
Abstract
Introduction:
Rural residency has been associated with lower reperfusion treatment rates for acute ischemic stroke in many countries. We aimed to explore urban-rural differences in IV thrombolysis rates in a small country with universal health care, and short transport times to stroke units.
Patients and methods:
In this nationwide cohort study, adult ischemic stroke patients registered in the Danish Stroke Registry (DSR) between 2015 and 2020 were included. The exposure was defined by residence rurality. Data from the DSR, Statistics Denmark, and the Danish Health Data Authority, were linked on the individual level using the Civil Registration Number. Adjusted treatment rates were calculated by balancing baseline characteristics using inverse probability of treatment weights.
Results:
Among the included 56,175 patients, prehospital delays were shortest for patients residing in capital municipalities (median 4.7 h), and longest for large town residents (median 7.1 h). Large town residents were predominantly admitted directly to a comprehensive stroke center (98.5%), whereas 30.9% of capital residents were admitted to a hospital with no reperfusion therapy available (non-RT unit). Treatment rates were similar among all non-rural residents (18.5%–18.7%), but slightly lower among rural residents (17.2% [95% CI 16.5–17.8]). After adjusting for age, sex, immigrant status, and educational attainment, rural residents reached treatment rates comparable to capital and large town residents at 18.5% (95% CI 17.7–19.4).
Discussion and conclusion:
While treatment rates varied minimally by urban-rural residency, substantial differences in median prehospital delay and admission to non-RT units underscored marked urban-rural differences in potential obstacles to reperfusion therapies.

Keywords
Introduction
Geographic location has been associated with large health disparities. Individuals residing in rural or remote areas generally face unfavorable health conditions, including a higher prevalence of cardiovascular risk factors and diseases, higher mortality rates, and reduced life expectancy.1–3 Moreover, disparities extend to the use of reperfusion therapies for ischemic stroke, with lower treatment rates among rural residents in several countries.4–6
Given the positive impact of intravenous (IV) thrombolysis on functional outcome following ischemic stroke, it is pivotal to ensure widespread and equal access to this treatment regardless of place of residence. 7 The association between rural residency and reduced IV thrombolysis rates could be explained, at least partially, by delayed admission resulting from greater distances to stroke units from remote locations. This is reinforced by the finding that several studies point toward admission outside the treatment window as the primary barrier for IV thrombolysis treatment.8–10 Yet, other competing factors could be associated with unequal access to thrombolysis for rural residents, such as age and socioeconomic status.
With access to detailed individual-level nationwide data on a wide range of covariates, it was possible to perform analyses distinguishing between total effects and the influence of patient related factors, such as comorbidities, living alone and socioeconomic status. To our knowledge, inequalities in IV thrombolysis rates according urban-rural residency has only rarely been explored in Europe.11,12 We aimed to investigate variations in thrombolysis rates across five distinct urban-rural strata, based on the patient’s municipality of residence. 13
Methods
Data access
Data from this study can be accessed by researchers from authorized institutions through the Danish Health Data Authority and Statistics Denmark. Approval for the study was granted by the Danish Data Protection Agency (journal number 2019-899/10-0033). According to Danish Legislation, registry-based studies are not required to obtain ethical approval or patient consent.
Study population
This nationwide register-based cohort study, included patients ⩾18 years of age diagnosed with ischemic stroke between January 2015 and December 2020. Ischemic stroke was defined as International Classification of Diseases, Tenth revision codes I63.0-I63.9. For each patient, only the first stroke event during the study period was included. Patients with in-hospital strokes, tourists, and patients with missing data on residence municipality were excluded.
Setting
In Denmark, all permanent residents have access to tax funded health care, and acute stroke treatment occurs exclusively in public hospitals. All departments responsible for acute stroke care are required to report stroke patients to a nationwide stroke register. Furthermore, Denmark is a small country with a land area of 43,000 km2 and a well-developed infrastructure. Transport durations for accessing stroke units are typically short (estimated to median 22 min (IQR 12–34 min) for patients admitted through emergency medical services 14 ), and the most extended travel times span up to 2 h. For islands not connected to mainland by bridge, helicopters generally provide expedient transportation, but delays exceeding 2 h can occur if the helicopter service is temporarily unavailable. This enables all residents to potentially reach a stroke unit offering reperfusion therapy within the required timeframe, thereby minimizing the possible impact of transportation-related delays on geographic inequalities in IV thrombolysis rates.
Data sources
Data for this study originate from various registers, which have been linked on the individual patient level by using the Civil Registration Number, a unique 10-digit personal identifier assigned to all permanent residents of Denmark at birth or upon immigration. 15
The study cohort was obtained from the Danish Stroke Registry (DSR), a nationwide registry encompassing prospectively collected data on stroke patients admitted to Danish hospitals since 2003. The DSR holds information on patient and stroke specific characteristics and has an estimated data completeness of 97%.16,17 Information on age and immigrant status is derived from the population register, which relies on data from the Civil Registration System, that is considered to have both high data validity and coverage. 15 Data on educational level were sourced from the attainment register, in which more than 80% of data originate from highly reliable administrative sources. 18 Data on previous hospitalizations for calculation of the Charlson Comorbidity Index (CCI) are derived from the National Patient Registry. Payments to hospitals rely on the registered diagnoses in this registry, thus providing an important incentive for hospitals to ensure accurate reporting. 19 Data on filled anticoagulation medicine were obtained from the Danish National Prescription Registry, which benefits from electronic registration at Danish pharmacies, ensuring high data accuracy and completeness. 20 All the remaining variables were derived from the DSR. The study adhered to the STROBE guidelines for observational studies with routinely collected data. 21
Exposure
Data on residence municipality were obtained from the DSR. To enhance comparability with international studies, a commonly utilized urban-rural classification of municipalities was adopted.4,22–25 We applied the classification provided by Statistics Denmark for this study, which categorizes municipalities into five urban-rural strata according to a decreasing number of inhabitants in the largest city and a decreasing number of available jobs (Supplemental Materials, Figure S1). 13 “Capital” was defined as municipalities with >200.000 available jobs. “Large town” was defined as municipalities with <200.000 available jobs, but >100.000 inhabitants in the largest town. “Small town” was defined as municipalities with <200.000 jobs available, and 30.000–100.000 inhabitants in the largest town. “Outskirt” was defined as municipalities with 40.000–200.000 available jobs and <30.000 inhabitants in the largest town. “Rural” was defined as <40.000 available jobs and <30.000 inhabitants in the largest town. Job availability was determined by the number of jobs accessible from each municipality based on the commuting distance in driving-time. As an example, jobs located within the same parish counted as 100%, while jobs situated a 10 min drive away counted as 50%, and those accessible within a 30-min drive counted as 12.5%. 13
Outcome
The outcome, IV thrombolysis, was defined as administered if an IV alteplase dosage exceeding 0 mg was registered.
