
Abstract
Introduction:
Migraine is a common, disabling chronic pain condition possibly related to changes in endothelial and vascular structure and function. Several observational studies have suggested an elevated risk of cervical artery dissection (CeAD) in patients with a history of migraine. We aimed to investigate this potential association using systematic review and meta-analytic methods.
Patients and methods:
We utilized a pre-defined search protocol to identify and screen studies related to migraine and CeAD in PubMed, Embase, and the Web of Science Core Collection. We assessed the risk of bias and performed a meta-analysis of selected studies to assess the association between migraine and CeAD. We also performed subgroup analyses by migraine subtype, biological sex, and the use of stroke versus non-stroke controls.
Results:
We identified 11 studies (N = 9857 patients) for inclusion in the meta-analysis. Meta-analysis showed an association between migraine and CeAD with an odds ratio of 1.74 (95%CI 1.38–2.19). There was high heterogeneity among the included studies (I2 = 61%). Publication bias was present but the Trim-Fill imputation suggested that the impact on results was likely minimal. Subgroup analyses revealed an association between migraine without aura and CeAD (OR 1.86, 95%CI 1.55–2.24) but not migraine with aura and CeAD (OR 1.15, 95%CI 0.71–1.88). There was no difference in the association between migraine and CeAD in men compared to women.
Discussion and conclusion:
A history of migraine is associated with an increased risk of CeAD. Further studies are needed to elucidate the potential pathophysiologic mechanisms underlying this association.
Introduction
Migraine affects approximately one billion people worldwide and is the leading cause of years lived with disability in individuals younger than 50 years. 1 Approximately one-third of individuals with migraine suffer from migraine with aura, characterized by transient neurological symptoms preceding a migraine attack. 2 Recent observational studies have indicated that migraine, particularly migraine with aura, is associated with an increased risk of ischemic stroke.3–5 A prior meta-analysis found that the association between migraine and stroke was the strongest among those aged <45 years. 4 However, the biological mechanisms underlying this association remain unclear.
Cervical artery dissection (CeAD) is an intimal tear in a cervical artery’s wall (i.e. carotid or vertebral artery) and is the most common reason for ischemic stroke in young and middle-aged adults.6–8 Although the etiology of spontaneous CeAD is not fully understood, research has suggested both genetic factors and vascular conditions such as hypertension and migraine could be risk factors for CeAD. 6
A prior meta-analysis observed an over two-fold increase in the risk of CeAD for individuals with migraine. 9 However, only five studies, all of fairly small size, were included in the meta-analysis. Since the publication of this meta-analysis, several additional studies, including larger-scale studies, have been published providing the opportunity to answer further questions, such as whether the association depends on migraine subtypes and the presence of stroke, both of which are clinically and etiologically important. We aim to provide an updated systematic review and meta-analysis of the association between migraine and CeAD and explore if this association varies by aura status, sex, and use of stroke versus non-stroke controls.
Methods
This study followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. 10
Data sources and searches
We searched PubMed, Embase, and Web of Science Core collection from database inception to August 2, 2022. We used the following search terms: (“migraine” OR “migraine disorders” OR “migrain*”) AND (“cervical dissection” OR “cervical artery dissection” OR “vertebral artery dissection” OR “vertebrobasilar artery dissection” OR “basilar artery dissection” OR “carotid artery, internal, dissection” OR “carotid artery injury” OR “artery dissection” OR “arterial dissection” OR “arterial tear” OR “intimal tear”) (Supplemental Table S1). We conducted reference mining of existing systematic reviews, meta-analyses, and relevant primary studies to identify additional literature.
Study selection
We included case-control, cohort, and cross-sectional studies that provided sufficient information to calculate a measure of association. Studies with case-report or case-series designs and conference abstracts were excluded. For the exposure, we recorded whether the study assessed active migraine or history of migraine, including self-reported diagnosis or medical diagnosis of migraine according to the International Classification of Headache Disorders (ICHD) (⩽3rd edition) criteria, 11 or the International Classification of Diseases (ICD) 9th or the ICD 10th revision12,13 for the outcome, we required studies to investigate participants with dissection of one or more cervical arteries, including carotid, vertebral, or basilar arteries with ascertainment of the dissection by direct visualization techniques, including angiography, duplex scan, magnetic resonance imaging, or computerized tomography. We excluded studies that investigated hereditary CeAD or major traumatic CeAD. Study selection was performed with a semi-automated software (Covidence, Veritas Health Innovation Ltd, Melbourne, Australia). Independent pairs of reviewers completed the title and abstract screen as well as the full-text screen. Any disagreement was resolved by a third investigator.
Data extraction and quality assessment
Extracted information included first author, publication year, study design, population description, sample size, mean age and its standard deviation, diagnostic criteria for migraine, migraine subtypes, diagnostic tools for CeAD, matching factors, covariates, effect estimates from the main and subgroup analyses, and their associated 95% confidence intervals. We applied the Newcastle-Ottawa Scale (NOS) to evaluate the quality of the selected studies with a maximum of 9 points. 14
Statistical analysis
Odds ratios (ORs) were chosen as the primary measure of association and multivariable-adjusted ORs were used in the analyses when provided. If adjusted ORs were not provided, we calculated a Mantel-Haenszel weighted OR if the study included sufficient information for univariable adjustment. Otherwise, we included an unadjusted OR. A random-effects restricted maximum likelihood (REML) model was used to allow high between-study variability. We performed the Cochran’s Q test and calculated the I2 statistic to quantify heterogeneity 15 and used the Galbraith plot to visualize the degree of heterogeneity and adequacy of the random-effects model. 16 We assessed publication bias via the Begg’s test 17 and Egger’s test. 18 We then quantified the magnitude of potential publication bias using the Trim and Fill method with the linear estimator 19 ; we visualized the result in a funnel plot.
