
Abstract
Introduction:
Whether atrial cardiopathy is associated with stroke prognosis remains unclear. We evaluated the association between atrial cardiopathy markers and outcomes in patients with ischemic stroke using a nationwide prospective registry.
Patients and methods:
Based on the Third China National Stroke Registry, we evaluated different atrial cardiopathy markers including increased P-wave terminal force in V1 (PTFV1), advanced interatrial block (aIAB), prolonged P-wave duration, prolonged P-wave dispersion, paroxysmal supraventricular tachycardia, premature atrial contractions, prolonged PR interval, and severe left atrial enlargement in ischemic stroke patients. The outcomes were death and ischemic stroke recurrence at 1 year. The association between atrial cardiopathy markers and outcomes was analyzed using Cox regression models.
Results:
At 1-year follow-up, 486 (3.4%) patients had died and 1317 (9.3%) patients had experienced ischemic stroke recurrence. After adjustment for clinical risk factors including atrial fibrillation, PTFV1 > 5000 μV·ms (adjusted hazard ratio [HR] 1.70, 95% confidence interval [CI]: 1.18–2.45, p = 0.004) and aIAB (adjusted HR 1.47, 95% CI: 1.14–1.91, p = 0.003) were significantly associated with mortality. PTFV1 > 5000 μV·ms was significantly associated with ischemic stroke recurrence (adjusted HR 1.54, 95% CI: 1.22–1.96, p = 0.0004). This association was observed although we excluded patients diagnosed with atrial fibrillation.
Discussion and Conclusion:
Atrial cardiopathy markers, especially PTFV1 and aIAB, are significantly associated with a higher risk of poor prognosis in patients with ischemic stroke.
Introduction
Stroke is a leading cause of death and disability worldwide. 1 The death rate for cerebrovascular disease in China was 149.49 per 100,000 in 2018. 2 Atrial cardiopathy refers to atrial structural and pathophysiologic changes that can occur before atrial fibrillation (AF). 3 A series of previous studies have found that atrial cardiopathy markers such as increased PTFV1, 4 aIAB, 5 prolonged P-wave duration, 4 prolonged P-wave dispersion, 6 paroxysmal supraventricular tachycardia, 7 premature atrial contractions, 8 prolonged PR interval, 9 and increased left atrial (LA) size 8 are associated with ischemic stroke in patients with or without AF. However, the relationship between atrial cardiopathy markers and stroke prognosis has not been thoroughly verified in large cohorts. Therefore, this study was conducted in a nationwide registry to explore the predictive value of atrial cardiopathy markers for prognosis in patients with ischemic stroke.
Methods
Study design
The Third China National Stroke Registry (CNSR-III) is a nationwide prospective registry for patients with ischemic stroke or transient ischemic attack (TIA) between August 2015 and March 2018. The study recruited consecutive 15,166 patients visiting 201 participating hospitals in 22 provinces and 4 municipalities in China. The patients were >18-year-old and encountered ischemic stroke or TIA within 7 days after onset of symptoms. CNSR-III was approved by the Ethics Committee of Beijing Tiantan Hospital (institutional review board approval number: KY2015-001-01) and all participating hospitals. Informed consent was obtained from all patients or their legally authorized representatives. The details of CNSR-III have been published previously. 10
Atrial cardiopathy markers
A standard 12-lead ECG was recorded for each patient at a speed of 25 mm/s and a calibration of 10 mm/mV at the time of admission. All ECGs were digitalized. ECG image was amplified by up to five times its original size. P-wave indices were measured using digital calipers by a well-trained cardiologist who was blinded to the clinical data of patients. All measurements were repeated three times, and the average values were obtained. P-wave duration was measured from P-wave onset to return to baseline. For biphasic P wave, P-wave duration encompassed both positive and negative deflections from baseline. P-wave duration was measured in all 12 leads to acquire the maximum and minimum durations. P-wave dispersion was defined as the difference between the maximum and minimum P-wave durations. aIAB was identified as the presence of prolonged P-wave duration and biphasic (positive negative) morphology in leads II, III, and aVF or biphasic (positive negative) morphology in leads III and aVF and notched P (positive positive) in lead II. 5 PTFV1 was defined as the duration (ms) of the downward deflection (terminal portion) of P wave in lead V1 multiplied by the absolute value of its amplitude (μV). PR interval was defined as the interval from the onset of P wave to the end of PR segment (junction with the QRS complex). Previous studies have shown excellent intrarater correlations for manual measurements of P-wave morphology. 11 A second well-trained cardiologist independently performed blinded measurements of a random sample of 200 ECGs to assess the interrater reliability of P-wave indices measurements. The interrater intraclass correlation coefficient (ICC) was 0.67 (95% CI 0.59–0.74) for maximum P-wave duration, 0.73 (95% CI 0.65–0.79) for P-wave dispersion, and 0.78 (95% CI 0.67–0.85) for PTFV1.
