
Abstract
Introduction
The objective of this study is to compare the clinical profile, risk factors, type and outcome of stroke patients in urban and rural areas of Punjab, India.
Methods
The primary data source was from the Ludhiana urban population-based stroke registry. The data of first-ever stroke patients with age ≥18 years were collected using WHO stepwise approach from all hospitals, general practitioners, physiotherapy and scan centres between 26 March 2011 and 25 March 2013.
Results
A total of 4989 patients were included and out of 4989 patients, 3469 (69%) were from urban areas. Haemorrhagic stroke was seen more in rural as compared to urban regions (urban 1104 (32%) versus rural 552 (36%); p = 0.01). There were significant differences seen in stroke risk factors; hypertension (urban 1923 (84%) versus rural 926 (89%); p = 0.001) and hyperlipidaemia (urban 397 (18%) versus rural 234 (23%); p = 0.001) between two groups. In the multivariable analysis the rural patients were more likely to be younger (age < 40 years) (OR: 1.82; 95% CI: 1.24–2.68; p = 0.002), Sikhs (OR: 2.57; 95% CI: 1.26–5.22; p = 0.009), farmers (OR: 9.41; 95% CI: 5.36–16.50; p < 0.001), housewives (OR: 2.71; 95% CI: 1.45–5.06; p = 0.002), and consumed alcohol (OR: 1.57; 95% CI: 1.19–2.06; p = 0.001) as compared to urban patients. In addition, use of imaging was higher in rural patients (OR: 1.99; 95% CI: 1.06–3.74; p = 0.03) as compared to urban patients.
Discussion and Conclusion
In this large cohort of patients, rural and urban differences were seen in risk factors and type of stroke. Stroke prevention strategies need to take into consideration these factors including regional sociocultural practices.
Introduction
Stroke is one of the leading causes of death and disability worldwide. According to WHO, stroke is the second commonest cause of mortality worldwide. By the year 2050, 80% of strokes will occur in low- and middle-income countries. 1 Differences in stroke rates have been noted from USA, France, Northern Portugal and Spain between urban and rural populations.2–5
Seventy per cent of Indian population lives in villages. The rural and urban differences in the stroke profile, risk factors and outcome have not been well studied in India and the results are conflicting. 6 The incidence rate per 100,000 was similar in Kolkata urban study (123.15) and rural Bengal (124) whereas higher case fatality rate (CFR) was seen in Kolkata (41.08%) as compared to rural Bengal (18%).7,8
The Trivandrum stroke registry from South India showed similar incidence rates in both urban and rural regions but the 28-day CFR was higher in the rural region (urban: 24.5% versus rural: 37.1%). 9 A recent study on stroke mortality conducted in rural area of Gadchiroli in Maharashtra showed that stroke was the leading cause of death. 6 Hence, the objective of this study is to compare the clinical profile, risk factors, type and outcome of stroke patients, in urban and rural areas of Punjab state.
Methods
Background of the Ludhiana population-based stroke registry
The data for this study were taken from Ludhiana population-based stroke registry which was conducted in the Northwestern state of Punjab in the city of Ludhiana. Punjab state has a total area of 50,362 km2 (rural area: 48,265 km2 and urban area 2097 km2). 10 The population density in urban areas is high as compared to rural areas.
Total population of Punjab as per 2011 census is 27,743,338 out of which the total rural population of Punjab is 17,344,192. 11 The city has good health care facilities hence patients come from all regions of Punjab and also from other neighbouring states. Urban and rural areas are defined according to the Government of India. Urban population was defined living within the municipal corporation limits and the rest of the areas were conferred rural. 12
The project was carried out in two phases: phase I (26 March 2010–25 March 2011) was the feasibility study and phase II (26 March 2011–25 March 2013) was the main study. 13 Inclusion criteria were all first-ever stroke patient’s ≥18 years of age. WHO STEPS approach was used for stroke surveillance (Steps 1, 2 and 3) which fulfils the WHO criteria for population-based stroke registry in low- and middle-income countries. 14 All the major hospitals (private and public), scan centres, general practitioners (GPs) and physiotherapy centres in the city participated in this registry and mortality data (hospital and home deaths) were collected from Municipal corporation (MC) centres. 13 Separate questionnaires were used by the research staff for data collection from hospitals/GPs/physiotherapy centres, scan centres and MC.
