
Abstract
Background:
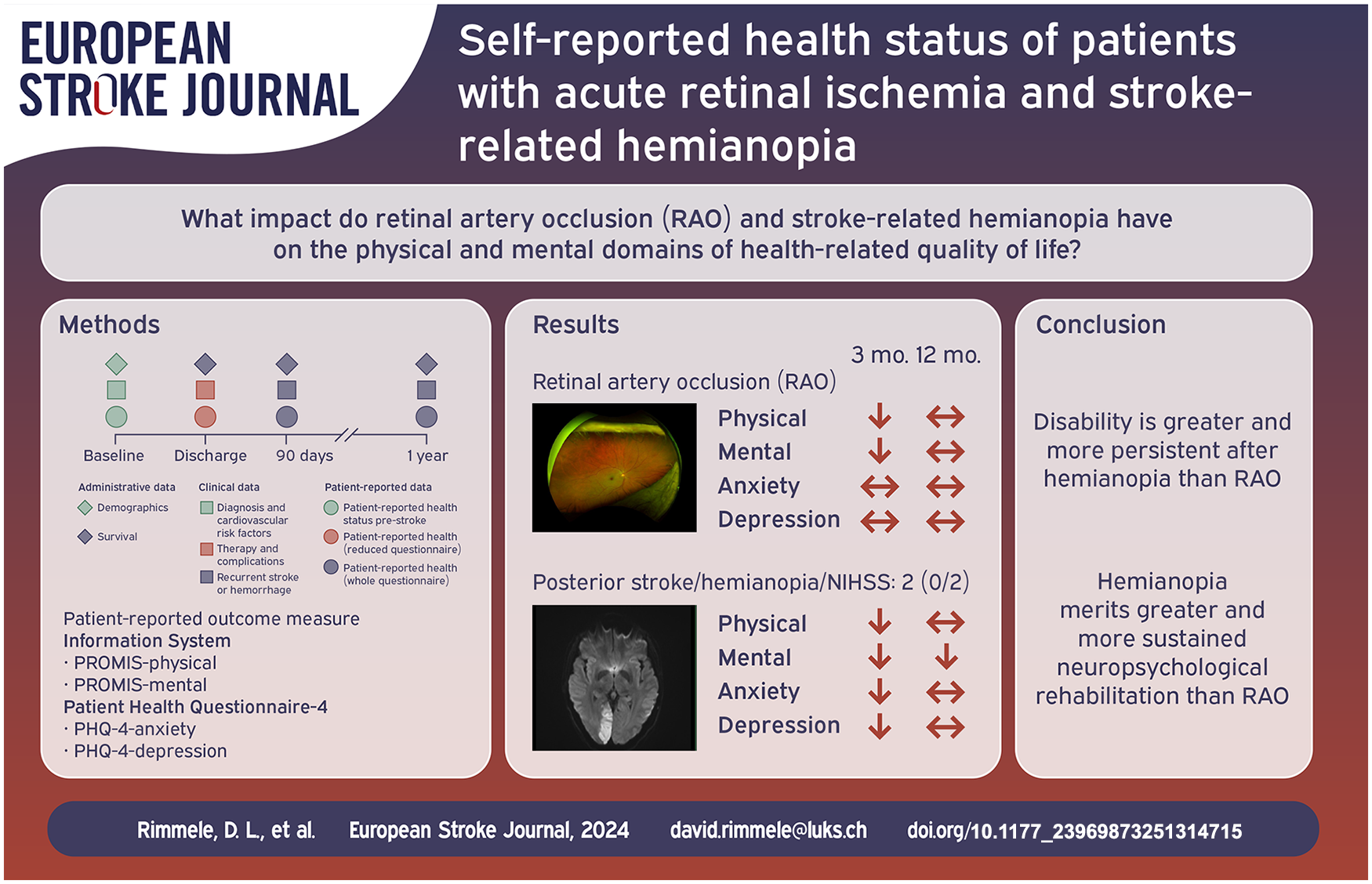
We aimed to assess impairments on health-related quality of life, and mental health resulting from Retinal artery occlusion (RAO) with monocular visual field loss and posterior circulation ischemic stroke (PCIS) with full or partial hemianopia using patient-reported outcome measures (PROMs).
