General Interest Session - Official welcome & Large Clinical Trials
Abstract N°: 2151
Category: 1.01 ACUTE MANAGEMENT - Neither thrombolysis nor thrombectomy
REMOTE ISCHEMIC PERCONDITIONING AMONG ACUTE ISCHEMIC STROKE PATIENTS IN CATALONIA: REMOTE-CAT PROJECT
Francisco Purroy*1,2,3, Gerard Mauri Capdevila1,3, Teresa Subirats4, Francesc Xavier Jiménez4, Mikel Vicente-Pascual5, Pere Cardona6, Andres Paipa6, Manuel Gomez-Choco7, Marián Muchada8, Gloria Arque2,3
1Hospital Universitari Arnau de Vilanova de Lleida, Neurology, Lleida, Spain, 2Universitat de Lleida - UdL, Lleida, Spain, 3Institut de Recerca Biomèdica de Lleida Fundació Dr. Pifarré, Lleida, Spain, 4Servei Emergencies Mediques, 5Hospital Sant Pau i Santa Tecla, Tarragona, Spain, 6Bellvitge University Hospital, L'Hospitalet de Llobregat, Spain, 7Hospital de Sant Joan Despí Moisès Broggi, Sant Joan Despí, Spain, 8Vall d'Hebron University Hospital, Barcelona, Spain
On behalf of: REMOTECAT trial: A Freixa, Y. Gallego, A. Garcia, C. Garcia, M. Gil, C. Gonzalez, P. Miriam, C. Pereira, A. Quilez, E. Ruiz, I. Saldaña, J. Sanahuja, A. Sancho, E. San Pedro, D. Vazquez, A. Garcia, JM Ropero, F. Castellvi, A. Rovira, J Pagola
Background and aims: Remote ischemic perconditioning during cerebral ischemia (RIPerC) refers to the application of brief episodes of transient limb ischemia, commonly to a limb. It represents a new, safe, simple, and low-cost paradigm in neuroprotection, demonstrated in preclinical models and some clinical stroke trials.
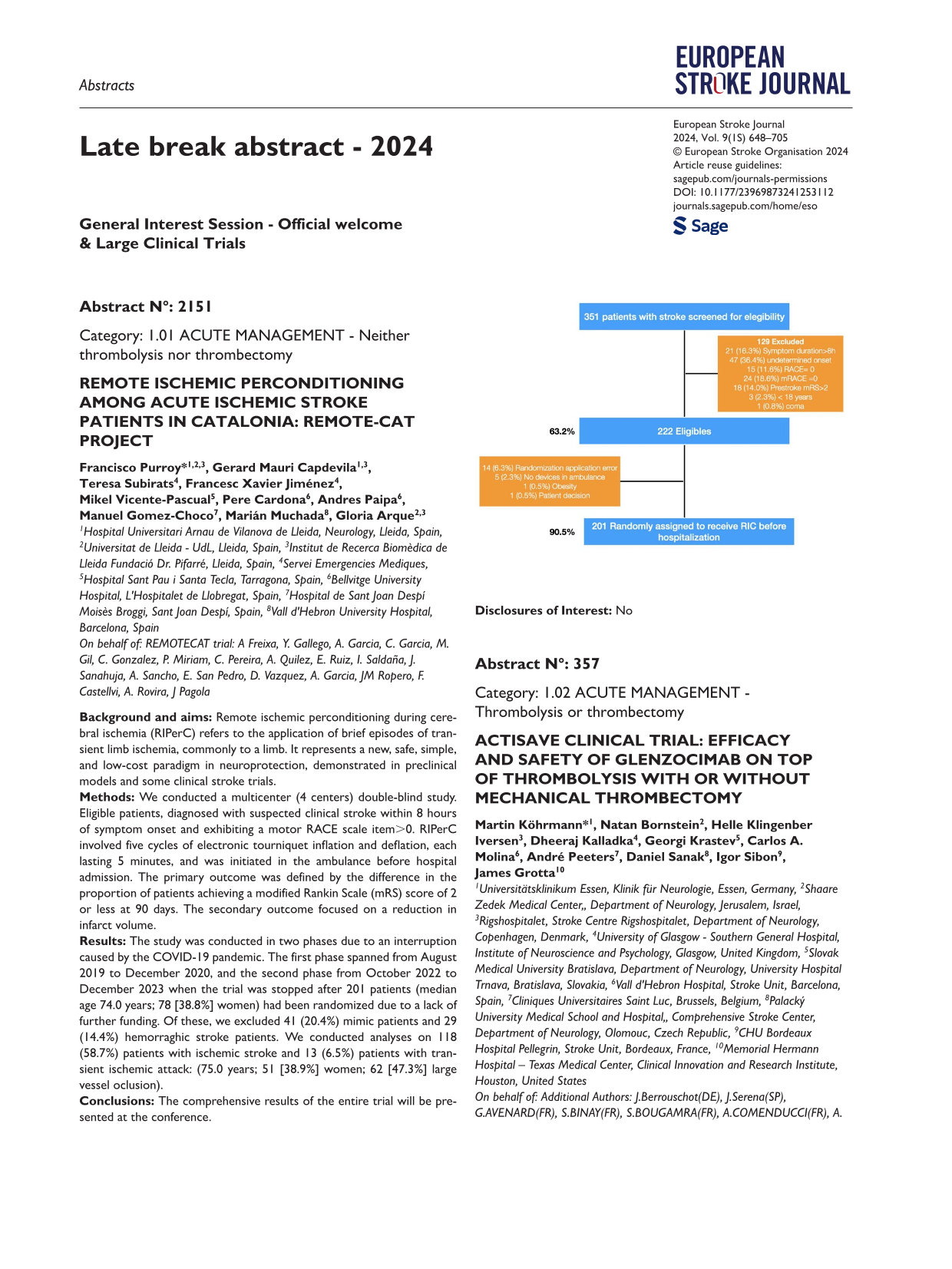
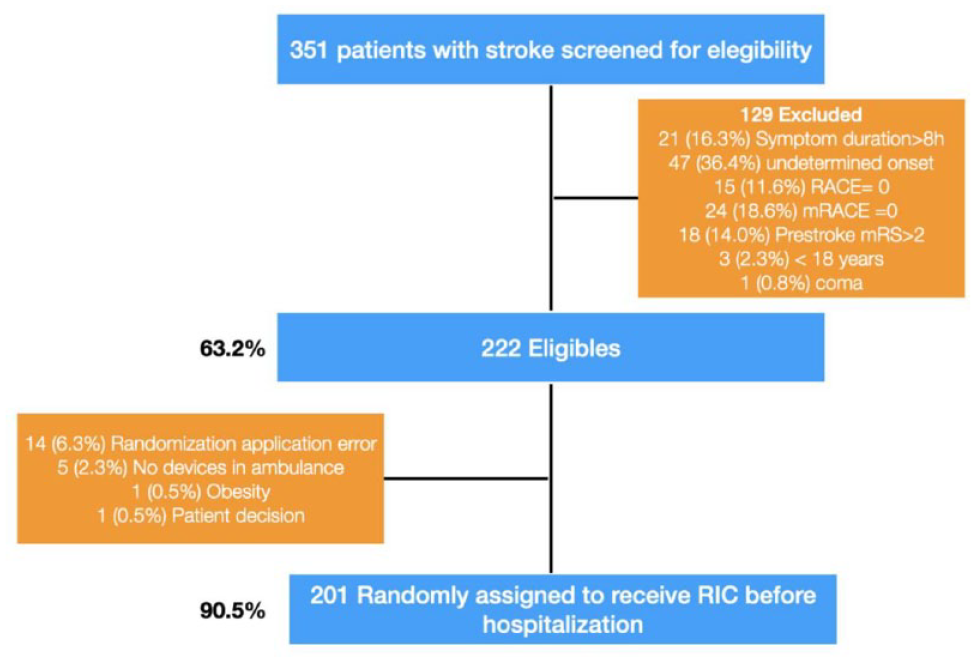
Methods: We conducted a multicenter (4 centers) double-blind study. Eligible patients, diagnosed with suspected clinical stroke within 8 hours of symptom onset and exhibiting a motor RACE scale item>0. RIPerC involved five cycles of electronic tourniquet inflation and deflation, each lasting 5 minutes, and was initiated in the ambulance before hospital admission. The primary outcome was defined by the difference in the proportion of patients achieving a modified Rankin Scale (mRS) score of 2 or less at 90 days. The secondary outcome focused on a reduction in infarct volume.
Results: The study was conducted in two phases due to an interruption caused by the COVID-19 pandemic. The first phase spanned from August 2019 to December 2020, and the second phase from October 2022 to December 2023 when the trial was stopped after 201 patients (median age 74.0 years; 78 [38.8%] women) had been randomized due to a lack of further funding. Of these, we excluded 41 (20.4%) mimic patients and 29 (14.4%) hemorraghic stroke patients. We conducted analyses on 118 (58.7%) patients with ischemic stroke and 13 (6.5%) patients with transient ischemic attack: (75.0 years; 51 [38.9%] women; 62 [47.3%] large vessel oclusion).
Conclusions: The comprehensive results of the entire trial will be presented at the conference.
Disclosures of Interest: No
Abstract N°: 357
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
ACTISAVE CLINICAL TRIAL: EFFICACY AND SAFETY OF GLENZOCIMAB ON TOP OF THROMBOLYSIS WITH OR WITHOUT MECHANICAL THROMBECTOMY
Martin Köhrmann*1, Natan Bornstein2, Helle Klingenber Iversen3, Dheeraj Kalladka4, Georgi Krastev5, Carlos A. Molina6, André Peeters7, Daniel Sanak8, Igor Sibon9, James Grotta10
1Universitätsklinikum Essen, Klinik für Neurologie, Essen, Germany, 2Shaare Zedek Medical Center,, Department of Neurology, Jerusalem, Israel, 3Rigshospitalet, Stroke Centre Rigshospitalet, Department of Neurology, Copenhagen, Denmark, 4University of Glasgow - Southern General Hospital, Institute of Neuroscience and Psychology, Glasgow, United Kingdom, 5Slovak Medical University Bratislava, Department of Neurology, University Hospital Trnava, Bratislava, Slovakia, 6Vall d'Hebron Hospital, Stroke Unit, Barcelona, Spain, 7Cliniques Universitaires Saint Luc, Brussels, Belgium, 8Palacký University Medical School and Hospital,, Comprehensive Stroke Center, Department of Neurology, Olomouc, Czech Republic, 9CHU Bordeaux Hospital Pellegrin, Stroke Unit, Bordeaux, France, 10Memorial Hermann Hospital – Texas Medical Center, Clinical Innovation and Research Institute, Houston, United States
On behalf of: Additional Authors: J.Berrouschot(DE), J.Serena(SP),G.AVENARD(FR), S.BINAY(FR), S.BOUGAMRA(FR), A.COMENDUCCI(FR), A. MEILHOC(FR), Y. Pletan(FR), E.Toledano(FR), J.Grouin(FR) on behalf of ACTISAVE Study Group
Background and aims: Glenzocimab, a monoclonal antibody fragment targeting platelet glycoprotein VI, inhibiting platelet activation and aggregation, was evaluated in ACTISAVE study (NCT05070260) for the treatment of Acute Ischemic Stroke (AIS). Previously, ACTIMIS clinical trial (NCT03803007) established the safety of glenzocimab in AIS patients, on top of thrombolysis with or without mechanical thrombectomy. Results from ACTIMIS also showed a decrease in IntraCranial Hemorrhages and mortality. ACTISAVE was a second independent confirmatory trial.
Methods: ACTISAVE is a multicenter, randomized, double-blind, placebo-controlled, parallel-group, adaptive phase 2/3 study in AIS patients, treated by thrombolysis within 4.5 hours of symptoms onset with or without mechanical thrombectomy. Patients were randomized in a 1:1 ratio and treated by an IV dose of glenzocimab (1000 mg) or placebo.
The primary outcome was the modified Rankin Scale (mRS) score of [4-6] at day-90. The key secondary outcome was mRS [0-2] at day-90. Mortality, mRS shift, NIHSS score, and quality of life were assessed. Safety outcomes, particularly intracranial hemorrhages, were included.
Results: Overall, 438 patients were randomized (September 2021 - October 2023) in 70 primary and comprehensive stroke centers in Belgium, Czech Republic, Denmark, France, Germany, Israel, Slovakia, Spain, United Kingdom, and USA. Of them, 421 were treated.
Median age [Q1-Q3] was 73 [63-80] with a gender-ratio (F/M) of (43/57%); 72% of patients were aged ⩾65 years, including 27% ⩾80 years. Of all patients treated with thrombolysis, 36% also underwent mechanical thrombectomy. Pre-thrombolysis NIHSS median [Q1-Q3] was 9 [6–15].
Conclusions: Results of ACTISAVE clinical trial will be presented at ESOC 2024.
Disclosures of Interest: ACTISAVE Study was sponsored by Acticor Biotech; MK and JCG were international coordinators of the study. JB, JS, NMB, HKI, DK, GK, CAM, AP, DS, IS were investigators of the study
Abstract N°: 4248
Category: 1.01 ACUTE MANAGEMENT - Neither thrombolysis nor thrombectomy
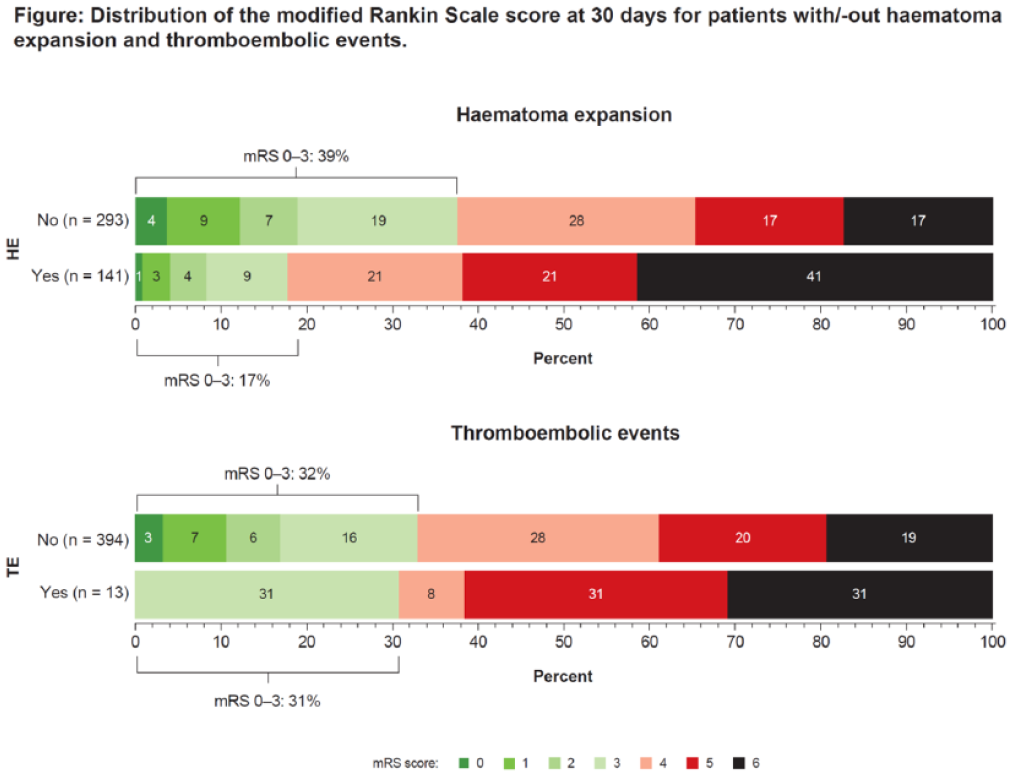
CLINICAL CONSEQUENCES OF HAEMATOMA EXPANSION AND THROMBOEMBOLIC EVENTS IN PATIENTS WITH FACTOR XA-INHIBITOR ASSOCIATED ICH IN ANNEXA-I
David Seiffge*1, Else Charlotte Sandset2, Ashkan Shoamanesh3,4, Mukul Sharma3,4, Lizhen Xu3, Magnus Andersson5, Per Ladenvall5, Stuart Connolly3
1Inselspital, Neurology, Bern, Switzerland, 2Oslo University hospital Ullevål, Neurology, Norway, 3PHRI, Hamilton, Canada, 4McMaster University, Neurology, Hamilton, Canada, 5AstraZeneca AB R&D, Gothenburg, Sweden
On behalf of: ANNEXa-I publication committee
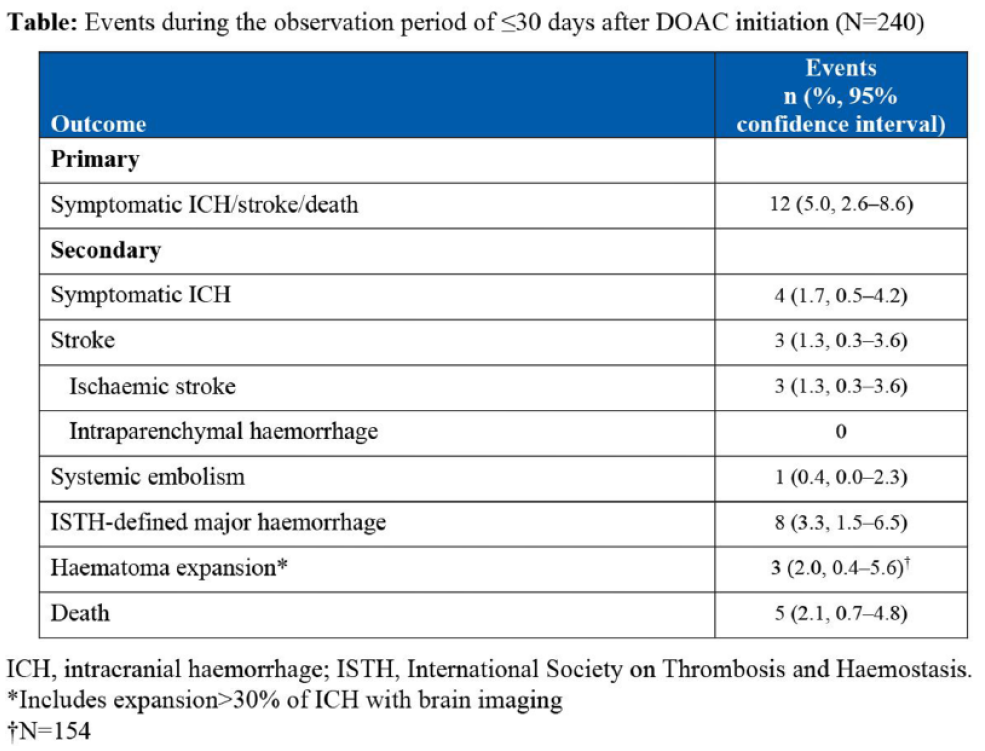
Background and aims: The ANNEXA-I trial reported lower rates of haematoma expansion and higher rates of thrombotic events with andexanet in patients with intracranial hemorrhage on factor Xa-inhibitors. We evaluated the clinical consequences of both outcomes.
Methods: Using patients with intracerebral haemorrhage in both treatment arms, we assessed the association of haematoma expansion and thrombotic events with mortality at 30 days using multivariate model that did not include treatment allocation. Thrombotic events were included as time-dependant co-variable. To assess modified Rankin Score (mRS) at 30 days, we performed a landmark analysis starting at day 5.
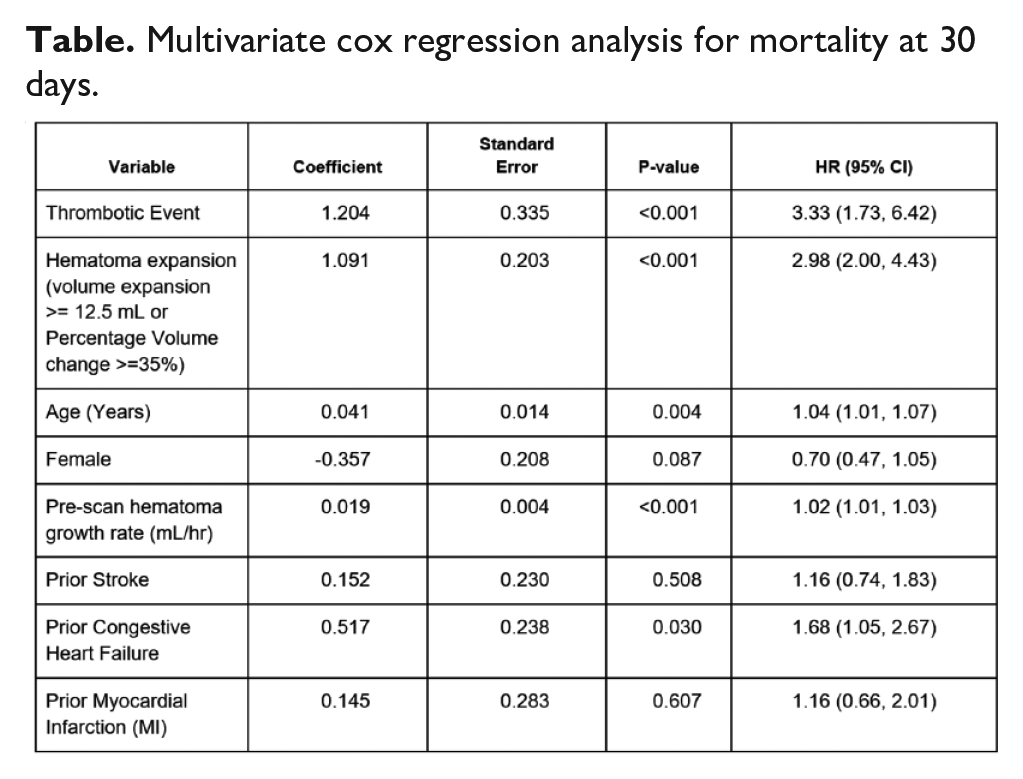
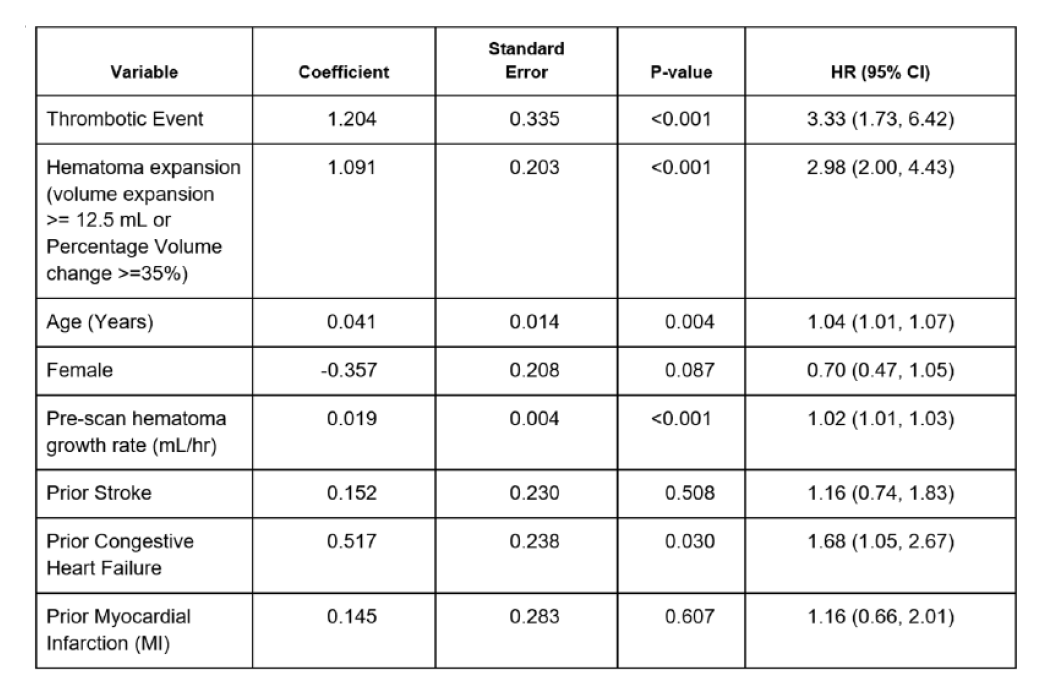
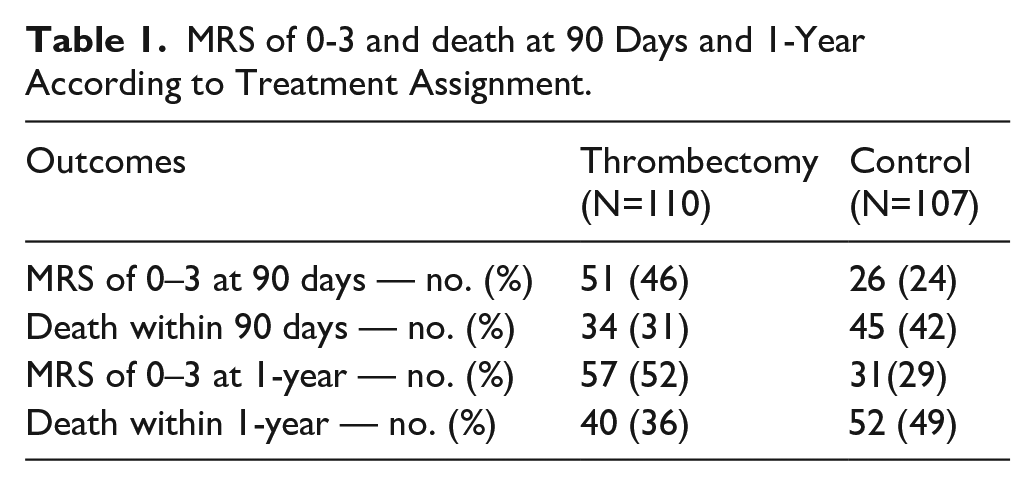
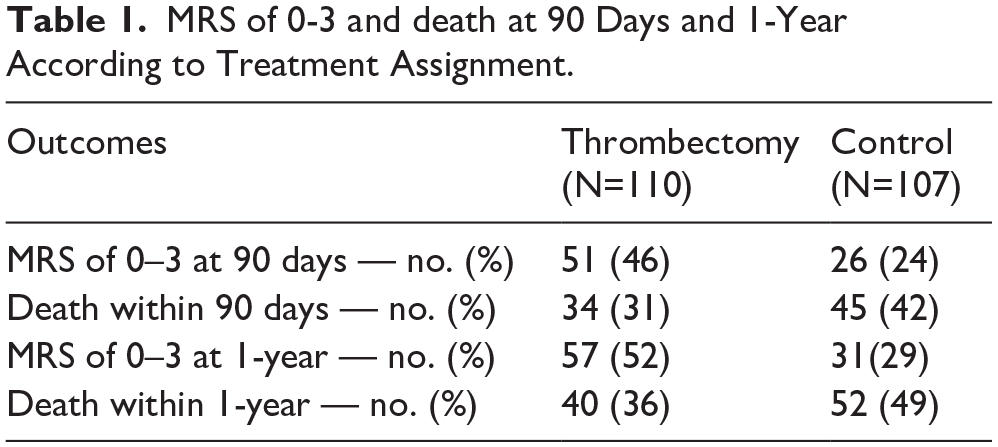
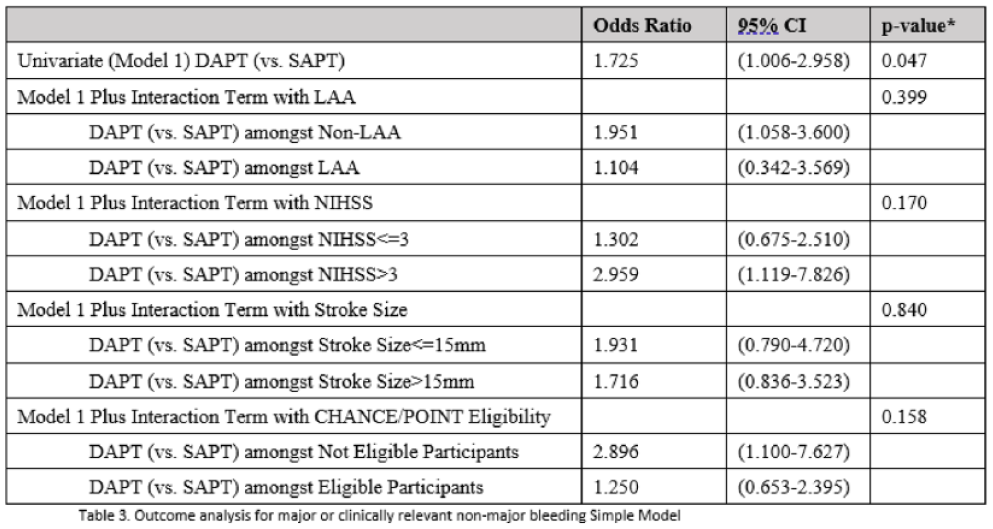
Results: There were 149/459 (32.5%) patients with haematoma expansion and 38/459 (8.3%) with a thrombotic event. Haematoma expansion (HR 3.33; 95% CI 1.73-6.42; p<0.001) and thrombotic events (HR 2.98; 95% CI 2.00-4.43; p<0.001) were associated with mortality (table). At 30 days, mRS of 0-3 occurred in 17.0% of patients with haematoma expansion and in 39% of those without. mRS 0-3 occurred in 31.0% of patients without thrombotic event and in 31% with one.
Conclusions: Haematoma expansion and thrombotic events are both independently associated with mortality. Haematoma expansion is significantly associated with poor functional outcome, but we have insufficient data to draw firm conclusions on the association between thrombotic events and functional outcome.
Multivariate cox regression analysis for mortality at 30 days.
Disclosures of Interest: Yes Study and research funding from AstraZeneca
Abstract N°: 772
Category: 1.01 ACUTE MANAGEMENT - Neither thrombolysis nor thrombectomy
SWISS TRIAL OF DECOMPRESSIVE CRANIECTOMY VERSUS BEST MEDICAL TREATMENT OF DEEP SUPRATENTORIAL INTRACEREBRAL HAEMORRHAGE (SWITCH)
Urs Fischer*1, Juergen Beck2
1University of Bern, Department of Neurology, Bern, Switzerland, 2University of Freiburg, Department of Neurosurgery, Freiburg, Germany
On behalf of: SWITCH Investigators
Background and aims: Decompressive craniectomy (DC) is beneficial in people with malignant middle cerebral artery infarction. Whether DC improves outcome in spontaneous intracerebral haemorrhage (ICH) is unknown. We aim to determine whether DC without haematoma evacuation plus best medical treatment (BMT) in people with ICH decreases the risk of death or dependence at 6 months compared to BMT alone.
Methods: SWITCH is an international, multicentre, randomised (1:1), two-arm, open-label, assessor-blinded trial. Key inclusion criteria are age ⩽75 years, stroke due to basal ganglia or thalamic ICH that may extend into cerebral lobes, ventricles or subarachnoid space, Glasgow coma scale of 8–13, NIHSS score of 10–30, and ICH volume of 30–100mL. Randomisation must be performed <66 hours after onset and DC <6 hours after randomisation. Both groups will receive BMT. Participants randomised to the treatment group will receive DC of at least 12 cm in diameter according to institutional standards. A sample of 300 participants randomised 1:1 to DC plus BMT versus BMT alone provides over 85% power at a two-sided alpha-level of 0.05 to detect a relative risk reduction of 33% using a chi-squared test.
Results: The primary outcome is the composite of death or dependence, defined as modified Rankin scale score 5–6 at 6 months. Secondary outcomes include death, functional status, quality of life, and complications at 180 days and 12 months.
Conclusions: SWITCH will inform physicians about the outcomes of DC plus BMT in people with spontaneous deep ICH, compared to BMT alone. NCT02258919.
Disclosures of Interest: No
Abstract N°: 1059
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
TENECTEPLASE VERSUS ALTEPLASE FOR STROKE THROMBOLYSIS EVALUATION (TASTE): A MULTICENTRE RANDOMISED CONTROLLED PHASE III TRIAL
Mark Parsons*1,2,3, Carlos Garcia-Esperon4,5, Vignan Yogendrakumar6,7,8, Leonid Churilov9, Bruce Campbell6,8,9, Michelle Russell2, Gagan Jyoti Sharma1,3,8, Chushuang Chen1,3,5, Neil Spratt4,5, Christopher Levi4,5
1UNSW, South Western Sydney Clinical School, Liverpool, Australia, 2Liverpool Hospital, Neurology, Liverpool (Sydney), Australia, 3Ingham Institute for Applied Medical Science, Sydney Brain Centre, Liverpool (Sydney), Australia, 4John Hunter Hospital, Neurology, Newcastle, Australia, 5University of Newcastle, Medicine, Newcastle, Australia, 6Royal Melbourne Hospital, Neurology, Melbourne, Australia, 7University of Melbourne, RMH Medicine, Melbourne, Australia, 8Melbourne Brain Centre, Melbourne, Australia, 9University of Melbourne, Melbourne Medical School, Melbourne, Australia
On behalf of: TASTE Investigators
Background and aims: Alteplase is the standard thrombolytic agent for acute stroke. A related plasminogen activator, Tenecteplase, has been shown to result in an improved rates of reperfusion in acute stroke patients with target mismatch on perfusion imaging. Aim: To assess the efficacy and safety of tenecteplase compared to alteplase in acute stroke patients with target mismatch on perfusion CT.
Methods: The tenecteplase (0.25mg/kg) versus alteplase (0.9mg/kg) for Stroke Thrombolysis Evaluation (TASTE) is a multicentre, prospective, randomised, open-label, blinded endpoint (PROBE), controlled phase III non-inferiority trial (2 arms with 1:1 randomisation) in patients with acute ischaemic stroke meeting target mismatch criteria on brain CT perfusion imaging.
The pre-specified adaptive sample size re-estimation after the first 546 participants recommended 832 participants to yield 90% power (two-sided alpha 0.05) to detect a treatment effect (risk difference) of 8% (26% mRS 0-1 in alteplase arm and 34% mRS 0-1 in Tenecteplase arm), with an absolute non-inferiority margin of 3%. Following the announcement of the outcomes of the ATTEST-2 trial that demonstrated non-inferiority of Tenecteplase to Alteplase in stroke patients eligible for thrombolysis <4.5 hours in October 2023, the TASTE steering committee, in consultation with the trial DSMB, made the decision to stop recruitment for TASTE, resulting in a final sample size of 680 participants.
Results: The primary outcome measure is proportion of patients with a modified Rankin Scale (mRS) 0-1 at 3-month. Secondary outcomes include categorical shift in mRS at 3-months; the proportion of patients of symptomatic intracerebral haemorrhage within 36-hours; and death.
Conclusions: TASTE will provide unique data.
Disclosures of Interest: No
Abstract N°: 3007
Category: 1.03 PREVENTION
PLACEHOLDER LATE BREAKING - RESULTS FROM THE ADDRESSING SLEEP APNEA POST-STROKE/TIA (ASAP) STEPPED-WEDGE CLUSTER RANDOMIZED TRIAL
Jason Sico*1,2, Laura Burrone1, Ali Sexson3,4, Anthony Perkins3,5, Stanley Taylor3,4, Brian Koo1,6, Seemant Chaturvedi7,8, Laura Myers3,4, Joanne Daggy9, Dawn Bravata10,11
1Department of Veterans Affairs, Neurology, West Haven, United States, 2Yale School of Medicine, Neurology, New Haven, United States, 3Department of Veterans Affairs (VA) Health Services Research and Development (HSR&D) Expanding Expertise Through E-health Network Development (EXTEND) Quality Enhancement Research Initiative (QUERI), Indianapolis, United States, 4VA HSR&D Center for Health Information and Communication (CHIC), Richard L. Roudebush VA Medical Center, Indianapolis, United States, 5Indiana University School of Medicine, Medicine, Indianapolis, United States, 6Yale School of Medicine, New Haven, United States, 7University of Maryland, Neurology, Baltimore, United States, 8VA Maryland Health Care System, Baltimore, United States, 9Department of Biostatistics and Health Data Science, Indiana University School of Medicine & Fairbanks School of Public Health, Indianapolis, United States, 10Department of Veterans Affairs (VA) Health Services Research and Development (HSR&D) Expanding Expertise Through E-health Network Development (EXTEND) Quality Enhancement Research Initiative (QUERI), 11Indiana University School of Medicine, Neurology, Indianapolis, United States
On behalf of: Addressing Sleep Apnea Post-Stroke/TIA (ASAP)
Background and aims: Despite current cerebrovascular guidelines recommending evaluating ischemic stroke/transient ischemic attack (TIA) patients for obstructive sleep apnea (OSA), sleep testing rates remain low. To improve rates of OSA-testing and treatment among Veterans hospitalized with stroke/TIA through quality improvement (QI) initiatives conducted at 6 diverse VA Medical Centers, with an additional 30 control sites. The Addressing Sleep Apnea Post-Stroke/TIA (ASAP) aims to evaluate the effectiveness of the intervention for the early diagnosis of OSA among stroke/TIA patients.
Methods: Stepped-Wedge Cluster Randomized Trial with baseline and active implementation periods at ASAP Intervention Sites engaging in a multi-faceted quality improvement intervention. The primary outcome is the 30-day OSA diagnostic rate. Secondary outcomes include 30-day OSA treatment rate, and 90-day recurrent vascular event rate and all-cause readmission rates. For the primary effectiveness analysis, the effect of active implementation on diagnostic rate at the 6 intervention sites will be evaluated with a generalized linear mixed-effects model (GLMM) fit to the patient-level data with appropriate site-level random effects. Effects in the model include time as categorical, indicators for the active implementation and sustainability phase, and an indicator for intervention vs control site. In secondary analyses we will adjust for important patient covariates (e.g., stroke severity).
Results: Active implementation is complete as of end of January 2024 with final analyses (including 90-day outcomes) to be completed for beginning of May 2024.
Conclusions: The study is high impact as it will involve approximately 768 patients and will be the first medical-center level intervention examining OSA testing rates and subsequent outcomes.
Disclosures of Interest: No
Abstract N°: 3010
Category: 1.03 PREVENTION
POLYPILL AND RISKOMETER TO PREVENT STROKE AND COGNITIVE IMPAIRMENT IN PRIMARY HEALTH CARE – FINAL RESULTS OF THE PROMOTE PILOT STUDY
1Stroke Center, Neurology, Porto Alegre, 2Donau University, Neurology, Krems, Austria, 3Hospital Moinhos de Vento, Neurology, Porto Alegre, Brazil, 4University of Western Australia, Perth, Australia, 5Western University, London, Canada, 6George Institute for Global Health, Sidney, Australia, 7Hospital Moinhos de Vento, Porto Alegre, Brazil, 8AUT University, Oackland, New Zealand
On behalf of: Promote Study Group. Further authors: Brunna Jaeger, Franciele Santos, Danielle Pereira, Magda Martins, Philip Bath, Renato Lopes, Otavio Berwanger, Gisele Silva, Octavio Pontes-Neto, Maicon Falavigna, Luiz Nasi
Background and aims: PROMOTE study aims to assess whether a polypill (valsartan 80mg, amlodipine 5mg, and rosuvastatin 10mg) used alone or in combination with lifestyle modification (through Stroke Riskometer) will reduce the incidence of stroke and cognitive impairment in a population of individuals at low to moderate risk of stroke. This pilot study aims to assess the feasibility, tolerability, and potential impact of the intervention, including a target reduction in 2.5mmHg in SBP and improvement in 0.4 points in the Life’s Simple 7 score over a 9-month period.
Methods: Phase III, randomized clinical trial, double blinded, placebo controlled in a population aged 50-75 years, no history of hypertension, diabetes, stroke, or other cardiovascular disease, systolic blood pressure (SBP) between 121-139mmHg and at least one lifestyle risk factor. All participants received polypill for 28-day in a run-in phase, to assess adherence and tolerance. Primary Health Care Units in south of Brazil were randomized as clusters to use Riskometer or usual care for lifestyle modification and individual participants to receive polypill or placebo. The calculated sample size for the pilot was 354.
Results: Were randomized 371 patients, mean age 59 years. The polypill was very well tolerated. Mean admission SBP was 130±8mmHg and in 30 days was 120±12mmHg. In 6 months, the greatest reduction in SBP occurred in the Polypill+Riskometer-Group. Among patients utilizing the Riskometer, 71% believed that it assisted in modifying their lifestyle.
Conclusions: The final results of the study will be presented at ESOC.
Disclosures of Interest: No
Abstract N°: 1250
Category: 1.04 REHABILITATION & RECOVERY
A MULTICENTRE, RANDOMISED PLACEBO-CONTROLLED TRIAL, TO DETERMINE SAFETY AND EFFICACY OF PERISPINAL ETANERCEPT ON QUALITY OF LIFE
Vincent Thijs*1,2,3, Geoffrey Cloud4,5, Nigel Gilchrist6, Brooke Parsons1, Jan Ho1, Nikola Sprigg7,8, Marion Walker7, Philip Bath7,8, Leonid Churilov2, Julie Bernhardt1
1Florey Institute of Neuroscience and Mental Health, Stroke, Heidelberg, Australia, 2University of Melbourne, Melbourne, Australia, 3Austin Health, Department of Neurology, Heidelberg, Australia, 4Alfred Health, Melbourne, Australia, 5Monash University, Department of Neuroscience, Central Clinical School, Melbourne, Australia, 6CGM Research Institute, Christchurch, New Zealand, 7University of Nottingham, Nottingham, UK, Stroke Trials Unit, Mental Health & Clinical Neuroscience, Nottingham, United Kingdom, 8Nottingham university Hospitals NHS Trust, Stroke, Nottingham, United Kingdom
On behalf of: PESTO investigators
Background and aims: Few efficacious medical treatment options are available for patients with chronic stroke. Perispinal injection of etanercept, an anti-inflammatory agent targeting tumor necrosis factor, improved post-stroke impairments in observational studies and one pilot randomised controlled trial. This has generated enthusiasm within the stroke patient community.
Perispinal Etanercept to improve STroke Outcomes (PESTO) investigates whether perispinal injection of etanercept improves quality of life and is safe in patients with chronic, disabling, effects of stroke.
Methods: In this phase 2b, international, randomised placebo-controlled trial, adult participants with a history of stroke between 1 and 15 years before enrolment and a current modified Rankin scale between 2 and 5 who are otherwise eligible for etanercept were randomised 1:1 to single dose injection of etanercept or placebo. The primary efficacy outcome is quality of life as measured using the Short Form 36 Health Inventory 28 days after injection. The sample size target is a total of 168 participants assuming an improvement of the SF-36 in 11% of participants in the control arm, in 30% of participants in the intervention arm, 80% power, 5% alpha.
Results: The trial was stopped due to end of funding on 31/12/2023. We enrolled 126 participants (38% percent female, median age 54 [IQR 45,60], median time since stroke 38[21-60] months). The baseline median NIHSS was 5.5[3-9] with 63% having a baseline mRS 2-3. Safety and efficacy outcomes will be presented at the conference.
Conclusions: PESTO provides randomized evidence on perispinal etanercept in patients with long-term disabling effects of stroke.
Disclosures of Interest: Yes VT reports no direct conflicts related to this publication. VT reports speaker fees for Amgen, Allergan, Astra Zeneca, Atricure, BMS, Bayer, Boehringer Ingelheim, Medtronic, unrelated to this work.
