
Abstract
Purpose:
Cervical artery dissection (CAD) represents a unique clinical entity with a high risk of ischemic stroke. Vitamin K antagonists (VKA) showed good efficacy in CAD management but are cumbersome to use with potentially higher bleeding rates. Novel oral anticoagulants (NOAC) are easier to use and may have similar effects but lower hemorrhagic risk. In this systematic review, we compare the efficacy of NOAC to VKA as a potential alternative treatment.
Methods:
The literature was searched on Pubmed, PMC, and Embase via API through the Nested Knowledge AutoLit software in February 2022 for studies evaluating both NOAC and VKA. Baseline characteristics, clinical and radiographic outcomes, and hemorrhagic and ischemic complications were collected for single and double-arm studies and analyzed using random-effect subgroup meta-analysis.
Findings:
Overall, 11 studies were included with 699 patients treated with VKA and 53 treated with NOAC (from three studies; two were head-to-head comparative studies). There was no statistical difference in the baseline characteristics of VKA and NOAC patients. The rates of TIA/stroke in VKA and NOAC groups were 12.3% (95% CI; 0%, 28.6%) and 5.7% (95% CI; 0%, 12.2%), respectively. Major bleeding or intracranial bleeding were comparable between groups. Lesions treated with VKA showed angiographic recanalization with a rate of 51.4% (95% CI; 35.6%, 67.1%) and for those treated with NOAC was 58.4% (95% CI; 23.9%, 93.9%). The rates of good clinical outcomes were 79.9% (95% CI; 67.6%, 92.2%) in the VKA group and 91.4% (95% CI; 78.1%, 100%) in NOAC. No statistical difference was noted among any of the outcomes between the two treatment groups.
Discussion and conclusion:
We highlighted comparable efficacy and safety of NOAC to VKA for stroke prevention in CAD. Further head-to-head studies are warranted to validate these results.
Keywords
Introduction
Cervical artery dissection (CAD) represents a unique clinical and morphological entity triggered by an intimal tear between the inner and medial layers of the wall of extracranial carotid or vertebral arteries due to poorly identified multifactorial mechanisms. 1 CAD comprises a significant cause of cerebral ischemic stroke, with a prevalence of up to 25% of ischemic stroke, especially among young patients (<50 years old). 2 Prompt management of CAD is crucial to prevent further ischemic events potentially leading to disabling neurological deficits. In this context, two previous randomized clinical trials (CADISS and TREAT-CAD) tested whether anticoagulation (ACT) or antiplatelet (APT) regimens have better efficacy in preventing ischemic stroke in patients with CAD. Although the CADISS trial did not show any difference between APT and ACT groups, potentially due to liberal choices in the APT group, the TREAT-CAD trial showed aspirin was not non-inferior to warfarin.3,4 In both trials, the oral ACT regimen was warfarin. However, in real-life practice, novel oral anticoagulants (NOAC) have been preferred to warfarin because of the warfarin’s slower onset of action, more interactions with food and other medications, the necessity of routine laboratory monitoring, more significant time in non-therapeutic range, potentially higher incidence of major bleedings compared to NOAC. Recently, several large studies have found a considerable efficacy and safety of NOAC in stroke prevention in patients with non-valvular atrial fibrillation.5–7 This has encouraged a few groups to explore the clinical and safety profiles of NOAC in CAD in small case series.8–10 No large-scale studies have compared the efficacy and safety of NOAC in patients with CAD. In this study, we conducted a systematic review and meta-analysis of the safety and efficacy of the NOAC for the management of CAD in comparison with VKA based on the most recent literature.
Methods
Search strategy
The literature was searched on Pubmed, PMC, and Embase via API through the Nested Knowledge AutoLit software in February 2022 for the use of vitamin K antagonist anticoagulants (VKA) and novel oral anticoagulants (NOAC) in the treatment of cervical artery dissection (CAD). We applied for registration of this systematic review on PROSPERO. The search was performed in accordance with PRISMA guidelines. Search strategies were created using a combination of keywords and standardized index terms, including “Cervical dissection,” “warfarin,” “Novel oral anticoagulant,” “Direct oral anticoagulant,” “Vitamin K antagonist,” “Extracranial,” “Vertebral artery,” and “Internal carotid artery.” Results were limited to the English language from inception until now.
Eligibility criteria
Inclusion criteria included studies reporting a consecutive series of patients with cervical artery dissection managed with either vitamin K antagonist anticoagulants (VKA) or novel oral anticoagulants (NOAC) with clear reporting of the primary outcomes. Exclusion criteria included: (1) Editorial or opinion article, (2) Review or secondary article, (3) Case report or <4 patients, (4) In vitro or animal study, and (5) Secondary study of previously reported data.
