
Abstract
Prevalence estimates of obstructive sleep apnea (OSA) continue to rise, partially due to better recognition of and screening for the disease, in part due to increase in obesity and in part due to changes in definitions of obstructive hypopneas. Despite increasing knowledge of the deleterious impact of OSA on health, underrecognition continues to be a major concern, especially in women. A middle-aged man that snores and is sleepy has been the accepted “textbook” picture of OSA; women may present with more atypical symptoms and excessive sleepiness that are not reflected on sleepiness scale questionnaires. Even when presenting with snoring and sleepiness, and in the presence of comorbidities, women are less likely to be evaluated for OSA. Symptom burden and poor health outcomes have been documented in women with OSA and treatment improves their health. In this article, we explore possible causes for this underrecognition of OSA in women, including gender bias and healthcare inequity, and propose solutions.
Obstructive sleep apnea (OSA) is a common sleep disorder characterized by recurrent episodes of partial (hypopnea) or complete (apnea) cessation of airflow, despite persistence of respiratory effort, associated with oxyhemoglobin desaturation and sleep disruption. This basic concept has remained since its original description in 1972; 1 however, the definitions of apnea, hypopnea, and oxyhemoglobin desaturation have changed over time. 2 We have included the most recent hypopnea definitions and other sleep medicine-related terms for reference (Table 1).
Definition of Sleep Medicine Related Terms.
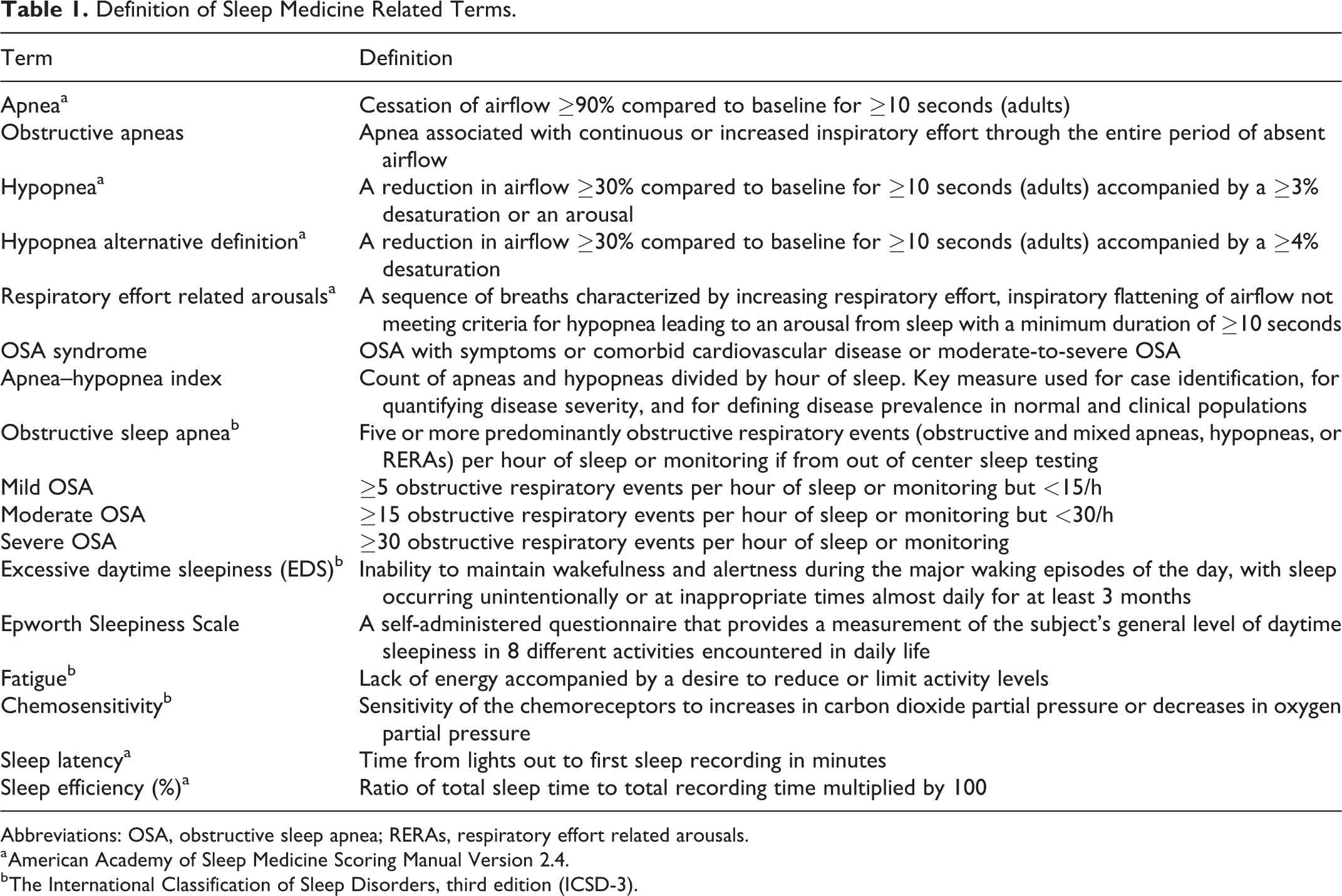
Abbreviations: OSA, obstructive sleep apnea; RERAs, respiratory effort related arousals.
