
Abstract
The therapeutic landscape of clear cell renal cell carcinoma (ccRCC) has dramatically evolved in the last decade. Immuno-oncology (IO) and/or tyrosine kinase inhibitor (TKI) based doublet therapies have become standard in the frontline setting for most patients with advanced ccRCC. For previously-treated advanced ccRCC, multiple agents are available including belzutifan, a hypoxia inducible factor 2 alpha (HIF2-α) inhibitor. However, the challenging goal of developing therapies with a unique mechanism of action remains. Many such promising agents are currently in development such as novel TKIs, inhibitors targeting alternative checkpoints, cellular therapies, radioligands, antibody-drug conjugates, and agents targeting fatty acid metabolism. Further, the role of microbiome is being actively investigated in advanced ccRCC, with ongoing studies evaluating its effect when combined with standard therapies. Mature data from trials with these agents is eagerly awaited.
Keywords
Introduction
The therapeutic landscape of clear cell renal cell carcinoma (ccRCC) has dramatically evolved in the past decade. For most patients with previously-untreated advanced ccRCC, the new standard-of-care has become doublet therapy, with a backbone of either two immuno-oncology (IO) agents or a combination of one IO agent and one vascular endothelial growth factor (VEGF) targeting tyrosine kinase inhibitor (TKI) agent. Phase 3 randomized, controlled trials such as CheckMate-214 (with ipilimumab/nivolumab), 1 KEYNOTE-426 (with pembrolizumab/axitinib), 2 JAVELIN Renal 100 (with avelumab/axitinib), 3 CheckMate-9ER (with nivolumab/cabozantinib), 4 and KEYNOTE-581 (with pembrolizumab/lenvatinib) 5 demonstrated the superiority of these doublet regimens over the historic standard of single-agent sutinitib, leading to multiple regulatory approvals in the frontline setting. The choice of first-line therapy should be individualized and depends on multiple factors, including patient characteristics, the timeframe within which treatment response is needed, drug regimen safety profiles, financial toxicity considerations, and physician preferences.
Selection of second-line therapy and beyond for advanced ccRCC depends on which front-line treatment regimen was used as well as other considerations, including disease activity status and the overall condition of the patient. No particular subsequent drug regimen is preferred and current guidelines list multiple options in this setting, based on whether the patient is IO-naive. These include an alternative TKI (alone or in combination), IO (if it has not yet been used in the frontline setting), or a mammalian target of rapamycin (mTOR) inhibitor (alone or in combination). 6 Other agents such as belzutifan, bevacizumab, and high-dose interleukin-2 (IL-2) are useful in certain circumstances. 6 Real world data regarding treatment patterns of advanced ccRCC patients with disease progression or intolerance of first-line systemic therapy suggests a significant drop off in percentage of patients who go on to receive second- and third-line therapy.7,8 As such, it is imperative to select frontline and subsequent therapies in a strategic manner. Awareness of novel therapies for advanced ccRCC can greatly optimize therapy selection and will be the focus of this review, which aims to highlight emerging classes of agents.