Study selection process
One author screened the titles and abstracts for inclusion using Nested Knowledge’s screening software. Full-text articles of the included abstracts were retrieved and screened by the same author, and all inclusion decisions were approved by the senior author.
Data extraction and outcome measures
Baseline characteristics of each study population were collected, including age, gender, lesion location, clinical presentation, past medical history, baseline NIHSS and mRS scores, and use rates of intravenous thrombolysis for stroke management.
Outcomes of interest were stratified by applied medical treatment into two groups; patients receiving VKA and ones treated with NOAC. Clinical outcomes included good outcomes (mRS 0–2), poor outcomes (mRS 3–5), mortality rates, rates of TIA or stroke, intracranial bleeding, and minor and major bleeding. Radiographic outcomes included partial or total angiographic recanalization rates of the occluded dissected vessel and rates of angiographic worsening. Angiographic worsening was defined as a progressive occlusive or aneurysmal morphological changes in the dissected vessel.
Risk of bias assessment and heterogeneity
Risk of bias was assessed in details among included studies using ROBINS-I tool for non-randomized observational studies provided by Cochrane. 11 Since only one arm was pooled from included RCTs, they were also evaluated using Newcastle Ottawa Quality Assessment Scale. When possible, sources of heterogeneity among the results of very high heterogeneity (I2 > 80%) were investigated using sensitivity meta-analysis by removing individual studies or subgrouping by identified potential co-variates.
Statistical analysis
Continuous variables were reported as mean and standard deviation. Combined means and SDs of included studies were calculated using the “Combine Means and SDs Into One Group Program” provided by the Department of Obstetrics and Gynecology at the Chinese University of Hong Kong (CUHK). 12 Statistical difference between the proportions of baseline characteristics pooled from included studies for VKA and NOAC groups was addressed by comparing the Z score of each group via the “Z Score Calculator for 2 Population Proportions” open-source tool provided by Social Science Statistics website. 13 The cumulative incidence (event rate per patient at the end of the study) for each study was estimated and 95% CI. We used a random-effects model to pool incidence rates across studies because of the marked heterogeneity that we expected in the populations and interventions across various studies. The I2 statistic was used to express the proportion of inconsistency not attributable to chance. Subgroup meta-analysis for all outcomes was conducted using Freeman-Tukey double arcsine transformation with restricted maximum likelihood (REML) methods. The correction factor was null for all events, including zero events. Statistical analysis was performed via MAJOR tool (METAFOR package) on JAMOVI R-based statistical Software and OpenMeta[Analyst] open source Statistical Software.
Results
Search results and baseline characteristics
After the title, abstract and full-text screenings (Figure 1), 11 studies were eligible for inclusion (Table 1).4,8–10,14–20 A total of 752 patients with cervical artery dissection (CAD) with a mean age of 44.7 (SD: 12.7) and 451 (60%) men. Overall, 218 (39.1%) out of 558 patients had a history of smoking, 182 (26.9%) out of 676 had hypertension, 120 (24.6%) out of 488 had a history of head or neck trauma, 137 (22.75%) out of 602 patients had hyperlipidemia, 67 (17.05%) out of 391 had migraine, and 11 (6.35%) out of 173 patients had a previous history of TIA or stroke (Table 2). History of head/neck trauma was higher in the NOAC (38.8%) compared to the VKA group (23%, p = 0.015). TIA/stroke was the main presenting symptom with a rate of 74.6% in 464 patients, followed by headache (61.2%; 208 out of 340), and neck pain (34.8%; 119 out of 310). The occlusion site included the internal carotid artery in 455 (60.5%) and the vertebral artery in 309 (41.1%) out of 752 patients with 764 dissections. The baseline mean NIHSS score was 4.21 (SD: 6.2) in 283 patients. VKA was applied in 699 (93%) of CAD patients, and the rest received NOAC; 12 out of 15 patients of 3 studies received Rivaroxaban and 3 had Dabigatran. The outcomes stratified by proportion of each drug were not reported in one NOAC study. 8 The prevalence of vertebral artery dissection was higher in the NOAC (64.2%) compared to VKA (39.3%, p < 0.001). Thrombolytics were administered in 22 (5.1%) out of 433 and endovascular thrombectomy was performed in 12 (2.9%) out of 413 patients. Diagnosis of CAD was performed with CT angiography in 105 (78.9%) out of 133 patients, with MRA in 261 (79.5%) out of 341, and 52 (15.5%) out of 335 patients. The median follow-up of 743 patients from 10 studies was 6 months (3–28 months). Baseline characteristics of CAD patients were summarized in Table 2.
