
Abstract
Introduction:
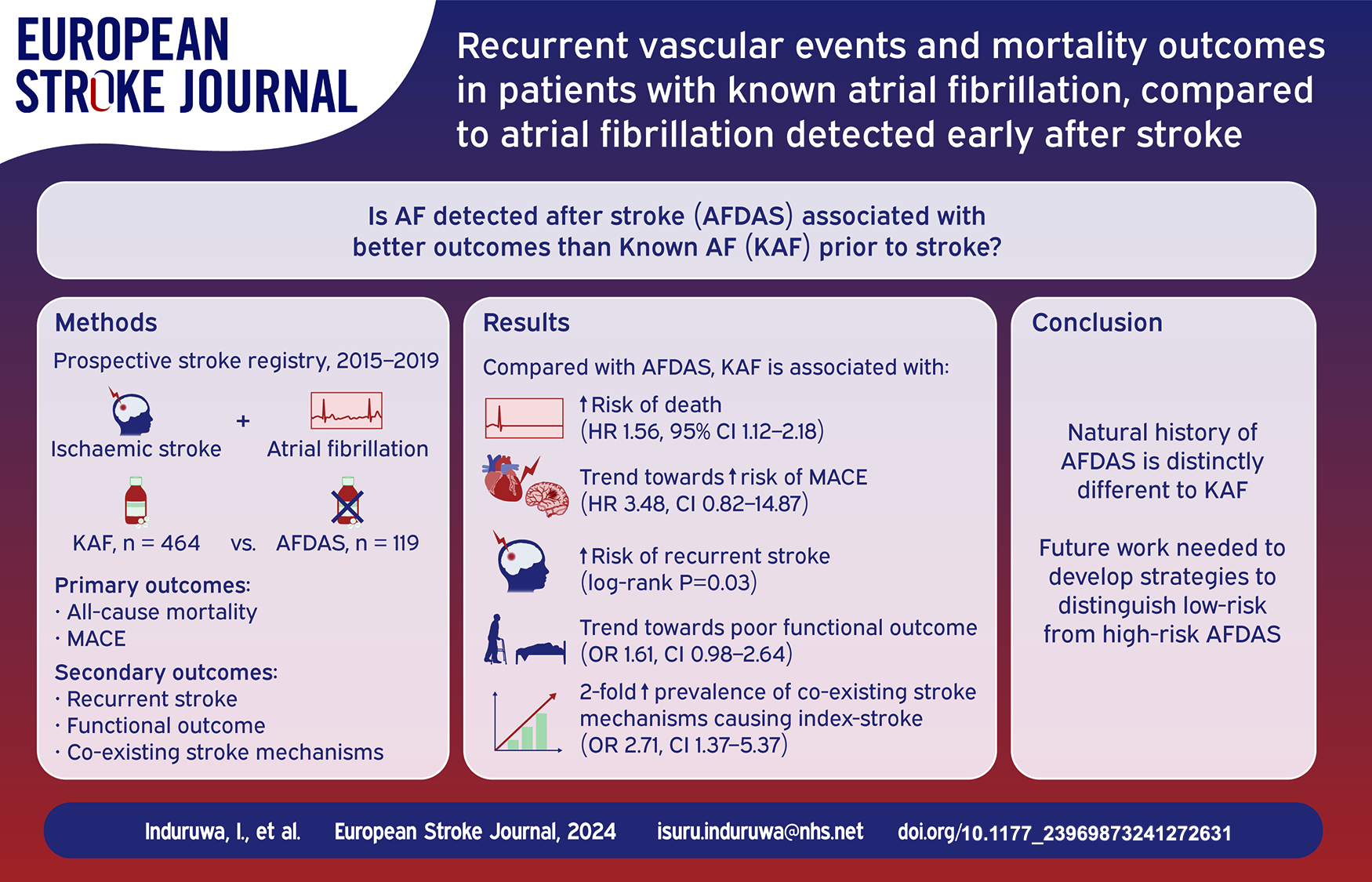
Atrial fibrillation (AF) detected after stroke (AFDAS) may represent a distinct clinical entity to that of known AF (KAF). However, there is limited long-term outcome data available for patients with AFDAS. More information regarding prognosis in AFDAS is required to inform future trial design in these patients.
Patients and methods:
We used data (2015–2019) from a national prospective stroke registry of consecutive patients with acute ischaemic stroke and AF. AFDAS was defined as a new diagnosis of AF after stroke detected on electrocardiograph or cardiac monitoring. The co-primary endpoints were: (1) all-cause mortality; (2) recurrent major adverse cardiovascular events (MACE) at 3 years. Secondary endpoints were: (1) recurrent stroke; (2) functional outcome at discharge; (3) presence of co-existing stroke mechanisms.
Results:
583 patients were included. After a median follow-up of 2.65 years (cumulative 1064 person-years) 309 patients died and 23 had recurrent MACE. Compared with AFDAS, KAF was associated with a higher risk of all-cause mortality (adjusted Hazard Ratio (aHR) 1.56, 95% CI 1.12–2.18), a higher prevalence of co-existing stroke mechanisms (adjusted odds ratio (aOR) 2.28, 95% CI 1.14–4.59), but not poor functional outcome (aOR 1.61, 95% CI 0.98–2.64). A trend towards a higher risk of MACE was observed in patients with KAF, but this was limited by statistical power (aHR 2.90, 95% CI 0.67–12.51). All 14 recurrent strokes occurred in the KAF group (Log-rank p = 0.03).
