
Abstract
Introduction:
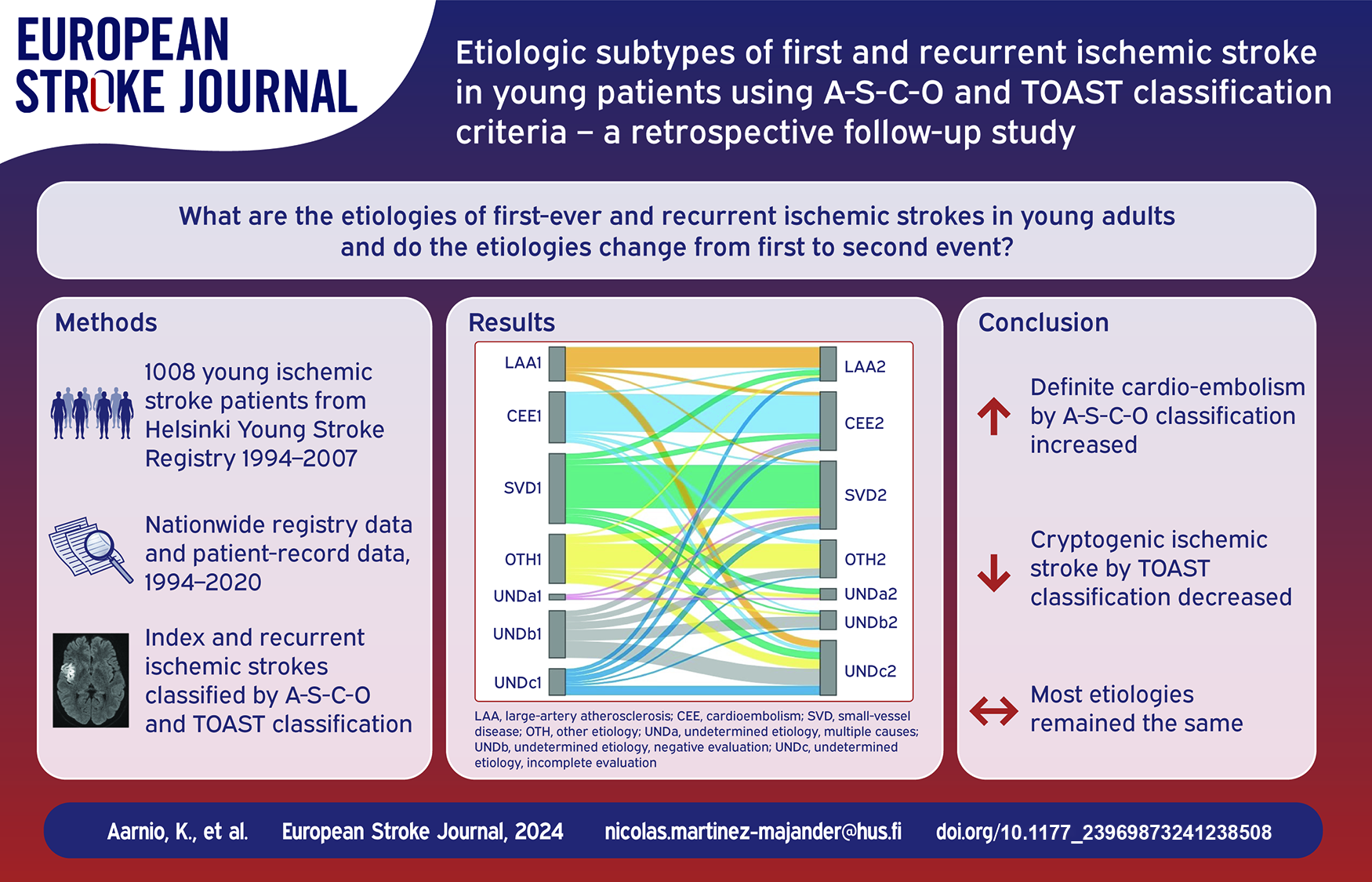
Scarce data exist on the etiology of recurrent ischemic strokes (ISs) among young adults. We analyzed the etiology of first-ever and recurrent events and the differences between them.
