In the second example, the shortcut bypasses the complexity of parental disputes (that the child would be unlikely to understand) and avoids the distressing recognition that both parents endanger the child. Psychological shortcuts enable children to organize protective strategies, albeit without subtlety or flexibility.
The Dynamic-Maturational Model (DMM) of strategies of attachment and adaptation and transformations of cognitive and affective information associated with each strategy.
Truncated psychological processes shape children’s neurological organization in ways that can be adaptive in the short-term, but also indicative of “psychological trauma.” 9 Children with psychological trauma are over-prepared for the types of threat that they have experienced, but unprepared for other threats or to reflect on discrepant outcomes when simple strategies fail. Repeated failures to identify actual danger or self-endangering responses to expected danger that does not occur can lead to feelings of depression.
PTSD and Prior Exposure to Danger
It is now widely recognized that people with PTSD have often been exposed to danger as children10–12 and that those who later develop chronic PTSD have structural changes in their brains. 13 However, not everyone who was exposed to childhood danger experiences either psychological trauma in childhood or PTSD following exposure to danger in adulthood. 14 Indeed, the problem is not danger per se; everyone experiences danger. The issue is the fit of the threat to the children’s readiness to protect and comfort themselves which in turn depends on parents’ ability to modulate the threat.
We propose that children who have not been sufficiently protected or comforted by their caregivers may generate information processing shortcuts to reduce the perception of vulnerability or increase their vigilance to threat or both. When carried forward over time and combined with reduced integrative correction, these can be considered psychological traumas and yield vulnerability to PTSD in adulthood. 15 This vulnerability might be recognized by the number and complexity of trauma-triggering stimuli. We expected that other psychiatric disorders would be associated with fewer and less complex psychological traumas from childhood events.
PTSD and Attachment Theory
We used attachment theory to address these issues because attachment theory is built around protection from danger,16,17 defines parents’ attachment role in terms of protection and comfort, describes three basic self-protective strategies that reflect infants’ responses to parents who differ in the provision of protection and comfort, 18 and connects the strategies to information processing. 17 The function of attachment figures is to protect children from dangers that exceed the child’s capacity for self-protection and to comfort children who have become distressed by danger or threat of danger. Children use information about their parents’ protection and comfort to organize their own self-protective strategies. When children cannot elicit parental protection and comfort, they may experience psychological trauma. Attachment theory, in other words, offers a developmental process from danger through parental caregiving to resultant information processing that yields behavioral strategies and, sometimes, psychological trauma. In cases of inadequate parental caregiving, children’s strategies and trauma may be among the long-term effects of unprotected and uncomforted endangerment.
The Type A strategy, as defined by Ainsworth, 18 reflects dismissing processes used with rejecting and sometimes dangerous attachment figures. The Ainsworth Type C strategy reflects preoccupying processes used with caring but unpredictable and sometimes deceptive parents. The Ainsworth Type B strategy reflects the judicious integration of dismissing and preoccupying processes in which irrelevant information is dismissed and relevant information is kept active. For example, a child who was attacked, when outside alone at night, by a man in a red jacket would dismiss the information about the red jacket as irrelevant to future danger and retain the information about being outside alone at night. This usually occurs in the context of protective and comforting attachment figures. 19 A child using a Type A strategy would dismiss the whole event, whereas a child using a Type C strategy would focus on red jackets as signals of danger and omit information about their own behavior. These ABC strategies are expanded over the course of childhood until there is a wide range of possible protective strategies in adulthood. 20 In addition, the Adult Attachment Interview (AAI), 21 is suitable for assessing adults’ psychological traumas, information processing, and protective strategies.
