
Abstract
Introduction:
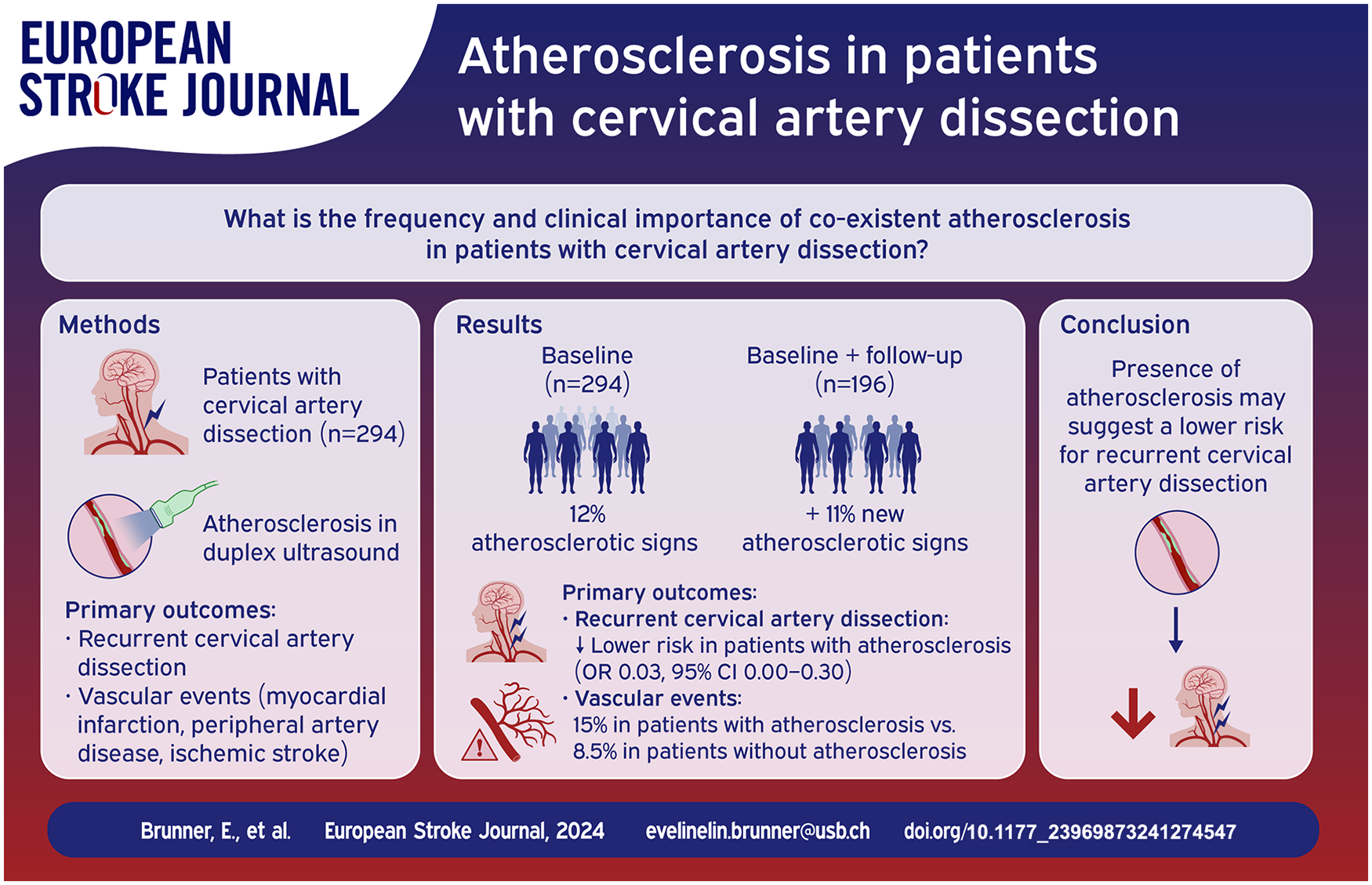
Cervical artery dissection (CeAD) is considered a non-atherosclerotic arteriopathy, but atherosclerosis of the cervical arteries may co-exist. We explored the frequency and clinical importance of co-existent atherosclerosis in patients with CeAD.