a American Academy of Sleep Medicine Scoring Manual Version 2.4.
b The International Classification of Sleep Disorders, third edition (ICSD-3).
In 1980s, the initial OSA prevalence in middle-aged adults was calculated at 0.3% to 1% 3 using screening questions derived from clinical studies that included, almost exclusively, males. 4 –6 Later on, larger community-based studies confirmed a higher OSA prevalence. In 1993, the prevalence of OSA in women, defined by an apnea–hypopnea index (AHI) greater than 5 per hour, was estimated at 9% from data from the Wisconsin Sleep Cohort Study. 7 Interestingly, there were marked differences in disease prevalence in the clinical setting (8:1 male to female ratio) compared to what was expected from epidemiological studies (2:1 male to female ratio), signaling OSA underrecognition in women. 8 –10 In 1997, 93% of women with moderate-to-severe OSA were thought to remain undiagnosed when comparing positive screening questionnaires against known diagnosis of OSA. 11 Prevalence estimates continue to rise, in the more recent HypnoLaus study, a population-based study conducted between 2009 and 2013 that included polysomnographic data from 2121 patients, the prevalence of moderate-to-severe OSA in women was 23.4%. 12
The increasing prevalence of OSA affects both sexes, partially due to the better recognition of and more screening for the disease, increases in the prevalence of obesity and changes in definition of sleep-related respiratory events such as hypopneas. 9 A recent study estimated that using the American Academy of Sleep Medicine 2012 definition of hypopneas increases the number of women in whom treatment is required by 15%, 13 the impact of which is still not well known.
It’s been 20 years since Dr Young’s landmark paper, male to female ratios have decreased in clinical studies to 5:1 compared to earlier clinical series, 10 and although more women with OSA get diagnosed correctly than in 1997, underrecognition continues to be a major concern. Subsequently, we expand on the topic, explore the potential causes for this aspect of health-care inequity, and propose solutions.
Why Are We Neglecting Women With OSA?
Differences in Symptomatology
Since OSA was first described in middle-aged men, its semiology in this group has become the accepted “textbook” picture of the illness.
Are women with complaints of insomnia, depression, headaches, or fatigue being referred for OSA diagnosis and treatment? Likely not, even in the presence of multiple comorbidities, such as hypertension, cognitive dysfunction, and insulin resistance. Women with OSA may report snoring and excessive daytime sleepiness (EDS) when asked directly but complain more of unrested sleep, insomnia, headache, anxiety, depression, restless legs, nightmares, palpitations, or fatigue. 14,15 Excessive daytime sleepiness itself presents differently in women, with women scoring lower on the subjective Epworth Sleepiness Scale (ESS), a self-administered questionnaire that provides a measurement of daytime sleepiness during common day-to-day activities. 16 In the Sleep Heart Health study, women were 38% less likely to have an abnormal ESS when compared to men, despite similar odds ratio (OR) to reporting daytime sleepiness. 14 When assessing the prevalence of OSA on Swedish women, EDS defined by an ESS score >10 was reported in only 34% of women with OSA. The authors concluded that OSA in women was related to age, obesity, hypertension, witnessed apneas, and snoring but not daytime sleepiness (defined by the ESS); of note habitual snoring occurred in only 7.6% of the sample. 17
Gender Bias
These differences in symptom presentation, common use of the ESS to evaluate subjective sleepiness in the clinical setting, and historical male predominance likely play a role in reduced suspicion for OSA among providers and result in lower referrals for OSA workup. 15,18 Not only do women present with more “atypical” symptoms and may be embarrassed to endorse snoring, but their bed partners are also less likely to report snoring and witnessed apneas. 10 Interestingly, a recent community-based study demonstrated that women, even when presenting with typical symptoms like loud snoring and EDS, were significantly less likely to be diagnosed (25% in men vs 14% in women) and treated (17% vs 11%), despite equal risks of developing hypertension and diabetes. 19
Pathophysiological Factors
A number of factors are thought to lead to differences in OSA presentation including smaller upper airways that are less prone to collapse, 20 less tongue, and neck fat accumulation. 21 Women with obesity and OSA may have greater hypercapnic and hypoxic responses that allow them to maintain minute ventilation at higher chest wall loads and differences in the arousal response to apneas. 22,23 These differences are likely related to the effect of sex hormones. Progesterone has been associated with increased ventilation, 24 increased hypoxic and hypercapnic responses, 25 and lower upper airway resistance. 26 Estrogen may have a role in ventilatory control as well, estrogen monotherapy in pilot studies of postmenopausal women have resulted in lower AHI indexes, 27 and the effect may be synergistic with progesterone. 28 Testosterone supplementation in men may increase the risk of OSA, 29 and OSA has been linked to polycystic ovary syndrome, a condition characterized by increased levels of endogenous testosterone. 30