PMB is Stroke Association Professor of Stroke Medicine and an emeritus NIHR.
Senior Investigator. He has consulted and received honoraria from CoMind, DiaMedica, Phagenesis and Roche.
General Interest Session - Presidential Symposium Award & Large Clinical Studies
Abstract N°: 469
Category: 1.01 ACUTE MANAGEMENT - Neither thrombolysis nor thrombectomy
INTERACT4 (INTENSIVE AMBULANCE-DELIVERED BLOOD PRESSURE REDUCTION IN HYPER-ACUTE STROKE TRIAL): MAIN RESULTS
Gang Li*1, Yapeng Lin2, Jie Yang3, Craig Anderson4, Lili Song5
1Shanghai East Hospital, Neurology, Shanghai, China, 2The First Affiliated Hospital of Chengdu Medical College, Neurology, Chengdu, China, 3Sichuan Provincial People's Hospital, University of Electronic Science and Technology of China, Neurology, Chengdu, China, 4The George Institute for Global Health, Global Brain Health, Sydney, Australia, 5The George Institute for Global Health, Stroke program, Shanghai, China
On behalf of: INTERACT4 Investigators
Background and aims: Uncertainty exists over whether early ambulance-initiated blood pressure (BP) control improves outcomes in patients with acute stroke, given results of two previous trials in this area. RIGHT-2 showed no overall benefit of transdermal glyceryl trinitrate (GTN) patch but greater hematoma expansion, death, and disability in patients (n=142) with ICH; and a trend towards greater death from GTN after ICH prompted early termination of MR-ASAP.
Methods: INTERACT4 (NCT03790800) randomly assigned ambulance-assessed patients with acute stroke (motor deficit <2 hrs) and elevated SBP (⩾150mmHg) to immediate BP-lowering (target 130-140mmHg) or standard in-hospital BP management in at 2 emergency medical services and 51 hospitals in 2 regions of China, from March 2020 to August 2023. Primary efficacy outcome was 90-day mRS scores in the modified intention-to-treat population (mITT; patients with ischemic stroke/TIA or spontaneous ICH but excluding stroke mimics, secondary ICH or subarachnoid hemorrhage) and with available outcome data.
Results: Of 2425 randomized patients, 21 withdraw or had no consent, and a stroke diagnosis could not be established in 223. The mITT population included 2149 patients, 1083 in prehospital group and 1966 in standard group, with primary outcome data: mean age 69.9 yrs, mean SBP 178mmHg at a median 61 min (IQR 41-94) from symptom onset, and 982 (45%) had ICH. At hospital arrival, mean SBP was 160mmHg in prehospital group and 170mmHg in standard group.
Conclusions: INTERACT4 will establish the balance of benefits and risks of very early prehospital BP-lowering in acute stroke.
Disclosures of Interest: Yes The study has received funding from industry grants
Abstract N°: 659
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
TENECTEPLASE FOR ISCHEMIC STROKE DUE TO LARGE VESSEL OCCLUSION AT 4.5 TO 24 HOURS WITH PERFUSION IMAGING SELECTION (TRACE III)
Yunyun Xiong*1, Bruce Campbell2, Lee Schwamm3, Mark Parsons4, Anding Xu5, Marc Fisher6, Yongjun Wang1
1Beijing Tiantan Hospital, Department of Neurology, Beijing, China, 2The University of Melbourne, Melbourne, Department of Medicine and Neurology, Victoria, Australia, 3Yale School of Medicine, Vascular Neurology, United States, 4University of New South Wales South Western Sydney Clinical School, Department of Neurology, New South Wales, Australia, 5The First Affiliated Hospital, Jinan University, Department of Neurology, Guangzhou, China, 6Beth Israel Deaconess Medical Center, Harvard Medical School, Neurology
On behalf of: TRACE III Investigators
Background and aims: Tenecteplase is a guideline-recommended thrombolytic agent for eligible patients with stroke who are treated within 4.5h after onset. However, there are limited data beyond 4.5h.
Methods: We randomly assigned patients with large vessel occlusion of the middle cerebral artery or internal carotid artery within 4.5 to 24h from the time the patient was last known to be well (including wake-up and unwitnessed stroke) and with salvageable tissue on perfusion imaging, for whom endovascular thrombectomy was not intended, to receive tenecteplase or standard medical treatment. The primary outcome was modified Rankin scale (range, 0 to 6, with higher scores indicating greater disability) 0-1 at day 90. Safety outcomes were symptomatic intracranial hemorrhage and death.
Results: The recruitment completed on 6 November,2023 with the total number of 516 patients. The final results will be available for presentation at the ESOC.
Conclusions: TRACE III will provide evidence about the efficacy and safety of tenecteplase in patients who had an ischemic stroke due to anterior circulation large vessel occlusion beyond 4.5 hours.
Disclosures of Interest: Yes Dr. Schwamm serves as a scientific consultant regarding trial design and conduct to Genentech and Member of steering committee (TIMELESS NCT03785678); consultant on user interface design and usability to LifeImage; and a member of a Data Safety Monitoring Boards (DSMB) for Penumbra (MIND NCT03342664). Dr. Fisher serves as a consultant for Simcere USA and Lumosa; and a member of DSMB for Moleac.
Abstract N°: 3108
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
THROMBOLYSIS IN UNCONTROLLED HYPERTENSION (TRUTH): AN OBSERVATIONAL, PROSPECTIVE, CLUSTER-BASED STUDY
Thomas Zonneveld1, Adrien Groot1, Diederik Dippel2, L. Jaap Kappelle3, Robert van Oostenbrugge4, Yvo Roos1, Marieke Wermer5, H. Bart van der Worp3, Paul Nederkoorn1, Nyika Kruyt*6
1Amsterdam University Medical Centers, Neurology, Amsterdam, Netherlands, 2Erasmus MC, Neurology, Rotterdam, Netherlands, 3UMC Utrecht, Neurology, Utrecht, Netherlands, 4Maastricht UMC+, Neurology, Maastricht, Netherlands, 5University Medical Center Groningen, Neurology, Groningen, Netherlands, 6Leiden University Medical Center (LUMC), Neurology, Leiden, Netherlands
On behalf of: The TRUTH investigators
Background and aims: Intravenous thrombolysis (IVT) in patients with acute ischaemic stroke (AIS) is contraindicated if blood pressure (BP) exceeds 185/110 mmHg. Guidelines recommend an active BP-lowering in order to administer IVT, but evidence for this strategy is lacking. Because rapid BP lowering may also adversely affect outcome, some centers adopted a conservative BP-strategy and administer IVT only when BP drops spontaneously below BP thresholds. We compared these two BP-strategies.
Methods: The ThRombolysis in UnconTrolled Hypertension (TRUTH) study was a prospective, observational, cluster-based, parallel-group, blinded endpoint study. Adult patients, with AIS and BP > 185/110 mmHg, but no other contraindications for IVT, were included. Participating centers adhered to a uniform BP-strategy, subjecting all eligible patients to either active or no BP-lowering in order to administer IVT. Primary outcome was functional status on the modified Rankin Scale at three months using a predefined ordinal shift analysis, adjusted for age, sex, stroke severity, and baseline imbalances (p < 0,10). In addition, a multi-level analysis including center as a random effect, to account for a possible cluster effect, was performed. Secondary outcomes were the occurrence of symptomatic intracranial hemorrhage, IVT rates, and door-to-needle time.
Results: Between 2015 and 2022 we included 853 patients from 27 centers using an active BP-lowering strategy, and 199 from 10 centers not using active BP-lowering. Baseline characteristics were well balanced.
Main results will be presented at ESOC 2024.
Conclusions:
Disclosures of Interest: No
Abstract N°: 1419
Category: 1.03 PREVENTION
COLCHICINE FOR PREVENTION OF VASCULAR INFLAMMATION IN NON-CARDIOEMBOLIC STROKE (CONVINCE). A RANDOMISED CONTROLLED TRIAL
Peter Kelly*1,2, Christian Weimar3,4, Robin Lemmens5, Francisco Purroy6,7, Ana Catarina Fonseca8, Christina R Kruuse9,10, Anna Czlonkowska11, Michael Hill12,13, Cathal Walsh14, Chris Price15
1SCHOOL OF MEDICINE, UNIVERSITY COLLEGE DUBLIN AND MATER UNIVERSITY HOSPITAL DUBLIN, DUBLIN, Ireland, 2HRB STROKE CLINICAL TRIALS NETWORK IRELAND, Ireland, 3Institute for Medical Informatics, Biometry and Epidemiology, Medical Faculty, University Duisburg-Essen, Essen, Germany, 4BDH Clinic Elzach, Elzach, Germany, 5Department of Neurology, University Hospitals Leuven and Department of Neurosciences, Experimental Neurology and Leuven Research Institute for Neuroscience and Disease (LIND), KU Leuven - University of Leuven, Leuven, Belgium, 6Stroke Unit, Department of Neurology, Hospital Universitari Arnau de Vilanova de Lleida, Lleida, Spain, 7Universitat de Lleida, Biomedical Research Institute of Lleida, Universitat de Lleida,, Lleida, Spain, 8Department of Neurosciences and Mental Health (Neurology), Hospital Santa Maria-CHLN, Faculdade de Medicina, Universidade de Lisboa, Lisboa, Portugal, Lisboa, Portugal, 9Herlev Gentofte Hospital, Denmark, 10University of Copenhagen, Copenhagen, Denmark, 11Institute of Psychiatry and Neurology, Warsaw, Poland, 12University of Calgary, Calgary, Canada, 13Foothills Medical Centre, Calgary, Canada, 14School of Medicine, Trinity College Dublin, Dublin, Ireland, 15Population Health Sciences Institute, Newcastle University, Newcastle, United Kingdom
On behalf of: THE CONVINCE INVESTIGATORS
Background and aims: Inflammation contributes to unstable atherosclerotic plaque and ischaemic stroke. In randomised trials, colchicine (a tubulin inhibitor with pleiotropic anti-inflammatory effects) reduced late recurrent stroke and coronary events in patients with coronary disease. The efficacy and safety of long-term colchicine therapy for secondary prevention after stroke is unknown.
Methods: In a multi-centre international Prospective, Randomised Open-label, Blinded-Endpoint assessed (PROBE) controlled Phase 3 clinical trial in 3,154 participants, we compared low-dose colchicine (0.5mg/day) plus usual care versus usual care alone (antiplatelet, lipid-lowering, antihypertensive treatment, lifestyle advice) for secondary prevention of major cardiovascular events (MACE, the first of recurrent ischaemic stroke, myocardial infarction, cardiac arrest, or hospitalisation with unstable angina [non-fatal or fatal]).
Main inclusion criteria were: Age 40 years or greater; ischaemic stroke (modified Rankin score ⩽3) or high-risk TIA (transient motor/speech symptoms with ABCD2>3, or positive DWI, or cranio-cervical artery stenosis); within 72 hours-28 days of randomisation; qualifying stroke/TIA most likely caused by large artery stenosis, lacunar disease, or cryptogenic embolism. Main exclusion criteria were stroke/TIA caused by cardio-embolism or other defined cause (eg. dissection), contra-indication to colchicine (including potential drug interactions), or incapacity for participation in a clinical trial.
Results: The estimated median follow-up will be 42 months (range 15-84 months). The pre-specified primary analysis will be by intention-to-treat. Primary, secondary and safety outcomes will be reported.
Conclusions: CONVINCE will provide the first large randomised trial evidence of the efficacy and safety of anti-inflammatory colchicine therapy for prevention of recurrent stroke, coronary events and death after stroke.
Disclosures of Interest: No
Abstract N°: 4107
Category: 1.04 REHABILITATION & RECOVERY
AI-POWERED NEUROMODULATION HOME THERAPY TO REDUCE GLOBAL DISABILITY IN SUBACUTE ISCHEMIC STROKE: PRIMARY RESULTS FROM THE EMAGINE TRIAL
Jeffrey Saver*1, Pamela Duncan2, Joel Stein3, Steven Cramer1,4, Emily Fox5, Richard Zorowitz6, Sandra Billinger7, Sarah Eickmeyer7, Steven Kirshblum8, Natan Bornstein9
1University of California, Los Angeles, Los Angeles, United States, 2Wake Forest University, Winston-Salem, United States, 3Cornell University, Ithaca, United States, 4California Rehabilitation Institute, Los Angeles, United States, 5Brooks Rehabilitation Hospital - University Campus, Jacksonville, United States, 6MedStar Health: Physical Medicine & Rehabilitation, Washington, United States, 7KU Medical Center, Kansas City, United States, 8Kessler Institute for Rehabilitation - West Orange, West Orange, United States, 9Shaare Zedek Medical Center, Jerusalem, Israel
On behalf of: The EMAGINE Investigators
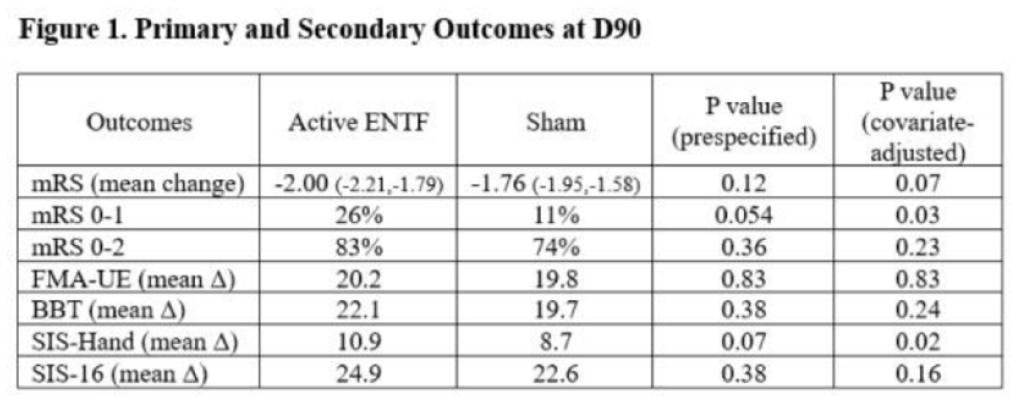
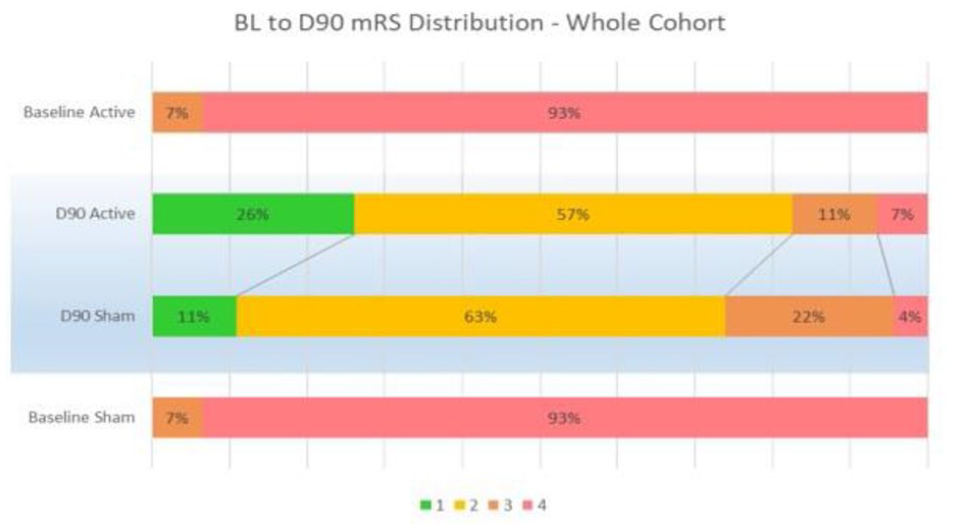
Background and aims: This trial evaluated the safety and efficacy of non-invasive, AI-powered, frequency-tuned, low-intensity electromagnetic therapy (ENTF) in reducing global disability in subacute ischemic stroke patients with moderate-severe disability and upper-extremity impairment.
Methods: Multicentre, double-blind, randomized, sham-controlled, trial. Participants 4-21 days post-stroke, baseline modified Rankin Scale 3-4 and Fugl-Meyer Assessment Upper-Extremity 10-45, allocated to 45 one-hour sessions of active/sham stimulation paired with home physical exercises. The primary endpoint was mRS change from baseline to 90d. Target sample size 150 patients.
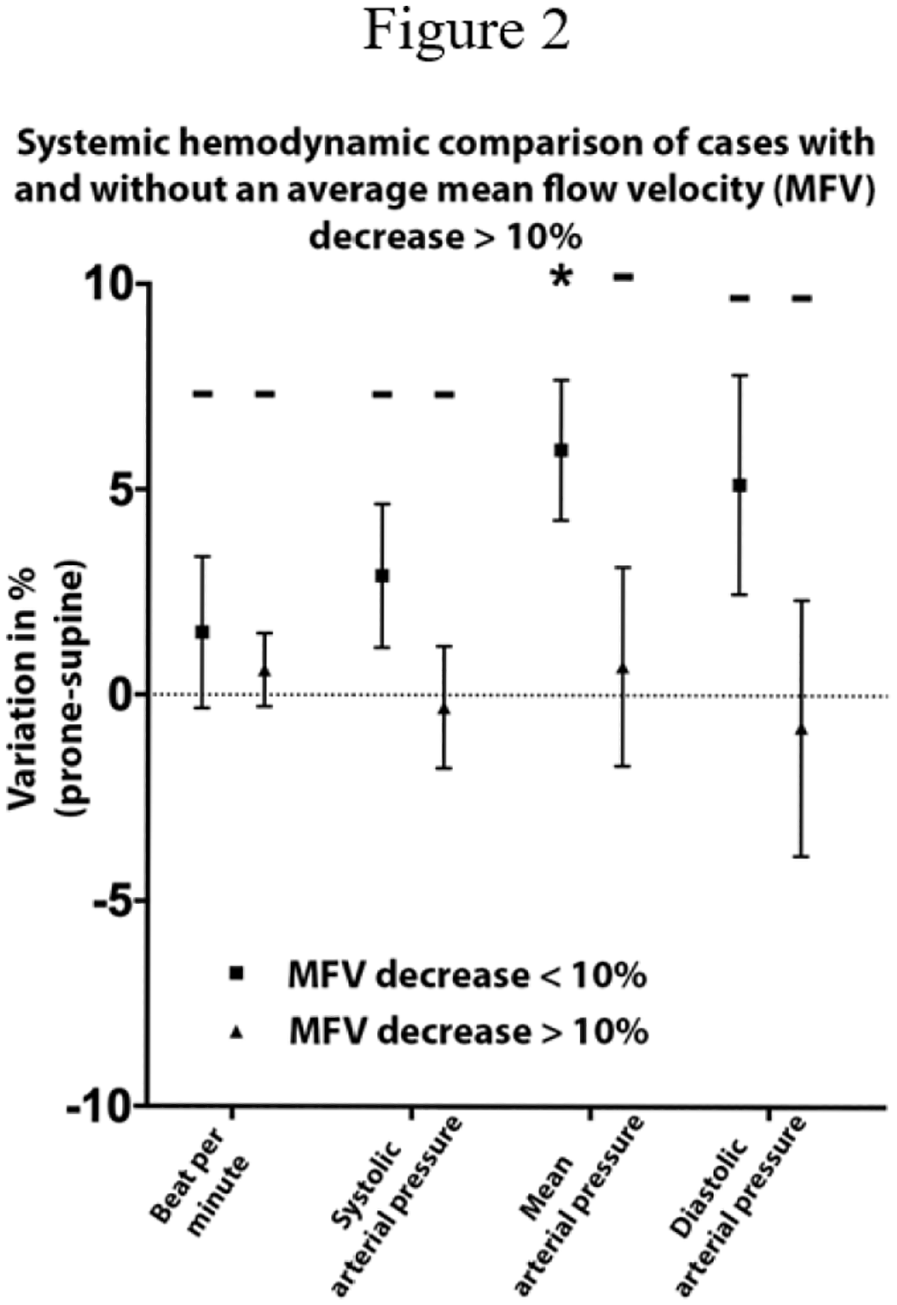
Results: The trial was stopped early after enrolment of 98 patients (49 active/49 sham) at 15 sites when a promising zone/futility threshold was crossed at planned interim analysis. Patient age was 59.0 (±12.4), 33% were female, and study treatment was initiated at 14d (IQR 12-19) post-stroke. Patient groups were similar in age, sex, baseline mRS, but imbalances were noted with active vs sham having more right hemisphere strokes (63% vs 45%), more severe upper extremity impairment (SAFE<5, 63% vs 49%), and fewer small vessel infarcts (31% vs 42%). For the primary outcome, the active vs sham group had 0.24 greater mean change in mRS at day 90 (p=0.12), including mRS 0-1 attained in 26% vs 11% (p=0.054). Secondary outcomes were also directionally favourable albeit nonsignificant in the prespecified analysis and strengthened after adjustment for baseline group imbalances (Figures 1,2). No related serious adverse events were noted.
Conclusions: ENTF therapy showed safety and a signal of efficacy in reducing global disability among subacute ischemic stroke patients with severe baseline disability.
Disclosures of Interest: Yes This study was funded by BrainQ Technologies. JLS, PWD, JS, SCC, and NMB served on the trial Steering Committee, advising on rigorous trial design and conduct, for which they received contracted payments. The remaining authors served as study site PIs and their institutions received funding for study conduct under formal clinical trial contract agreements.
General Interest Session - Closing Ceremony & Large Clinical Trials 2
Abstract N°: 4001
Category: 1.01 ACUTE MANAGEMENT - Neither thrombolysis nor thrombectomy
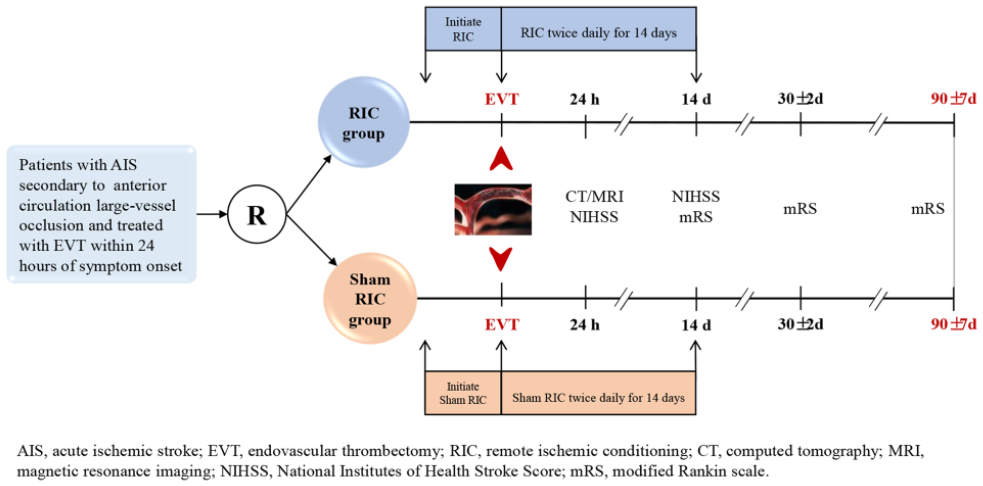
SAFETY AND EFFICACY OF REMOTE ISCHEMIC CONDITIONING FOR SPONTANEOUS INTRACEREBRAL HAEMORRHAGE (RICH-2): A MULTICENTER RANDOMISED CONTROLLED TRIAL
1Xuanwu Hospital, Capital Medical University, Neurology, Beijing, China, 2Wayne State University
On behalf of: RICH-2 investigator
Background and aims: Remote ischemic conditioning has been shown to improve neurological recovery in animal models of intracerebral haemorrhage (ICH) and to be safe and feasible in patients with ICH. We investigated whether RIC improves the functional outcomes in patients with ICH.
Methods: RICH-2 is an investigator-initiated, multicenter, prospective, randomised, sham-controlled, outcome-blinded parallel-group trial being conducted across 21 centres in China. Patients with supratentorial ICH presenting within 24–48 hours of symptom onset who do not need surgical treatment were recruited. All enrolled patients are randomly assigned in a 1:1 ratio to receive RIC or sham RIC for seven consecutive days after randomisation in addition to the general management. The primary outcome is functional independence (defined as modified Rankin Scale⩽2) at 90 days, and secondary outcomes include functional independence at 180 days and shift analysis of 90-day mRS.
Results: From April 22, 2021, to October 30, 2023, 458 patients were randomised, with 229 assigned to each treatment group. Mean age was 58.7 years (SD 12.0), and 134 (29.3%) were female. The median baseline NIHSS was 9.0 (IQR: 6.0 to 13.0). The RICH-2 trial is scheduled to complete its final follow-up at the end of April 2024, and we will present detailed demographics and the main results at the 2023 ESOC late-breaking clinical trials session.
Conclusions: The RICH-2 trial aims to provide evidence of whether RIC for 7 consecutive days could improve the functional outcome of patients with ICH who do not need surgical treatment. ClinicalTrials.gov: NCT04657133.
Disclosures of Interest: No
Abstract N°: 4078
Category: 1.01 ACUTE MANAGEMENT - Neither thrombolysis nor thrombectomy
IMAGING OUTCOMES FOR THE EMBOLIZATION OF THE MIDDLE MENINGEAL ARTERY WITH ONYX IN THE TREATMENT OF SUBDURAL HEMATOMA (EMBOLISE)
Jens Fiehler*1, Jason Davies2, Jared Knopman3, Adnan Siddiqui2, Maxim Mokin4, Ameer Hassan5, Robert Harbaugh6, Khalessi Alexander7
1Neuroradiology, Hamburg, Germany, 2Neurosurgery, Buffalo, United States, 3Neurosurgery, New York, United States, 4Neurosurgery, Tampa, United States, 5Neurology, Harlingen, United States, 6Neurosurgery, Hershey, United States, 7Neurosurgery, San Diego, United States
On behalf of: EMBOLISE investigators
Background and aims: EMBOLISE, a multicenter, prospective, randomized trial, revealed superior effectiveness of Onyx Liquid Embolic System (LES) embolization of the middle meningeal artery (MMA) as an adjunct to conventional treatment for symptomatic subacute or chronic subdural hematoma (SDH) compared to conventional treatment. While the initial clinical data were presented previously, we wish to present the results of the pre-defined imaging data analysis.
Methods: The study included 400 patients in Surgery Cohort who were randomly assigned to treatment (MMA embolization + Surgery) or control (Surgery only), with 180-day follow-up still ongoing. Imaging data were collected at screening, 24 hours, and at 14, 90, and 180 days and adjudicated by an independent imaging core laboratory with double reading for the major variables. CT/MRI readings included hematoma thickness, hematoma volume, and midline shift. Derived from these, absolute and relative changes were calculated. Angiographic images were analyzed using regular angiographic runs in two planes and unsubtracted images. Late angiographic contrast filling and filling of subdural membranes after embolization was independently assessed from distribution of Onyx LES.
Results: The imaging analysis is still ongoing with the final 180 days data being currently transferred and analyzed. The detailed results for the different variables will be presented.
Conclusions: This data allows the estimation of treatment effects on different SDH characteristics. It improves our understanding of the relation between the degree of embolization and the treatment effects. Predictive factors for the highest therapy response will be identified to inform patient selection and treatment strategies in the future.
Disclosures of Interest: Yes Consultancy and presentations: Acandis, Cerenovus, Medtronic, Microvention, Penumbra, Phenox, Stryker
Stock: Tegus Medical, Vastrax, Eppdata
Executive functions: University Medical Center Hamburg-Eppendorf, Eppdata GmbH
Abstract N°: 4065
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
A RANDOMIZED CONTROLLED TRIAL OF TENECTEPLASE VERSUS STANDARD OF CARE FOR MINOR ISCHEMIC STROKE WITH PROVEN OCCLUSION (TEMPO-2)
Shelagh COUTTS*1, Carol Kenney1, Philip Barber1, Philip Choi2, Thalia Field3, Brian Buck4, Timothy Kleinig5, Michael Hill1
1University of Calgary, Canada, 2Monash University, 3University of British Columbia, 4University of Alberta, 5Royal Adelaide Hospital
On behalf of: on behalf of the TEMPO-2 investigators
Background and aims: Almost half of patients with acute ischemic stroke present with initially minor symptoms and large variations in their treatment exists. Patients with minor stroke and intracranial occlusion are particularly at high risk of early neurological deterioration and poor outcomes.
Methods: TEMPO-2 (A Randomized Controlled Trial of TNK-tPA Versus Standard of Care for Minor Ischemic Stroke With Proven Occlusion) was a prospective, open label with blinded outcome assessment, randomized controlled trial, designed to test the superiority of intravenous tenecteplase (0.25mg/kg) over non thrombolytic standard care. Adult patients presenting with acute ischemic stroke with minor deficits (NIHSS 0-5) with visible intracranial occlusion or perfusion deficit within 12-hour from onset were randomized to receive either Tenecteplase (0.25 mg/kg) or non-thrombolytic standard of care. Patients in both groups had a follow up CTA completed 4-8 hours after randomization. Primary outcome was return to baseline neurological functioning defined as a sliding dichotomy based upon pre-stroke neurological function using the modified Rankin Scale (mRS) at 90 days. Safety outcomes include death, symptomatic hemorrhage (intra or extra-cranial). Other secondary outcomes include mRS 0-1, mRS 0-2, ordinal shift analysis on mRS, partial and full recanalization on follow up CT Angiogram, Lawton Instrumental Activities of Daily Living Scale (IADL) and quality of life measured on EQ5QD-5L.
Results: Full results will be available at the time of presentation at ESOC 2024.
Conclusions: TEMPO-2 will provide us with high quality data showing whether thrombolysis with tenecteplase in minor stroke patients with intracranial occlusion is efficacious.
Disclosures of Interest: No
Abstract N°: 4240
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
FINAL RESULTS OF THE REPERFUSION WITH COOLING IN CEREBRAL ACUTE ISCHEMIA II TRIAL (RECCLAIM II)
Rishi Gupta*1, Tareq Kass Hout2, Chung-Huan Sun3, Albert Yoo4, Syed Zaidi5, Osama Zaidat6, Alex Abou-Chebl7, Neeraj Badjatia8, Alhamza Al-Bayati9, Christopher Horn10
1Wellstar Medical Group, Neurosurgery, marietta, United States, 2University of Chicago, Neruology, 3Queens Medical Center, Neurology, Honolulu, United States, 4Texas Stroke Institute, Dallas, United States, 5University of Toledo, Neurology, Toledo, United States, 6Mercy, Neurology, toledo, United States, 7, Henry Ford Health, Detroit, United States, 8University of Maryland, Neurology, Baltimore, United States, 9UPMC, Neurology, Pittsburgh, United States, 10Wellstar Medical Group, Neurology
On behalf of:
Background and aims: Hypothermia reduces ischemic injury in pre-clinical stroke models. We hypothesized combining systemic cooling with mechanical thrombectomy(MT) is safe, feasible without delaying reperfusion.
Methods: Ten sites in the United States enrolled patients in a prospective, randomized core lab adjudicated study to determine the safety of systemic hypothermia to 33 degrees C for six hours with MT. Patients with MCA or ICA occlusion with an ASPECT score of more than 5 under 24 hours from onset were included. The trial was terminated at 66 (planned 80) patients due to catheter supply chain issues. The primary end point compared door to reperfusion time in both groups and secondary endpoint of final infarct volume.
Results: Between May 2019-October 2023 and a total of 95 patients were enrolled (29 lead-in phase and 66 randomized). The mean age of the randomized cohort was 65±12 years with a median NIHSS of 15. The mean time to reach a target temperature was 9±3.7 minutes with 29 of 33 (87.8%) patients achieving target temperature of 34 degrees C within one hour. There was no difference in the time from arrival to first pass between the cooling group 86.2±38.7 minutes vs. 84.2±32 minutes in the control group (p=0.74). There was a trend towards lower final infarct volume in the treatment group with a mean infarct of 31.2±46.6 cc compared to 55.7±68.5 cc (p<0.13). There were no differences in intracranial hemorrhages or pneumonia rates.
Conclusions: Systemic hypothermia does not delay care of thrombectomy patients and can be performed safely.
Disclosures of Interest: Yes PI for RECCLAIM II Zoll
PI for DISTALS Rapid Medical
PI for ASSIST Registry Stryker
Abstract N°: 1808
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
TRIAL OF ADVANCED CT IMAGING AND COMBINED EDUCATION SUPPORT FOR DRIP AND SHIP(TACTICS): PRIMARY RESULTS
Candice Delcourt*1,2,3, Andrew Bivard4, Leonid Churilov4, Andrew Wong5, Timothy Kleinig6, Carlos Garcia-Esperon7,8, Mark Parsons2,9, Sarah Kuhle10, Martine Cox8,11, Christopher Levi7,8,11
1The George Institute for Global Health, Sydney, Australia, 2The University of New South Wales, Sydney, Australia, 3Department of Clinical Medicine, Faculty of Medicine, Health and Human Sciences, Macquarie University, Sydney, Australia, 4Department of Medicine and Neurology, Melbourne Brain Centre, Royal Melbourne Hospital, University of Melbourne, Australian Stroke Alliance, Melbourne Brain Centre, Royal Melbourne Hospital, University of Melbourne, Melbourne, Australia, 5Royal Brisbane and Women's Hospital, University of Queensland, Brisbane, Australia, 6Department of Neurology, Royal Adelaide Hospital, Adelaide, Australia, 7John Hunter Hospital, Neurology, New Lambton Heights, Australia, 8Hunter Medical Research Institute, New Lambton Heights, Australia, 9Liverpool Hospital, Ingham Institute for Applied Medical Research, Liverpool, Australia, 10Queensland State-wide Stroke Clinical Network, Healthcare Improvement Unit, Queensland Health, Herston, Australia, 11School of Medicine and Public Health, College of Health, Medicine and Wellbeing, The University of Newcastle,, Newcastle, Australia
On behalf of:
Background and aims: Treatment of large vessel occlusion (LVO) stroke patients with endovascular thrombectomy (EVT) has demonstrated remarkable efficacy, however achieving equity of access is challenging, especially for rural and regional patients in geographically dispersed countries. In the present trial, we sought to provide an intervention with staff consisting of face to face and virtual reality-based education targeting workflow optimisation, and imaging implementation to optimise EVT provision in regional Australia.
Methods: TACTICS was a non-randomised, cluster cross-over intervention trial. Six clusters, each comprising one EVT hub and a minimum of two primary stroke spokes were exposed to the package intervention. Each cluster sequentially progressed through a 3-month pre-intervention period, a 3-month intervention period, and a 3-month post-intervention monitoring period. The primary outcome was the proportion of patients treated with EVT compared between pre-intervention and pooled intervention/post-intervention periods. Secondary outcomes included the proportion of patients treated with EVT, and the proportion of patients with good (modified Rankin 0-2) and poor (modified Rankin 5-6) functional outcomes between study phases. ACTRN12619000750189; UTNU1111-1230-4161.
Results: Between 13/5/2019 and 29/3/2023, 1009 patients were enrolled into the trial across 6 clusters and 34 hospitals. The odds of receiving EVT by patients with ischaemic stroke and stroke of undetermined cause increased by 44% in the pooled intervention and post intervention periods compared to the pre intervention period, OR 1.44 (95%CI: 1.14-1.80). We did not observe statistically significant between-cluster heterogeneity.
Conclusions: The TACTICS trial successfully tested a novel practice-changing multicomponent, multidisciplinary implementation intervention aiming to optimise regional and rural patient access to EVT.
Disclosures of Interest: No
Abstract N°: 4051
Category: 1.03 PREVENTION
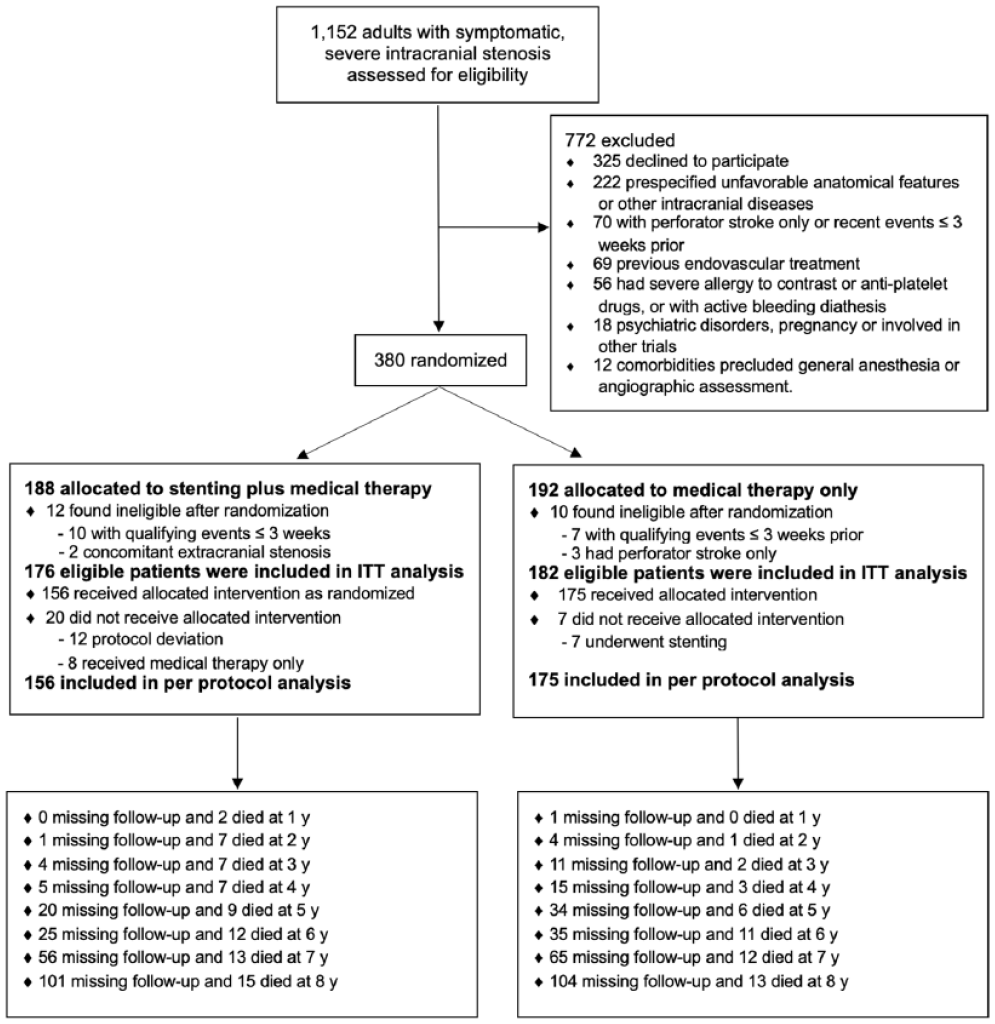
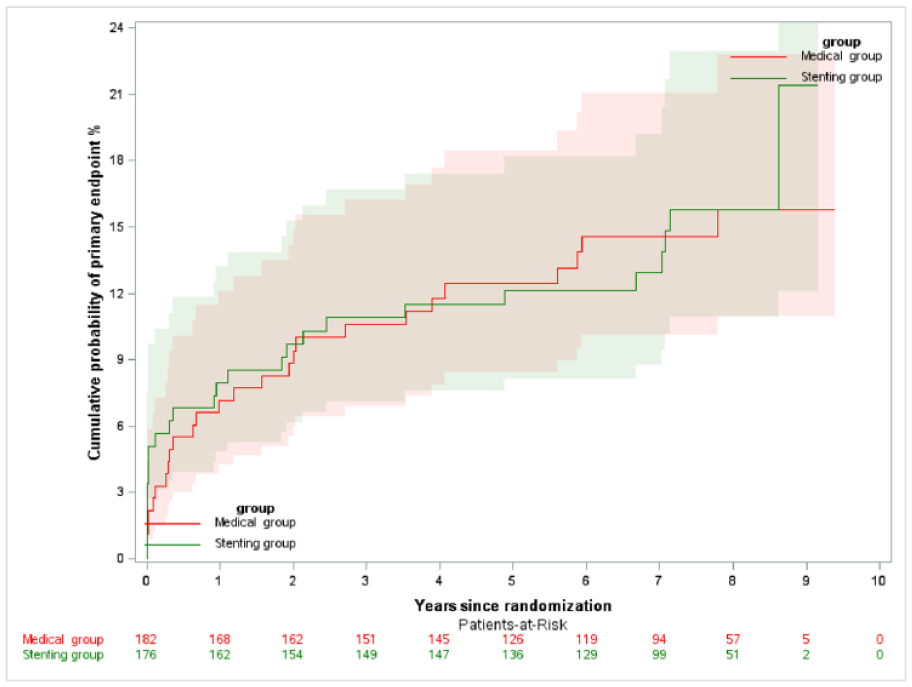
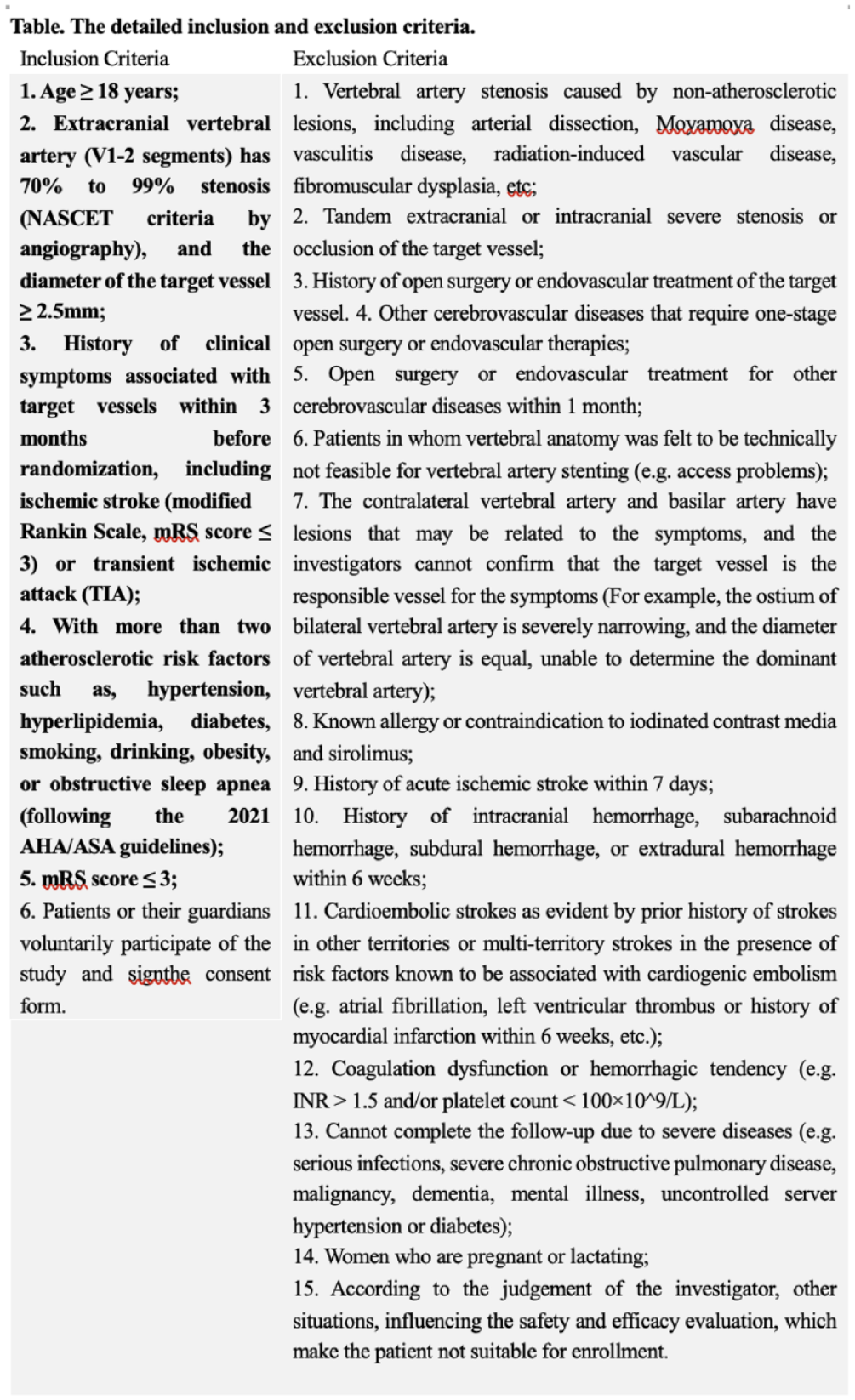
STENTING PLUS MEDICAL THERAPY VS MEDICAL THERAPY ALONE FOR SYMPTOMATIC INTRACRANIAL STENOSIS: 7-YEAR RESULTS OF A RANDOMIZED CONTROLLED TRIAL
1Xuanwu Hospital, China International Neuroscience Institute, Capital Medical University, National Center for Neurological Disorders, Neurosurgery and Interventional Neuroradiology, Beijing, China, 2Beijing Hospital, National Center of Gerontology; Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Neurosurgery, Beijing, China, 3First Affiliated Hospital of Harbin Medical University, Neurosurgery, Harbin, China, 4Henan Provincial People’s Hospital, Cerebrovascular and Neurosurgery, Zhengzhou, China, 5Tangdu Hospital of Air Force Medical University, Neurosurgery, Xi’an, China, 6Strategic Support Force Medical Center, Neurology, Beijing, China, 7Qilu Hospital of Shandong University, Neurology, Ji’nan, China, 8Second Affiliated Hospital of Guangzhou Medical University, Neurosurgery, Guangzhou, China
On behalf of: the CASSISS Trial Investigators
Background and aims: Whether the long-term benefit of stroke prevention of stenting added to medical therapy (MT) over MT alone for symptomatic severe intracranial atherosclerotic stenosis (ICAS) offsets the perioperative risks of the stenting has not been directly evaluated in a randomized trial.