All major hospitals and scan centres participated in the study; thus, the chances of missing information about a nonfatal stroke were very low. Stroke subtypes were categorised based on the scans reported by radiologists. The diagnosis of stroke was established in the hospitals by the participating practitioner based on the clinical signs, symptoms and imaging reports.
Duplication of the cases
The duplicate cases were identified on the basis of name, age, gender, address and contact numbers. When there was duplication of cases, the questionnaire with complete information was entered in the dataset. 13
In order to capture minor strokes and patients who solicit treatment outside the city, advertisements were placed in the newspaper every six months requesting these patients to contact the research team. 13 During the study, a total of 15 patients were ascertained by this method. The principal investigator (JDP) appraised all the completed forms.
Selection of dataset for this study
The first year of the study (26 March 2010–25 March 2011) was feasibility phase hence we did not include that data. All first-ever stroke patients (excluding transient ischemic attack) recruited from hospitals, GP, physiotherapy and scan centres between 26 March 2011 and 25 March 2013 were included in the analysis. On the basis of their addresses the data were further divided into two groups: rural versus urban stroke patients. 12
The data regarding demographic details, presenting symptoms, risk factors, type of stroke, diagnosis modalities were collected from hospitals, GPs and physiotherapy centers. 13 Information regarding demographic details, type of stroke and diagnosis modalities were collected from scan centres. The modified Rankin Scale was documented at 28 days using a structured interview on telephone for all hospital and scan centres patients. 13 Only demography and cause of death were available from MC (home and hospital deaths). Hence we did not include MC data for this sub-paper. Moreover, the MC records maintain mortality information only of Ludhiana residents.
Statistical analysis
SPSS version 21 (Armonk NY: IBM Corp.) software was used for the analysis. For the comparison of categorical variables, Chi Square test and for continuous variables independent t-test (two sided and p < 0.05: significant) were used. Binary logistic regression analysis was performed to describe the characteristics of rural stroke patients as compared to urban patients. The variables included in the analysis were age, gender and all other significant variables in univariate analysis.
Results
In this registry a total of 7199 patients were recruited from 26 March 2010 to 25 March 2013. After excluding duplicate cases (n = 713), a small proportion of patients with incomplete addresses (n = 49) and transient ischemic attack (TIA) patients (n = 724), there were 5713 patients.We included only patients from hospitals/GPs/physiotherapy and scan centres from the state of Punjab which was 4989 (public hospitals: 207(4%), private hospitals: 3075 (62%), GPs: 35 (0.7%), physiotherapy centres: 13 (0.3%), scan centres: 1659 (33%)).Out of 4989, 3469 (69%) were from urban and 1520 (31%) were from the rural areas (Figure 1).