We performed three pre-specified subgroup analyses based on sources of heterogeneity that we anticipated a priori due to differences in migraine subtypes (migraine with aura [MA] versus migraine without aura [MO]), sex, and control group selection (stroke vs non-stroke controls). The Cochran’s Q test (Qb) with 1 degree of freedom was used to assess the between-group difference for each subgroup analysis.
Three sensitivity analyses evaluated the robustness of the results. First, we performed a leave-one-out test to assess the impact of each study on the pooled estimate. Second, during the full-text screening, we identified two publications with overlapping study populations. In the primary analysis, we only included the study which reported adjusted ORs. In a sensitivity analysis, we replaced this study with the one that only provided unadjusted ORs. Third, for studies in which we calculated Mantel-Haenszel weighted ORs, we exchanged these estimates with the unadjusted ORs and re-computed the pooled result. For all analyses, we set the significance level to an alpha of 0.05, two-sided. All analyses were performed using Stata version 17 (Stata, College Station, TX, USA).
Results
Identification of studies
The study selection process is summarized in Figure 1. We identified 237 studies from PubMed, 516 studies from Embase, and 296 from the Web of Science Core Collection. After removal of duplicates, 707 studies were screened. After screening titles and abstracts, we excluded 649 studies irrelevant to the study topic and selected 58 studies for the full-text review. The inter-rater reliability had a
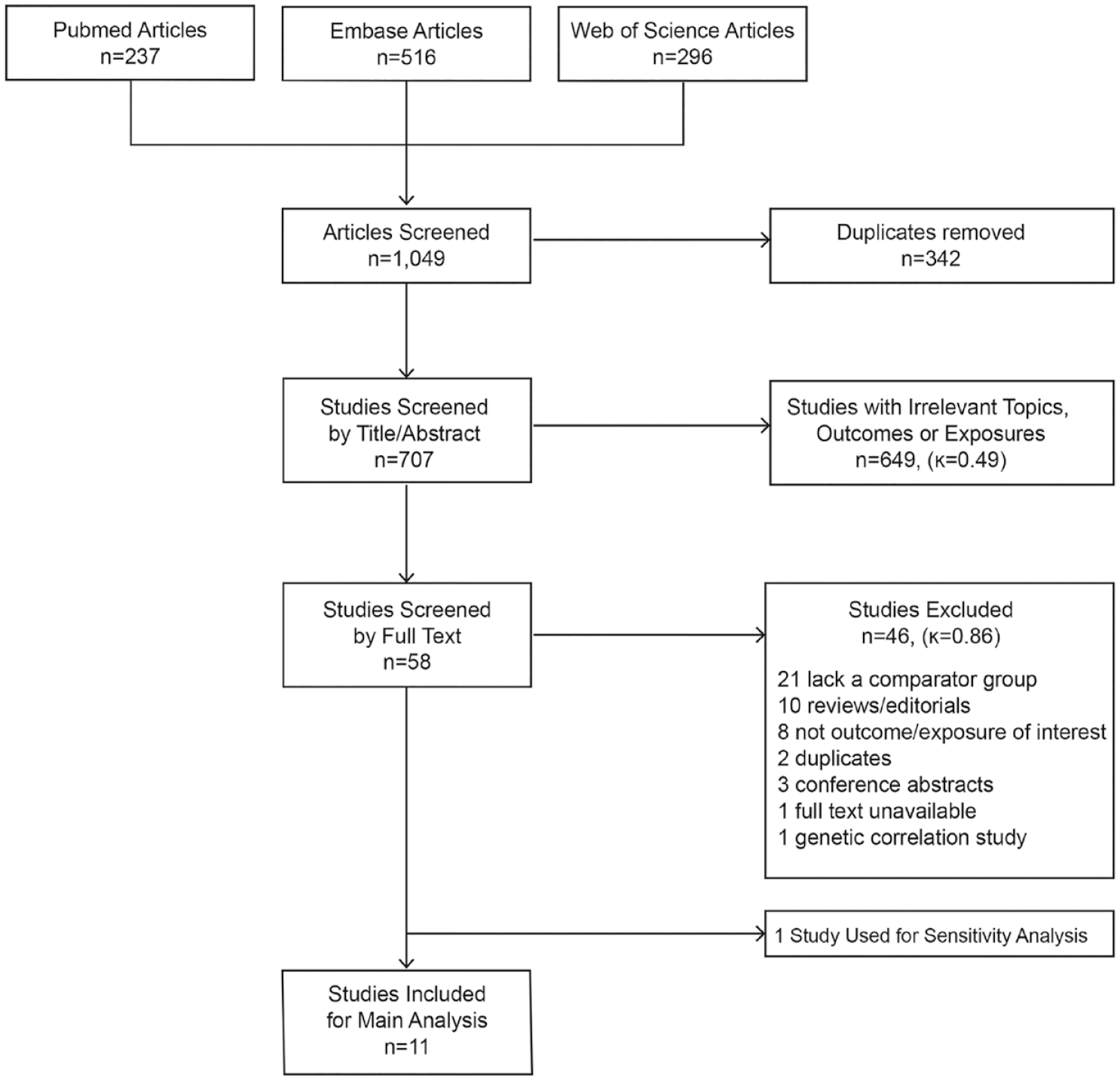
Flowchart of study selection.