Discussion and conclusion:
These data provide further evidence that AFDAS differs to KAF with respect to risk of recurrent stroke, MACE, and all-cause mortality.
Keywords
Introduction
Atrial Fibrillation (AF) is a well-established risk factor for ischaemic stroke and is frequently first diagnosed during an admission for stroke.1,2 In the UK, approximately 19% of stroke patients have known AF (KAF) before their stroke and 6% of stroke patients have a new or first diagnosis of AF detected after stroke (AFDAS). 3 Continuous and prolonged cardiac monitoring (PCM) is increasingly used to identify patients with AF after stroke and guidelines support the use of anticoagulation for secondary stroke prevention if AF is detected. 4
However, due to the increased utilisation of both short-term and PCM for AF detection, clinicians increasingly identify brief episodes of AF after stroke, which often do not contribute to a large arrhythmia burden. There is uncertainty whether these episodes then confer the same risk of stroke recurrence and morbidity compared to patients with KAF and crucially, whether anticoagulation imparts the same net clinical benefit for stroke prevention. 5 It has been suggested that at least in some instances, AFDAS might represent a more benign form of AF, seen in patients with fewer cardiovascular risk-factors and carrying an altogether lower risk of stroke recurrence compared to KAF. 5 The STROKE-AF trial demonstrated that AF is still frequently identified in patients who have had a large artery or small vessel disease stroke. 6 Furthermore, the rates of AF detection in these patients were similar to those with cryptogenic stroke, suggesting that some cases of low-burden AF are not causally related to their index stroke. It is therefore uncertain whether stroke prevention strategies in patients with AFDAS should be different to KAF.
Recently it has been proposed that AFDAS should be classified as a separate clinical entity to KAF. 7 However, to date there have been limited data comparing late outcome recurrence and all-cause mortality in patients with AFDAS and KAF and published reports have yielded inconsistent conclusions.5,8,9 Until evidence from randomised control trials (RCTs) become available, we propose that a better understanding of the natural history of AFDAS compared to KAF is required to support clinical practice decisions and inform guideline recommendations. In this study, we investigated the prevalence of vascular risk-factors, echocardiographic parameters, and co-existing index stroke aetiologies in patients with AFDAS compared with KAF. We also investigated the risk of recurrent stroke or transient ischaemic attack (TIA), major adverse cardiovascular events (MACE) and mortality over a three-year period.
Methods
Patient selection and follow-up
The Cambridge AF Failure of Anticoagulation Study (CAFFAS) leveraged data collected in a prospective stroke registry (UK Sentinel Stroke National Audit Programme (SSNAP)) from a single comprehensive stroke centre in Cambridge UK, between October 2015 and December 2019. Consecutive patients with (1) imaging-confirmed acute ischaemic stroke; (2) new or pre-existing diagnosis of persistent, permanent, or paroxysmal AF; and (3) follow-up in Cambridge University Hospitals National Health Service (NHS) Trust were included. Exclusion criteria were: (1) intracerebral haemorrhage; (2) TIA without radiological evidence of infarction; and (3) no vascular imaging performed (computerised tomography angiography (CTA), duplex ultrasonography, or magnetic resonance angiography). Where available, echocardiograms were analysed to investigate cardiac structural parameters in AFDAS and KAF patients (see Supplemental Section for methods). To ensure complete data collection and outcome ascertainment, patients with incomplete medical records, or those originating outside the hospital Trust (where medical records could not be reliably accessed) were excluded.
For the purposes of the study, KAF was defined as patients who were known to have a diagnosis of AF (paroxysmal or permanent) prior to their admission with ischaemic stroke. AFDAS was defined as no known history of AF, with a new diagnosis made after stroke identified on electrocardiograph (ECG) or cardiac monitoring. All patients with acute stroke at this centre are admitted to the Acute Stroke Unit (ASU) and undergo telemetry for the duration of their stay on the ASU (approximately 4–7 days). Selected patients undergo PCM at the discretion of the treating clinician.
Follow up data for 3 years were collected, including recurrent major adverse cardiovascular events (MACE), functional outcome at discharge, and death. Outcome events were ascertained using multiple overlapping strategies including hospital records and general practitioner electronic medical records.
Outcomes
The co-primary endpoints were: (1) all-cause mortality at 3 years; (2) recurrent MACE at 3 years. The secondary endpoints were: (1) recurrent stroke; (2) functional outcome at discharge; (3) presence of co-existing stroke mechanisms. Recurrent stroke was defined as any recurrent TIA, ischaemic or haemorrhagic stroke. Major adverse cardiovascular events were any recurrent stroke or any major coronary event (myocardial infarction, hospitalisation for unstable angina, or sudden cardiac death) during follow-up. Poor functional outcome was defined as modified Rankin scale (mRS) of ⩾3 at discharge. In a subgroup analysis, we investigated mortality outcomes in AFDAS patients who were diagnosed with AF on the admission ECG, compared to those who were discovered to have AF during days 0–14 on telemetry (Supplemental Section).