Recruitment algorithm.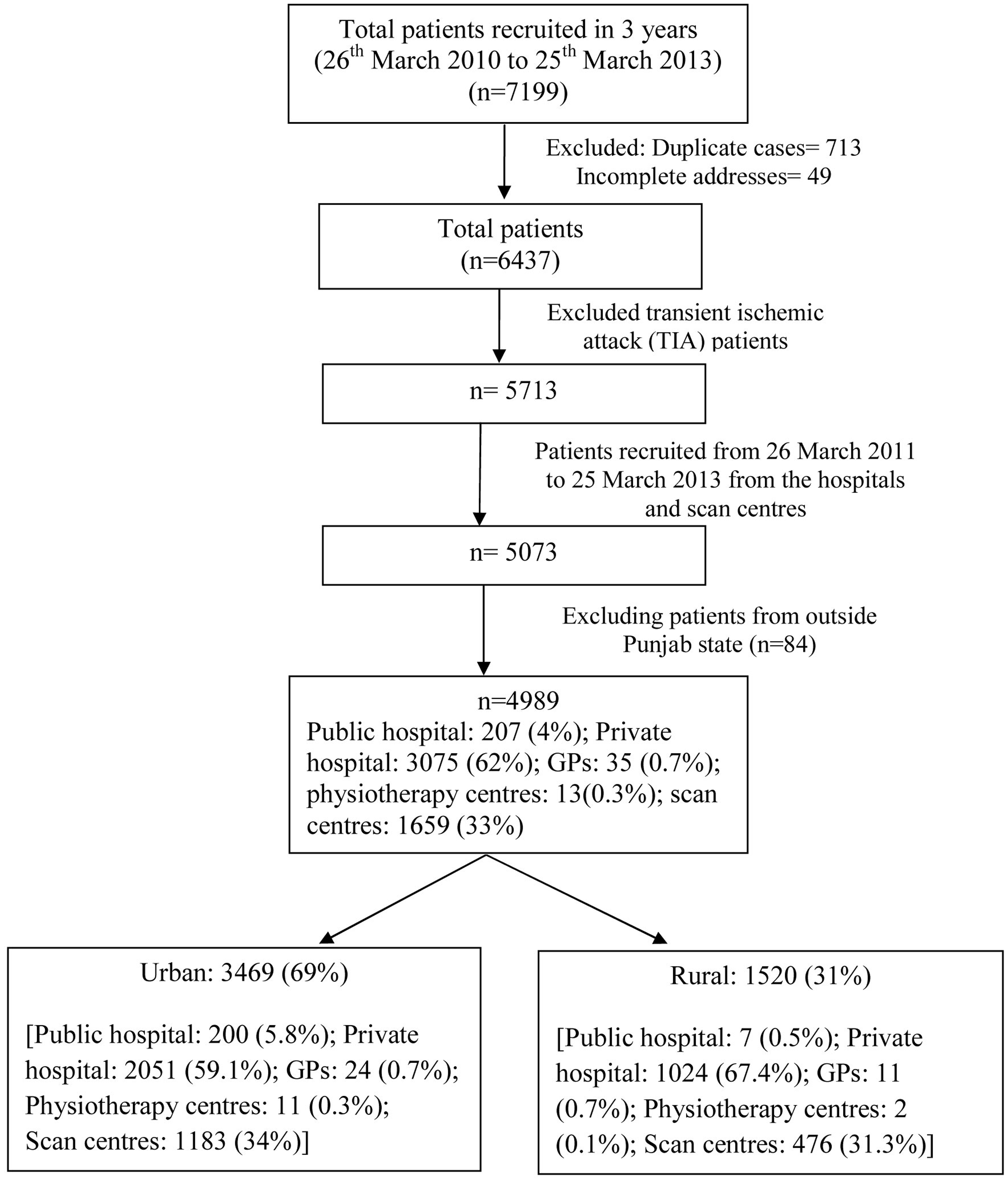
Comparison of demographic details between two groups
Comparison of demographic details between the two groups.