Statistical analyses
Covariates were selected based on expected strong associations with either exposure, outcome or both. Selections were guided by clinical experience and existing evidence prior to any data analysis. A Directed Acyclic Graph was used to display our assumptions about the causal structures, and to distinguish confounding from mediating variables (Figure 1). As illustrated, a confounder is defined as a covariate that serves as a cause of both exposure and outcome, whereas a potential mediator could be on the causal pathway from exposure to outcome.
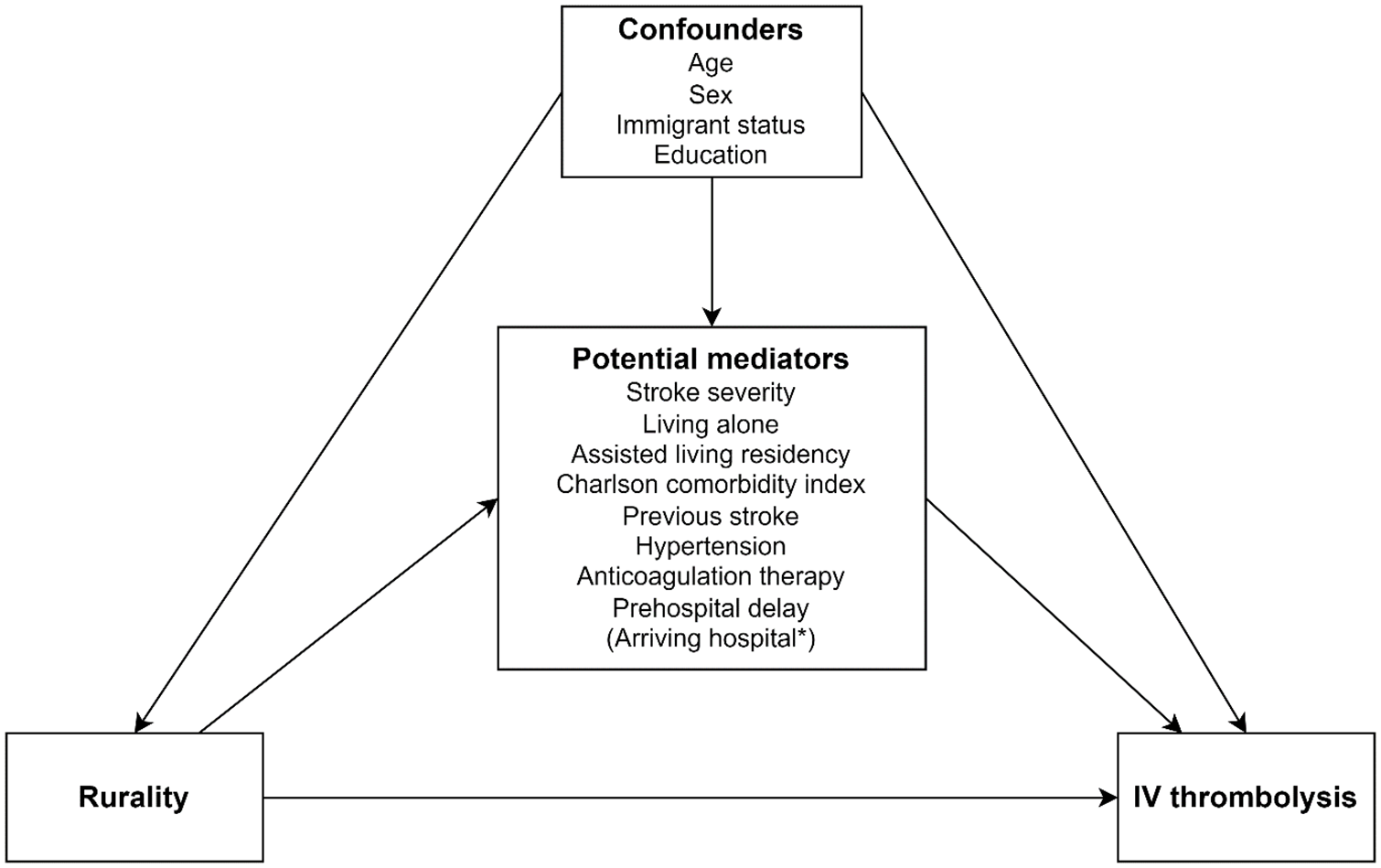
Simplified causal diagram illustrating the causal relationship between rurality, IV thrombolysis and relevant covariates. The graph is not exhaustive.