There are several models of attachment theory that extend Ainsworth’s infant A1-2, B, and C1-2 strategies to adulthood. We used the Dynamic-Maturational Model of Attachment and Adaptation (DMM)19,22 because it structures the A and C strategies as information processing opposites of dismissing (A) and preoccupying (C) processes, 23 differentiates among at risk adults 24 and is validated by functional magnetic resonance imaging (fMRI) data that connect the strategies to information processing.25,26 One finding in the fMRI studies stands out as particularly relevant to the childhood experience of adults with chronic PTSD: mothers using a Type A strategy showed little neural activation when shown photographs of their own sad or crying infants, whereas mother using a Type B strategy showed substantial activation. This provides a neural correlate for Ainsworth’s observation that mothers of infants using a Type A strategy were rejecting of the infants’ attachment behavior; further, it suggests that in cases of substantial threat some children might not be protected or comforted. The Ainsworth strategies have been associated with infants, children, and adolescents from advantaged populations who faced few dangers and were adequately protected and comforted whereas the DMM strategies have been associated with risk populations and families. 19
The DMM offers six “dismissing” strategies (A3-8) and six “preoccupying” strategies (C3-8) as well as A/C combinations; each strategy is defined by differences in transformations of information (see Figure 1). Further, the DMM offers 14 types of trauma that describe increasingly complex attempts to make meaning of the danger; the extreme points of lack of understanding are “depressed” (non-activating) and “disorganized” (excessively activating) trauma (see Figure 2). In addition, a generalized state of depressed absence of strategic motivation can be discerned; this is coded from AAIs when the participant’s arousal is low (e.g., sighs), and there are statements of futility. DMM-depression renders the individual’s strategy ineffective; being more narrowly defined, it is not identical to the broader psychiatric diagnosis of depression.
Fourteen DMM types of dismissed and preoccupying psychological trauma.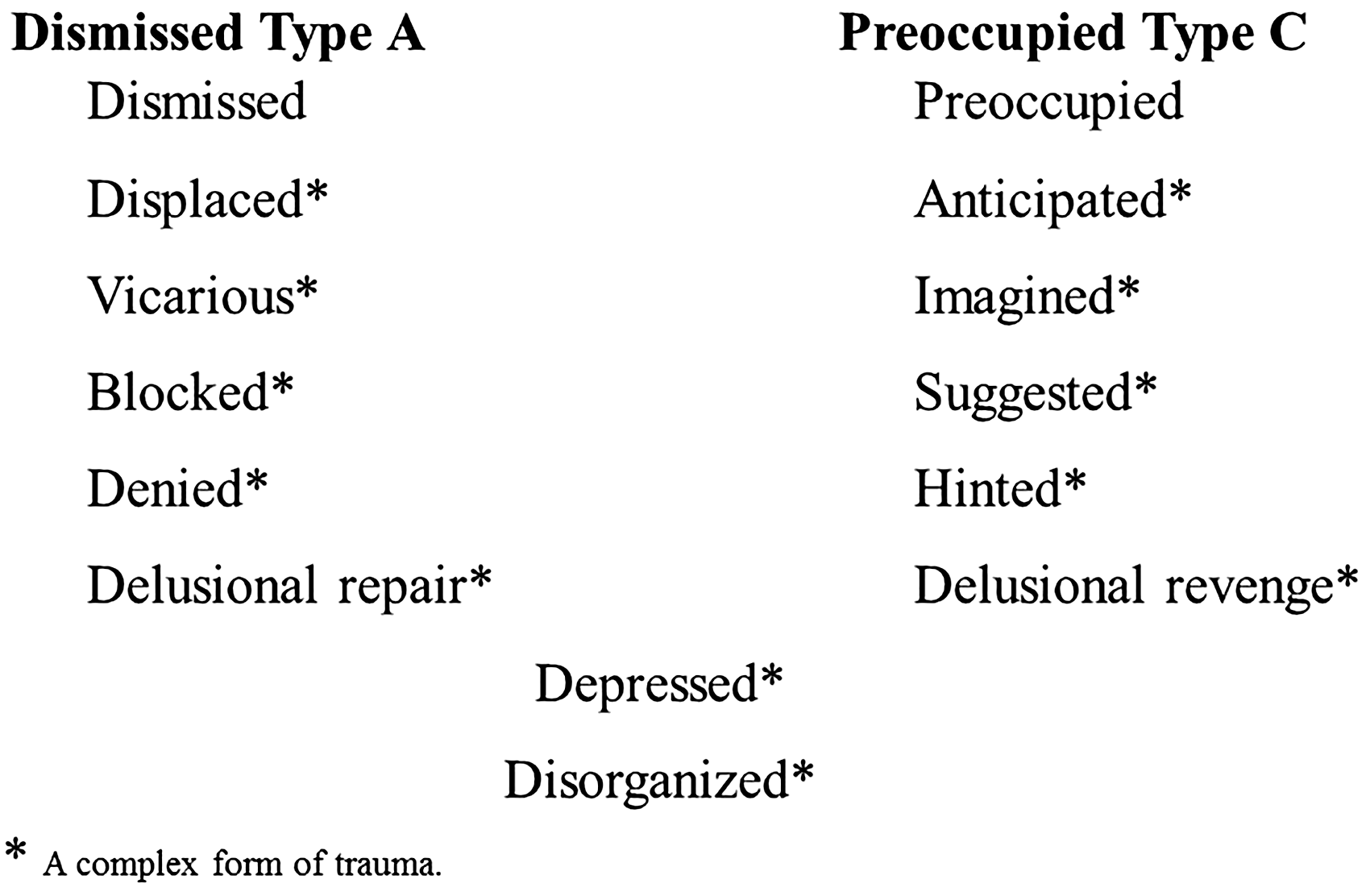