Study characteristics
In the main analysis, we included 11 case-control studies (Table 1). The sample size of the individual studies ranged from 45 to 4055 participants. Seven studies included sufficient information on migraine subtypes and five studies presented sufficient data on sex to allow for subgroup analyses by these factors. All 11 studies provided criteria for control selection; notably, the type of control groups varied across studies. Three studies compared cases to healthy controls.22–24 One study compared cases to hospitalized patients who had cervical vascular imaging but did not have stroke. 25 We categorized these four studies into the subgroup of non-stroke controls.22–25 Six studies compared CeAD cases to patients who had ischemic stroke unrelated to CeAD.26–31 One study compared cases to two separate control groups – healthy controls as well as patients with non-CeAD induced stroke. 21 For this study, we included the stroke controls since they were more likely to resemble cases and thus reduce residual confounding. These seven studies were categorized into the subgroup of stroke controls.21,26–31
Characteristics of studies investigating the association between migraine and cervical artery dissection.
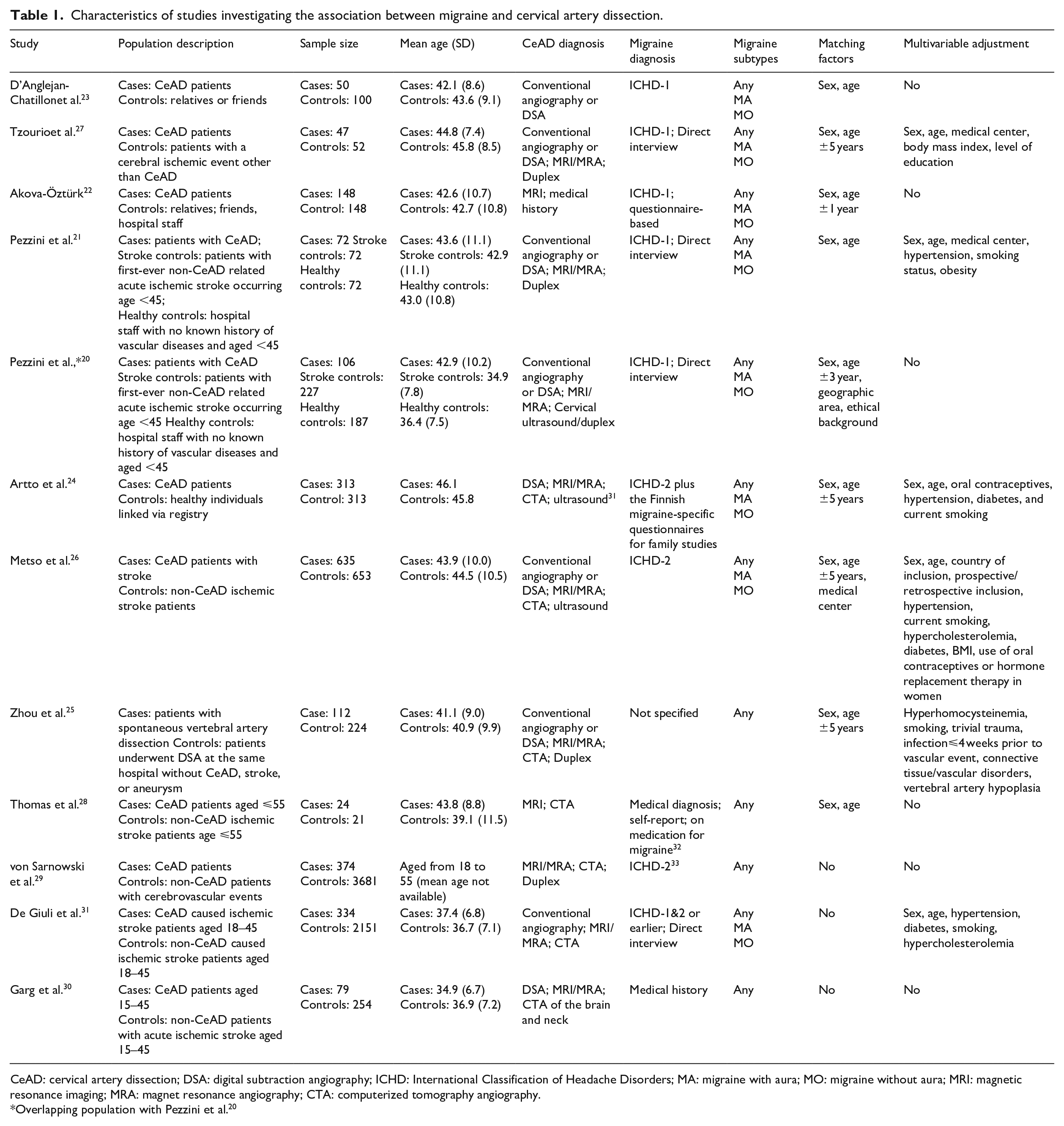
CeAD: cervical artery dissection; DSA: digital subtraction angiography; ICHD: International Classification of Headache Disorders; MA: migraine with aura; MO: migraine without aura; MRI: magnetic resonance imaging; MRA: magnet resonance angiography; CTA: computerized tomography angiography.