Highest attained pre-stroke educational level was used to reflect the patient’s socioeconomic status before stroke. Categories encompassed low education (primary and secondary school), medium education (upper secondary school and vocational education), or high education (short, medium, and long-term higher education). Stroke severity was defined by the Scandinavian Stroke Scale and recorded as mild (45–58), moderate (30–44), severe (15–29), or very severe (0–14). Comorbidity was determined according to the CCI and categorized as low (0 points) moderate (1–2 points) or high (⩾3 points). Scores were based on discharge diagnoses from hospital admissions within 10 years before stroke onset, excluding age as a contributing factor, as this was accounted for separately. Previous stroke was characterized as any occurrence of stroke preceding the current episode and included both hemorrhagic and ischemic types. Hypertension was defined as hypertension registered either before or during the current hospital admission. Anticoagulant therapy was defined as ongoing if a prescription for anticoagulant drugs had been filled within 6 months preceding stroke. Prehospital delay was defined as the total time delay from symptom onset or last known well to admission at the first hospital, thus including both delay in seeking medical attention as well as transportation delay.
Arriving hospital was defined according to the availability of reperfusion therapy at the first hospital to which the patient was admitted, as either comprehensive stroke centers (CSC) equipped to provide both IV thrombolysis and thrombectomy, primary stroke centers (PSC) with IV thrombolysis available and non-reperfusion therapy (non-RT) centers with no reperfusion therapy available.
Missing covariate data were imputed by multiple imputation, with the exception of the variables sex and anticoagulation therapy, which had complete data.
Adjustments were performed at two different levels: Confounder-weighted models controlled for age, sex, immigrant status and education and fully weighted models additionally controlled for potential mediating covariates (stroke severity, living alone, assisted living residency, CCI, previous stroke, hypertension, anticoagulation therapy, and prehospital delay). The rationale behind this approach was to reduce bias from confounding in the confounder adjusted model, while exploring potential mediating pathways in the fully adjusted model.
Although available reperfusion therapies at the arriving hospital was considered a potential mediator, it was not feasible to incorporate this variable in adjustment due to a notably different distribution across the urban-rural strata. Consequently, arriving hospital could not be integrated into the fully adjusted models, but a simple presentation of differences across the urban-rural strata was presented in Table 1.
Patient and hospital characteristics according to rurality.
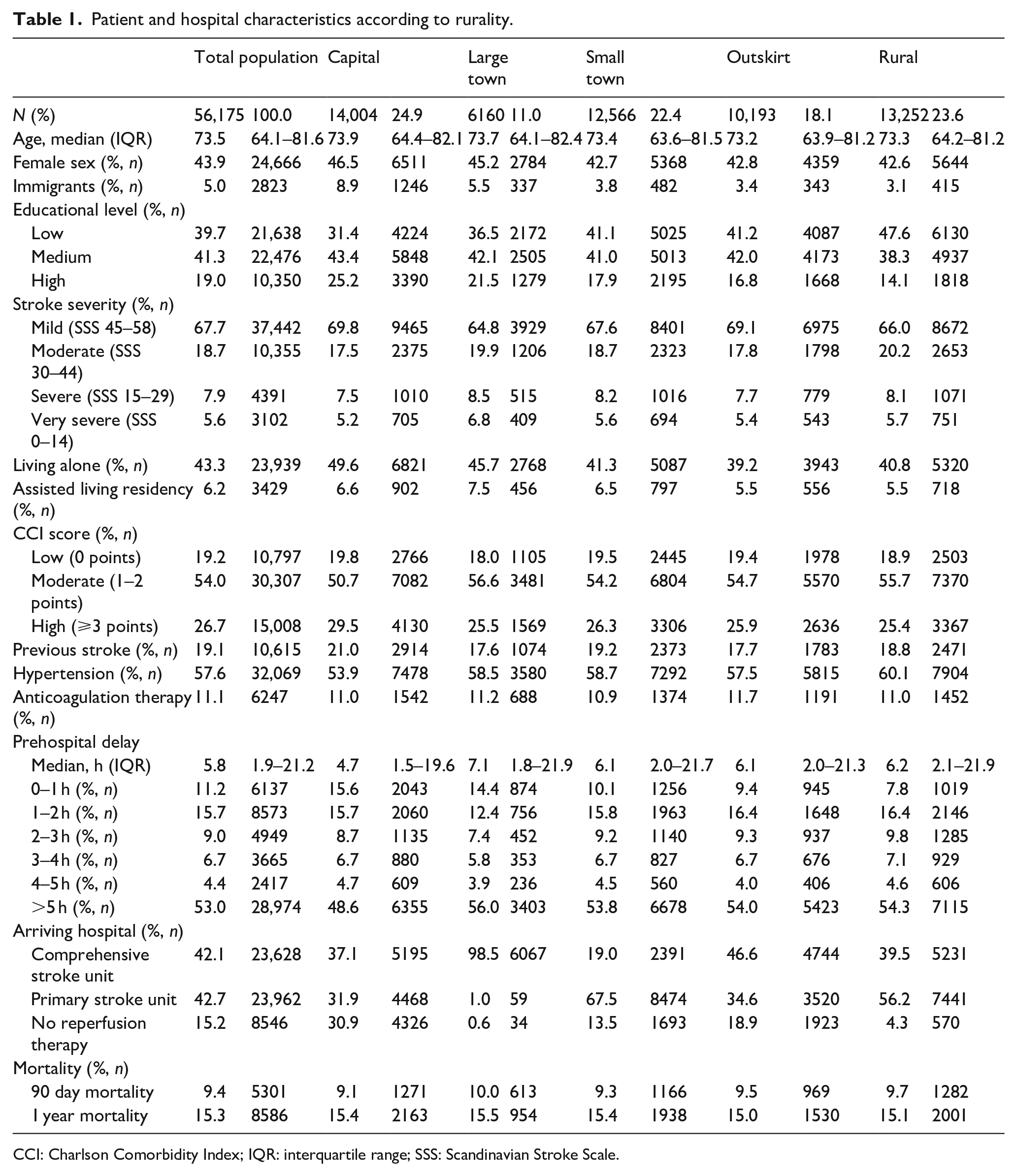
CCI: Charlson Comorbidity Index; IQR: interquartile range; SSS: Scandinavian Stroke Scale.