Co-existing mechanisms for index-stroke
Stroke classification was performed by an experienced stroke specialist (JMC) blinded to anticoagulation status. A high-risk co-existing mechanism was defined as per TOAST criteria. 10 Small vessel occlusion was considered as a potential co-existing cause to AF only if there was imaging evidence of a single and clinically relevant acute infarct <15 mm in diameter within the territory of basal or brainstem penetrating arteries in the absence of any focal pathology in the parent artery. Large artery atherosclerosis was considered relevant if there was either ⩾50% stenosis or occlusion, or ⩽50% if evidence of acute thrombus or plaque rupture of the extra/intra-cranial vasculature proximal to the acute infarct.
Statistical analysis
Data was analysed using PRISM (version 9.4.1, GraphPad, USA) and Stata (version 18, StataCorp, College Station, USA) and a p-value <0.05 was considered statistically significant. Clinical characteristics were compared using t test for parametric or Mann-Whitney for non-parametric or x2 for categorical data. Continuous variables were expressed as mean (standard deviation (SD)) or median ([interquartile range (IQR)) and categorical variables as number (%). Bivariate comparisons were carried out using simple linear regression and then multiple linear regression was used to identify independent predictors in the whole population. The association between KAF and time to recurrent MACE, stroke, and all-cause mortality was evaluated using backward stepwise multivariable Cox proportional hazards regression. The proportional hazards assumption was assessed using visual inspection of Kaplan Meier curves and Schoenfeld’s test. Co-variates were included in the final model with a p < 0.10. Logistic regression was used to assess the association with poor functional outcome and death at 90 days.
Results
Baseline characteristics
We included 583 patients (AFDAS n = 119, KAF n = 464) in the final analysis and the derivation of the final cohort is demonstrated in Figure 1. Patients with AFDAS were significantly younger (median age AFDAS 82 [IQR 75–87]; KAF 85 [IQR 78–90], p = 0.01) and had a lower median CHA2DS2-VASc score (AFDAS 4 [IQR 3–5]; KAF 5 [IQR 4–6], p = 0.0004). There was a higher proportion of cardiovascular risk factors including heart failure (p = 0.02), ischaemic heart disease or vascular disease (p = 0.007), and a prior history of stroke or TIA (p = 0.007) in patients with KAF (Table 1). 49% of KAF patients were already anticoagulated at the time of their stroke and, of those alive and not discharged with palliative intention, 84.2% were on anticoagulation at discharge. By comparison 92.5% of patients with AFDAS were prescribed anticoagulation on discharge from hospital. Patients with KAF had evidence of more advanced atrial cardiopathy compared with the AFDAS group. Both left atrial area (27 cm2 [IQR 22–32] vs 21 cm2 [IQR 17–26]; p < 0.0001) and left atrial volume (50 ml/m2 [IQR 38–72] vs 41 ml/m2 [IQR 29–51); p = 0.005) were significantly increased in patients with KAF (Table 1).
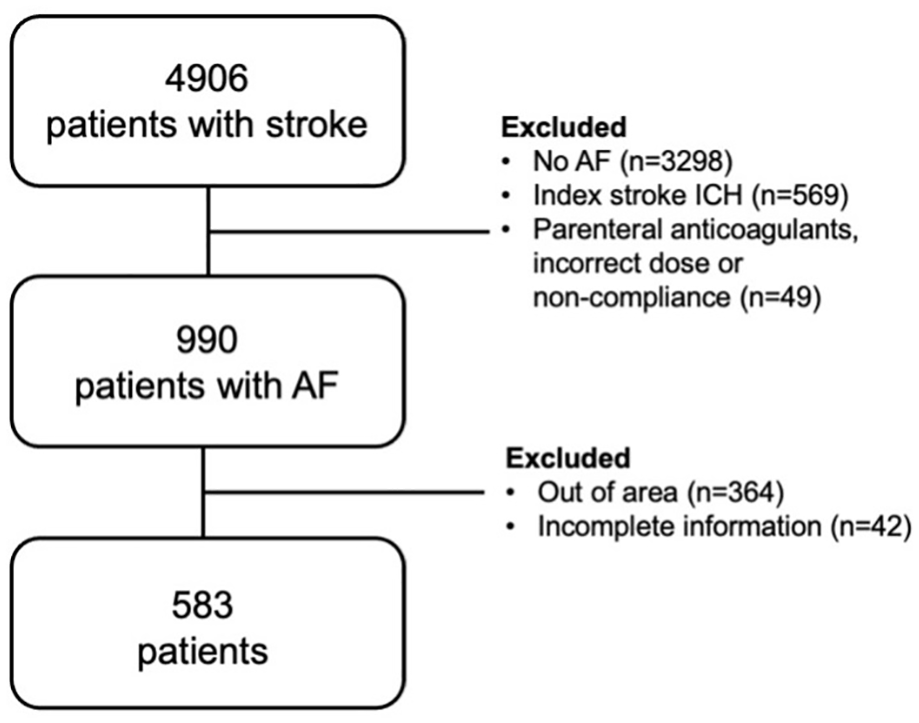
Derivation of final study cohort.