Overlapping population with Pezzini et al. 20
All 11 studies ascertained the outcome using cervical imaging techniques, including angiography, computed tomography (CT), magnetic resonance imaging (MRI), and duplex ultrasound. There were variations in the ascertainment of migraine status. Eight studies assessed migraine history before CeAD or stroke occurrence.21,22,24,26,27,29–31 One study asked the participants to recall their migraine status as of the time of dissection. 23 Two studies did not specify whether history of migraine prior to dissection or active migraine at the time of dissection was ascertained.25,28 Eight studies assessed migraine according to guidelines of the International Classification of Headache Disorders (ICHD).21–24,26,27,29,31 Two studies relied on self-reported diagnosis or medical records with unspecified criteria.27,29 One study did not provide information on how migraine was ascertained. 25
We directly obtained the adjusted OR from six studies.21,24–27,31 We computed the univariable-adjusted OR for two studies using Mantel-Haenszel weights by sex.23,29 We calculated the crude OR for three studies.22,28,30 For the selected studies, the overall quality of the evidence was moderate, with the NOS scores ranging from 4 to 7 points (Supplemental Table S2).
Results from meta-analysis
There were 2188 CeAD cases and 7669 controls identified from the 11 selected studies; 713 (32.6%) of the cases had migraine while 1867 of the controls (24.3%) had migraine. Meta-analysis showed a positive association between migraine and cervical artery dissection (OR 1.74, 95%CI 1.38–2.19; Figure 2). Heterogeneity among studies was high (I2 = 60.73%, p = 0.01). The Galbraith plot showed that all studies fell within the 95% confidence interval of the pooled OR except for the von Sarnowski et al. study (Supplemental Figure S1). 29 The presence of publication bias was suggested by the Egger test (p = 0.003) and the Begg test (p = 0.020). The funnel plot also showed moderate asymmetry (Supplemental Figure S2). However, the pooled OR was only slightly attenuated toward the null after the imputation of three small studies (OR 1.56, 95%CI 1.23–1.99). This result indicated that the overall pooled estimate was not significantly impacted by the potential publication bias.
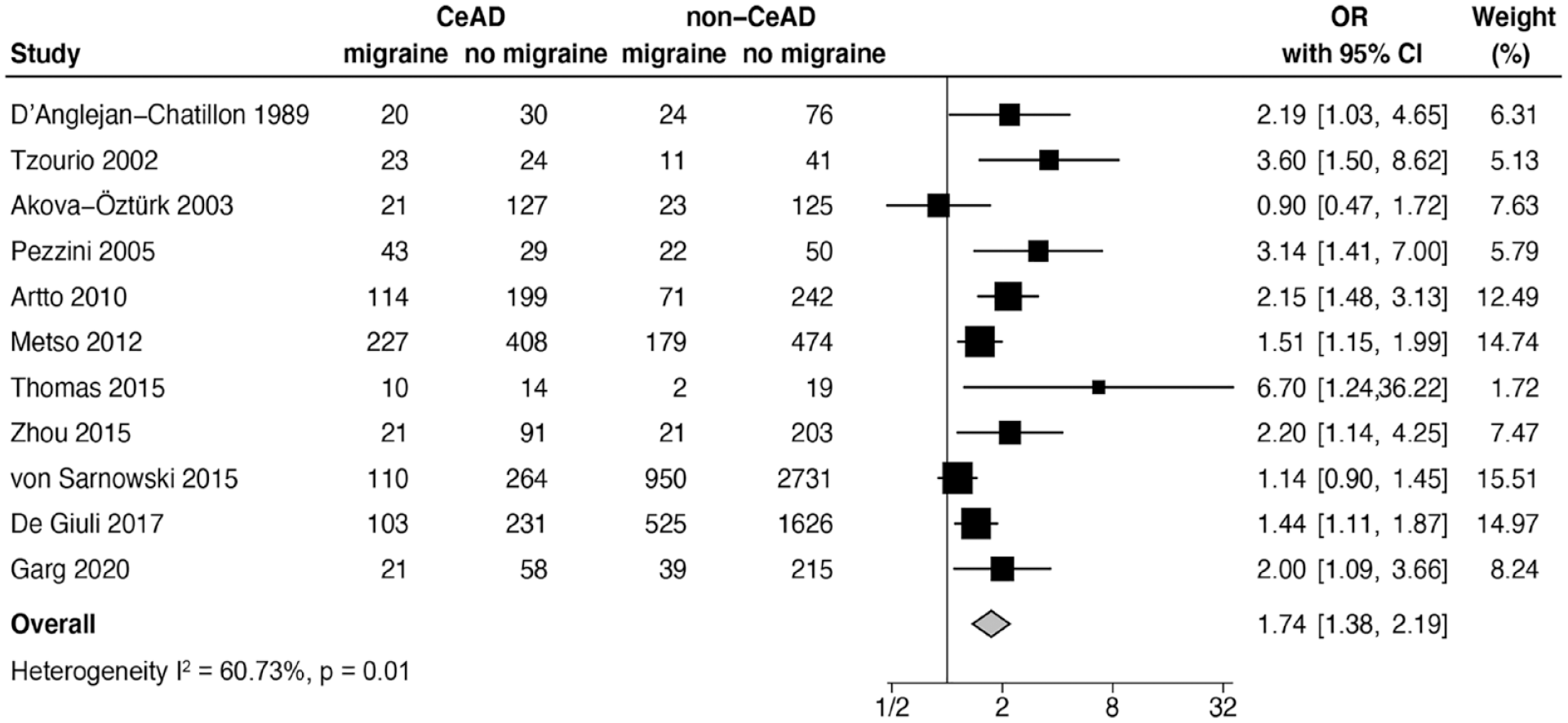
Forest plot showing the meta-analysis of 11 studies.