Adjusted treatment rates were obtained by balancing baseline characteristics from each urban-rural category. Balancing was performed by applying weights to each individual from non-capital municipalities using inverse probability of treatment weights (IPTW) to estimate average treatment effect on the treated with capital municipalities as the stable category. This approach effectively aligned the four non-capital categories to approximate the baseline characteristics seen in the capital category for the included covariates (Supplemental Tables S1 and S2). For categorical variables, balance was assessed by comparing frequencies between capital and non-capital municipalities. For continuous variables, balance was assessed by comparing medians and interquartile ranges (IQR) between capital and non-capital municipalities.
Baseline characteristics for the study population were presented as medians and IQR for continuous variables and counts and frequencies for categorical variables.
Two different sensitivity analyses were carried out. First, patients with high weights after IPTW (weights >10) were trimmed to evaluate the impact of high weights on the final treatment rates. Second, patients from island municipalities lacking mainland bridge connections were excluded, as their potential for disproportionately long travel times, coupled with their categorization as rural municipalities, could theoretically skew treatment rates unfavorably within the rural category.
All analyses were performed for the total study population as well as for patients with early hospital arrival (prehospital delay <4 h). Restricting the population to patients with early hospital arrival was performed before any data imputation. Effect modification was assessed by evaluating stratum specific age and sex analyses. There were no signs of artifacts from multicollinearity.
All analyses were performed in Stata Statistical Software (Release 16.1 College Station, TX: StataCorp LLC). Graphic displays were produced using R Statistical Software (v4.2.1, R Core Team 2022) using the t-map tools package (v3.1.1).
Results
During the study period, 96,995 stroke episodes were identified from the DSR, after applying the specified inclusion and exclusion criteria, we finally included 56,175 patients (Figure 2). For the analyses on early arriving patients, we excluded patients with prehospital delay > 4 h (n = 31,390) as well as patients with unknown prehospital delay (n = 1461). In total, 23,324 patients were finally included in these analyses.
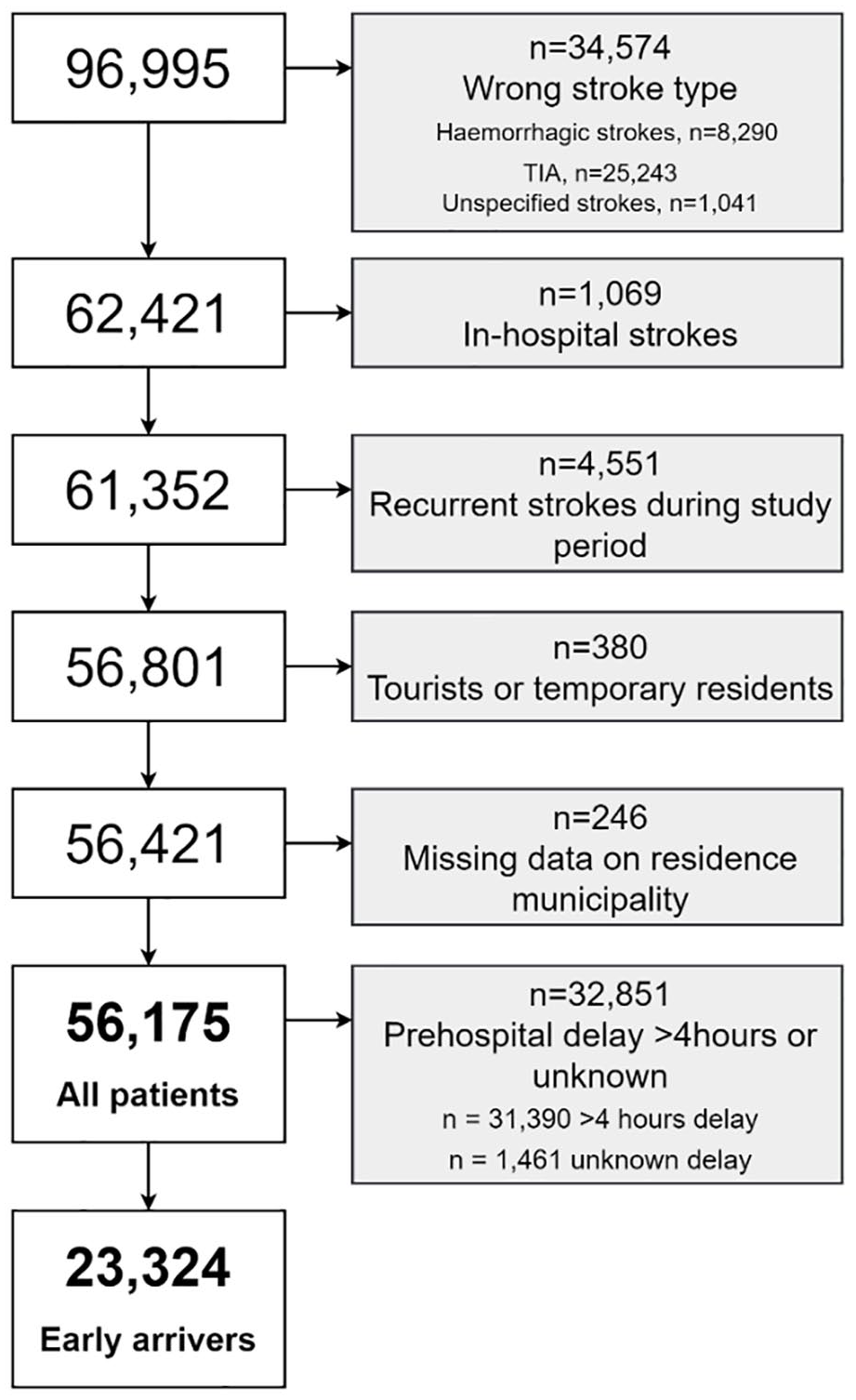
Study flow chart.