Hypoxia-inducible factor 2 alpha (HIF2-α) inhibitors
Bi-allelic inactivation of the von Hippel Lindau (VHL) tumor suppressor gene is an early genetic event that arises in the majority of ccRCC cases. 9 Subsequent mutations or chromosomal copy number alterations in epigenetic regulatory genes (including PBRM1, BAP1, SETD2, and KDM5C), cell-cycle regulatory genes (including TP53, CDKN2A, and MYC), or PI3K pathway genes (including PIK3CA, PTEN, MTOR, and TSC1) arise recurrently in ccRCC and are believed to cooperate with VHL inactivation to promote the development and evolution of ccRCC tumors.10,11 The VHL protein acts as an E3 ubiquitin ligase and leads to ubiquitination of the alpha subunit of hypoxia-inducible factor (HIF) in an oxygen-dependent fashion, which results in proteolysis of HIF. 12 Pathogenic VHL variants reduce VHL protein activity, resulting in stabilization of HIF subunits and subsequent constitutive activation of HIF-mediated transcriptional pathways, independent of oxygen concentrations. 13 HIF-mediated transcription facilitates gene expression of vascular endothelial growth factor (VEGF), cyclin D1, glucose transporter 1, and erythropoietin. 13 These factors normally function to counteract the effects of hypoxia by promoting vascularization, enhancing glucose utilization, and increasing red-cell production through transcriptional signals. 12
Belzutifan is a first-in-class, potent, selective, oral small-molecule HIF-2α inhibitor with anti-tumor activity in ccRCC. 12 Selected clinical trial data with this agent is summarized in Table 1. Belzutifan has received its first regulatory approval in 8/2021 for patients who require systemic therapy for tumors associated with VHL disease, including ccRCC. VHL disease is an autosomal dominant hereditary disorder that is caused by germline pathogenic variants in the VHL gene and is associated with benign and malignant neoplasms such as ccRCC, pancreatic neuroendocrine tumors and hemangioblastomas. 12 This approval was based on results of the LITESPARK-004 trial, which is a phase 2, single-arm study of belzutifan monotherapy in patients with VHL disease associated RCC and other tumors. 