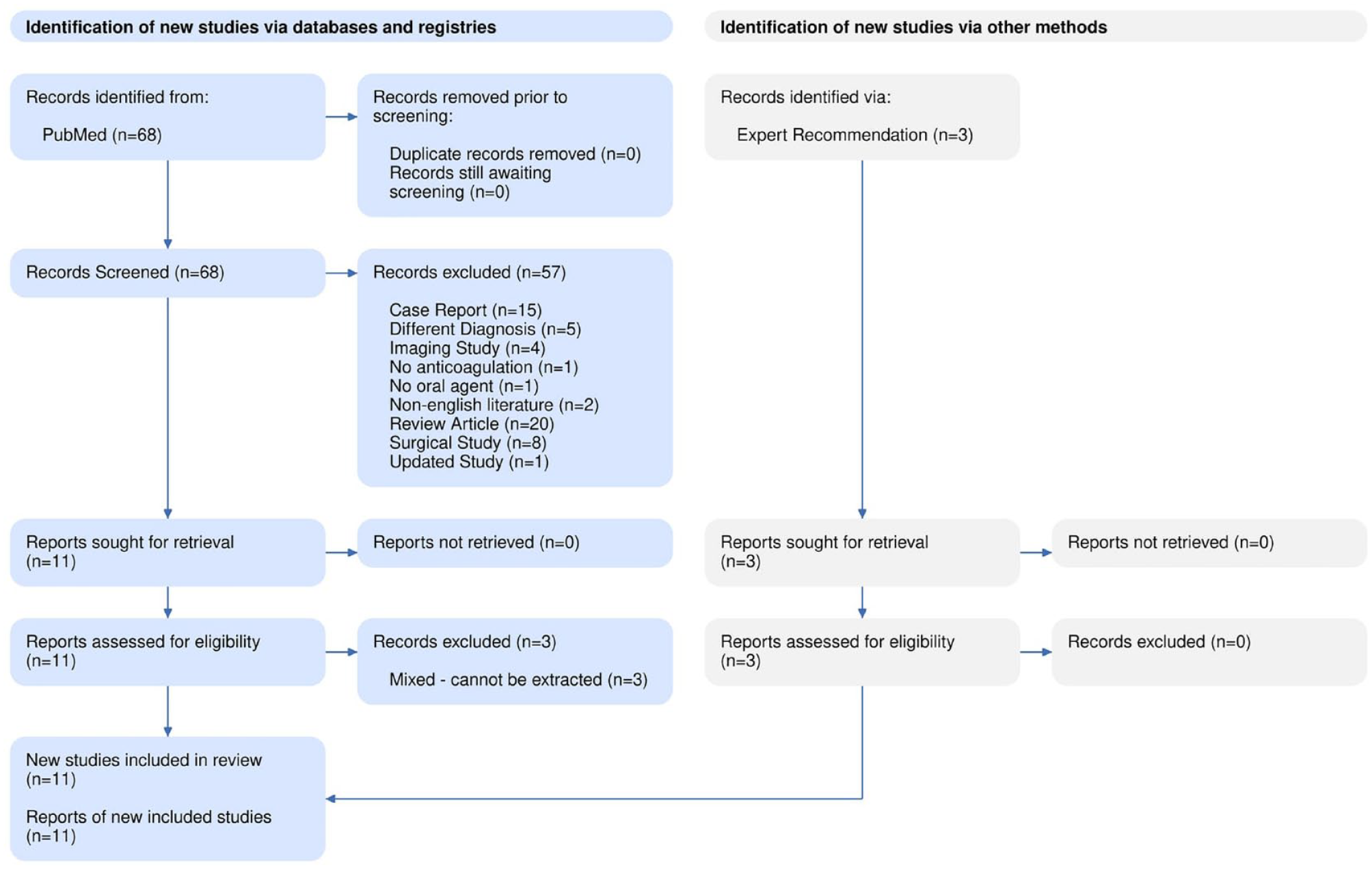
PRISMA flow diagram of included studies.
Summary of included studies.