Atrial cardiopathy markers were defined according to the previous studies. Prolonged P-wave duration was determined as being present if the maximum P-wave duration was >120 ms. 4 Prolonged P-wave dispersion was defined as >40 ms. 12 Increased PTFV1 was defined as >5000 μV·ms. 13 Prolonged PR interval was defined as >200 ms. 14 LA enlargement was measured as anterior-posterior linear LA diameter (mm) on a baseline 2D echocardiogram (UCG), with severe enlargement defined using sex-specific cut-offs (⩾47 mm for women and ⩾52 mm for men). 15 Atrial ectopy and paroxysmal supraventricular tachycardia were measured on the baseline 24-h Holter. Excessive atrial ectopy was defined as a frequency of atrial premature beats per hour of >30. 8
Outcomes and follow-up
In this study, the outcomes included all-cause mortality and ischemic stroke recurrence at 1 year. Patients were followed up at 3 months, 6 months, and 1 year after onset. Patients were interviewed face-to-face at 3 months and contacted over the telephone by trained research coordinators at 6 months and 1 year. Confirmation of cerebrovascular events were sought from the treating hospital, and suspected recurrent cerebrovascular events without hospitalization were judged by independent endpoint judgment committee. Each case fatality was either confirmed on a death certificate from the attended hospital or the local citizen registry. Details of the determination of outcome events have been published in previous study. 10
Statistical analysis
Continuous variables were presented as means with standard deviations or medians with interquartile ranges. Statistical comparisons were performed with one-way analysis of variance or the Kruskal–Wallis test. Categorical variables were presented as frequencies with percentages and were compared by χ 2 test. The risks of outcomes were evaluated by Kaplan–Meier survival analysis and the significance of differences was evaluated using the log-rank test. Multivariable Cox regressions were used to determine significant predictors of outcomes. In multivariable Cox regressions, we excluded the patients without complete marker data, respectively. The receiver-operator curve (ROC) with area under curve was calculated to evaluate improvement in risk classification by atrial cardiopathy markers over iScore and Essen Stroke Risk Score. In the sensitivity analysis, we excluded patients diagnosed with AF. We also tested the association between atrial cardiopathy markers and vascular mortality at 1 year as a sensitivity analysis. All tests were two-sided. A p < 0.05 was considered statistically significant. All analyses were conducted with SAS software, version 9.4 (SAS Institute, Inc, Cary, NC).
Results
Baseline characteristics
Between August 2015 and March 2018, 15,166 patients with acute ischemic stroke or TIA were recruited for the CNSR-III study. After excluding patients with TIA, 14,146 ischemic stroke patients (mean age, 62.3 years; median National Institutes of Health Stroke Scale (NIHSS) score, three [interquartile range, 2–6]) were finally included in this analysis. Of these patients, 68.7% were men. Among 14,146 ischemic stroke patients, besides patients with a medical history of AF, some patients were newly detected with AF during hospitalization. After excluding patients both with known and newly detected AF, 13,015 patients were included. At 1-year follow-up, 486 (3.4%) patients had died, and 1317 (9.3%) patients had experienced ischemic stroke recurrence. The baseline characteristics of patients are summarized in Table 1 and Supplemental Table 1. All atrial cardiopathy markers, except prolonged P-wave dispersion (p = 0.06), were more frequent in patients who had succumbed during the 1-year period. Patients with ischemic stroke recurrence had a significantly higher frequency of PTFV1 > 5000 μV·ms, aIAB, prolonged PR interval, and severe LA enlargement than patients without. Among 14,146 ischemic stroke patients, the proportion of patients who underwent ECG, UCG, and 24-h Holter was 94.1%, 94.3%, and 82.3%, respectively. The median timing of ECG, UCG, and Holter with respect to the index stroke was 1, 3, and 4.8 days, respectively. The baseline characteristics of patients with and without cardiac examination variables were presented in Supplemental Table 2–4, respectively. Baseline characteristics between two groups were largely comparable.
Characteristics of patients with or without death and ischemic stroke recurrence.
