
Abstract
Background:
Atrial fibrillation (AF) detected after stroke or transient ischemic attack (AFDAS) is a critical but often underdiagnosed condition with implications for secondary stroke prevention. This distinctive type of AF is increasingly studied to provide a more comprehensive understanding of its complex pathophysiology, which may involve both cardiogenic mechanisms and stroke-induced autonomic dysfunction, a concept known as the neurogenic hypothesis. This study aims to identify the prevalence and predictors of AFDAS to help refine monitoring strategies and improve patient outcomes.
Methods:
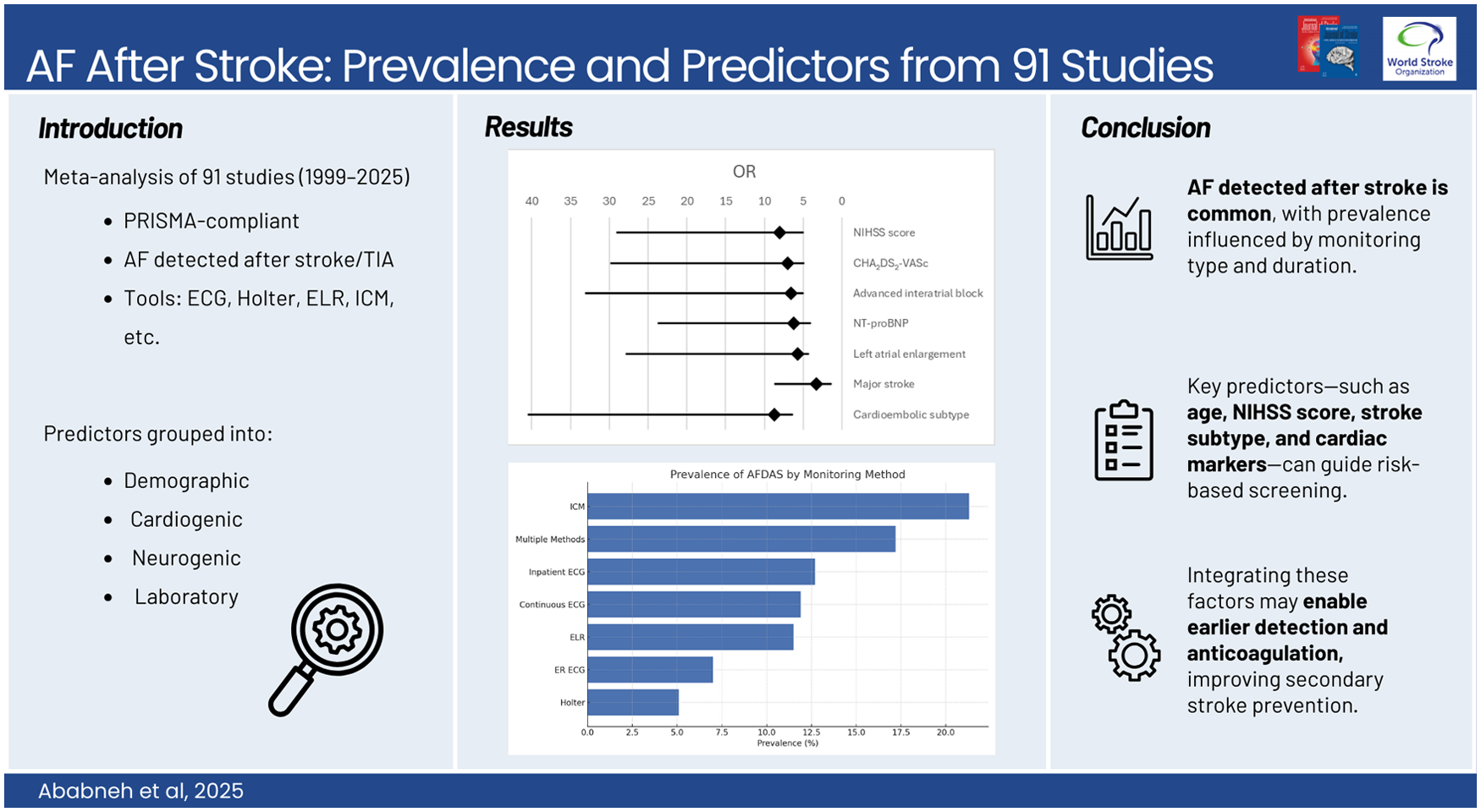
We conducted a systematic review and meta-analysis following Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. We included English-language retrospective and prospective cohort studies published from January 1999 to January 2025, analyzing data from 91 studies for prevalence and 54 studies for predictors. We categorized AF detection by different monitoring methods, including electrocardiogram (ECG), Holter monitoring, external loop recorders, and implantable cardiac monitors (ICM). Predictors were grouped into demographic, cardiogenic, neurogenic, and laboratory factors.
Results:
The overall prevalence of AFDAS varied significantly based on monitoring technique. The pooled prevalence was 7% (95% CI 4.6–10.5) by emergency room ECG, 12.7% (95% CI 9–17.8) by inpatient ECG, 11.9% (95% CI 7.8–17.9) by continuous ECG monitoring, 11.5% (95% CI 8–16.1) by external loop recording, 5.1% (95% CI 2.6–9.7) by Holter monitor, 21.3% (95% CI 18.3–24.7) by ICM, and 17.2% (95% CI 10–28.1) by multiple monitoring methods. Key predictors of AFDAS included older age, female sex, hypertension, chronic kidney disease, left atrial enlargement, advanced interatrial block, and higher NIHSS scores. Insular involvement and major strokes were strongly associated with AF detection, supporting the neurogenic hypothesis. Elevated N-terminal pro-B-type Natriuretic Peptide (NT-proBNP) and B-type Natriuretic Peptide (BNP) levels were also linked to a higher AF risk.
Conclusion:
AFDAS is a frequent but variably detected condition, with its prevalence strongly dependent on monitoring duration and modality. Identifying high-risk patients using a combination of clinical, cardiogenic, neurogenic, and laboratory markers can optimize screening strategies and early anticoagulation initiation, potentially reducing stroke recurrence. Future research should focus on refining risk scores integrating neurogenic and cardiogenic markers to guide personalized monitoring approaches and to define the distinct characteristics of AFDAS from known atrial fibrillation (KAF).
Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.