Patients tended to be older, and with a higher proportion of females in capital and large town municipalities. Capital municipalities also had notably more immigrants at 8.9% compared to 3.1% in rural municipalities. A gradient was observed in educational attainment, with higher frequency of low educational level in the most rural municipalities and high educational level in the most urban municipalities. Living alone was less frequent in the three most rural municipalities with 39.2%–41.3% living alone compared to 45.7%–49.6% in capital and large town municipalities. Assisted living was less common in the two most rural municipalities (5.5% compared to 6.5%–7.5% in the remaining municipality groups). Capital residents had a higher frequency of a high comorbidity index (29.5% compared to 25.4%–26.3%) and a greater prevalence of previous strokes (21.0% compared to 17.6%–19.2%), but lower rates of hypertension (53.9% compared to 57.5%–60.1%) compared to patients from the remaining municipality groups. However, mortality rates at 90 days and 1 year after stroke only exhibited minimal variation between the different exposure groups (from 9.1% to 10.0% and 15.0% to 15.5% respectively). Median prehospital delay differed markedly across the urban-rural strata, with shortest delays in capital municipalities, 4.7 h (IQR 1.5–19.6 h), and longest delays in large town municipalities, 7.1 h (IQR 1.8–21.9 h). Nearly all residents in large town municipalities (98.5%) were admitted directly to CSCs, whereas 30.9% of capital residents were initially admitted to a non-RT center (Table 1). Admission to a hospital lacking reperfusion therapy was more prevalent among patients with late compared to early hospital arrival (17.6% vs 11.9%, table S1). A comparison of baseline characteristics according to early versus late hospital arrival is presented in the Supplemental Table S1. Baseline characteristics for each weighted population is presented in the Supplemental Tables S2 and S3.
Missing covariate data were most frequent for educational level, with 3.0% missing (n = 1.711), and prehospital delay with 2.6% missing (n = 1.463). The remaining covariates had ⩽2.0% missing.
As capital municipalities was selected as the stable category, treatment rates in this stratum was identical in both the unadjusted, confounder adjusted and fully adjusted model at 18.6% (95% CI 17.9–19.2). Results from the analyses including all patients revealed almost identical treatment rates across all non-rural municipalities, ranging from 18.5% (95% CI 17.8–19.2) to 18.7% (95% CI 17.9–19.4). In contrast, rural municipalities had a lower treatment rate of 17.2% (95% CI 16.5–17.8) (Figure 3(a)). Treatment rates in all non-capital municipalities were higher after confounder adjustment. The highest treatment rate was observed in outskirt municipalities; 20.5% (95% CI 19.6–20.8), and rural municipalities reached treatment rates similar to capital municipalities; 18.5% (95% CI 17.7–19.4) (Figure 3(b)). In the fully adjusted model, lower treatment rates among rural municipalities were observed once again (17.2%, 95% CI 16.3–18.0) (Figure 3(c)).
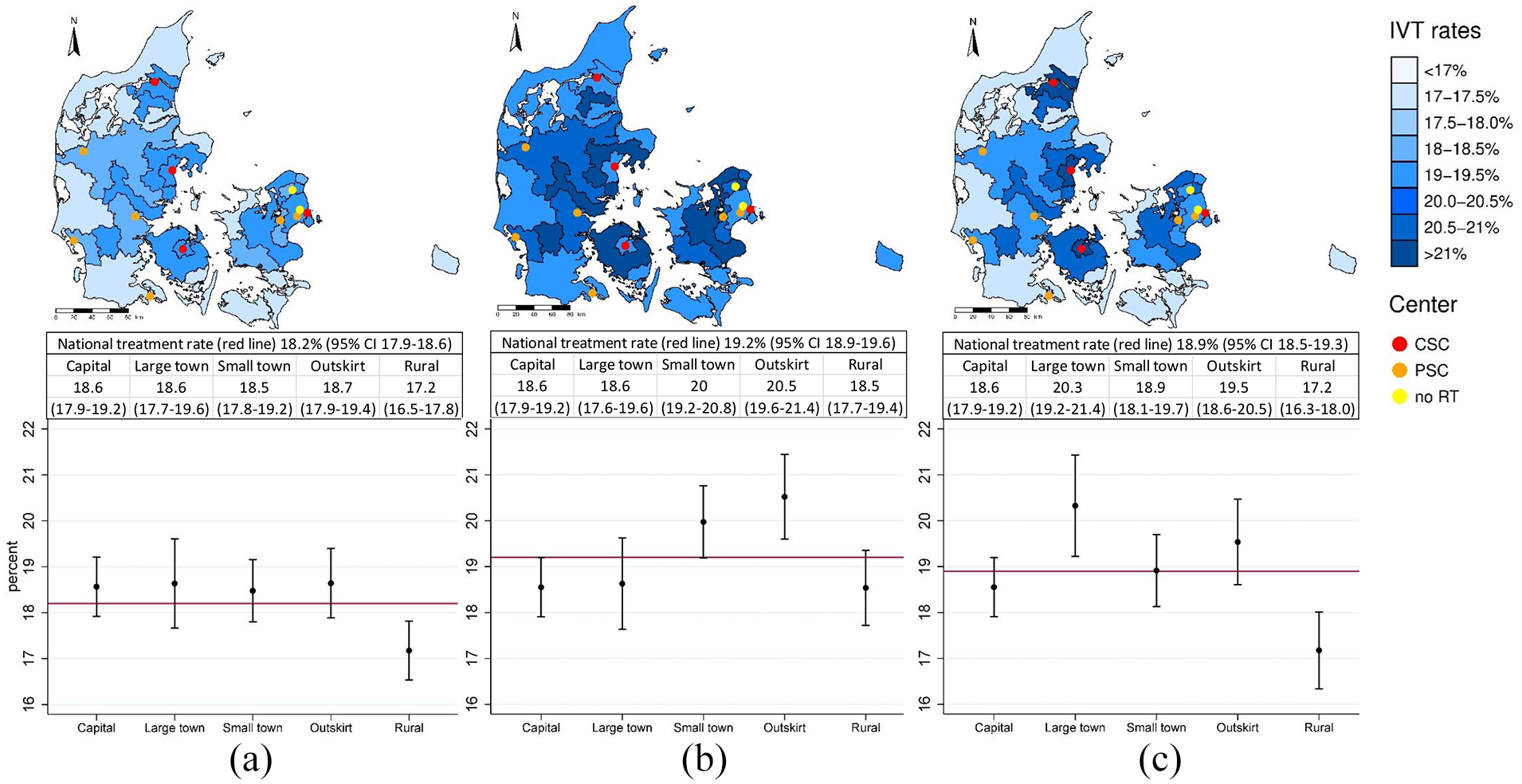