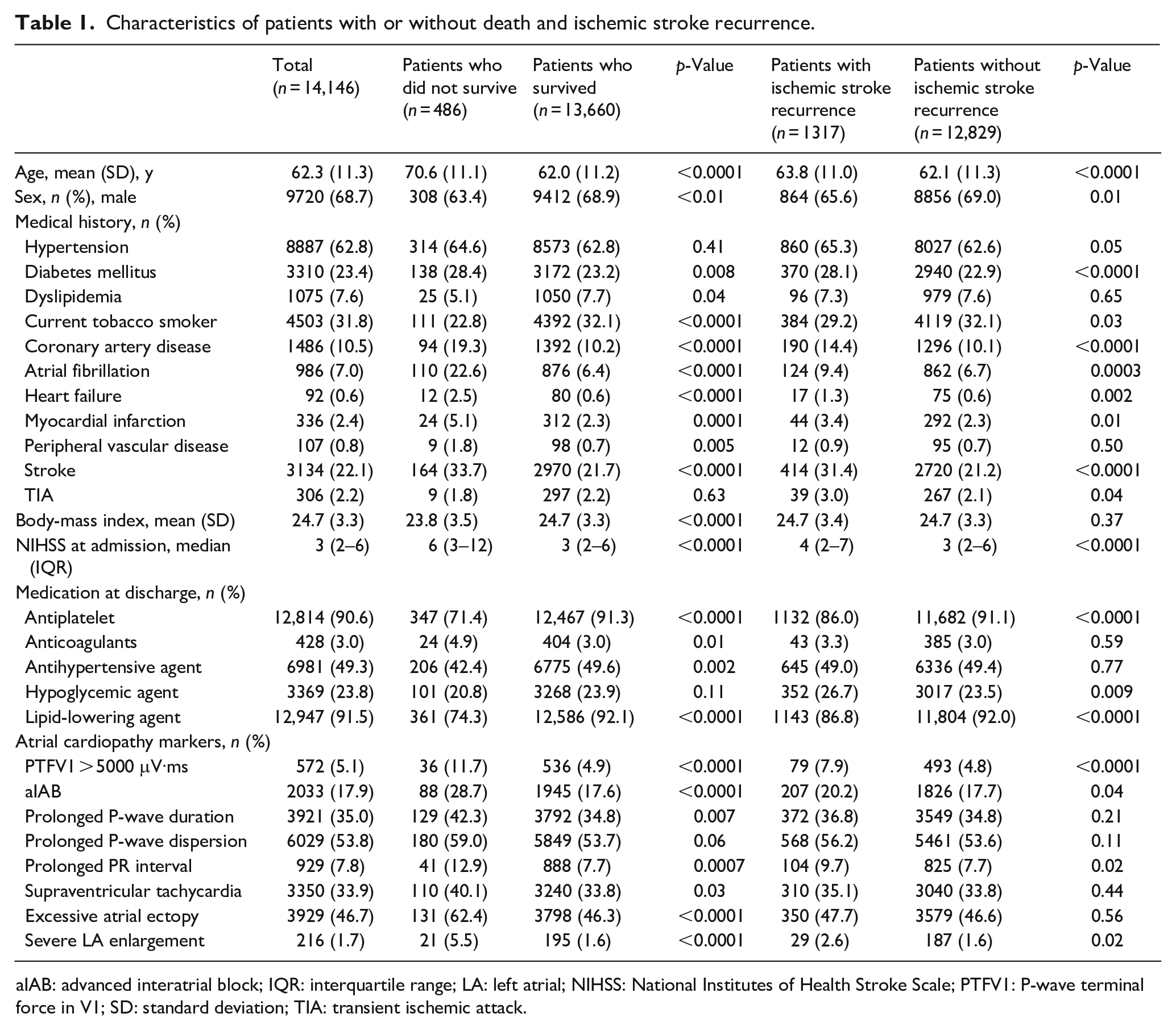
aIAB: advanced interatrial block; IQR: interquartile range; LA: left atrial; NIHSS: National Institutes of Health Stroke Scale; PTFV1: P-wave terminal force in V1; SD: standard deviation; TIA: transient ischemic attack.
Associations of atrial cardiopathy markers with mortality
In multivariable models, PTFV1 > 5000 μV·ms (adjusted HR 1.70, 95% CI: 1.18–2.45, p = 0.004) and aIAB (adjusted HR 1.47, 95% CI: 1.14–1.91, p = 0.003) were significantly associated with mortality (Table 2). The association was true after we excluded patients diagnosed with AF; PTFV1 > 5000 μV·ms (adjusted HR 1.77, 95% CI: 1.21–2.59, p = 0.003) and aIAB (adjusted HR 1.43, 95% CI: 1.09–1.88, p = 0.009) still exhibited significant associations with mortality (Table 2). Kaplan–Meier survival curves demonstrated that the cumulative incidence of mortality was highest in patients with both markers (log-rank test, p < 0.01; Figure 1).
Risk of death for atrial cardiopathy markers.