Studies have shown women have higher minute ventilation at rest compared to men 31 and cyclic fluctuations in ventilation with menstrual cycle that stop with menopause. 32 In women, there is a rapid decline in estrogen and progesterone at menopause, while testosterone decreases gradually. 33 Studies in rodents also suggest that the effect of hormones may change with aging, perhaps related to changes in receptor and signaling molecules downstream in the aging neuron, and sex hormones can modulate breathing directly by binding to receptors or indirectly via changes in gene expression. 34
Sex hormones implication in the pathogenesis of OSA is supported by the fact that OSA is higher in postmenopausal compared to premenopausal women and postmenopausal women on hormone replacement therapy. Perhaps high progesterone and estrogen and low testosterone protect premenopausal women from developing OSA to a certain degree.
These differences in pathophysiology reflect on gender-specific polysomnographic and clinical findings. A clinical study of 2827 patients found women have greater clustering of apneas and hypopneas during Rapid Eye Movement (REM) sleep (43.2 vs 38.5 REM AHI), longer latency to sleep (21.2 vs 16.1 minutes), and lower sleep efficiency (81.6% vs 83.1%) than men. 35 Postmenopausal women have significantly higher OSA severity indices such as AHI and oxyhemoglobin desaturation index than premenopausal women at same levels of obesity and the difference in AHI and the prevalence of OSA between women and men decreases with age, 35 all of which further supports an important role of sex hormones in the pathophysiology of OSA.
Impact on Health
There are gender and sex differences in the way comorbidities present as well. Analysis of a health claim database of over 1.5 million working adults and retirees showed that comorbidities were higher in patients with OSA compared to matched controls, with hypertension and depression being more prevalent in women with OSA. 36 A study of 289 women found that women with OSA have higher risk of diabetes mellitus (OR: 1.6 [confidence interval, CI: 1.01-2.6]), hypothyroidism (OR: 1.6 [CI: 0.95-2.6]), asthma (OR: 2.1 [CI: 1.1-4]), cardiovascular disease (OR: 1.4 [CI: 1.02-2.04]), hyperlipidemia (OR: 1.5 [CI: 1.1-2.1]), arthropathy (OR: 1.6 [CI: 1.1-2.3]), and reflux/esophagitis/gastritis (OR: 2.5 [CI: 1.02-6.1]). 37 Others have also confirmed higher prevalence of cardiac disease, diabetes mellitus, hypothyroidism, and asthma in women compared to men with OSA, despite milder disease severity. 35 Regardless of hypopnea definition (reduction in airflow with 3% oxyhemoglobin desaturation, 3% with an arousal or with 4% oxygen desaturation), an AHI ≥30 events/h was associated with cardiovascular mortality in women (OR between 3.44 and 5.19) even after adjusting for age, sex, body mass index, arterial hypertension, diabetes mellitus, and previous cardiovascular events. 13 Other studies have reported 2- to 3-fold increased risk of first stroke or coronary heart disease in untreated women with OSA compared to women without OSA. 38
Adequate use of continuous positive airway pressure (CPAP) therapy, a machine that pumps air via face mask into the airway keeping it open, 39 was independently associated with mortality risk reduction in women with OSA (hazard ratio: 0.72 [CI: 0.63-0.83]). 13,40 Treatment with CPAP has also shown to improve quality of life (QOL) and decrease anxiety and depressive symptoms and EDS when compared to conservative treatment (sleep hygiene and weight loss counseling) in peri- and postmenopausal women with moderate-to-severe OSA. Daytime alertness improved in this group even when EDS (as defined by an ESS of 10 or higher) was not the presenting complaint. 41
Treatment Differences
Adequate treatment with CPAP, the main treatment for OSA and first line for moderate-to-severe disease, 42 is however challenging with more than 50% of patients discontinuing or using less than the recommended 4 hours per night. 43 There is also no consensus on the definition of compliance, some studies showing improvement in sleepiness and cognition with more than 4 hours of use per night and other studies showing greater benefit with greater use (6 hours or more). 44 In women, a minimum of 4 hours per night is likely to be insufficient to treat REM-related obstructive sleep apneas and hypopneas and, therefore, insufficient to improve health and functional outcomes.