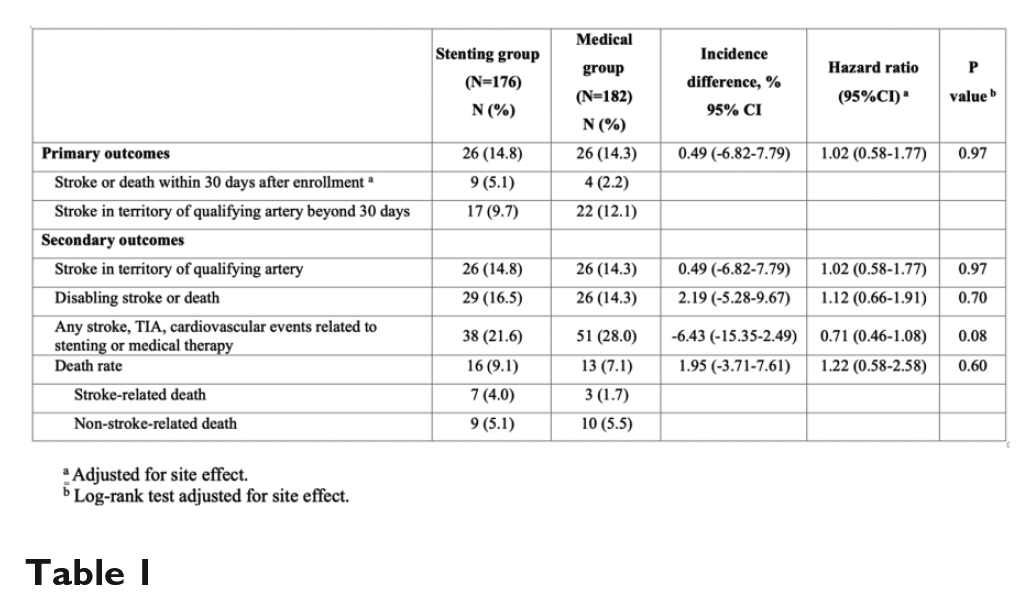
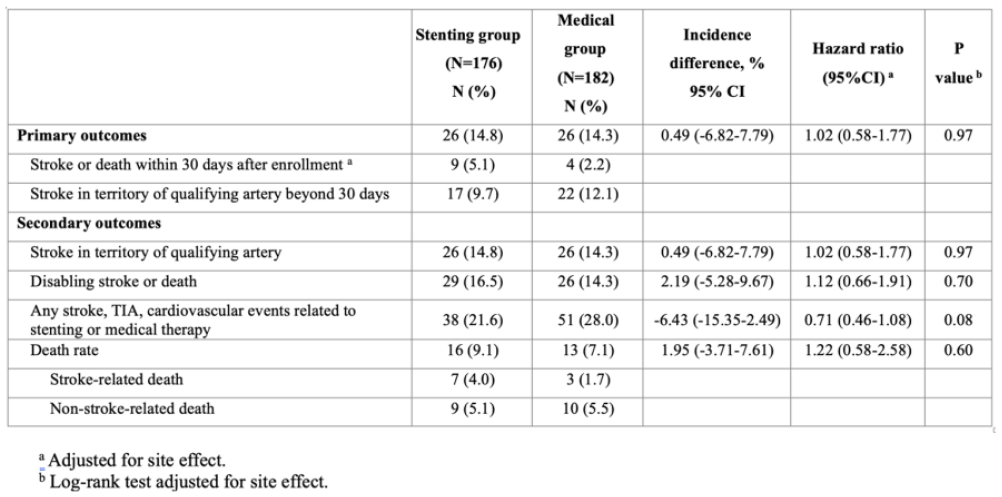
Methods: CASSISS was multicenter, open-label, randomized trial conducted at 8 centers in China. We enrolled patients with TIA or ischemic stroke (mRS 0-2) attributed to severe ICAS (70%-99%). Eligible patients were randomized in a 1:1 ratio to stenting plus MT vs MT alone. The primary outcome was a composite of stroke or death within 30 days or ipsilateral ischemic stroke beyond 30 days. Other secondary outcomes included ipsilateral stroke, disabling stroke or death as well as death after enrollment. This trial was registered in ClinicalTrials.gov with identifier NCT01763320.
Results: 358 patients (stenting 176 vs medical 182) were recruited from Mar 5, 2014 and followed up till Jan 22, 2024 (Figure 1). Median follow-up was 7.4 years (IQR 6.0-8.0). The primary outcome was not significantly different (stenting 14.8% vs medical 14.3%; HR, 1.02 [95% CI, 0.58-1.77]; P = .97; Figure 2). No significant difference was found between groups for the secondary outcomes: ipsilteral ischemic stroke (14.8% vs 14.3%), disabling stroke or death (16.5% vs 14.3%) and death (9.1% vs 7.1%) (Table 1).
Conclusions: No benefit from stenting plus MT over MT alone was found regarding stroke prevention even in long-term follow-up of 7 years. Medical therapy remains the first-line therapy in long-term stroke prevention for symptomatic severe ICAS.
Disclosures of Interest: No
Abstract N°: 860
Category: 1.04 REHABILITATION & RECOVERY
SCREENING FOR EMOTIONAL AND COGNITIVE PROBLEMS IN PATIENTS DISCHARGED HOME AFTER STROKE: A MULTICENTER, CLUSTER RANDOMIZED CONTROLLED TRIAL
Jos Slenders*1, Renske M. Van den Berg-Vos1,2, Caroline Van Heugten3,4, Anne Visser-Meily5,6, Vincent I.H. Kwa1
1OLVG, Neurology, Amsterdam, Netherlands, 2Amsterdam UMC, Neurology, 3Maastricht University, Department of Neuropsychology & Psychopharmacology, 4Maastricht University, Limburg Brain Injury Center, 5UMC Utrecht Brain Center, University Medical Center Utrecht, Department of Rehabilitation, Physical Therapy Science & Sports, 6UMC Utrecht Brain Center, University Medical Center Utrecht, Center of Excellence for Rehabilitation Medicine
On behalf of: ECO-stroke study group
Background and aims: Evidence regarding effectiveness of screening for emotional and cognitive problems after stroke is lacking. This trial examined effectiveness of screening and patient-tailored care for emotional and cognitive problems after stroke.
Methods: This multicenter, patient-blinded, cluster-randomized controlled trial assigned 1:1 hospitals to intervention or usual care. Ischemic stroke patients discharged home were included. The intervention, six weeks post-stroke, included screening for emotional and cognitive problems, screening for participation restrictions, self-management support and referral to rehabilitation services. Primary outcome was societal participation (Restriction subscale of the Utrecht Scale for Evaluation of Rehabilitation – Participation; USER-P-R) at one year. Secondary outcomes included cognitive and emotional complaints (CLCE-24), symptoms of anxiety (HADS-A), symptoms of depression (HADS-D), quality of life (QoL) (EQ-5D-5L, EQ-VAS and PROMIS-10), self-efficacy (GSES) and disability (mRS) at three and twelve months.
Results: 531 patients were included: 267 in intervention and 264 in usual care clusters. Primary analysis demonstrated no difference in USER-P-R one year post-stroke (mean difference (MD) 0.77; 95%-CI -2.46 – 4.06; p-value 0.652). After the intervention, patients reported a lower HADS-A score (MD -0.86; 95%-CI -1.33 – -0.39; p-value <0.001), higher EQ-5D-5L index score (MD 0.044; 95%-CI 0.022 – 0.065; p-value <0.001) and higher EQ-VAS (MD 2.90; 95%-CI 0.69 – 5.10; p-value 0.011) at three months and a higher EQ-5D-5L index score (MD 0.043; 95%-CI 0.021 – 0.064; p-value <0.001) at one year.
Conclusions: This intervention did not improve societal participation, but did improve anxiety and QoL. Implementation should be considered if the intervention is cost-effective in our upcoming economic evaluation.
Disclosures of Interest: No
Abstract N°: 4143
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
ASSOCIATION OF ISCHAEMIC CORE HYPODENSITY ON ENDOVASCULAR THERAPY TREATMENT EFFECT IN LARGE CORE ISCHAEMIC STROKE
Vignan Yogendrakumar*1, Bruce Campbell1, Hannah Johns1, Leonid Churilov1, Deep Pujara2, Felix Ng1, Clark Sitton3, Prodipta Guha1, Gagan Jyoti Sharma1, Amrou Sarraj2
1The Royal Melbourne Hospital, Neurology, Parkville, Australia, 2Memorial Hermann Texas Medical Center, Houston, United States, 3McGovern Medical School at UTHealth Houston, Houston, United States
On behalf of: SELECT2 Investigators
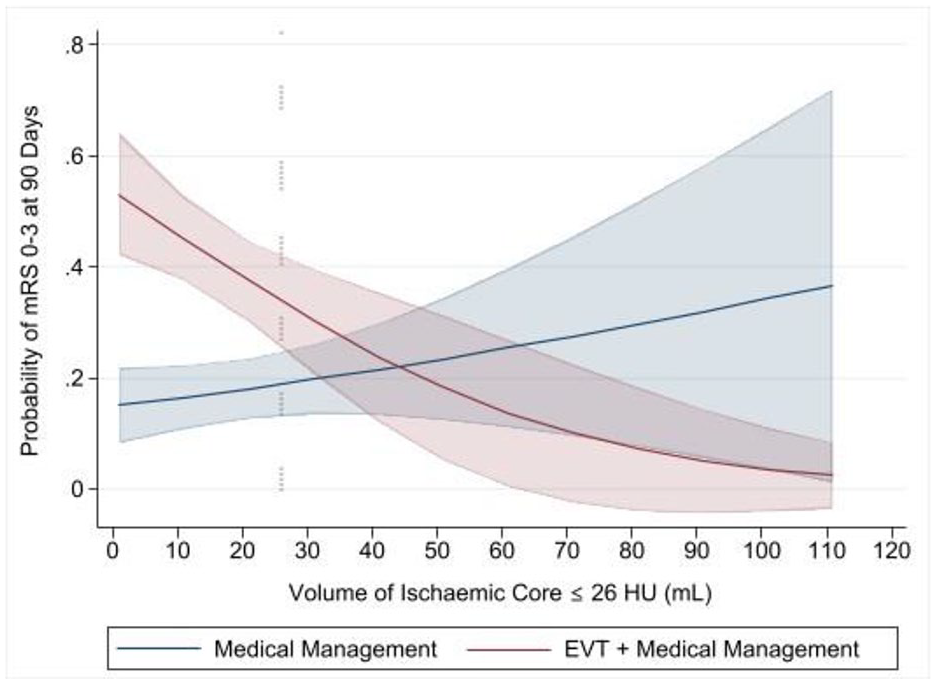
Background and aims: Core volumes are prognostic, but do not modify the treatment effect of endovascular thrombectomy(EVT) versus medical management(MM). We hypothesised that extensive severe CT-hypodensity, representing blood-brain-barrier injury, would be associated with a reduced benefit of EVT.
Methods: The SELECT2 trial assigned patients with large ischaemic core to EVT or MM. Visible CT-hypodensity was outlined and a threshold of severe CT-hypodensity was defined as the lower 99%CI of contralateral thalamic grey matter in Hounsfield units(HU). The association between the volume of severe CT-hypodensity and mRS0-3 was evaluated within EVT and MM arms using logistic regression models, adjusted for age, NIHSS, total CT-core volume, and volume-by-treatment interactions. The plotted relationship between severe CT-hypodensity volume and mRS0-3 was used to select clinically-relevant volume cut-points for further evaluation (Figure). The effect of EVT versus MM on mRS0-3 and hemicraniectomy was assessed in subgroups based on these cut-points.
Results: In 322 patients, median CT-density within the stroke was 31HU(IQR:28-34). The selected threshold of severe CT-hypodensity was 26HU. The volume of ischaemic core ⩽26HU (per 1mL increase) was associated with lower odds of mRS0-3 after EVT (aOR=0·96, 95%CI:0·94-0·99), but not MM (aOR=1·01, 95%CI:0·98-1·03, p-interaction<0·01). In patients with ⩾26mL of severe CT-hypodensity, EVT, compared to MM, was not associated with mRS0-3 (n=101, aOR=0·98, 95%CI:0·33-2·88) versus patients with <26mL of severe hypodensity (n=221, aOR=7·20, 95%CI:3·55-15·47, p-interaction<0·01), but was associated with hemicraniectomy (⩾26mL: aOR=3·45, 95%CI:1·09-10·86 versus <26mL: aOR=0·74, 95%CI:0·31-1·75, p-interaction=0·03).
Conclusions: Severe hypodensity within an ischemic region modifies the treatment effect of EVT and increases the likelihood of hemicraniectomy.
Disclosures of Interest: No
Young Stroke Physicians and Researchers; Research Design Workshop for Studies in Development
Oral presentations
Abstract N°: 4144
Category: 4.30 YSPR – Study Design Workshop
GLUCAGON-LIKE PEPTIDE 1 RECEPTOR AGONIST IN ACUTE LARGE VESSEL OCCLUSION STROKE TREATED BY REPERFUSION THERAPIES – A PILOT STUDY
Bonaventure YM Ip*1, Hao Wang2, Sze Ho MA1, Sangqi Pan1, Trista Hung1, Haipeng LI1, Jill Abrigo3, Thomas Leung1, Ho Ko1, Fengyuan Che2
1The Chinese University of Hong Kong, Medicine and Therapeutics, Shatin, Hong Kong, 2Linyi People’s Hospital, Neurology, Linyi, China, 3The Chinese University of Hong Kong, Diagnostic Imaging and Interventional Radiology, Shatin, Hong Kong
On behalf of: Hanson Leung, KT Wong, CM Chu, Anselm Hui, Billy Lai, Wai Ting Lui
Background and aims: Glucagon-like peptide receptor agonist (GLP-1RA) has been shown to enhance blood-brain barrier function and inhibit neuronal apoptosis in animal stroke models. We aim to evaluate the efficacy and safety of semaglutide, a GLP-1RA, in patients undergoing endovascular thrombectomy (EVT) for large-vessel-occlusion (LVO) strokes.
Methods: In this multicenter, randomized, open-label, outcome assessor-blinded study patients with acute LVO within a 12-hour window were randomized in a 1:1 ratio to subcutaneous semaglutide 0.5mg weekly twice or standard therapy before EVT. Primary outcome was modified Rankin Scale (mRS) score at 90 days. Secondary outcomes included the change in National Institute of Health Stroke Scale (NIHSS) on day 3, malignant cerebral edema, symptomatic intracerebral hemorrhage (sICH) and death. The intention-to-treat population was used for primary analyses.
Results: From September 2023 to February 2024, 83 patients were randomized to semaglutide (n=43) or standard therapy (n=40). Among 58 patients who completed the study, 20 patients (77%) in the semaglutide group and 16 patients (50%) in the control group achieved an mRS score of 0-3 (risk ratio 3.33, 95% CI 1.1-10.5, p=0.036). Semaglutide group showed a greater median improvement in NIHSS on day 3 (-9 vs -5, p=0.049), and a lower incidence of sICH (2.3% vs 15%, p=0.046) compared to the control group. Serious adverse events were similar between the two groups.
Conclusions: In this interim analysis, semaglutide treatment improved clinical outcomes at three months in patients undergoing EVT for LVO strokes. Semaglutide treatment was associated with greater degree of early neurological improvement and a reduced incidence of sICH. (NCT05920889).
Disclosures of Interest: No
Abstract N°: 4165
Category: 4.30 YSPR – Study Design Workshop
ENDOVASCULAR TREATMENT OF SEVERE CEREBRAL VENOUS THROMBOSIS
Na Liu1, Chuanjie Wu1, Jian Chen2, Qingfeng MA1, Ran Meng1, Yan Wu1, Wenbo Zhao1, Jiangang Duan1, Xunming Ji2, Chuanhui Li*1,3
1Xuanwu Hospital of Capital Medical University, Departments of Neurology, Beijing, 2Xuanwu Hospital of Capital Medical University, Department of Neurosurgery, Beijing, 3Xuanwu Hospital of Capital Medical University, Stroke center, Beijing
On behalf of:
Background and aims: Results from case reports and small retrospective studies shown endovascular treatment (EVT) may be a promising therapy for severe cerebral venous thrombosis (CVT) patients. However, the TO-ACT (Thrombolysis or Anticoagulation for Cerebral Venous Thrombosis) clinical trial showed that EVT with standard medical care did not appear to improve functional outcome of patients with CVT. The primary aim of this study is to explore the safety and efficacy of EVT for severe CVT patients via a newly designed randomized controlled trial.
Methods: This is a prospective, multi-center, randomized, controlled, open-label and blinded-endpoint trial. The randomization employs a 1:1 ratio of endovascular treatment and standard medical care vs. standard medical care alone. Adult patients with radiologically confirmed CVT who were defined as severe CVT (Glasgow coma scale ⩽8 or NIHSS⩾10) were included.The primary outcome will be the proportion of patients achieving modified Rankin Scale (mRS) 0–2 at 6 months. Secondary end points are the proportion of patients with mRS score of 0 to 2 at 12 months and mRS 0–3 at 6 and 12 months, ordinal (shift) mRS analysis at 6 and 12 months, recanalization rates at 5(±2) day and 6 months in both treatment arms and surgical interventions in relation to CVT. Safety end points included mortality at 6 and 12 months and symptomatic intracranial hemorrhage.
Results: N/A
Conclusions: Results from this trial will indicate whether EVT is superior to medical management alone in achieving favorable outcomes in CVT subjects.
Disclosures of Interest: No
Abstract N°: 1385
Category: 4.30 YSPR – Study Design Workshop
COGNITIVE IMPROVEMENT AFTER CAROTID REVASCULARIZATION IN ASYMPTOMATIC PATIENTS
Georgina Figueras- Aguirre*1,1, Itziar Abad-Inchaurrondo1, Victor Silva1, Elena Gonzalez2, Albert Martínez Toiran2, Nicolás Augusto Romero Flórez3, David Cánovas1
Background and aims: In patients with asymptomatic carotid stenosis (ACS) over 70%, the management has been slightly changed, taking into account more clinical and radiological factors such as cerebral hemodynamic reserve, silent lesions in MRI and plaque study.
There are several studies that report cognitive impairment associated with asymptomatic carotid stenosis, which is important when examining patient with seemingly “symptom-free” carotid stenosis.
In this context, identifying cerebral hemodynamic impairment can aid in identifying individuals who are at the greatest risk of experiencing cognitive decline and understanding the risk-benefit ratio associated with various treatment approaches.
Methods: We aim to study cognitive impairment in patients with ACS and its evolution after treatment. Selected patients discussed in a multidisciplinary committee (vascular surgery, neurology, and neuroradiology) will undergo a neuropsychological study at baseline, 4 months after surgery or stenting, and at one year. In addition to brain magnetic resonance imaging and previous blood tests.
Results: Many patients evaluated or under follow-up for ACS report cognitive impairment. We designed a study to determine whether there are alterations in the baseline neuropsychological studies and whether there is improvement after revascularization and if it is maintained over time, compared with those who have not undergone revascularization.
Conclusions: In patient with cognitive impairment associated with ACS, the question if it is really "asymptomatic," as well as the importance of improvement or not after revascularization, should be raised, as it could change future clinical practice guidelines.
Disclosures of Interest: No
Abstract N°: 4167
Category: 4.30 YSPR – Study Design Workshop
DEVELOPMENT OF A MULTIVARIABLE PREDICTION MODEL FOR RELEVANT INTRACRANIAL HEMORRHAGE FOLLOWING ENDOVASCULAR TREATMENT IN POSTERIOR CIRCULATION STROKE
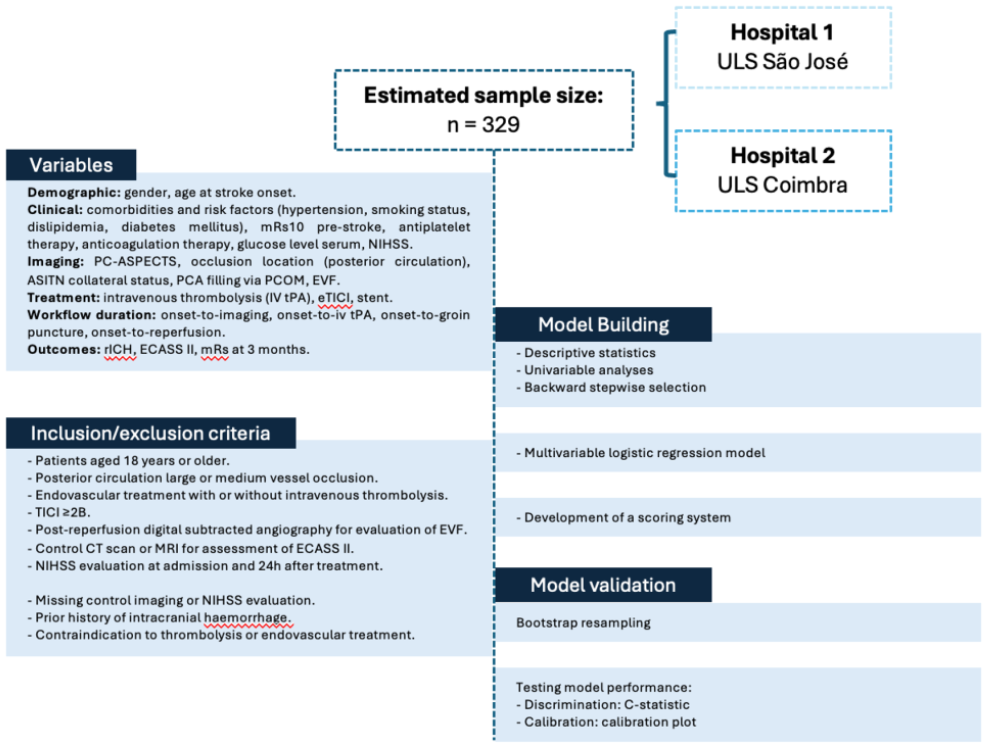
Alexandra Rodrigues*1,2,3, Francisco Miguel Rodrigues4, João Pedro Gonçalves1,3, Catarina Perry Da Câmara3, Ricardo Veiga4, Ana Paiva Nunes5, Isabel Fragata2,3, João Sargento Freitas4,6,7, Diana Aguiar De Sousa5,8,9
1Neuroradiology Unit, Hospital Central do Funchal, Funchal, Portugal - SESARAM, 2NOVA Medical School, Universidade Nova de Lisboa, Lisbon, Portugal, 3Hospital de S. José, Unidade Local de Saúde São José, Lisboa, Portugal - Centro Clínico Académico de Lisboa, Lisboa, Portugal, Neuroradiology, Lisbon, Portugal, 4Center for Neurosciences and Cell Biology, Faculty of Medicine, University of Coimbra, Coimbra, Portugal, 5Stroke Center, Unidade Local de Saúde São José, Lisboa, Portugal - Centro Clínico Académico de Lisboa, Lisboa, Portugal, 6Department of Neurology, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal, 7Faculty of Medicine, University of Coimbra, Coimbra, Portugal, 8Faculdade de Medicina da Universidade de Lisboa, Lisboa, Portugal, 9Instituto de Medicina Molecular, JLA, Lisboa, Portugal, Lisboa, Portugal
On behalf of:
Background and aims: Intracranial hemorrhage significantly affects recovery in ischemic strokes treated with reperfusion therapies. Early Venous Filling (EVF), a novel imaging marker, shows promise for assessing hemorrhage risk after thrombectomy of the anterior circulation. Our study aims to: (1) identify independent risk factors for relevant intracranial hemorrhage (rICH) post-successful endovascular treatment in posterior circulation acute ischemic strokes, (2) develop a predictive algorithm that incorporates EVF for rICH risk, and (3) validate this model to assist clinical decision-making.
Methods: This retrospective, multicentric study follows the TRIPOD checklist, combining data from two Portuguese stroke centers (2016-2023). We estimate 329 patients for both derivation and validation cohorts, with 138 currently enrolled. Eligibility criteria encompasses adults with posterior circulation strokes undergoing endovascular treatments, achieving a final TICI score ⩾2B. Collected variables include demographics, clinical and imaging data, treatment specifics, and outcomes, with rICH defined per ECASS II as PH1 or PH2. Through descriptive, univariable analyses, and a backward stepwise selection for variable inclusion, we aim to devise a multivariable logistic regression model predicting rICH risk, further refined into a user-friendly scoring system. The model’s discrimination accuracy and calibration will be appraised using the C-statistic and a calibration plot, respectively, alongside bootstrap resampling for validation.
Results: Data collection and refinement of the study design are ongoing; no results are yet available.
Conclusions: This study aims to pioneer an early rICH risk prediction tool, potentially guiding therapeutic strategies and improving outcomes for posterior circulation stroke patients treated with endovascular methods.
Disclosures of Interest: No
Scientific Communication - Atherosclerosis & Stroke
Abstract N°: 4027
Category: 1.03 PREVENTION
DRUG-COATED BALLOON FOR ENDOVASCULAR TREATMENT OF SYMPTOMATIC INTRACRANIAL STENOTIC DISEASE: A MULTICENTER RANDOMIZED TRIAL
1Beijing Tiantan Hospital, Department of Neurology, China, 2Taiji Weiye Steel Material Base, Quality Department, Beijing, China, 3The First Affiliated Hospital of Zhengzhou University, Zheng Zhou Shi, China
On behalf of:
Background and aims: The elevated rate of restenosis remained a major issue for bare-metal stents (BMS) stenting in symptomatic intracranial atherosclerotic disease (sICAD). Observational studies showed that drug-coated balloons (DCB) angioplasty could reduce restenosis. Further randomized trials are needed to provide more definitive evidence for DCB application. Thus, we designed a multicenter randomized trial to evaluate the efficacy and safety of DCB angioplasty (Taijieweiye, China) versus BMS stenting (Wingspan, USA) in sICAD patients with high-grade stenosis.
Methods: Eligible patients in 14 tertiary hospitals of China were randomly assigned in a 1:1 ratio to undergo DCB angioplasty or BMS stenting. The primary efficacy outcome was restenosis at 6 months. The primary safety outcome was stroke or death within 30 days.
Results: A total of 209 patients (157 men; median age 59 years) were included in the analysis, with 103 and 106 assigned to the DCB and BMS group, respectively. The 6-month restenosis rate was lower in the DCB group than BMS group (9 [11.1%] vs 24 [28.9%]; risk ratio = 0.38, 95% CI = 0.19-0.78). The DCB group also had a significantly lower rate of symptomatic restenosis at 6 months (1 [1.2%] vs 8 [9.6%]; risk ratio = 0.13, 95% CI = 0.02-0.96). No significant difference in the rate of stroke or death within 30 days was observed between the DCB and BMS groups (6 [5.8%] vs 5 [4.7%]; hazard ratio = 1.24, 95% CI = 0.38-4.05).
Conclusions: DCB angioplasty reduced the risks of restenosis and symptomatic restenosis at 6 months in sICAD patients than BMS stenting.
Disclosures of Interest: Yes Chuan Qin reports related interests (Director of Quality Department, Beijing Taijieweiye Technology Co., Ltd). All other authors declare no competing interests.The study is funded by the Beijing Taijieweiye Technology Co., Ltd. This trial was registered at ChiCTR.org.cn, ChiCTR2100046829.
Scientific Communication - Cardioembolism & Heart-Brain Interactions
Abstract N°: 1517
Category: 1.03 PREVENTION
DEVICE CLOSURE OF PATENT FORAMEN OVALE IN PATIENTS >60 YEARS WITH ISCHEMIC STROKE: RESULTS FROM U.S. MEDICARE BENEFICIARIES
Ruby Satpathy1, Josep Rodés-Cabau2, David Thaler3, David Kent3, Samuel Turner4, Srini Potluri5, Kranthi Kolli6, Nils Peter Borgstrom6, Julie Prillinger6, Jeffrey Saver*7
1Baptist Health, Structural Heart Program, Jacksonville, United States, 2Quebec Heart and Lung Institute, Cardiology, 3Tufts Medical Center, Neurology, 4Novant Health, Cardiology, Winston-Salem, United States, 5Baylor Scott & White Legacy Heart Center, Plano, United States, 6Abbott, United States, 7UCLA Health, Neurlogy
On behalf of:
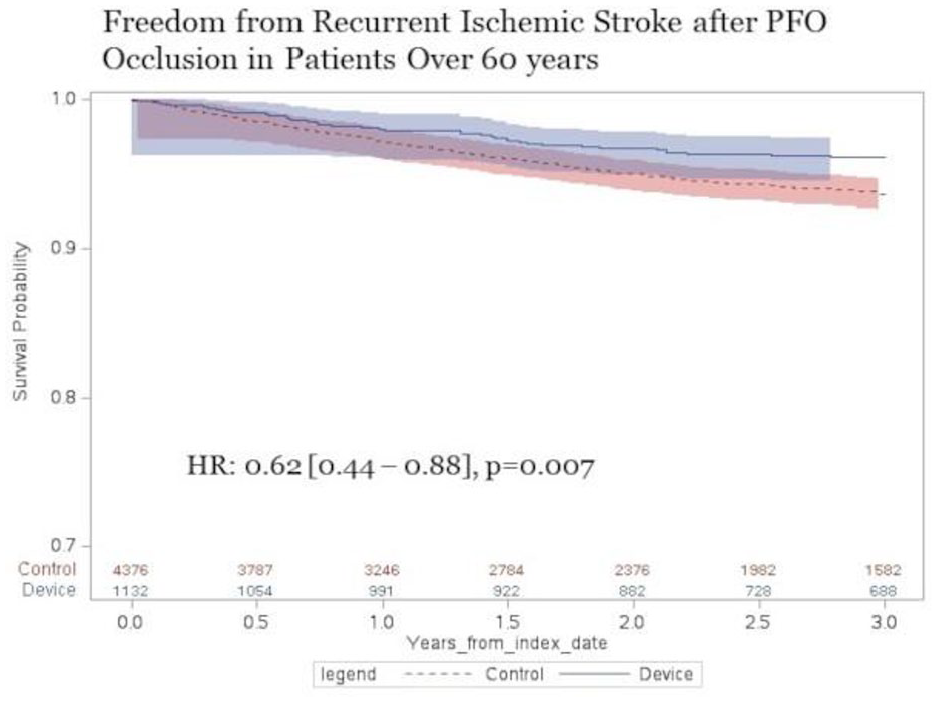
Background and aims: Transcatheter closure of patent foramen ovale (PFO) is a recommended stroke reduction strategy in patients ⩽60 years of age with cryptogenic ischemic stroke, but data on clinical outcomes following PFO closure in patients >60 years are scarce.
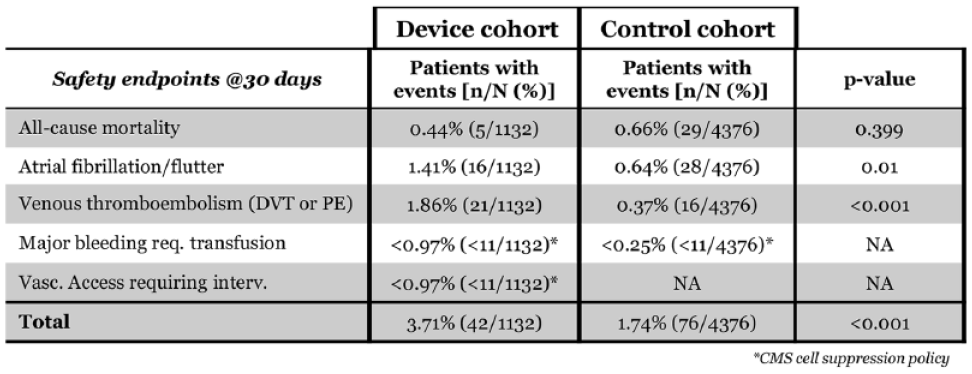
Methods: Medicare Fee-for-Service (FFS) claims data from 2016–2022 were used to identify patients >60 years who were hospitalized with ischemic stroke and diagnosed with PFO or atrial septal defect, and also had ⩾6 months prior FFS coverage. Patients who received an AmplatzerTM PFO Occluder or TalismanTM occluder (device group) were identified by linkage to a manufacturer device-tracking database and were 1:4 propensity-score matched to those who did not receive any closure device (control group). Acute safety events through 30 days and recurrent ischemic stroke through 3 years were evaluated.
Results: A total of 20,999 Medicare beneficiaries (device=1,132; control=19,867) met inclusion criteria. The matched cohort consisted of 5,508 Medicare beneficiaries (device=1,132; control=4,376) with 45% female and median age of 71 years (IQR:67-75). The risk of recurrent ischemic stroke was significantly lower in the device than the control group (HR: 0.62 [0.44 – 0.88], p=0.007). Rates of 30-day safety events were not different for death, but venous thromboembolism (1.86% vs 0.37%, p<0.001) and atrial fibrillation/flutter (1.41% vs 0.64%, p=0.01) were more common in the device group.
Conclusions: In a real-world U.S. cohort of patients >60 years, PFO closure was associated with a reduced rate of recurrent ischemic stroke, compared to control group alone, while maintaining a clinically acceptable safety profile.
Disclosures of Interest: Yes Abbott
Scientific Communication - Service Organisation
Abstract N°: 4129
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
MOBILE STROKE UNIT DISPATCH AND FUNCTIONAL OUTCOMES IN BERLIN: RESULTS FROM B_PROUD-2.0 AND POOLED B_PROUD-1.0+2.0 ANALYSES
Jessica L Rohmann*1,2, Marco Piccininni1,2, Martin Ebinger1,3, Joachim Weber1,4,5,6, Peter Harmel5, Ira Rohrpasser-Napierkowski4,5, Bruno-Marcel Mackert7, Andreas Hartmann8, Matthias Endres1,4,5,6,9,10,11, Heinrich Audebert1,4
1Charité - Universitätsmedizin Berlin, Center for Stroke Research Berlin, Berlin, Germany, 2Charité - Universitätsmedizin Berlin, Institute of Public Health, Berlin, Germany, 3Medical Park Berlin (MPB) Humboldtmühle, Klinik für Neurologie, Berlin, Germany, 4Charité - Universitätsmedizin Berlin, Klinik und Hochschulambulanz für Neurologie, Berlin, Germany, 5Berlin Institute of Health at Charité – Universitätsmedizin Berlin, Berlin, Germany, 6German Centre for Cardiovascular Research (DZHK), partner site Berlin, Berlin, Germany, 7Vivantes Auguste-Viktoria-Klinikum, Klinik für Neurologie mit Stroke Unit, Berlin, Germany, 8Klinikum Frankfurt (Oder), Klinik für Neurologie, Frankfurt (Oder), Germany, 9NeuroCure Cluster of Excellence, Berlin, Germany, 10German Center for Neurodegenerative Diseases (DZNE), partner site Berlin, Berlin, Germany, 11German Center for Mental Health (DZPG), partner site Berlin, Berlin, Germany
On behalf of: The B_PROUD-2.0 Study Group (M Wendt, E Schwabauer, E Freitag, M Zuber, L Bernhardt, J Lange, H Erdur, J Behrens, R Ganeshan, L Schlemm, T Liman, I Lorenz-Meyer, A Hille, G Bohner, D G Nabavi, I Schmehl, A Ekkernkamp, G J Jungehuelsing)
Background and aims: Prehospital stroke management on Mobile Stroke Units (MSUs) shortens time from dispatch to intravenous thrombolysis (IVT) and improves functional outcomes. Given time-dependent IVT effects, further optimising MSU-related procedures may enhance MSU benefits.
Methods: We evaluated process indicators and clinical outcomes in the non-randomized, controlled B_PROUD-2.0 study (05/2019-01/2021, clinicaltrials.gov:NCT03931616) in Berlin (Germany), in which MSUs were dispatched whenever available. Workflow modifications were planned to improve dispatch accuracy and operational processes. The primary population consisted of ischaemic stroke/TIA patients with disabling neurological symptoms upon first ambulance arrival and no contraindications to reperfusion therapies. We also performed analyses on pooled populations of the original B_PROUD-1.0 study and B_PROUD-2.0 (02/2017-01/2021).
Results: The planned procedural improvements were in part disrupted by the COVID-19 pandemic, and a smaller-than-expected sample resulted from time-limited funding (B_PROUD-2.0 N=1,050, planned N=1,500). In B_PROUD-2.0, we found no statistically significant effect of MSU dispatch on primary (common OR (cOR)=0.90, 95%CI:0.72-1.14) or co-primary (cOR=0.86, 95%CI:0.63-1.17) outcomes, despite substantially higher odds of IVT⩽1h of dispatch in the MSU group (OR=10.15, 95%CI:7.10-14.51). In pooled analyses of primary populations (n=2,666), we found a beneficial effect on both primary (cOR=0.80, 95%CI:0.67-0.96) and co-primary (cOR=0.79, 95%CI:0.64-0.97) outcomes. The average effect across all stroke/TIA patients (including those with treatment contraindications; N=4,336) was favourable (primary cOR=0.85, 95%CI:0.75-0.95; co-primary cOR=0.86, 95%CI:0.75-0.99).
Conclusions: No statistically significant differences in functional outcomes were observed in B_PROUD-2.0; however, we observed statistically significant beneficial effects consistent with prior work when considering both B_PROUD study periods, the largest analysis of MSU effectiveness to date.
Disclosures of Interest: Yes J.L.R. and M.P. report a grant from Novartis Pharma for conducting a self-initiated research project on migraine outside the submitted work. M.En. reports grants from Bayer and fees paid to the Charité from Amgen, AstraZeneca, Bayer Healthcare, Boehringer Ingelheim, BMS, Daiichi Sankyo, Sanofi, Pfizer, all outside the submitted work. H.J.A. reported receiving personal fees from Boehringer Ingelheim, Roche and Novo Nordisk, which produce products for the prehospital setting.