Patients and methods:
Single-center exploratory study from the Stroke Center Basel, Switzerland. We re-reviewed duplex ultrasound images at (i) baseline and (ii) last follow-up visit for the presence versus absence of the following atherosclerotic manifestations in the carotid arteries: (i) abnormal carotid intima-media thickness, (ii) plaques, and (iii) atherosclerotic stenosis. We investigated whether CeAD patients with versus without co-existing atherosclerosis differ regarding (a) recurrence of CeAD and (b) occurrence of vascular events (myocardial infarction, peripheral artery disease, or ischemic stroke) using logistic regression with adjustment for age and follow-up time.
Results:
Among 294 CeAD patients (median age 46 [IQR 37–53], 41.8% women), 35 (12%) had any atherosclerotic signs at baseline. Among 196 patients with available follow-up, another 21/196 (11%) patients developed atherosclerosis during a median follow-up of 55.7 months. Patients with atherosclerosis had decreased odds of recurrent CeADs when compared to patients without atherosclerosis (OR 0.03, 95% CI = 0.00-0.30). During follow-up, 6 (15%) vascular events occurred among 40 CeAD patients with atherosclerosis and 13 (8.5%) among 153 patients without atherosclerosis (OR 1.38, 95% CI = 0.39-4.55, data for 3 patients were missing).
Discussion and conclusion:
Signs of atherosclerosis in the carotid artery were detectable in 12% of CeAD patient at baseline. Additionally, 11% of CeAD patients developed new signs of atherosclerosis within the following 5 years. The presence of atherosclerosis may suggest a lower risk for recurrent CeAD. Whether it might indicate an increased risk for late clinical vascular events deserves further studies.
Introduction
Cervical artery dissection (CeAD) is a leading cause of stroke in the young.1–3 CeAD is considered a non-atherosclerotic arteriopathy 4 with an intramural hematoma as pathophysiologic hallmark, which is thought to be caused by a subintimal tear into the arterial wall of the carotid or the vertebral artery or by rupture of the vasa vasorum. 5 However, atherosclerosis of the cervical arteries may co-exist 6 in CeAD. This assumption is supported by the fact, that atherosclerosis 6 and CeAD7,8 share arterial hypertension as major risk factor. Nevertheless, little is known about the frequency and the clinical significance of atherosclerostic manifestations in the cervical arteries among patients with CeAD.
Duplex ultrasound is an established, non-invasive, and widely available diagnostic tool to monitor CeAD patients3,9 and also to detect atherosclerosis of the carotid arteries. 10
In this study, our objective was to examine the frequency of signs of atherosclerosis in the carotid arteries, as identified by duplex ultrasound images, among patients with CeAD at baseline and over time. Particularly, we aimed to determine whether CeAD patients with co-existing atherosclerosis differ from those without atherosclerosis regarding the risk of recurrent CeAD and vascular events of atherosclerotic or embolic origin during follow-up.
Methods
We looked at signs of atherosclerosis in the carotid arteries only, as the assessment of atherosclerosis in the vertebral arteries is associated with great uncertainty. All reviewers assessed the presence or absence of the following ultrasound findings (at baseline and follow-up examination): (i) carotid intima-media thickness (CIMT), (ii) plaque, and (iii) atherosclerotic stenosis. CIMT is defined as the distance from the lumen-intima interface to the media-adventitia interface. 13 As suggested for standard examination, we analyzed the CIMT of the common carotid artery (CCA) in long-axis view to describe beginning atherosclerosis.14,15 A CIMT > 0.9 mm was considered abnormal.16,17 A plaque was defined as (i) focal thickening thought to be atherosclerotic in origin protruding into the lumen or (ii) diffuse increase of CIMT in any segment of the carotid artery exceeding the thickness of the surrounding area by >50%. 15 Identifying the difference between medial thickening and diffuse atherosclerotic plaque is recognized as a matter of debate. Consequently, we followed the recommendations provided by the American Society of Echocardiography. 15 Each plaque was assessed for echogenicity, and a distinction was made between predominantly hypoechoic or hyperechoic features. Plaques that could not be assigned to either group were termed mixed plaques. Artery stenosis through atherosclerosis was further analyzed with Doppler spectral waveforms and flow parameters to determine the hemodynamic status of the artery. Atherosclerotic stenosis of the carotid artery was classified according to the following criteria as done in prior research 18 : normal (0%–49% stenosis), moderate (50%–69%), or severe (70%–99%). If atherosclerosis was detected, we assessed whether it was located in the artery affected by CeAD.