Empirically, the AAI coded with the DMM method, i.e., the DMM-AAI, differentiates several types of disorder: trauma, 27 anxiety disorders, 28 maltreatment,29,30 eating disorders,31,32 avoidant personality disorder, 33 and borderline personality disorder (BPD). 34 With regard specifically to psychological trauma, BPD was typified by “blocked” trauma from child sexual abuse; that is, there were many discourse markers associated with abuse in the AAIs of women with BPD, but the women could not recall the event and denied its occurrence. Women with eating disorders frequently “imagined” erroneously that the eating disorder had been caused by an actual event that was very unlikely to be causal to the eating disorder. Several of these studies (for example, maltreatment and eating disorders) revealed subgroups within the diagnostic group; we thought that might be the case with PTSD as well. In this study, we used the DMM-AAI to differentiate adults with chronic PTSD from adults with other psychiatric diagnoses and adults with no diagnosis and to explore differences within the PTSD group.
Hypotheses
Our central hypothesis was that adults with chronic PTSD would have experienced childhood dangers beyond their readiness to adapt and without parental protection and comfort, with the outcome of psychological trauma that left them vulnerable in adulthood to PTSD in the event of further endangerment. We tested this general hypothesis with three specific hypotheses:
Adults with psychiatric diagnoses would more often use DMM self-protective strategies, and have evidence of complex forms of trauma and depression than adults without diagnoses. Adults with chronic PTSD would use a narrower range of strategies and have more childhood traumas, more complex dismissed and preoccupying forms of trauma, and more depression than adults with other diagnoses. Among adults with PTSD, there would be subgroups that would differ in strategy and information processing about trauma.
Method
Participants
The participants were 66 White adults (33 men) ranging in age from 30 to 67 years (mean 47 years). Their 66 AAIs were drawn from an archive of almost 1000 normative and clinical adults in England whose anonymized AAIs had been gathered by participants in DMM-AAI courses. Each participant had given written consent, in a manner that was accepted by their local authority, for the anonymized use of their AAI. The use of such archival data is excluded from approval by research ethics committees. 35 The clinical adults comprised two groups: chronic PTSD (without comorbidity) and mixed diagnosis (all other diagnoses). Because the participants with chronic PTSD completed other assessments, their participation was approved by the research ethics committee of their local National Health Service Trust. 36 The two comparison groups, normative and mixed diagnosis, were drawn to match the 22 PTSD participants on age, sex, and geographic location within England. When more than one AAI in the archive met the criteria of age, gender, and location, the one gathered closest in time to the PTSD AAI was selected.