Methods:
In a prospective study, consecutive patients with acute RAO on fundoscopy and PCIS on imaging were recruited during their surveillance on a stroke unit over a period of 15 months. Baseline characteristics were determined from medical records and interviews. Health-related quality of life (PROM Information System 10-Question-Short-Form, PROMIS-10), and mental health symptoms (Patient-Health-Questionnaire-4, PHQ-4) were assessed 3 and 12 months after admission postally and via phone.
Results:
Ffity-seven patients with RAO and 19 with isolated full or partial hemianopia determined by the NIHSS (median = 2; IQR:0/2) according to PCIS were included. Characteristics of cardiovascular risk factors, and functional status pre-stroke were comparable between the groups. At 3 months, mean ± standard deviation T-scores of PROMIS physical and mental health were 47.1 ± 8.8 and 46.7 ± 8.8 for patients with RAO, and 43.4 ± 9.8 and 43.2 ± 6.2 for PCIS. Compared to 50 ± 10 in the general population, scores after RAO (p = 0.04; p = 0.02) and PCIS (p = 0.01; p < 0.001) were lower in both domains after 3 months. Concerning PCIS, scores in the mental health domain remained decreased at 12 months (p = 0.04). On the PHQ-4, 25% of patients with RAO, and 62% with PCIS scored indicative for anxious and/or depressive syndromes at 3 months.
Conclusions:
RAO led only to partial and to less persistent mental impairments than PCIS. This suggests that a different approach involving complex visual and neuropsychological treatment over a longer period of time needs to be considered for post-stroke care of PCIS.
Trial Registration Information:
The trial was submitted at http://www.clinicaltrials.gov, under NCT03795948.
Keywords
Introduction
Stroke has long-lasting detrimental effects on the ability to work and quality of life. 1 Efforts have been made to assess these by patient reported outcome measures (PROMs) additional to traditional medical examinations. 2 Apart from physical and mental deficits, stroke can lead to visual impairments like monocular vision loss or hemianopia. Hemianopia is mainly caused by ischemic lesions of the visual cortex or post-chiasmatic tract in the posterior arteries’ circulation. It is shown to lead to a reduced health-related quality of life by impairments of visual and behavioral functions assessed by PROMs like the National Eye Institute Visual Function Questionnaire (NEI-VFQ) and Symptom-Checklist-90 revised (SCL-90-R).3–5 Monocular impairments are caused by acute retinal artery occlusion (RAO) of central or peripheral branches. Patients with peripheral branch RAO suffer from moderate, and patients with central RAO from profound monocular visual loss with 80% having a visual acuity of 20/400 or worse.6,7 Instead visual acuity remains in most cases unaffected by hemianopia after posterior cerebral ischemic stroke (PCIS) due to the relatively large cortical representation of the macular and a dual arterial supply of this region.8,9 Further differences are the binocular congruous visual field defects caused by occipital lobe lesions after PCIS opposed to monocular central or temporal scotoma after RAO. 10 RAO leads to visual loss through necrosis of retina cells and impairment of the perception itself. While PCIS impairs the construction and consciousness of the perceived visual image by the cortex and its tracks. The damage of cerebral cortex involves functions beyond the loss of direct visual perception. These comprise saccadic eye movements necessary for fluent reading and keeping moving objects in focus and abstract functions, like spatial memory or imagination. The pathophysiology may be an impaired delivery of constructed visual images to different cerebral networks like the frontal ones. Effects of RAO on functional health status and health- related quality of life have not been investigated with PROMs so far. Concerning the impairment of vision, RAO may lead to visual impairments more comparable to chronic ocular diseases than to the ones caused by cerebral ischemic lesions,11,12 considering the character of visual deficit. On the other hand, it might comprise psychological sufferings as shown for hemianopia caused by stroke. Both have in common the acute onset and vascular risk profile. 13 Due to the unreplaceable function for perception of retina cells, there is a less likelihood of recovery after RAO. Though connected in a neural network offering plasticity, recent studies demonstrated, that apart from early improvements, severe impairments remain after ischemic cerebral stroke 12 months or longer, too. 14
The aim was to assess impairments of quality of life due to RAO or PCIS, which are relevant for rehabilitation. Rehabilitative treatment of patients with hemianopia or monocular vision loss after stroke should pursue to restitute daily function “ad integrum.” Therefore, we took the general population as the most appropriate group for comparison.