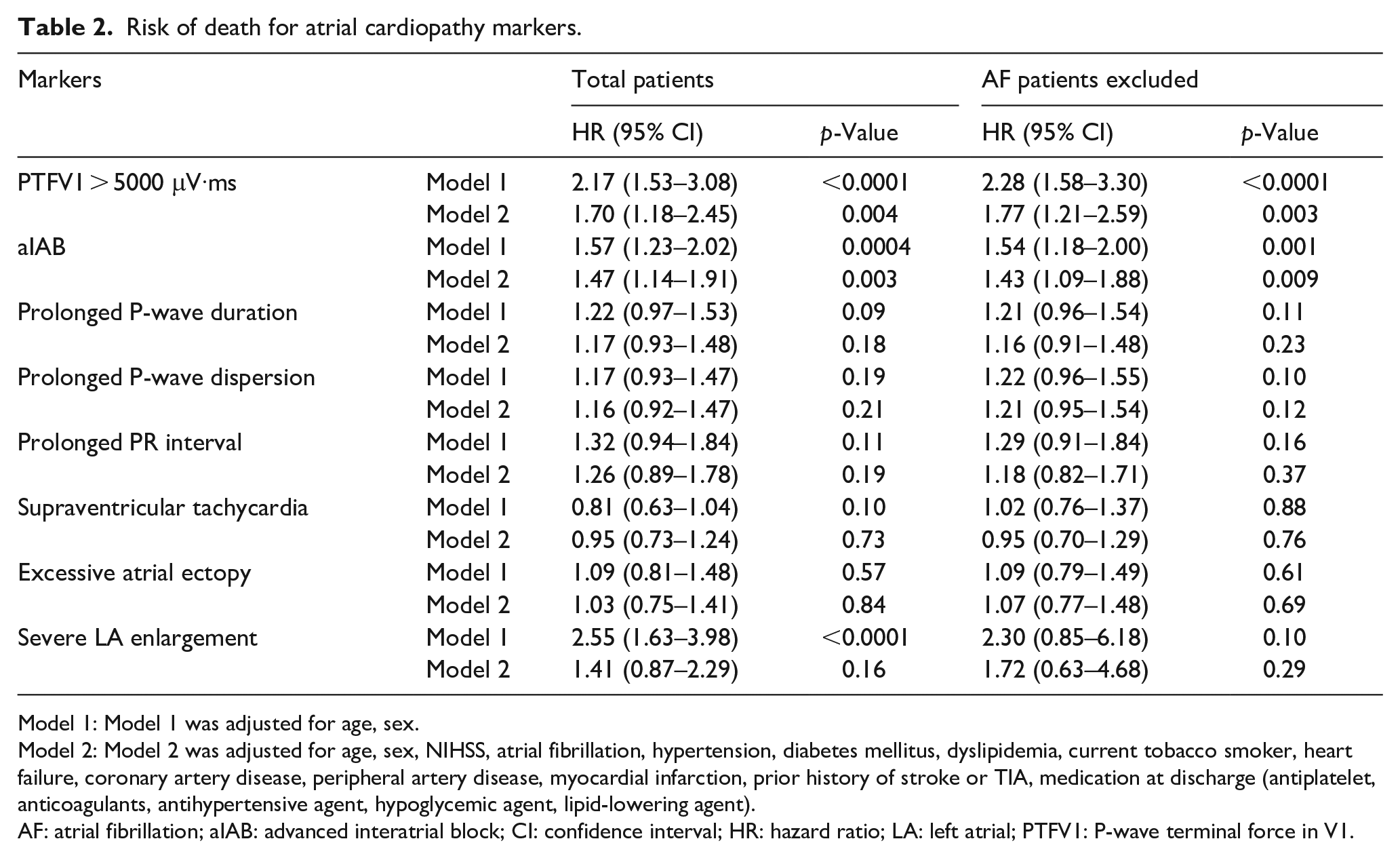
Model 1: Model 1 was adjusted for age, sex.
Model 2: Model 2 was adjusted for age, sex, NIHSS, atrial fibrillation, hypertension, diabetes mellitus, dyslipidemia, current tobacco smoker, heart failure, coronary artery disease, peripheral artery disease, myocardial infarction, prior history of stroke or TIA, medication at discharge (antiplatelet, anticoagulants, antihypertensive agent, hypoglycemic agent, lipid-lowering agent).
AF: atrial fibrillation; aIAB: advanced interatrial block; CI: confidence interval; HR: hazard ratio; LA: left atrial; PTFV1: P-wave terminal force in V1.