The traumatic events experienced by the participants with PTSD included industrial accidents (18%, four men), violent personal assault (45%, four men and six women), road traffic accidents (27%, two men and four women), and death/murder of a closely attached person (9%, two men). The conditions in the mixed diagnosis group included anxiety disorder, dysphoria, bulimia, anxiety disorder with gender reassignment, alcohol dependency, hysteria, incest, depression, panic disorder, bipolar disorder, dependent personality disorder, narcissistic personality disorder, borderline personality disorder, paranoid psychosis, and rape with murder (with and without comorbidity), but none had a diagnosis of PTSD. The participants in the normative group had no history of mental illness. The participants came from all walks of life, from the long-term unemployed to professions such as law, teaching, and nursing but were not matched on socioeconomic status (SES). There were, however, no significant differences among the groups in SES.
Procedure
All participants were seen twice, once to explain the interview procedure and obtain informed consent and once to administer the AAI and gather demographic data. At this point, the data were added to the archive.
Assessment
Patient diagnoses, using DSM-IV guidelines, were extracted from the medical records; the diagnoses of PTSD were confirmed by the Impact of Events Scale. 37 We did not directly assess childhood exposure to danger in the sample because retrospective information is subject to precisely the recall biases for which we were seeking evidence, and it was the biases, not the dangers, that were our focus.
Protective strategies and psychological trauma were assessed by coding discourse elicited by the AAI. 20 The AAI explores childhood experience, beginning with non-threatening topics and moving, in a series of pre-defined probes, to increasingly threatening topics. It concludes with integrative questions about the current meaning of childhood events for the self.
By coding the linguistic structure of responses (and not their content), we sought an index of dismissing and preoccupying transformations of information that was not under participants’ conscious control. It is noteworthy that recall is not identical to experiencing the event, 38 and psychological trauma may affect what is recalled and how it is recalled. 39 Further, recall alone cannot determine whether the event actually occurred.40,41 Nevertheless, the linguistic form of recall indicates how the mind represents danger at the time of recall. The DMM-AAI identifies transformations in the structure of the participant’s language when the participant discusses childhood endangerment. The interview does not address the event in adulthood that precipitated PTSD. Because recall is often inaccurate regarding what dangerous events occurred, we did not attempt to gather a list of the dangers themselves. Instead, we assessed the structure of the participants’ language when discussing the dangers that they recalled or when denying that specific dangers had occurred. Put another way, we were interested in how the participant discussed danger, not in the array of dangers per se.
Coding and Classification of the AAIs
DMM protective strategies, strategic behavior, and sample discourse markers.

Introduced by Ainsworth 18 for infants, described here for adults.
Introduced by Crittenden. 19
Introduced by both Crittenden and Radke-Yarrow 43
All strategies have multiple markers in all six memory systems. These are only examples.
P: procedural memory; I: imaged memory; S: semantic memory; C: connotative language; E: episodic memory; N: integration; DMM: Dynamic-Maturational Model.
After coding, the discourse markers were clustered into six memory systems (with “memory systems” being a construct to denote different forms of information, derived differently through the brain, and with differing degrees of consciousness and ease of accessibility). 44 Two memory systems were preconscious (procedural and imaged memory), two were verbal and conscious (semantic memory and connotative language), and two required cortical integration (episodic memory and reflective integration).