Demographic details, vascular risk-factors, echocardiogram findings, proportion of co-existing index-stroke aetiologies, recurrent vascular events and mortality data in patients with AFDAS and KAF. To assess differences between AFDAS and KAF groups, non-parametric data were analysed using Mann-Whitney U test and categorical data using x2 testing. Continuous data was expressed as median (interquartile range). Categorical data was expressed as number (%).
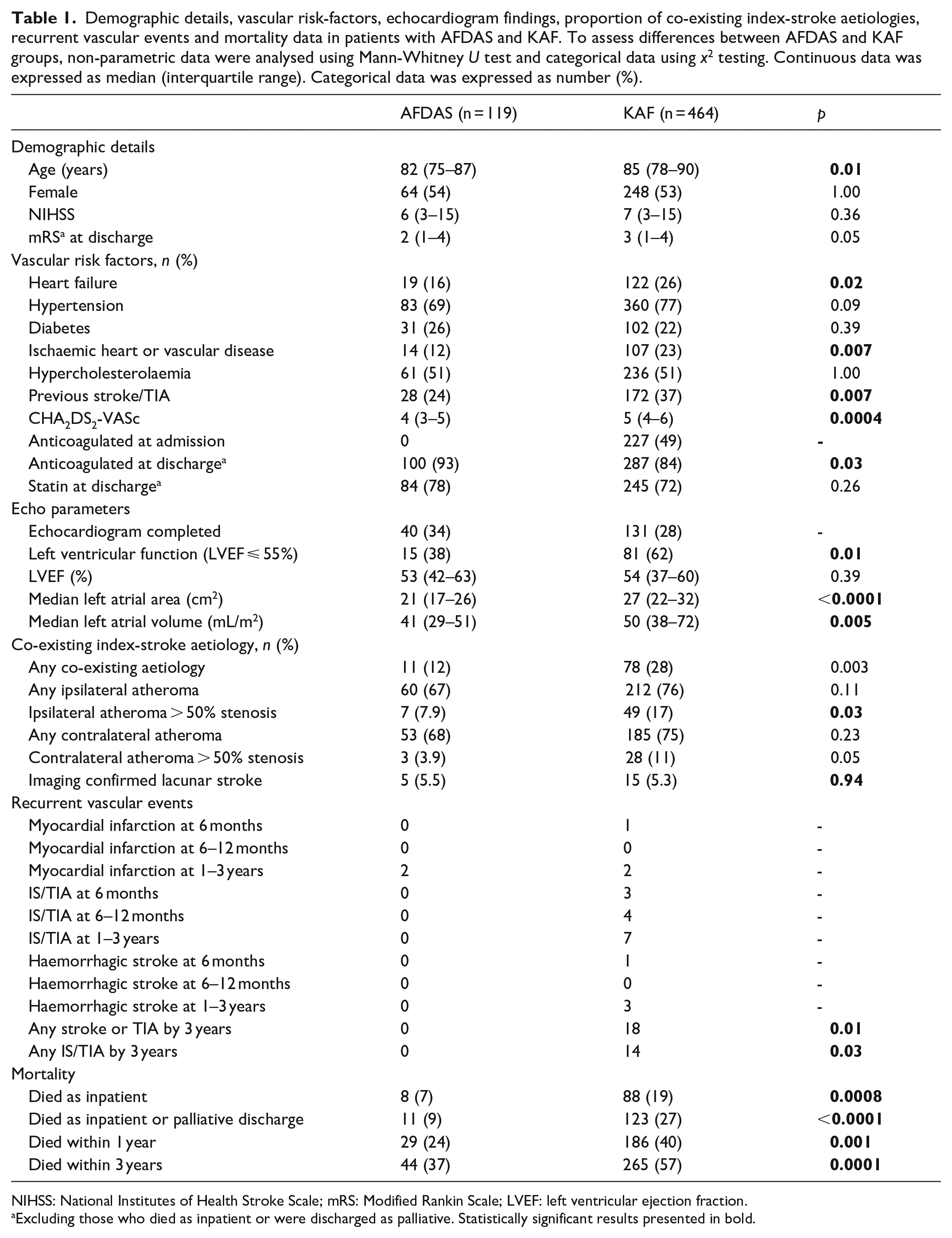
NIHSS: National Institutes of Health Stroke Scale; mRS: Modified Rankin Scale; LVEF: left ventricular ejection fraction.
Excluding those who died as inpatient or were discharged as palliative. Statistically significant results presented in bold.