We also reassessed the arterial characteristics of the dissected arteries on duplex ultrasound at baseline, applying criteria from prior research: (i) mural hematoma,19,20 (ii) intimal flap, 20 (iii) double lumen,20,21 (iv) dissecting aneurysm, 20 (v) stenosis of the dissected artery, 22 and (vi) occlusion. 23
We then assessed the primary outcomes (i) recurrent CeAD (i.e. detection of at least one of the aforementioned CeAD imaging criteria on follow-up duplex ultrasound in a previously unaffected artery based on both the baseline (or prior) duplex ultrasound and the report of the baseline (or prior) MR imaging) and (ii) clinical events of presumably atherosclerotic or embolic cause (i.e. myocardial infarction, peripheral artery disease, ischemic stroke). To effectively handle the low number of primary outcomes, exploratory logistic regression analyses using maximum penalized likelihood method were conducted to investigate the relationship between atherosclerosis and the primary outcomes. Post hoc, we conducted similar logistic regression analyses to investigate the vascular events in cases where both dissection and atherosclerosis occurred in the same cervical artery. For all logistic models, we adjusted for age and follow-up time.
We specifically assessed manifest atherosclerosis (i.e. plaques or atherosclerotic stenosis) in the primary outcomes with absolute numbers in a separate table. To ensure completeness and demonstrate generalizability, we have included a separate table displaying the baseline characteristics of patients who did not have a follow-up ⩾12 months after the index event (Supplemental Table 2). Additionally, to analyze the risk factors associated with recurrent dissection, we have provided an extra table (Supplemental Table 4).
For all results, we provided relative effects (odds ratio (OR) with 95% confidence intervals (CI)). Because of the exploratory nature of the study, no adjustments for multiple testing were made. All statistical analyses were performed using R Studio version 4.3.2 (2023-10-31 ucrt).
Results
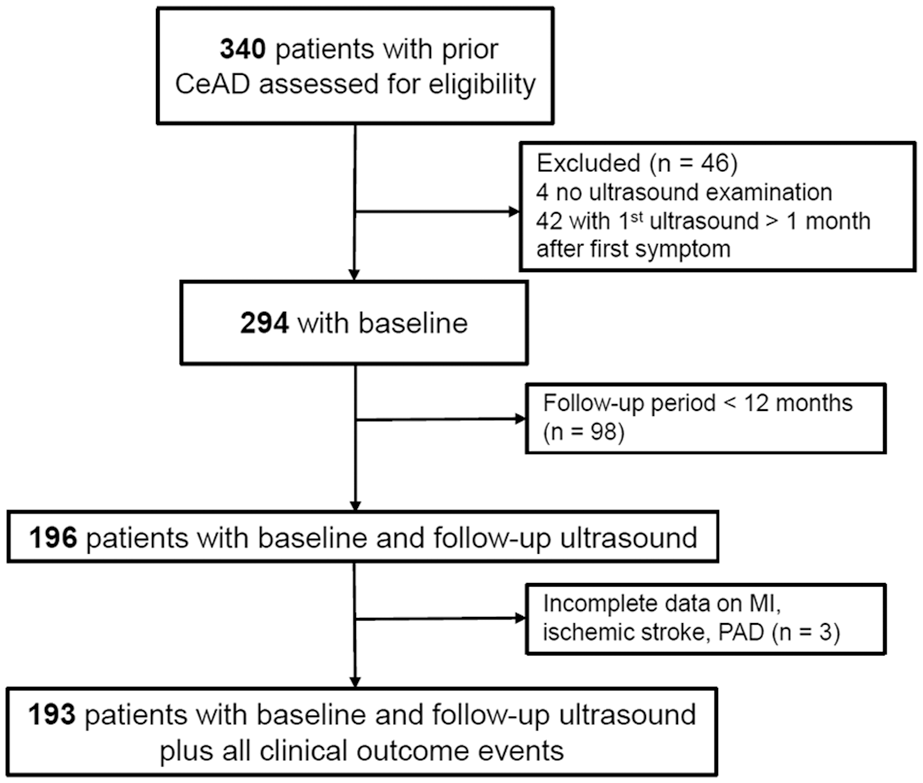
Flowchart of enrolled patients.