Transcripts were assigned to the highest numbered strategy for which there was evidence in three or more memory systems by two coders who had passed the DMM-AAI reliability test. Both coders were blind to the diagnostic status of the participants. Coder 1 classified all the AAIs, with Coder 2 classifying a random selection of half of the AAIs. Disagreements were decided by conference. Inter-coder agreement, assessed using Cohen’s Kappa, between the coders was significant, based on 32 AAIs with 12 different classifications (
Results
Because the major variables were categorical, the analyses were based on the Chi-square statistic. Somers’d and linear-by-linear statistics were used to test for ordinal relations among the groups when both the independent and dependent variables were ordered. The multivariate analyses used discriminant and cluster analysis.
Hypothesis 1: Ainsworth versus DMM Strategies
The purpose of this set of analyses was to demonstrate that the DMM strategies and types of trauma were (1) used frequently enough to justify coding them and (2) associated with diagnostic status.
Strategies
All strategies in the DMM model (see the “pie slices” in Figure 1) were used by at least one participant, indicating wide variation in protective strategy within the sample (see Figure 3). Comparing the three groups indicated that only 27% of normative cases were assigned to the DMM strategies as compared to 95% of mixed-diagnosis cases and 100% of PTSD cases (
Distribution of the DMM self-protective strategies by patient group.
Psychological Trauma
To test evidence of trauma in the three groups, a dichotomous variable was constructed for the presence or absence of any trauma. The three-group analysis was significant (
Depression
We compared the three groups for the presence or absence of DMM-defined depression in AAI discourse; the two patient groups had approximately one-third of participants with depression, whereas the normative group had none (
Hypothesis 2: PTSD Patterning Compared to Other Psychiatric Disorders
These analyses tested whether there was a “signature” pattern for chronic PTSD as compared to the mixed-diagnosis group. If there were, patients with chronic PTSD would differ in a particular way from other patients in strategy, psychological traumas, or depression.
Strategies
There was no difference in the distribution of strategies between the PTSD and mixed-diagnosis groups.