Subgroup analysis based on migraine type showed that migraine without aura was significantly associated with CeAD (OR 1.86, 95%CI 1.55–2.24, I2 = 0.00%) but migraine with aura was not (OR 1.15, 95%CI 0.71–1.88, I2 = 66.77%; Figure 3). Migraine was significantly associated with CeAD among both men (OR 1.55, 95%CI 1.25–1.92, I2 = 12.80%) and women (OR 1.35, 95%CI 1.10–1.66, I2 = 10.74%) and the strength of the association did not differ significantly by sex (p = 0.37; Figure 4). The association between migraine and CeAD was observed whether the studies used non-stroke controls (OR 1.78, 95%CI 1.18–2.69, I2 = 49.29%) or stroke controls (OR 1.77, 95%CI 1.29–2.42, I2 = 71.09%) and the strength of the association was similar regardless of the control group used (p = 0.98; Figure 5). The results from our sensitivity analyses were consistent with those from the main analyses (Supplemental Figures S3, S4, and S5).
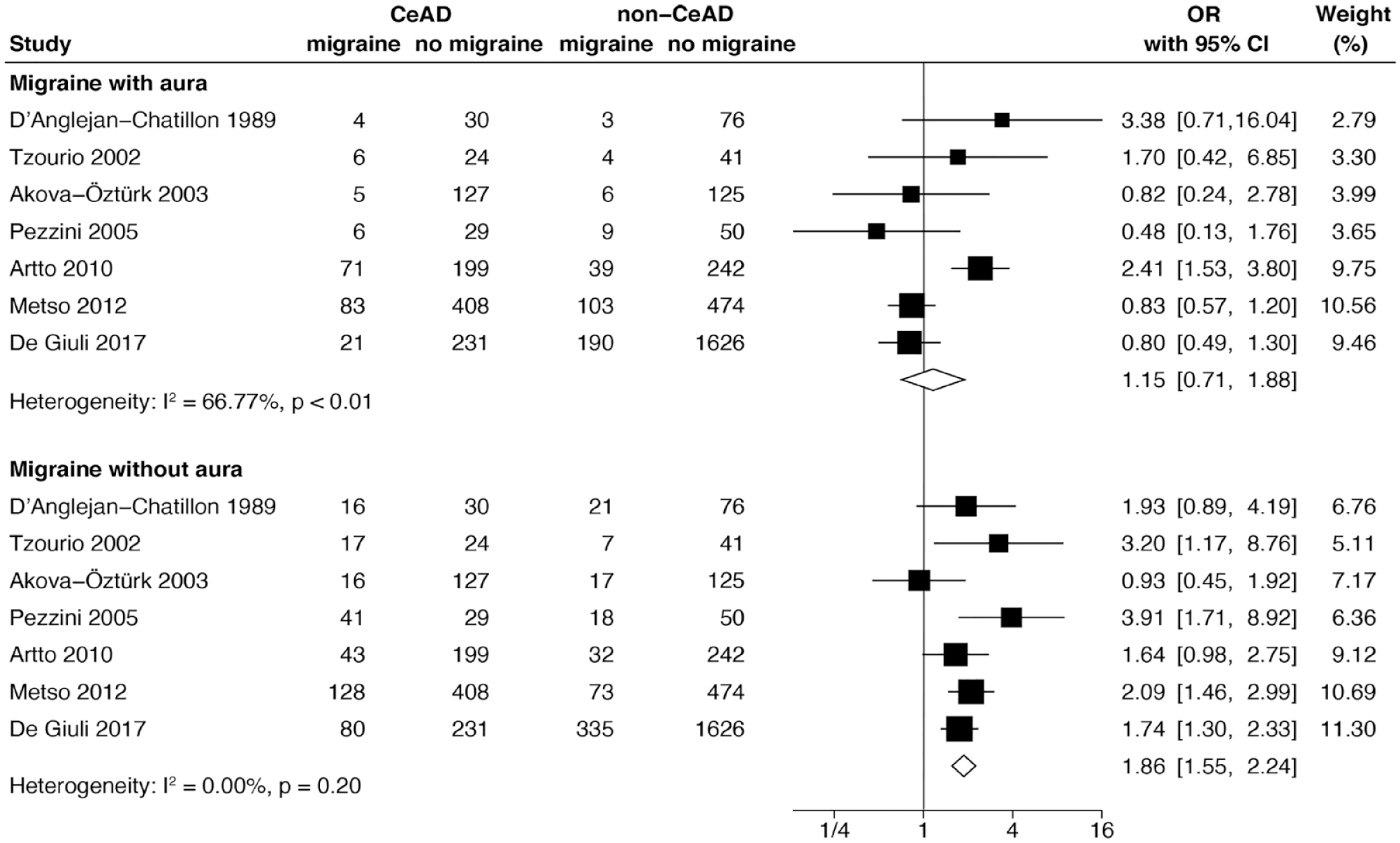
Forest plot showing the meta-analyses by migraine subtypes.