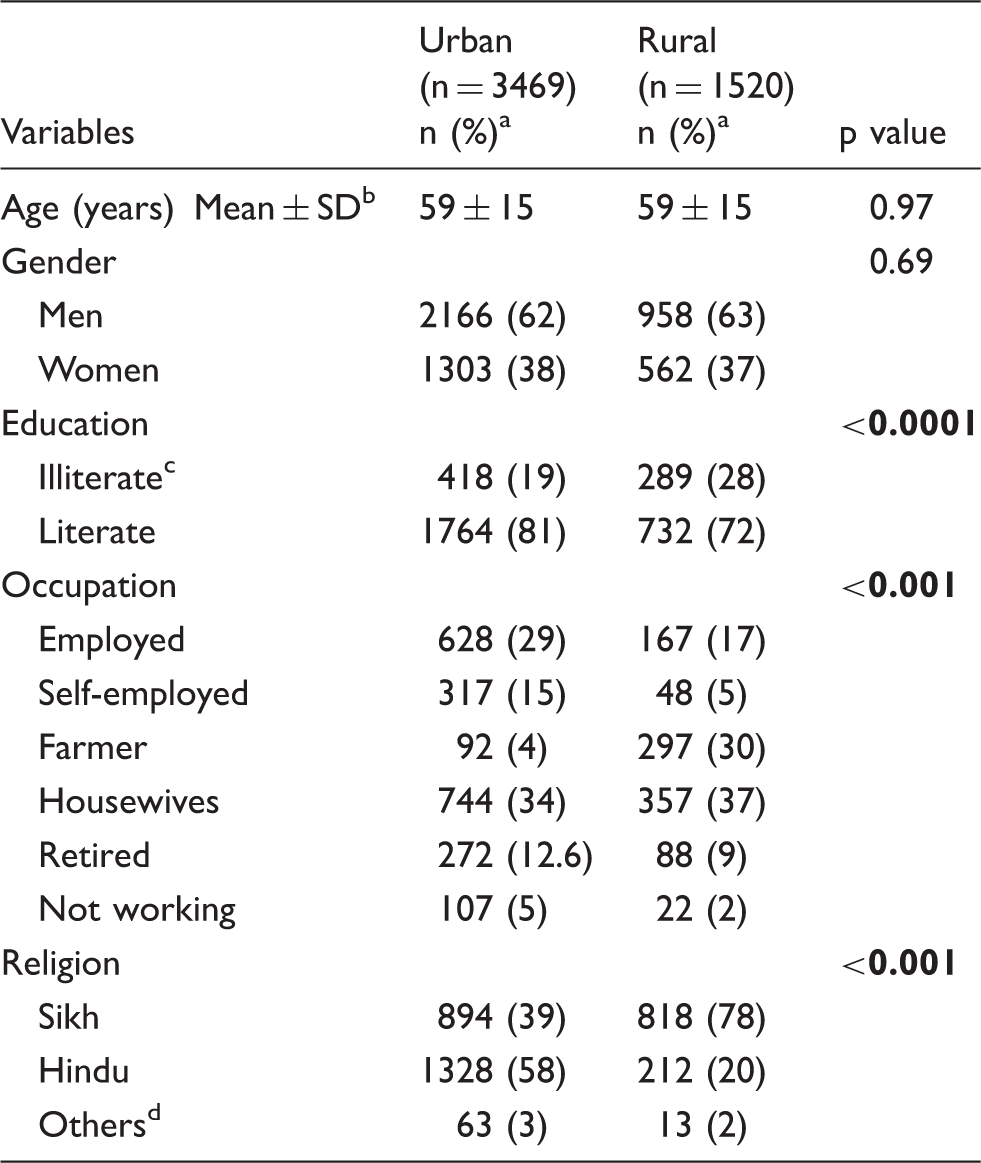
Percentage calculated after excluding missing data.
Standard deviation.
Less than primary school completed.
Muslim, Jain, Christian.
Comparison of type of stroke, imaging modality and outcome
Comparison of type of stroke, diagnosis modalities and outcome between the two groups.