Co-existing mechanisms for index stroke
A complete stroke work-up for co-existing stroke mechanisms was performed in 371 patients. Of these, there were 89 patients (24.0%) who had at least one co-existing stroke mechanism other than AF for their index stroke. There was evidence of ipsilateral large artery atherosclerosis in 56 patients (15.1%), small vessel occlusion in 20 (5.3%), an additional high-risk cardiac mechanism in 15 (4.0%), and fibromuscular dysplasia in two patients (0.5%). The presence of any co-existing stroke mechanism was almost three-times more likely in patients with KAF compared with AFDAS (Odds Ratio (OR) 2.71, 95% CI 1.37–5.37, p = 0.004). The presence of large artery atherosclerosis as a co-existing mechanism was also more common in KAF (OR 2.46, 95% CI 1.07–5.66, p = 0.03), but there was no significant association for small vessel occlusion (OR 1.19, 95% CI 0.39–3.69, p = 0.76). On stepwise backward logistic regression after adjustment for CHADS2VA2SC and history of vascular disease (ischaemic heart disease or peripheral arterial disease), patients with KAF remained at higher odds of having a co-existing stroke mechanism than patients with AFDAS (OR 2.28, 95% CI 1.14–4.59, p = 0.02). After adjustment, there was a non-significant statistical trend towards association for presence of stenosing atherosclerotic plaque with KAF (OR 2.12, 95% CI 0.91–4.95, p = 0.08) (Table 2).
Analysis for the association between co-existing stroke aetiology and AF type (AFDAS vs KAF). Effect estimates derived from logistic regression. Multivariate analysis adjusted for CHADS2VA2SC and history of vascular disease.
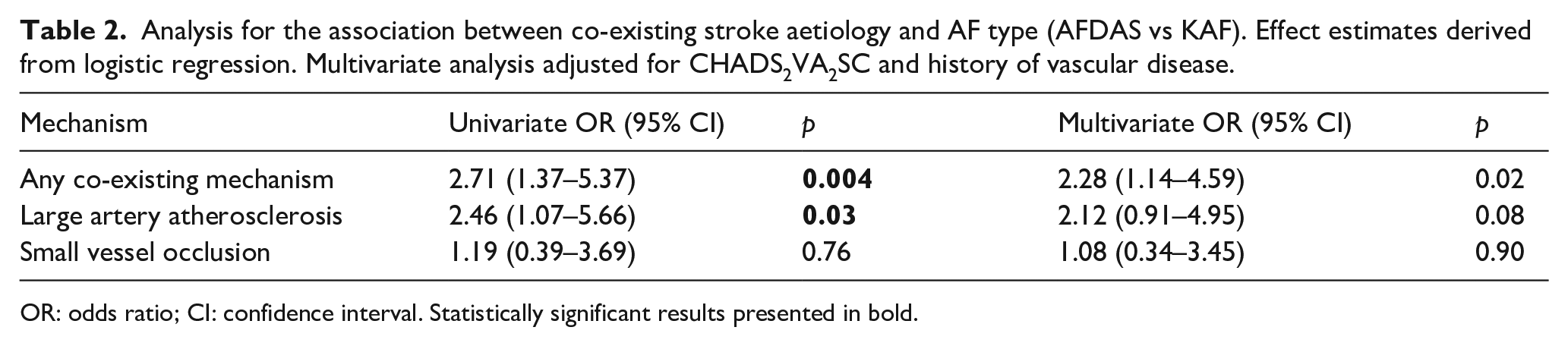
OR: odds ratio; CI: confidence interval. Statistically significant results presented in bold.
All-cause mortality
The median duration of follow-up was 2.65 years (cumulative follow-up 1064 person-years) during which time 309 (53%) patients died. A significantly higher proportion of KAF patients had died as inpatients, within the first year and within the first 3 years after their index stroke (Table 1). Ninety-one patients (15.6%) had died within 90 days of stroke. On survival analysis, patients with KAF had a higher risk of death than patients with AFDAS (log-rank test p < 0.001, Figure 2). On Cox regression analysis, KAF was associated with a higher all-cause mortality at 3-years (Figure 2; unadjusted hazard ratio (HR) 1.81, 95% CI 1.31–2.49, p < 0.001). On multivariable analysis after adjustment for age, prior vascular disease, NIHSS, and hyperlipidaemia, patients with KAF had a greater than 50% increased risk of death during follow-up (adjusted HR (aHR) 1.56, 95% CI 1.12–2.18, p = 0.009).