Scientific Communication - Risk Factors, Primary Prevention
Abstract N°: 4139
Category: 1.03 PREVENTION
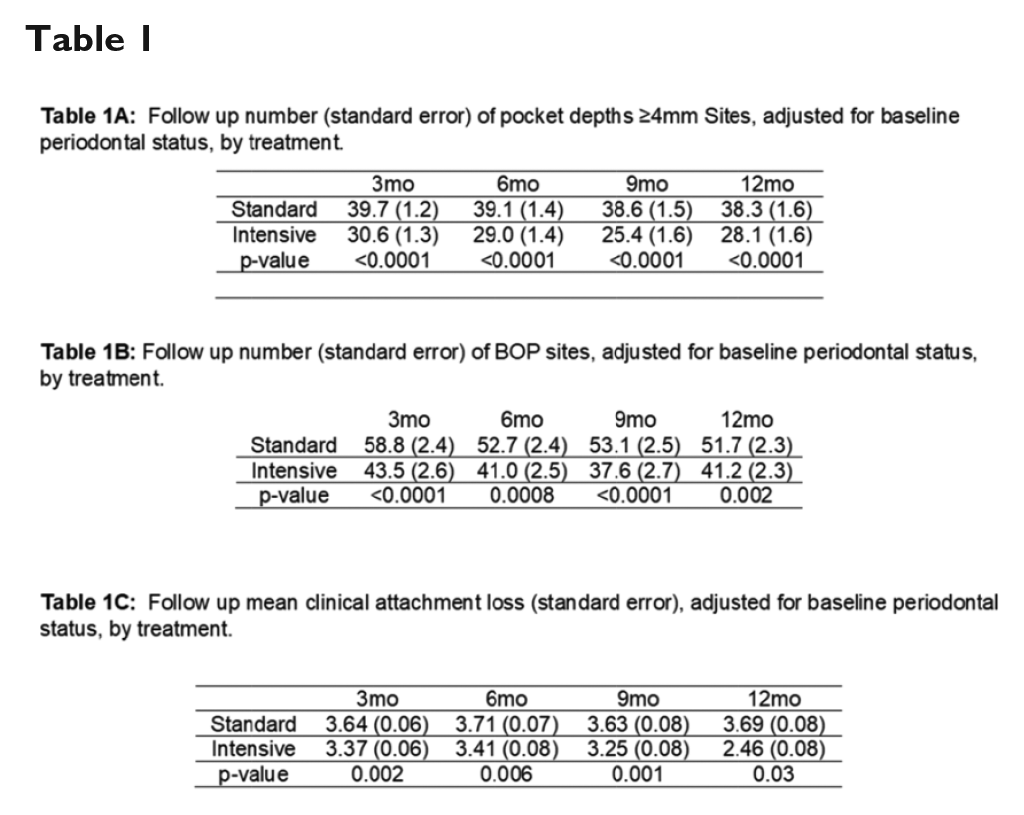
IMPACT OF PERIODONTAL TREATMENT, TREATMENT COMPLIANCE, AND DURATION OF THERAPY ON OUTCOME: SECONDARY ANALYSES OF PREMIERS TRIAL
Souvik Sen*1, Stefanie Wood1, Cynthia Nichols2, James Curtis2, David Hicklin2, David Huang3, Cristiano Susin4, Kevin Moss5, James Beck6
1University of South Carolina School of Medicine, Neurology, Columbia, United States, 2Prisma Health Dentistry–Richland, Columbia, United States, 3UNC Hospitals Neurology Clinic, Chapel Hill, United States, 4UNC Adams School of Dentistry, Dentistry, Chapel Hill, United States, 5Indiana University Bloomington, Bloomington, United States, 6UNC Adams School of Dentistry, Chapel Hill, United States
On behalf of: PeRiodontal Treatment to Eliminate Minority Inequality and Rural Disparities in Stroke (PREMIERS) study group
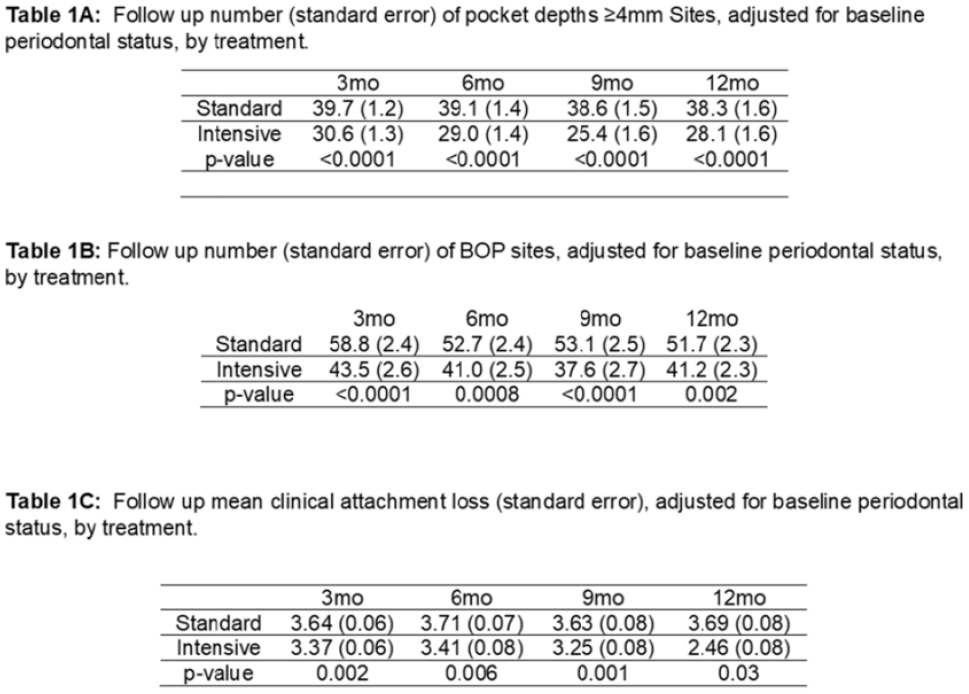
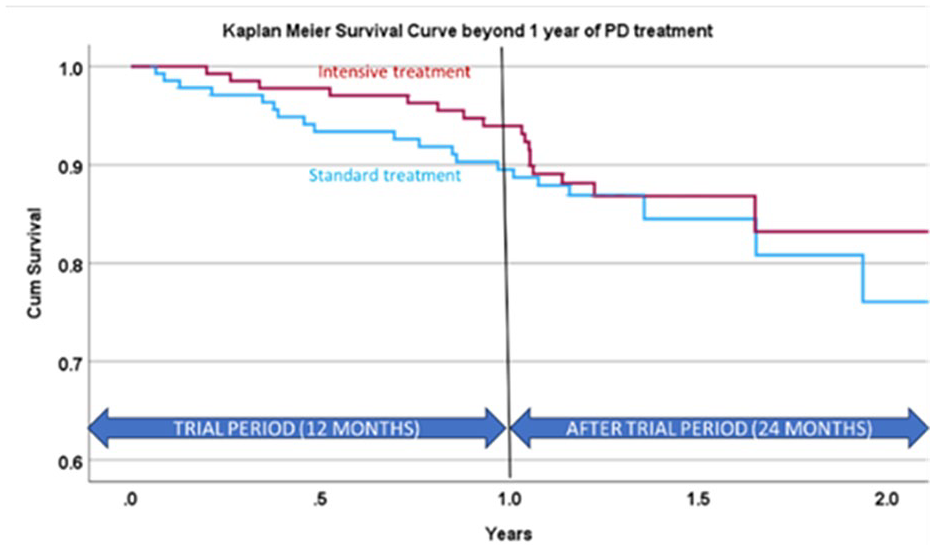
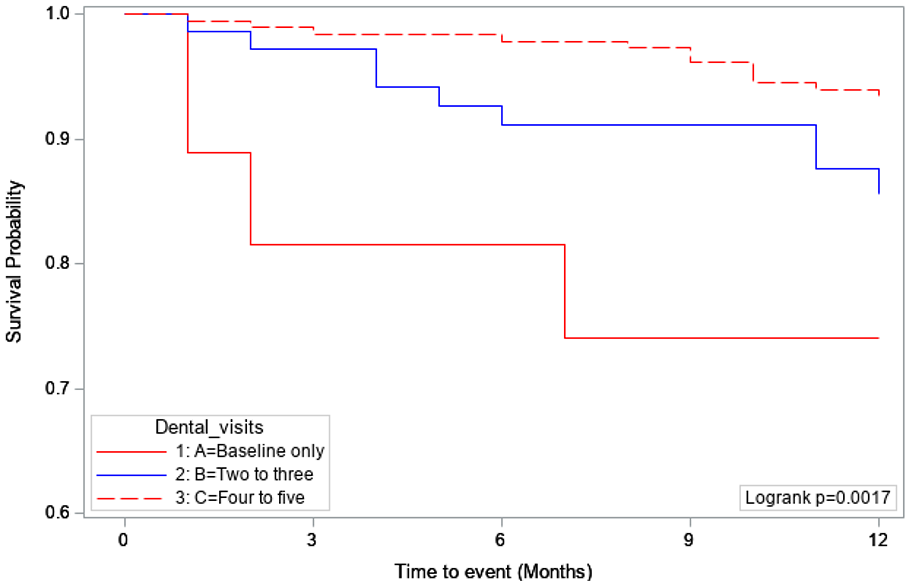
Background and aims: The PREMIERS trial showed safety, reduced vascular events and improvement in vascular risk factors in those receiving periodontal disease (PD) treatment. The next goal was to investigate the effect of treatment frequency on composite vascular outcome, effect after treatment period, effect on PD recovery.
Methods: Two-hundred-eighty stroke/TIA patients with PD were assigned to intensive or standard PD treatment. PD outcomes measured (sites with pocket depth ⩾4 mm, bleeding on probing (BOP), and clinical attachment loss) and treated over 5-visits over 12-months. Composite vascular outcomes were assessed beyond the study period.
Results: The PD outcomes were better in the intensive arm compared to the standard arm (Table-1). However, near complete PD improvement was uncommon (4%). Lower grades of PD were likely to achieve improvement of PD status X2-test, p=0.005. Anecdotally, none of the 10 showing improvement had recurrent vascular event. K-M curve (Figure-1) showed separation of the survival curves in year-1 (HR 0.65, 95% CI 0.30-1.38) however the lines merged after 1 year. Over the study period, 10% attended baseline-dental visit only, 25% 2-3 visits, and 65% 4-5 visits. Compared to the first group, those attending 2-3 visits (HR 0.47, 95% CI 0.18-1.26) and 4-5 visits (HR 0.21, 95% CI 0.08-0.54) had lower composite vascular event rates (Figure-2).
Conclusions: We report significant improvements in the PD outcomes. Those participating in 4-5 dental visits in the 12-month period reaped the most benefit in secondary prevention. The potential benefit reaped seems to be lost beyond the study period.
Disclosures of Interest: No
Scientific Communication - Prognosis and Outcome after Stroke
Abstract N°: 4258
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
HETEROGENEOUS EFFECT ACCORDING TO AGE OF ENDOVASCULAR TREATMENT IN ACUTE STROKE DUE TO LARGE VESSEL OCCLUSION TRIAL IN THE EXTENDED TIME WINDOW
1University of Pittsburg, 2Universidade federal de Sao Paulo, 3Hospital Geral de Fortaleza, 4Hospital de Base de Brasília, 5Hospital Estadual Central, 6Hospital de Base de Sao jose do Rio Preto, 7Hospital de Clinicas de Uberlandia, 8Hospital das Clinicas da Faculdade de Medicina de Ribeirao Preto, 9Hospital de Clinicas de Porto Alegre, Neurology, Brazil
On behalf of: Resilient Study Group
Background and aims: The lack of available advanced imaging techniques for hyperacute stroke is a significant challenge for implementing endovascular therapy in an extended time window. This randomized clinical trial in public hospitals in Brazil aims to assess whether mechanical thrombectomy (MT) is superior to best medical treatment (BMT) in achieving better outcomes for ischemic stroke patients caused by large vessel occlusion (LVO) in the anterior circulation within 8-24 hours last time seen well.
Methods: Participants aged ⩾ 18 had to meet inclusion criteria, including NIHSS scores and involvement in Cortical ASPECTS areas (score 5-10) based on age. Treatment selection was based exclusively on non-contrast CT and CT angiography. In this substudy, we evaluated the effect of the treatment on functional independence (mRs0-2) according to the subgroups.
Results: 245 patients were randomized (126 MT vs. 119 controls). The baseline NIH score was 18±5. In the group, 34 patients (27%) had functional independence in 90 days, compared to 16 patients (13.4%), p=0.009. In the subgroup analysis, patients aged ⩽68years had a higher effect size of MT (36% MTgroup vs 14% BMT, OR 3.5, CI95% 1.6-7.6,p=0.001) compared to >68years (5% MT vs 12% BMT, OR 0.4, CI95% 0.73-2.2, p=0.28). In the logistic regression analysis adjusted for the baseline characteristics, the OR for functional independence was 2.82 (CI 95% 1.4-5.8,p=0.005). Higher age and baseline NIHSS scores were predictors of bad outcomes.
Conclusions: Age was a significant modifier of the effect size for MT in our study, with no benefit of the treatment in older patients.
1The George Institute for Global Health, Global Brain Health, Camperdown, Australia, 2The George Institute China, Stroke program, Shanghai, China
On behalf of: INTERACT Investigators
Background and aims: Uncertainty persists over the effects of blood pressure (BP) lowering in mitigating hematoma growth in acute spontaneous intracerebral hemorrhage (ICH), especially in regard to the timing of initiating treatment.
Methods: We undertook an individual patient data (IPD) pooled analysis of all four Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trials, where serial CT imaging was available to assess hematoma characteristics in participants: INTERACT1 (n=346), INTERACT2 (n=964), INTERACT3 (n=989), and INTERACT4 (N=500+). Primary outcome was hematoma expansion at 24-hours according to standard metrics.
Results: We report the overall treatment effects of intensive BP lowering treatment versus usual care control on hematoma growth, including subgroup analysis to assess the degree of modification by time and key patient characteristics.
Conclusions: This IPD pooling of randomised data, involving a standard treatment protocol using of intravenous agents to achieve a treatment target, is to provide robust evidence to inform clinical guidelines over the use of BP lowering, and to guide the selection and management of patients participating in future clinical trials targeting hematoma growth.
Disclosures of Interest: Yes The study has received funding from industry grants.
Abstract N°: 4255
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
BRIDGING THROMBOLYSIS WITH TENECTEPLASE VERSUS ENDOVASCULAR TREATMENT ALONE FOR LARGE-VESSEL ANTERIOR CIRCULATION STROKE
Valerian Altersberger*1,2, Johannes Kaesmacher3, Leonid Churilov1, Vignan Yogendrakumar1, Jan Gralla3, Peter Mitchell4, Timothy Kleinig5, Bruce Campbell1, Urs Fischer2,6
1Melbourne Brain Centre at the Royal Melbourne Hospital, University of Melbourne, Department of Medicine and Neurology, Parkville, Australia, 2University Hospital Basel and University of Basel, Department of Neurology and Stroke Center, Basel, Switzerland, 3University Hospital Bern, Inselspital, University of Bern, University Institute of Diagnostic and Interventional Neuroradiology, Bern, Switzerland, 4The Royal Melbourne Hospital, University of Melbourne, Department of Radiology, Parkville, Australia, 5Royal Adelaide Hospital, Department of Neurology, Adelaide, Australia, 6University Hospital Bern, Inselspital, University of Bern, Department of Neurology, Bern, Switzerland
On behalf of: on behalf of the SWIFT DIRECT and EXTEND-IA TNK investigators
Background and aims: Multiple randomized controlled trials (RCTs) trials have investigated the effect of endovascular treatment (EVT) alone compared to intravenous thrombolysis (IVT) before EVT. As alteplase was used almost exclusively as thrombolytic agent the effect of IVT with Tenecteplase (TNK) before EVT remains unclear.
Methods: This study is a causal inference study using observational data of the RCTs SWIFT-DIRECT and EXTEND-IA TNK Part 1&2 based on a target trial emulation. We compared patients from SWIFT DIRECT receiving EVT alone to patients from EXTEND-IA TNK Part 1 & 2 receiving TNK 0.25mg/kg or 0.40mg/kg before EVT. The primary outcome was functional independence (defined as mRS of 0-2) at 90 days. Non-disabling outcome (mRS 0-1) was analyzed post-hoc. Secondary outcomes included symptomatic intracerebral hemorrhage (sICH) and successful reperfusion. Additionally, time-dependent subgroups were analyzed. The average causal treatment effect was estimated via inverse probability of treatment weighting (IPTW) and G-Computation.
Results: According to the target trial emulation, 507 patients (198 from SWIFT DIRECT and 309 from EXTEND-IA TNK Part 1 & 2) were included in the analysis. TNK before EVT did not increase the odds for functional independence (ORIPTW 1.13[0.77-1.65]). However, treatment with TNK before EVT resulted in a higher proportion of non-disabling functional outcome (ORIPTW 1.54[1.05-2.25]) compared to EVT alone.
Conclusions: TNK before EVT was not associated with higher rates of functional independence compared to EVT alone. However, we observed an increased likelihood of non-disabling functional in patients treated with TNK before EVT. Final results will be presented at the conference.
Disclosures of Interest: No
Abstract N°: 4250
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
CLEVIDIPINE INFUSION FOR BLOOD PRESSURE MANAGEMENT AFTER SUCCESSFUL REVASCULARIZATION IN ACUTE ISCHEMIC STROKE (CLEVER)
1Promedica Stroke Network, Interventional Neurology / Stroke, 2University of Toledo, Vascular Neurology, 3Barrow Neurological Institute, 4University of Toledo
On behalf of:
Background and aims: Optimal blood pressure target after mechanical thrombectomy (MT) remains unclear. “Clevidipine Infusion for Blood Pressure Management After Successful Revascularization in Acute Ischemic Stroke (CLEVER)”, ClinicalTrials.gov Identifier: NCT05175547, was a prospective, 2-arm, randomized, core- lab adjudicated, single-center pilot study to assess the safety and efficacy of intensive blood pressure control using Clevidipine (on-label use) in AIS patients undergoing standard of care mechanical thrombectomy (MT) within 24-hours of symptoms onset.
Methods: Patient with anterior circulation LVOs, who had SBP >130 mmHg after they achieved TICI2c/3 reperfusion, were screened and randomized between November of 2021 and October 2023 to one of two treatment arms (SBP: 90-120 mmHg vs 90- 160 mmHg) for 24 hrs post-MT. Baseline characteristics, treatment metrics, clinical and radiographic outcomes were recorded per study protocol. The primary efficacy endpoint was time from drug initiation to target BP, and the primary safety endpoint was incidence of any hemorrhagic conversion on follow-up CT/MRI brain at 24 hours.
Results: 80 patients were randomized, 40 per group. Baseline characteristics did not differ between the two groups. Rate of any hemorrhagic conversion per core lab did not differ between the two groups (33% in the BP 90-120 arm and 35% in the BP 90-160 group, P-value 1.00), There was a numerically higher rate of good and excellent clinical outcomes in the 90-160 arm. One patient experienced pulmonary edema while on Clevidipine, that resolved with treatment.
Conclusions: Clevidipine is safe and efficacious as an intravenous antihypertensive medication in stroke patients who undergo MT.
Disclosures of Interest: No
Scientific Communication - Secondary Prevention
Abstract N°: 4045
Category: 1.03 PREVENTION
EARLY STENT-ASSISTED ANGIOPLASTY IN SYMPTOMATIC INTRACRANIAL STENOSIS: A RANDOMIZED TRIAL
Bonaventure YM Ip*1, Sze Ho MA1, Wt Lui1, Xinyi Leng1, Jill Abrigo2, Kwok Tung Lee2, Vincent Ct Mok1, K.S. Wong1, Simon Yu2, Thomas Leung1
1Faculty of Medicine, The Chinese University of Hong Kong, Medicine and Therpauetics, Shatin, Hong Kong, 2Faculty of Medicine, The Chinese University of Hong Kong, Diagnostic Imaging and Interventional Radiology, Shatin, Hong Kong
On behalf of: Yannie Soo, Lisa Au, Vincent Ip, Anne Chan, Florence Fan, Karen Ma, Joseph Choi, Charlie Chan, KT Wong, Sangqi Pan, Trista Hung, Howard Chan, Alexander Lau, Tom Cheung, Bonnie Lam, Andrew Kwok, Ho Ko
Background and aims: Stenting of symptomatic intracranial stenosis (ICAS) under general anesthesia was harmful in previous randomized trials. We aimed to compare the efficacy and safety of stenting under local anesthesia versus medical therapy in patients with symptomatic severe ICAS.
Methods: In this single-centred, open-label, randomized, outcome assessor-blinded trial conducted in Hong Kong, we randomized patients with transient ischemic attack (TIA) or non-perforator non-disabling ischemic strokes attributed to severe ICAS (70-99%) to stenting plus medical therapy, and medical therapy alone within 6 weeks of a qualifying event. Primary safety endpoint was a composite of TIA, ischemic stroke, intracranial hemorrhage and death within 30 days, or any ischemic stroke from 30 days to 1 year. Secondary endpoints were ischemic stroke/TIA in the same artery territory (SIT) and any strokes at 1 year. Cox proportional hazard model was used to compare the study endpoints between the two treatment arms.
Results: From November 2006 to February 2022, 150 patients were randomized into stenting (n=74) versus medical therapy (n=76). No significant difference was observed for the primary endpoint (16.2% vs 23.7%, HR 0.66 [95%CI 0.32–1.36], p=0.260), SIT at 1 year (12.2% vs 19.7%, HR 0.60 [95%CI 0.26-1.34], p=0.210), and any strokes at 1 year (13.5% vs 22.4%, HR 0.57 [95%CI 0.27-1.24], p=0.160).
Conclusions: In patients with TIA or non-disabling ischemic stroke attributed to severe ICAS, percutaneous transluminal angioplasty with stenting under local anesthesia did not result in a significant difference in the risk of stroke or death at 30 days, or stroke from 30 days to 1 year. (CUHK-CCT00116).
Disclosures of Interest: No
Scientific Communication - Intracerebral Hemorrhage
Abstract N°: 4232
Category: 1.01 ACUTE MANAGEMENT - Neither thrombolysis nor thrombectomy
PREDICTORS OF THROMBOTIC EVENTS IN PATIENTS TREATED WITH ANDEXANET ALFA - POOLED ANALYSIS OF TREATED PARTICIPANTS IN THE ANNEXA-4 AND ANNEXA-I TRIALS
Mukul Sharma*1, Ashkan Shoamanesh1, Lizhen Xu1, Magnus Andersson2, Per Ladenvall3, Stuart Connolly1
1Population Health Research Institute, McMaster University, Hamilton, Ontario, Canada, 2AstraZeneca Biostatistics, Gothenburg, Sweden, 3AstraZeneca Biopharmaceuticals Research and Development, Late-stage Development, Cardiovascular, Renal, and Metabolism (CVRM), Gothenburg, Sweden
On behalf of: the ANNEXA-I Investigators
Background and aims: Andexanet alfa rapidly reverses the anticoagulant effect of Factor Xa (FXa) inhibitors and reduces hematoma expansion compared with standard of care but is associated with an increased risk of thrombotic events (TE). We sought to determine the predictors of TE associated with the use of andexanet alfa to identify groups that may be at higher risk.
Methods: We included participants treated with andexanet alfa in ANNEXA-4 (ClinicalTrials.gov identifer, NCT02329327) and ANNEXA-I (NCT03661528). Thrombotic events were defined as arterial ischemic events including ischemic stroke, systemic embolism, and myocardial infarction (MI), or venous thromboembolism (VTE) occurring within 30 days of treatment. A logistic regression model was used to determine the association of baseline demographics and blood pressure, history of prior TE, vascular risk factors, site of bleeding (intracranial, gastrointestinal, or other), and dose of andexanet alfa and FXa inhibitor. Separately we examined the association between baseline variables and arterial TE (excluding VTE).
Results: We included 741 participants, mean age 78.5 +/- 9.9 and 54.5% male. Atrial fibrillation (85.3%) and hypertension (81.9%) were common, and 22% had prior stroke, 11.7% MI, and 19.4% VTE. Intracranial hemorrhage was present in 80%. TE occurred in 10.4% of participants treated with andexanet and included 39 ischemic strokes, 22 MIs, and 26 VTE. We found no significant impact on risk of TE of any potential predictor.
Conclusions: TE occured in 10% of participants treated with andexanet alfa but no baseline variables denoted a higher risk. Predictors of arterial TE will also be presented.
Disclosures of Interest: Yes MS: research grants and/or consulting fees from AstraZeneca, Bristol Myers Squibb, Bayer, HLS Therapeutics, Janssen, and Javelin Medical. AS: grants and advisory honoraria from AstraZeneca. LX: nothing to disclose. MA and PL: employees of AstraZeneca. SC: grant support and consultant for Portola, Bristol Myers Squibb, Bayer, and Daiichi Sankyo; consultant for Javelin; and holds patent (US 2010/0255000) and pending patent (US 2017/0369862 A1).
Scientific Communication - Sex Matters
Abstract N°: 4170
Category: 1.03 PREVENTION
BLOOD BIOMARKERS INFLUENCING SEX DIFFERENCES IN POST-STROKE FUNCTIONAL OUTCOMES OF ACUTE ISCHEMIC STROKE
Meng Wang*1, Zixiao LI1, Yongjun Wang1
1Beijing Tiantan Hospital, Neurology, Beijing, China
On behalf of:
Background and aims: Female patients with acute ischemic stroke (AIS) experienced worse functional outcomes. However, the reasons remain largely unexplained.
Methods: Patients with AIS were recruited in the Third China National Stroke Registry between August 2015 and March 2018. The primary outcome was an unfavorable functional outcome at 3-month, defined as an mRS>2. Blood samples were collected within 24 hours of admission. The blood biomarkers were identified as inflammation, coagulation, and metabolism biomarkers, according to their biological functions. We then used an elastic net model within a tenfold cross-validation framework to generate a composite metric for each group of biomarkers. Finally, mediation analysis under the counterfactual framework was used to determine whether the association of sex and unfavorable functional outcomes was mediated by blood biomarkers represented by the composite metrics.
Results: A total of 11997 patients were included [62.4±11.3years; 3766 (31.4%) women]. Female patients tended to have a higher prevalence of risk factors, except for smoking and drinking. Women also showed different expression patterns in blood biomarkers with men (eg. FPG: women 6.7±2.8 mmol/L vs. men 6.3±2.5 mmol/L, p<0.001). At 3-month, women (17.9%) suffered significantly worse functional outcomes than men (13.2%). The explainable proportion of sex-related differences in the functional outcomes by inflammation, coagulation, and metabolism biomarkers were 41.9%, 23.3%, and 30.2%, respectively (all p<0.05, Figure).
Conclusions: The current study suggests that sex partially influences stroke functional outcomes through inflammation, coagulation, and metabolism pathways, which provides new insights into prevention and treatment strategies.
Disclosures of Interest: No
Abstract N°: 4046
Category: 1.03 PREVENTION
SEX-RELATED DIFFERENCES IN GASTROINTESTINAL BLEEDING RISK WITH DIRECT ORAL ANTICOAGULANTS: UK NATIONAL PHARMACOVIGILANCE STUDY OF ADVERSE DRUG EVENTS
David Ryan*1,2,3, Ahmed Hassan1,4, Benjamin Johnstone2, Fiona Humphries2
1University College London Hospital, Clinical Pharmacology, London, United Kingdom, 2National Hospital for Neurology and Neurosurgery, Stroke Medicine, London, United Kingdom, 3London School of Hygiene and Tropical Medicine, Medical Statistics, London, United Kingdom, 4School of Medicine, Cardiff University, Cardiff, United Kingdom
On behalf of:
Background and aims: Direct oral anticoagulants (DOACs) are commonly prescribed to reduce stroke risk in patients with atrial fibrillation, but are associated with an increased risk of gastrointestinal (GI) bleeding. The influence of sex on GI bleeding risk remains uncertain, and trials often lack sufficient power to assess safety signals within subgroups. Understanding real-world sex-related differences are crucial to promote the safe use of DOACs.
Methods: Serious or fatal adverse drug events (ADEs) data for DOACs (apixaban, dabigatran, edoxaban and rivaroxaban) were obtained from the UK medicines regulator. Proportional reporting ratios (PRRs) and 95% confidence intervals for GI bleeding were estimated for each DOAC according to sex. The PRR compares the signal for GI bleeding in the DOAC to the background signal for the ADE across all other drugs. A PRR > 1 suggests a deleterious effect.
Results: Whilst females had higher reporting of all ADEs, they had less reports of GI bleeding compared to males (8,125/658,114; 0.012% vs. 8,151/935,193; 0.009%, p < 0.001). Dabigatran and edoxaban had the highest proportion of reported GI bleeds (452/3,826; 11.81% and 217/1,764; 12.30% respectively). Signals for GI bleeding with DOACs were higher in females compared to males in all DOACs, reaching statistical significance for dabigatran, apixaban and rivaroxaban, but not edoxaban.
Conclusions: There are sex-related differences in reporting of GI bleeding related to DOACs. This could be related to biological susceptibility, pharmacokinetic differences or confounding associated with spontaneous reporting. Sex-specific safety of DOACs warrants further study.
Disclosures of Interest: No
Scientific Communication - Cognition and Vascular Cognitive Impairment
Abstract N°: 182
Category: 1.03 PREVENTION
PREVENTION OF DEMENTIA USING MOBILE PHONE APPLICATIONS (PRODEMOS)
Edo Richard*1, Eric Moll van Charante2, Marieke Hoevenaar-Blom2, Manshu Song3, Nicola Coley4, Melanie Hafdi2, Ron Handels5, Youxin Wang3, Carol Brayne6, Wei Wang3
1Radboud University Medical Centre, Neurology, Nijmegen, Netherlands, 2Amsterdam University Medical Centre, Public and Occupational Health, Amsterdam, Netherlands, 3Capital Medical University, School of Public Health, Beijing, China, 4INSERM - University of Toulouse, Epidemiology and Public Health, Toulouse, France, 5Karolinska Institutet, neurobiology, Stockholm, Sweden, 6Cambridge University, Psychiatry, Cambridge, United Kingdom
On behalf of: PRODEMOS Study Group
Background and aims: The prevalence of dementia and stroke will increase in low-and middle-income countries and those with low socioeconomic status (SES) in high-income countries. Mobile health interventions can help reach underserved populations globally to improve lifestyle and reduce risk factors for dementia and stroke.
Methods: This 18-months open label, blinded endpoint, hybrid effectiveness-implementation randomised controlled trial (RCT) investigated whether a coach-supported mHealth intervention can reduce dementia risk in persons 55-75 years of low SES in UK or from China with ☒2 risk factors (hypertension, diabetes, dyslipidemia, obesity, physical inactivity, smoking, cardiovascular disease, depression). Primary outcome was change in CAIDE risk score (including blood pressure, total cholesterol, BMI, physical activity). Secondary outcomes include individual risk factors and 10-year cardiovascular disease risk (Framingham). Implementation outcomes included coverage, acceptability, appropriateness, adoption, feasibility, sustainability, and costs. ISRCTN15986016.
Results: Between January 2021 April 2023, 1,488 persons were included and randomised, with 1,229 (82.6%) available for analysis of the primary effectiveness outcome. Effect on the primary and secondary effectiveness outcomes will be presented at ESOC 2024 (confidentially already available upon request). Implementation appeared feasible, but reaching these populations is challenging. Of all participants, 81% adopted the intervention and 50% participated actively throughout the study.
Conclusions: Full results of this large randomized controlled trial on a coach-supported mHealth intervention to improve lifestyle and reduce risk factors for dementia, stroke and cardiovascular disease in persons with low SES in the UK and any SES in China will be presented at ESOC 2024.
Disclosures of Interest: No
Abstract N°: 2419
Category: 1.04 REHABILITATION & RECOVERY
INCIDENCE, RISK FACTORS, AND TRAJECTORIES OF COGNITIVE IMPAIRMENT TO TWO YEARS POST STROKE: THE R4VAD MULTICENTRE STUDY OF 2437 PATIENTS
Joanna Wardlaw*1, Ellen Backhouse1, Lisa Woodhouse2, Rosalind Brown1, Terence J Quinn3, Fergus Doubal1, David Werring4, Thompson Robinson5, John O'brien6, Philip Bath2
1University of Edinburgh, United Kingdom, 2University of Nottingham, United Kingdom, 3University of Glasgow, United Kingdom, 4University College London, United Kingdom, 5University of Leicester, United Kingdom, 6University of Cambridge, United Kingdom
On behalf of: The Rates, Risks and Routes to Reduce Vascular Dementia (R4VaD) Study Group
Background and aims: Post-stroke cognitive impairment (PSCI) is of major concern with limited understanding of risks, rates or trajectories. R4VaD, a UK-wide longitudinal cohort study, determined PSCI incidence, trajectories and risk factors up to two years post-stroke.
Methods: R4VaD recruited patients aged ⩾18yrs from 53 UK centres 09/2018-09/2022, within 6 weeks after stroke, excluding those likely to die ⩽12weeks, and collected baseline demographics, stroke severity (NIHSS), cognition (Montreal Cognitive Assessment [MoCA], verbal fluency, telephone interview cognitive scale-modified [TICS-M]), education, socioeconomics, dependency, mood. We assessed cognitive, vascular, functional, mood outcomes and self-reported memory/thinking problems subacutely (6+/-2 weeks later), at 1- and 2-yrs. We mapped outcomes to a Diagnostic and Statistical Manual of Mental Disorders-5 (DSM-5) 7-level ordinal neurocognitive scale, and analysed PSCI to 2 years with covariate adjustment.
Results: We recruited 2437 patients, mean age 68.2yrs, (range 19-97), 40% female, mean worst NIHSS 4.9 (range 0-35), retaining 92% at 2yrs. At baseline (median 6days), 48.4% had ⩾single domain PSCI (Figure). At subacute, 1 and 2yrs, ⩾single domain PSCI was respectively 21.9%, 12.1% and 10.5% while 2.4%, 6.4%, 11.1% had died. Self-reported memory or thinking problems were 19.5% baseline, 38.6% subacutely, 47.2% 1yr, to 42.1% 2yrs.
Conclusions: In this large representative multi-centre study of stroke survivors, objective PSCI reduced from baseline 48.4% to 10.5% at 2yrs, but may underestimate patient-experienced cognitive impairment, while 11% had died.
Full risk predictors and trajectory analysis will be presented.
DSM-5 7-level PSCI to 2-years, n=2437.
Disclosures of Interest: No
Scientific Communication - Rare Causes, Stroke in the Young
Abstract N°: 4132
Category: 1.03 PREVENTION
APIXABAN VERSUS ASPIRIN IN PATIENTS WITH CANCER AND CRYPTOGENIC STROKE: A SUBGROUP ANALYSIS OF THE ARCADIA TRIAL
Babak Navi*1, Mitchell Elkind2, David Tirschwell3, W. T. Longstreth Jr3, Richard Kronmal4, Jordan Elm5, Joseph Broderick6, Hooman Kamel1, Benjamin Miller7, Christopher Streib7
1Weill Cornell Medicine, Neurology, New York, United States, 2Columbia University, Neurology, New York, United States, 3University of Washington, Neurology, Seattle, United States, 4University of Washington, Biostatistics, Seattle, United States, 5Medical University of South Carolina, Biostatistics, Charleston, United States, 6University of Cincinnati College of Medicine, Neurology and Rehabilitation Medicine, Cincinnati, United States, 7University of Minnesota, Neurology, Minneapolis, United States
On behalf of: the ARCADIA Study Group
Background and aims: Limited data exist on the utility of different antithrombotic strategies in patients with cancer and cryptogenic stroke. We compared apixaban versus aspirin for the prevention of adverse clinical outcomes in patients with history of cancer and cryptogenic stroke.
Methods: We analyzed data from ARCADIA, a multicenter, randomized, double-blind clinical trial (ClinicalTrials.gov Identifier: NCT03192215), conducted from 2018-2023. Patients with recent cryptogenic stroke and biomarker evidence of atrial cardiopathy were randomized to standard-dose apixaban versus aspirin 81 mg daily. We examined subgroups of patients with and without history of cancer at baseline. The primary outcome for this post-hoc analysis was a composite of major ischemic or major hemorrhagic events. Major ischemic events were recurrent ischemic stroke, myocardial infarction, systemic embolism, and symptomatic venous thromboembolism. Major hemorrhagic events included symptomatic intracranial hemorrhage and major extracranial hemorrhage.
Results: Among 1,015 participants, 137 (13.5%) had history of cancer. Participants with history of cancer, compared to those without, had a higher risk of major ischemic or major hemorrhagic events (HR, 1.77; 95% CI, 1.14-2.75). Among those with history of cancer, during a median follow-up of 534 days (IQR, 214-901), 8 of 61 participants (13.1%) randomized to apixaban and 17 of 76 participants (22.4%) randomized to aspirin had a major ischemic or major hemorrhagic event (HR, 0.58; 95% CI, 0.25-1.33).
Conclusions: Among ARCADIA participants with history of cancer, the risk of major ischemic and hemorrhagic events did not differ significantly with apixaban versus aspirin, but a clinically important benefit of apixaban could not be ruled out.
Disclosures of Interest: Yes BN served on adjudication committee for MindRhythm Inc. ME is a salaried AHA employee; received study drug from BMS-Pfizer Alliance and ancillary funding from Roche for ARCADIA; and royalties from UpToDate. HK serves as Deputy Editor for JAMA Neurol; served on steering/executive committees for Medtronic, Janssen, and Javelin Medical; served on adjudication committees for AstraZeneca, Novo Nordisk, and BI; and has ownership interests in TETMedical, Spectrum Plastics Group, and Burke Porter Group.
Moderated Poster - Acute Management
Abstract N°: 1650
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
ADVANCING TECHNIQUES IN ENDOVASCULAR TREATMENT FOR CEREBRAL VENOUS THROMBOSIS: AN INTERNATIONAL TWO-CENTER REGISTRY
Maider Iza Achutegui*1, João André Sousa2, Jesús Juega1, Manuel Requena1, Marta Olive1, Noelia Rodriguez-Villatoro1, David Rodriguez-Luna1, Jorge Pagola1, Marta Rubiera1, Carlos A. Molina1
1Vall d'Hebron University Hospital, Barcelona, Spain, 2coimbra hospital, neurology, coimbra, Portugal
On behalf of:
Background and aims: After several uncontrolled studies and one randomized clinical trial, there is still uncertainty regarding the role of endovascular treatment (EVT) in Cerebral Venous Thrombosis (CVT). Our aim was therefore to evaluate the safety and efficacy of EVT in CVT along with the best medical care.
Methods: We performed a retrospective analysis of an international two-center registry of CVT patients admitted since 2019. Good outcome was defined as a return to baseline modified Rankin scale at three months. We compared EVT vs no-EVT patients.
Results: We included 61 patients, of which 60 (99%) patients received systemic anticoagulation. EVT was performed in 13/61 (20%). EVT patients had a higher baseline NIHSS [6 (2-17) vs 0 (0-2.7), p=0.002)] and a higher incidence of intracerebral hemorrhage (53.8% vs 20.3%, p=0.03). Recanalization was achieved in 10/13 (77%) patients. Angioplasty was carried out in 7 out of 12 patients and stenting in 3 cases. No postprocedural complications were observed. Improvement of median NIHSS from baseline to discharge was observed in patients treated with EVT [6 (2-17) vs 1(0-3.75) p<0.001]. Adjusting to NIHSS and ICH, EVT had a non-significant increase in the odds of a good outcome [aOR 1.42 (95%CI 0.73-2.8, p=0.307)]. Motor symptoms (aOR =8.1 95%CI 1.9-34.3, p=0.004) and ICH (aOR=4.5, 95%CI 1.1-17.7, p=0.03) were independent predictors with poor outcomes.
Conclusions: EVT in combination with anticoagulation was safe and efficacious in acute treatment of CVT as suggested by NIHSS improvement. Neutral results of TO-ACT trial should not withhold clinicians from considering this treatment.
Disclosures of Interest: No
Moderated Poster - Clinical Trials
Abstract N°: 4005
Category: 1.01 ACUTE MANAGEMENT - Neither thrombolysis nor thrombectomy
RESCUE: A PHASE 2 RANDOMIZED TRIAL SHOWS SAFETY AND EARLY SIGNS OF EFFICACY OF RNS60 AS AN ADJUNCTIVE THERAPY IN ISCHEMIC STROKE
Supurna Ghosh*1, Jordan Dubow1, Jocelyn Sutherland1, Grayson Baird2, Wendy Smith2, David Chiu3, Wayne M. Clark4, Christopher Favilla5, David Liebeskind6, Ryan Mctaggart2
1Revalesio Corporation, Tacoma, United States, 2Rhode Island Hospital, Brown University, Providence, 3Houston Methodist Hospital, Houston, 4Oregon Health and Science University, Portland, 5University of Pennsylvania, Philadelphia, United States, 6University of California Los Angeles, Los Angeles, United States
On behalf of: Andreas Kalmes1, Jarrad Mock1, Douglas J. Cook2, Sameer A. Ansari3, Tracy Madsen4, Mahesh Jayaraman4, Krisztina Moldovan4 and Radmehr Torabi4; 1Revalesio Corp, USA 2Queen's University, Canada; 3Northwestern Univ, USA and 4Rhode Island Hospital, USA
Background and aims: Despite significant improvements in early reperfusion, there remains a need for cerebroprotective therapies for stroke. RNS60 is an experimental drug with demonstrated therapeutic benefits in rodent and primate stroke models. RESCUE tested RNS60 in ischemic stroke patients with large vessel occlusions (LVO) undergoing endovascular thrombectomy (EVT).
Methods: The multicenter, placebo controlled, double-blind, Phase 2 study enrolled 82 EVT eligible participants randomized 1:1:1 (block urn randomization for age, NIHSS SPECTS), A to a 48-h infusion (0.5 mL/kg/h RNS60, 1 mL/kg/h RNS60, or 1 mL/kg/h placebo) starting before arterial access closure. Participants were followed for 90 days. The primary objective was safety. The primary efficacy endpoint was dichotomized day-90 mRS; other secondary endpoints included change in infarct volume, BI, and NIHSS.
Results: The study met its primary endpoint of safety and mortality, with similar rates of serious adverse events between treatment arms and numerically lower number of deaths in the RNS60 groups. The 1-mL/kg/h RNS60 group showed 63% of subjects with Day-90 mRS of 0-2 compared to 46% on placebo (Odds ratio 4.1,p=0.35),reduced infarct growth at 48-hours post EVT by 50% (nominal P <0.05), and numerically outperformed placebo in other functional outcomes, e.g., day-90 BI (71% on 1-mL/kg/h RNS60 vs. 43% on placebo had ⩾ 95; OR 7.2, p=0.12) and NIHSS (absolute value and change from baseline) at each specified time point.
Conclusions: RNS60 was generally safe and well tolerated as an adjunct protective treatment to EVT and demonstrated numerical improvement in all efficacy outcomes. A Phase 3 study is in development.
Disclosures of Interest: No
Abstract N°: 1181
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
TWO-YEAR OUTCOMES AFTER COLLATERAL-BASED SELECTION FOR ENDOVASCULAR TREATMENT IN THE LATE WINDOW
Ilse Huijberts*1,2, Florentina Pinckaers1,3,4, Susanne Olthuis4,5, Sander van Kuijk6, Yvo Roos7, Charles Majoie8, Aad van der Lugt9, Diederik Dippel10, Wim Van Zwam1,4, Robert van Oostenbrugge4,5
1Maastricht University Medical Centre+, Department of Radiology and Nuclear Medicine, Maastricht, Netherlands, 2Maastricht University, Faculty of Health, Medicine & Life Sciences (FHML), Maastricht, Netherlands, 3Maastricht University, Care and Public Health Research Institute (CAPHRI), Maastricht, Netherlands, 4Maastricht University, School for Cardiovascular Diseases (CARIM), Maastricht, Netherlands, 5Maastricht University Medical Centre+, Department of Neurology, Maastricht, Netherlands, 6Maastricht University Medical Centre+, Department of Clinical Epidemiology and Medical Technology Assessment (KEMTA), Maastricht, Netherlands, 7Amsterdam UMC location University of Amsterdam, Department of Neurology, Amsterdam, Netherlands, 8Amsterdam UMC location University of Amsterdam, Department of Radiology and Nuclear Medicine, Amsterdam, Netherlands, 9Erasmus, University Medical Center Rotterdam, Department of Radiology and Nuclear Medicine, Rotterdam, Netherlands, 10Erasmus, University Medical Center Rotterdam, Department of Neurology, Rotterdam, Netherlands
On behalf of: The MR CLEAN-LATE investigators
Background and aims: The MR CLEAN-LATE trial showed the safety and efficacy of late-window endovascular treatment (EVT) for acute ischaemic stroke (AIS) in the anterior circulation due to large vessel occlusion in patients preselected on the presence of collateral flow on CT-angiography. The present study reports outcomes at two years post-randomisation.
Methods: MR CLEAN-LATE (trial registration: NL58246.078.17; ISRCTN19922220) randomly assigned 502 patients to either the EVT- or control group. Clinical outcomes were assessed at several timepoints post-randomisation. The modified Rankin Scale (mRS) at two years was the primary outcome of this study. Treatment effect on the mRS was analyzed using ordinal logistic regression, yielding an adjusted common odds ratio (acOR). Secondary two-year end points included all-cause mortality, quality of life (EQ-5D-5L), and the Barthel Index score.