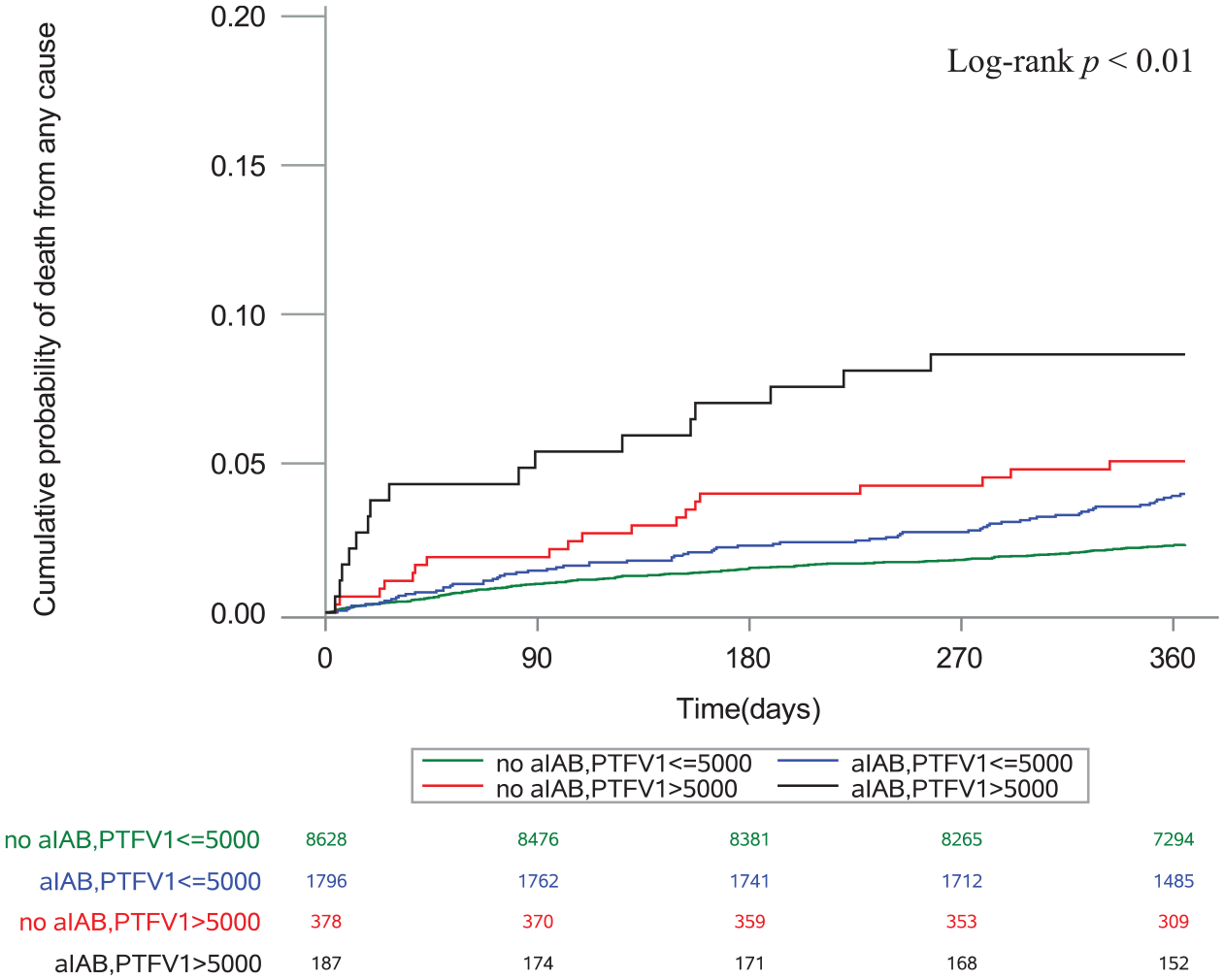
Cumulative probability of death stratified by aIAB and PTFV1.
The multivariable model showed a trend that PTFV1 > 5000 μV·ms increased the risk of vascular mortality in ischemic stroke patients (adjusted HR 1.71, 95% CI: 0.95–3.09, p = 0.07), although there is no statistical significance. After we excluded patients diagnosed with AF. PTFV1 > 5000 μV·ms was the only marker associated with vascular mortality (adjusted HR 2.03, 95% CI: 1.13–3.66, p = 0.02; Supplemental Table 5, Supplemental Figure 1).
Associations of atrial cardiopathy markers with ischemic stroke recurrence
In the multivariable models, PTFV1 > 5000 μV·ms was the only marker associated with ischemic stroke recurrence (adjusted HR 1.54, 95% CI: 1.22–1.96, p = 0.0004; Table 3). After excluding patients diagnosed with AF, PTFV1 > 5000 μV·ms still exhibited a significant association with ischemic stroke recurrence (adjusted HR 1.62, 95% CI: 1.27–2.07, p = 0.0001; Table 3). The Kaplan–Meier survival curves depicted that the cumulative incidence of ischemic stroke recurrence was significantly higher in patients with increased PTFV1 than in those without increased PTFV1 (log-rank test, p < 0.01; Figure 2).