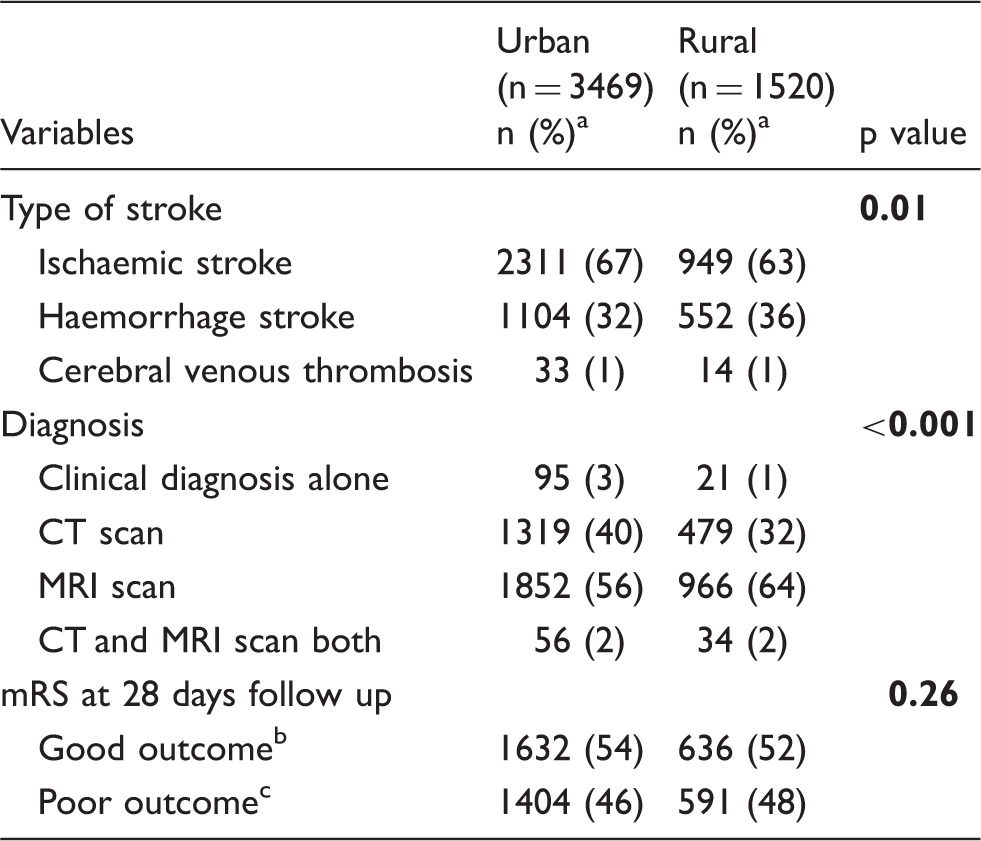
CT: computed tomography; MRI: magnetic resonance imaging; mRS: modified Rankin Scale.
Percentage calculated after excluding missing data.
mRS: 0–2.
mRS: 3–6.
Comparison of risk factors between two groups
Comparison of risk factors between two groups.
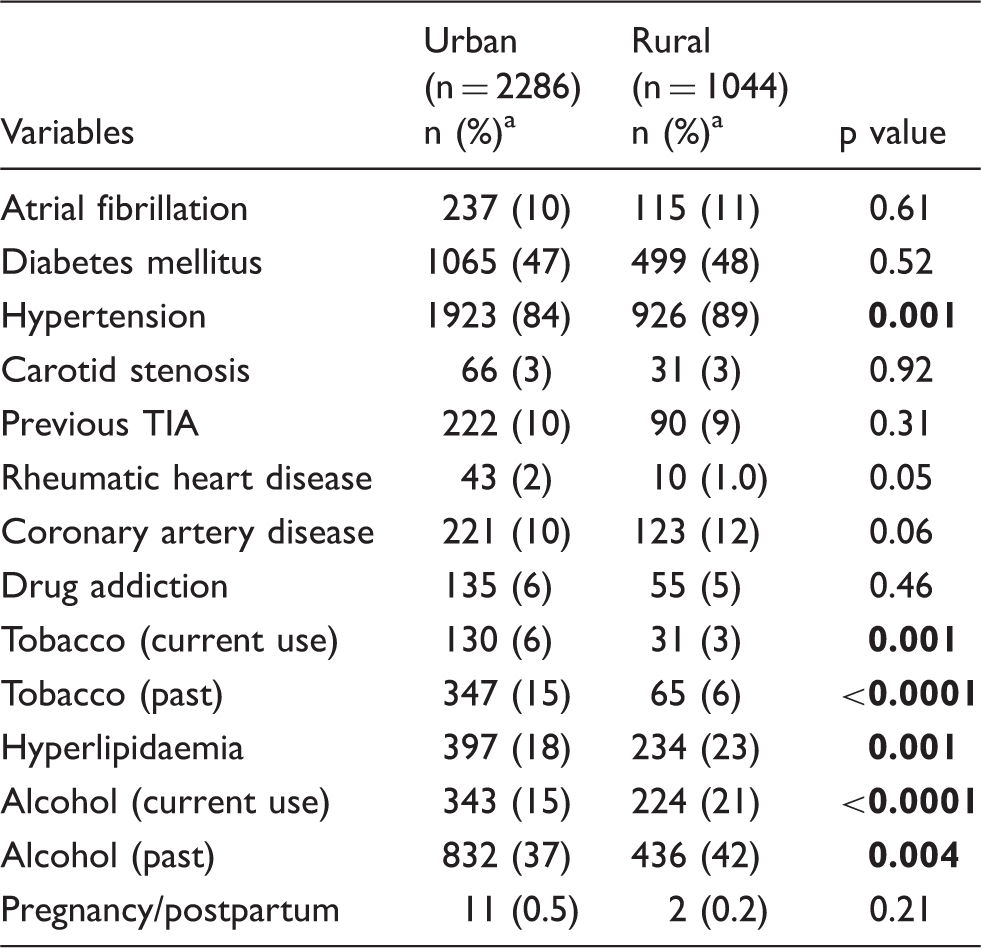
TIA: transient ischemic attack.
Percentage calculated after excluding missing data.
Multivariable analysis
Rural and urban differences: Multivariable analysis.
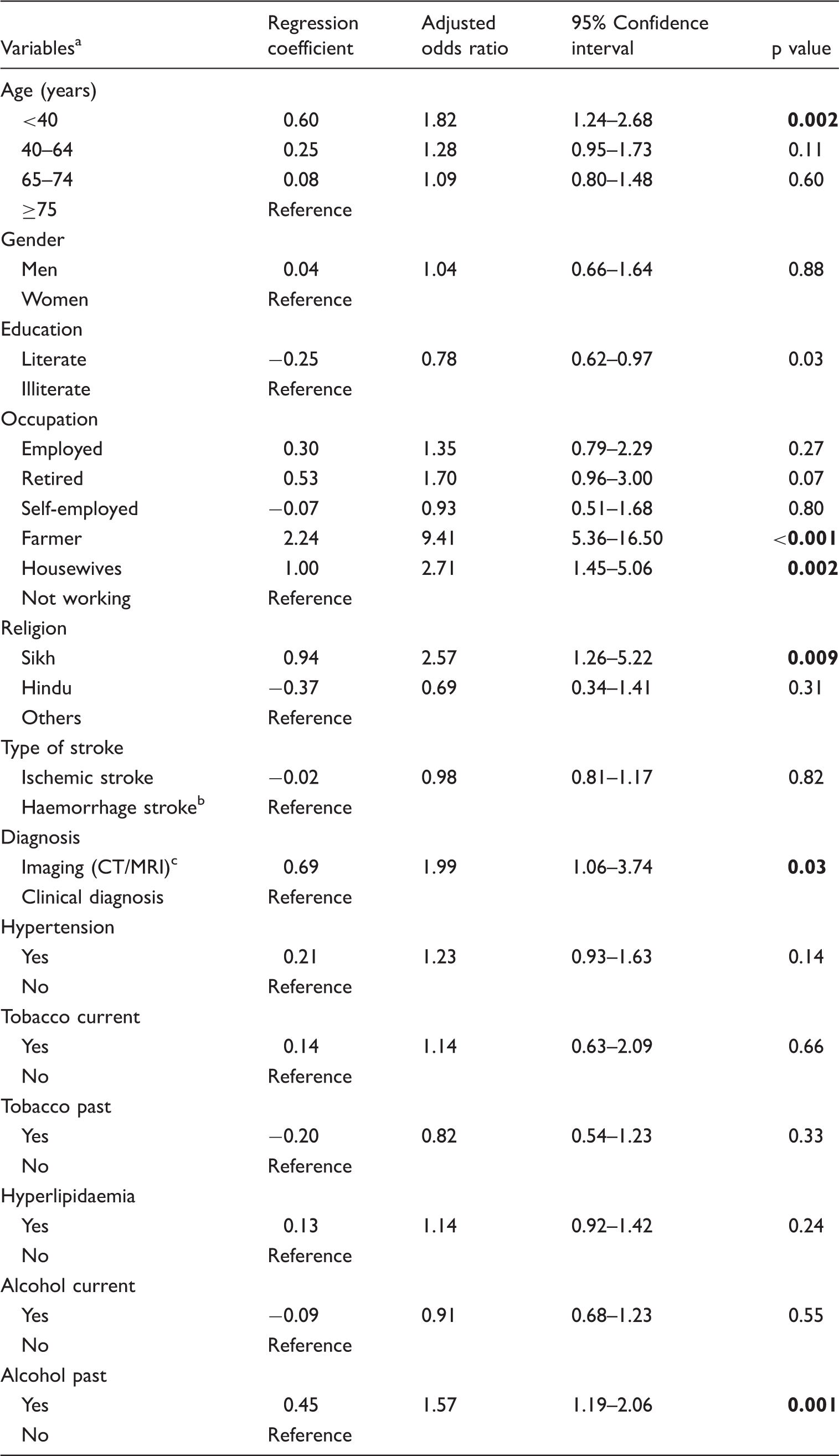
CT: computed tomography; MRI: magnetic resonance imaging.
Dependent variable is coded as rural: 1; urban: 0.
Includes CVT cases.
CT, MRI and CT/MRI both grouped as imaging.
Discussion
In this large population-based stroke registry, rural and urban differences were observed in various stroke characteristics. There was a high proportion of haemorrhagic stroke in rural patients. In multivariable analysis, the rural patients were younger, belonged to Sikh religion, were farmers and house wives. Among the risk factors only alcohol consumption was significant in the rural cohort.