Results: The mRS-score at two-years was available for 428 patients (85%). The median mRS-score was 4 (2-6) in the EVT-group and 6 (2-6) in the control group. EVT was associated with reduced disability on the mRS (acOR 1.41, 95%CI 1.00-1.99), and improved functional independence (mRS 0-2: aOR 1.79, 95%CI 1.11-2.91; mRS 0-3: aOR 1.62, 95%CI 1.04-2.52). All-cause mortality during the two-year follow-up was lower in the EVT-group (adjusted hazard ratio 0.81, 95%CI 0.60-1.08). EQ-5D-5L utility values (adjusted β 0.06, 95%CI -0.01-0.12) and Barthel Index scores (adjusted β 7.20, 95%CI 0.51-13.88) also favoured the EVT-group.
Conclusions: The effectiveness of late-window EVT sustained for up to two years after AIS. This is important for prompting further evaluations of (cost-)effectiveness, health care policy development, and clinical decision making.
Disclosures of Interest: Yes This research was supported by the Dutch organization for Health research and Health innovation, and the Collaboration for New Treatments of Acute Stroke consortium (CONTRAST), which is supported by the Dutch Heart Foundation, Stryker, Medtronic, Cerenovus, Top Sector Life Sciences & Health, and The Netherlands Brain Foundation.
Abstract N°: 4011
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thromb
INTRAVENOUS Y-3 FOR THE TREATMENT OF ACUTE ISCHEMIC STROKE: A MULTI-CENTER, RANDOMIZED, DOUBLE-BLIND, PLACEBO-CONTROLLED PHASE II CLINICAL TRIAL
Shuya Li*1, Baoyu Feng1, Yongjun Wang1
1Beijing Tiantan Hospital affiliated to Capital Medical University, Department of Neurology and Department of Clinical Trial Center, Beijing, China
On behalf of:
Background and aims: Y-3, a dual-target small molecular blocking nNOS-PSD-95 while potentiating α2-containing GABAAR, has been proven effective in animals. We aimed to investigate the safety and efficacy of intravenous Y-3 in acute ischemic stroke (AIS) patients within 48 h of symptom onset.
Methods: Subjects were randomly assigned in a 1:1:1:1 ratio to the Y-3 low-dose group (20 mg/dose), medium-dose group (40 mg/dose), high-dose group (60 mg/dose), and placebo group. All subjects received continuous intravenously infused treatment for 10 days (qd., 60±10 min/dose). The primary efficacy outcome was excellent functional outcome defined as a modified Rankin Scale score of 0-1 at 90 days. The primary safety outcomes was incidence of adverse events (AEs).
Results: A total of 240 subjects completed randomization and 224 subjects received treatment form June 4, 2023 to November 18, 2023. A total of 210 subjects experienced 730 AEs, with 173 AEs in 48 (80.0%) subjects in the high-dose group, 211 AEs in 53 (88.3%) subjects in the medium-dose group, 208 AEs in 54 (91.5%) subjects in the low-dose group, and 138 AEs in 55 (90.2%) subjects in the placebo group (P=0.260). The proportion of subjects with excellent functional outcome was 70.0% (42/60) in the high-dose group, 76.7% (46/60) in the medium-dose group, 67.8% (40/59) in the low-dose group, and 60.7% (37/61) in the placebo group (P=0.164).
Conclusions: Intravenous Y-3 was well tolerated in the AIS patients within 48 h of onset in China. The efficacy and appropriate dosage of Y-3 for the AIS need prospective validation.
Registration Number: ChiCTR2400081662
Disclosures of Interest: No
Abstract N°: 4187
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
ENDOVASCULAR THROMBECTOMY FOR STROKE DUE TO BASILAR-ARTERY OCCLUSION: 1-YEAR OUTCOMES OF THE BAOCHE TRIAL
1Xuanwu Hospital of Capital Medical University, Stroke center, Beijing, China, 2Xuanwu Hospital of Capital Medical University, Department of Neurology, Beijing, China, 3Xuanwu Hospital of Capital Medical University, Department of Neurosurgery, Beijing, China, 4Capital Medical University, Capital Medical University, Beijing, China, 5Cooper University Health Care, Department of Neurology, Camden, United States
On behalf of:
Background and aims: Two recent clinical trials (ATTENTION and BAOCHE) demonstrated superiority of endovascular therapy over medical management for stroke due to basilar-artery occlusion. The aim of this study was to evaluate 1-year evidence of benefit of thrombectomy for these patients.
Methods: BAOCHE was an investigator-initiated, multi-center, open-label, randomized, controlled trial with blinded outcome evaluation conducted in China. Patients with basilar-artery stroke who presented between 6 to 24 hours after symptom onset were assigned, in a 1:1 ratio, to receive either medical therapy plus thrombectomy or medical therapy only. The primary outcome for this pre-specified secondary analysis was the proportion of patients achieving good functional status defined as modified Rankin Scale (mRS) 0-3 at 1-year follow-up in an intention-to-treat population. The trial is registered at ClinicalTrials.gov (NCT02737189).
Results: Enrollment was halted at a pre-specified interim analysis because of the superiority of thrombectomy. A total of 217 patients were included in the analysis. Thrombectomy led to a higher percentage with good functional status at 1-year than medical therapy alone.
Conclusions: In patients with stroke due to basilar-artery occlusion, the benefit of thrombectomy noted at 90 days was sustained at 12 months.
MRS of 0-3 and death at 90 Days and 1-Year According to Treatment Assignment.
Disclosures of Interest: No
Abstract N°: 4131
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
STROKE LATERALITY ASSOCIATION WITH CLINICAL OUTCOMES AND THROMBECTOMY TREATMENT EFFECT IN PATIENTS WITH LARGE CORE STROKES FROM SELECT2 TRIAL
Marc Ribo Jacobi*1, Michael Abraham2, Michael Chen3, M Shazam Hussain4, Santiago Ortega-Gutierrez5, Leonid Churilov6, Clark Sitton7, Ameer Hassan8, Bruce Campbell9, Amrou Sarraj10
1Vall D'hebron Hospital, Neurology, Spain, 2University of Kansas Medical Center, Neurology, United States, 3Rush University Medical Center, Neurology, Chicago, United States, 4Cleveland Clinic, Neurology, Cleveland, United States, 5University of Iowa, Neurology, United States, 6University of Melbourne, Medicine, Melbourne, Australia, 7UT McGovern Medical School, Radiology, Houston, United States, 8Valley Baptist Hospital, United States, 9University of Melbourne, Neurology, Melbourne, Australia, 10University Hospitals Cleveland Medical Center, Neurology, Cleveland, United States
On behalf of: SELECT2 investigators
Background and aims: Whether stroke laterality modifies thrombectomy treatment effect in patients with large core strokes is unknown.
Methods: From SELECT2 trial, patients were stratified based on the stroke laterality and their association with clinical outcomes and thrombectomy treatment effect was evaluated. Functional outcome, measured using modified Rankin Scale scores(with scores of 5 & 6 combined) was the primary outcome.
Results: Of 352 randomized patients, 196(56%) had occlusion involving right hemispheric circulation(98 EVT, 98 MM); whereas 156(44%, 82 EVT, 74 MM) had left hemisphere involvement. Baseline characteristics were largely similar between those with left vs right hemisphere involvement, except for higher stroke severity(Left: 22(19-25) vs right: 17(14-19), p<0.001). Overall, EVT treatment effect was preserved across both left hemisphere(aGenOR: 1.79, 95% CI:1.31-2.45) and right hemisphere(aGenOR: 1.64, 95% CI:1.20-2.26), without significant heterogeneity(p-int: 0.73). Similar results were observed for independent ambulation(left: aRR: 2.84, 95% CI:1.56-5.18 vs right: aRR: 1.74, 95% CI:1.16-2.61, p-int: 0.18) & complete dependence or death(mRS 5-6)(left: aRR: 0.72, 95% CI:0.58-0.91 vs right: aRR: 0.79, 95% CI:0.60-1.04, p-int: 0.79). No heterogeneity was observed for left vs right hemisphere across volume strata of ⩾70ml(p-int: 0.87); ⩾100ml(p-int:0.34) and ⩾150ml(p-int:0.71) or ASPECTS of 3(p-int:0.25); 4(p-int:0.72) and 5(p-int:0.60). Treatment effect was also preserved at 1-year follow-up(left: aGenOR: 1.79, 95% CI:1.31-2.45 vs right: aGenOR: 1.64, 95% CI:1.20-2.26, p-int 0.96).
Conclusions: In patients presenting with large core strokes, involvement of left hemisphere was associated with worse clinical presentation. However, EVT treatment effect was preserved without significant effect modification by stroke laterality across ASPECTS and core volume strata.
Disclosures of Interest: Yes Dr. Sarraj is the principal investigator of SELECT and SELECT2 trials, funded by Stryker Neurovascular through research grants to UT McGovern Medical School and UH Cleveland Medical Center.
Abstract N°: 4174
Category: 1.01 ACUTE MANAGEMENT - Neither thrombolysis nor thrombectomy
INTRAVENOUS GLIBENCLAMIDE FOR LARGE HEMISPHERIC INFARCTION: ANALYSIS OF BASELINE LESION VOLUME IN THE CHARM TRIAL
W. Taylor Kimberly*1, Kevin Sheth2, Gregory W. Albers3, Bruce Campbell4, Charlotte Cordonnier5, H.E. Hinson6, Bradley Molyneaux7, Nogueira Raul G8, Jeffrey Saver9, On Behalf of the Charm Study10
1Massachusetts General Hospital, Neurology, Boston, United States, 2Yale University, New Haven, United States, 3Stanford University, Stanford, United States, 4The University of Melbourne, Parkville, Australia, 5University of Lille, Lille, France, 6University of California San Francisco Parnassus Campus, San Francisco, United States, 7Brigham and Women's Hospital, Boston, United States, 8UPMC Presbyterian, Pittsburgh, United States, 9Peter Morton Medical Building - UCLA Medical Center, Los Angeles, United States, 10Various Institutions
On behalf of: Thorsten Steiner, Kazunori Toyoda, Max Wintermark, J. Marc Simard, Thomas W. MacAllister, Ann C. Tunstall, Mark Etherton, Michael Wald, Sven Jacobson
Background and aims: The CHARM trial evaluated the safety and efficacy of intravenous glibenclamide as a treatment for ischemic stroke patients at high risk for cerebral edema. It is not known whether the treatment effect varies based on size of presenting stroke.
Methods: CHARM subjects who were enrolled with CTP or DWI volume >80mL were included in this analysis. The primary endpoint was the 90-day mRS and analysis included participants aged ⩽70 years who received any study drug. An interaction term between treatment and stroke volume was included in an ordinal logistic regression model with 90-day mRS (0/1, 2, 3, 4, 5/6) as the dependent variable. Independent variables included age, sex, baseline NIHSS, world region, tPA, and thrombectomy.
Results: Of the 431 subjects that comprised the mITT population, 280 (65%) had baseline stroke volume assessed on CTP or DWI. The mean age was 58±9 years, baseline NIHSS was 19 [16-23], and baseline infarct volume was 140mL [104-186]. There was interaction between glibenclamide and baseline stroke volume of ⩽120mL (p=0.031), with a favorable outcome among glibenclamide-treated subjects in the ⩽120mL subgroup (n=105, cOR 2.31, 95%CI 1.07-5.01, adjusted p=0.034). Among thrombectomy-treated subjects (n=81), there was a glibenclamide-by-stroke volume interaction (p=0.009), and glibenclamide-treated subjects had a favorable outcome (cOR 4.69, 95%CI 1.10-20.1, p=0.037).
Conclusions: This exploratory analysis supports the hypothesis that glibenclamide may be associated with improved functional outcome depending on baseline stroke volume. Confirmation of these results would identify a group of stroke patients who may benefit from treatment with glibenclamide.
Disclosures of Interest: Yes WTK, KNS: research funding related to the conduct of the trial; JMS: holds a patent related to glibenclamide, is a member of the Board of Directors and holds shares in Remedy Pharmaceuticals; MW: current Biogen employee; TWM, ACT, SJ: current Remedy Pharmaceuticals employee.
Disclosures of Interest: No
Moderated Poster - Diagnosis and Imaging
Abstract N°: 1687
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
MRI SELECTION FOR THROMBECTOMY IN ISCHEMIC STROKE:A PROSPECTIVE MULTICENTER RANDOMIZED TRIAL OF FVH-DWI MISMATCH VERSUS PERFUSION
Ming Wei*1, Leilei Luo2, Fanlei Meng3
1Tianjin Huanhu Hospital, Tianjin, China, Department of Neurosurgery, Tianjin, China, 2Tianjin Huanhu Hospital, Tianjin, China, Department of Neurology, Tianjin, China, 3he Second Hospital of Tianjin Medical University, Tianjin, China, Department of Neurosurgery, Tianjin, China
On behalf of:
Background and aims: Perfusion imaging and intelligent analysis software recommended by the guidelines for patient selection in endovascular thrombectomy are not widely available. Therefore, FVH-DWI mismatch may be a simpler surrogate biomarker that provides an alternative to PWI- or clinical-DWI mismatch. However, the consistency between FVH-DWI and perfusion mismatch has not been extensively studied.
Methods: We conducted a multicenter, prospective, randomized controlled, open-label, blinded outcome assessment with a non-inferiority design, in patients with thrombectomy, 6-24 hours from onset, with acute large-vessel occlusion in the anterior circulation, at thirteen centers in China. Patients with an Alberta Stroke Program Early Computed Tomography Score of 6 to 10 and a National Institutes of Health Stroke Scale greater than 6 were randomly assigned in a 1:1 ratio to MR and perfusion groups. The primary outcome was 90-day functional independence rate, defined as a score of 0 to 2 on the modified Rankin scale (range, 0 [no symptoms] to 6 [death]). Safety outcomes included symptomatic intracranial hemorrhage (sICH), neurological deterioration, and 90-day mortality rate.
Results: The sample size of this trial is 352 cases, with 176 cases in each group. We have currently completed the enrollment of the 352 patients,and the follow-up will be completed in March 2024.We look forward to releasing our final results in ESOC 2024.
Conclusions: FVH-DWI mismatch may be a simpler and more available alternative biomarker in selecting patients for endovascular thrombectomy.
Disclosures of Interest: No
Moderated Poster – Prevention
Abstract N°: 4230
Category: 1.03 PREVENTION
DUAL VERSUS SINGLE ANTIPLATELET THERAPY IN PATIENTS WITH ACUTE ISCHEMIC NON-CARDIOEMBOLIC STROKE AND AVAILABLE CMRI
Gian Marco De Marchis*1,2, Anna Toebak1,2, Tolga Dittrich1,2, Angela Wang3, Ashkan Shoamanesh3, Eric Smith4, Hardi Mundl5, Pablo Colorado6, Stuart Connolly3, Robert Hart3
1Cantonal Hospital St. Gallen, Department of Neurology and Stroke Center, 2University of Basel, Department of Clinical Research, 3McMaster University, Population Health Research Institute, 4Hotchkiss Brain Institute, Cumming School of Medicine, University of Calgary, Department of Clinical Neuroscience, Calgary, Canada, 5Bayer AG, TA Thrombosis and Vascular Medicine, Wuppertal, Germa, 6Bayer US Pharmaceuticals, Hanover, United States
On behalf of:
Background and aims: The POINT/CHANCE trials enrolled patients with non-cardioembolic stroke with NIHSS⩽3. Dual antiplatelet therapy (DAPT) is superior to single antiplatelet therapy (SAPT), at the expense of more bleedings. We aimed to assess whether stroke size on baseline MRI modified the efficacy and safety of DAPT over SAPT.
Methods: Post-hoc analysis of the PACIFIC-STROKE Trial, which enrolled patients with non-cardioembolic stroke and NIHSS⩽15. Participants were prescribed antiplatelet treatment at physician’s discretion and randomized to placebo or Asundexian, a factor XIa inhibitor. The efficacy endpoint was the rate of recurrent symptomatic ischemic stroke, the safety endpoint major or clinically relevant non-major bleeding during follow-up. On baseline MRI, stroke size was dichotomized at >15mm versus ⩽15mm.
Results: Among 1590 patients eligible for this analysis (32% NIHSS >3), 634 (40%) received DAPT. Median follow-up was 11.5 months. 642(40.4%) were CHANCE/POINT non-eligible (Table 1). In the overall population, comparing DAPT vs. SAPT we did not observe a significant difference for the efficacy endpoint, however, an increase of safety endpoints with DAPT (OR 1.725, CI: 1.006-2.958). In the CHANCE/POINT eligible group, we observed a trend towards superiority of DAPT over SAPT for the efficacy endpoint, at the expense of more safety endpoints. Interaction analysis stratified by the size of the qualifying stroke on baseline MRI was not significant (Table 2, 3).
Conclusions: In the PACIFIC-STROKE population, infarct size in the baseline MRI does not appear as a viable tool to broaden the indication for DAPT beyond the CHANCE/POINT eligibility criteria.
Disclosures of Interest: Yes Authors were part of the steering committee of PACIFIC Stroke
Moderated Poster - Rehabilitation and Outcomes
Abstract N°: 4228
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
HEALTH-RELATED QUALITY OF LIFE AMONG PATIENTS WITH ACUTE ISCHEMIC STROKE AND LARGE VESSEL OCCLUSION IN THE RESILIENT TRIAL
Gisele Sampaio*1, Raul Nogueira2, Octavio Pontes3, Fabrício Oliveira Lima4, Francisco Mont'alverne5, Leticia Rebello6, Jose Antonio Fiorot Junior7, Viviane DE H. Zetola8, Fabricio Cardoso9, Sheila Cristina Ouriques Martins10
1Universidade Federal de São Paulo (UNIFESP) e HIAE, 2University of Pittsburgh, 3Universidade de São Paulo Ribeirão Preto, 4Hospital Geral de Fortaleza, Neurology, 5Hospital Geral de Fortaleza, 6Hospital de Base de Brasília, 7Hospital Estadual Central de Vitória, 8Universidade Federal do Paraná, 9Universidade Estadual de Campinas, 10Universidade Federal do Rio Grande do Sul
On behalf of: for the RESLIENT trial investigators
Background and aims: Endovascular thrombectomy (EVT) is effective in reducing 90-day disability in patients with acute ischemic stroke caused by large vessel occlusion. However, there is limited understanding of patient-reported outcome measures, particularly in low- and middle-income countries.
Methods: The RESILIENT trial, a prospective multicenter randomized clinical trial conducted in Brazil, assessed the impact of EVT on proximal vessel occlusion in acute ischemic stroke compared to standard care within 8 hours of symptom onset. EuroQol-5D (EQ-5D) 3L outcomes were evaluated at 90 days post-stroke, with EQ-5D index scores calculated using the Brazilian valuation algorithm. We used the Wilcoxon Rank Sum Test to evaluate the association between EVT and EQ-5D index scores and ordinal regression for the association between EVT and EQ-5D status among 90-day survivors for each EQ-5D dimension.
Results: Of the 221 patients enrolled, 111 were randomized to EVT and 110 to control. At 90 days, 54 patients (24%) had died, and 14/169 (8.2%) had missing EQ-5D values. Median EQ-5D was significantly higher in the EVT group compared to best medical management (0.44 versus 0.21, p=0.01). EVT resulted in improvements within all EQ-5D domains of ( mobility OR 1.96, 95% CI [1.05, 3.73], p=0.03), self-care ( OR 2.67, 95% CI [1.45, 4.98, p<0.01), usual activities (OR 2.27, 95% CI [ 1.24, 4.2], p<0.01), anxiety/depression (OR 1.96, 95% CI 1.05, 3.69], p=0.03) and pain/discomfort OR=1.90 95% CI 1.02- 3.57, p=0.04).
Conclusions: EVT-treated patients in the RESILIENT trial showed marked improvements in health-related quality of life across multiple dimensions.
Disclosures of Interest: Yes Supported by the Ministry of Health of Brazil, Departamento de Ciência e Tecnologia, Conselho Nacional de Desenvolvim- ento Científico e Tecnológico (grant numbers 402401/2013-1; 401821/2015-3; 402388/2013-5; and 443861/2018-8), with unre- stricted grants for device or software donations from Medtron- ic, Penumbra, iSchemaView, Brainomix, and Allm.
Abstract N°: 4147
Category: 1.04 REHABILITATION & RECOVERY
A MESSAGE FRAMING GUIDED RECURRENCE RISK COMMUNICATION PROGRAMME FOR ISCHAEMIC STROKE PATIENTS: A RANDOMISED CONTROLLED TRIAL
1Zhengzhou University, Nursing and Health School, Zhengzhou, China
On behalf of:
Background and aims: Recurrence risk communication could help promote health behaviour, but how to communicate risk needs to be explored. This study explores the effectiveness of a Message-framing-guided, Recurrence Risk Communication (MRRC) programme in ischaemic stroke patients.
Methods: A three-arm randomised controlled trial was performed. A total of 141 participants were divided into the loss-framing group(n=47), the gain-framing group(n=48) and the control group(n=46). Patients in intervention groups received an 8-week MMRC programme based on loss-frame or gain-frame, respectively. Perceived risk of stroke recurrence, health behavioural decision-making, health behaviour, self-efficacy, and anxiety were measured at baseline(T0), immediately(T1), 1 month(T2) and 3 months(T3) after intervention. The registration number is ChiCTR20000034244.
Results: Participants in the gain and loss framing groups had significantly better recurrence risk perception, behavioural decision-making, health behaviour and self-efficacy at T1, T2, and T3 than the control group. Moreover, patients in the loss-framing group showed better health behaviours(P<0.05), perceived severity (P<0.001), physical activity(P<0.05), and smoking/alcohol cessation(P<0.05) than those in the gain-framing group. Inversely, patients in the gain-framing group showed higher self-efficacy(P<0.05). In addition, patients in the loss framework group showed a higher level of anxiety than those in the control group immediately after intervention (P = 0.021 < 0.05).
Conclusions: Loss framing might be more convincing in promoting health behaviours, and it seemed not to elicit strong, excessive negative emotions in stroke patients. Message framing helps develop recurrence risk communication and foster patients’ health behaviour.
Acknowledgements: Thanks to all the participants who contribute their time and effort in this study.
Disclosures of Interest: No
Moderated Poster - SAH and ICH
Abstract N°: 1417
Category: 1.03 PREVENTION
PREVENTION OF HYPERTENSIVE INJURY TO THE BRAIN BY INTENSIVE TREATMENT AFTER INTRACEREBRAL HAEMORRHAGE: 1-YEAR NEUROIMAGING FOLLOW-UP RESULTS
Philip Nash*1,2, Iain Mcgurgan3, Baris Kanber4, Ferran Prados Carrasco4, David Thomas5, Beatriz Gomez-Anson6,7, Hans Rolf Jager6, Frederik Barkhof8,9, Peter Rothwell3, David Werring1,2
1UCL Queen Square Institute of Neurology, Stroke Research Centre, London, United Kingdom, 2National Hospital for Neurology and Neurosurgery, University College London Hospitals NHS Trust, Comprehensive Stroke Service, London, United Kingdom, 3University of Oxford, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom, 4UCL Queen Square Institute of Neurology, NMR Research Unit, Queen Square Multiple Sclerosis Centre, Department of Neuroinflammation, London, United Kingdom, 5UCL Queen Square Institute of Neurology, Dementia Research Centre, Department of Brain Repair and Rehabilitation, London, United Kingdom, 6UCL Queen Square Institute of Neurology, Lysholm Department of Neuroradiology and the Neuroradiological Academic Unit, Department of Brain Repair and Rehabilitation, London, United Kingdom, 7Corachan Clinic, Barcelona, Spain, 8UCL Queen Square Institute of Neurology, 9Queen Square Institute of Neurology and Centre for Medical Image Computing, London, United Kingdom, 9Amsterdam UMC, Vrije Universiteit, Department of Radiology & Nuclear Medicine, Amsterdam, Netherlands
On behalf of: The PROHIBIT-ICH Collaborators
Background and aims: PROHIBIT-ICH investigated whether centrally-coordinated intensive blood pressure treatment, via remote-telemetric home-BP monitoring (RT-HBPM): (1) is safe; or (2) modifies progression of cerebral small vessel disease (SVD) after intracerebral haemorrhage (ICH).
Methods: We recruited patients to a parallel-group, open-label, randomised (1:1) trial of 3 months of RT-HBPM-guided treatment versus standard care. White matter hyperintensity (WMH) lesion masks were obtained using automated pipelines and manually corrected. The primary outcome was change in WMH volume at follow-up.
Results: 15 UK hospitals recruited 86 patients (mean age 67.5±12.5 years, 26% female). 58 underwent MRI at baseline and follow-up. The median (IQR) WMH volume change was -0.1 (-1.7 to 2.4) ml in the intervention group and 0.4 (-1.5 to 3.3) in the control group. Analysis using a linear regression model estimates a follow-up volume of -3.2% (95% CI -19.2% to +15.9%) in the intervention group compared to the control group, but this was not statistically significant (p=0.718). There were with 5 clinical events (1 ischemic stroke, 2 ICH, 1 dementia diagnosis and 1 death) in 2 participants in the control group and none in the intervention group. There was a significant association of WMH volume change and BP change at follow-up; a 10-mmHg systolic BP decrease predicted an 8% WMH volume decrease (95% CI 4 to 12%, p<0.001).
Conclusions: BP reduction via RT-HBPM after ICH is safe, with no adverse clinical outcomes. Reduction of systolic BP at follow-up was independently associated with a reduction in WMH volume. Further randomised studies might determine whether this approach prevents recurrent stroke.
Disclosures of Interest: No
Moderated Poster - Small Vessel Disease and Cognition
Abstract N°: 4203
Category: 1.03 PREVENTION
EFFECT OF A SMARTPHONE-BASED MULTI-DOMAIN INTERVENTION ON COGNITION IN POPULATION WITH HIGH RISK OF STROKE: A RANDOMIZED CONTROLLED TRIAL
Wansi Zhong*1, Ying Zhou1, Min Lou1
1The second affiliated hospital of Zhejiang University, school of medicine, Neurology, Hangzhou, China
On behalf of:
Background and aims: Prevention of cognitive decline for individuals with high risk of stroke is largely unknown and the management is a very troublesome issue. This study aims to assess the effect of the smartphone-based multidomain intervention on cognition in participants with high risk of stroke.
Methods: In this randomized clinical trial, participants were recruited between June 21, 2020, and August 05, 2021 in China. Participants were randomized in a 1:1 ratio to a intervention group or a control group. The intervention group received 12-month smartphone-based multidomain intervention, including management of risk factors, cognitive training, management of sleep health, and management of mental health. The control group received regular health advice. The primary outcome was the change in global cognitive score.
Results: A total of 238 participants (age, 59 [6.7] years; 90 [37.8%] women) were randomized to the intervention group (n=119) or control group (n=119), of whom 217 were included in the modified intention-to-treat analysis. Estimated mean change in global cognitive total Z score was 0·10 (0.04, 0.39) in the intervention group and -0.05 (0.03, 0·29) in the control group. Intervention group underwent an improved change of global cognitive score per year, compared with the control group (MD: 0·101, 95% CI 0.041–0.161, p=0.001). We also noted a significant intervention effect for visuomotor speed (p=0·037) and visuospatial function (p=0.027).
Conclusions: The smartphone-based multidomain intervention improved global cognitive function among individuals with high risk of stroke, providing a feasible therapeutic option for management of brain health.
Disclosures of Interest: No
Paper Poster - Acute Management
Abstract N°: 1397
Category: 1.01 ACUTE MANAGEMENT - Neither thrombolysis nor thrombectomy
PREHOSPITAL DIFFERENTIAL DIAGNOSIS OF ACUTE STROKE PATIENTS BY MEASURING THE PLASMA RELEASE RATE OF GFAP
Olli Mattila*1, Heini Harve-Rytsälä2, Saana Pihlasviita1, Gerli Sibolt1, Tiina Nukarinen1, Sami Curtze1, Daniel Strbian1, Turgut Tatlisumak1, Markku Kuisma2, Perttu Lindsberg1
1University of Helsinki and Helsinki University Hospital, Neurology and Clinical Neurosciences, Finland, 2University of Helsinki and Helsinki University Hospital, Department of Emergency Care, Finland
On behalf of: The Helsinki Ultra-acute Stroke Biomarker Study
Background and aims: Plasma glial fibrillary acidic protein (GFAP) is a promising biomarker candidate for differentiating hemorrhagic stroke (HS) from acute cerebral ischemia (ACI) and stroke mimics (SM) in the prehospital setting when neuroimaging is not available, to aid in early prehospital triage. Proof of concept data suggest that following the prehospital release rate of GFAP with sequential sampling significantly improves its diagnostic performance, but validation in a large clinical cohort is still warranted before further prehospital trials.
Methods: We designed a prospective diagnostic clinical study aiming to define the early diagnostic performance of GFAP in patients with suspected acute stroke. The study prospectively recruited 1015 patients with suspected acute stroke transported by ambulance to a tertiary stroke center for recanalization therapies and included ultra-early serial blood sampling beginning in the ambulance setting. In March 2024 we gained access to a novel highly sensitive and rapid measurement technique for plasma GFAP and aim to utilize this method to provide further insight into the utility of GFAP in acute stroke, to be presented at ESOC 2024.
Results: TBA
Conclusions: TBA
Disclosures of Interest: No
Abstract N°: 2238
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
PROSPECTIVE OBSERVATIONAL COHORT STUDY OF TENECTEPLASE: RESULTS FROM INDIAN REGISTRY IN ISCHEMIC STROKE- TENECTEPLASE (IRIS-TNK)
Amit Saraf*1, Usha Kant Misra2, Jayantee Kalita3, Bhalchandra Vaidya1, Mark Parsons4, Sanjay Singh1
1Gennova Biopharmaceuticals Limited, Pune, India, 2Apollomedics Super Specialty Hospital, Neurology, Lucknow, India, 3Sanjay Gandhi Post Graduate Institute of Medical Sciences, Neurology, Lucknow, India, 4Liverpool Hospital, University of New South Wales, Neurology, Liverpool (Sydney), Australia
On behalf of: Indian Registry in Ischemic Stroke-Tenecteplase (IRIS-TNK) Investigators
Background and aims: Indian made tenecteplase has been approved since 2016 for acute ischemic stroke treatment at 0.2 mg/kg dose by the Indian licensing authority. A registry to evaluate the safety of Indian tenecteplase was mandated by the licensing authority. Aims: To evaluate the safety and effectiveness of tenecteplase (0.2 mg/kg dose) in ischemic stroke patients in India.
Methods: A prospective, registry-based observational, cohort study was designed to assess the safety and clinical outcomes in patients treated with tenecteplase. The primary outcome was the proportion of symptomatic intracerebral haemorrhages at 36 ± 6 h post treatment. Secondary outcomes included improvement on NIHSS score and 3- months functional outcomes based on modified Rankin Scale score.
Results: A total of 1015 patients with median (IQR) age 62 (52-71) years, were recruited from 20 sites. The median (IQR) baseline NIHSS score was 9 (7 - 12). A total of 38 (3.7%) patients were lost to follow-up during the study. The proportion of patients with symptomatic ICH was 0.6% (95% CI: 0.1 - 1.1) and 10 patients (1%, 95% CI: 0.4 - 1.7) died within 3- months post stroke. Improvement on NIHSS score by ⩾4 points or 0 was observed in 34.4% (95% CI: 31.5 - 37.4) patients at 24 h. The excellent outcome and functional independence at 3- months was achieved in 55.4% (95% CI: 52.3 -58.5) and 75.1% (95% CI: 72.4 -77.8) patients respectively.
Conclusions: Tenecteplase at 0.2 mg/kg dose is safe in routine clinical practice when administered within 4.5 h of symptom onset.
Disclosures of Interest: Yes The study is being funded by Gennova Biopharmaceuticals Limited. Dr. Amit Saraf is an employee of Gennova Biopharmaceuticals Limited.
Abstract N°: 2426
Category: 1.01 ACUTE MANAGEMENT - Neither thrombolysis nor thrombectomy
DO AI-MACHINE LEARNING MODELS OUTPERFORM STATISTICAL REGRESSION FOR DIAGNOSIS OF ACUTE STROKE? RESULTS FROM THE SAVANNAS STUDY
Lisa Woodhouse*1, Xin Chen2, Jonathan Garibaldi2, Diane Havard1, Alan Montgomery3, Terence J Quinn4, Nikola Sprigg1, Philip Bath1
1University of Nottingham, Stroke Trials Unit, Mental Health & Clinical Neurosciences, Nottingham, United Kingdom, 2University of Nottingham, School of Computer Sciences, Nottingham, United Kingdom, 3University of Nottingham, Nottingham Clinical Trials Unit, Nottingham, United Kingdom, 4University of Glasgow, Academic Geriatric Medicine, Glasgow, United Kingdom
On behalf of: SAVANNAS Collaborators
Background and aims: Stroke is common and can be mimicked by other conditions. We assess here the accuracy of machine learning and statistical regression models for the diagnosis of acute stroke.
Methods: High-fidelity data on patients with acute stroke were sought. Data include trial characteristics, patient demographics, baseline clinical data and final diagnosis (stroke, TIA, mimic). We used machine learning models (artificial neural networks, deep neural networks and random forest) and regression models (binary logistic regression, Bayesian binary logistic regression). These modelling methods will be compared for diagnosis of acute stroke/TIA versus mimic. We developed models using all available covariates, the most collected characteristics and selection model, using an optimal covariate list determined using backwards elimination.
Results: The Statistical Analysis Versus Artificial Neural Networks in Acute Stroke (SAVANNAS) collaboration has received individual participant data for 79 trials/studies and consists of 112,083 patient records. Overall, 92,701 (82.7%) had a diagnosis of ischaemic stroke, 13,177 (11.7%) ICH, 3,899 (3.5%) TIA and 2,306 (2.1%) a stroke mimicking condition. For diagnosis prediction, the performance of models was better for training versus test data sets. When considering the test datasets, the accuracy and AUCs were superior with BLR (selection model AUC 0.82, 95% CI 0.76-0.88) performing better than the AI-ML approaches (for all comparisons with BLR, p<0.001). Bayesian BLR was slightly inferior. Of the AI-ML approaches, RF classification (accuracies 0.72-0.73 across models) was more accurate in predicting diagnosis than the others.
Conclusions: In general, BLR tended to perform better than AI-ML when diagnosing stroke/TIA vs. Mimic.
Disclosures of Interest: No
Abstract N°: 2454
Category: 1.01 ACUTE MANAGEMENT - Neither thrombolysis nor thrombectomy
DOES AI-MACHINE LEARNING OUTDO STATISTICAL REGRESSION FOR OUTCOME PREDICTION AFTER ACUTE STROKE? RESULTS FROM THE SAVANNAS STUDY
Lisa Woodhouse*1, Xin Chen2, Jonathan Garibaldi2, Diane Havard1, Alan Montgomery3, Terence J Quinn4, Nikola Sprigg1, Philip Bath1
1University of Nottingham, Stroke Trials Unit, Mental Health & Clinical Neurosciences, Nottingham, United Kingdom, 2University of Nottingham, School of Computer Sciences, Nottingham, United Kingdom, 3University of Nottingham, Nottingham Clinical Trials Unit, Nottingham, United Kingdom, 4University of Glasgow, Academic Geriatric Medicine, Glasgow, United Kingdom
On behalf of: SAVANNAS Collaborators
Background and aims: Stroke is common and often has a poor outcome. The Statistical Analysis Versus Artificial Neural Networks in Acute Stroke (SAVANNAS) study assessed the accuracy of machine learning (AI-ML) models and regression methods for predicting post-stroke outcomes.
Methods: Data included patient demographics, clinical data, final diagnosis and outcome measures. We used AI-ML models (neural networks [ANN/DNN], RPART and random forest [RF]) and regression models (binary, ordinal and linear, including Bayesian-approaches). These were compared for prediction of end-of-trial death and dependency. We developed models using all available covariates, the most collected characteristics and selection models, using an optimal covariate list determined using backwards elimination. We also considered the inclusion of early stroke impairment, using NIHSS.
Results: SAVANNAS received data from 79 studies/trials and consists of 109,777 acute stroke/TIA patient records. For mortality (n=107,879), most models found that AI-ML approaches were comparable to BLR (accuracies for test data (0.65-0.71). The inclusion of early follow-up NIHSS score improved prediction, e.g. selection models AUC BLR 0.88 with NIHSS vs 0.76 without. For dependency (mRS>1, n=82,203) although ANN and RF did not differ statistically from BLR (AUC 0.77, 95% CI 0.73-0.81) for selection models when comparing test results, DNN and RPART were inferior. The inclusion of early follow-up NIHSS score in the models improved prediction, e.g. selection models AUC BLR 0.83 with NIHSS vs 0.77 without.
Conclusions: Regression tended to perform similarly to AI-ML when predicting outcomes. Unsurprisingly, the inclusion of data regarding stroke impairment improved the predictive ability of models.
Disclosures of Interest: No
Paper Poster - Rehabilitation and Recovery
Abstract N°: 4158
Category: 1.04 REHABILITATION & RECOVERY
SPEECH THERAPY COMBINED WITH CEREBROLYSIN IN ENHANCING APHASIA RECOVERY AFTER ACUTE ISCHEMIC STROKE: ESCAS PILOT STUDY
Dafin-Fior Muresanu*1
1Cluj-Napoca, Neurosciences, Cluj-Napoca, Romania
On behalf of:
Background and aims: Stroke-induced aphasia significantly impacts communication and quality of life. Despite the standard treatment being speech and language therapy (SLT), outcomes vary, highlighting the need for additional therapies. Cerebrolysin, a neuroprotective and neurotrophic agent, has shown potential in stroke management. This study examines the effectiveness of combining Cerebrolysin with SLT in treating post-stroke aphasia.
Methods: The ESCAS trial, a prospective, randomized-controlled, double-blinded phase 4 study, was conducted in two Romanian stroke centers. Participants included those with left middle cerebral artery territory ischemic stroke and Broca or mixed non-fluent aphasia, enrolled 3-5 days post-stroke. Inclusion criteria were right-handedness and Romanian as mother tongue; exclusion criteria were prior strokes, severe comprehension deficits, contraindications to MRI, and pre-existing neurodegenerative or psychiatric diseases. Participants received Cerebrolysin or a placebo combined with SLT in ten-day cycles over three intervals.
Results: Out of 132 enrolled patients, 123 were included in the Intention To Treat analysis, and 120 in the Per Protocol analysis. The Cerebrolysin group showed significant improvement in Western Aphasia Battery scores (p < 0.001) and National Institutes of Health Stroke Scale scores (p < 0.001). Modified Rankin Scale and Barthel index scores also improved, with notable differences at the final study visit (Day 90). Safety analysis raised no concerns.
Conclusions: Cerebrolysin combined with SLT offers promising potential for enhancing recovery in post-stroke aphasia. Significant improvements were observed in language and neurological deficits, underscoring the importance of adjunctive therapies in aphasia rehabilitation. Further research with larger cohorts is needed to fully establish the efficacy of this combination therapy.
Disclosures of Interest: Yes D.M. discloses discloses major financial activities (travel/accommodation/meeting expenses) with the Foundation for the Study of Nanoneuroscience and Neuroregeneration.
E-Poster - Acute and Hyperacute Management
Abstract N°: 1492
Category: 1.01 ACUTE MANAGEMENT - Neither thrombolysis nor thrombectomy
PHYSICAL AND PSYCHOLOGICAL IMPACT OF STROKE ON CARERS AND RELATIVES
Julia Marshall*1, Jonathan Hewitt1, Rhian Daniel1
1University Hospital of Wales, United Kingdom
On behalf of:
Background and aims: Stroke can have significant physical and psychological impacts on carers and relatives. This cross-sectional study aimed to examine the effects of stroke on carers and relatives in Scotland, Wales, and England.
Methods: A total of 1,291 participants completed an online questionnaire. Participants were recruited through various channels, including HealthWise Wales, the NHS portfolio, social media, and collaborations with charities and organizations. Three groups were identified: stroke carers, other carers, and non-carers. Data were collected using a background questionnaire, health neglect questions, SF-36 Health Survey, GAD-7, PHQ-9, caregiving questionnaire, modified Abbreviated Mental Test (m-AMT), and Barthel Index (BI).
Results: The analysis of the collected data is currently ongoing, and no specific findings can be reported at this time.
Conclusions: This study aims to shed light on the significant physical and psychological impact experienced by carers and relatives of stroke survivors. The ongoing analysis will provide valuable insights into the challenges faced by stroke carers and the importance of support and resources to address their unique needs.
Disclosures of Interest: No
Abstract N°: 1999
Category: 1.01 ACUTE MANAGEMENT - Neither thrombolysis nor thrombectomy
NEURORADIOLOGICAL PATTERNS OF STROKE IN AN ICU COHORT WITH SEVERE COVID-19: PANDEMIC STUDY ANALYSIS
Rebecca Jöbges*1, Moritz Schmidbauer2, Robert Forbrig3, Konstantinos Dimitriadis2, Julian Bösel4
Background and aims: The PANDEMIC study explored neurological disorders in ICU patients with COVID-19. Cerebrovascular events like Acute Ischaemic Stroke (AIS) and intracerebral hemorrhage (ICH), were associated with heightened morbidity and mortality.
Methods: Imaging data from the PANDEMIC study was analyzed by two reviewers to identify the neuroradiological pattern of strokes in an ICU cohort. Data was stratified into radiological pattern, localization, space occupying effect, progress, and acuity.
Results: Out of 392 PANDEMIC study patients, 242 imaging studies from 113 (28.82%) patients were analyzed. Demographics revealed 28 females (24.77%), 83 males (73.45%), and 2 of unknown sex. Median age was 65 years (SD 12.26). ECMO therapy was administered in 44 cases (38.9%). Among the 63 cases with new intracranial pathology, 18 (28.57%) were AIS, 34 (53.97%) were ICH, and 11 (17.46%) were non-cerebrovascular pathologies. 27 (42.85%) patients received ECMO treatment and exhibited AIS (n4 /9%) and ICH (n23/52%). 14 (77,78%) of the AIS cases presented with MCA territory infarction, 3 (11.11%) with PCA stroke, 1 (5.56%) with SCA territory stroke and 1 (5.56%) with PICA stroke. Of these cases, 2 were multi-territory infarctions (11.11%).Primary ICH cases presented 15 (44.15%) cases of atypical bleeds, 6 (17.64%) cases of subarachnoid bleeds, 5 (14.71%) cases of loco-typico bleeds, 2 (5.88%) cases with traumatic head injury, 2 (5.88%) cases of generalized multilocular microbleeds, 1 (2.94%) case of intraventricular bleeding, and 1 (2.94%) case of subdural hematoma.
Conclusions: Initial findings suggest an elevated incidence of haemorrhagic strokes.We acknowledge ECMO treatment skewed results towards hemorrhagic strokes.
Disclosures of Interest: No
Abstract N°: 4137
Category: 1.01 ACUTE MANAGEMENT - Neither thrombolysis nor thrombectomy
ISCHEMIC STROKE EVALUATED AT BED SIDE WITH ULTRASOUND - STAND STUDY
Laurine Bedoucha*1, Claire Gobron1, Peggy Reiner1, Candice Sabben2, Michael Obadia2, Perrine Boursin2, Dubus Estelle1, Fabrice Vallee1, Stéphanie Guey1, Lucas DI Meglio1
1Lariboisière Hospital AP-HP, Paris, France, 2Hospital Foundation Adolphe De Rothschild, Paris, France
On behalf of:
Background and aims: The optimal timing for transitioning stroke patients from prone to supine positions during the acute phase of ischemic stroke remains uncertain. Prior research has yielded conflicting outcomes and often failed to account for the influence of arterial stenosis or occlusion on cerebral blood flow regulation. This study seeks to determine if transitioning to a seated position early in the acute phase of ischemic stroke is linked with notable changes in intracranial hemodynamics, specifically considering the presence of upstream arterial stenosis or occlusion.