We hypothesized that RAO and stroke related hemianopia have an impact on health-related quality of life assessed with PROMs and that they have differences in the affected domains.
Methods
Study design
In a prospective observational implementation study, we included patients with acute ischemic or hemorrhagic stroke, transient ischemic attack, and retinal ischemia treated on the stroke unit of the University Medical Center Hamburg-Eppendorf over a period of 15 months. 15 Informed consent was obtained by patients or authorized guardians at the latest prior to collecting outcome information at 90 days after stroke. Patient reported outcomes were assessed at admission, at 90 days, and at 12 months. Results of the implementation and patient reported outcome measures concerning acute ischemic stroke, transient ischemic attack and intracerebral hemorrhage have been published previously.16,17 For the present analysis, we included patients with RAO confirmed on fundoscopy, TVL lasting less than 24 h, and patients with isolated partial or full hemianopia on the NIHSS and with posterior circulation ischemic stroke (PCIS) on cranial CT or MR imaging. We included only patients with hemianopia due to PCIS without other neurological deficits scored on the NIHSS. The isolated hemianopia comprised full homonymous and partial, for example, quadrant, impairment. Patients with transient monocular vision loss (TVL) were included to determine potential influence of diagnosis and an experienced event of visual impairment on anxiety and the mental domains measured by the patient centered questionnaires. Informed consent was obtained. The study protocol of the original prospective study was approved by the ethics committee of the Hamburg chamber of physicians. The study was registered at ClinicalTrials.gov, NCT03795948. 15
Assessments
Data were collected according to the International Consortium for Health Outcome Measurement (ICHOM)-Standard Set for Stroke. 18 Patients’ demographics, clinical characteristics and history were determined from electronic medical records and interviews after admission to inpatient treatment. Cardiovascular risk factors were monitored by diagnoses reported in the medical record or interview. Patient-reported outcomes were assessed 3 and 12 months after admission postally by questionnaires. If patients did not respond and could not be reached for at least three times via phone call over a period of 2 weeks, they were considered as lost to follow-up. Patients who have died were considered as completers, but not included in the statistical analysis.
Outcomes
The PROM Information System 10-Question Short-Form (PROMIS-10) version 1.1. assesses patients physical and mental health by two main domains each consisting of four items, which are used to calculate T-scores, respectively. The general population reference norm is 50 with a standard deviation of 10. 18 Lower values reflect a poorer outcome. Additionally, two single questions of PROMIS-10 measure achievement of social function and general health reaching from 1 (poor) to 5 (excellent).
The simplified modified Ranking Scale questionnaire (smRSq) estimates disability in overall functioning by a score reaching from 0 for no symptoms to 6 for death, comparable to the traditional scale. 19
In addition to the ICHOM-Standard Set for Stroke, we administered the Patient Health Questionnaire-4 (PHQ-4). It consists of four four-level items, testing potential presence of anxiety and depressive symptoms with two items each. 20 We used the two items through dichotomized outcomes with a cut-off value between “normal findings” and “potentially clinically relevant findings.” 20 Reference mean values of a general population for anxiety are 0.82 (CI:0.79, 0.85; SD: 1.10) and for depressive symptoms 0.94 (CI:0.90, 0.97; SD: 1.20). 20
Statistical analysis
Categorical variables were presented as counts and percentages and differences were tested using the χ2 test. Continuous variables were presented as means and standard deviations and comparisons were performed using analysis of variance (ANOVA). smRSq was presented as median and interquartile range and compared using the Kruskal–Wallis test. Comparisons of group means with reference population values were conducted using one sample t-tests.