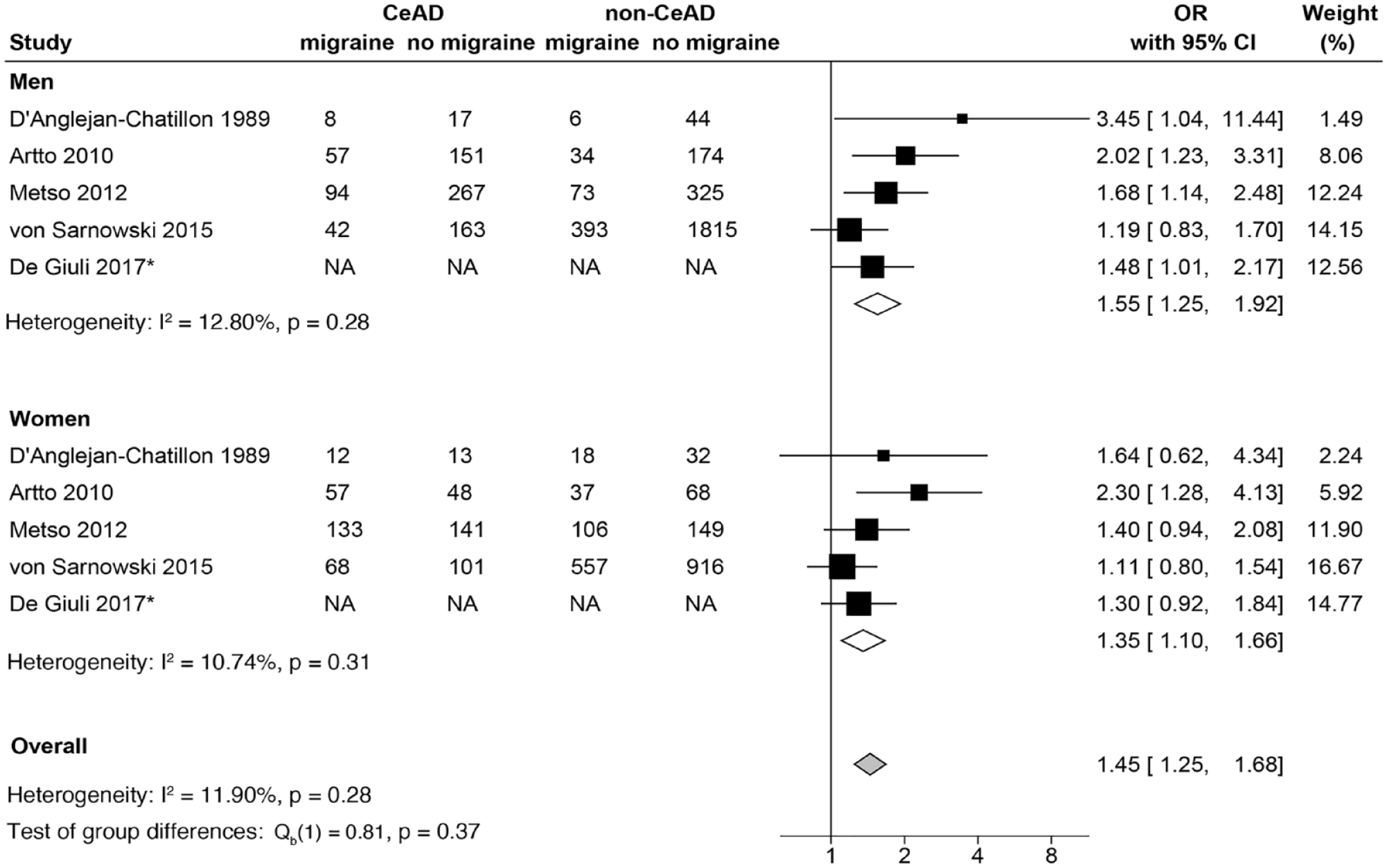
Forest plot showing the meta-analyses by men and women.