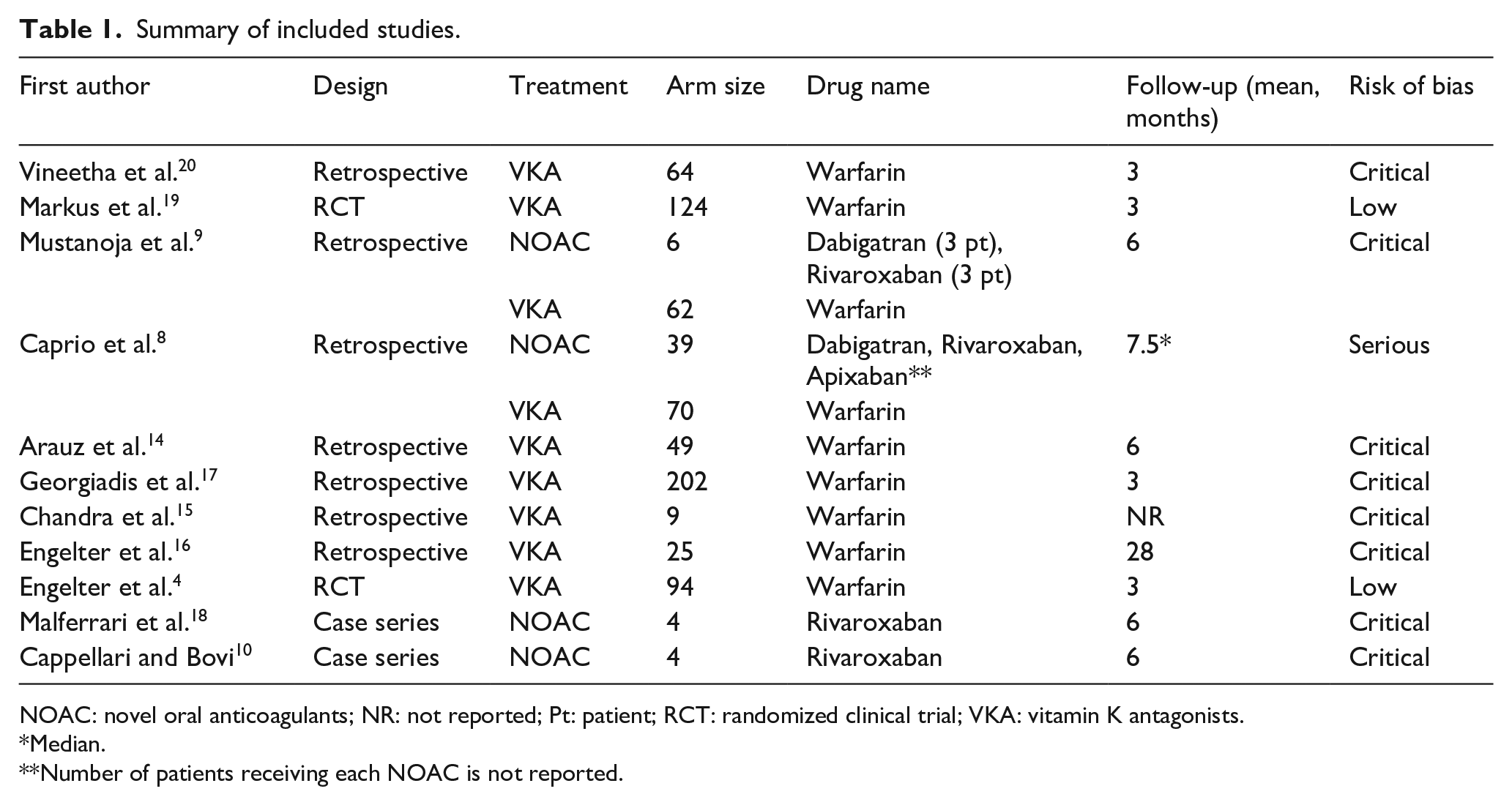
NOAC: novel oral anticoagulants; NR: not reported; Pt: patient; RCT: randomized clinical trial; VKA: vitamin K antagonists.
Median.
Number of patients receiving each NOAC is not reported.
Baseline characteristics.