Statistical analysis was carried out using IBM SPSS Statistics, Version 25.0 (Armonk, NY: IBM Corp) and R Version 4.3.3.
Data availability
Deidentified individual participant data will be made available upon reasonable request and where necessary after approval of the ethics committee by the corresponding author within 24 months after publication. Additional information can be taken from our study protocol. 15
Results
Characteristics
We included 57 patients with the diagnosis of RAO, 25 with TVL, and 19 with PCIS (Table 1). Patients with RAO had a mean age of 72.3 years and 45.6% were female. 54.4% of them had hypertension, 14.0% diabetes and 10.5% prior events of stroke or 7% of myocardial infarction. 8.8% had atrial fibrillation. Patients with TVL and PCIS had comparable demographics and similarly distributed cardiovascular risk factors. Diabetes was least frequently present in patients with PCIS. The median NIHSS of patients with PCIS was 2 (IQR: 0/2) compared to 0 (IQR: 0/0) of patients with RAO or TVL.
Characteristics at time of diagnosis.
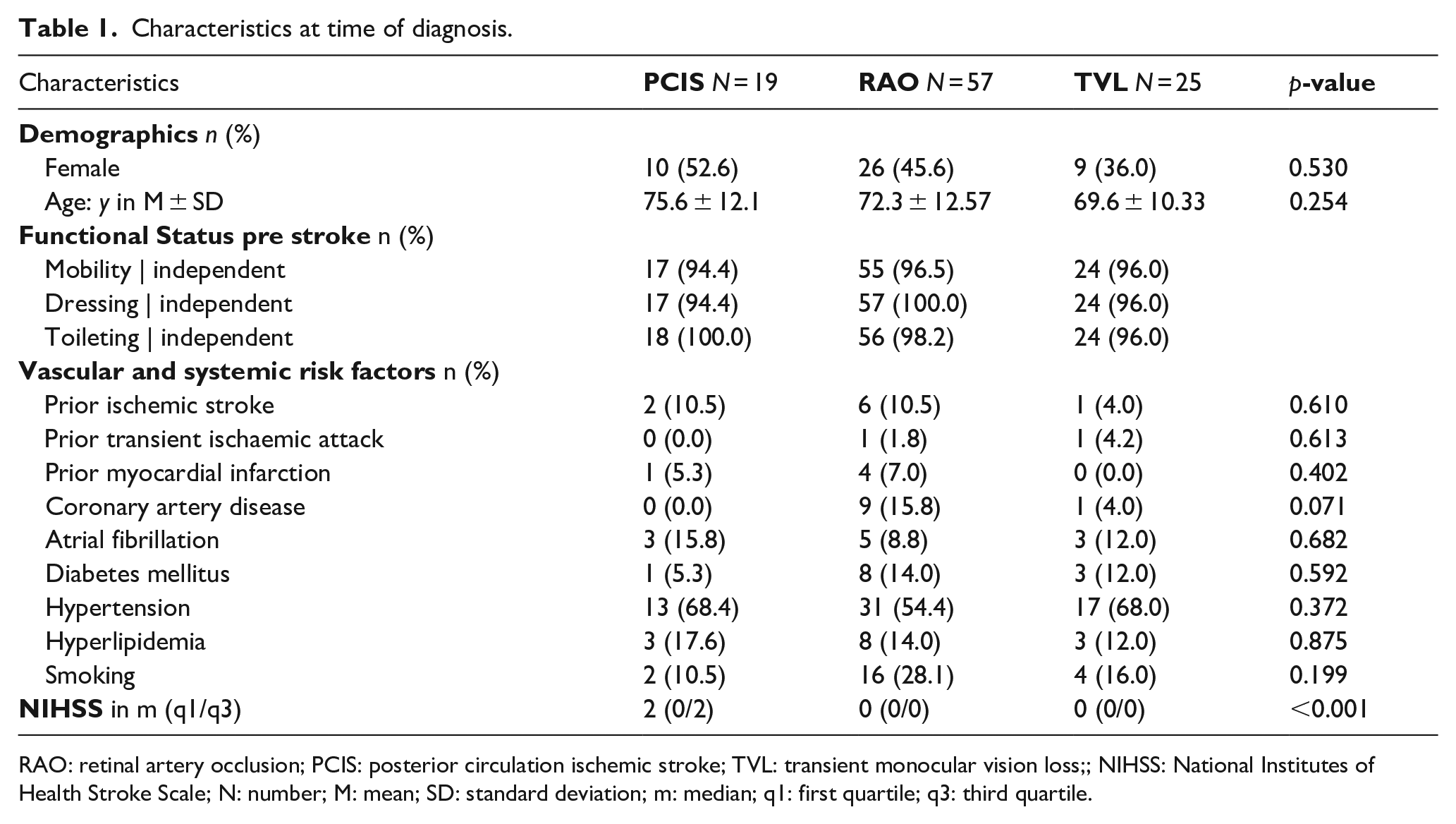
RAO: retinal artery occlusion; PCIS: posterior circulation ischemic stroke; TVL: transient monocular vision loss;; NIHSS: National Institutes of Health Stroke Scale; N: number; M: mean; SD: standard deviation; m: median; q1: first quartile; q3: third quartile.
Patient reported outcomes