Treatment rates according to urban-rural stratum. (a) Unadjusted treatment rates, (b) confounder adjusted rates, and (c) fully adjusted rates. Confounder adjustments included age, sex, immigrant status, and educational level. Full adjustments additionally included stroke severity, living alone, assisted living residency, CCI, previous stroke, hypertension, ongoing anticoagulation therapy and prehospital delay. Top: Treatment rates by urban-rural stratum displayed in geographic maps with stroke centers plotted as dots. CSC’s: Both thrombectomy and IV thrombolysis, PSC’s: Only IV thrombolysis, no RT: No reperfusion therapy. Middle: Treatment rates with 95% CI’s are at national level and according to urban-rural stratum. Bottom: Plots displaying treatment rates by urban-rural stratum with 95% CI. National treatment rates are indicated with a red line for comparison.
When restricting the study population to include only patients with early hospital arrival (prehospital delay <4 h), we observed the lowest treatment rates in capital municipalities: 38.5% (95% CI 37.3–39.8) followed by rural municipalities: 40.0% (95% CI 38.7–41.3). Meanwhile, the remaining three urban-rural strata displayed higher and similar treatment rates, ranging from 42.3% to 42.8% (Figure 4(a)). This pattern persisted after controlling for confounding variables (Figure 4(b). In the fully adjusted models, only rural municipalities exhibited particularly low treatment rates at 35.7% (95% CI 34.0–37.4), while treatment rates in the remaining urban-rural strata ranged from 38.5% to 41.4% (Figure 4(c)).
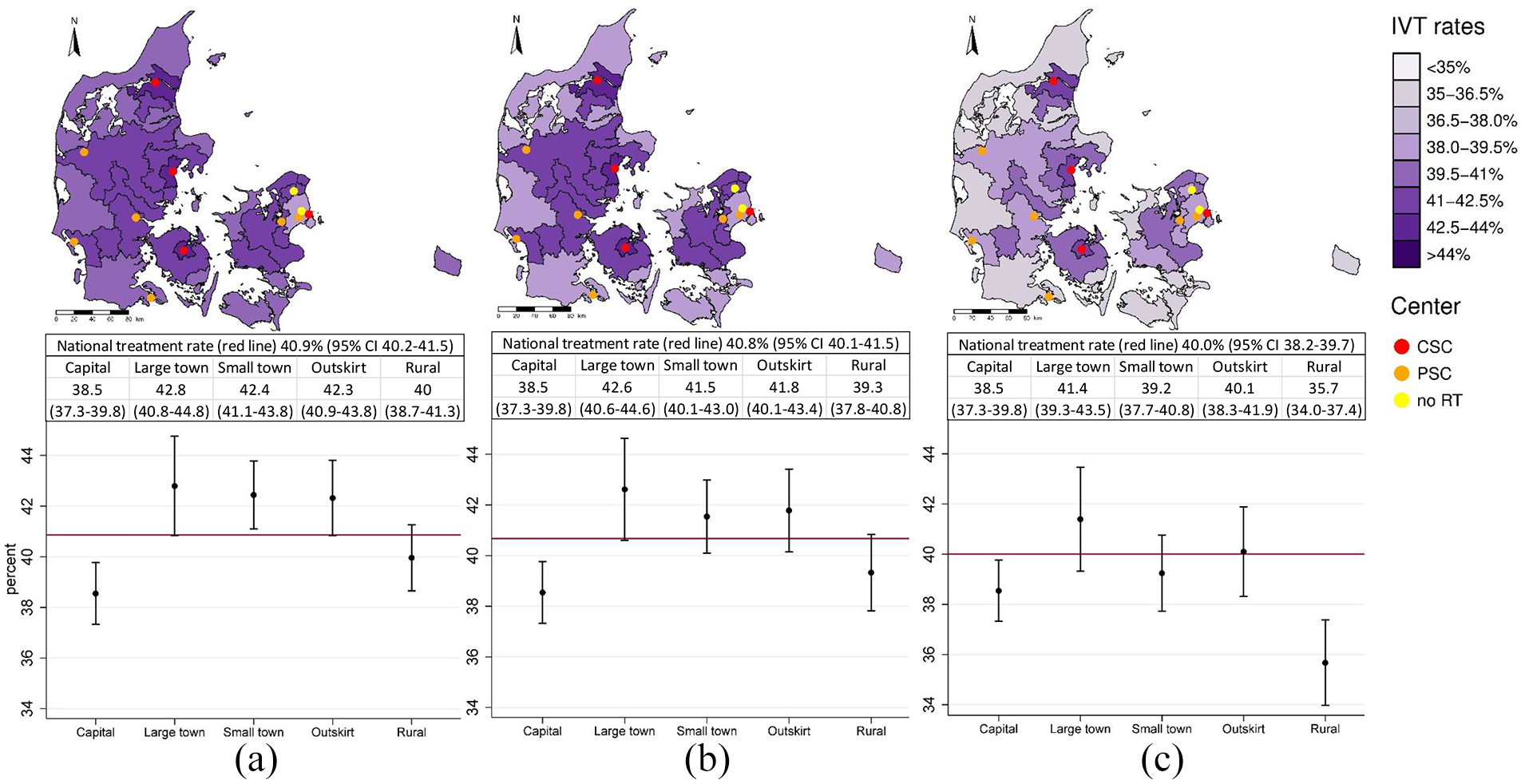
Treatment rates according to urban-rural stratum among patients with early hospital arrival (<4 h). (a) Unadjusted treatment rates, (b) confounder adjusted rates, and (c) fully adjusted rates. Confounder adjustments included age, sex, immigrant status, and educational level. Full adjustments additionally included stroke severity, living alone, assisted living residency, CCI, previous stroke, hypertension, ongoing anticoagulation therapy and prehospital delay. Top: Treatment rates by urban-rural stratum displayed in geographic maps with stroke centers plotted as dots. CSC’s: Both thrombectomy and IV thrombolysis, PSC’s: Only IV thrombolysis, no RT: No reperfusion therapy. Middle: Treatment rates with 95% CI’s are at national level and according to urban-rural stratum. Bottom: Plots displaying treatment rates by urban-rural stratum with 95% CI. National treatment rates are indicated with a red line for comparison.
The two sensitivity analysis excluding patients from island municipalities and patients with high weights (>10) respectively, revealed minimal impact on the final outcomes, with a maximum rate change of 0.1% points. Consequently, the decision was made not to proceed with trimming.
Discussion
In general, only minor differences in treatment rates between the five urban-rural categories were observed with unadjusted treatment rates ranging between 17.2%−18.7% for the entire study population and 38.5%−42.8% among those with early hospital arrival. These inequalities, which are comparatively smaller than those seen in other countries,4,6,22,24 may be attributed to Denmark’s tax-funded healthcare system, compact geography, well-developed infrastructure, as well as a dispersed network of stroke centers, ensuring relatively easy access to stroke units from all geographic locations.