12 At 21.8 months of follow up, the objective response rate (ORR) was 49% and an additional 49% had stable disease (SD). Median time to response was 8 months, median duration of response (DoR) was not reached, and 56% of responders had durable responses of ≥12 months. Grade 3 treatment-related adverse events (TRAEs) were noted in 15% of patients, with no grade 4 or 5 TRAEs observed. Only 2% of patients discontinued treatment due to a TRAE. Most common adverse events were anemia (90%), fatigue (66%), headache (41%), and dizziness (39%). A total of 7% of patients received blood transfusions due to anemia, 20% received erythropoietin-stimulating agents, while 2% had grade 3 transient hypoxia that resolved with dose interruption and dose reduction of belzutifan. With longer follow up of 29.3 months, ORR in ccRCC was 59%, with 3% complete responses (CR) and 56% partial responses (PR), while median DoR was still not reached. 14 No extra safety events were identified and the most common grade 3 TRAE was anemia (10%). Belzutifan was discontinued in 3% of patients due to a TRAE including dizziness (grade 1) and intracranial hemorrhage (grade 2).
Selected clinical trials with belzutifan.
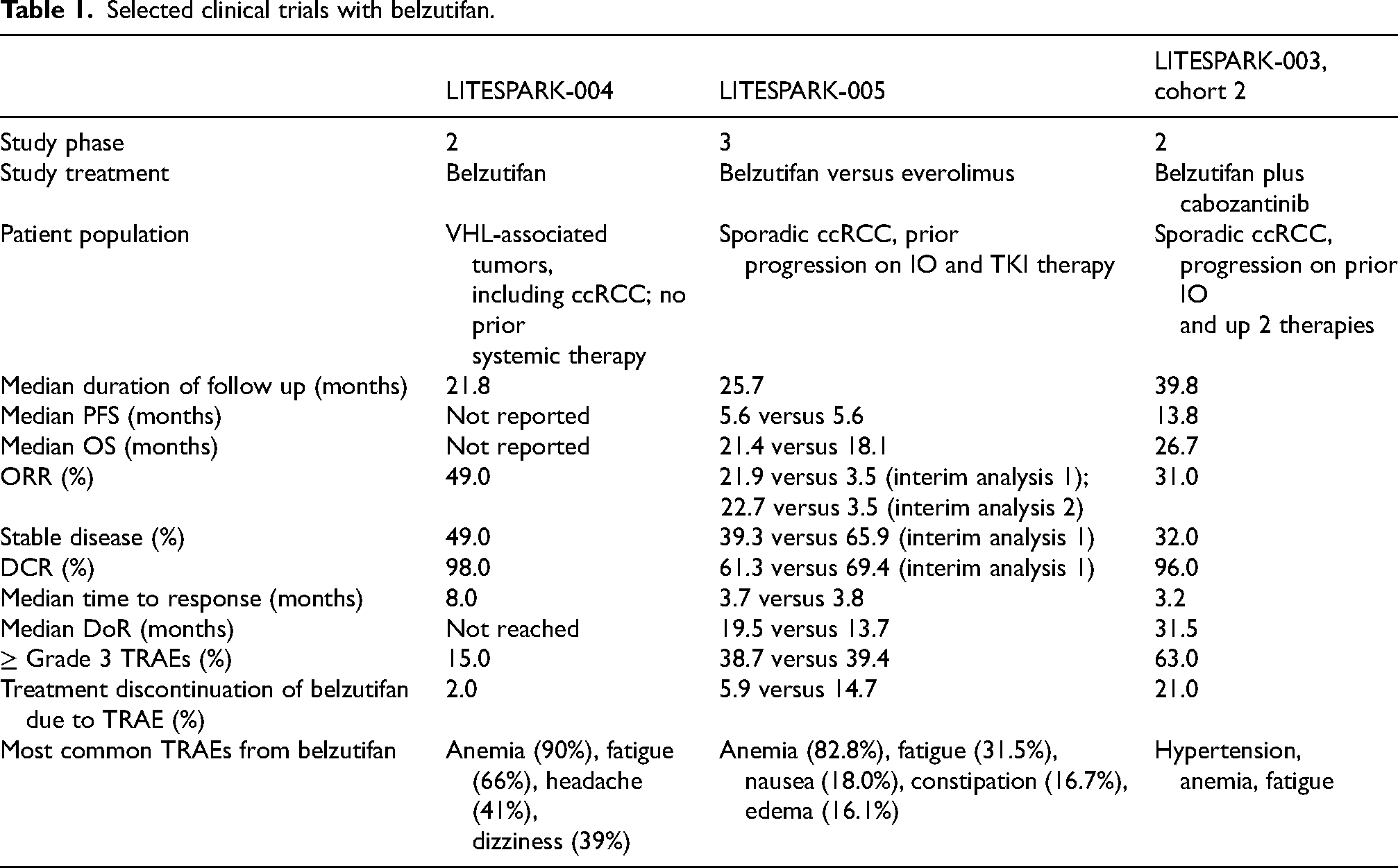
Single-agent belzutifan was subsequently evaluated in patients with sporadic ccRCC in the LITESPARK-005 trial, 15 which was a phase 3 randomized study of belzutifan versus everolimus in patients with advanced ccRCC following progression on prior IO and TKI therapy. More patients remained progression-free with belzutifan compared to everolimus at 12 months (progression free survival (PFS) rate of 33.7% versus 17.6%) and at 18 months (PFS of 22.5% versus 9.0%). With median follow up of 25.7 months, median PFS was 5.6 months versus 5.6 months [HR, 0.74], median overall survival (OS) was 21.4 months versus 18.1 months [HR, 0.88, p = 0.09941], and ORR was 22.7% versus 3.5% with belzutifan and everolimus, respectively. Grade 3 or higher TRAEs occurred in 38.7% of patients on belzutifan and 39.4% of patients on everolimus, while 5.9% versus 14.7% of patients have discontinued therapy due to a TRAE. Based on results of this study, belzutifan received regulatory approval in 12/2023 for patients with advanced pre-treated sporadic ccRCC.