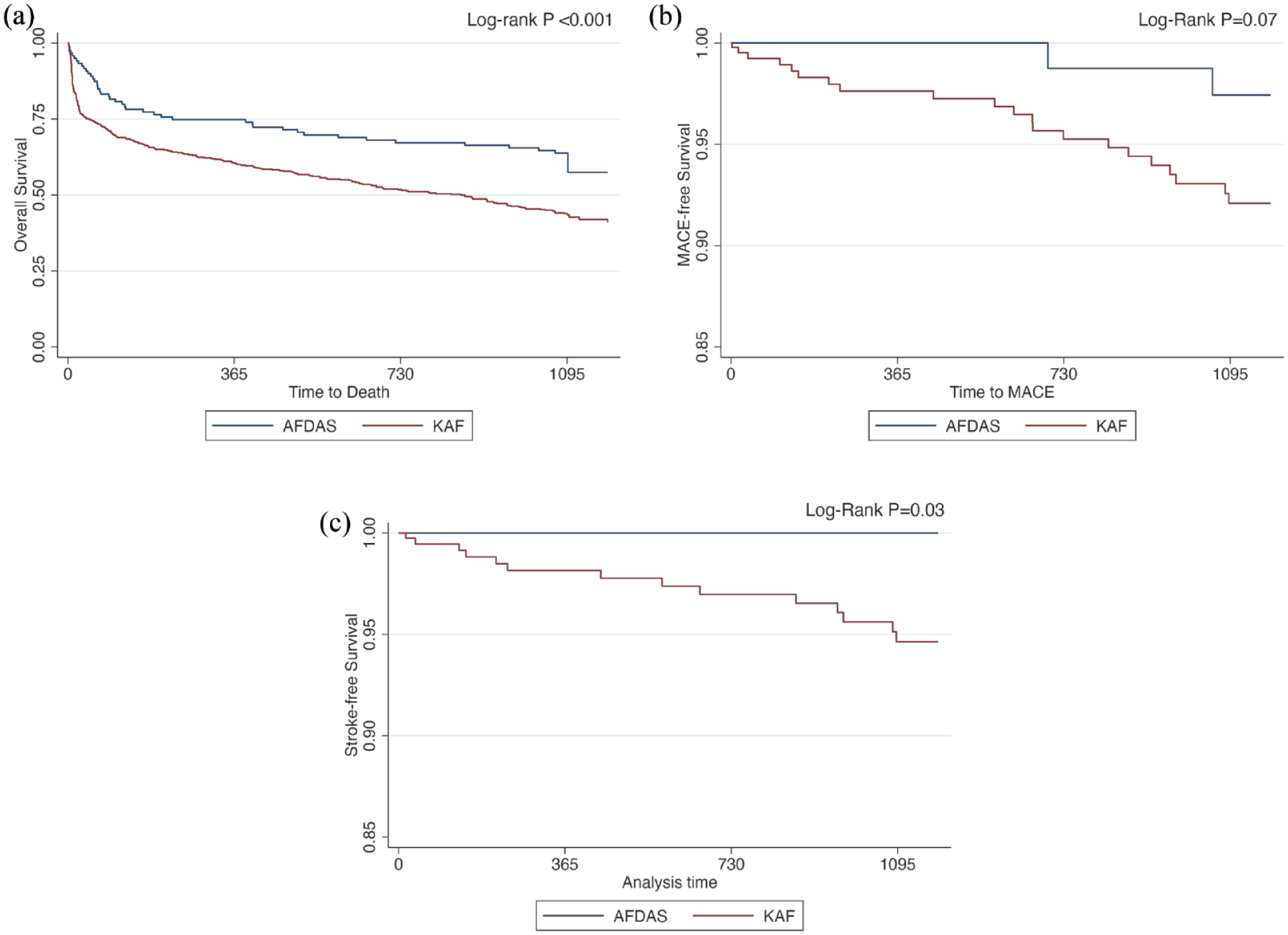
Kaplan-Meier curves for AFDAS and KAF and (a) all cause mortality, (b) recurrent MACE, and (c) recurrent stroke.
The risk of mortality at 90 days was also substantially higher in patients with KAF compared with AFDAS (odds ratio (OR) 3.25. 95% CI 1.53–6.90, p = 0.002). In the final model, this association remained significant after adjustment for age and NIHSS (OR 3.08, 95% CI 1.34–7.06, p = 0.008). Although there was also an association between KAF and mortality after hospital discharge on unadjusted analysis (HR 1.55, 95% CI 1.08–2.22, p = 0.02), this was not significant after adjustment (aHR 1.17. 95% CI 1.17, 95% CI 0.81–1.68, p = 0.40).
Recurrent vascular events
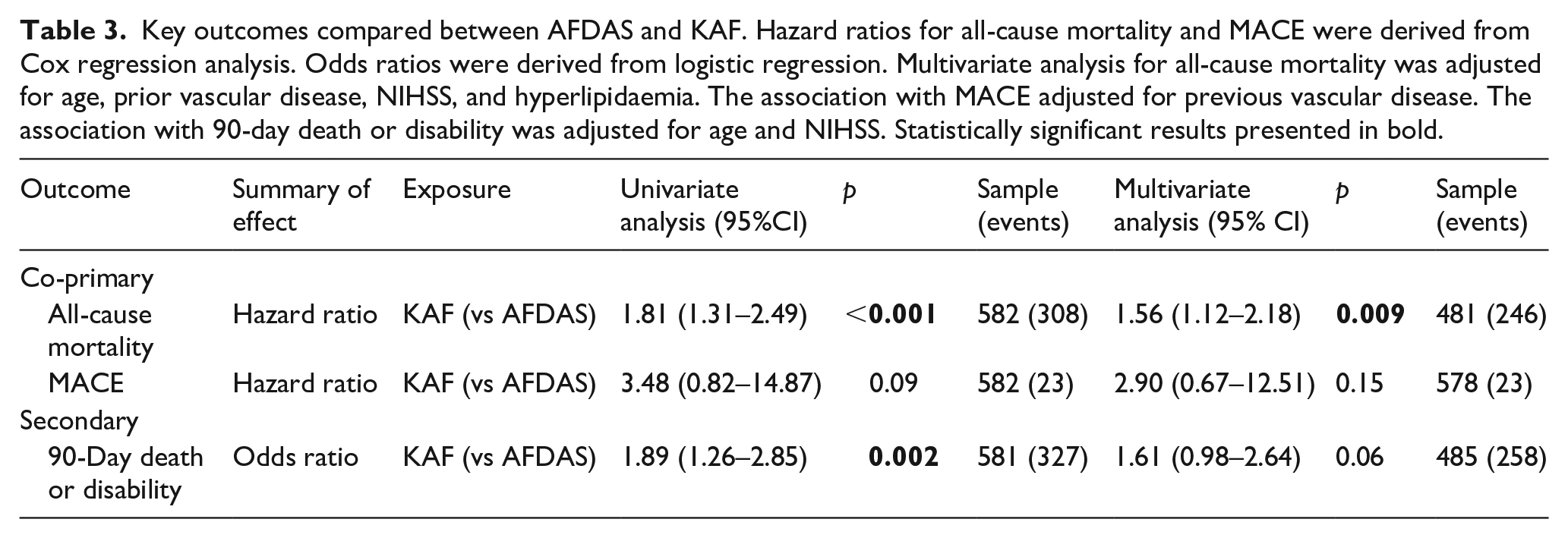
During the 3-year period of follow-up there were 14 recurrent ischaemic strokes or TIAs. All the recurrent ischaemic cerebrovascular events occurred in the KAF group (Log-rank p = 0.03, Figure 2). The aetiology of those recurrent events were cardioembolic in nine patients, small vessel occlusion in 4, and stroke due to other determined cause (vasculitis) in one case. Due to low statistical power, it was not possible to reliably estimate the coefficients for KAF and recurrent stroke using Cox regression. Of the 14 patients with recurrent stroke 11 were discharged on an anticoagulant. There were 23 patients with MACE during the 3-year follow-up period including 14 ischaemic strokes or TIAs, five major coronary events, and four intracerebral haemorrhages. Despite low statistical power there was a trend towards association with recurrent MACE for KAF compared to AFDAS (HR 3.48, 95% CI 0.82–14.87, p = 0.09), but this was not significant after adjustment for prior vascular disease (HR 2.90, 95% CI 0.67–12.51, p = 0.15) (Table 3).
Key outcomes compared between AFDAS and KAF. Hazard ratios for all-cause mortality and MACE were derived from Cox regression analysis. Odds ratios were derived from logistic regression. Multivariate analysis for all-cause mortality was adjusted for age, prior vascular disease, NIHSS, and hyperlipidaemia. The association with MACE adjusted for previous vascular disease. The association with 90-day death or disability was adjusted for age and NIHSS. Statistically significant results presented in bold.
Poor functional outcome