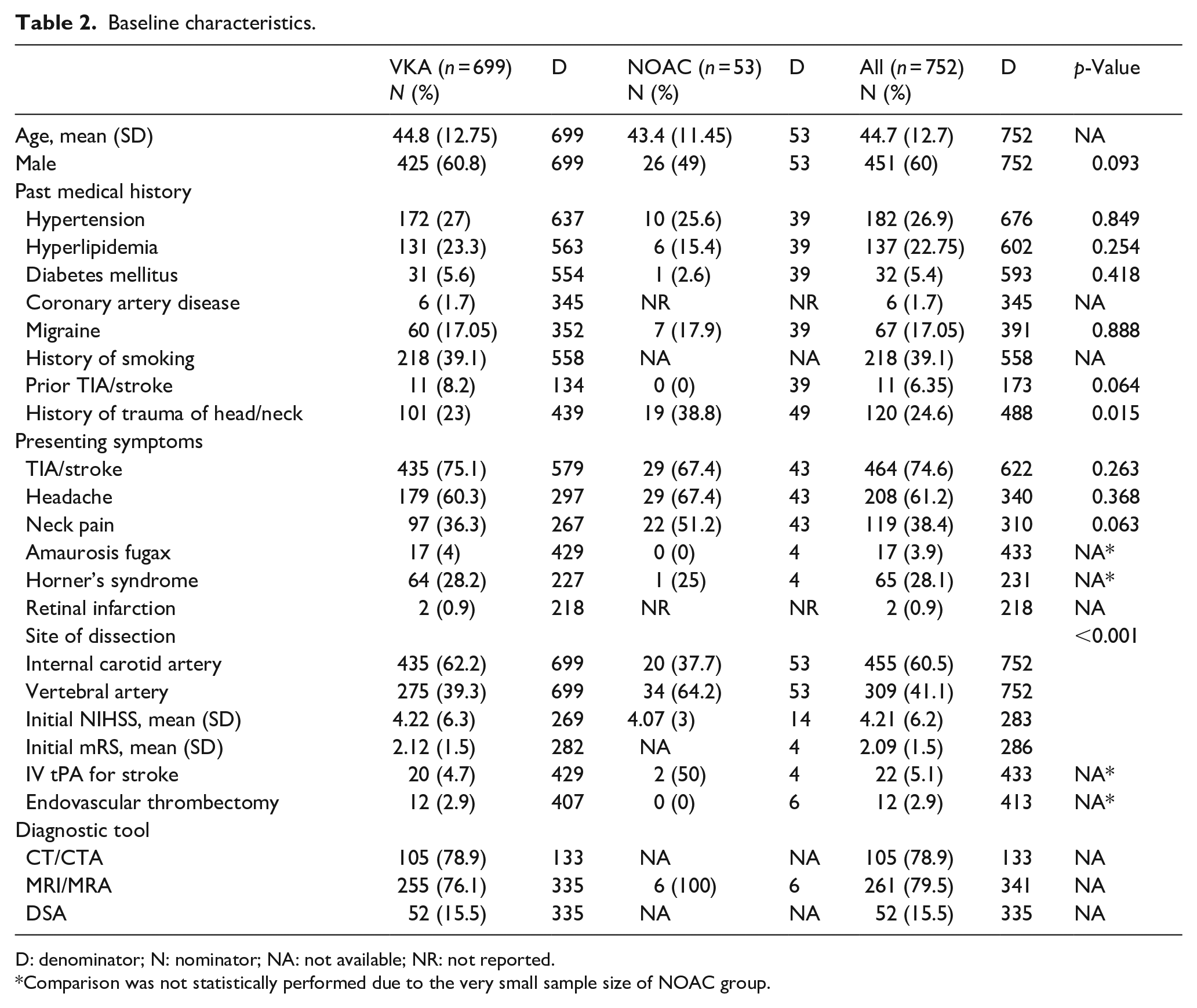
D: denominator; N: nominator; NA: not available; NR: not reported.
Comparison was not statistically performed due to the very small sample size of NOAC group.
Vitamin K antagonist anticoagulants (VKA)
Overall, of 699 patients receiving VKA for CAD, the rate of recurrent/de Novo stroke was 12.3% [29 out of 588, 95% CI; 0%, 28.6%] and 12 out of 571 (1.2% [95% CI; 0.3%, 2%]) patients suffered from intracranial bleeding. Minor bleeding was reported in 7 out of 189 patients (3.7% [95% CI; 1%, 6.3%]) and the rate of major bleeding was 1.2% [13 out of 577, 95% CI; 0.3%, 2.1%]. Angiographic recanalization was reported in 146 out of 327 patients (51.4% [95% CI; 35.6%, 67.1%]). Good clinical outcomes were reported in 236 out of 296 patients (79.9% [95% CI; 67.6%, 92.2%]), with mortality rates of 0.5% [4 out of 699, 95% CI; 0%, 1%]), respectively.