Patients and methods:
Patients aged 15–49 years with a first-ever IS in 1994–2007 were included in the Helsinki Young Stroke Registry. In this retrospective cohort study, data on recurrent ISs were identified from Care Register for Health Care until the end of 2017 and Causes of Death Register and from patient records until the end of 2020. All first-ever and recurrent ISs were classified using Atherosclerosis-Small vessel disease-Cardioembolism-Other Cause (A-S-C-O) and Trial of Org 10172 in Acute Stroke Treatment (TOAST) classifications.
Results:
A total of 970 patients were included (median age at index IS 46 years, interquartile range 43–48, 33% women), of which 155 (16.0%) patients had recurrent IS, with 8 (5.2%) fatal cases and 5 (3.2%) unverifiable cases. The median follow-up was 17.4 (IQR 13.9–21.7) years. Median time from the index event to the first recurrent event was 4.5 (interquartile range [IQR] 1.6–10.2) years. Recurrence was more often due to definite cardioembolism (10.7% vs 18.0%, p = 0.013), while the proportion of other definite A-S-C-O subgroups remained the same. With TOAST classification, the proportion of true cryptogenic ISs decreased (16.7% vs 6.7%, p = 0.003), while those with incomplete evaluation increased (9.3% vs 19.3%, p = 0.015). Other TOAST phenotypes remained the same.
Conclusion:
The proportion of definite cardioembolism increased at recurrence using the A-S-C-O classification and the number of cryptogenic ISs decreased using the TOAST classification, while cases with incomplete evaluation increased. Most etiologies remained the same.
Introduction
Ischemic stroke (IS) is one of the leading causes of death and disability worldwide. 1 Around 10% of all ISs affect young adults, who typically have several years of active life ahead of them and family and work to attend. 2 Therefore, their recurrent vascular events and long-term outcome after IS are important, but still understudied.
The etiology of young-onset IS differs from that of the elderly. 3 Young-onset ISs are more frequently caused by less well-established mechanisms, such as cervical artery dissection, or more strongly associated with findings, such as patent foramen ovale (PFO), compared to older adults with more ISs associated with large-artery atherosclerosis (LAA) and small vessel disease (SVD). 4 However, the most widely used etiological classification Trial of Org 10172 in Acute Stroke Treatment (TOAST) does not take into account several less well-established etiologies nor does it consider the probability of the etiology. 5 TOAST classification also lacks detailed criteria for the etiologic work-up. A prospective multicenter study on young-onset IS using a newer A-S-C-O classification (A for atherosclerosis, S for SVD, C for cardiac source, O for other cause) 6 showed that many young patients presenting with acute IS had concomitant stroke etiologies associated with substantial atherosclerotic risk profile. 7
Although there are some studies reporting the etiologies of recurrent ISs in older patients, little is known about the etiologies of stroke recurrence among younger adults. 8 One recent study exploring recurrent IS after young-onset embolic stroke of undetermined source (ESUS) found that a substantial number, as much as 68%, of recurrent ISs could also be classified as ESUS. 9 Also, up to 30% of the etiologies of recurrent IS remained undetermined despite comprehensive and timely diagnostic work-up. However, another study reported that even in young-onset cryptogenic ISs, some risk factors and triggers were still present, including vigorous physical exercise and fever. 10
The aim of this study was to analyze the etiology of the index and recurrent IS in young adults from the Helsinki Young Stroke Registry (HYSR) using both the A-S-C-O and TOAST criteria, and to explore whether the etiology differs between the index and recurrent event.