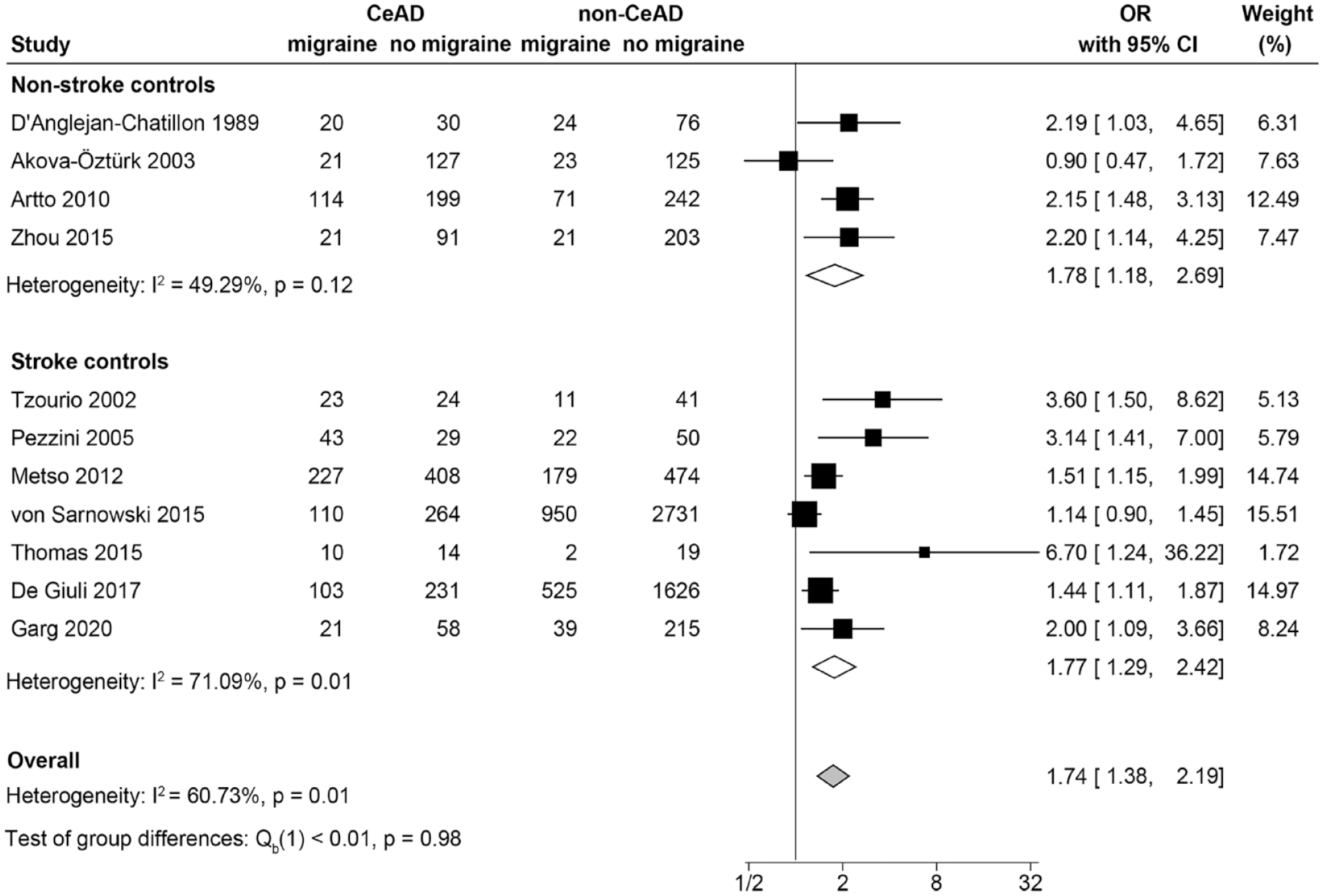
Forest plot showing the meta-analyses by control selection.
Discussion
Our meta-analysis shows that having a history of migraine is associated with 1.74-fold increased odds of CeAD. Consistent with a prior meta-analysis on migraine and CeAD, 9 this association was primarily driven by individuals with migraine without aura. In contrast, we observed no association between migraine with aura and CeAD, although significant heterogeneity between studies was observed. The finding of an association between CeAD and migraine without aura but not migraine with aura is intriguing as migraine with aura is a stronger risk factor for ischemic stroke and is therefore thought to have more shared vascular pathology. 35
The prior meta-analysis on migraine and CeAD had limited ability to explore potential effect modification by factors such as sex. Although some studies have suggested that the migraine-stroke association may be strongest among young women, 4 we observed similar associations between migraine and CeAD among both men and women. Unfortunately, we were unable to further explore whether age could modify the relationship between migraine and CeAD, because most included studies enrolled younger stroke patients with mean age ranging from 36 to 47 years old.
Both non-CeAD ischemic strokes and ischemic strokes secondary to CeAD have been associated with a history of migraine.9,35 Thus, we anticipated that using non-CeAD stroke patients as controls rather than controls derived from the healthy population, might underestimate the strength of the association between migraine and CeAD. However, subgroup analyses did not reveal any significant differences when CeAD patients were compared with individuals with no history of stroke or patients who had experienced a non-CeAD-related stroke. Limited by sample sizes, we were unable to stratify by both migraine aura status and the type of control group used. Given that there is a stronger association between migraine with aura and ischemic stroke than between migraine without aura and ischemic stroke, 36 the use of controls with a history of stroke may be one reason for the lack of association between migraine with aura and CeAD.