Physical and mental health measured by PROMIS-10 had mean T-Scores (±standard deviation) of 47.1 ± 8.8 and 46.7 ± 8.8 for 41 patients with RAO and 49.4 ± 8.8 and 46.9 ± 8.0 for patients with TVL measured at 3 months follow-up after admission (Table 2). Patients with PCIS had T-Scores 43.4 ± 9.8 and 43.2 ± 6.2 in physical and mental domains of the PROMIS-10 at 3 months follow up. Compared to the T-score of 50 ± 10 measured in general populations, patients with RAO or PCIS scored statistically significantly lower on scales of both PROMIS physical (p = 0.043; p = 0.011) and PROMIS (p = 0.021; p < 0.001) mental at 3 months of follow-up, while patients with TVL showed no statistically significant difference (Table 2). After 12 months of follow-up, only the difference in PROMIS mental scores between PCIS and the general populations was statistically significant (p = 0.043).
Patient-reported outcome 90 days and 12 months after surveillance on stroke unit compared to the general population.
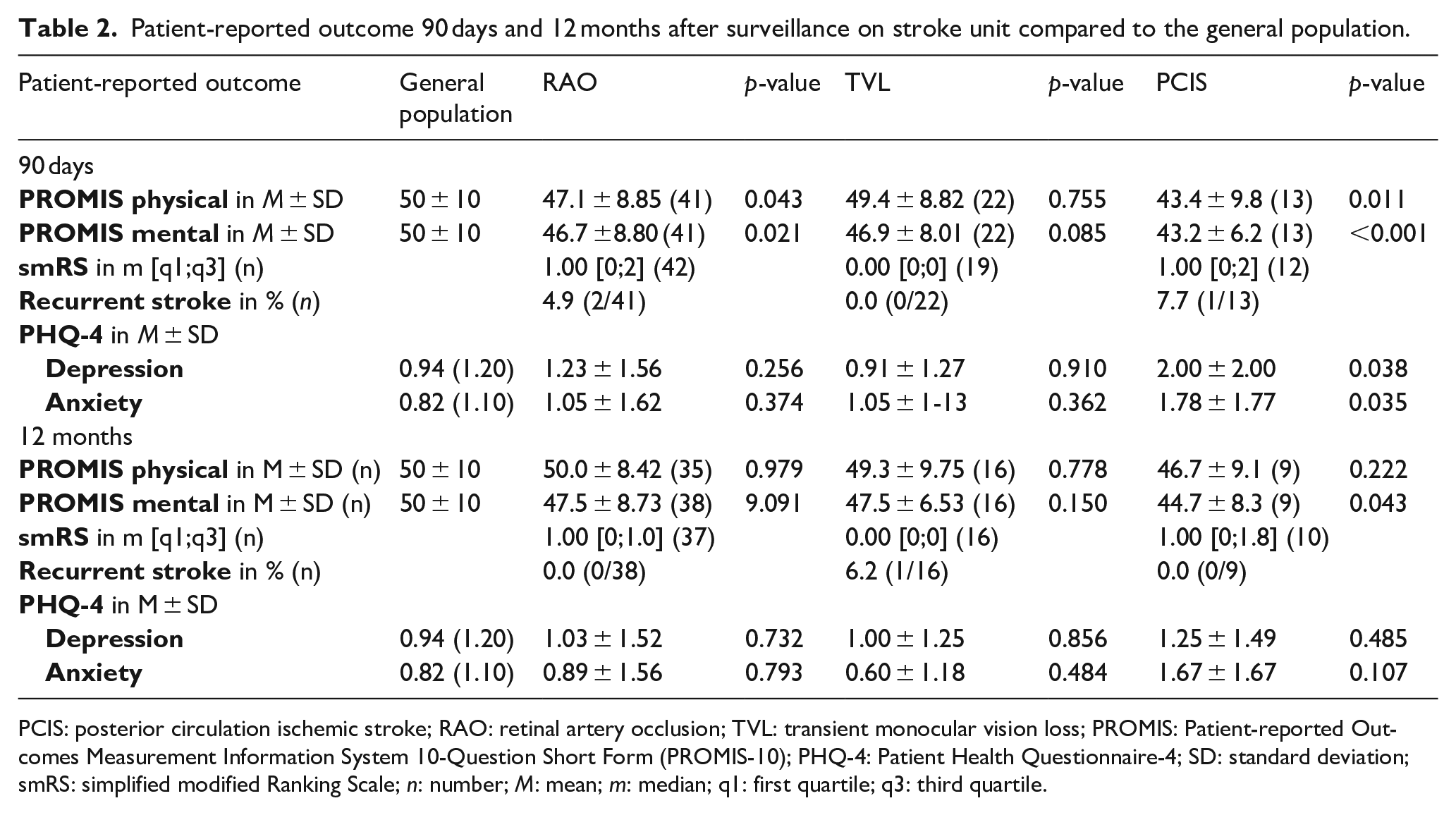
PCIS: posterior circulation ischemic stroke; RAO: retinal artery occlusion; TVL: transient monocular vision loss; PROMIS: Patient-reported Outcomes Measurement Information System 10-Question Short Form (PROMIS-10); PHQ-4: Patient Health Questionnaire-4; SD: standard deviation; smRS: simplified modified Ranking Scale; n: number; M: mean; m: median; q1: first quartile; q3: third quartile.