Novel oral anticoagulants (NOAC)
Among 53 patients with CAD treated with NOAC, the rate of recurrent/de Novo stroke was 5.7% [2 out of 47, 95% CI; 0%, 12.2%] and none out of 14 [8.6% per weighted analysis, 95% CI; 0%, 34.4%] patients suffered from intracranial bleeding. Minor bleeding was reported in 4 out of 47 patients (6.5% [95% CI; 0%, 13.9%]) and none of the 53 patients suffered from major bleeding (1.7% per weighted analysis, 95% CI; 0%, 5%]. Angiographic recanalization was reported in 30 out of 53 patients (58.9% [95% CI; 23.9%, 93.9%]) and 3 out of 47 (8.1% [95% CI; 0.5%, 15.7%]) showed angiographic worsening. Good clinical outcomes were reported in 14 out of 14 patients (91.4% [95% CI; 73.5%, 100%]), with mortality rates of 1.7% [0 out of 53, 95% CI; 0%, 5%]), respectively. No statistical difference was observed among any of the reported outcomes except for the angiographic worsening which was higher in the VKA group (p = 0.031) (Table 3). Forest plots of the meta-analysis results are provided in Figure 2(a)–(i).
Results of random effect meta-analysis.
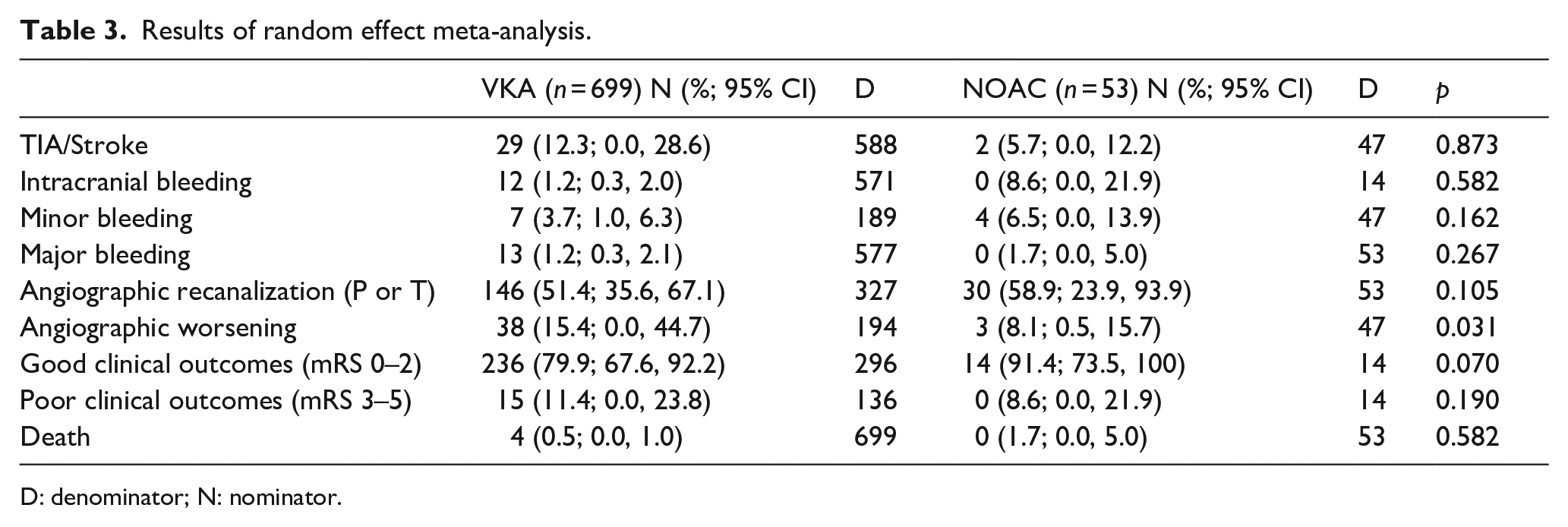
D: denominator; N: nominator.