Psychological Trauma
The PTSD group had more traumatizing events than the mixed-diagnosis group (Somers’d = −.456, p < .001; PTSD = 32, mixed-diagnosis = 20) and more complex traumas (Somers’d = −.393, p = .006; PTSD = 73%, mixed-diagnosis = 36%).
We tested the presence of both preoccupied and dismissed trauma by combining all forms of dismissing trauma and all forms of preoccupying trauma for each AAI, then comparing the two patient groups on the use of both processes. The groups were significantly different with 13 in the PTSD versus only 3 in the mixed-diagnosis group using both dismissing and preoccupying processes (Somers’d = − .472, p < .001). There was also a group difference in disorganized trauma (Somers’d = −.273, p = .01; PTSD = 8, mixed-diagnosis = 1).
Depression
There was no difference in depression.
Group Discrimination
To test the overall hypothesis of a difference in PTSD as compared to the other two groups on the DMM-AAI variables, we performed a discriminant analysis. The grouping variable was diagnostic status with three discriminating variables: strategy, type of childhood trauma, and presence of depression. The result was significant with all three variables in the equation (Wilks’ lambda = .873, F2, 63 = 4.57 p < .014) for both factors 1 and 2 (Wilks’ lambda = .844,
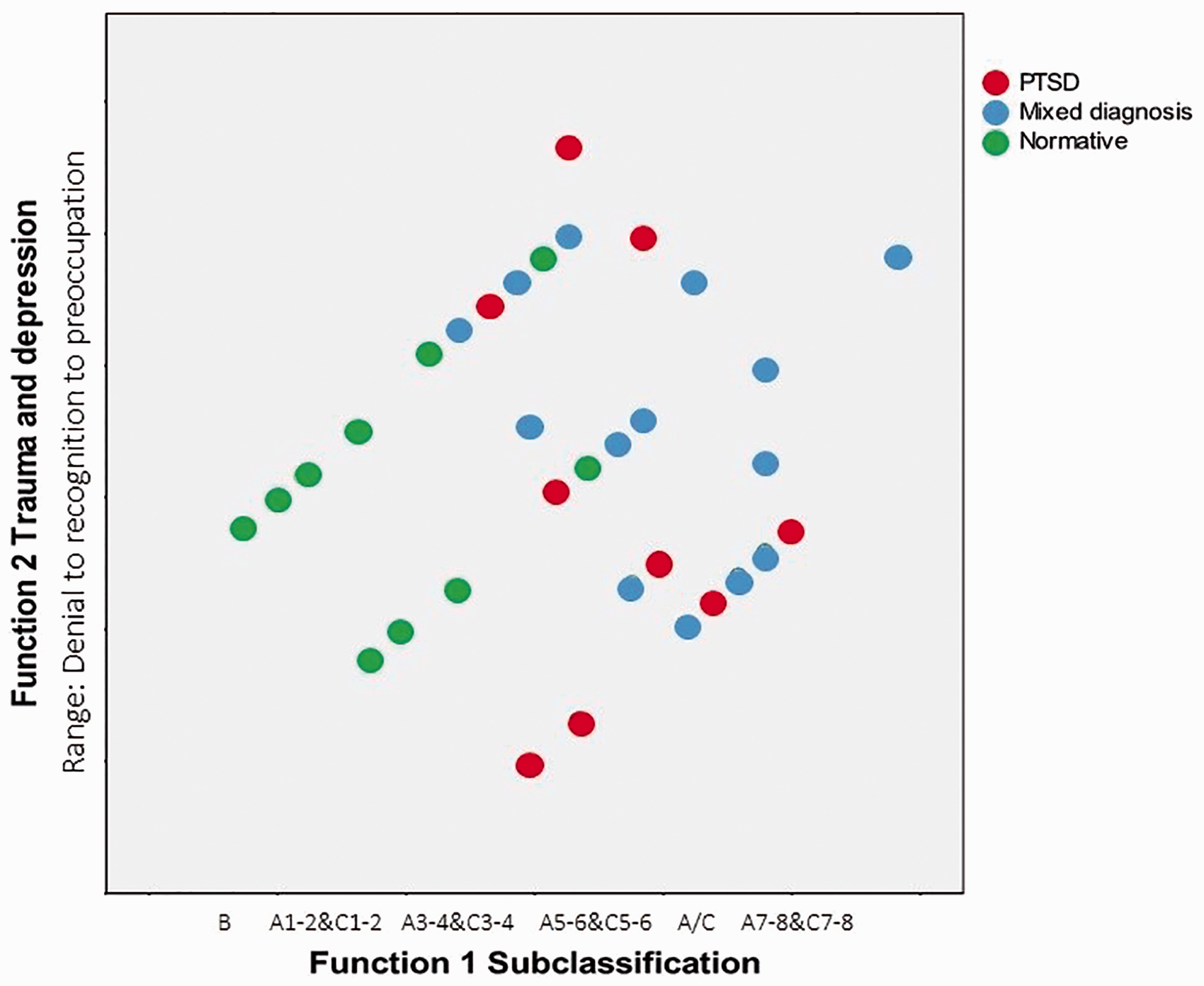
Scatterplot of the discriminant analysis of the PTSD, mixed diagnosis, and normative groups.
Hypothesis 3: Differentiating Subgroups within PTSD
To explore subgroups within the chronic PTSD group, we performed a series of cluster analyses, specifying 2–4 groups and using different means of managing the clustering. The most comprehensible outcome was a specified three-cluster solution using (1) strategy, (2) total number of traumas, (3) the presence of preoccupied-and-dismissing or disorganized trauma, and (4) depression. Cluster 1 consisted of eleven cases with C3-6 strategies, several traumas, and no depression. Cluster 2 consisted of five cases with an A/C3-6 strategy, several traumas, and no depression. Cluster 3 stood out; it consisted of six cases with a compulsive A strategy, complex traumas that always included a dismissing or disorganizing process, and depression (five of six cases). That is, the four variables differentiated three clusters of PTSD cases, with Cluster 3 being defined by Type A strategies, complex traumas and depression.