The average age of stroke patients in this cohort is younger which is similar to other studies.7,9 However, the difference in age (younger) among rural patients has not been observed in other population-based studies in India. In the reports from France, Northern Portugal and Morocco, the rural patients were older than urban patients.3,4,15 The change in lifestyle among the rural cohort especially farmers 16 and high prevalence of vascular risk factors could be the possible reasons. Agriculture is the principal industry in Punjab and the diet is rich in fats. 16 Over the years, the manual hard labour of the farmer has been replaced by the cheap labour of the migrant labourers from central India but the diet of the Punjab farmer has still remained the same. 17
There was a high proportion of haemorrhagic stroke seen in rural patients. Similar studies from France, China and Trivandrum showed higher rates of haemorrhagic strokes in rural regions.3,9,18 However, in Portugal, haemorrhagic stroke was higher in urban population. 4 Hypertension was the main risk factor in both urban and rural patients. The difference observed in univariate analysis was no longer present in multivariable analysis. Other factors such as poor control of blood pressure and monitoring could be related to high proportion of haemorrhagic stroke. In low-income countries the awareness and treatment of hypertension in rural areas is low as compared to urban population. 19 Raising community awareness about hypertension can reduce its prevalence and improve its treatment. Hyperlipidaemia was higher in rural patients; however, it was not significant in multivariable analysis.
In our study, the rate of CVT was very low. In India there has been a regional difference in CVT prevalence, it is more common in South India. Most of the studies published from India are hospital-based reports.20–22 Hence the current burden of CVT from India may not be accurate since the majority is hospital-based information. Punjab has better antenatal care and free hospital deliveries offered by the government with free ambulance services. This could be the reason for a lower incidence of CVT in this cohort.