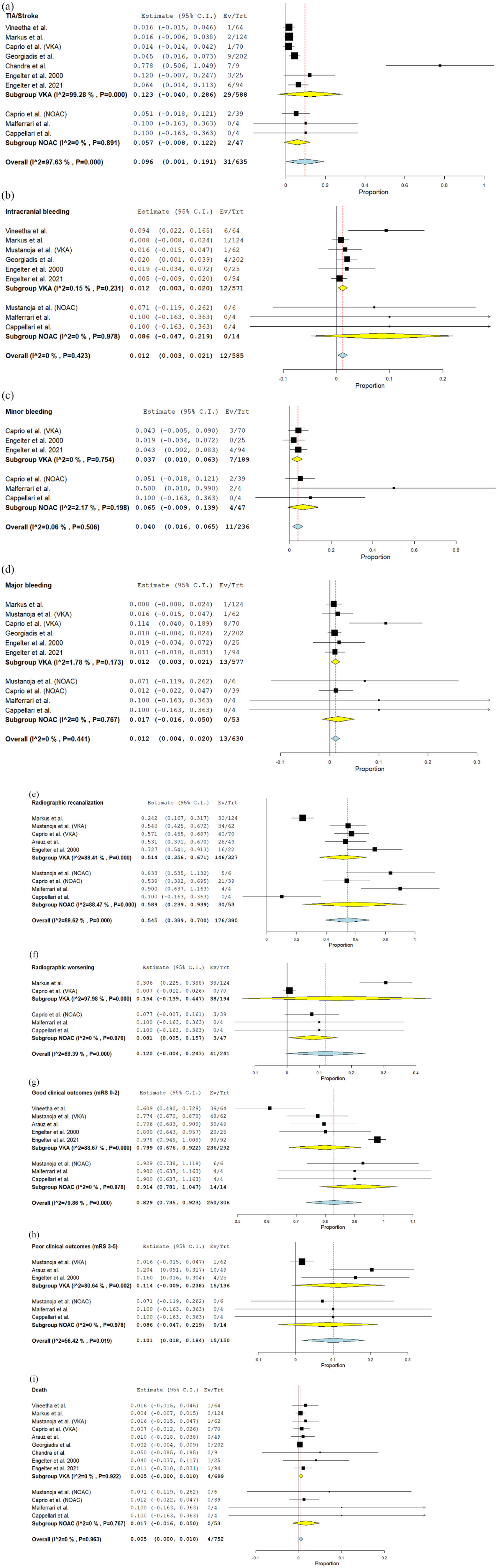
Forest plots of the meta-analysis outcomes: (a) TIA/stroke, (b) intracranial bleeding, (c) minor bleeding, (d) major bleeding, (e) angiographic recanalization, (f) angiographic worsening, (g) good clinical outcomes, (h) poor clinical outcomes, and (i) death.
Risk of bias and heterogeneity
The risk of bias was critical in eight, serious in one, and low in two studies (two RCTs) based on ROBINS-I tool (Supplemental Table 1). The largest study included 202 patients, and the lowest included 4 patients. Two studies included were RCTs and the rest were retrospective observational studies; two were two-arm studies.
High heterogeneity was observed among three outcomes. I2 value of TIA/Stroke outcome in VKA cohort was 99.28%. Sensitivity analysis was performed by removing Chandra et al. study which was thought to be the source of this high heterogeneity; I2 value decreased to 21% and the results changed considerably (from 12.3% [95% CI; 0.0%, 28.6%] to 2.7% [95% CI; 1.2%, 4.2%]) (Supplemental Figure 1). Radiographic outcomes suffered from high heterogeneity. I2 was around 88% in outcome of radiographic recanalization of both VKA and NOAC groups, which can be referred to the variations in recanalization ratios (partial or total); scarcely reported among the studies. Radiographic worsening outcomes showed I2 of 98% in VKA group due to many causes; only two studies were included for this outcome and due to variations in angiographic worsening which was defined as progression of narrowing to near complete or complete occlusion or to aneurysm formation. Clinical outcomes (either good or poor) showed also very high heterogeneity (I2 ≈ 90%). Thus, we applied sensitivity analysis using subgroup analysis approach and we identified time point of assessment (3 vs 6 months) as one of the major causes of the high heterogeneity in good (Supplemental Figure 2) and poor clinical outcomes (Supplemental Figure 3). However, considerable heterogeneity (I2 = 80%–90%) of an undetermined source, might be related to the small number of studies (2–3), is still standing among the clinical outcomes of VKA group.
Discussion
Our meta-analysis of 752 patients provides an updated snapshot of the current data on the safety and efficacy of VKA and NOACs in CAD. Overall, 53 patients were treated with NOAC, and 699 patients received VKA. There was no significant discrepancy in terms of admitting characteristics among the treatment groups except for the higher prevalence of vertebral artery dissection and the history of neck trauma in the NOAC group, which can be random or due to a selection bias. Furthermore, outcomes were overall similar among the NOAC and VKA cohorts with a higher rate of angiographic worsening in the VKA group but with no clinical sequela, suggesting the non-inferiority of NOAC compared to VKA for the management of CAD.