Belzutifan is also being evaluated in combination with other agents, including TKIs. Since HIF-2α activation may be a resistance pathway for anti-VEGF therapy, it is hypothesized that combining belzutifan with a TKI may lead to repression of HIF-2α-regulated VEGF production at the level of transcription by belzutifan as well as inhibition of VEGF production downstream of HIF-1α by TKI at the growth factor level. 16 LITESPARK-003 (NCT03634540) is phase 2, single-arm study evaluating the combination of belzutifan with cabozantinib in two separate patient cohorts - cohort 1 contained treatment-naive metastatic ccRCC patients and cohort 2 contained patients with progression on IO and up to 2 systemic treatment regimens. 17 Data from cohort 2 has been published. At median follow up of 24.6 months, ORR was 30.8%, including 2% with CR and 29% with PR, with an additional 65% who had SD. As such, disease control rate (DCR), defined as CR + PR + SD, was 92.3%. Median PFS was 13.8 months, median DoR was 18.6 months, and median time to response was 3.2 months. Serious TRAEs occurred in 29% of patients, most commonly hypertension (27%), anemia and fatigue. No grade 4 TRAEs and one grade 5 event of respiratory failure was noted. Adverse events (AEs) leading to treatment discontinuation of belzutifan were observed in 19% of patients and cabozantinib in 21% of patientsand is listed in (Table 1). now from cohort with median follow up of 39.8 months is also available
Meanwhile, KEYMAKER-U03B (NCT04626518) is a phase 1/2, multi-arm, umbrella study, with available preliminary results from Arm B5, 18 where patients with metastatic ccRCC following progression on prior IO and TKI therapy received a combination of belzutifan and lenvatinib. Among 24 patients with ≥2 post baseline scans, ORR was 50%, with all PRs, and clinical benefit rate (CBR; CR + PR + SD ≥6 months) was 54%. median PFS was 11.2 months and 74% of responders remained in response for ≥12 months. Grade 3 or 4 TRAEs occurred in 50% of patients, most commonly hypertension (27%) and anemia (17%). LITESPARK-011 (NCT04586231) is an ongoing phase 3 study combining belzutifan and lenvatinib versus cabozantinib in patients with advanced ccRCC after progression on IO therapy, 19 which completed accrual and results are being eagerly awaited. Belzutifan is also currently being evaluated in the frontline setting in combination with other agents. For instance, LITESPARK-012 (NCT04736706) is a phase 3 study of first-line therapy with belzutifan plus lenvatinib and pembrolizumab versus lenvatinib plus pembrolizumab and quavonlimab (anti-CTLA-4) versus lenvatinib plus pembrolizumab in patients with advanced ccRCC that has also completed accrual, although no results are yet available. 20
Other HIF2-α inhibitors are also in development. For instance, early data from 40 patients with pre-treated metastatic ccRCC enrolled on a phase 1 study with DFF332 (NCT04895748), which is small-molecule HIF-2α inhibitor, demonstrated an SD rate of 45%, PR of 5%, and DCR of 50%. 21 TRAEs were reported in 60% of patients, with most common being anemia (13%), increased cholesterol (13%), fatigue (13%), and hypertriglyceridemia (10%). Grade 3 TRAEs were increased weight (2.5%) and hypertension (2.5%), while no grade 4 TRAEs or dose-limiting toxicities were noted. Importantly, none of the patients reported hypoxia. Other agents directly targeting HIF2-α or other mechanisms around this molecule are under investigation. 22
IO-based therapies
Several IO agents targeting PD-1/PD-L1 and CTLA-4 have previously received regulatory approval in ccRCC. There is significant interest in exploring “alternative checkpoints”, which are other targets such as LAG3, TIGIT, and TIM-3 along the immune-stimulatory pathway, as outlined in Figure 1. It is hypothesized that adding novel inhibitors targeting alternative checkpoints to existing IO and TKI therapies may lead to more robust immune stimulation and potentially more durable clinical treatment responses. A preclinical model demonstrated that RCC tumors can be immunohistologically divided into three cohorts based on dominant expression of one of these molecules. 23 LAG3, TIGIT, and TIM-3 were subsequently examined in a study evaluating their expression in primary versus metastatic ccRCC tumor samples. 24 In both primary and metastatic tumors, LAG3 subtype was associated with a worse prognosis and a more immunosuppressive tumor microenvironment compared to TIGIT and TIM-3, as defined by higher infiltration with exhausted T-cells and tumor associated macrophages. Meanwhile, another study found that LAG3 protein levels are on average lower at metastatic sites compared to matched primary tumors and that the difference was more pronounced in patients with high-risk clinical characteristics, including those with a larger primary tumor size, WHO grade 4 tumors, IMDC poor-risk disease, and initial presentation with brain metastasis. 25 Further, relatively higher LAG3 levels at metastatic sites may predict for improved response to immunotherapy and longer OS after development of metastatic disease.

Alternative checkpoints along the immune-oncology pathway.