Methods: A prospective observational study with a 1:1 case-control design monitored cerebral and systemic hemodynamics noninvasively during the transition from prone to supine positions. Cases comprised patients with homolateral carotid stenosis >50% per NASCET criteria. Primary outcome measure was >10% decrease in mean flow velocity (MFV) in the homolateral middle cerebral artery (MCA) from supine to sitting.
Results: Among 42 screened patients, 36 (19 controls, 17 cases) were included. Nine cases (53%) versus one control (5%) experienced a >10% MFV decrease (p=0.0061, Figure 1). Notably, cases with MFV reduction showed no increase in arterial pressure during the transition. Factors associated with significant MFV decrease in cases included a shorter time from stroke onset to sitting (p=0.0008), lower mean arterial pressure (p=0.0295), lower hemoglobin level (p=0.0006), lower hematocrit (p=0.0206), and higher BNP levels (p=0.0196).
Conclusions: Early transitioning to a seated position during acute ischemic stroke more frequently leads to significant MFV decrease in the MCA among patients with carotid stenosis compared to those without, possibly due to systemic adaptation failure (Figure 2).
Disclosures of Interest: No
Abstract N°: 2487
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
RATIONALE AND DESIGN OF TREATMENT OF ACUTE ISCHAEMIC STROKE WITH EDARAVONE DEXBORNEOL II (TASTE-2): A MULTICENTRE RCT
Chunjuan Wang1,2,3, Hongqiu Gu1,2, Qiang Dong4, Anding Xu5, Ning Wang6, Yi Yang7, Feng Wang8, Yongjun Wang*1,2,3,9,10
1China National Clinical Research Center for Neurological Diseases, Beijing Tiantan Hospital, 2National Center for Healthcare Quality Management in Neurological Diseases, Beijing Tiantan Hospital, 3Department of Neurology, Beijing Tiantan Hospital, 4Huashan Hospital, Fudan University, Neurology, 5The First Affiliated Hospital of Jinan University,, Neurology, 6The First Affiliated Hospital, Institute of Neuroscience, Fujian Medical University, 7The First Hospital of Jilin University, Neurology, 8State Key Laboratory of Neurology and Oncology Drug Development, 9Chinese Institute for Brain Research, 10Research Unit of Artificial Intelligence in Cerebrovascular Disease, Chinese Academy of Medical Sciences
On behalf of:
Background and aims: Edaravone dexborneol is believed to be a novel cytoprotective agent, exhibiting synergistic antioxidative and anti-inflammatory effects in animal models. The TASTE trial demonstrated its superior efficacy over edaravone alone for acute ischaemic stroke (AIS) patients. However, its efficacy in individuals undergoing endovascular therapy (EVT) remains uncertain. The treatment of acute ischaemic stroke with edaravone dexborneol II (TASTE-2) trial was designed to investigate the efficacy and safety of edaravone dexborneol in patients with AIS and large-vessel occlusion (LVO) in the anterior circulation.
Methods: The eligible participants, presenting with a NIHSS score between 6 to 25 and an ASPECTS score between 6 to 10 within the initial 24 hours after symptom onset, will be randomly allocated to either the edaravone dexborneol group or the placebo group in equal proportions prior to thrombectomy. The treatment will be continuously administered for a duration of 10-14 days. A follow-up period of 90 days will be implemented for all participants in this study.
Results: The TASTE-2 trial is a multicenter, randomized, double-blind, placebo-controlled study. The primary efficacy outcome is defined as achieving favorable functional independence, measured by a mRS of 0-2 at 90 days. The primary safety outcome focuses on the incidence of serious adverse events.
Conclusions: The TASTE-2 trial will provide evidence to determine whether the administration of edaravone dexborneol in AIS patients undergoing EVT could yield significant improvements in neurological function.
Disclosures of Interest: No
Abstract N°: 4226
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
ENDOVASCULAR THERAPY FOR MILD ISCHEMIC STROKE WITH LARGE VESSEL OCCLUSION: SYSTEMATIC REVIEW AND META-ANALYSIS
Hong-Jie Jhou*1, Kuan-Chih Chen1, Po-Huang Chen2
1Changhua Christian Hospital, Department of Neurology, Changhua, Taiwan, 2Tri-Service General Hospital, National Defense Medical Center, Division of Hematology and Oncology, Department of Internal Medicine, Taipei, Taiwan
On behalf of:
Background and aims: The aim of study is to compare endovascular therapy (EVT) with best medical management (BMM) for mild stroke patients with large vessel occlusion.
Methods: We reviewed articles from PubMed, Cochrane, and Embase up to December 12, 2023. Patients were divided based on rescue EVT use: those given BMM but later EVT upon deterioration were labeled as the crossover group, while those receiving rescue EVT and remained in the BMM group were termed the non-crossover group.
Results: In the crossover group, EVT did not significantly alter the odds of achieving a modified Rankin scale (mRS) score of 0-1 (Figure 1A). However, in the non-crossover group, EVT significantly increased the likelihood of an mRS score of 0-1 (Figure 2A). No significant difference was observed in the rate of mRS scores of 0-2 in the crossover group (Figure 1B), unlike in the non-crossover group, where a significant difference was noted (Figure 2B). EVT did not significantly impact the rate of mRS scores of 0-3 in either group (Figure 1C; Figure 2C). A higher risk of symptomatic intracerebral hemorrhage (sICH) was observed with EVT in both the crossover (Figure 1D) and non-crossover groups (Figure 2D). Mortality at 3 months did not significantly differ between patients undergoing EVT and those who did not in both the crossover (Figure 1E) and non-crossover groups (Figure 2E).
Conclusions: Thrombectomy does not enhance functional outcomes in mild stroke patients and raises the risk of sICH. Further randomized controlled trials are crucial to refine EVT use in this group.
Disclosures of Interest: No
Abstract N°: 4241
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
FIRST-IN-MAN MULTICENTER TRIAL OF A NOVEL STENT-RETRIEVER WITH SPIRAL FUSIFORM TECHNOLOGY IN LOW-MIDDLE-INCOME COUNTRIES
1University of Toledo Medical School, Toledo, United States, 2National Institute of CardioVascular Diseases (NICVD), Karachi, Pakistan, 3HonorHealth Research and Innovation Institute, Scottsdale, United States, 4, Chicago, United States, 5Virginia Mason Medical Center, Seattle, United States, 6Barrow Neurological Institute, Phoenix, United States, 7University of Miami Miller School of Medicine, Miami, United States
On behalf of: GRASSROOT Trial Investigators (Trial registration number: NCT06249776)
Background and aims: Despite massive benefit and cost-effectiveness, access to MT in LMICs remains under 1% of eligible patients. Also, efficacy of revascularization has plateaued. The SuperNova stentreiver, developed with non-traditional in-silico device development, incorporates novel spiral-fusiform cell technology, superior struts for improved engagement, and spatially-optimized radial force, and has been designed to substantially improve first pass effect for red and white clots. GRASSROOT study aims to evaluate the safety and efficacy of the SuperNova Stentriever.
Methods: Prospective, multicenter, single-arm study conducted in low-middle-income countries (NCT06249776). GRASSROOT study is evaluating the performance of the SuperNova stentriever in recanalizing LVOs including internal carotid artery,M1/M2 middle cerebral artery, and vertebrobasilar arteries, within 24-hours of onset. Primary efficacy endpoint is rate of mTICI score >=2b. Primary safety endpoints are 90-day mortality and/or 24-hour symptomatic intracranial hemorrhage(sICH).
Results: A total of nine subjects have been enrolled to date. Median NIHSS score was 16 (IQR 12-20), median ASPECTS is 9 (8-10), and median time-to-arrival is 6 (3-9) hours. mTICI 2b–3 within 3 SuperNova passes occurred in 89% (8/9) and First pass mTICI 2b–3 was observed in 67% (6/9) of cases. Median number-of-passes was 1 (IQR 1-2). Rate of 24-hour sICH was 11% (1/9). 90-day outcomes data will be available at conference presentation.
Conclusions: Preliminary data suggests excellent safety and efficacy of the novel SuperNova stentriever. It has the potential to substantially advance first pass success rates and increase access to MT in LMICs.
Disclosures of Interest: No
E-Poster - Prevention and Secondary Prevention
Abstract N°: 4151
Category: 1.03 PREVENTION
CARDIAC MAGNETIC RESONANCE IMAGING IN PATIENTS WITH EMBOLIC STROKE OF UNKNOWN SOURCE AND NO ATRIAL FIBRILLATION (CARM-AF STUDY)
Irum Kotadia*1, Robert O'dowling1, Akosua Aboagye2, Amedeo Chiribiri1, Pier Giorgio Masci1, Jonathan Birns2, Peter Sommerville2, Ajay Bhalla2, Mark O'neill2, Steven Williams3
1King's College London, United Kingdom, 2Guy's and St Thomas' NHS Foundation Trust, United Kingdom, 3University of Edinburgh, United Kingdom
On behalf of: CARM-AF Investigatory Group (Richard J. Crawley, Neil Bodagh, Ali Gharaviri, Jose Alonso Lemus-Solis, Iain Sim, Deborah Ramsey, Sven Plein, Laszlo Sztriha, Paul Scott, James Harrison, Steven Niederer)
Background and aims: Undiagnosed atrial fibrillation (AF) causes 25% of embolic strokes of unknown source (ESUS), with annual stroke recurrence rates of 3-6%. Guidelines mandate AF diagnosis prior to anticoagulation causing delays in therapy and significant cost and resource implications for follow-up. This study aims to produce a substrate-based predictive model identifying ESUS patients at high-risk of developing AF that may benefit from early anticoagulation.
Methods: CARM-AF is a prospective, multiXXX-centre, observational study. All patients underwent CMR imaging and ILR (implantable loop recorder) implantation for AF detection within 3 months of stroke. Patients were allocated to the study group if AF>30 seconds was detected by ILR during the first year of follow-up. MultiXXXvariable logistic regression models were used to predict AF.
Results: 91 patients were included in the final analysis. AF was detected in 17 patients at 1-year post-ILR insertion (18.6%). Patients with AF were more likely to be female (p-value=0.02).
Increased leftXXX atrial (LA) area, volume, surface area and reduced LA ejection fraction quantified using CMR were associated with increased risk of AF detection (p-value=0.046, 0.006, 0.044, 0.008). LA fibrosis and sphericity were not associated with AF detection (p-value = 0.84, 0.98).
A logistic regression model combining patient and CMR parameters outperformed assessment of all other models, achieving an AUC of 0.847 for predicting AF occurrence (p-value<0.005) and Pseudo R2 of 0.257 indicating excellent model fit.
Conclusions: A randomised controlled trial initiating anticoagulation in ESUS patients at high-risk of AF detection using the CARM-AF model for patient selection is recommended.
Disclosures of Interest: No
Abstract N°: 1358
Category: 2.03 PLACEHOLDER - Prevention
GENETIC POLYMORPHISM OF CYP2C19 IN RECURRENT ISCHEMIC STROKE PATIENTS: PREVALENCE AND ROLE IN SECONDARY PREVENTION
Noha T sarhan*1, Amal Elmotayam1, Sara F. Saadawy2, Mai M. Eldaly2
1Zagazig University, Faculty of Medicine, Neurology Department, Zagazig, Egypt, 2zagazig University, Faculty of Medicine, Medical Biochemistry, Egypt
On behalf of:
Background and aims: Antiplatelet therapy taking clopidogrel alone or in combination with aspirin is commonly used for the secondary stroke prevention in at-risk individuals. clopidogrel is an inactive pro-drug that requires a 2-step biotransformation by a number of CYP450. This study aims at evaluating the prevalence of CYP219 loss of function alleles among Egyptian population, determining their role in clopidogrel response and identifying their relation with recurrent ischemic stroke.
Methods: a prospective cohort study included 91 randomly selected patients with acute ischemic stroke within 14 days of onset, The CYP2C19 genotype was determined via allelic discrimination plots using TaqMan realtime PCR primers and probes on the Applied Biosystems 7500 Fast Real-Time PCR system. The samples were analyzed in 2 allelic discrimination assays each for the presence or absence of CYP2C19*2, CYP2C19*3 variant alleles. Patients followed up for 1 year. The primary endpoint was ischemic events and the secondary endpoint was bleeding.
Results: A total of 110 patients were admitted to this study from August 2022 to July 2023; 91 patients completed the follow-up for 1 year,the carriers of GA and AA genotype in CYP2C19*2 (681 G>A) were non-responder to clopidogrel drug compared to responder OR (95% CI) (7.5(2.3-24.4)). While in CYP2C19*3 (636 G>A) GA+AA were resistant to clopidogrel drug compared with the responder group OR (95% CI)( 5.7(1.71-19.1)).
Conclusions: Egyptian patients with ischemic stroke carrying CYP2C19 LoF alleles have increased clopidogrel resistance and higher stroke recurrence rates when receiving clopidogrel, patients may benefit from CYP2C19 genotyping before determining antiplatelet therapy.
Disclosures of Interest: No
E-Poster - Rehabilitation and Recovery
Abstract N°: 4074
Category: 1.04 REHABILITATION & RECOVERY
ABILITY TO STAND AND SIT IN PREDICTING INDEPENDENT LIVING IN STROKE PATIENTS
Shuen-Loong Tham*1, Anna Rosiana1, Yan Ming Soh1, Lay Fong Chin1, Suresh S/O Subramaniam2, Genieve Zhe Hui Gan1, Su Mon Htwe1, Nur Atiqah Binte Sidek2, Kevin Wei Wen Sim1, Keng He Kong1
1Tan Tock Seng Hospital, Singapore, Singapore, 2Woodlands Health Campus, Singapore, Singapore
On behalf of:
Background and aims: Stroke presentations are heterogenous and levels of disability can vary widely. Stratifying and grouping cohorts with similar characteristics can enhance rehabilitative care and facilitate discharge planning.
Methods: A retrospective study of electronic medical records was conducted between 1 January 2017 and 31 December 2017 in a tertiary rehabilitation center. Patients who completed their rehabilitation stints were stratified into 3 groups: Group 1) Able to sit and stand unsupported for > 2 minutes; Group 2) Able to sit but not stand unsupported for > 2 minutes; Group 3) Unable to sit and stand unsupported for > 2 minutes. The patients’ ability to perform such tasks were assessed within 72 hours of admission into the center. The primary outcome examined was independent living in the community.
Results: A total of 311 eligible patients’ records were analyzed. There were 112, 129 and 70 patients in groups 1, 2 and 3 respectively. Ability to stand and sit unsupported for 2 minutes was significantly associated with independent living following discharge (1, N=311) =53.56, p=0.00. Within group 1 patients, admission Functional Independent Measure (FIM) cognitive subscale of ⩾ 30 was better associated with independent living on discharge than use of the Montreal Cognitive Assessment (⩾ 30 as cut-off).
Conclusions: Early assessment of sitting and standing ability has the potential to predict discharge outcomes and hence facilitate discharge planning.
Disclosures of Interest: No
E-Poster - Ongoing Trials
Abstract N°: 4122
Category: 3.01 ONGOING TRIALS
BETTER ORAL HYGIENE IS ASSOCIATED WITH LOWER RISK OF STROKE
Ho Geol Woo*1
1Kyung Hee University College of Medicine, Departments of Neurology, Seoul, South Korea
On behalf of:
Background and aims: Periodontal disease or poor oral hygiene may lead to local infection, inflammation, and systemic inflammatory reactions, which are important mediators of development of stroke. We aimed to investigate the association of oral hygiene with risk of stroke in a nationwide population-based cohort.
Methods: From Korean National Health Insurance System-Health Screening Cohort, 206,602 participants were included. The presence of periodontal disease and indicators of oral hygiene, such as number of tooth brushings, dental visit history, dental scaling, and number of teeth loss and dental caries were evaluated. Occurrence of stroke including cerebral infarction, cerebral hemorrhage, and subarachnoid hemorrhage was defined as newly registration of International Classification of Diseases-10 codes from I60 to I64 accompanying brain CT and/or MR examination at that time of diagnosis.
Results: The 7337 (3.6%) cases of stroke including 5795 (79.0%) cases of cerebral infarction, 1568 (21.4%) cases of cerebral hemorrhage, and 621 (8.5%) cases of subarachnoid hemorrhage occurred during a median 10.4 years follow-up. In multivariable analysis, frequent tooth brushing (⩾3 times per day) was negatively associated with risk of stroke occurrence (hazard ratio [HR]: 0.78, 95% confidence interval [CI]: 0.73-0.84). Number of dental caries (⩾4) was positively related to stroke occurrence (HR: 1.28, 95% CI: 1.13-1.44).
Conclusions: Regular oral hygiene behavior was negatively, and infrequent oral hygiene care was positively associated with risk of occurrence for stroke, respectively. Brushing one's teeth three or more times daily may be associated with lower risk of stroke.
Disclosures of Interest: No
Abstract N°: 4259
Category: 3.01 ONGOING TRIALS
OPTIMIZING ACUTE ISCHEMIC STROKE DIAGNOSTICS USING ARTIFICIALINTELLIGENCE – EXPERIENCE FROM A NATIONAL PROJECT
Linn Heitmann*1, Thor Håkon Skattør2, Jon André Totland3, Brian Enriquez4, Agnethe Eltoft5, Dag Ottar Sætre6, Mayank Goyal7, Atle Bjørnerud8, Anne Hege Aamodt4,9
1Østfold Hospital Trust, Dept. of Neurology, Norway, 2Oslo University Hospital, Dept. of Radiology, Norway, 3University Hospital of North Norway, Dept. of Radiology, Norway, 4Oslo University Hospital, Dept. of Neurology, Norway, 5University Hospital of North Norway, Dept. of Neurology, Norway, 6Østfold Hospital Trust, Dept. of Radiology, Norway, 7Hotchkiss Brain Institute, University of Calgary, Dept. of Radiology and Clinical Neurosciences, Canada, 8Computational Radiology and AI (CRAI), Oslo University Hospital, Center for Radiology and Nuclear Medicine, Norway, 9The Norwegian University of Science and Technology, Neuromedicine and Movement Science, Norway
On behalf of: AI-STROKE group
Background and aims: Although the numbers of acute ischemic stroke (AIS) patients with large vessel occlusions (LVO) being offered endovascular treatment (EVT) are increasing, there is still a need to improve acute diagnostics reducing the time from symptom onset to treatment. The purpose of the project is to streamline the acute stroke pathway by using artificial intelligence to automatically analyze CT images.
Methods: In an ongoing national multicentre study, the use of multiphase CT angiography (mCTA) with software for automatic detection of LVO, calculation of infarct volume and penumbra is compared with standard radiological diagnostics. It is being assessed whether the time to EVT start can be reduced and whether a greater proportion of patients with LVO can be detected using the software compared to standard diagnostics. 465 patients are planned to be included within a 48-month periode.
Results: So far, 601 patients have been analyzed by AI-software. 16 patients have been treated with EVT. Primary stroke centres in Health South-East had median 8 min shorter time from CT start to EVT start in AIS patients compared to time before implementation of AI-software,156 min (IQR119,176) vs 164 min (IQR145,198). Primary stroke centres in Health North using software had median 3,5 min shorter time from CT start to contact air ambulance in AIS patients compared to hospitals with standard diagnostics, 36,5 min (IQR26,48) vs 40 min (IQR22,68) respectively.
Conclusions: The use of artificial intelligence in acute radiological diagnostics is promising to make the acute stroke pathway more efficient and contribute to equalizing differences in the health service.
Disclosures of Interest: No
Abstract N°: 4121
Category: 3.01 ONGOING TRIALS
ASSOCIATION OF MORTALITY WITH ANTIPLATELET TREATMENT IN PATIENTS WITH STENT PLACEMENT
Ho Geol Woo*1
1Kyung Hee University College of Medicine, Departments of Neurology, Seoul, South Korea
On behalf of:
Background and aims: Antiplatelet drugs are essential in patients with cardiovascular disease who undergo stent placement. We hypothesized that risks of mortality would differ according to adherence to antiplatelet agents, number of antiplatelet agents, and antiplatelet regimens in patients undergoing stent placement or angioplasty.
Methods: Between 2002 and 2013, we initially enrolled 8671 subjects who underwent stent placement in the National Health Insurance Service-National Sample Cohort in Korea. Using the International Classification of Diseases, 10th revision, the incidence of all-cause death, including cardiovascular disease, cerebrovascular disease, and cancer, was defined. Using a nested case-control study design, controls were matched to cases at a ratio of 4:1, and a total of 5415 subjects were eligible for this study.
Results: During a median follow-up period of 3.51 years, the incidence rate of all-cause death was 40 per 1000 person-years. We found that adherence to antiplatelet monotherapy significantly decreased risk of death by cerebro-cardiovascular disease, compared with discontinuation of antiplatelets [adjusted odds ratio (OR) 0.62, 95% confidence interval (CI) (0.41-0.96)]. Compared with dual antiplatelet therapy (DAPT), aspirin and clopidogrel monotherapy significantly reduced death by cerebro-cardiovascular disease [adjusted OR 0.65, 95% CI (0.44-0.95) and adjusted OR 0.58, 95% CI (0.35-0.96), respectively]. There was no significant difference of mortality between aspirin monotherapy and clopidogrel monotherapy.
Conclusions: Our study demonstrated that adherence to antiplatelet therapy and antiplatelet monotherapy, compared with DAPT, in patients with stent placement or angioplasty may have a beneficial effect on mortality in cerebro-cardiovascular disease.
Disclosures of Interest: No
Abstract N°: 4154
Category: 3.01 ONGOING TRIALS
DRUG-ELUTING STENTING VERSUS MEDICAL TREATMENT ALONE FOR PATIENTS WITH EXTRACRANIAL VERTEBRAL ARTERY STENOSIS: THE VISTA TRIAL
Delin Liu*1, Tao Wang1, Wenlong Xu1, Bin Yang1, Haibo Wang2, Hugh Markus3, Huanzhang Shi4, Liqun Jiao5
1Xuanwu Hospital, China International Neuroscience Institute, Capital Medical University, National Center for Neurological Disorders, Neurosurgery, Beijing, China, 2Peking University First Hospital, eking University Clinical Research Institute, Beijing, China, 3University of Cambridge, Cambridge, United Kingdom, 4First Affiliated Hospital of Harbin Medical University, Department of Neurosurgery, Harbin, China, 5Xuanwu Hospital, China International Neuroscience Institute, Capital Medical University, National Center for Neurological Disorders, Department of Neurosurgery and Interventional Neuroradiology, Beijing, China
On behalf of: VISTA Investigators
Background and aims: Two previous randomized controlled trials focusing on vertebral artery stenting, the Vertebral Artery Stenting Trial (VAST) and the Vertebral Artery Ischaemia Stenting Trial (VIST), were underpowered because they failed to reach expected recruitment, and they found no difference in stroke prevention between stenting and medical treatment alone. Drug-eluting stents have shown better performance than bare metal stents. To further determine the effect of drug-eluting stenting in reducing stroke in patients with extracranial vertebral artery stenosis, we designed this study.
Methods: Multicenter, randomized, open-label, outcome assessor-blinded trial will be conducted at 31 centers in China. Patients with extracranial vertebral artery (V1-2) 70% to 99% stenosis and transient ischemic attack or ischemic stroke within the past 3 months will be recruited (first patient enrollment: Sep 15, 2023).
Results: A total of 472 patients will be enrolled. Patients will be randomized (1:1) to drug-eluting stenting plus medical therapy or medical therapy alone. Medical treatment includes dual antiplatelet (aspirin 100mg per day + clopidogrel 75mg per day or ticagrelor 90mg twice per day) for 6 months. The primary outcome is any fatal or non-fatal stroke within 30 days, or ischemic stroke in the targeted area within 30 days to 1 year. Secondary outcomes includes stroke, death, crescendo TIA in the targeted area within 1 year.
Conclusions: The study has been registered on ClinicalTrials.gov (Identifier: NCT05885932) and enrollment is ongoing. This trial aims to reveal whether drug-eluting stenting is safe and effective in vertebral artery stenosis.
Disclosures of Interest: No
Abstract N°: 4221
Category: 3.01 ONGOING TRIALS
OPTIMAL BLOOD PRESSURE FOR THE PREVENTION OF MAJOR VASCULAR EVENTS IN STROKE PATIENTS(OPTIMAL - STROKE)
Gisele Sampaio*1, Otavio Berwanger2, Karla Santo3, Octavio Pontes4, Sheila Cristina Ouriques Martins5, Adriana Conforto6, Flavio Fuchs5, Joao Andrade3, Maria Julia Machline Carrion7
1Hospital Albert Einstein and UNIFESP, Neurology, 2Georges Institute UK, 3Hospital Albert Einstein, 4Universidade de São Paulo Ribeirão Preto, 5Universidade Federal do Rio Grande do Sul, 6Universidade de São Paulo, 7EPHealth
On behalf of:
Background and aims: Despite the evidence suggesting the use of antihypertensives in patients with ischemic stroke (IS), the heterogeneity of the clinical trials included in guidelines compromises the recommendation of a blood pressure (BP) target and the intensity of the BP reduction required. Objective:The primary objective of the OPTIMAL-Stroke trial is to determine if a more intensive BP control target compared to the standard BP target in a population of patients with previous IS has an impact on the reduction of major cardiovascular events.
Methods: OPTIMAL-Stroke is a randomized, controlled, 1:1 open-label clinical trial with blind assessment of clinical outcomes. Population-Patients are eligible to the study if they are over 18 years and have a history of IS or transient ischemic attack, clinically stable for at least 48 hours prior to study inclusion and have a systolic blood pressure of 130-180 mmHg. Sample Size-4060 patient.
Results: Intervention: Patients were randomized to either an intensive BP control group targeting SBP <120 mmHg or to a control group, targeting SBP <140 mmHg. Outcome-The primary outcome is the first occurrence of a composite outcome of major cardiovascular events (cardiovascular death, non-fatal myocardial infarction (MI), non-fatal stroke, hospitalization for unstable angina or hospitalization for heart failure). Statistical Analysis-The analysis of primary efficacy outcome will be the comparison between the two groups using a long-rank test procedure.
Conclusions: Trial Status-Enrollment is finished at 30 sites. A total of 4368 patients were randomized and are currently being followed.
Disclosures of Interest: Yes Trial Sponsor Brazilian Ministry of Health
Abstract N°: 4145
Category: 3.01 ONGOING TRIALS
PISCES-ZODIAC: A RANDOMISED CONTROLLED TRIAL OF REMOTELY DELIVERED FITNESS TRAINING FOR BRAIN HEALTH IN ISCHAEMIC STROKE SURVIVORS
Kate Hayward*1, Liam Johnson2, Kimberley Adkins3, Ruwayda Haibe3, Julie Bernhardt4, Leonid Churilov5, Amy Brodtmann3
1The University of Melbourne, Physiotherapy, Parkville, Australia, 2Australian Catholic University Melbourne Campus, School of Behavioural and Health Sciences, Fitzroy, Australia, 3Monash University, Faculty of Medicine, Nursing and Health Sciences, Neuroscience, Melbourne, Australia, 4The Florey Institute of Neuroscience and Mental Health, Stroke, Parkville, Australia, 5The University of Melbourne, Medicine, Parkville, Australia
On behalf of: PISCES-ZODIAC Investigators
Background and aims: Stroke increases subsequent dementia risk yet there are no specific post-stroke therapies to protect cognition. Cardiorespiratory exercise may be neuroprotective. The Post Ischaemic Stroke Cardiovascular Exercise Study (PISCES) aimed to reduce neurodegeneration via in-person fitness training. We pivoted to a remotely delivered intervention to reduce pandemic-amplified barriers to exercise in 2020: our ZOom Delivered Intervention Against Cognitive decline (ZODIAC).
Methods: PISCES-ZODIAC is an investigator initiated, multi-centre, Phase IIb assessor-blind randomised (1:1 allocation) controlled trial testing the preliminary efficacy and feasibility of an eight-week cardiorespiratory exercise intervention compared to those receiving balance and stretching training (active control). Participants are assessed before (two-months post-stroke t1) and after (four-months t2) the exercise intervention and followed up at 12-months (t3). Primary outcome is hippocampal and total brain volume change at t2; secondary outcome is the ADAS-Cog at t3. Our estimated total sample size is 110 participants allowing for attrition.
Results: Thirty-four participants were consented for the PISCES (2017-2020) intervention; 64 have completed ZODIAC (2021-23) t1 and t2 at time of writing. Final recruited participants commenced their intervention March 2024. All participants will have completed their intervention May 2024 with final study visits in December 2024. Data base lock is expected early 2025 with primary outcome analyses predicted for presentation at ESOC 2025.
Conclusions: Post-stroke cardiorespiratory exercise interventions appear feasible when remotely delivered to stroke survivors in their home. Our novel trial design will provide information on the efficacy of exercise to preserve brain volume and cognition after stroke.
Disclosures of Interest: No
Abstract N°: 4155
Category: 3.01 ONGOING TRIALS
ACUTE LARGE VESSEL OCCLUSION REVASCULARIZATION COMBINED WITH TOCILIZUMAB TREATMENT: A RANDOMIZED, DOUBLE-BLIND, PLACEBO-CONTROLLED CLINICAL TRIAL
Xuehong Chu1, Zhengfei MA2, Anzhi LI2, Yan Feng2, Chen Zhou3, Chuanhui LI1, Wenbo Zhao1, Ming LI1, Xunming Ji1, Chuanjie Wu*1
1Xuanwu Hospital, Capital Medical University, China, 2Suzhou Municipal Hospital, Su Zhou Shi, China, 3Beijing Institute of Brain Disorders, Capital Medical University, China
On behalf of:
Background and aims: Research has confirmed the close association between interleukin-6 and the onset and progression of cardio-cerebrovascular diseases. Furthermore, tocilizumab, an interleukin-6 receptor antagonist, has shown notable anti-inflammatory properties and myocardial protective effects in cardiovascular conditions, particularly among individuals undergoing coronary artery interventional therapy. Despite promising indications from preclinical studies suggesting tocilizumab's potential efficacy post-cerebral ischemia reperfusion, its safety and effectiveness in patients undergoing thrombectomy for cerebral infarction remain uncertain.
Methods: In this randomized, double-blind, placebo-controlled clinical trial, 108 eligible subjects were randomly assigned to the placebo group or tocilizumab group in a 1:1 ratio. The dose of tocilizumab was 240mg, given as a single infusion. The primary endpoint was the change in cerebral infarction volume relative to baseline at 72 hours postoperatively. Measurement of high-sensitivity C-reactive protein, fibrinogen, inflammatory factors, etc., was performed daily for the first three days postoperatively.
Results: By March 19, 2024, 31 patients have been enrolled.
Conclusions: Tocilizumab may have a positive impact on patients with acute anterior circulation occlusion reperfusion, thus improving the clinical prognosis of these patients.
Disclosures of Interest: No
Abstract N°: 4179
Category: 3.01 ONGOING TRIALS
STANDARDISED ADAPTIVE MULTIPHASE PLATFORM FOR UNMET STROKE NEEDS (SEAMLESS) TRIAL
Kate Hayward*1, Bruce Campbell1,2, Natasha Lannin3,4, Carlos Garcia-Esperon5,6, Mark Parsons7, Amy Brodtmann3, Vignan Yogendrakumar1,2, Eva Mistry8, Michael Hill9, Leonid Churilov1
1University of Melbourne, 2Royal Melbourne Hospital, 3Monash University, 4Alfred Health, 5Hunter Medical Research Institute, 6John Hunter Hospital, 7University of New South Wales, 8University of Cincinnati, 9University of Calgary
On behalf of: SEAMLESS adaptive platform trial collaboration
Background and aims: Adaptive platform trials (APT) have been used to definitively evaluate the effectiveness of multiple treatments across one or more subgroups of participants. The APT approach is yet to capitalise upon advantages provided by the phased nature of treatment identification and development in clinical trials. StandardisEd Adaptive Multiphase pLatform for unmEt Stroke needS (SEAMLESS) is a novel “adaptive pipeline-platform” trial. This trial is designed to establish evidence of dose, safety and sufficient promise of efficacy (Phase I-IIa) before establishing efficacy/effectiveness (Phase IIb-III) within the structure of a master protocol with a priori defined adaptations. Our aim is to develop and maintain SEAMLESS trial to test innovative acute and recovery focused treatments for unmet stroke needs.
Methods: SEAMLESS is an adaptive pipeline-platform trial with domain-specific treatment protocols. Each domain may be represented as a hierarchical combination of basket and/or umbrella components implementable at each phase of clinical trial conduct. Any basket component applies an adaptive master protocol to test a hypothesis of a treatment across multiple subpopulations. Any umbrella component enables hypothesis testing of various treatments within a domain-specific subpopulation. Prespecified rules govern transition between clinical trial phases and within phase adaptations.
Results: The first SEAMLESS domain is in preparation. Our international team (Australia/Canada/USA) is interdisciplinary and spans neurology, rehabilitation medicine, physiotherapy, occupational therapy, speech pathology, biostatistics, and people with lived experience.
Conclusions: SEAMLESS is an innovative trial that will help deliver unprecedented efficiency to narrow the translational gap between evidence generation and clinical care.
Disclosures of Interest: No
Abstract N°: 4206
Category: 3.01 ONGOING TRIALS
STUDY II ON THE EFFICACY OF REMOTE ISCHEMIC CONDITIONING FOR PREVENTING STROKE-ASSOCIATED PNEUMONIA
1Xuanwu Hospital, Capital Medical University, Neurology, Beijing, China, 2Capital Medical University, Beijing Institute of Brain Disorders, Beijing, China
On behalf of:
Background and aims: Research shows that stroke-associated infection is one of the most common and significant complications of stroke, severely affecting the recovery of stroke patients. Remote ischemic conditioning (RIC) therapy is a non-invasive physical treatment modality that exerts protective effects on various organs by subjecting limbs to repeated cycles of ischemia and reperfusion. Numerous domestic and international studies have demonstrated the safety and feasibility of RIC, with some suggesting its protective effect against infection. However, the safety and efficacy of RIC for stroke-associated pneumonia remain uncertain.
Methods: In this randomized, double-blind, sham-controlled multicenter clinical trial, 1650 acute ischemic stroke patients within 24 hours of onset were allocated in a 1:1 ratio to either the Sham-RIC group or RIC group. During treatment, inflatable cuffs were wrapped around the upper arm with cuff pressures of either 60 mmHg or 200 mmHg, applied for 5 minutes followed by 5 minutes of rest, cycled 5 times, and continued for 7 days. The primary endpoint was the incidence of stroke-associated pneumonia within 7 days post-stroke.
Results: By March 20, 2024, 198 participants have been enrolled.
Conclusions: RIC may potentially have a positive impact on patients with acute ischemic stroke, thereby reducing the incidence of stroke-associated pneumonia.
Disclosures of Interest: No
Abstract N°: 4218
Category: 3.01 ONGOING TRIALS
EFFICACY OF ADD ON HOLISTIC AYURVEDIC TREATMENT AND CONVENTIONAL STANDARD MEDICAL CARE IN POST STROKE CASES
1Indraprastha Apollo Hospital, New Delhi, Neurology, New Delhi, India, 2All India Institute of Ayurveda (AIIA), India
On behalf of:
Background and aims: Stroke poses significant economic and productivity challenges, Ayurveda emerges as a promising alternative, although scientific studies on its role in stroke management are lacking. This study aims to evaluate Ayurveda's efficacy in post-stroke recovery through clinical and biochemical assessments. Traditional medicine, particularly Ayurveda, is increasingly sought by stroke patients for better outcomes. Post-stroke management is crucial, and Ayurvedic offers Panchakarma treatments for conditions like Pakshaghata (Stroke). Case reports and research suggest comparable safety and efficacy between Ayurveda and conventional biomedicine in acute ischemic stroke management. The study aims to enhance post-stroke patient care by investigating the efficacy of Holistic Ayurvedic treatment compared to Conventional Standard Medical Care. Primary objectives include assessing reduction in stroke symptoms, Modified Rankin Scale (MRS), Modified Ashworth Scale (MAS), and NIHSS scores at presentation and Day 90. Secondary objectives involve evaluating changes in Quality of Life (QoL), laboratory parameters, and disease-related anxiety scale.
Methods: This prospective comparative clinical trial, with 90 participants (45 in each group), is non-randomized and follows an active conventional medicine-controlled intervention model. It employs an open-label masking approach and is classified as a Phase II trial with a duration of 90 days. Group 1 receives conventional stroke management followed by Ayurveda, while Group 2 receives standard medical care.
Results: Ongoing Trial
Conclusions: The discussions highlight the pressing need for alternative approaches like Ayurveda in stroke management, emphasizing the importance of scientifically evaluating Ayurvedic interventions for post-stroke recovery to address clinical symptoms and biochemical parameters effectively.
Disclosures of Interest: No
Abstract N°: 4256
Category: 3.01 ONGOING TRIALS
A RANDOMIZED, DOUBLE-BLIND, PLACEBO-CONTROLLED PHASE 2B TO EVALUATE THE EFFECT OF NA-911 ON UPPER EXTREMITY MOTOR FUNCTION FOLLOWING ISCHEMIC STROKE
Lloyd Tran*1, Zung Tran1, Fern Vu1
1Biomed Industries, Inc., Research and Development, San Jose, United States
On behalf of:
Background and aims: NA-911 is neuroprotective drug that has showed a proof of safety and efficacy in Phase 2 clinical trial for patients with early Alzheimer’s disease and ALS. This is a randomized, double-blind, placebo-controlled parallel group outpatient treatment study.
Methods: The study will utilize standard stroke rehabilitation outcome measures to evaluate the effect of NA-911 on upper extremity motor recovery in subjects following ischemic stroke. Eligible subjects will be randomly assigned to be treated with either NA-911 or placebo, in addition to standard treatments.
Intervention/Treatment: NA-911 at 60 mg per day orally vs. placebo over 12 weeks.
Enrolment: 120 participants.
Key Inclusion Criteria:
Experienced an ischemic stroke documented by CT or MRI resulting in upper extremity deficit
Medically stable subjects, with expected survival > 12 months
Mild to moderately severe upper extremity motor impairment
mRS score of 1 to 4 from index stroke
Mini Mental State Examination (MMSE) score of ⩾ 22
Key Exclusion Criteria:
Residual motor deficit from any prior stroke
Hemorrhagic stroke. Ischemic stroke with limited hemorrhagic conversion (i.e., petechial hemorrhage or micro-hemorrhage) is acceptable.
Severe or total sensory loss
Stroke Impact Scale
Modified Rankin Scale
Primary Outcome Measures: (over 84 days)
Fugl-Meyer Assessment of Upper Extremity Motor Function, Parts A-D.
Type and incidence of treatment emergent adverse events
Safety Laboratory Assessments
Vital signs and 12-lead ECG
Secondary Outcome Measures: (over 84 days)
Nine-Hole Peg Test and
Action Research Arm Test
Stroke Impact Scale
Results: The clinical trial is on-going.
Conclusions: The results will be updated and presented.
Disclosures of Interest: Yes I am an employee of Biomed Industries, Inc.
Abstract N°: 3038
Category: 3.01 ONGOING TRIALS
CORRELATION BETWEEN CEREBRAL VASOREACTIVITY AND RETINAL BLOOD FLOW PARAMETERS IN PATIENTS WITH SIGNIFICANT INTERNAL CAROTID ARTERY STENOSIS
Anna Gaál*1,2, Rita Stang1, Hanga Pál1, Lilla István3, Zsuzsanna Mihály4, Péter Sótonyi4, Tamás Horváth5, Dániel Bereczki1, Illés Kovács3, Róbert Debreczeni1
1Semmelweis University, Department of Neurology, Budapest, Hungary, 2Semmelweis University, Doctoral School, Budapest, Hungary, 3Semmelweis University, Department of Ophtalmology, Budapest, Hungary, 4Semmelweis University, Department of Vascular Surgery, Budapest, Hungary, 5University of Physical Education, Research Center for Sport Physiology, Budapest, Hungary
On behalf of:
Background and aims: The retinal and cerebral circulation are developmentally, anatomically, and physiologically similar. We aimed to investigate the relationship between cerebral and retinal circulation in patients with atherosclerotic internal carotid artery stenosis.
Methods: 24 patients with significant ICA stenosis were consecutively enrolled. Cerebrovascular reactivity was estimated by TCD measurement of the common carotid artery compression (CCC) test. The following variables of CCC test were calculated: Transient Hyperemic Response Ratio–THRR (the increase of blood flow velocity after CCC relative to the baseline value), Cerebral Arterial Resistance Transient Hyperemic Response Ratio-CAR-THRR (the change of flowresistance after CCC relative to the baseline value).
Optical Coherence Tomography Angiography (OCTA) was performed to determine the vessel density (VD) on the papilla (P) 4,5x4,5 mm whole image (WI) for all vessel types (VDP-WIall) and selectively for small vessels (VDP-WIsmall) only. In the peripapillary (PP) region, the VD was also determined for all vessel types (VDPPall) and selectively for small vessels (VDPPsmall).
Results: A significant, negative correlation was found between CAR-THRR and VDPPsmall vessel type (p=0.003; Spearman's r=-0.57), as well as between VDPPall vessel types (p=0.01; Spearman's r=-0.48). There was also a significant, negative correlation between CAR-THRR and VDP-WIsmall (p=0.01; Spearman's r=-0.52) and between VDP-WIall (p=0.02; Spearman's r =-0.45) too.
Conclusions: The study showed a significant correlation between decreased cerebrovascular reactivity and retinal functional vessel density in patients with ICA stenosis suggesting common mechanisms of action. The combined use of OCTA and TCD was found to be suitable for assessing the condition of cerebral vasculature in significant ICA stenosis.
Disclosures of Interest: No
E-Poster – Case Reports
Abstract N°: 1484
Category: 4.29 CASE REPORTS
INTRAVENOUS THROMBOLYSIS IN A 75-YEAR-OLD STROKE PATIENT WITH FABRY DISEASE. CASE REPORT AND LITERATURE REVIEW
Efstratia-Maria Georgopoulou*1, Myrto Palkopoulou1, Aggelos-Michail Kalaentzis1, Ioannis Kyriakopoulos1, Anastasia Kaliontzoglou1
1General Hospital of Rhodes, Neurology Department, Rhodes, Dodecanese, Greece
On behalf of: Kerazi Eleni, Foti Georgia-Angeliki, Tsioumitas Thomas, Liapis Ioannis
Background and aims: Fabry-Anderson’s disease (FD) is a rare X-linked recessive lysosomal storage disease, caused by mutations of the gene (GLA) encoding the enzyme a-galactosidase. Multiorgan involvement is common and includes acute ischemic stroke (AIS) in ~13% of the cases. Intravenous thrombolysis (IVT) is the gold-standard treatment in selected AIS patients. We present an elder AIS and late-onset FD patient with an underreported GLA variant, treated with IVT. Additionally, literature and variant databases review was conducted.