Discussion
The central hypothesis of this study was that chronic PTSD in adulthood might reflect a long-term detrimental outcome of the immature mind’s attempt to solve the problem of unprotected and uncomforted exposure to danger in childhood. To address this hypothesis, we first outlined how experience shapes the development of cognitive processes and how that, in turn, affects the manner in which the two basic processes of attention and reflection are applied to instances of danger. We hypothesized that PTSD might reflect shortcuts in attentional processes and minimal learning of reflective processes that maximized safety in the short-term. Nevertheless, dismissing important information, maintaining an excessive array of trauma-triggers, and failing to reflect on errors could reduce adaptation in the long-term. Of course, if one does not survive in the short-term, the long-term is not relevant; PTSD, in other words, may be an uncomfortable outcome of early life-preserving processes.
Utility of the DMM Classifications
Because we used the DMM expansion of Ainsworth’s infant strategies, we first tested the utility of the DMM classifications. Adults with psychiatric diagnoses were assigned, with only one exception, exclusively to the DMM strategies. Moreover, they were assigned to almost all of the DMM strategies, indicating a wide range of variation among adults with psychiatric disorder. Three-quarters of the normative controls were assigned to the Ainsworth strategies. In addition, depression and the full array of forms of trauma were found in the two patient groups. This demonstrates the relevance of the DMM strategies to clinical samples and is consistent with previous findings using the DMM-AAI.
Findings Regarding Chronic PTSD
We tested whether the chronic PTSD group (1) differed from adults with other psychiatric diagnoses in protective strategy, psychological trauma, and depression, (2) had a “signature” pattern, and (3) was heterogeneous in ways that might affect vulnerability to and treatment of PTSD. Our results indicated that adults with PTSD and other psychiatric disorders were similar in using unbalanced strategies and having high rates of depression. They differed on psychological trauma, with the PTSD group having more ongoing traumas from childhood, more complex traumas, and more dismissing-and-preoccupied traumas. These constituted the “signature” of chronic PTSD. Thus, our results suggest that adults who developed chronic PTSD in adulthood may, in childhood, have been left (or at least later perceived themselves to have been left) to fend for themselves and to draw their own meanings from experience. However, because they were immature, some of their conclusions were erroneous and maladaptive when acted upon in adulthood. Thus, chronic PTSD may reveal the limitation of children’s attempts, in the absence of supportive attachment figures, to accommodate harsh realities early in life. This suggests a possible benefit to addressing childhood issues in the treatment of adult PTSD.
Finally, there were three subgroups within the chronic PTSD group. The identification of three clusters within the PTSD group was not predicted with specificity nor are our numbers large enough for the findings to stand on their own. The finding does, however, suggest a clinically relevant hypothesis for further investigation. PTSD patients using preoccupying Type C strategies that invite assistance from others may need a different sort of treatment than patients using a dismissing Type A strategy. The latter group stands out for having been repeatedly and very seriously harmed as children. Often they recalled no loving and protective attachment figure at all. In the face of unremitting threat, they appeared to have found ways to appease powerful people at the cost of awareness of their own desires and feelings. In five of six cases, they were also depressed, indicating that the strategy was not functional.
Limitations and Future Research
This study addressed chronic PTSD, not acute PTSD. Further, using archival data has many limitations, including correlational results that do not indicate the direction of effects, lack of uniform diagnosis, and limited assessments. In addition, we did not compare individuals who do and do not develop PTSD after exposure to danger in adulthood; others have found that psychiatric status prior to being exposed to the danger that precipitated the PTSD predicted PTSD. 14 Our results need replication with a larger sample, gathered entirely for the study, and including a wider array of assessed constructs. A prospective longitudinal study of exposure to danger would be a great advantage. The economy of an archival study can lay the basis for more extensive studies.