Patients and methods
Study population
The HYSR covers all consecutive patients aged 15–49 years with first-ever IS from January 1994 to May 2007 selected from a prospective electronic hospital discharge database at the Department of Neurology, Helsinki University Hospital (HUH), which has the only 24/7 neurological emergency unit for a population of 1.5 million. 4 We used the World Health Organization definition of stroke with the exception that patients with imaging-positive findings in the territory corresponding to clinical presentation were classified as an IS even if the symptoms lasted less than 24 h.
Diagnostic tests have already been previously described. 4 All patients underwent brain computed tomography (CT) or magnetic resonance imaging (MRI). The size of the infarct was determined as the size of the largest ischemic lesion based on documented criteria as previously described. 11 The use of secondary preventive medication at 3 months after the index event is based on information received from the patient over the phone and patient medical records. Modified Rankin Scale (mRS) score was used to depict the functional outcome of patients at 3 months after the index and recurrent event. 12 We retrospectively classified the causes of stroke using the A-S-C-O and TOAST classifications based on medical records and available imaging and laboratory data.5,6
We excluded patients who could not be linked to any of the databases needed to obtain outcome data, patients with a false primary diagnosis, patients with no medical records available of the index/recurrent IS, and those who died within 30 days of the index IS.
Follow-up data
We obtained data on hospitalizations until the end of 2017 from the Care Register for Health Care of the National Institute for Health and Welfare, Finland, and data on dates and primary and contributory causes of death as International Classification of Diseases (ICD)-codes from the Statistics Finland until the end of 2020. The Care Register for Health Care includes all patients hospitalized in Finland since 1994, and reporting is mandatory for all public healthcare delivery facilities. 13 The Causes of Death Registry maintained by Statistics Finland covers all deaths and causes of death of Finnish citizens reported by treating physicians using ICD codes since 1936. 14 We included all IS-related hospitalizations with discharge diagnosis codes for primary or secondary cause of hospitalization using the ICD 9th Revision 1994–1995 (434, 436, 437) and the 10th Revision from 1996 onwards (I63, I64, I67). In addition, we verified and performed a search of patient records for recurrent events not found from the registry and until the end of 2020 for all included patients. The follow-up period started from the index IS and ended on December 31, 2020, or the date of moving outside the HUH catchment area, or the date of death, whichever occurred first.
Recurrent stroke
E.H., K.A., and N.M.M. verified all first non-fatal and fatal recurrent ISs from medical records where possible. In discrepant cases a consensus was reached by J.P., K.A., and N.M.M. We defined recurrent ISs as a rapid onset of a new persistent neurological deficit caused by cerebrovascular obstruction without an apparent non-vascular cause verified by CT or MRI. 15 We excluded events that were considered to be transient ischemic attacks (TIA) if symptoms lasted less than 24 h and no imaging findings of acute infarction were found. However, imaging-positive events were considered as recurrent ISs despite the short duration of symptoms. The patient characteristics were as defined at the index event. The use of secondary preventive medications at the time of recurrent IS is based solely on patient records.
A-S-C-O and TOAST modified classifications
All index and recurrent events were classified by A-S-C-O and TOAST classifications (E.H., K.A., N.M.M). The A-S-C-O classifications of those with recurrent events and those with discrepancies between A-S-C-O and TOAST classifications based on clinical, radiographical and laboratory data were cross-checked by another investigator (K.A. or N.M.M.). At admission of the index event, all patients underwent routinely a range of blood tests, chest x-ray, electrocardiogram (ECG), and brain imaging, as well as other previously described tests. 4 The A-S-C-O classifications were based on the predefined minimum number of investigations. 6 For the TOAST classifications of recurrent ISs, the minimum requirements included brain CT or MRI, cervical vessel imaging by ultrasound, CT or MR angiography, basic laboratory tests, ECG, and echocardiogram, to be classified as TOAST 5b, negative evaluation, if these investigations yielded negative results.