Methods: A 75-year-old male with sudden onset of dysarthria and right hemiparesis and National Institutes of Health Stroke Scale (NIHSS) of 6, is presented. Patient’s history included pacemaker placement, paroxysmal atrial fibrillation, diabetes mellitus type 2, smoking, chronic pelvic pain and hypertension. Following indicated investigations including brain CT scan (Fig.1a), AIS diagnosis was established. IVT using alteplase was initiated at 90 minutes from symptom onset. Subsequent work-up revealed severe leucoaraiosis, past (Fig.1a,b) and acute (arrow) ischemic lesions, heart failure, concentric left ventricular hypertrophy, ascending aorta dilatation and left atrium enlargement.
Results: High FD prevalence (33 cases per 125.000 population) prompted confirmatory testing detecting increased lyso-Gb3 levels, decreased a-galactosidase activity and a missense pathogenic class I GLA mutation [c.638A>C p.(Lys213Thr), K213T, (Fig.2, Varsome®11.8)]. The patient suffered no complications (Fig.1b) and was discharged with NIHSS=2.
Conclusions: This is the first case, to our knowledge, of safe administration of IVT to an elder FD patient with severe comorbidities and of AIS associated with mutation K213T, which could be related to late-onset cardiovascular involvement.
Disclosures of Interest: No
Young Stroke Physicians and Researchers - E-Poster
Abstract N°: 4052
Category: 4.30 YSPR – Study Design Workshop
SAFETY AND EFFICACY OF REMOTE ISCHEMIC CONDITIONING IN PATIENTS WITH ACUTE ISCHEMIC STROKE UNDERGOING ENDOVASCULAR THROMBECTOMY: A RANDOMIZED TRIAL
1Xuanwu Hospital, Capital Medical University, Neurology, Beijing, China, 2School of Medicine - Wayne State University
On behalf of:
Background and aims: Endovascular thrombectomy is generally recognized as the most effective therapy for patients with acute ischemic stroke (AIS) caused by large-vessel occlusion; however, the clinical prognosis of these patients remains relatively poor, with significant room for improvement. Remote Ischemic Conditioning (RIC) has been demonstrated to be safe and feasible in AIS patients undergoing thrombectomy. This study aims to evaluate whether RIC could improve the functional outcomes of this patient population.
Methods: This is an investigator-initiated, multicenter, prospective, randomized, sham-controlled, outcome-blinded parallel-group trial. A total of 1068 patients will be recruited if they experienced AIS secondary anterior circulation large-vessel occlusion within 24 hours of symptom onset and will undergo thrombectomy. All enrolled patients are randomly assigned in a 1:1 ratio to receive RIC or sham RIC, which will be initiated before thrombectomy procedures and continued for 14 consecutive days. The primary outcome is functional independence (defined as mRS= 0-2) at 90 days. Secondary outcomes include ordinal shift analysis of scores on the mRS at 90 days, the proportion of patients with mRS scores 0-3 at 90 days, and changes in NIHSS within 14 days of treatment. All outcomes and serious adverse events are adjudicated blinded to treatment.
Results: NA
Conclusions: This trial holds immense potential in evaluating the efficacy of RIC before and after thrombectomy in patients with acute anterior circulation large-vessel occlusive stroke. If successful, it could provide randomized evidence on the role of RIC in this patient population, potentially revolutionizing stroke treatment and research.
Disclosures of Interest: No
Abstract N°: 4126
Category: 4.30 YSPR – Study Design Workshop
SAFETY AND EFFICACY OF EARLY INTRAVENOUS ADMINISTRATION OF TIROFIBAN IN PATIENTS WITH ACUTE ISCHEMIC STROKE AFTER THROMBOLYSIS: A RANDOMIZED TRIAL
1Xuanwu Hospital, Capital Medical University, Neurology, Beijing, China
On behalf of: The TREND-IVT investigator
Background and aims: Neurological deterioration (ND) is a common phenomenon in patients with acute ischemic stroke (AIS) treated with intravenous thrombolysis (IVT) and is strongly associated with poor clinical outcomes. Antithrombotic therapy is the primary strategy for preventing ND in patients with AIS. This trial aims to evaluate whether early intravenous administration of tirofiban within 24 h after IVT can safely prevent ND and improve functional outcomes compared with oral antiplatelet therapy 24 h after IVT.
Methods: This is an investigator-initiated, multicentre, prospective, randomized, sham-controlled, outcome-blinded parallel-group trial. A total of 1380 patients with AIS who are treated with IVT and displayed no significant change in NIHSS after IVT (change of NIHSS±2), and no intracerebral haemorrhage will be recruited. All enrolled patients are randomly assigned in a 1:1 ratio to receive intravenous tirofiban within 1 h after IVT, bridging with oral antiplatelet therapy 24 h after IVT, or oral antiplatelet therapy 24 h after IVT. The primary outcome is an excellent functional outcome (defined as mRS= 0-1) at 90 days. Secondary outcomes include ND within 24 h of IVT and the proportion of patients with mRS scores of 0-2 at 90 days. Safety outcomes include symptomatic intracerebral haemorrhage and any intracerebral haemorrhage within 24 hours of IVT.
Results: NA
Conclusions: This trial aims to evaluate the safety and efficacy of intravenous tirofiban within 24 h of IVT in patients with AIS. If successful, it may provide empirical evidence for the role of early antiplatelet therapy within 24 h of IVT in this patient population.
Disclosures of Interest: No
Abstract N°: 4205
Category: 4.30 YSPR – Study Design Workshop
TRIAL OF ENDOVASCULAR THERAPY FOR ACUTE VERTEBROBASILAR OCCLUSION WITH LARGE INFARCT
1Xuanwu Hospital of Capital Medical University, Department of Neurology, Beijing, China, 2Xuanwu Hospital of Capital Medical University, Department of Neurosurgery, Beijing, China, 3Xuanwu Hospital of Capital Medical University, Stroke center, Beijing, China
On behalf of:
Background and aims: There are no randomized trials examining the best treatment for acute basilar artery occlusion with Large Infarct. The primary aim of this study is to assess the safety and efficacy of thrombectomy for stroke due to basilar artery occlusion in patients with large infarct within 72 hours from symptom onset.
Methods: This is a prospective, multi-center, randomized, controlled, open-label and blinded-endpoint trial involving patients with acute basilar-artery occlusion and a posterior circulation Acute Stroke Prognosis Early CT score (pc-ASPECTS) of 3 to 5 (range, 0 to 10, with lower values indicating larger infarction) . The randomization employs a 1:1 ratio of mechanical thrombectomy and best medical therapy (BMT) vs. BMT alone. The primary outcome will be the proportion of patients achieving modified Rankin Scale (mRS) 0–3 at 90 days. Key secondary outcomes are: ordinal (shift) mRS analysis at 90 days, dichotomized mRS score (0–2 vs. 3–6 and 0–4 vs. 5–6) at 90 days, vessel recanalization at 24 h in both treatment arms, and successful recanalization in the thrombectomy arm according to the modified thrombolysis in cerebral infarction (mTICI) classification defined as mTICI 2 b or 3. Safety outcomes are mortality at 90 days, symptomatic intracranial hemorrhage rates at 24 hours, and procedure-related complications.
Results: N/A
Conclusions: Results from this trial will indicate whether mechanical thrombectomy plus best medical management is superior to best medical management alone in achieving favorable outcomes in subjects with large infarct stroke caused by basilar artery occlusion presenting within 24 hours from symptom onset.
Disclosures of Interest: No
Abstract N°: 1784
Category: 4.30 YSPR – Study Design Workshop
ESTABLISHING AN INTERNATIONAL NETWORK FOR STANDARDISED POPULATION INSIGHTS AND REAL-WORLD EVIDENCE FOR STROKE (INSPIRE-STROKE)
Lachlan Dalli*1, Muideen Olaiya1, Dominique A. Cadilhac1,2, Mathew Reeves3, Seana Gall1,4, Lee Nedkoff5,6, Amy Yu7, Moira Kapral8,9,10, Monique Kilkenny1,2
1Stroke and Ageing Research, Department of Medicine, School of Clinical Sciences at Monash Health, Monash University, Clayton, Australia, 2Stroke Division, Florey Institute of Neuroscience and Mental Health, Heidelberg, Australia, 3Department of Epidemiology and Biostatistics, Michigan State University, East Lansing, United States, 4Menzies Institute for Medical Research, University of Tasmania, Hobart, Australia, 5Cardiovascular Epidemiology Research Centre, School of Population and Global Health, School of Population and Global Health, The University of Western Australia, Perth, Australia, 6Victor Chang Cardiac Research Institute, Darlinghurst, Australia, 7Department of Medicine (Neurology), Sunnybrook Health Sciences Centre, Toronto, Canada, 8Division of General Internal Medicine, Department of Medicine, University of Toronto, Toronto, Canada, 9ICES, Toronto, Canada, 10Toronto General Hospital Research Institute, Toronto, Canada
On behalf of: INSPIRE-STROKE Collaborators
Background and aims: Current global collaborations on the surveillance of important stroke outcomes, such as readmissions, recurrent stroke, and medication adherence, are lacking. We aim to establish an enduring global network to support routine pooling and reporting of country-level administrative data on these outcomes.
Methods: A steering committee was established in October 2023, comprising leaders in stroke research using administrative data from Australia, Canada, and the United States. This committee set the vision, terms of reference, and priorities for the collaborative network. A strategy was developed to identify suitable collaborators, mainly via review of literature and existing research networks. It is anticipated that each project will involve: 1) drafting a statistical analysis plan; 2) creating a common data model to harmonise variables and definitions; 3) assessing data quality; 4) developing standardised statistical coding in multiple programming languages; 5) implementing statistical codes using a distributed approach; 6) analysis and reporting of pooled data.
Results: We have established an International Network for Standardised Population Insights and Real-world Evidence for STROKE (INSPIRE-STROKE). Personalised invitation emails and registration forms will be sent to a further 100+ potential collaborators identified across 20+ countries. The first collaborative project is in the planning stages, involving multi-country comparisons of readmissions following stroke.
Conclusions: INSPIRE-STROKE will generate global insights into clinically relevant outcomes for stroke, using standardised methods. Efforts are ongoing to expand INSPIRE-STROKE membership across Europe and beyond. This network will complement existing global collaborations on stroke surveillance to inform national and international health policy for stroke.
Disclosures of Interest: No
Abstract N°: 2702
Category: 4.30 YSPR – Study Design Workshop
IDENTIFICATION OF PLASMA BIOMARKERS TO DIFFERENTIATE BETWEEN TRANSIENT ISCHAEMIC ATTACKS (TIAS), MINOR STROKES, AND TIA MIMICS
Deeksha Sharma*1, Rachael Protzman2, Marten Snel2, Austin Milton3, Joshua Mahadevan3, Craig Kurunawai3, Timothy Kleinig3, Jim Jannes3, Simon Koblar1, Anne Hamilton-Bruce3
1The University of Adelaide, Adelaide, Australia, 2SAHMRI (South Australian Health and Medical Research Institute), Adelaide, Australia, 3Central Adelaide Local Health Network, Adelaide, Australia
On behalf of: Suzanne Edwards, Dr Paul Trim
Background and aims: Stroke is a leading cause of death, with over 80% being ischaemic strokes. Approximately 20% of these are preceded by a TIA, allowing for possible risk reduction if diagnosed rapidly. TIA diagnosis is complex due to transience and symptomatic overlap with similar neurological conditions (TIA mimics). This study aims to use a multiomic approach to identify biomarkers to differentiate between TIAs, minor strokes, and TIA mimics and reduce the risk of ischaemic stroke.
Methods: Patients presenting to the Royal Adelaide Hospital with TIA-like symptoms ≤48 hours of the event were enrolled, with ≤10mL plasma collected and stored for processing. Discovery lipidomic and proteomic investigations were conducted using LC-MS, with preliminary lipidomic data processing via Skyline and MetaboAnalyst. Proteomic processing was conducted using DIA-PASEF with protein identification done via Spectronaut. All patients were clinically classified retrospectively by a panel of vascular neurologists as TIA/TIA mimic/minor stroke.
Results: Over 100 patients have been enrolled to date, with the first 50 patient samples having undergone investigation (29 Females, 21 Males) with ages ranging from 39–94 years (Median:72y) at time of enrolment. All patients were classified based on clinical data (56% as TIA Mimics). A total of 467 lipids and 863 proteins have been detected in the cohort with statistical and pathway analysis ongoing.
Conclusions: This is an active project, with the first phase of multiomic investigation reaching completion. Lipidomic and proteomic investigations have yielded valuable outcomes currently underway. All investigations are in the process of being expanded and retested with a larger sample population (n=100+).
Disclosures of Interest: No
Abstract N°: 2882
Category: 4.30 YSPR – Study Design Workshop
DIAGNOSIS AND DIFFERENTIATION OF STROKE THROUGH MICRORNA (MIRNA) PROFILING AS POTENTIAL BIOMARKERS USING A DEEP NEXT-GENERATION SEQUENCING APPROACH
1All India Institute Of Medical Sciences, Neurology, New Delhi, India, 2Yale University, Neurology, Connecticut, United States, 3All India Institute Of Medical Sciences, Clinical Research Unit, New Delhi, India
On behalf of:
Background and aims: The timely diagnosis of stroke is critical for determining the appropriate treatment approach, reducing mortality rates, and improving functional outcomes. Brain imaging techniques like Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) are used to differentiate between ischemic stroke (IS) and intracerebral hemorrhage (ICH). However, there is a need for blood-based biomarkers to enhance clinical decision-making and prevent misdiagnosis. MicroRNAs are small molecules that can be easily measured in venous blood and provide quantifiable gene expression information, potentially distinguishing stroke subtypes and improving diagnostic accuracy. The primary objectives of this study are to diagnose and differentiate IS from ICH and healthy controls using next-generation sequencing (NGS) to analyze miRNA gene expression profiles.
Methods: Blood samples will be collected within six hours of symptom onset from individuals diagnosed with IS, ICH, and healthy controls. RNA extraction and miRNA isolation will be performed using commercial kits, followed by cDNA library construction. Deep next-generation sequencing will be employed to identify mature miRNAs during the discovery phase. The identified miRNA transcripts will undergo validation using quantitative reverse transcription-polymerase chain reaction (qRT-PCR). Statistical analysis will be conducted using R version 4.0.2 and STATA software.
Results: This study attempts to identify novel miRNAs that can effectively differentiate and diagnose IS from ICH and healthy controls.
Conclusions: MiRNAs are easily quantifiable and readily available in extracellular fluids. Their involvement in various cellular processes offers increased predictability, sensitivity, and specificity for stroke diagnosis and differentiation, particularly within six hours after symptom onset.
Flowchart.
Timeline.
Disclosures of Interest: No
Abstract N°: 4071
Category: 4.30 YSPR – Study Design Workshop
EEG CHANGES IN HYPERACUTE MALIGNANT STROKE FOLLOWING INITATION OF HYPEROSMOLAR THERAPY AS A PROGNOSTIC BIOMARKER IN NEUROCRITICAL PATIENTS
1Spitalul Universitar de Urgență Elias, Stroke Unit, București, Romania, 2Carol Davila University of Medicine and Pharmacy, Neurology, București, Romania, 3Spitalul Universitar de Urgență Elias, Epilepsy and Sleep Disorders, București, Romania, 4Spitalul Universitar de Urgență Elias, Neurology, București, Romania
On behalf of:
Background and aims: Malignant stroke carries a high risk of mortality and severe disability. Identifying early prognostic biomarkers could improve decision-making in the hyperacute setting and guide the escalation of care. Little to no data is available regarding EEG changes in regards to hyperosmolar therapy initiation in acute stroke. This study aims to investigate the potential of EEG changes during hyperosmolar therapy to predict outcomes in malignant stroke patients.
Methods: This prospective, single-center study will enroll 40 acute ischemic stroke patients who fulfill malignant stroke criteria, are between 18-80 years old, and are eligible for hyperosmolar therapy with simultaneous EEG recording within 12 hours of symptom onset. EEG recordings will be obtained during the initial Mannitol bolus (1 mg/kg over 30 minutes). Changes in EEG patterns will be correlated with clinical and imaging outcomes. Main outcomes will be NIHSS and mRS scores at discharge and 3 months, and mortality.
Results: Recruitment is scheduled to begin starting April 8th 2024. Enrolment should be fulfilled in 4 months. All patients will be followed for up to 3 months after discharge.
Conclusions: This study will explore whether quantitative and qualitative EEG changes occurring during hyperosmolar therapy administration can serve as an early prognostic biomarker in malignant stroke. Identifying such a marker could potentially improve patient selection for aggressive treatment options and aid in clinical decision-making for this critical patient population.
Disclosures of Interest: No
Abstract N°: 4207
Category: 4.30 YSPR – Study Design Workshop
EXTENDING THE TIME WINDOW OF ENDOVASCULAR TREATMENT FOR ACUTE VERTEBROBASILAR OCCLUSION
1Xuanwu Hospital of Capital Medical University, Department of Neurology, Beijing, China, 2Xuanwu Hospital of Capital Medical University, Department of Neurosurgery, Beijing, China, 3Xuanwu Hospital of Capital Medical University, Stroke center, Beijing, China
On behalf of:
Background and aims: Two recent clinical trials (ATTENTION and BAOCHE) demonstrated superiority of endovascular therapy over medical management among patients with stroke due to basilar-artery occlusion within 24hours. The primary aim of this study is to evaluate the hypothesis that mechanical thrombectomy is superior to medical management alone in achieving favourable outcomes in subjects presenting with stroke due to basilar-artery occlusion in the extending time window of 24-72 hours from symptom onset.
Methods: A prospective, multi-center, randomized, controlled, open-label and blinded-endpoint trial. The randomization employs a 2:1 ratio of mechanical thrombectomy and best medical therapy (BMT) vs. BMT alone. The primary outcome will be the proportion of patients achieving modified Rankin Scale (mRS) 0–3 at 90 days. Key secondary outcomes are: ordinal (shift) mRS analysis at 90 days, dichotomized mRS score (0–2 vs. 3–6 and 0–4 vs. 5–6) at 90 days, vessel recanalization at 24 h in both treatment arms, and successful recanalization in the thrombectomy arm according to the modified thrombolysis in cerebral infarction (mTICI) classification defined as mTICI 2 b or 3. Safety variables are mortality at 90 days, symptomatic intracranial hemorrhage rates at 24 h, and procedure-related complications.
Results: N/A
Conclusions: Results from this trial will indicate whether mechanical thrombectomy is superior to medical management alone in achieving favorable outcomes in subjects with acute stroke caused by basilar artery occlusion presenting within 24–72 hours from symptom onset.
Disclosures of Interest: No
Abstract N°: 173
Category: 4.30 YSPR – Study Design Workshop
INTERNATIONAL COMPARISON OF AMBULANCE TIME INTERVALS FOR STROKE/TIA ACROSS SEVEN COUNTRIES BEFORE AND DURING THE COVID-19 PANDEMIC
1University College Cork, School of Public Health, Cork, Ireland, 2National Ambulance Service, Clinical Directorate, Limerick, Ireland, 3National Ambulance Service, Technology, Data & Business Analytics, Trim, Ireland, 4University College Cork, School of Nursing and Midwifery, Cork, Ireland, 5Cork University Hospital, Department of Neurology, Cork, Ireland, 6University of Glasgow, School of Cardiovascular and Metabolic Health, Glasgow, Ireland, 7National Ambulance Service, Portfolio Management Office, Tralee, Ireland
On behalf of: Prehospital Care of Stroke (PHoCoS) Consortium
Background and aims: Prehospital management of stroke/transient ischemic attacks (TIA) aims to shorten time to diagnosis and treatment. International reports have acknowledged the wide-ranging impact of the COVID-19 pandemic on acute stroke services including the marked decline in acute stroke presentations. Thus we aimed to investigate if ambulance time intervals for adults with suspected stroke/TIA differed before and during the COVID-19 pandemic in The Republic of Ireland, compared to six other countries.
Methods: We are conducting a secondary data analysis with a quasi-experimental design, using data from seven international ambulance services. These services include those from: the Republic of Ireland, Northern Ireland, Scotland, New Zealand, Netherlands(Utrecht), Austria(Vienna) and Australia (Queensland). We are including all cases assigned code 28 (suspected stroke/TIA) by the emergency call-taker, from 2018-2021. The COVID-19 period is defined as the date of the first identified COVID-19 case in a country, with the pre-COVID-19 period extending from 01/01/2018 to the day before the first identified case. We will analyse demographic characteristics using descriptive statistics. We will compare five ambulance time intervals: “allocation performance”, “mobilisation performance”, “response time”, “on scene time” and “conveyance time” between the two periods using descriptive and regression analyses. We will also compare call volume for suspected stroke/TIA between the pre-COVID-19 and COVID-19 periods using time series analysis.
Results: Data on ambulance time intervals and call volume pre-COVID-19 and during COVID-19 will be provided.
Conclusions: This study will provide insights into the international impact of the COVID-19 pandemic on prehospital care for suspected stroke/TIA.
Disclosures of Interest: No
Abstract N°: 346
Category: 4.30 YSPR – Study Design Workshop
PREDICTORS OF GOOD OUTCOMES IN THROMBECTOMY FOR LARGE INFARCT CORE STROKE EVALUATION
Trung Nguyen*1, Khang Nguyen2, Hang Tran3, Huy Quang Dang1, Thien Le4, Lanh Nguyen5, Dung Bach2, Anh Truong1, BA-Thang Nguyen6, Thang Nguyen1
1Bệnh viện Nhân Dân 115, Cerebrovascular Disease, Ho Chi Minh, Viet Nam, 2University Medical Center HCMC, Neurology, Ho Chi Minh, 3Pham Ngoc Thach University of Medicine, Neurology, Ho Chi Minh, 4Da Nang General Hospital, Stroke, Da Nang, Viet Nam, 5Can Tho Central General Hospital, Can tho, Viet Nam, 6University of Medicine & Pharmacy HCMC (UMP), Neurology, Ho Chi Minh
On behalf of: PROMISE Collaboration
Background and aims: Endovascular treatment (EVT) for acute large-core stroke patients has demonstrated efficiency along with safety. However, the rate of good outcomes remains low, while the mortality and disability rates are very high. We hypothesize that an infarct core is not the sole factor for predicting good outcomes in large core patients undergoing EVT. We aimed to determine predictors of functional independence (FI) following thrombectomy in large infarct core stroke patients.
Methods: PROMISE, a prospective multicenter study in Vietnam involving four comprehensive stroke centers, screened all consecutive patients undergoing EVT. Inclusion criteria were age ⩾18, NIHSS ⩾6, pre mRS 0-2, ICA or M1 MCA occlusion, and mechanical thrombectomy within 24 hours of stroke onset. Large core strokes were defined by ASPECTS <6 or perfusion core >50 ml. Imaging was assessed by two certified neurologists, with disagreements resolved by a senior reader. The primary outcome was FI (mRS 0-2) at 3 months. Secondary outcomes included ambulatory function (mRS 0-3), recanalization success, and safety analysis. The study adheres to STROBE criteria and is registered as NCT06016348. Based on the FI and death rates of 30.0% and 21.7% in the ANGEL ASPECT trial, we aim to recruit at least 250 patients. Multivariable binary logistic regression, using AIC-based backward selection, will identify independent predictors of FI outcome after 90 days.
Results:
Conclusions: PROMISE will provide more evidence to identify predictors of functional independence outcomes following large infarct core thrombectomy.
Disclosures of Interest: No
Abstract N°: 475
Category: 4.30 YSPR – Study Design Workshop
SCORE FOR DECISION MAKING IN DEEP INTRACEREBRAL HEMORRHAGES
Larrey Valere Kamabu*1,2
1Makerere University, Neurosurgery, Kampala, Uganda, 2Universite Catholique du Graben, Neurosurgery, Butembo, DR Congo
On behalf of:
Background and aims: Deep or basal ganglia hemorrhages contribute significantly to worldwide morbidity and mortality, accounting for 50-70% of intracerebral hemorrhages(ICH). This study will focuse on creating a decision-making score for intracerebral hemorrhages, considering factors such as CT evidence, clinical condition, and operative indications among stroke patients at CIMAK Hospital
Methods: A prospective study will recruit 414 patients with deep intracerebral hemorrhages, evaluating their outcomes based on NIHSS, quality of life, complications, GOS, time of hospital stay, recovery, and mortality. The data will be securely submitted to the Redcap system. Binary logistic regression analysis will be employed to assess predictors of mortality at different time points (24 hours, 30, 90, and 180 days). Variables with P˂0.05 in univariate analysis will be considered for inclusion in the multivariate model. The study aims to determine the therapeutic time window through sensitivity, specificity, and area under the curve (AUC) using receiver operating characteristic curves.
Results: Anticipated outcomes will include the development of a comprehensive decision-making score for ICH, incorporating factors like GCS, NIHSS, ICH score, modified ICH score, spot sign score, and leakage sign. The study will utilize GOS, Barthel index, and Rankin scale at various time points to monitor outcomes for both surgical and conservative treatment approaches. The resulting compendium will encompass anatomical, clinical, treatment, surgical technical, and radiological aspects of hemorrhagic lesions, contributing valuable insights to the management of intracerebral hemorrhages.
Conclusions: This research has the potential to enhance clinical decision-making, improve patient outcomes, and contribute significantly to the understanding of ICH.
Disclosures of Interest: No
Abstract N°: 4058
Category: 4.30 YSPR – Study Design Workshop
BLOOD VISCOSITY RELATED TO FALSE-NEGATIVE DIFFUSION-WEIGHTED IMAGING IN LATERAL MEDULLARY INFARCTION
Ho Geol Woo*1, Dae-Il Chang1, Sung Hyuk Heo1
1Kyung Hee University College of Medicine, Departments of Neurology, Seoul, South Korea
On behalf of:
Background and aims: Diffusion-weighted imaging (DWI) using magnetic resonance imaging (MRI) is widely used for the early detection of ischemic stroke. However, false-negative DWI results are often reported in patients with lateral medullary infarction (LMI) during the acute period. Our aim was to investigate the predictive factors of false-negative DWI results in patients with acute LMI.
Methods: In this retrospective cohort study, we collected data from acute ischemic stroke patients with LMI on DWI within 1 week of symptom onset who were hospitalized between June 2016 and June 2023. The patients were divided into an initially positive DWI group and a false-negative DWI group, in which the lesion was found on follow-up DWI after an initially negative DWI result. Predictive factors for false-negative DWI results were evaluated.
Results: Of the 156 patients, 113 (72.4%) were men. The mean age was 62.0 years. False-negative DWI results were noted in 19.9% of patients. The time to first image in the false-negative DWI group was shorter than that in the initial positive DWI group (10.3 ± 6.8 vs. 46.2 ± 40.5, P<0.001). Multivariate logistic analysis showed that systolic blood viscosity (adjusted odds ratio, 0.091; 95% confidence interval, 0.026–0.321; P<0.001) and time to first image (adjusted odds ratio, 0.771; 95% confidence interval, 0.655–0.909; P=0.002) were significantly associated with false-negative DWI results.
Conclusions: Our study demonstrated that lower viscosity and shorter time to first image was significantly associated with false-negative DWI results in patients with acute LMI.
Disclosures of Interest: No
Abstract N°: 4066
Category: 4.30 YSPR – Study Design Workshop
DEVELOPING A COMMUNITY-BASED INTERVENTION FOR POST-STROKE COGNITIVE IMPAIRMENT: REFERRAL FOR EXERCISE AND COGNITIVE TRAINING AFTER STROKE (REACTS)
James Smith*1, Philip Nagy1, David Tod1, Carol Holland1, Hannah Jarvis1
1Lancaster University, Lancaster Medical School, Lancaster, United Kingdom
On behalf of:
Background and aims: Post-stroke cognitive impairment (PSCI) affects almost half of all stroke survivors. However, there is currently no consensus on best management, reflected in the ambiguity and variability of clinical guidelines. A growing body of evidence suggests that physical exercise and cognitive rehabilitation can have a synergistic effect on improving PSCI. Using co-production methods, the aim of this study is to develop program theory for a community-based exercise and cognitive rehabilitation intervention.
Methods: Program theory will be informed by two prior evidence reviews – an overview of reviews investigating the efficacy of the proposed interventions and a qualitative scoping review investigating stroke survivors’ perspectives of community-based exercise programs. Focus groups will be conducted with patients, carers, fitness instructors, clinicians, service managers, and academics. The transcripts of each stakeholder group will be thematically analysed independently, and themes will be compared across the groups. A stakeholder panel, made of selected members of each stakeholder group, will meet iteratively during the study to continually refine program theory.
Results: Some key areas of program theory to clarify are treatment parameters, educational components, eligibility criteria, and outcome measures. The resulting program theory will be used to design a community-based exercise and cognitive rehabilitation intervention, with the primary aim of reducing PSCI.
Conclusions: This will be the first study to develop a community-based exercise intervention specifically designed to improve post-stroke cognitve function. The developed intervention will be evaluated using a mixed-methods feasibility study to further refine program theory.
Disclosures of Interest: No
Abstract N°: 4084
Category: 4.30 YSPR – Study Design Workshop
THE ROLE OF OXYTOCIN IN ACUTE ISCHEMIC STROKE RECONVALESCENCE: THE ROXANE STUDY
Background and aims: Evidence suggests that oxytocin has a neuroprotective role in the context of acute ischemic stroke (AIS). Further oxytocin may attenuate effects of centrally regulated stress hormones (cortisol), which has proven negative prognostic utility in stroke patients. We hypothesize that a) high levels of circulating oxytocin measured within the first 48 hours after symptom onset are associated with lower mortality and favorable outcome in acute ischemic stroke. Furthermore, we want to explore b) the associacion of oxytocin with post-stroke depression as well as social support c) other markers of the HPA-axis such as cortisol/copeptin d) and the dynamics of oxycotin over-time.
Methods: In our prospective single center cohort study we plan to enroll 400 patients with acute ischemic stroke (the ROXANE cohort) and measure (blinded) the Oxytocin value within 24 hours after symptom onset and again within 48 hours. Primary outcome parameter is the modified Rankin scale (mRS) measured via structured telephone interview after 3 months. Multivariate logistic regression will be performed with oxytocin plasma value as independent variable and mRS as dependent variable.
Results: Not yet applicable
Conclusions: We want to demonstrate an independent association of Oxytocin with functional outcome after stroke -in combination with the existing pre-clinical evidence of a causal relationship - we hope to lay the ground for an intervention trial using oxytocin that is commercially available and safe to apply via nasal spray. (Overall, the careful investigation of the role of oxytocin in stroke recovery in patients could be a first step towards further research.)
Disclosures of Interest: No
Abstract N°: 4166
Category: 4.30 YSPR – Study Design Workshop
MINIMALLY INVASIVE SURGERY FOR INTRACEREBRAL HEMORRHAGE: META-ANALYSIS OF HIGH-QUALITY RANDOMIZED CLINICAL TRIALS
Fahad Alajlan*1, Ahmed Alkhiri2, Aser Alamri2, Ahmed Almaghrabi2, Basil Alghamdi2, Fahad Alturki2, Abdullah Alharbi3, Wendy Ziai4, Christopher Kellner5, Adel Alhazzani1
1King Faisal Specialist Hospital and Research Centre, Neuroscience Center, 2King Saud Bin Abdulaziz University for Health Sciences, College of Medicine, Saudi Arabia, 3King Abdullah Medical City, Department of Neurology, Makkah, 4The Johns Hopkins Hospital, 1800 Orleans Street, Phipps 455, Baltimore, MD 21287, USA, 5Department of Neurosurgery, Icahn School of Medicine at Mount Sinai, New York, NY, 10029, USA, New York, United States
On behalf of:
Background and aims: Spontaneous intracerebral haemorrhage (ICH) poses high mortality and morbidity rates with limited evidence-based therapeutic approaches. Minimally invasive surgery (MIS) has emerged as a promising treatment, offering the potential to improve functional outcomes and decrease mortality rates. Our main objective was to evaluate the current evidence for the role of MIS in the management of ICH.
Methods: We performed a systematic review and meta-analysis following PRISMA guidelines. Independent authors searched four electronic databases (Medline, Embase, Web of Science, and CENTRAL) and assessed methodological quality of included studies using the Cochrane risk of bias tool (RoB2). Only high-quality randomised clinical trials (RCTs) were included, ensuring they were not deemed to have a high risk of bias in any of the RoB2 domains. We pooled odd ratios (ORs) and 95% confidence intervals (CIs). Primary outcomes were good functional outcome (modified Rankin Scale 0-3) and mortality at 90 to 365 days.
Results: Fourteen high-quality RCTs were included. There were 3027 (62.7% males) patients with ICH (1475 randomised to MIS, and 1452 randomised to medical management or craniotomy). MIS resulted in higher odds of achieving long-term good functional outcome (OR, 1.49 [95% CI, 1.23-1.79]) and lower odds of long-term mortality (OR, 0.71 [95% CI, 0.56-0.90]). Rebleeding rates were similar (OR, 1.30 [95% CI, 0.55-3.09]). The treatment effect of MIS was consistent across multiple sensitivity and subgroup analyses.
Conclusions: This meta-analysis provides high-quality clinical trial evidence supporting the use of MIS as a primary treatment strategy in the management of ICH.
Disclosures of Interest: No
Abstract N°: 4177
Category: 4.30 YSPR – Study DesigWorkshop
SHATTERING BOUNDARIES: REVOLUTIONIZING STROKE TREATMENT WITH HISTOTRIPSY
Ameer Hassan*1, Rick Ducharme2, Robert Hamilton3, Adnan Siddiqui2, Adnan Qureshi4
1University of Texas Rio Grande Valley - School of Medicine, Harlingen, United States, 2University at Buffalo (South Campus), Buffalo, United States, 3NeuraSignal, Los Angeles, United States, 4University of Missouri, Columbia, United States
On behalf of:
Background and aims: Stroke poses a substantial healthcare burden in the U.S. and around the world, necessitating innovative treatment approaches. Traditional methods lack widespread accessibility, with recent studies showing mechanical thrombectomy worldwide access limited to approximately 2.6%. To assess the effectiveness of a novel non-invasive ultrasound technology (histotripsy) in disintegrating stroke-causing clots, focusing on our initial tests with soft and mixed clots.
Methods: In-vitro experimental trials were conducted in simulated use conditions with porcine clot analogs. Clots were lodged in tubing with an inner diameter mimicking the middle cerebral artery. The novel histotripsy device was then activated to disrupt the clots. The residual clot analog components were captured downstream with an in-line 50um mesh filter. Captured particulate characterized by number and size using digital microscopy.
Results: The histotripsy device demonstrated successful thrombolysis, re-establishing flow in all soft porcine clot conditions. Ongoing testing is being performed to evaluate the histotripsy device settings perform best across a range of clot types including both soft red and fibrin rich clots. Further data will be provided following completion and analysis of the ongoing testing.
Conclusions: The development of Histotripsy in the realm of stroke management marks a significant leap forward, promising a non-invasive, swift, and precise method for clot treatment. This innovation is poised to revolutionize stroke treatment and neurointerventional surgery, making treatment more accessible and efficacious.
Histotripsy probes with a silicon model with clot at the Middle Cerebral Artery.
Disclosures of Interest: Yes Co-founder of Quantanosis
Abstract N°: 4178
Category: 4.30 YSPR – Study Design Workshop
SLEEP-DISORDERED BREATHING IS ASSOCIATED WITH INCREASED MORTALITY AND POOR OUTCOMES IN ACUTE ISCHEMIC STROKE: THE BERNESE SLEEP&STROKE REGISTRY
Xiaoli Yang1, Julian Lippert*1, Stefan Bauer1, Thomas Meinel2, Tobias Reichlin2, Anne-Kathrin Brill2, Corrado Bernasconi2, David Seiffge2, Markus Schmidt2, Claudio Bassetti2
1Inselspital, Department of Neurology, Bern, Switzerland, 2Inselspital, Bern, Switzerland
On behalf of:
Background and aims: In acute stroke, SDB is common and associated with poor outcomes, but large cohort studies are sparse. We assessed respiratory indices' impact on mortality, MACE, and functional outcome.
Methods: In this prospective cohort study, stroke patients underwent RP within 72h after admission, categorizing SDB severity by AHI (mild ⩾5, moderate ⩾15, severe ⩾30/h). We assessed outcomes - mRS at 3 months, all-cause mortality and MACE over 84 months, analyzing two subgroups: patients with supplemental oxygen due to low baseline oxygen saturation (⩽ 92% SpO2), and without during RP. Cox and logistic regression, adjusted for relevant confounders including age, sex, BMI, hypertension, atrial fibrillation and NIHSS, evaluated associations, presenting results as adjusted hazard ratio (aHR) or adjusted odds ratio (aOR) with 95%CI.
Results: We studied 1556 patients (60.9% males, mean age 68.4 ± 13.7), with 72.9% having SDB (AHI ⩾ 5/h): mild (29.6%), moderate (21.5%), severe (21.8%). Central sleep apnea occurred in 6%. Initial NIHSS mean was 5.6 ± 6.3. In the non-oxygen-supplied group (n=1083), SDB increased mortality risk (aHR 2.25, 1.06-4.77), notably severe SDB (HR 2.74, 1.19-6.34). MACE correlated with mild (HR 1.47, 1.06-2.04), moderate (HR 2.01, 1.43-2.82), and severe SDB (HR 1.53, 1.07-2.18). Poor functional outcome (mRS score ⩽3) at three months is associated with severe SDB (aOR 2.5, 1.45-4.38). In the oxygen-supplied subgroup (n=473), SDB biomarkers showed non-significant associations with outcomes.
Conclusions: The study emphasizes the association between SDB in stroke patients and poor long-term outcomes. Differential associations in patients receiving oxygen warrant further investigation.
Disclosures of Interest: No
Abstract N°: 4257
Category: 4.30 YSPR – Study Design Workshop
SAFETY AND EFFICACY OF DIRECT-ACTING ANTICOAGULANTS. FOLLOW-UP IN LARGE POPULATIONS
Alfredo Palomino1, Jose Ramón Torres-Martín2, Antonio Cristobal Luque-Ambrosiani*1,3, German Escobar Rodriguez4, Javier Jiménez2, Auxiliadora Caballero5, Francisco José Hernández Ramos1, Maria Dolores Jiménez-Hernández1
1Virgen del Rocío University Hospital, Neurology, Sevilla, Spain, 2Drimay Consultores S.L., Sevilla, Spain, 3Virgen del Rocío University Hospital, Sevilla, Spain, 4FISEVI, Sevilla, Spain, 5Empresa Pública Emergencias Sanitarias, Sevilla, Spain
On behalf of:
Background and aims: A longitudinal study of a large number of patients with ischemic stroke due to Atrial Fibrillation (AF). Our aim is to analyze whether changes in anticoagulation therapies have had an impact on recurrence of stroke in certain patient risk groups.
Methods: We followed-up patients from 1994 to 2023 and collected information on anticoagulant therapy used between 2003 and 2023. We defined two periods, 2002-2008 and 2010-2016, for analysis due to higher data quality.
Results: We studied 35130 patients. There was a small reduction of recurrence from 12,85% to 12,77% in patients with AF. Patients with arterial hypertension had a reduction of recurrence from 14,18% to 13,52% and patients with Diabetes Mellitus had a reduction from 16,26% to 14,66%. Incidence was greater in the second period due to an improvement in patient diagnosis.
Conclusions: The recurrence of stroke due to AF did not increase with the introduction of new anticoagulants. The highest reduction in recurrence was observed in patients with additional risk factors such as hypertension or diabetes.
Disclosures of Interest: No
Abstract N°: 2075
Category: 4.30 YSPR – Study Design Workshop
EFFICACY, SAFETY AND TIME-DEPENDENT IMPACT OF INTRAVENOUS TROMBOLYSIS VERSUS CONSERVATIVE TREATMENT IN CRAO: RICCRAOS
Sven Matthijs*1, Jorgen Rovers1, Marjolein Ronday2, Maurits Joosse3, Ido van den Wijngaard3
Background and aims: Central retinal artery occlusion (CRAO) has a high risk of permanent blindness. Literature suggests that IVT treatment for CRAO may be effective, but no randomized clinical trials are available. We investigate the effect, the door-to-needle time (DTNT) and safety outcomes of IVT in a large group of IVT treated CRAO patients.
Methods: We are conducting a retrospective meta-analysis of IVT treated CRAO patients versus conservative treated CRAO patients. Analysis is performed on patient level data, which is derived from previously published literature and unpublished data received of multiple centers. The primary outcome is the proportion of patients with ⩽ 0.7 logMAR best corrected visual acuity in the affected eye IVT treatment. Furthermore we investigate the effect of the DTNT and occurred serious adverse events.
Results: Thus far we included 166 patients CRAO IVT patients for analysis and we know the adverse events of 289 IVT treated CRAO patients. Because we are still including IVT and conservative treated patients we only have preliminary Results: a mean recovery rate of 0.7 DTNT 0 - 1.5 hours (h), 0.30 DTNT 1.5 – 3 h, 0.21 DTNT 3.0 - 4.5 h and 0.15 DTNT 4.5 - 6 h. In 5 of 289 IVT treated CRAO patients (1.7 %) developed a symptomatic intracranial hemorrhage of which 3 were also treated with heparin. Final results and statistical analysis (with conservative treated patients) is expected to be completed in the next months.
Conclusions: Will be presented by Mid May at the ESOC
Disclosures of Interest: No
Abstract N°: 2899
Category: 4.30 YSPR – Study Design Workshop
PROSPECTIVE REGISTRY OF ISCHEMIC STROKE IN YOUNG ADULTS. CLINICAL CHARACTERISTICS, COGNITIVE AND OCCUPATIONAL PROGNOSIS AND UNMET NEEDS
David Seoane*1,2, Fernando Ostos Moliz1,2, Maria Gutiérrez Sánchez de la Fuente1,2, María Teresa Montalvo Moraleda3, Rodrigo Terrero Carpio4, Lorena Fernandez Gil5, Angel Ruiz Molina5, Patrica Calleja1,2
1Hospital Universitario 12 de Octubre, Stroke Unit, 2Instituto de Investigación i+12, Neurovascular Sciences, 3Hospital Universitario Rey Juan Carlos, Stroke Unit, 4Hospital Universitario de Getafe, Stroke Unit, 5Puerta de Hierro Majadahonda University Hospital, Stroke Unit, Spain
On behalf of:
Background and aims: : Ischemic stroke incidence keeps increasing in young adults (18-50 years-old), representing a major public health issue and research need. Subsequent cognitive and psychosocial problems and long-term unemployment are frequently neglected.
Methods: Prospective muti-center cohort study of young stroke (YS) incident cases. Recollection of clinical data and baseline conventional and emerging risk factors. Evaluation at 3 and 12 months of cognitive function (MOCA test), employment status (compared to pre-stroke and to the general Spanish population), anxiety and depression symptoms screening and assessment of multi-domain sequelae (Stroke Impact Scale compared to a simple visual scale designed by the authors (Image 1), under validation by this study). Proxys can help to answer if needed.