Risk of ischemic stroke recurrence for atrial cardiopathy markers.
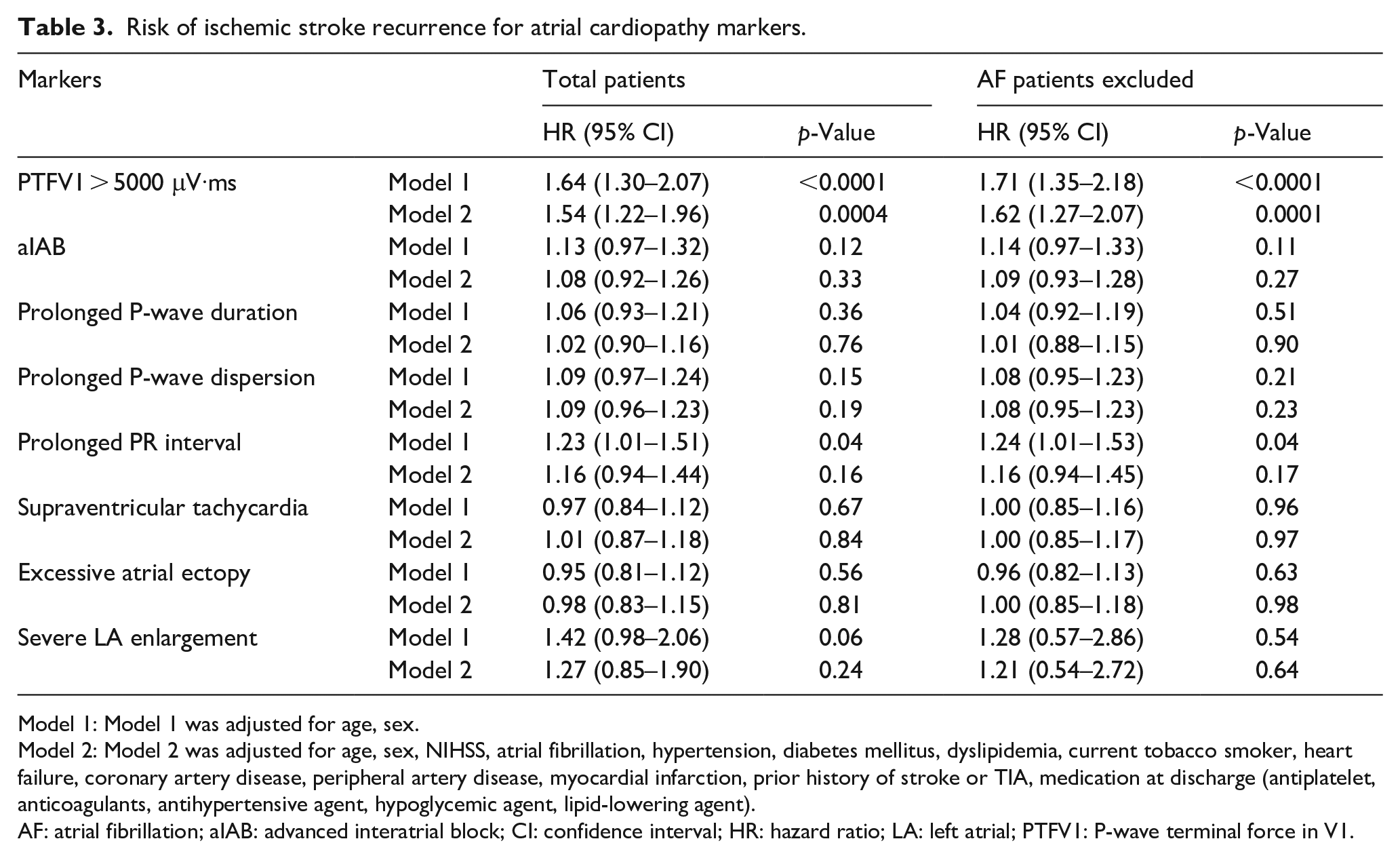
Model 1: Model 1 was adjusted for age, sex.
Model 2: Model 2 was adjusted for age, sex, NIHSS, atrial fibrillation, hypertension, diabetes mellitus, dyslipidemia, current tobacco smoker, heart failure, coronary artery disease, peripheral artery disease, myocardial infarction, prior history of stroke or TIA, medication at discharge (antiplatelet, anticoagulants, antihypertensive agent, hypoglycemic agent, lipid-lowering agent).