The A-S-C-O classification provides three grades of evidence/likelihood: 1) definitely a potential cause of IS (1), 2) causality uncertain (2), 3) unlikely a direct cause of IS but disease is present (3); and 4) insufficient work-up (9). Post-radiation angiopathy was considered as A-S-C-O O=1. To better adapt to young stroke, we also applied a modified TOAST criteria by dividing TOAST 2 into high-risk causes of cardioembolism (CE high-risk) and low-risk causes of cardioembolism (CE low-risk), the latter comprising PFO and/or atrial septal aneurysm (ASA), wall hypokinesia/akinesia/history of myocardial infarction (MI) and other/undetermined valve disease. 16 Also, both carotid and vertebral dissections were reported separately from the other etiology group, TOAST 4, as subgroups. TOAST 1 (LAA), TOAST 2 (SVD), and TOAST 5 (5a two or more causes identified, 5b negative evaluation, and 5c incomplete evaluation) were left unchanged. The Risk of Paradoxical Embolism (RoPE) scores were calculated for all PFO-related strokes. 17
Standard protocol approvals, registrations, and patient consents
We coded all data anonymously into the study database. A regional Ethics Committee approved the study protocol. According to Finnish legislation, a written informed consent is waived in registry-based studies.
Statistical analyses
We analyzed data using IBM SPSS Statistics, Version 25 for Windows (IBM, Armonk, NY) and with R Studio. The characteristics of included patients were presented with descriptive statistics (numbers and percentages; medians and interquartile ranges [IQRs]). For comparison of independent samples, we used Pearson’s chi-squared test and Mann-Whitney U test. We used McNemar’s test to compare the difference between binary index and recurrent stroke characteristics, as well as A-S-C-O and TOAST categories within classes, Wilcoxon signed rank test for non-normally distributed continuous variables, and Marginal homogeneity (SPSS 2-related samples) test for the total categorical comparison for TOAST and A-S-C-O classes. We used the Sankey diagram to depict the change of etiologies from the index to the recurrent event. p < 0.05 were considered significant.
Results
Characteristics at baseline and at recurrence
Figure 1 describes patients included in the final analyses. Of the 1008 patients in the HYSR, a total of 970 patients were included (median age at first-ever IS onset 46 years, interquartile range 43–48, 33% women). Of these, 155 (16.0%) patients had recurrent IS, of which data from 5 (3.2%) patients could not be verified, which resulted in 150 patients with complete etiological classifications. A search for recurrent events from medical records yielded in five new first recurrent ISs not recorded in the Hospital Discharge or Death Registries and seven new cases between 2018 and 2020, when registry data for hospitalizations were lacking. The median follow-up was 17.4 (IQR 13.9–21.7) years. The median time from the index event to the first recurrent IS was 4.5 (1.6–10.2) years. Comparison of baseline characteristics at the index IS showed that patients without recurrent IS were younger, less likely to be current smokers, and less likely to have hypertension, any type of diabetes, or peripheral artery disease. At 3 months, they were more often on anticoagulants but less likely to use antiplatelets or antihypertensives (Table S1).