Results: The study protocol was approved by the local ethics committee and recruitment started in May 2023, with four participating Stroke Units. Sample size pre-determination is 248 patients for a multi-variant logistic regression model of returning to work. Other expected results are a present clinical description of YS and risk factors, to highlight the multi-domain sequelae and validation of an operational scale to evaluate them within the available time in clinical practice.
Conclusions: We present a triple line of research about YS: clinical description, return to work evaluation and scale validation, trying to fulfill a knowledge gap and patient community demand.
Designed scale Visual Quality of Life (VQoL).
Disclosures of Interest: No
Abstract N°: 4118
Category: 4.30 YSPR – Study Design Workshop
RELATIONSHIP OF POSTURAL CONTROL WITH SENSORIMOTOR FUNCTION,BALANCE AND SPATIAL NEGLECT IN PATIENTS WITH ACUTE STROKE
Ceren Bayrak*1,2, Ela Tarakci3, Hatice Yelda Yildiz2, Yakup Krespi2
1Istanbul University -Cerrahpasa, Graduate Education Institute, Physiotherapy and Rehabilitation Department, İSTANBUL, Turkey, 2Istinye University Hospital, Brain Angiography and Stroke Center, İstanbul, Turkey, 3Istanbul University- Cerrahpasa, Physiotherapy and Rehabilitation Department, İstanbul, Turkey
On behalf of:
Background and aims: The importance of early evaluation of sensory and cognitive problems as well as motor deficits associated with postural control in patients with ischemic stroke in the acute phase.
Methods: Between January and August 2023, 65 individuals with acute ischemic stroke were included in the study. Postural control impairment was assessed with the Posture Assessment Scale for Patients with Stroke (PASS T), upper and lower extremity motor function with the Stroke Rehabilitation Assessment of Movement (STREAM), neglect phenomenon with the Extinction and Inattention subscale of the NIHSS (National Institutes of Health Stroke Scale) and the Broken Hearts subtest of the Oxford Cognitive Screen (OCS). Within sensory functions, superficial sensation, position sensation and vibration sensation with diapozon were examined.
Results: As a result of the evaluations, a significant correlation was found between postural control and upper and lower extremity motor function, vibration sensation, balance and unilateral spatial neglect in individuals with acute ischemic stroke (p<0,001). When the severity of postural control was divided into two groups as severe and mild postural control disorder with a cut-off value of 12,5 points of PASS T, upper extremity motor function, vibration, superficial and position sense, balance and unilateral spatial neglect were significantly different in patients with severe postural control disorder (p<0,05). According to logistic regression analysis, upper extremity motor function and vibration sensation had a significant effect on postural control impairment severity (p<0,05).
Conclusions: This study underscores the importance of integrating sensory and cognitive treatment approaches with motor rehabilitation in acute stroke rehabilitation.
Disclosures of Interest: No
Abstract N°: 4235
Category: 4.30 YSPR – Study Design Workshop
CONTRIBUTION OF NESFATIN 1 AND GALECTIN 3 VALUES TO MORTALITY IN ACUTE ISCHEMIC STROKE
1Antalya Training and Research Hospital Neurology Department, Antalya, TURKEY, Neurology Department, Antalya, Turkey, 2Alanya Alaaddin Keykubat University Faculty of Medicine, Biochemistry, Antalya, Turkey, 3Korkuteli State Hospital, Neurology Department, Antalya, Turkey, 4Akdeniz University Faculty of Medicine, Biochemistry, Antalya, Turkey
On behalf of:
Background and aims: Nesfatin 1 and galectin 3 levels are markers whose importance is being investigated especially in cardiovascular diseases. Their levels can be different in acute stroke.
Methods: A total of 154 patients (acute stroke, chronic stroke and non-stroke group) were included in the study.Sample width was calculated using G*Power V. 3.1.9.6 program. The number of cases to be included in the study for 4 groups was determined as 152 in total, with 95% confidence (1-α), 95% test power (1-β), and an effect size of f = 0.341. Since the study was completed with 154 cases, the power of the test was found to be 95.3% according to the PostHoc power analysis result.
Results: There is a difference between the median values of nesfatin according to groups (p <0.001). While there is no difference between the groups with and without ICA (internal carotid artery) stenosis, the value obtained in these two groups is different from the others.
Galectin median values also differ between groups (p<0.001). The median value of the group with ICA stenosis differs from both the chronic and non-stroke groups. There is no difference between the group without ICA stenosis, chronic and non-stroke groups.
Conclusions: Further studies are needed especially in specific groups of stroke.
Disclosures of Interest: No
Abstract N°: 4251
Category: 4.30 YSPR – Study Design Workshop
FUNCTIONAL CONNECTIVITY AND MRI RADIOMICS BIOMARKERS IN POST-STROKE COGNITIVE IMPAIRMENT PREDICTIVE MODELS – A STUDY PROTOCOL
Hanna-Maria Dragos*1,2
1University of Medicine and Pharmacy "Iuliu Haţieganu" Cluj-Napoca, Neuroscience, Cluj-Napoca, Romania, 2RoNeuro Institute for Neurological Research and Diagnostic, Cluj-Napoca, Romania
On behalf of:
Background and aims: Post-stroke cognitive impairment (PSCI) occurs in about 20% of acute ischemic stroke (AIS) patients and it is associated with poor long-term prognosis. The mechanisms contributing to PSCI are insufficiently understood. A quantitative approach to understanding PSCI is needed, considering the concept of brain reserve assessed by functional connectivity and brain MRI radiomics analysis. Our hypothesis is that predictive models that integrate clinical features, connectivity and MRI radiomics markers of brain reserve could better predict the occurrence of PSCI. The primary objective of the study is to evaluate the predictive role of functional connectivity and MRI radiomics markers in PSCI occurrence at six months and one year after AIS.
Methods: This study is an observational hospital-based cohort study of AIS patients. Patients with supratentorial mild or moderate AIS confirmed by brain MRI, with National Institute of Health Stroke Scale between 5 and 15 are included. Patients with prior cognitive decline or dementia are excluded. The participants will be followed up for one year, comprising four visits. Quantitative EEG and brain MRI will be performed at baseline using specific protocols. Neuropsychological assessment will be perfomed at every visit.
Results: This is an ongoing prospective, hospital-based study, aiming to develop a predictive score of PSCI based on clinical, electrophysiological, and neuroimaging quantitative data. Thirty patients were already included.
Conclusions: The proposed multi-modal approach for associating clinical and neuropsychological features with potential markers derived from advanced EEG and brain MRI techniques will enhance our capability to outline the individual cognitive profile of response to AIS.
Disclosures of Interest: No
Abstract N°: 816
Category: 4.30 YSPR – Study Design Workshop
INVESTIGATING THE EFFECTS OF A NOVEL VIRTUAL REALITY MUSIC-BASED MIRROR THERAPY ON UPPER LIMB MOTOR FUNCTION IN CHRONIC STROKE
Thomas Beltrame*1, Max Hollis1, Kenneth Pope1, Belinda Lange2, Susan Hillier3, David Hobbs1
1Flinders University, College of Science & Engineering, Medical Device Research Institute, Bedford Park, Australia, 2Flinders University, College of Nursing & Health Sciences, The Caring Futures Institute, Bedford Park, Australia, 3University of South Australia, Allied Health & Human Performance, Adelaide, Australia
On behalf of:
Background and aims: The cost of stroke is significant; unilateral motor impairments are experienced by 50% of chronic stroke survivors, and delivering long-term, ongoing rehabilitation is challenging. Thus, there is a need to provide accessible therapy, that can be undertaken independently.
The project aims to address this need by developing a novel Virtual Reality (VR) intervention for Upper Limb (UL) rehabilitation. The VR program combines virtual musical instruments with Virtual Reality Mirror Therapy (VRMT).
Methods: The VR application (Figure 1 & Figure 2) is currently being co-designed with two populations: stroke survivors and professionals (clinicians, researchers & engineers). The co-design will conclude in April 2024 and the resultant feedback is expected to increase participant engagement, system usability, and UL outcomes.
A 12-week in-home Single Case Experimental Design pilot trial with 30 participants is scheduled for June 2024.
The pilot trial will be delivered via the Meta Quest 3 VR headset and use an Axivity AX6 Activity Monitor (AM) to quantify changes in affected arm use during the intervention.
Assessments include the Fugl-Meyer Assessment of Motor Recovery for Upper Extremity, Stroke Impact Scale, and Profile of Mood States.
Results: To date, the co-design has obtained feedback from six participants (one stroke survivor and five professionals). The insights highlighted critical improvements that will be implemented prior to pilot trial commencement. Importantly, no participants reported experiencing motion sickness (Table 1).
Conclusions: VR shows significant rehabilitative promise, and the upcoming pilot trial will evaluate the feasibility and preliminary effectiveness of this novel music-based VRMT.
Disclosurses of Interest: No
Abstract N°: 2990
Category: 4.30 YSPR – Study Design Workshop
OPTIMIZING MANAGEMENT STRATEGIES IN ACUTE ISCHEMIC STROKE CARE IN PATIENTS AGED 80 YEARS OR OLDER
Greta Sahakyan*1,2, Mira Orduyan2, Gurgen Hovhannisyan3, Hovhannes Manvelyan3
1YEREVAN STATE MEDICAL UNIVERSITY, Neurology, 2Astghik Medical Center, 3YEREVAN STATE MEDICAL UNIVERSITY
On behalf of:
Background and aims: Acute stroke care approach in patients ⩾ 80 years remains controversial based on routine clinical practice scenarios. The aim of the research study is to investigate and evaluate the applicability, safety and efficacy of reperfusion therapies (intravenous thrombolysis and/or endovascular thrombectomy) in ischemic stroke patients aged 80 years or older in five years period, which will lead to the development of post-intervention poor prognostic criteria and age-related optimal management strategies in a resource limited context.
Methods: All patients treated in stroke unit and general neurology department are being prospectively recruited starting from February of 2021. Primary objective is the evaluation of mRs, Barthel index and cognitive functioning at 3 and 24 months after stroke. Secondary objective is the identification of clinical and radiological factors associated with poor prognostic outcome. Tertiary objective is the evaluation of patients’ post-stroke experience and age-related specific needs.
Results: Till December of 2023, a total of 137 patients treated with reperfusion therapies and 80 patients treated with standard therapy have been included in the study. Patients in the standard therapy group have worse outcome in the terms of increased mortality, disability and cognitive impairment (p<0.01). Nonsignificant difference is found regarding patient experience and needs between the 2 groups.
Conclusions: Our research project is designed to address the unique challenges in stroke care of patients aged ⩾ 80 years aiming to optimize clinical outcomes, reduce healthcare costs and improve the quality of life of stroke survivors.
Disclosures of Interest: No
Abstract N°: 4039
Category: 4.30 YSPR – Study Design Workshop
LEFT OR RIGHT? UNCOVERING THE EFFECT OF LATERALIZATION ON INSULAR STROKE CLINICAL OUTCOMES
Sara Tartaglia*1, Fedra Kuris1, Roberto Sperotto1, Laura Ceccarelli1, Daniele Bagatto2, Giovanni Merlino1,3, Simone Lorenzut3,4, Lorenzo Verriello4, Mariarosaria Valente1,5, Giada Pauletto6
1Clinical Neurology Unit Udine, Udine University Hospital,, udine, Italy, 2Division of Neuroradiology, Udine University Hospital, udine, Italy, 3University of Udine, Stroke Unit, udine, Italy, 4Udine University Hospital, Neurology Unit, udine, Italy, 5Udine University Hospital, Department of Medicine (DAME), udine, Italy, 6Udine University Hospital, Neurology Units, udine, Italy
On behalf of:
Background and aims: Historically, much evidence in literature suggest that right insular strokes may be associated with worse clinical outcome compared to left insular strokes. Nonetheless, data are controversial and emerging multicentric studies suggested that lateralization of stroke does not influence the outcome. To broad knowledge on this topic, in the present study, we investigated a monocentric insular stroke population, analyzing the impact of lateralization on clinical outcomes and mortality.
Methods: We conducted a retrospective study on consecutive patients with ischemic insular strokes occurred between January 2020 and December 2021, visually assessed by a board-certified Neuroradiologist. Patients were distinguished in right insular stroke (RIS) group and left insular stroke (LIS) group and they were statistically compared. Outcome measures included major NIHSS score at discharge, major neurological improvement at discharge (improvement of 8 points on the NIHSS baseline or NIHSS of 0-1 at discharge); 3-months favorable outcome (mRS 0-2 or same anamnestic mRS at 3 months from discharge), in-hospital mortality and 3-months mortality.
Results: A total of 113 patients were included: 43 in the RIS group and 70 in the LIS group. Statistically significant difference between the two groups was not found in terms of major NIHSS score at discharge, major neurological improvement at discharge, 3-months favorable outcome, in-hospital mortality and 3-months mortality.
Conclusions: According to our results, lateralization of insular stroke does not influence clinical outcomes and mortality. Prospective studies are needed to better investigate these aspects.
Disclosures of Interest: No
Abstract N°: 4062
Category: 4.30 YSPR – Study Design Workshop
A STUDY ON THE CORRELATION BETWEEN HYPERURICAEMIA AND ACUTE ISCHEMIC STROKE PROGNOSIS
Teodora Manolova1,2, Dimitra Chatzithoma*1,2, Lachezar Manchev2,3, Georgi Georgiev1,2
1UMHAT Prof. Dr Stoyan Kirkovich, Neurology, Stara Zagora, Bulgaria, 2Trakia University, Medical Faculty- Stara Zagora, Neurology, Psychiatry and Radiology, Stara Zagora, Bulgaria, 3Heart and brain hospital- Burgas, Radiology, Burgas, Bulgaria
On behalf of:
Background and aims: Elevated serum uric acid (SUA) levels have been associated with an increased Risk of cardiovascular (CV) disease and acute ischemic stroke (AIS). It is hypothesized that uric acid causes vascular damage by several mechanisms.
We aimed to discover a correlation between elevated SUA and NIHSS score and between hyperuricaemia and disability outcome at the patients‘ discharge. We investigated SUA in 160 hospitalized patients with acute ischaemic stroke not treated with thrombolysis or thrombectomy. All investigated patients suffered an AIS in the internal carotic artery (ICA). We performed a statistical analysis of a quantitive research on the correlation between hyperuricaemia, NIHSS score and also between hyperuricaemia and the neurological outcome of patients with AIS.
Methods: Statistical methods used: 1. Descriptive statistics for qualitative and quantitative variables. 2. Kolmogorov-Smirnov and Shapiro-Wilk test. 3. One-way ANOVA with Post Hoc Multiple Comparisons, Dunnett test. 4. Non-parametric correlation – Spearman‘s correlation coefficient. 5.Significance level set equal to P<0.05. 6. Statistical analyzes were performed with the IBM SPSS Statistics 25 statistical package.The disability degree is measured by using the Modified Rankin Score (mRS). NIHSS was used to define the ischemic stroke severity.
Results: 1.Direct moderate statistically significant correlation ρ=0.37, P<0.0001 was found between SUA and disability at discharge.
2. There was no statistically significant correlation between uric acid levels and NIHSS severity (P>0.05).
Conclusions: Although, no correlation between hyperuricaemia and NIHSS score was found, our research showed a significant correlation between hyperuricaemia and disability outcome at discharge.
Disclosures of Interest: No
Abstract N°: 4103
Category: 4.30 YSPR – Study Design Workshop
TRANSCRANIAL DOPPLER AS A FUNCTIONAL PROGNOSTIC TOOL INCENTRAL NERVOUS SYSTEM VASCULITIS
José de Jesús García Rivera1, Jacqueline Moreno Arias1, Kevin Giuseppe Enriquez Peregrino1, Idarmis Brisseida Reyes Cortés1, Vanessa Cano Nigenda*1, Antonio Arauz Gongora1, Andrés Alberto Mercado Pompa1, Adrián Pereda Castillo1, Andony Isabel Camacho Gámez1, Ricardo Romero Vucovich1
1Instituto Nacional de Neurología y Neurocirugía
On behalf of: Liliana Escobar Pérez, Luis Esteban Ramírez González, Paul Jhovanny Rodríguez Flores, Thalia Esmeralda Morfín Morales, Jefferson Ramirez, Enrique Isaac Tetlalmatzi Azuara
Background and aims: Transcranial Doppler(TCD) is a low-cost, noninvasive test that can provide accurate information on intracranial blood flow velocities. Information on its use as a diagnostic tool in Central Nervous System(CNS) vasculitisis is scarce.
Methods: retrospective cohort since 2016-2023 in patients with diagnosis of CNS vasculitis. Vessels evaluated in TCD: Anterior Cerebral Artery(ACA), Middle Cerebral Artery(MCA) and Posterior Cerebral Artery(PCA). Their association with an unfavorable functional outcome (mRS 3-6) at 3 months was evaluated. Descriptive and inferential statistics were performed.
Results: Total 187 participants of which 148 with complete records were included, 85(57.4%) men, mean age 39.9(±13.6), 45(30.4%) were infectious vasculitis and 103(69.6%) of undetermined etiology. The most frequent infectious etiologies were 23(46%) for cryptococcosis, 12(24%) tuberculosis and 8(16%) neurocysticercosis, 43(30.9%) patients had immunodeficiency, the most frequent: HIV 28(59.6%), diabetes 13(27.7%), immunosuppressant use 2(4.3%). MRI studies showed infarction in 29(28.2%), hemorrhage in 4(5.3%), pachymeningitis in 21(20.4%) and 33(32%) were normal. Parameters of the first TCD, Mean Velocity.
(MV) and Pulsatility Index(PI) were: ACA MV 59.8 cm/s(±24.93) and PI 1.03(±0.30); MCA MV 92.3cm/s(±80.1) and PI 1.01(±0.34); PCA MV 45.6 cm/s(±13.4) and PI 0.97(±0.31). MV elevation in MCA at initial TCD was associated with an increased likelihood of having an unfavorable functional outcome at 3-month follow-up (OR 4.06;95% CI 1.55-10.63; p=0.003).
Conclusions: TCD is a valid adjunctive tool to assess the functional prognosis of patients with CNS vasculitis. Increased MV in the MCA in the initial TCD study is associated with an unfavorable functional outcome at 3 months in CNS vasculitis.
Disclosures of Interest: No
Abstract N°: 4111
Category: 4.30 YSPR – Study Design Workshop
DEVELOPMENT OF HEMORRHAGIC STROKE IN CHRONIC LYMPHOCYTIC LEUKEMIAS AND ITS CLINICAL FEATURES
Rustambek Matmurodov*1, Guzal Eshchanova1
1Tashkent Medical Academy, Neurology, Tashkent, Uzbekistan
On behalf of:
Background and aims: Chronic lymphocytic leukemia is more common in older people, and recently this disease is getting younger. One of the main causes of hemorrhagic complications is thrombocytopenia.
Aim. Study of development and clinical characteristics of hemorrhagic stroke in patients with chronic lymphocytic leukemia.
Methods: To conduct research, 56 patients (38 men and 18 women) suffering from chronic lymphocytic leukemia were examined in the multidisciplinary clinic of Khorezm region. The average age of the patients was 61.7±5.6 years. The average duration of the disease is 3.8 ± 2.1 years. Clinical-neurological and neurovisual MRI and CT examination methods were used.
Results: Hemorrhagic stroke was noted in 18 of 56 patients with chronic lymphocytic leukemia (32.1%). When comparing the patients by gender, it was found that 12 men (66.7%) and 6 women (33.3%) were found. When comparing the types of hemorrhagic stroke, parenchymatous strokes were 8 (44.4%) and subarachnoid hemorrhage was 6 (42.8%), ventricular hemorrhage was 1 (5.5%), and mixed hemorrhage was 3 (7.3 %) met. The average age of men who had a hemorrhagic stroke was 45.5±5.6 years, and 77.9 years in women. Parenchymatous stroke predominated in men (58.3%), while subarachnoid hemorrhages were more common in women (66.65%). It has been found that the mortality rate is earlier in men than in women, and the duration of the disease is also shorter.
Conclusions: The development of hemorrhagic strokes in chronic lymphocytic leukemias depends on the gender of the patients, and in turn, it differs sharply according to the types of hemorrhagic stroke
Disclosures of Interest: No
Abstract N°: 4115
Category: 4.30 YSPR – Study Design Workshop
ENDOVASCULAR THROMBECTOMY FOR LARGE CORE STROKES - A SYSTEMATIC REVIEW AND META-ANALYSIS WITH TRIAL SEQUENTIAL ANALYSIS
Marco Antonnio Rocha Dos Santos1, Pierludovico Moro*2, Abner Lucas Balduino de Souza3, Lauren Nirta4, Márcio Rodrigues Venturini5, Thaís Pereira Mendes6, Laura de Lima Xavier7, Ming-Chieh Ding7
1University of the Santa Catarina plateau, Lages, Brazil, 2Università La Sapienza, Dipartimento di Neurologia e Psichiatria, Rome, Italy, 3Evangelical University of Goiás, Anápolis, Brazil, 4Pusan National University Yangsan Hospital, Yangsan, South Korea, 5SARAH Network of Rehabilitation Hospitals, Brazil, 6Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, Brazil, 7University of North Carolina, United States
On behalf of:
Background and aims: Endovascular thrombectomy (ET) is the standard care for large vessel occlusion in acute ischemic stroke, but initial trials excluded large core stroke patients. Recent studies suggest ET's feasibility and potential neurological benefit in this population. We conducted a systematic review and meta-analysis to assess ET's efficacy and safety in large core strokes.
Methods: Literature searches in PubMed, Embase, and Cochrane databases were performed until November 2023. Peer-reviewed randomized controlled trials comparing mechanical thrombectomy to best medical treatment among large core stroke patients (ASPECTS<6 or core >50 mL in perfusion imaging) within 24 hours of symptom onset were included.
Results: Five articles including 1,564 patients were analyzed, with 786 patients undergoing ET. ET showed improved neurological outcomes defined as Modified Rankin Scale (mRS) ⩽2, indicating no significant disability (OR 2.91, 95% CI 2.09–4.06, p<0.001, I2 30%) and mRS ⩽3, indicating slight disability with independent walking (OR 2.22, 95% CI 1.72–2.86, p<0.001, I2 10%) but increased intracranial bleeding risk (OR 2.65, 95% CI 1.35–5.22, p= 0.005, I2 67%) and symptomatic intracranial bleeding (OR 1.87, 95% CI 1.06–3.30, p=0.03, I2 0%). No differences were found in mortality or decompressive craniectomy. Subgroup analysis of patients with plain brain computed tomography (CT) with CT angiography also showed favorable outcomes (OR 3.24, 95% CI 1.52–6.92, I2 57%).
Conclusions: ET improved neurological outcomes and independent walking in large core acute ischemic stroke. However, it increased the risk of intracranial bleeding.
Baseline characteristics of the included studies.
Risk of Bias 2 Tool
Disclosures of Interest: No
Abstract N°: 4211
Category: 4.30 YSPR – Study Design Workshop
BRIDGING THROMBECTOMY OUTPERFORMS DIRECT ENDOVASCULAR THROMBECTOMY BY REDUCING FUTILE RECANALIZATION: EVIDENCE FROM A MULTICENTER CHINESE COHORT
Zhicai Chen*1, Min Lou1, Xin Huang1
1The Second Affiliated Hospital of Zhejiang University, School of Medicine, Neurology, Hangzhou, China
On behalf of:
Background and aims: In real-world settings where longer onset-to-puncture (OPT) are common, the effectiveness of bridging endovascular therapy (EVT) with intravenous thrombolysis (IVT) versus direct EVT without IVT remains uncertain.
Methods: We conducted a retrospective analysis using data from a national prospective stroke registry. A favorable outcome was defined as a modified Rankin Scale (mRS) score of 0–2 at 3 months, and good outcome as mRS score 0–3. Futile recanalization was defined as 3-month mRS score 3-6 (definition 1) or 4-6 (definition 2), despite achieving a modified Thrombolysis in Cerebral Infarction (mTICI) score of 2b/3 post-EVT. Univariate analysis and binary logistic regression model were applied to investigate the relationship of bridging EVT and different outcome parameters in both full cohort and the subgroup cohort with OPT ⩽ 4.5 hours and without IVT contraindication.
Results: A total of 5926 patients were enrolled in the final analyses. Binary logistic regression analyses revealed that bridging EVT was independently associated with an increased likelihood of a favorable outcome (Odds Ratio [OR], 1.182; 95% Confidence Interval [CI], 1.045-1.336; P=0.008) and good outcome (OR, 1.177; 95% CI, 1.042-1.328; P=0.009). It was also associated with a decrease in futile recanalization (OR, 0.873; 95% CI, 0.767-0.994; P=0.040 for both definitions). These associations were consistent in the subgroup analysis for patients with an OPT ⩽ 4.5 hours without contraindications to IVT.
Conclusions: Bridging EVT demonstrates superior outcomes compared to direct EVT in real-world settings, where extended OPT are more prevalent, supporting the utilization of IVT in eligible patients.
Disclosures of Interest: No
Abstract N°: 4217
Category: 4.30 YSPR – Study Design Workshop
FUNCTIONAL COGNITION ASSESSMENT AMONG COMMUNITY DWELLING STROKE SURVIVORS
Background and aims: Functional cognition is essential for accomplishing everyday activities strongly relying on cognitive abilities. Stroke frequently causes impairments in functional cognition and restrictions in daily participation. Several different measures of cognition are used by clinicians, and there is a need to examine which assessments have the strongest correlations with daily participation and quality of life. The aim of this study was to examine correlations between three different measures of cognition and functional cognition, and their correlation with participation and quality of life.
Methods: 52 stroke survivors, men and women, ages 47-87, at least half a year post stroke onset, living independently in the community, with a MoCA (Montreal Cognitive Assessment) score of 19+, were included. Several assessment tools were used to examine aspects of participants’ cognition, activity, participation, and QOL.
Results: The neuropsychological cognitive test final score had significant medium-strong correlations with the ecological cognitive test final score (p<0.001) and with participation (p=.017). however, no significant correlations were found between the functional cognition self-report measure and other cognitive tests, participation or quality of life (n.s.).
Conclusions: Study findings may provide rehabilitation professionals with essential knowledge of relevant functional cognition measures, and their relation to participation and quality of life. The lack of correlations of functional cognition subjective report with other tests may indicate that it reflects additional aspects, besides cognition. Future studies including larger samples are needed to develop measures of functional cognition, for clinical populations, including stroke.
Disclosures of Interest: No
Abstract N°: 4231
Category: 4.30 YSPR – Study Design Workshop
RESISTANCE TO ANTIPLATELET AGENTS IN PATIENTS WITH NONCARDIOEMBOLIC ISCHEMIC STROKE
Tatyana Batenkova*1
1UGMU, Neurologist, Ekaterinburg
On behalf of:
Background and aims: Antiplatelet therapy is effective as a secondary prevention of noncardioembolic stroke. Resistance to aspirin is 5-60%, and to clopidogrel is 17-25%. Inadequate dosage of antiplatelet drugs or the development of resistance to them can provoke repeated brain catastrophes. Evaluate the effectiveness of antiplatelet therapy in patients aged 18 to 59 years who have suffered an ischemic noncardioembolic stroke.
Methods: using the "Optical aggregation" method in this cohort of patients, to evaluate the effectiveness of antiplatelet therapy in dynamics with an interval of 3,6,9,12 months.
Results: 32 patients aged 18-44 years (young stroke group), 41 patients aged 45-59 years (middle age group) who had suffered a non-cardioembolic stroke were analyzed. Everyone was taking acetylsalicylic acid (ASA). When optical aggregation was performed after 3 months, resistance was revealed in 2 men only in the young stroke group. Their adrenaline value was within the normal range. Each of them was transferred to clopidogrel. One of them was found to be resistant to clopidogrel. Subsequently, the dosage of acetylsalicylic acid was increased 2x, clopidogrel 75 mg per day was left. This combination of antiplatelet agents made it possible to achieve effective platelet aggregation (no bleeding was observed). In the middle-aged stroke subgroup, only one woman had an extremely low decrease in adrenaline (result 1, ADP 2.5 35) against the background of taking ASA 100 mg per day. Her dosage was reduced to 75 mg per day with subsequent control of optical aggregation.
Conclusions: This method is important for timely change of therapy and prevention of repeated strokes.
Disclosures of Interest: No
Abstract N°: 4246
Category: 4.30 YSPR – Study Design Workshop
EFFECTIVENESS OF WOVEN ENDOBRIDGE DEVICE FOR THE TREATMENT OF INTRACRANIAL BIFURCATION AND WIDE NECK ANEURYSMS: A SYSTEMATIC REVIEW AND META-ANALYSIS
César Bigran Espinosa-Cantú*1, Jorge Alberto Cantú Hernández1, Pablo Adrián Luna Pérez1, Maurilio Ochoa González1, Paula Fernanda Zarate Ángeles1, Jesus Morales1, Ángel Raymundo Martínez Ponce de León1
1Universidad Autónoma de Nuevo León, Neurocirugía y Terapia Endovascular Neurológica, Monterrey
On behalf of:
Background and aims: The use of Woven Endobridge (WEB) is a contemporary and effective approach to wide-neck bifurcation aneurysm.
Methods: A systematic review was conducted by searching non-randomized interventional studies that compared the use of the WEB with any other endovascular device for the treatment of wide neck and bifurcation intracranial aneurysms, regardless if they were ruptured or not, in several electronic databases. The main outcomes were angiographic occlusion classification (rated by RRCO), functional status after embolization (mRS score ⩽2), and post-surgical complications (related or not to the procedure). Outcomes were analyzed using Odds Ratios (OR), using a random-effects model through the Mantel-Haenszel method. Cochran's Q-statistic and I²-statistic were used to assess heterogeneity. R studio software was employed.
Results: Among 751 studies that were screened, only 9 references were considered for the final review and 7 for quantitative synthesis. A total of 894 patients were included, and 327 of these were treated with the WEB device. Meta-analysis of the safety-related outcome showed a significant decrease in the complications rates of patients treated with WEB compared with Stent-Assisted Coiling (Overall OR [CI95%] 0.34[0.14-0.83], p=.02). In the clinical and functional outcome assessment, patients treated with WEB showed a significantly higher rate of good outcome by mRS than those treated by Coiling (Overall OR [CI95%] 1.47[1.01-2.13], p=.04).
Conclusions: Our team's analysis revealed that WEB-treated patients compared to those treated with SAC showed decrement in complications and better functional outcome compared with the patients treated with Coiling.
Disclosures of Interest: No
Scientific Communication - Large Clinical Trials Session
Abstract N°: 374
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
FUNCTIONAL OUTCOME AND QUALITY OF LIFE AT 12 MONTHS AFTER THROMBECTOMY FOR STROKE WITH EXTENDED LESION IN THE TENSION TRIAL
Götz Thomalla*1
1Universitätsklinikum Hamburg-Eppendorf, Klinik und Poliklinik für Neurologie, Hamburg, Germany
On behalf of: On behalf of the TENSION investigators
Background and aims: In the TENSION trial, endovascular thrombectomy was associated with improved functional outcome and lower mortality at 90 days in patients with acute ischaemic stroke from large vessel occlusion with established large infarct. In a secondary analysis we studied the long-term effect of thrombectomy on functional outcome and self-reported quality of life at 12 months.
Methods: TENSION was a randomized, open label, blinded endpoint evaluation trial to compare the safety and efficacy of thrombectomy as compared to best medical care alone in stroke patients with extended lesions defined by an Alberta Stroke Program Early CT Scan score (ASPECTS) of 3-5 and in an extended time window (up to 12 hours, or unknown time of symptom onset). Secondary endpoints at 12 months after stroke comprised a shift in the mRS, self-reported functional health status evaluated by the EQ-5D and PROMIS-10 questionnaires, and post-stroke anxiety and depression evaluated by the PHQ-4 questionnaire. TENSION is registered at ClinicalTrials.gov (NCT03094715).
Results: 253 patients were randomly assigned, with 125 patients assigned to endovascular thrombectomy and 128 to medical treatment alone. Long-term follow-up at 12 months after stroke was available for 244 (96.4%) of randomized patients. Results on long-term effect of thrombectomy on functional outcome and self-reported health status at 12 months will be presented at the conference.
Conclusions: This analysis of the TENSION trial will provide important additional results on long-term efficacy and safety of thrombectomy including patient reported outcome measures in patients with large ischemic core in an extended time window.
Disclosures of Interest: Yes TENSION received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No 754640.
Scientific Communication - Intracerebral Hemorrhage
Abstract N°: 622
Category: 1.04 REHABILITATION & RECOVERY
CLINICAL OUTCOMES IN PATIENTS WITH ICH RECEIVING ANDEXANET ALFA – RESULTS FROM THE PROSPECTIVE OBSERVATIONAL ASTRO-DE STUDY
Nils Kuklik1,2, Anika Hüsing1, Marcus Brinkmann1,2, Andreas Stang1,3, Hans-Christoph Diener*1
1Institute for Medical Informatics, Biometry and Epidemiology, Medical Faculty, University of Duisburg-Essen, Essen, Germany, 2Centre for Clinical Trials Essen, University Hospital Essen, Essen, Germany, 3School of Public Health, Department of Epidemiology, Boston University, Boston, United States
On behalf of: ASTRO-DE Investigators
Background and aims: Haematoma expansion after intracranial haemorrhage (ICH) significantly influences clinical outcomes, emphasising the need for effective reversal agents. Andexanet alfa is a specific antidote for factor Xa inhibitors. The ASTRO-DE study provides real-world evidence on the effect of andexanet alfa on mitigating haematoma expansion and altering prognosis in rivaroxaban or apixaban-treated patients with ICH.
Methods: Andexanet alfa: non-interventional study in Stroke Units in Germany (DE) (ASTRO-DE) is a prospective observational study on the effect of andexanet alfa after acute ICH, conducted in 25 German stroke units. Primary outcomes are change in haematoma volume, and proportion of patients with good haemostasis (haematoma growth below 33% at first control imaging).
Results: In total, 137 patients (47.5% male, mean age 80.0 years) with ICH (93% spontaneous, 7% trauma-related, mean NIHSS on admission 11.2 (SD 8.1), mean initial haematoma volume 26.5 mL (SD 32.5) were analysed, 66% of patients were treated with apixaban and 34% with rivaroxaban. Andexanet alfa was applied on average 5.4 hours (SD 5.1) after index event. Good haemostasis occurred in 94% of 98 evaluable patients, mean change in haematoma volume was 0.4 mL (95% CI, -2.0-2.8) evaluated by first control imaging, which was 21.4 hours (mean, SD 18.2) after initial imaging. During hospitalization, 30 patients (21.9%) died, 10 (7.3%) had thromboembolic events.
Conclusions: ASTRO-DE is the first prospective observational study systematically collecting standardised clinical routine data on the treatment with andexanet alfa. The conference presentation will provide further in-depth results on haematoma expansion and functional outcomes.
Disclosures of Interest: Yes The ASTRO-DE study was funded by an unrestricted grant from Alexion Pharmaceuticals
Scientific Communication - Secondary Prevention
Abstract N°: 964
Category: 1.01 ACUTE MANAGEMENT - Neither thrombolysis nor thrombectomy
EARLY DIRECT ORAL ANTICOAGULANT INITIATION POST INTRACRANIAL HAEMORRHAGE AMONG JAPANESE PATIENTS WITH ATRIAL FIBRILLATION
1National Cerebral and Cardiovascular Center, Department of Cerebrovascular Medicine, Suita, Japan, 2The Jikei University School of Medicine, Department of Neurology, Tokyo, Japan, 3Iwate Medical University, Division of Neurology and Gerontology, Department of Internal Medicine, School of Medicine, Yahaba, Japan, 4National Cerebral and Cardiovascular Center, Department of Neurosurgery, Suita, Japan, 5Jichi Medical University, Division of Neurology, Department of Medicine, Shimotsuke, Japan, 6University of Miyazaki, Clinical Research Support Center, University of Miyazaki Hospital, Faculty of Medicine, Miyazaki, Japan, 7Yamagata City Hospital Saiseikan, Department of Neurosurgery, Yamagata, Japan, 8Iwate Prefectural Central Hospital, Department of Neurosurgery, Morioka, Japan, 9Japanese Red Cross Kumamoto Hospital, Department of Neurosurgery, Kumamoto, Japan
On behalf of: SAFE-ICH Registry group
Background and aims: Efficacy and safety of early direct oral anticoagulation (DOAC) in atrial fibrillation (AF) patients after onset of intracranial haemorrhage (ICH) is unknown. The SAFE-ICH registry is the first prospecitve study to investigate the occurrence of ischemic and haemorrhagic events after early DOAC initiation post-ICH in Japanese AF patients.
Methods: This multicentre, prospective, observational study included AF patients aged ⩾20 years scheduled to receive DOAC ⩽14 days following symptomatic ICH. Primary composite outcome was the occurrence of symptomatic ICH, all-stroke, or death ⩽30 days after DOAC initiation (key secondary outcomes, see Figure).
Results: Of the 247 patients included in the final data analysis from 254 enrolled, 240 patients (97%) initiated DOAC ⩽14 days of ICH onset while 7 (3%) did not. Among the 240 patients who initiated, 61% were male with a mean[SD] age of 79±9.3 years; 84.6% suffered from intraparenchymal haemorrhage, 1.6% from intraventricular haemorrhage, 0.8% from acute epidural haematoma, and 12.9% from acute subdural haematoma. The median (interquartile range) baseline NIHSS score was 7 (2–16), and hematoma volume was 10ml (3.5–25.0). Median (interquartile range) days of DOAC initiation following ICH was 7 (5–10). Within 30 days after DOAC initiation, the primary endpoint occurred in 12 (5%) patients. Five patients died none of which were due to any stroke. For a summary of secondary outcome events, see Table.
Conclusions: In Japanese AF patients, early DOAC initiation ⩽14 days post-ICH appears to have an acceptable risk profile for ischaemic and haemorrhagic events.
Disclosures of Interest: Yes This study is a collaborative study conducted by clinical researchers in partnership with Daiichi Sankyo Company, Limited.; MK received honoraria from Bayer Yakuhin, Daiichi-Sankyo, and BMS/Pfizer, and research support from Nippon Boehringer Ingelheim outside of the submitted work.
Scientific Communication - Imaging
Abstract N°: 978
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
ATTEST2 IMAGING SUBSTUDY
Ammad Mahmood*1, Sam Neilson1, Gary Ford2, Chris Price3, Mary Joan Macleod4, Nikola Sprigg5, Joanna Wardlaw6, Ian Ford7, Grant Mair6, Keith Muir1
1University of Glasgow, School of Neuroscience and Psychology, United Kingdom, 2University of Oxford, United Kingdom, 3Newcastle University, United Kingdom, 4University of Aberdeen, United Kingdom, 5University of Nottingham, United Kingdom, 6University of Edinburgh, United Kingdom, 7University of Glasgow, United Kingdom
On behalf of:
Background and aims: ATTEST2 (NCT02814409) was a trial comparing tenecteplase to alteplase in patients treated for acute ischaemic stroke (AIS) within 4.5 hours of onset. We analysed the subgroup of patients with perfusion imaging.
Methods: Patients conventionally eligible for intravenous thrombolysis presenting within 4.5 hours of symptom onset were randomised to receive tenecteplase 0.25mg/kg or alteplase 0.9mg/kg. All patients had baseline and follow up non-contrast CT (NCCT) scans, further imaging was at the discretion of the site. All patients undergoing baseline CT perfusion (CTP) imaging were included in the imaging substudy. Baseline NCCT, CTP and CT angiography (CTA); and follow up NCCT and MRI were analysed. Central imaging analysis determined presence of intracranial occlusion, dense vessel sign, and collateral scoring. RAPID software was used to calculate automated ASPECTS score, and areas of predicted ischaemic core (CBF<30) and penumbra (Tmax>6, CBF>30). Follow up infarct volumes were manually calculated using Mango software for MRI by 2 readers (AM and SN) and MiSTAR software for NCCT. The association of tenecteplase with greater salvage of ischaemic tissue; greater rates of recanalisation; and greater improvement in clinical outcome in those with large vessel occlusion and small ischaemic core will be tested.
Results: Of the 1776 patients recruited to ATTEST2, 314 had CTP imaging and were included in the imaging substudy. Unblinded clinical and central imaging data is awaited.
Conclusions: The ATTEST2 imaging substudy will give further insights into the differences between tenecteplase and alteplase in AIS in pre-specified subgroups.
Disclosures of Interest: Yes KM is Chief Investigator of ATTEST2 funded by the Stroke Association and British Heart Foundation and supported by Boehringer Ingelheim and UK CI for the TEMPO-2 trial supported by Canadian Institute of Health Research and British Heart Foundation.
Scientific Communication - Service Organisation
Abstract N°: 3020
Category: 1.02 ACUTE MANAGEMENT - Thrombolysis or thrombectomy
SUSTAINABILITY OF THE FLYING INTERVENTION TEAM FOR ENDOVASCULAR TREATMENT IN STROKE: A 6-YEAR OBSERVATIONAL STUDY
Nikolai Hubert1, Lucie Esterl-Pfäffl1, Jan Rothaupt2, Thomas Witton-Davies2, Moritz Leitner1, Philip Bath3, Heinrich Audebert4, Anastasios Mpotsaris2, Roman Haberl1, Gordian Hubert*1
1Munich Clinic, Academic teaching hospital of the Ludwig-Maximilians-University, TEMPiS Telemedical Stroke Center, Department of Neurology, Munich, Germany, 2Munich Clinic, Academic teaching hospital of the Ludwig-Maximilians-University, Department of Diagnostic and Interventional Radiology and Neuroradiology, Munich, Germany, 3University of Nottingham, Stroke Trials Unit, Nottingham, United Kingdom, 4Charité Universitätsmedizin Berlin, Department of Neurology, Campus Benjamin Franklin, Berlin, Germany
On behalf of: FIT study group
Background and aims: Deploying a Flying Intervention Team (FIT) for endovascular treatment has been shown to be effective in reducing treatment delays for patients in nonurban areas. In this system of care, a team comprising a neurointerventional radiologist and an assistant is airlifted via helicopter from a network hub to rural primary stroke centers to perform thrombectomy on-site. However, the long-term sustainability of this effect remains unexplored. This study aims to comprehensively evaluate the impact of the FIT model over a 6-year period.
Methods: Consecutive patients eligible for thrombectomy and enrolled in the FIT trial as well as a subsequent prospective registry between 02/2018 and 12/2023 were included in this multicenter observational study. All patients were admitted to one of 15 regional primary stroke centers and received either FIT care or patient interhospital transfer to a comprehensive stroke center. We analyze time metrics, treatment rates, workflow, safety and clinical outcome parameters.
Results: Among 1505 patients included, 53% were female, and mean age was 75±12. FIT was deployed in 660 (44%) patients and 845 (56%) underwent interhospital transfer. The findings will provide a comprehensive overview of demographic and baseline variables, workflow and outcomes, including temporal trends of key parameters within the study period.
Conclusions: Since its establishment in 2018, the Flying Intervention Team has marked a significant advancement in the provision of endovascular treatment for stroke patients in rural areas. The analysis will show the level of sustainability of this system of care over an extended time period.
Disclosures of Interest: Yes N. D. Hubert and G. J. Hubert received funding from the Bavarian Ministry of Health and the Björn Steiger Foundation