The aspect of this systematic review was to review all published series evaluating NOAC for CAD treatment, in which we found four observational studies with 53 patients. The rates of ischemic and hemorrhagic events were similar between NOAC and VKA patients and also similar to previous studies that used other antithrombotics for CAD.3,14,17 Moreover, despite the small sample size of the NOAC cohort in our study, there were no events of intracranial or major bleeding among patients receiving NOAC, and both treatment groups had similar angiographic and clinical outcomes. Caprio et al. 8 published a series of 149 patients with CAD stratified into three treatment groups as follows; 70 patients with VKA, 40 with APT, and 39 with NOAC. The authors found no statistical difference in outcomes among the three medications except in angiographic outcomes (worse in NOAC), proposing NOAC as a promising alternative for VKA and APT. Angiographic worsening was more common in the VKA cohort, which is more likely to be associated with new ischemic problems. However, it did not reflect on the recurrent TIA and stroke rates or clinical outcomes of the patients. We did not observe a difference in other angiographic outcomes between NOAC and VKA in our cumulative cohort.
CAD constitutes one of the leading causes of ischemic stroke, especially in young patients, which highlights the importance of antithrombotic treatment in stroke prevention. The choice of antithrombotic regimen remains controversial. Ye et al. 21 conducted a meta-analysis of seven studies with 1126 patients receiving ACT and APT for CAD and found no significant difference in any outcome among the treatment groups. This similarity in outcomes among APT and ACT was valid independent of dissection location, as proved in large series of cervical carotid and vertebral arteries dissections.14,17 However, the most recent randomized trial suggested a potentially better efficacy profile of warfarin over aspirin in stroke prevention. 4 Additionally, Liu et al. 22 just focused their analysis on two CAD RCTs3,4 in a recent systematic review and found a lower risk of ischemic stroke with ACT but without difference in rates of hemorrhagic complications or favorable clinical outcomes at 3 months.
In the last decade, NOACs replaced the VKA in various indications because of the necessity of routine laboratory monitoring, a slow onset of action, more interactions with food and other medications, and potentially a higher incidence of major bleeding.5–7,23,24 Previous studies also showed close to 50% of the time; patients are not therapeutic on warfarin. 25 As pointed out by Engelter et al. in the TREAT-CAD study, NOAC can potentially replace VKA in stroke prevention after CAD in the future. Additionally, majority of the ischemic events occurred within the first days in TREAT-CAD trial and while VKA was becoming therapeutic, low molecular heparin potentially provided the most antithrombotic benefit in preventing stroke. NOACs have an advantage of not requiring heparin bridging over VKA. As more and more patients with cervical dissections are treated with NOAC, further studies are needed to investigate the efficacy and safety of NOACs in CAD.
Limitations
The main limitations of this meta-analysis are a small size and the retrospective design of studies with NOAC patients comparing to the VKA group, which included two RCTs and a few large observational studies. The reasons for a scarce number of studies evaluating NOAC in CAD are (1) the relatively recent application of these drugs in clinical practice and (2) insufficient access to NOACs in most countries. Furthermore, the number of two-arm studies evaluating NOAC versus VKA was only two. Thus, two-arm meta-analysis and meta-regression to investigate the correlation of baseline characteristics with outcomes were inapplicable. Another limitation is some outcome measures (such as intracranial bleeding, functional outcomes) were not consistently reported in NOAC studies. The follow-up periods among included studies were heterogeneous, which makes it harder to have uniform comparisons among the study outcomes. Most included studies were assessed as of critical risk of bias, particularly studies reporting outcomes of NOAC group, which weakens profoundly the evidence of comparative analysis between the two interventions in our meta-analysis. Due to the small size of the NOAC group, the evidence comparing NOAC to VKA is weak, and large observational studies, and RCTs are warranted to validate these results.
Conclusion
CAD is an important cause of stroke in the young adult population. The main goal of CAD management is to diminish the stroke risk while the vessel wall healing and remodeling occur without increasing the risk of intracranial hemorrhage. In addition to the low risk of hemorrhagic complications and the convenient usage of NOAC, our findings suggest a comparable efficacy of NOAC to VKA in stroke prevention after CAD. Further head-to-head clinical trials are to validate these findings.
Supplemental Material
sj-docx-1-eso-10.1177_23969873221111051 – Supplemental material for Vitamin K antagonist versus novel oral anticoagulants for management of cervical artery dissection: Interactive systematic review and meta-analysis
Supplemental material, sj-docx-1-eso-10.1177_23969873221111051 for Vitamin K antagonist versus novel oral anticoagulants for management of cervical artery dissection: Interactive systematic review and meta-analysis by Muhammed Amir Essibayi, Giuseppe Lanzino and Zafer Keser in European Stroke Journal
Footnotes
Acknowledgements
The authors acknowledge Karl Holub, Stephen Mead, Jeffrey Johnson, and Darian Lehmann-Plantenberg for their design, development, and support of the Nested Knowledge meta-analytical software.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
ZK.
Contributorship
MAE and ZK researched literature and conceived the study. MAE analyzed the data and wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.