Frequencies of patients with scores of PHQ-4 indicative for anxiety or depressive symptoms are shown in Table 2. The mean values enable comparisons with the general population. In questions concerning anxiety and depression patients with RAO scored affirmative in 25% (mean: 1.05 ± 1.62 and 1.23 ± 1.56), patients with TVL affirmative in 9% (mean: 1.05 ± 1.23 and 0.91 ± 1.27), and patients with PCIS affirmative in 62% (mean: 1.78 ± 1.77and 2.00 ± 2.00). Compared to the average value measured in general populations, patients with PCIS had statistically significantly higher values in both domains (anxiety: p = 0.035; depression: p = 0.038) at 3 months of follow-up. After 12 months, no statistically significant difference was determined between the three groups and the general population in the two domains.
In the smRSq 42 patients with RAO and 12 with PCIS scored a median of 1 (IQR: 0/2) with no difference in comparison of the two groups. 19 patients with TVL had a median score of 0 (IQR: 0/0) at 3 months follow-up. It was statistically significantly lower than the one of RAO (p < 0.001) and PCIS (p = 0.007). Values for PCIS and TVL remained unchanged at 12 months follow-up and decreased for RAO to 1 (IQR: 0/1.5) with a statistically significant difference between TVL and RAO (p = 0.011), TVL and PCIS (p = 0.035), and no statistically significant difference between RAO and PCIS.