Adherence has been defined differently in different studies; limited data in women suggests it is lower but results have been contradictory. 45 In one study, women were 1.72 times more likely to be nonadherent to CPAP therapy compared to men, even after adjusting to race, marital status, and age; in another study women showed less hours of use. 46,47 Fourteen months of data from the sleep center in Helsinki University Hospital showed that women were 1.2 times more likely to switch masks than men even after initial individualized mask fitting and that patients who switched masks had 7 times higher risk for stopping CPAP therapy within 1 year. 39 Other factors such as being married or living with a partner, greater perceived social support, and higher relationship quality (less conflict) have been predictive of higher adherence in women. 45
Treatment options have been traditionally developed and tested in men including interfaces and auto-titrating CPAP machine algorithms. New algorithms with longer ramps, aiming at being more responsive to flow limitation and better at treating REM events have been recently developed. 48 Masks have also been designed and marketed for women; however, there are no large, well-designed clinical trials evaluating effect of gear, designed specifically for women, on compliance. There are also limited data on treatment outcomes for mild OSA and non-CPAP therapy specifically in women. 23
Conclusion
In summary, some women with OSA have different symptomatology, underreport snoring, or present with EDS is not often captured on standardized sleepiness questionnaires. Those, however, who present with typical male-associated symptoms of EDS and snoring are less likely to be evaluated and treated for OSA. Underdiagnosis of OSA in women may be more pronounced in the milder OSA range, and at the same time women are more symptomatic at lower AHIs, 49 potentially leaving a significant proportion untreated and consequently with lower QOL, well-being, and health status. 41 Obstructive sleep apnea has historically been regarded as a male disease, 17 women have been notoriously underrepresented in clinical studies, 23 with about only 20% female representation in cohort from sleep clinics, 19 and premenopausal and postmenopausal women are not generally studied separately. 35
It has become clear that for variety of reasons, primarily significant gender bias, women with OSA still remain underdiagnosed. Early diagnosis and management of OSA in women is critical. Increased awareness of atypical symptoms, low threshold to test middle-aged women with obesity, and development of female-specific questionnaires may also help identify women at risk. 35 Obstructive sleep apnea is truly a common disorder in women with estimated prevalence between 6% and 23% for moderate-to-severe disease. 41 Differences in prevalence, age of presentation and reproductive status, symptoms, severity, impacts on QOL, and health status should be taken into account when evaluating women, taking in consideration that women with OSA tend to be older, heavier, and have a higher rate of medical comorbidities and symptom burden.
The Knowledge Gap
Research is needed to clarify the role of sex hormones in the pathophysiology and treatment of OSA. Future studies should focus on the phenotyping of OSA in women, evaluation of newly developed gender-specific CPAP algorithms, and interfaces. This knowledge will help develop gender-specific tools, increase disease recognition, and development of personalized treatment approaches that lead to more effective treatment. Higher representation of women in clinical trials will allow assessing the impact of treatment of the entire OSA severity spectrum in women, under the new hypopnea definitions, on the incidence of comorbidities and implications on public health.
Gender and sex differences are prevalent in the pathophysiology and therapeutics of most illnesses, but this element is often ignored in health care. As we move toward a more personalized medicine, gender and sex differences in general, and in the diagnosis and treatment of OSA in particular, need to be better understood. As it seems, we are still underdiagnosing women with OSA, and this is resulting in possible devastating health consequences and societal costs. 50
Solutions
We propose the following solutions. (1) Primary care providers and others at the forefront of health care need to keep an open mind when screening women with sleep complaints. (2) There needs to be increased education about OSA and its presentation and impact on women. (3) Perhaps the “classic” definitions for OSA need be revised. (4) It may be helpful to develop easy-to-use screening tools for both the health-care community and the lay public to raise awareness of the variety of symptomatology of OSA in women and help in early presentation and diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.