While overall differences in treatment rates across the five urban-rural strata were relatively minor, a clear pattern emerged with rural municipalities consistently exhibiting the lowest or second lowest treatment rates. This pattern persisted after accounting for potential confounding factors. Moreover, after accounting for potential mediators in the fully adjusted model, the differences in treatment rates between rural and non-rural municipalities not only remained but, surprisingly, became even more pronounced. This finding could be attributed to the more favorable living conditions among rural residents, where fewer patients lived in assisted facilities or alone, when compared to capital or large town residents. To investigate this possibility, we conducted a separate analysis excluding assisted living residency and living alone from the fully adjusted models, but rural residents continued to exhibit the lowest treatment rates (data not shown). These results could indicate the presence of either or both of these scenarios: There is a direct impact of rurality on the likelihood of receiving thrombolysis, or unconsidered factors contribute to the remaining urban-rural inequalities in the fully adjusted model.
Capital municipalities did not consistently achieve the highest treatment rates and, among early arriving patients, actually had the lowest treatment rates. This contradicts the idea that proximity to a comprehensive or primary stroke center increases the chance of receiving IV thrombolysis. This paradoxical finding could be attributed to the fact that two non-RT centers (North Zealand Hospital and Herlev and Gentofte Hospitals) are situated in capital municipalities. In this setting, some patients, who are initially considered ineligible for IV thrombolysis, will be admitted to these non-RT centers. However, based on clinical experience, patients initially deemed ineligible for IV thrombolysis may later be found eligible. It is conceivable that patients initially admitted to a non-RT center may miss the opportunity for IV thrombolysis due to time lost during this admission. This possibility is reinforced by the discovery that even among early arriving patients, more than 10% were initially admitted to a non-RT center. This would argue for all stroke patients being admitted at a center capable of reperfusion therapy.
Another unexpected finding was the large variations in median prehospital delay across the different urban-rural categories with capital municipalities having much shorter delays in general. The large contrast in median prehospital delay between capital municipalities and large town municipalities was intriguing, because patients from the latter usually reside close to a stroke unit, rendering differences in transportation times an insufficient explanation for this phenomenon. This underscores the importance of elements beyond transportation time in the cumulative prehospital delay, such as differences in delays to seek medical attention, which could vary due to different cultural norms across the country.
The importance of prehospital delay in mediating treatment likelihood according to rurality was indicated by treatment rates consistently decreasing in capital relative to non-capital municipalities whenever prehospital delay was taken into account (either by including prehospital delay in the fully adjusted model or by restricting the population to patients with early hospital arrival). This observation aligns with the expectations, given the much shorter median prehospital delay in capital compared to non-capital municipalities.