Following the regulatory approval of relatlimab, which is a first-in class LAG3 inhibitor, 26 for metastatic melanoma based on results of the RELATIVITY-047 study, this agent as well as other LAG3 and alternative immune checkpoint inhibitors are being actively studied in advanced ccRCC.25,27 For instance, early data on 30 patients with pre-treated advanced ccRCC from a phase 1 study of fianlimab (anti-LAG3) with cemiplimab (anti-PD-L1) (NCT03005782) demonstrated DCR of 60% and 73% in dose-escalation cohorts 3 and 4 of this trial, with median treatment duration of 27 weeks and 18 weeks, respectively. 28 Grade ≥3 TRAEs occurred in 53% and 33% of patients in cohorts 3 and 4, respectively. The most common TRAEs of any grade were rash (27%) and infusion-related reaction (27%) in cohort 3 as well as fatigue (20%) in cohort 4. Meanwhile, an ongoing randomized phase 2 study of immune checkpoint inhibitor combinations (NCT05805501) adds alternative checkpoint inhibitors to the backbone of standard therapy with pembrolizumab and axitinib in previously untreated metastatic ccRCC patients. In this study, which is currently open to enrollment, patients are randomized to receive pembrolizumab with axitinib versus tobemstomig (a bispecific antibody to LAG3 and PD-1) with axitinib versus tiragolumab (anti-TIGIT) with tobemstomig and axitinib. Another phase 1b/2 multi-arm umbrella study of investigational immune and targeted combination therapies (NCT04626518) for patients with advanced ccRCC is ongoing and has several arms evaluating MK-4280A, a co-formulation of favezelimab (anti-LAG3) and pembrolizumab (anti-PD-1). 29
Other agents with immune stimulatory mechanisms of action are also being investigated. Historically, high-dose IL-2 has been used in management of metastatic ccRCC, with durable treatment responses,30,31 although it has fallen out of favor due to its significant toxicity profile. Attempts to develop agents within the IL-2 pathway, but with fewer associated TRAEs, are underway. Bempegaldesleukin (BEMPEG) is a pegylated IL-2 cytokine prodrug engineered to provide controlled and sustained activation of the IL-2 pathway, with the goal of preferentially activating and expanding effector CD8+ T-cells and natural killer cells over immunosuppressive regulator T-cells in the tumor microenvironment. 32 PIVOT-02 (NCT03729245) is a single-arm phase 1/2 multi-cohort study with BEMPEG plus nivolumab. 32 Analysis of the previously-untreated metastatic RCC cohort of 49 patients with median follow up of 32.7 months showed an ORR of 34.7%, with CR of 6.1%, while 35.3% of patients remaining in response for >24 months. Median PFS was 7.7 months and median OS was not reached. Grade 3 and 4 TRAEs were noted in 38.8% of patients, most commonly syncope (8.2%) and increased lipase (6.1%). Meanwhile, PIVOT-09 (NCT03729245) is a phase 3 study, which randomized 623 previously-untreated metastatic RCC patients to receive BEMPEG plus nivolumab versus investigator's choice of TKI (i.e., sunitinib or cabozantinib). 33 This was a negative trial as it failed to meet its primary endpoints. In patients with International Metastatic RCC Database Consortium (IMDC) intermediate- and poor-risk disease, ORR with BEMPEG plus nivolumab versus TKI was 23.0% versus 30.6% (p = 0.0489), while median OS was 29.0 months versus not estimable (HR, 0.82 [95% CI, 0.61 to 1.10]; p = 0.192), respectively. Grade 3/4 TRAEs were less frequent with BEMPEG plus nivolumab (25.8%) versus TKI (56.5%).