We observed an association between KAF and poor functional outcome at discharge. This association was present on unadjusted analysis (OR 1.90, 95% CI 1.27–2.86, p = 0.002), but was attenuated after adjustment for age and NIHSS (OR 1.61, 95% CI 0.98–2.64, p = 0.06).
Discussion
This study investigated the stroke patients with AF, and their outcomes, depending on whether they were known to have AF before their stroke, or not. The main findings of the study are that compared to KAF, patients with AFDAS identified early after stroke: (1) are younger, have a lower burden of cardiovascular risk factors, and have less severe atrial cardiopathy on echocardiography; (2) are less likely to have evidence of co-existing stroke mechanisms at the time of their stroke; (3) are at an approximately 50% lower risk of death and disability; (4) may be at a lower risk of late-outcome recurrent stroke and MACE.
Our study adds further evidence that the clinical phenotype and natural history of AFDAS differs to that of KAF. AF in patients with AFDAS is frequently of short duration, low burden, and may occasionally be due to neurogenic mechanisms secondary to insular infarction. 11 Atrial fibrillation as a chronic disease, can manifest as short, frequently subclinical, paroxysms that can increase in frequency or duration over time to become sustained. This often occurs in the context of progressive atrial dysfunction or fibrosis. 12 It is likely that AFDAS, therefore, represents an earlier disease state than KAF, leading to the uncertainty in whether anticoagulation is universally beneficial in AF. Two recent RCTs of anticoagulation in device-detected subclinical AF or atrial high-rate episodes demonstrated a reduction in stroke risk and a comparatively higher excess risk of major bleeding, 13 although these trials mostly enrolled patients without prior stroke. Despite the increasing use of PCM after stroke, there is no RCT evidence demonstrating that routine PCM reduces recurrent stroke risk 14 or that anticoagulation delivers a net clinical benefit to patients with AF detected on PCM compared with anti-platelet therapy. There is a clear and growing need to understand the clinical significance of AFDAS, to risk stratify patients into low- and high-risk groups, and for future RCTs to demonstrate benefit of anticoagulation, especially in those with low-burden AF and those with AFDAS who also have co-existing stroke mechanisms.