While the majority of studies originate from the United States, and have consistently reported lower reperfusion treatment rates among rural residents compared to their urban counterparts,4,23–26 a Colombian and Austrian study, showed a contrasting trend with lower reperfusion treatment rates in urban areas.12,22 Furthermore, a Canadian study found lowest treatment rates in medium urban areas compared to large urban or rural areas. 27 Other comparable studies have investigated the effect of rural compared to urban hospital location or hospital system type on the chance of receiving reperfusion therapy. An Australian study found thrombolysis rates of 0% in rural hospitals compared to 8% in urban hospitals. 6 Conversely, a Finnish study could not detect any differences in thrombolysis rates between a decentralized and centralized hospital system. 28 All the remaining studies originated from the United States, and these consistently reported higher treatment rates in urban hospitals,29,30 large metropolitan hospitals 31 or hospitals located in the most densely populated areas. 32
Putting our results into this context, it becomes clear that urban-rural inequalities in reperfusion treatment rates differ markedly between countries. While rural residency appeared beneficial in Colombia and Austria, the opposite was true in Australia and all of the US studies, whereas our study and the other Northern European study suggested minimal or no differences in thrombolysis rates according to urban-rural residency or with a centralized versus decentralized hospital system. These cross-country differences could be explained by fundamental differences in the health care systems in each country, or the different geographic layouts and accessibility to a stroke unit for rural resident.
The role of potential confounding and mediating factors has so far received little attention in studies on the role of geographic residency on access to IV thrombolysis. Only a few (all US studies) accounted for simple confounding covariates such as age and sex, or considered the role of prehospital delay as a key mediator for the association between rurality and reperfusion treatment rates. However, even these studies revealed that lower chances of reperfusion treatment remained among hospitals or residents of rural origin after adjustments.4,24,30,31
This study has several strengths, including the large nationwide collection of data with very few missing observations and individual-level data on all patients. This study stands out as the first study on this area applying a detailed covariate adjustment strategy with a distinction between variables with clear confounding from potential mediating effects. While it is possible that other geographic inequalities in thrombolysis rates might exist in Denmark, we found the stratification into five urban-rural categories to be particularly robust, as it was conducted independently of the healthcare system and the demographics of stroke patients. Furthermore, this stratification facilitated meaningful comparisons with other countries that have employed similar categorizations.4,6,22,24
Limitations include the fact that we were unable to account for the availability of reperfusion therapy at the first hospital of arrival. Including arrival at a non-RT center in weight creations was not possible due to a minimal overlap between patients arriving at a non-RT center across the five urban-rural categories. Similar to all register-based studies, potential coding errors represent another limitation. Furthermore, the external validity of this study is most likely confined to countries with similar healthcare systems and geography, although the results can serve as valuable points of comparisons for future studies conducted in any country. Lastly, while the choice to omit potential mediators from the confounder adjusted models preserved the entire causal effect from exposure to outcome while reducing the risk of collider stratification bias, it also increased the risk of residual confounding in these estimates. Due to dissimilar indications and contraindications for treatment with IV thrombolysis and thrombectomy, we decided to focus exclusively on IV thrombolysis rates to simplify the adjustment strategy. However, investigating urban-rural inequalities in thrombectomy rates remains interesting for future research.
Conclusion
In this large nation-wide register-based study of more than 50.000 ischemic stroke patients, we report almost similar thrombolysis rates according to residence municipality, with only slightly lower treatment rates among rural compared to non-rural residents. Capital municipalities had the lowest treatment rates when restricting the study population to patients arriving within the treatment window. This could be attributed to earlier hospital arrival as well as more frequent admission to non-RT units in capital compared to non-capital municipalities. Qualitative studies are needed to highlight the reasons behind both the large variations in prehospital delay according to urban-rural strata, and to assess the potential adverse effects of initial admission to a non-RT unit.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241244591 – Supplemental material for Urban-rural inequalities in IV thrombolysis for acute ischemic stroke: A nationwide study
Supplemental material, sj-docx-1-eso-10.1177_23969873241244591 for Urban-rural inequalities in IV thrombolysis for acute ischemic stroke: A nationwide study by Sine Mette Øgendahl Buus, Anne Brink Behrndtz, Marie Louise Schmitz, Jakob Nebeling Hedegaard, Pia Cordsen, Søren Paaske Johnsen, Thanh Phan, Grethe Andersen and Claus Ziegler Simonsen in European Stroke Journal
Footnotes
Acknowledgements
None
Abbreviations
CCI: Charlson Comorbidty Index
CI: Confidence interval
DSR: Danish Stroke Registry
ICC: Intraclass correlation coefficient
IPTW: Inverse probability of treatment weights
IQR: Interquartile range
IV: Intravenous
Non-RT center: Non reperfusion therapy center
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CS: Supported by research grants from Novo Nordisk Foundation and Health Research Foundation of Central Denmark Region. SB, AB, MS, JN, PC, SJ TP and GA declare no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: TrygFonden [grant number 117615], Helsefonden [grant number 19-B-011], Aase og Ejnar Danielsens Fond [grant number 18-10-0446], and Aarhus University [research training supplement].
Ethical approval
Ethical approval is not required for register-based studies in Denmark. The Danish Data Protection Agency approved the study (journal number 2019-899/10-0033).
Informed consent
Informed consent is not required for register-based studies in Denmark.
Guarantor
CS
Contributorship
SB, AB, MS, SJ, GA, and CS conceived the study idea. SB wrote the study protocol. SB performed data management and statistical analyses supervised by JH. SB created plots, and AB created graphs for the manuscript. SB drafted the manuscript. AB, MS, JN, PC, SJ, TP, and CS provided critical revisions to the study protocol and manuscript. All authors approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.