Meanwhile, chimeric antigen receptor (CAR) T-cell therapy has received regulatory approval in multiple hematologic malignancies and is actively being studied in solid tumors. CARs are engineered fusion proteins designed to target T-cells to antigens expressed on cancer cells. 34 In 6/2023, IVS-3001 was granted a fast-track designation to expedite its development as a potential therapeutic option in patients with RCC based on preclinical data. IVS-3001 is a CAR-T cell immunotherapy that targets an immune checkpoint called human leukocyte antigen-G (HLA-G). The latter is a non-classical HLA-class I molecule, which is exclusively expressed on the surface of preimplantation embryos and extravillous trophoblasts in the placenta at the maternal-fetal interface. 35 HLA-G aides in creating an immunosuppressive environment, thereby establishing maternal immunological tolerance towards the fetus. Multiple tumors, including ccRCC, demonstrate increased HLA-G expression as one of the ways in which tumor cells avoid immune cell detection,36,37 which makes this an attractive candidate target for cellular therapy. IVS-3001 is currently being evaluated in a phase 1/2 study (NCT05672459) in patients with previously-treated locally advanced solid tumors that express HLA-G, including RCC. Meanwhile, Clustered Regularly Interspaced Short Palindromic Repeats (CRISPR) - Cas9 technology allows for targeted gene editing and is also being evaluated in early phase solid tumor trials. For instance, COBALT-RCC (NCT04438083) is a phase 1 study evaluating CTX130, which is a CD70-targeting allogeneic CRISPR-Cas9–engineered CAR T-cell therapy, in patients with pre-treated metastatic ccRCC. 38 Early data from 14 patients in this study demonstrated a 76.9% DCR, with 7.7% of patients experiencing a durable CR maintained at 18 months. A similar phase 1/2 study of CTX131 (NCT05795595), an allogeneic CD70-directed CAR-T cell immunotherapy genetically modified using CRISPR-Cas9 gene editing technology, in patients with advanced solid tumors including RCC is ongoing.
Novel TKIs
Several novel TKIs are also being developed, with a goal of improved toxicity and additional efficacy within this drug class. One example is zanzalintinib, which is a novel, potent, oral, small molecule TKI that inhibits several receptor tyrosine kinases including VEGFR2, MET, and TAM kinases (i.e., AXL and MER). 39 MET and AXL are known to play important roles in the development of resistance to anti-angiogenic therapies. Further, drugs targeting TAM kinases are thought to promote an immune-permissive environment, potentially enhancing responses to IO agents. 39 In a phase 1 study (NCT03845166), zanzalintinib alone or in combination with atezolizumab showed a manageable safety profile and promising clinical activity in patients with advanced or metastatic solid tumors, including ccRCC. 40 STELLAR-002 (NCT05176483) is an ongoing phase 1b study of zanzalitinib in combination with checkpoint inhibitor combinations in patients with advanced solid tumors, including ccRCC. 41 Sitravatinib is another multi-target TKI against TYRO3, AXL, VEGFR2 and TAM kinases. 42 A phase 2 trial (NCT04904302) of sitravatinib plus nivolumab in patients with metastatic ccRCC post progression on IO therapy demonstrated only a modest clinical benefit, with ORR of 15.4% and DCR of 35.7% at 24 weeks follow up. 43 Median PFS was 5.5 months and median OS was 13.3 months. Grade 3 or 4 TRAEs were noted in 42.9% of patients. Enrollment on this study was terminated early.
Meanwhile, batiraxcept is a soluble fusion protein comprised of the extracellular domain of the receptor tyrosine kinase (RTK) AXL fused to a human immunoglobulin G1 (IgG1) Fc domain, with potential anti-neoplastic activity. 44 Batiraxcept selectively binds to growth arrest-specific protein 6 (GAS6), the endogenous ligand for AXL. This may inhibit GAS6/AXL-mediated signaling, which plays a key role in tumor cell proliferation, survival, invasion and metastasis as well as immune evasion and resistance to other anticancer agents. Batiraxcept is a first-in class agent that was evaluated in a phase 2 study (NCT04300140) as monotherapy, in combination with cabozantinib, and in combination with cabozantinib and nivolumab in patients with advanced ccRCC. 44 In this study, ORR was 0%, 36%, and 55% across the three study arms, while CBR was 10%, 72%, and 64%, respectively. Meanwhile, median PFS was 1.8 months, 7.2 months, and 7.6 months, respectively. Grade 3 or higher TRAEs were noted in 10%, 28%, and 46% of patients, respectively. Most common batiraxcept-related AEs of all grades included diarrhea (28%), fatigue (28%), increased alkaline phosphatase (20%), and infusion-related reaction (20%). Batiraxcept therapy was discontinued in 12% of patients due to TRAEs.