Recent genetic analyses have suggested that common genetic factors related to the vascular structure and function underly both migraine and CeAD. A genetic correlation study on pairwise traits identified AMAMTSL4/ECM1, PLCE1, and MRVI1 as new candidate genes implicated in the susceptibility to both migraine and CeAD. 37 The study also confirmed shared loci between migraine and CeAD at PHACTR1/EDN1, LRP1, and FHL5, which had been identified in a prior genome-wide association study on CeAD. 38 The observed genetic correlation was primarily driven by the migraine without aura subtype; however, the lack of genetic instruments for the migraine with aura subtype may have made this study underpowered to detect any correlation between migraine with aura and CeAD if it exists. Furthermore, the authors found an odds ratio of 1.69 (95%CI 1.24–2.3) for CeAD per doubling migraine prevalence using Mendelian randomization techniques. Their findings were consistent with not only our result in the primary analysis but also the differences by aura status in the subgroup analysis.
Strengths of this study include the use of three extensive databases to identify the 11 included studies. Additionally, most included studies had moderate to high quality (NOS ⩾ 4). Furthermore, we performed pre-planned subgroup analyses by aura status, sex, and the use of stroke controls to further understand the association between migraine and CeAD and potentially identify subgroups who are at most risk of CeAD. Nevertheless, several limitations remain. First, we found relevant publication bias indicating a shortage of small negative studies. However, the imputation of three studies assumed to be missing did not substantially change the pooled effect estimate. Second, the studies included in the primary analysis showed high heterogeneity (I2 = 60.73%). In addition to using the random-effects model to account for heterogeneity, we also examined heterogeneity within each subgroup to identify potential sources of heterogeneity. It is likely that the overall heterogeneity is primarily driven by the within group differences for the migraine with aura subtype and the control selections. A potential source of heterogeneity that we were unable to systematically investigate was the differences in the adjustments made for confounding among individual studies. Third, some studies asked participants to retrospectively report their migraine status, including migraine aura status, prior to the index event or study enrollment which may result in recall bias. However, this bias may not substantially affect the results since the use of stroke comparators made both cases and controls equally likely to recall migraine episodes. Fourth, studies often did not provide detailed information on how migraine aura was assessed and did not provide information on specific migraine aura features. It is possible the differences in migraine aura features or differences in the method of diagnosing migraine aura may underlie the high heterogeneity seen in this subgroup. Future studies with detailed migraine phenotype information will be needed to determine which migraine features are most likely to increase the risk of CeAD.
While we were able to perform some subgroup analyses to address specific gaps in knowledge, unanswered questions remain. For example, none of the included studies reported the frequency of migraine attacks, the severity of the headaches, details about the aura presentation, other migraine subcategories (i.e. hemiplegic migraine), or the use of preventative or abortive medications for migraine treatment. Areas of interest for future investigation would be whether the risk of CeAD or ischemic stroke is modifiable by use of preventative or abortive headache medications which decrease migraine frequency or duration of migraine attacks. Triptan use is of particular interest, since triptans have been linked to cardiovascular events and are the first line treatment for migraine headaches refractory to simple analgesics. 39 However, a large case-control study found no increase in all-cause stroke or cardiovascular death in migraine patients who were prescribed triptans compared to those who were not. 40
In conclusion, this study strengthens the evidence that history of migraine, and particularly migraine without aura, is associated with CeAD risk. Further investigations need to understand whether the use of migraine medications may modify this association, and to identify other modifiable risk factors to lower the risk of CeAD among individuals with migraine, and to explore if screening strategies may be beneficial in this population.
Supplemental Material
sj-docx-1-eso-10.1177_23969873231191860 – Supplemental material for Migraine and the risk of cervical artery dissection: A systematic review and meta-analysis
Supplemental material, sj-docx-1-eso-10.1177_23969873231191860 for Migraine and the risk of cervical artery dissection: A systematic review and meta-analysis by Zihan Sun, Julian Kleine-Borgmann, Joome Suh, Gregory C McDermott, Anastasia Vishnevetsky and Pamela M Rist in European Stroke Journal
Supplemental Material
sj-docx-2-eso-10.1177_23969873231191860 – Supplemental material for Migraine and the risk of cervical artery dissection: A systematic review and meta-analysis
Supplemental material, sj-docx-2-eso-10.1177_23969873231191860 for Migraine and the risk of cervical artery dissection: A systematic review and meta-analysis by Zihan Sun, Julian Kleine-Borgmann, Joome Suh, Gregory C McDermott, Anastasia Vishnevetsky and Pamela M Rist in European Stroke Journal
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Given that this study was a meta-analysis of previously published studies and data from those studies, we did not seek IRB approval for our analysis. The original manuscripts describe the process of obtaining patient consent.
Ethical approval
Given that this study was a meta-analysis of previously published studies and data from those studies, we did not seek IRB approval for our analysis. The original manuscripts describe the process of obtaining patient consent.
Guarantor
Dr. Kleine-Borgmann and Ms. Sun take full responsibility for the data.
Contributorship
ZS & JKB: study conception and design, data extraction and analysis, drafted the manuscript and figures; JS & GCM & AV: study conception and design, data extraction and analyses, drafted the manuscript and figures; PMR: study design; data analyses and interpretation; revision of the manuscript for intellectual content; provided supervision.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.