AF: atrial fibrillation; aIAB: advanced interatrial block; CI: confidence interval; HR: hazard ratio; LA: left atrial; PTFV1: P-wave terminal force in V1.
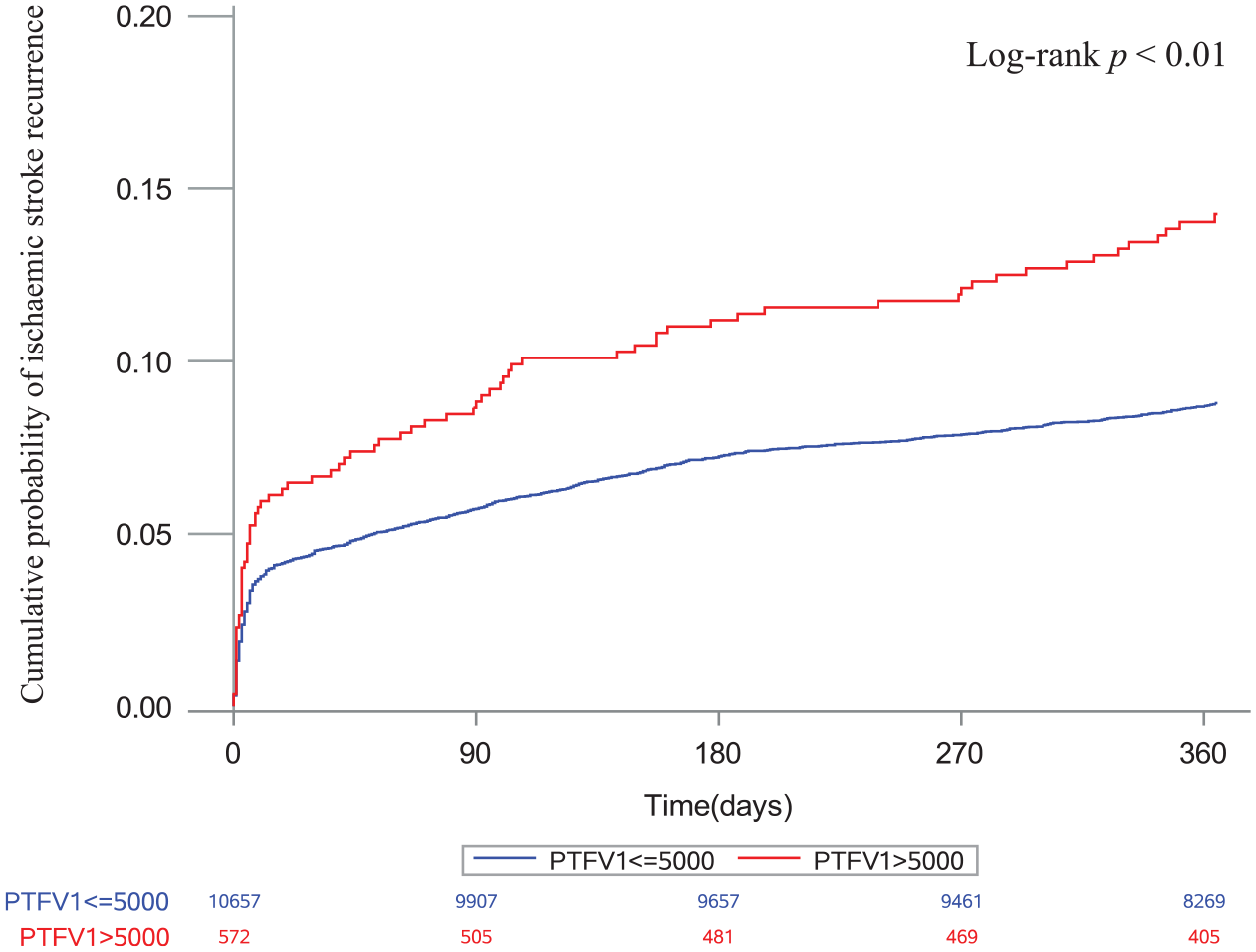
Cumulative probability of ischemic stroke recurrence stratified by PTFV1.
Improvement in prediction model for mortality and ischemic stroke recurrence by addition of atrial cardiopathy markers
We established the performance of iScore for predicting mortality and Essen Stroke Risk Score for predicting ischemic stroke recurrence at 1 year. Adding PTFV1 and aIAB slightly increased the area under the ROC for iScore (0.013, p = 0.02) (Supplemental Table 6). Besides, adding PTFV1 slightly increased the area under the ROC for Essen Stroke Risk Score (0.008, p = 0.04) (Supplemental Table 6).