The use of tobacco was higher in urban areas whereas alcohol consumption is higher in rural areas. Sikhism is the main religion of Punjab (58% of total population of Punjab) and more number of Sikhs resides in the rural area (77% of total Sikh population) whereas in the urban areas people from all religions reside. 23 The consumption of alcohol and tobacco is forbidden in Sikh religion. However, Sikhs (who are not baptised Sikh) consume some alcohol in social functions but tobacco intake is strictly prohibited in this religion. 24 From recent years, the rate of migration to Punjab state from other states like Uttar Pradesh and Bihar is very high and these migrants live in cities.17,25 The people from these states have higher rate of tobacco consumption than other states. 26 Moreover, the tobacco and alcohol consumption would have been under-reported due to religious reasons.
In both the groups, there were high proportion of patients who underwent imaging especially so in rural areas. The patients from villages are usually referred by their primary health centres to the city to get the diagnosis confirmed. In the population-based studies done in France and Portugal, imaging rates were similar in urban and rural patients.3,4
The strength of the study is that it is a population-based data with large number of patients from both urban and rural areas. Ludhiana city is the hub of health care facilities in Punjab state. All major hospitals and scan centres participated in the study so chances of missing non-fatal stroke are very low.
The rural stroke patients may not be representative of Punjab population since only patients who came to Ludhiana were included. The other cities of Punjab cater to their own urban patient population as well and also the adjoining rural populations. We accept dissimilarities in the quality of data as a limitation of the study; however, similar rural and urban differences are being observed in our ongoing Ludhiana rural population-based stroke registry. Lack of information on lifestyle risk factors like physical activity, obesity, diet habits of rural and urban populations is another important limitation of the study.
Conclusion
In this large cohort of patients rural and urban differences were seen in terms of risk factors and type of stroke. In addition, religion and cultural influences were also noted in the prevalence of risk factors in this patient population. India is a vast country with diverse sociocultural practices across regions. Stroke prevention strategies need to take into consideration the rural and urban differences and the regional sociocultural practices.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Indian Council of Medical Research, Task Force Project, New Delhi (SWG/22/Neuro/2008-NCD-I).
Ethical approval
The ethics committee of Christian Medical College and Hospital, Ludhiana, and Dayanand Medical College and Hospital, Ludhiana, approved this study and all other centres granted permission.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.
Guarantor
JDP.
Contributorship
PK: Data analysis, data interpretation and writing; SJV: Data collection, data interpretation and writing; GS: Study design, data acquisition and writing; RB, BSP, and MS: Study design and data acquisition; SS and CJS, Literature search, study design, data interpretation and writing; JDP: Literature search, study design, data collection, data interpretation and writing.
Collaborators
Om P Arora, Arun K Dhanuka, Manoj K Sobti, Harish Sehgal, Mohanjeet Kaur, Sarvpreet S Grewal, Sukhdeep S Jhawar, TN Shadangi, Tushar Arora, Ashish Saxena, Gaurav Sachdeva, Jeetamol S Gill, Ramandeep S Brar, Anakhvir Gill, Sandeep S Bakshi, Sandeep S Pawar, Gurmeet Singh, Praveen Sikka.
Acknowledgements
The authors thank Madhu Bala for managing the database; Premjeeth Moodbidri, Gagandeep Mehmi, Amber Sharma, Rohit and Manpreet Kaur for helping with data collection; the following general practitioners for sharing data: Nitin Sood, Bhushan Bansal, BL Malhotra, RS Bhatia, Punit Midha, Rahul Jain, and Subhash Sachdeva; and members of The Indian Council of Medical Research (ICMR) Task Force Group: M Gourie Devi: Department of Neurology, Institute of Human Behaviour and Allied Sciences (IHBAS), Sri Ganga Ram Hospital, New Delhi; Meenakshi Sharma A: Non-Communicable Diseases Division, Indian Council of Medical Research, New Delhi; Nanda Kumar: National Center for Disease Informatics and Research, Bangalore; Kameshwar Prasad: Department of Neurology, Neurosciences Center, All India Institute of Medical Sciences, New Delhi; P Satish Chandra: National Institute of Mental Health and Neurosciences, Bangalore; K Radhakrishnan: Kasturba Hospital, Manipal, Karnataka; KR Thankappan: Achutha Menon Center for Health Sciences Studies, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Thiruvananthapuram, Kerala.