Radioligand therapies
Similar to the regulatory approval of 177-Lutetium-PSMA therapy in prostate cancer, targeted radioligand therapies are also being investigated in advanced ccRCC. One example is Girentuximab, which is a monoclonal antibody that targets carbonic anhydrase IX (CAIX) and can be radiolabeled to various DNA damaging molecules. CAIX is a cell-surface transmembrane metalloenzyme involved in acid-base balance and a tumor-associated antigen that is overexpressed in VHL-mutated ccRCC and other hypoxic tumors, but is not significantly expressed in normal kidney tissue. 45 Loss of VHL leads to increased CAIX expression. Due to its unique expression in ccRCC, CAIX has potential as both a diagnostic and therapeutic target. The ZIRCON study (NCT03849118) is a phase 3 study that evaluated girentuximab radiolabeled to 89-Zirconium (89-Zr-DFO-girentuximab or TLX250-CDx) PET/CT imaging for non-invasive detection of ccRCC in patients with indeterminate renal masses up to 7 cm in size (cT1) scheduled for nephrectomy. 46 Enrolled patients received a single dose of TLX250-CDx on Day 0 and underwent PET/CT imaging on Day 5 (± 2 days) prior to surgery. Of 288 patients with central histopathology of surgical samples, only 193 (67%) had ccRCC and 179 (62%) had cT1a. Of 284 evaluable patients, the average sensitivity and specificity was 86% and 87% respectively for co-primary as well as 85% and 90% respectively for key secondary endpoints. For all evaluable patients, positive and negative predictive values were ≥91.7% and ≥73.7%. Of 263 AEs in 124 patients, 2 AEs of mild intensity were treatment related. Meanwhile, a small dosimetry study of CAIX targeting peptide, [68Ga]Ga-DPI-4452, which is an imaging agent of a theranostic pair with [177Lu]Lu-DPI-4452, in ccRCC patients with 36 evaluable lesions demonstrated very high tumor-to-background ratios and no significant TRAEs, suggesting potential diagnostic and therapeutic applications. 47 Further, girentuximab radiolabeled to 177-lutetium (177-Lu-girentuximab) is also being evaluated as a therapeutic agent in two investigator-initiated trials. STARLIGHT 2 (NCT05239533) is a phase 2 study examining 177-Lu-girentuximab plus nivolumab in pre-treated metastatic ccRCC patients post progression on prior IO therapy. 48 STARLIGHT 1 (NCT05239533) is a phase 1b/2 study evaluating 177-Lu-girentuximab plus nivolumab and cabozantinib in treatment-naïve patients with advanced ccRCC. 49
Antibody drug conjugates (ADCs)
Several ADCs have received regulatory approval in solid tumors. These molecules consist of a monoclonal antibody designed to bind to a target on a malignant cell, which is conjugated to a potent cytotoxic drug (i.e., payload) through a chemical linker. Multiple ADCs are being evaluated in phase 1 trials in advanced RCC, which appear to be well tolerated, although the efficacy data has not been robust thus far.
50
One explanation is that RCC is generally not a chemotherapy responsive tumor, while ADCs typically have a chemotherapy-like agent as a payload. As an example, AGS-16C3F was studied in a randomized phase 2 study (NCT02639182) against axitinib in patients with pretreated advanced ccRCC.