35/294 (12%) showed signs of atherosclerosis at baseline. All 35 (100%) of them had an abnormal CIMT, 1 (2.9%) presented with atherosclerotic stenosis ⩾50%, and 16 (45.7%) showed plaques. Most plaques showed mixed echogenicity (8/16, 50%) or were classified as hyperechogenic (7/16, 44%). Among 35 patients with atherosclerosis, 13 (37.1%) had atherosclerosis on the artery affected by CeAD.
Patients with co-existing atherosclerosis at baseline were older (median age 56 [IQR 51.50–62]) and more frequently male patients (80% of 35) than patients without atherosclerosis (median age 44 [IQR 37–52], 55.2% male). Vascular risk factors were more prevalent in patients with co-existing atherosclerosis than in those without (hypertension in 51.4% vs 31.0%, hypercholesterolemia in 34.3% vs 12.8%, and smoking at index event in 40.0% vs 27.2%). Diabetes mellitus was present in only a minimal percentage of the study population (3/294 (1%); Table 1).
Patient baseline characteristics and comparisons among those with atherosclerosis and without (n = 294).

IQR: interquartile range; NIHSS: National Institutes of Health Stroke Scale.
Refers to n = 255, data for four patients are missing.
Patient characteristics at follow-up and comparisons among those with atherosclerosis and without (n = 196).

IQR: interquartile range; CeAD: cervical artery dissection; PAD: peripheral artery disease.

Forest plot: Impact of atherosclerosis on recurrent CeAD and vascular events.
Looking at manifest atherosclerosis only, it was detected in 20 of 196 patients with long-term follow-up (10.2%). None (0%) of these patients suffered a recurrent CeAD during follow-up and vascular events occurred in 4/19 (21.1%, data for 1 patient was missing) patients with manifest atherosclerosis (Supplemental Table 3).
Discussion
This single-center study exploring atherosclerosis in CeAD patients revealed the following key findings: (i) atherosclerosis was present in 12% of CeAD patients at baseline and developed in an additional 11% within the following 4.6 years (55.7 months) after CeAD; (ii) patients with atherosclerosis (either at baseline or during follow-up) had lower odds of recurrent cervical artery dissections; and (iii) myocardial infarction, ischemic stroke, and peripheral artery disease occurred numerically more often in CeAD patients with atherosclerosis than in those without, while this difference did not reach significance.
Our finding that 12% of CeAD patients showed signs of atherosclerosis at baseline was important, as hardly any comparable published data specifically investigating atherosclerosis in CeAD patients are available. Brkić et al. reported a prevalence of atherosclerosis in 17.5% of 188 patients with vertebrobasilar and/or internal carotid artery dissection with a mean age of 53.7 years. 33 They observed atherosclerosis significantly more often in vertebral artery dissection than in internal carotid artery dissection patients. Chien et al. analyzed atherosclerosis specifically in patients with vertebrobasilar artery dissection in a patient group with a mean age of 65.5 years, 34 differing from the typical age group of CeAD patients. Age is one of the main risk factors for atherosclerosis 35 and could thus present a major confounder in the assessment of atherosclerosis in CeAD patients. The median age in our study was 46, which is more representative of a typical CeAD patient population. However, patients with atherosclerosis in our study were also older compared to those without atherosclerosis.