Discussion
Patient reported outcome measures are important tools to assess impairments of quality of life caused by stroke and to adapt and improve its rehabilitation. This study emphasizes the difference in outcome between patients with monocular vision impairment due to RAO or TVL and patients with hemianopia due to PCIS. Patients with TVL showed no statistically significant difference compared to the general population in all measured domains. Patients with RAO scored statistically significantly lower on physical and mental domains at 3 months, while PCIS was associated with statistically significantly decreased values of physical, mental, and behavioral health with mental impairments lasting up to 12 months of follow up. These results suggest that a different approach in planning post-stroke care may need to be considered for RAO and PCIS. The different impairments of managing every-day life are not yet based in clinical routine of stroke centers, which commonly initiate the same ophthalmologic rehabilitative steps for both RAO and PCIS, or solely for RAO.
The patients were consecutively recruited on our stroke unit and represent a part of the inpatient clientele for acute treatment of a stroke center. Cardiovascular risk factors were similarly distributed between the three diagnoses and encourage an equal surveillance, search for cause, and preventive treatment. 21 Slightly higher rates of smokers and a lower percentage of determined atrial fibrillation in patients with RAO support known data. 22
We used a pragmatic standardized set of PROMs developed by ICHOM to assess patients in course of acute stroke. Patients’ partial or full hemianopia was assessed and judged to be isolated by the NIHSS. Visual deficits are therefore paramount. the patients had no paresis, ataxia, or moderate-severe sensory deficits. However, the assessment by NIHSS does not rule out more complex deficits. For example, an impaired conceptualization of movements would be possibly not scored. Due to the posterior occipital localization on CT or MRI, however, it would then likely be part of the visual system. Their score in the PROMIS-10 revealed impairments in physical and mental domains of self-reported quality of life comparable or concerning the mental domain even lower than the ones of the average ischemic stroke patients with higher NIHSS scores.2,17 The outcomes addressing anxiety and depressive symptoms further support the reported association of hemianopia with psychological impairments of quality of life. 4 Self-reported outcomes of RAO in the behavioral domains were somewhat closer to the level in the general population. These outcomes stand in contrast to the ones of PROMs developed for assessment of ophthalmologic diseases. They measured a negative influence of chronic monocular vision impairment on quality of life. This may rely on focused domains, for example, one for spatial vision,11,12 reflecting visual tasks and challenges to a higher degree than impairments of every-day life.
Therefore, the reason for the only marginally lower values of patients with RAO after 12 months reported in this study are possibly a consequence of the questionnaire than an absence of impairments. Questions about fatigue and communication might not be relevant for patients with RAO. Consequently, disease-specific PROMs might be more suitable for this population than generic measures. Yet, the generic measures used in this study highlight the difference between visual deficits caused by hemianopia and RAO. Patients with hemianopia scored lower in mental and behavioral domains sustaining long lasting impairments in every-day life. This may be explained by more subtle neurological deficits as discussed above, or by a more functional character of visual deficits as shown for the ability to read. Ceased or ameliorated visual deficits after RAO are unlikely the cause of less or no mental and behavioral impairments after 12 months. Up to 39% of patients with RAO recover slightly and gradually in peripheral and paracentral fields while the central field and visual acuity are the least likely to recover. 10 The long-lasting impairment of mental health opposed to recovery of anxiety and depressive symptoms after PCIS supports causes of reduced cognition or fatigue beyond behavioral disorders, e.g. difficulties in spatial orientation and imagination, reading and focusing moving objects. In contrast to monocular vision loss, patients with stroke related hemianopia suffer from alexia. They have a lack of reading saccades and recognition of words, 23 while reading performance of monocular and binocular vision is comparable. 