Our findings are similar to that observed in a recent systematic review and meta-analysis by Fridman et al. 5 which reported a higher prevalence of vascular risk factors in patients with KAF compared to AFDAS. They also noted a smaller left atrial diameter and higher left ventricular ejection fraction in patients with AFDAS, which is consistent with our observations and supports the concept that patients with KAF have a more advanced atrial cardiopathy at the time of their stroke. We also found that patients with KAF were more than twice as likely to have a co-existing mechanism for their index stroke than patients with AFDAS. This observation may be explained by a higher burden of cardiovascular risk factors in patients with KAF and may partially account for a higher risk of recurrent stroke despite anticoagulation in this group. In their meta-analysis, the risk of recurrent stroke was 26% lower in patients with AFDAS than those with KAF. 5 However, these risk estimates did not adjust for cardiovascular risk factor burden, which raises the potential for residual confounding, and the studies included had a small sample size and short follow-up duration. Although limited by a low event rate, our study provides further compelling data indicating a lower risk of recurrent stroke or TIA in patients with AFDAS compared to patients with KAF. Furthermore, our study found that a higher proportion of KAF patients died as inpatients and the likelihood of mortality was 50% higher in KAF patients within the three-year follow up period. This association was robust even after adjusting for age, stroke severity, and cardiovascular risk factors. The differences in our results could be explained by an older, more advanced population of patients included, with a longer follow up period compared to the studies carried out previously. 5
The strengths of the study are a large sample size of consecutive patients identified from a prospectively stroke registry with late-outcome follow-up for recurrent vascular events and mortality. Our results provide important and new information supporting the classification of AFDAS as distinct from KAF and our work will help inform future RCTs in these patients. We acknowledge that our work has limitations. Data were derived from a single centre so findings may not be generalisable to the broader stroke population. However, our findings were largely consistent with prior work. Although we know who was discharged on an anticoagulant and/or statin, we do not know if they were taking it at the time of their recurrent vascular event or at the time of death. Our definition of AFDAS included patients who had a new diagnosis of AF on ECG at stroke diagnosis, which differs from the recently proposed operational definition. 7 However, there is limited data supporting this updated definition and most prior work still included ECG-detected AF. Furthermore, in a subgroup analysis of our patients, we detected no significant differences in mortality between AFDAS patients where AF was diagnosed on their admission ECG at day 0, compared to those where AF was diagnosed between day 0 and 14 after stroke (Supplemental Table 1). As AFDAS in this study was almost exclusively detected on ECG or short-term cardiac monitoring in the days following stroke, our findings cannot be extended to patients with late-detected AFDAS identified months or years after stroke. We do not have information on the duration of cardiac monitoring at an individual level. It is therefore possible that some patients may have received relatively short periods of monitoring and consequently some cases of AFDAS may have been missed. There were relatively high rates of anticoagulant use in our cohort, but there were lower rates of anticoagulant use in the KAF group. We did not capture data for the reasons why anticoagulant therapy was not prescribed and acknowledge that variability in anticoagulant use may partially account for differences in outcomes between both groups. Finally, patients in this study were generally older and multi-morbid, and hence our results may not be generalisable to younger patients. However, we recruited consecutive patients at our centre and our findings are likely reflective of a growing demographic shift in AF-related stroke. It is possible that some of the differences in outcomes could be explained by frailty which was not captured in this study and should be included in future prognostic stroke research studies to improve their interpretation.
Conclusion
Our study suggests that patients with AFDAS differ to those with KAF in respect to burden of cardiovascular risk factors, severity of atrial cardiopathy, and presence of co-existing stroke mechanisms. Patients with AFDAS appear to be at lower risk of all-cause mortality and may also have a lower risk of recurrent stroke, MACE, and have better functional outcomes than patients with KAF. These data support the recently proposed concept that AFDAS represents an earlier disease state to KAF. Future research in this area is required to identify strategies to distinguish low-risk patients with AFDAS from those at high-risk, requiring well-designed prospective observational studies with long-term follow-up data and RCTs investigating the efficacy of anticoagulation in patients deemed to be low risk.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241272631 – Supplemental material for Recurrent vascular events and mortality outcomes in patients with known atrial fibrillation, compared to atrial fibrillation detected early after stroke
Supplemental material, sj-docx-1-eso-10.1177_23969873241272631 for Recurrent vascular events and mortality outcomes in patients with known atrial fibrillation, compared to atrial fibrillation detected early after stroke by Isuru Induruwa, Shiv Bhakta, Rahul Herlekar, Akangsha Sur Roy, Saur Hajiev, Elizabeth A Warburton, Kayvan Khadjooi and John J McCabe in European Stroke Journal
Footnotes
Acknowledgements
The authors acknowledge the Cambridge University Hospitals stroke research department for their contribution to data collection.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. II is now employed by Boehringer Ingelheim but was working full-time as a Clinical Lecturer at the University of Cambridge during the time this work was carried out and Boehringer Ingelheim have had no input into this work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: II’s work was funded by a NIHR Academic Clinical Lectureship (RG85316). SB is supported by a Research Training Fellowship from The Dunhill Medical Trust [JBGS22\20].
Ethical approval & informed patient
This study was registered with Cambridge University Hospitals’ Quality Surveillance Team (ID 14396). Formal confirmation was received that ethical approval from the Institutional Review Board was not required and the need to obtain written informed patient consent was therefore waived.
Guarantor
JMC
Contributorship
RH, ASR and SH collected and analysed the data. SB analysed the data and critically read the manuscript. EAW and KK critically read the manuscript. II and JMC conceptualised the study, analysed the data and wrote the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.