Ibanez et al. reported a prevalence of atherosclerosis detected by ultrasound of the carotid artery in healthy middle-aged subjects (mean age 46 years) of 24% in women and 36% in men. 36 These higher rates of atherosclerosis in healthy subjects compared to our CeAD patients, the typically young age of occurrence of CeAD, 2 and the inverse association of CeAD with hypercholesterolemia 37 all suggest that atherosclerosis is probably not a predisposing condition to CeAD, in contrast with aortic dissection. 38 Therefore, we hypothesize that CeAD patients are less likely to show signs of atherosclerosis, which is probably supported by the significantly higher occurrence of recurrent CeAD in patients without atherosclerosis. A potential explanation is that as individuals develop atherosclerosis, changes in the structure of the cervical arterial wall enhance its resistance to (intimal) tears. This is also speculated to be due to increased production and decreased breakdown of extracellular matrix components, as well as increasing collagen and elastin cross-links.37,39,40 Further, potential confounding factors include the genetic profiles of patients, as genetic studies showed an inverse association between atherosclerosis and CeAD for specific alleles. 41
Prior studies have shown that atherosclerosis is firmly established as the culprit causing clinical events (i.e. coronary heart disease and stroke).42,43 In our study, vascular events of atherosclerotic or embolic origin were more frequent in CeAD patients with co-existing atherosclerosis, although the difference to patients without atherosclerosis was not statistically significant. This is most likely attributed to the limited size of the study population and the small number of vascular events.
Our study has the following limitations: (i) despite performing a thorough review of all data, the analyses are based on retrospectively assessed, non-monitored, non-randomized data, hence raising the risk of chance findings. Furthermore, we had experienced raters, but did not assess the interrater reliability of our results. (ii) The retrospective design of the study with no predefined numbers or time points of follow-up examinations also increases the risk of selection bias, for example, toward patients at risk for complications that may be more likely to be followed up over a longer period of time and meanwhile develop atherosclerosis. (iii) Among other features, we distinguished atherosclerosis through abnormal carotid intima media thickness (CIMT), but as our observations were based on retrospective analyses, exact measurements were faced with technical limitations. (iv) Due to the limited sample size and primary outcomes, our main analyses not only included manifest atherosclerosis but also beginning atherosclerosis. This study should be regarded as an exploratory pilot study, with results that support the need for a larger multicenter study.
The strength of the current research includes the characteristics of our CeAD cohort, which closely resemble those of previous single- as well as multicenter CeAD studies,22,24 allowing for generalizability. Furthermore, we used duplex ultrasound as a tool to assess both (i) CeAD characteristics and (ii) atherosclerotic findings at different time points, conducted by raters experienced in both CeAD and atherosclerosis of the carotid arteries. 9 Due to the relatively young age of the patients at baseline, we were able to include individuals with early-stage atherosclerosis. Lastly, with a relatively long follow-up period, featuring a median of 4.6 years and extending up to 22 years, our study provides longitudinal data, enabling a comprehensive evaluation of the long-term outcomes and progression of CeAD.
In conclusion: Signs of atherosclerosis in the carotid artery were detectable in 12% of CeAD patient at baseline. Additionally, 11% of CeAD patients developed new signs of atherosclerosis within the following 5 years. The presence of atherosclerosis may suggest a lower risk for recurrent CeAD. Whether it might indicate an increased risk for late clinical vascular events deserves further studies. Likewise, individualized antithrombotic and statin therapy in patients with CeAD is to be considered and further explored.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241274547 – Supplemental material for Atherosclerosis in patients with cervical artery dissection
Supplemental material, sj-docx-1-eso-10.1177_23969873241274547 for Atherosclerosis in patients with cervical artery dissection by Eveline Brunner, Josefin E Kaufmann, Sandro Fischer, Henrik Gensicke, Annaelle Zietz, Alexandros A Polymeris, Valerian L Altersberger, Philippe A Lyrer, Christopher Traenka and Stefan T Engelter in European Stroke Journal
Footnotes
Acknowledgements
We thank all study participants and their families for their support. Open access funding provided by Universität Basel.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Wissenschaftsfonds Rehabilitation of FelixPlatter.
Ethical approval and informed consent
This study was approved by the Ethics Committee “Ethikkommission Nordwest- und Zentralschweiz” (EKNZ), and patients’ consent was obtained.
Guarantor
E.B.
Contributorship
E.B.: designed/conceptualized the study, analyzed/interpreted the data, drafted the manuscript, and collected data. J.E.K.: designed/conceptualized the study, analyzed/interpreted the data, revised the manuscript. C.T.: initiated, designed, conceptualized, and supervised the study, analyzed/interpreted the data, revised the manuscript, and collected data. S.T.E.: initiated, designed, conceptualized, and supervised the study, analyzed/interpreted the data, revised the manuscript, and collected data. All authors: critical review of the manuscript and editing manuscript for content. All authors agreed on submission of the present version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.