24 The impaired and slowed refixation due to hemianopia may contribute to the reduced visual attention shown for PCIS and cause general fatigue in managing tasks of every-day life.25,26 Furthermore, difficulties in recognizing faces after PCIS reflects disability beyond pure visual field loss and a character of impairment different to RAO. 27 More complex consequences of hemianopia due to stroke like hallucinations may contribute to the reported anxiety or depressive symptoms in every-day life. 28 This impaired function of the primary and secondary visual cortex is reflected by the low scores on PROMs of our patients with PCIS and raises the hypothesis that different approaches to assess and treat retinal and cerebral causes of visual impairments after stroke may be necessary. The currently used ophthalmologic training comprises prismatic correction to expand the intact visual field, training of compensatory eye movements to increase the ability of searching objects, and the induction of optokinetic nystagmus to ameliorate reading skills. 29 Focusing on visual deficits alone may be sufficient for RAO, but need to be expanded by abstract visual and behavioral tasks with neuropsychological direction and evaluation concerning hemianopia due to PCIS. 30
Limitations of this study are the small sample size, a selective patient clientele from a university stroke center with losses at follow-up, the lack of characterization of visual field loss upon admission and discharge, the pragmatic assessment of neurological deficits by the NIHHS, and the missing comparison with ophthalmologic PROMs. In addition, the statistical significance level was not adjusted for multiple testing, cautioning that all findings should be interpreted as strictly exploratory and in need for further confirmation. The strengths of the study include the long period of follow up and its selectively chosen patients based on neurological deficits, imaging data, and fundoscopy.
Our study shows a similar profile of risk factors of PCIS, RAO and TVL and supports equal surveillance, diagnostics, and preventive treatment. It suggests, however, a difference in impairment of quality of life. While impairments caused by ischemic stroke with hemianopia are reflected by PROMs with behavioral and stroke adapted domains, patients with RAO showed only in parts and less long-lasting impairments on every-day life measured by the used scales. The study highlights the necessity of a more detailed characterization and adapted treatment of visual impairments with consideration of a different concept for post-stroke care.
Footnotes
Acknowledgements
None.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DLR, ELP, ES, SA, MP, FN, CM, BC, SK, TZ, and CT have nothing to report. CG reports personal fees from Amgen, Bayer Vital, Bristol-Myers Squibb, Boehringer Ingelheim, Sanofi Aventis, Abbott, and Prediction Biosciences outside the submitted work. GT reports receiving consulting fees from Acandis, grant support, and lecture fees from Bayer, lecture fees from Boehringer Ingelheim, Bristol-Myers Squibb/Pfizer, and Daiichi Sankyo, and consulting fees and lecture fees from Stryker outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is funded by the Innovation Fund of the German Federal Joint Committee with the grant number 01VSF16023. The German Federal Joint Committee reviewed and approved the study design during the grant application process. It had no role in the conduct of the study or publication process.
Informed consent
Informed consent was obtained by patients or authorized guardians at the latest prior to collecting outcome information at 90 days after stroke.
Ethical approval
The study protocol of the original prospective study was approved by the ethics committee of the Hamburg chamber of physicians. This study was comleted in accordance with the Helsinki Declaration as revised in 2013. The study was registered at ClinicalTrials.gov, NCT03795948.
Guarantor
DLR; All authors had access to all data in the study and have read and approved the final version of the manuscript. They have no potential conflicts of interest. The material in the manuscript has not been published or is under consideration for publication elsewhere.
Contributorship
D. Leander Rimmele contributed to the planning of the study, acquisition, analysis and interpretation of the data and drafted the manuscript. Elina L. Petersen contributed to the analysis of data and revised the manuscript for intellectual content. Theresa Schrage contributed to the analysis of data and revised the manuscript for intellectual content. Martin Härter contributed to the planning of the study and revised the manuscript for intellectual content. Levente Kriston contributed to the planning of the study and revised the manuscript for intellectual content. Götz Thomalla contributed to the planning of the study, interpretation of the data and revised the manuscript for intellectual content.
Consent to participate
Written informed consent was obtained from all subjects or legally authorized representatives before the study.
Consent for publication
Not applicable.
Trial Registration
Data availability
Deidentified individual participant data will be made available upon reasonable request by the corresponding author. Where necessary approval of the ethics committee will be obtained in advance.