51
AGS-16C3F is an ADC that targets cell-surface ectonucleotide pyrophosphatase/phosphodiesterase 3 (ENPP3) and is conjugated to a microtubule disruptive agent, mono methyl auristatin F (MMAF). In 84 evaluable patients, median PFS was 2.9 months versus 5.7 months (HR, 1.676; p = 0.015) and OS was 13.1 months versus 15.4 months
Fatty acid metabolism targeting therapy
TPST-1120 is a first-in-class oral antagonist selective for peroxisome proliferator-activated receptor alpha (PPARα). PPARα is a transcription factor that regulates fatty acid oxidation (FAO) and inflammation and is over-expressed in many cancers and in immune cells. A PPARα deficiency in both tumor cells and the host shows reduced angiogenesis and a failure to support tumor growth. 53 TPST-1120 is a competitive antagonist of PPARα that can displace endogenous and synthetic agonists resulting in inhibition of FAO gene expression, a key metabolic adaptation of cancer and immunosuppressive cells. In addition, TPST-1120 may block the ability of PPARα to transrepress NF-kB resulting in reversal of immune suppression. 53 Early data from a phase 1 study of TPST-1120 (NCT03829436) as monotherapy or in combination with nivolumab in patients with advanced solid tumors, including RCC, is available. 54 In 18 patients treated with combination therapy, ORR was 20% across all TPST-1120 doses and 30% at TPST-1120 dose of ≥400 mg twice daily, with 3 patients achieving PR including 2 patients with ccRCC. Most common TRAE were nausea (20%), fatigue (15%), and diarrhea (10%). No grade 4 or 5 TRAEs were reported and no patient discontinued therapy due to a TRAE.
Microbiome
Recent evidence demonstrates that gut microbiota composition may play a role in responses to cancer-directed therapy, particularly immunotherapy, and early data in genitourinary malignancies is available.55,56 The exact mechanism by which the gut microbiome enhances therapeutic responses or contributes to drug resistance is unknown, although factors such as diet including high fiber intake, antibiotic or other medication use, and host genetic makeup seem to play a role. One preclinical study evaluating mice with melanoma showed that presence of Bifidobacterium was associated with improved efficacy of cancer therapeutics, including IO-based therapies. 56 The live bacterial product CBM588 contains Clostridium butyricum, a butyrate-producing anaerobic spore-forming bacterium, which in preclinical studies appeared to be bifidogenic, possibly through expansion of interleukin (IL)-17A-producing γδ T cells and CD4 cells in the colonic lamina propria. 57 One randomized phase 1 study evaluated nivolumab plus ipilimumab with or without live bacterial supplementation with CBM588 (NCT03829111) in metastatic ccRCC. 57 PFS was significantly longer in patients receiving nivolumab and ipilimumab with CBM588 than without (12.7 months versus 2.5 months; HR, 0.15, p = 0.001). Although not statistically significant, ORR was also higher in patients receiving CBM588 (58% versus 20%, p = 0.06). No significant difference in toxicity was observed between the study arms. Another phase 1 trial (NCT05122546) evaluating the use of CBM588 in combination with nivolumab and cabozantinib in patients with metastatic ccRCC is underway.
Conclusions
The recent decade saw a Renaissance of interest in developing novel therapies for advanced ccRCC. A first-in-class HIF2-α inhibitor, belzutifan, has received regulatory approval in VHL-associated as well as sporadic advanced ccRCC, providing a novel therapeutic option for this patient population. Data from combination therapies with belzutifan is eagerly awaited. Meanwhile, agents targeting alternative checkpoints, including LAG3 and TIGIT, as well as cellular therapies are conceptually promising, although scant data is available at this time. Other new-in-class agents, such as radioligands, antibody-drug conjugates, and therapeutics targeting fatty acid metabolism are exciting. The emerging role of microbiome on response and resistance to cancer therapies is also being elucidated. Continued development of agents with distinct mechanisms of action as well as identification and validation of predictive biomarkers remains of paramount importance.
Footnotes
Author contributions
Nataliya Mar, MD - designed the concept, collected data, interpreted data, co-wrote the manuscript, edited the manuscript, finalized the manuscript.
Sami Dwabe, MD - designed the concept, collected data, interpreted data, co-wrote the manuscript, edited the manuscript.
Dalia Kaakour, MD - reviewed and edited the manuscript.
Steven N. Seyedin, MD - reviewed and edited the manuscript.
Arash Rezazadeh, MD - reviewed and edited the manuscript.
Michael Daneshvar, MD - reviewed and edited the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available within the article and/or its supplementary material.