Discussion
Fibrotic atrial remodeling and enlargement are crucial components of the prothrombotic and proarrhythmic substrates in the development of LA thromboembolism. The measurement of P-wave indices generates the basis for the ECG-based detection of the substrate. PTFV1 and aIAB are both markers of atrial fibrosis and LA abnormalities.3,16 In this study, we found that PTFV1 was a predictor of death and ischemic stroke recurrence in patients with ischemic stroke. In addition, aIAB was associated with a higher risk of death after ischemic stroke.
In several different longitudinal cohorts, PTFV1 has been related to incident stroke in populations free of stroke or AF at baseline, and the associations remain constant even after adjusting for incident AF.4,11,17 –19 The relationship of increased PTFV1 with a new stroke occurring in patients without AF further supports the hypothesis that the increased risk of stroke may be mediated via atrial cardiopathy, independent of the effects of AF. 3 PTFV1 may reflect atrial changes, such as LA hypertrophy and inter-atrial conduction defects, 20 and its increase has been associated with impaired LA function.21,22 Furthermore, PTFV1 has been associated with low LA appendage ejection velocity on transoesophageal echocardiography. 23 The Cardiovascular Health Study reported PTFV1 to be associated with prevalent magnetic resonance imaging (MRI)-defined infarcts, especially nonlacunar infarcts. 24 The results suggest that PTFV1 may reflect a thromboembolic mechanism that induces ischemic stroke.
Recent work has confirmed an association between abnormal PTFV1 and left ventricular fibrosis on cardiac MRI. 21 In addition, PTFV1 may be an early manifestation of left ventricular diastolic dysfunction 25 which is an independent predictor of mortality. 26 In the general population, PTFV1 is also associated with sudden cardiac death, cardiovascular death, 27 and all-cause death 28 independent of clinical cardiovascular risk factors.
Patients with aIAB present low atrial mobility and reduced strain as assessed by speckle-tracking echocardiography. 29 Furthermore, aIAB has been reported to be associated with larger LA volumes, lower LA emptying fraction, and increased fibrosis on MRI. 30 There is growing evidence that aIAB is a powerful marker of increased risk of a poor prognosis in different clinical groups, such as the general population, 5 and patients with heart failure, 31 acute myocardial infarction, 32 stress cardiomyopathy, 33 and ischemic stroke. 34 The results indicate that electrocardiographic abnormalities as markers of changes in the cardiac structure and function are effective predictors of poor prognosis.
This study has several limitations. First, as we excluded some patients without complete markers, potential biases may exist in our study. However, the characteristics of patients with and without complete cardiac examination variables were well balanced. Second, All-cause mortality was lower in our study because patients in CNSR-III were younger and had relatively mild stroke severity. This could have the tendency to underestimate the magnitude of associations between atrial cardiopathy markers and mortality. Finally, this study relied on manual measurements rather than automated measurements. However, blinded measurements were performed by two independent investigators to confirm the objectivity of the results.
Conclusions
In conclusion, this study revealed the effect of PTFV1 and aIAB on the prognosis of ischemic stroke. Clinicians should apply these easily accessible markers to help the risk classification and more well-designed clinical studies are needed to explore optimal strategies for stroke patients with these atrial cardiopathy markers.
Supplemental Material
sj-docx-1-eso-10.1177_23969873221126000 – Supplemental material for Prognostic significance of atrial cardiopathy in patients with acute ischemic stroke
Supplemental material, sj-docx-1-eso-10.1177_23969873221126000 for Prognostic significance of atrial cardiopathy in patients with acute ischemic stroke by Yueyang Wu, Xiaomeng Yang, Jing Jing, Xia Meng, Zixiao Li, Yuesong Pan, Yong Jiang, Hongyi Yan, Xinying Huang, Liping Liu, Xingquan Zhao, Yilong Wang, Hao Li and Yongjun Wang in European Stroke Journal
Footnotes
Acknowledgements
The authors thank the staff and participants of the CNSR-III study for their contribution.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Capital’s Funds for Health Improvement and Research (grant number: 2020-1-2041), Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (grant number: 2019-I2M-5-029), and National Natural Science Foundation of China (grant number: 81870905, U20A20358, 82001237).
Ethical approval
CNSR-III was approved by the Ethics Committee of Beijing Tiantan Hospital (institutional review board approval number: KY2015-001-01) and all participating hospitals.
Informed consent
Informed consent was obtained from all patients or their legally authorized representatives.
Guarantor
YW
Contributorship
All authors were involved in the design and planning of the work. YP, YJ, HY, and XH performed data analysis. YW and XY wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.