These preliminary findings are exciting because they suggest ways to predict more precisely who is at risk for PTSD: adults with evidence of ongoing complex trauma from numerous occasions of not being protected and comforted by their parents from danger in childhood. This suggests that the basis for PTSD may be the premature application of universal protective psychological processes that were truncated because the children were too young to understand the dangers occurring early in their lives. If supported in fuller studies, this idea can move our understanding of the origins of PTSD forward from simple exposure to danger to considering the parent–child relationship as the buffer when children are not developmentally ready to cope with the threats to which they are exposed. Such awareness might not only prevent some cases of PTSD, but it would also promote the healthy development of all children.
In addition, the second author considered whether aspects of the PTSD-eliciting event in adult echoed aspects of the unresolved traumas in childhood. Although the review was subjective, she did think there were connections between the childhood and adulthood events and that these narrowed the range of possible eliciting events, for each participant, in adulthood. 36 This observation warrants systematic replication with appropriate controls in the design of the research.
Conclusions
This study leads to both clinical and theory-based conclusions. Clinically, if these characteristics of adults with chronic PTSD are replicated, then it may be possible to identify adults who might be at risk for PTSD if they were to experience severe danger. People in many occupations, including rescue workers and the military, might benefit from preventive identification of risk. Further, our findings suggest that resolution of past traumas might not be sufficient to protect vulnerable individuals because, in our sample, the adults with PTSD also used quite extreme protective strategies. Adding balanced strategies (Type B) to their repertoire might reduce exposure to danger by enabling them to avoid conflictual relationships while also improving their close relationships. Accomplishing this might be promoted by having a therapist who functioned as a transitional attachment figure, using the therapy to generate the missing resilience-building processes of childhood. 19 Finally, the best techniques to accomplish this with any particular person might be harmful for another person. For example, adults in Clusters 1 and 2 who use preoccupying Type C strategies without depression might benefit from treatment techniques that emphasize minimizing feelings, attending to contingencies, and dissociating irrelevant signals. Offering such treatment to adults in Cluster 3 (using dismissing Type A strategies, often with depression) might augment the very processes underlying their dysfunction. Similarly, exploration of feeling states would be recommended when feelings were disassociated, but not when they were over-associated. Detailed knowledge about how individuals processed information (such as can be derived from an AAI) might promote personalized treatment better than a psychiatric diagnosis.45–47 The benefits of such precision would include increased safety, reduced suffering, and comfort for both vulnerable individuals and people in close relationships with them.
The theory underlying this study emphasizes adaptation, coping, and ultimately resilience. Mental illness is often treated as a discrete illness, as if it were the psychological equivalent of a virus, a bacterial infection, or an injury. PTSD, as a psychiatric disorder, relies on an injury model: something dangerous happened that caused a psychological injury and the individual is unable to recover spontaneously. An alternative model is that the brain is evolved to adapt to the dangers inherent in life and uses experience with danger to shape its own development around the threats present in the individual’s context. This is not a new idea.48–50 Our findings both add to the growing chorus that conceptualizes mental illness in terms of universal lifespan processes that support adaptation and also illuminates the link between early exposure to danger and later dysfunction. Specifically, we found that chronic PTSD in adulthood may result from the confluence of childhood exposure to danger that is beyond children’s capacity for self-protection and self-comfort, in the context of lack of parental protection and comfort both at that time and afterwards. The result may be that the growing child fails to correct the psychological shortcuts of omission and excessive inclusion and, thus, as an adult is vulnerable to PTSD when threats in adulthood are connected to the misrepresented childhood danger. By positing that attachment figures’ protection and comfort—or absence thereof—guides the child’s developing mind, a process for predicting individual differences in outcomes is articulated. This can generate new possibilities for early identification of risk for PTSD, prevention, and treatment.
Footnotes
Acknowledgments
The authors would like to thank Robbie Duschinsky, PhD and Andrea Landini, MD for their helpful comments on earlier drafts of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.