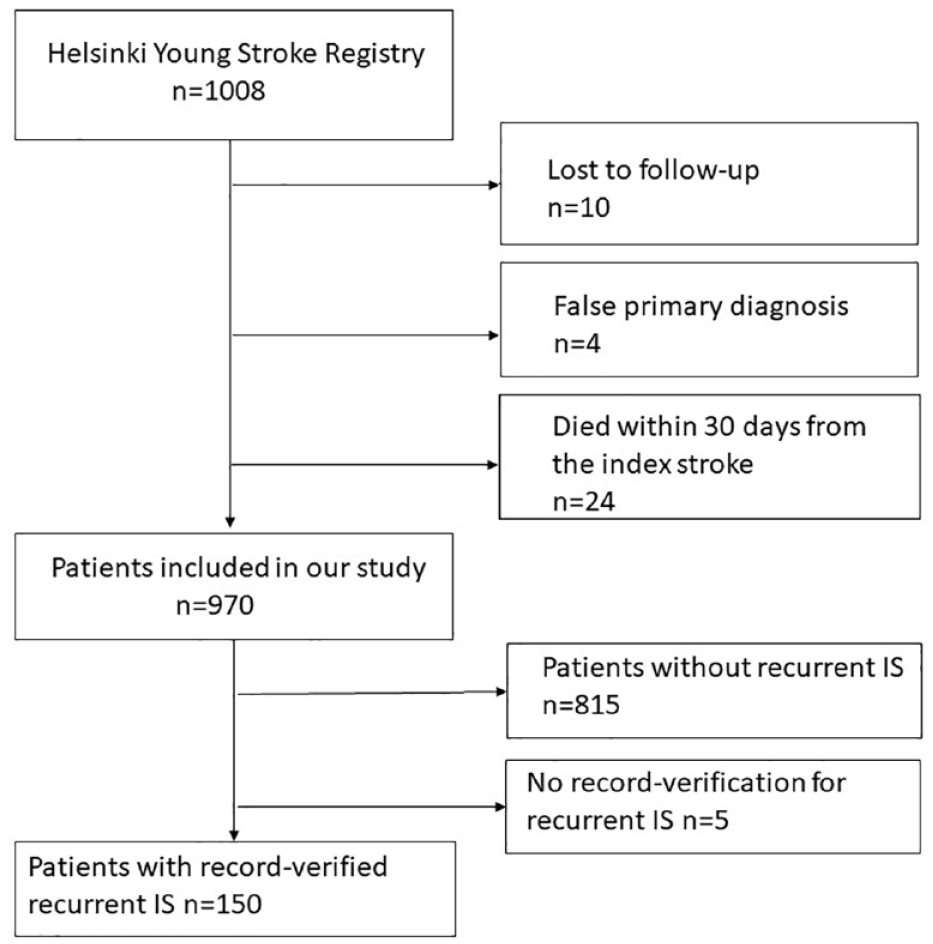
Flow chart of the study population.
Of these 150 verified and imaging-positive patients, 8 (5.2%) had fatal recurrent events, and 107 (71.3%) had imaging-positive lesions. A head CT was performed for 144 (96.0%) patients and/or a brain MRI for 63 (42.0%) patients with recurrent ISs. Initially, 9 (6.0%) recurrent ISs using the TOAST classification and 12 (8.0%) recurrent ISs using the ASCO classification were differently classified by two investigators. In these cases, the investigators reached a consensus.
In the 150 patients with recurrent IS, the overall number of risk factors per patient shown in Table 1 increased significantly between the index and recurrent IS (2 [1–3], vs 3 [2–3], p < 0.001). At recurrence, patients had more frequently hypertension (72.7% vs 50.7%, p < 0.001), type 2 diabetes mellitus (21.3% vs 12.0%, p = 0.001), atrial fibrillation (10.0% vs 4.7%, p = 0.008), coronary heart disease (13.3% vs 6.0%, p = 0.003), prior MI (8.0% vs 3.3%, p = 0.039), and peripheral artery disease (10.0% vs 4.0%, p = 0.022) compared to index IS. In contrast, current cigarette smoking decreased (54.0% vs 39.3%, p < 0.001). Furthermore, recovery from the recurrent IS was poorer compared to index IS (median mRS 2 [IQR 1–3] vs 2 [IQR 1–2], p < 0.001). There were no differences in other risk factors, infarct location or size, or in admission National Institutes of Health Stroke Scale (NIHSS) score. A significant proportion of patients had discontinued antiplatelet (77.0% vs 65.3%, p = 0.012) and anticoagulant (23.0% vs 15.3%, p = 0.035) therapy between the 3 months after the index IS and recurrent IS, while the use of statins and antihypertensives was more frequent at the time of recurrent IS.
Risk factors and stroke features in patients with recurrent IS (n = 150) at index and recurrent event.
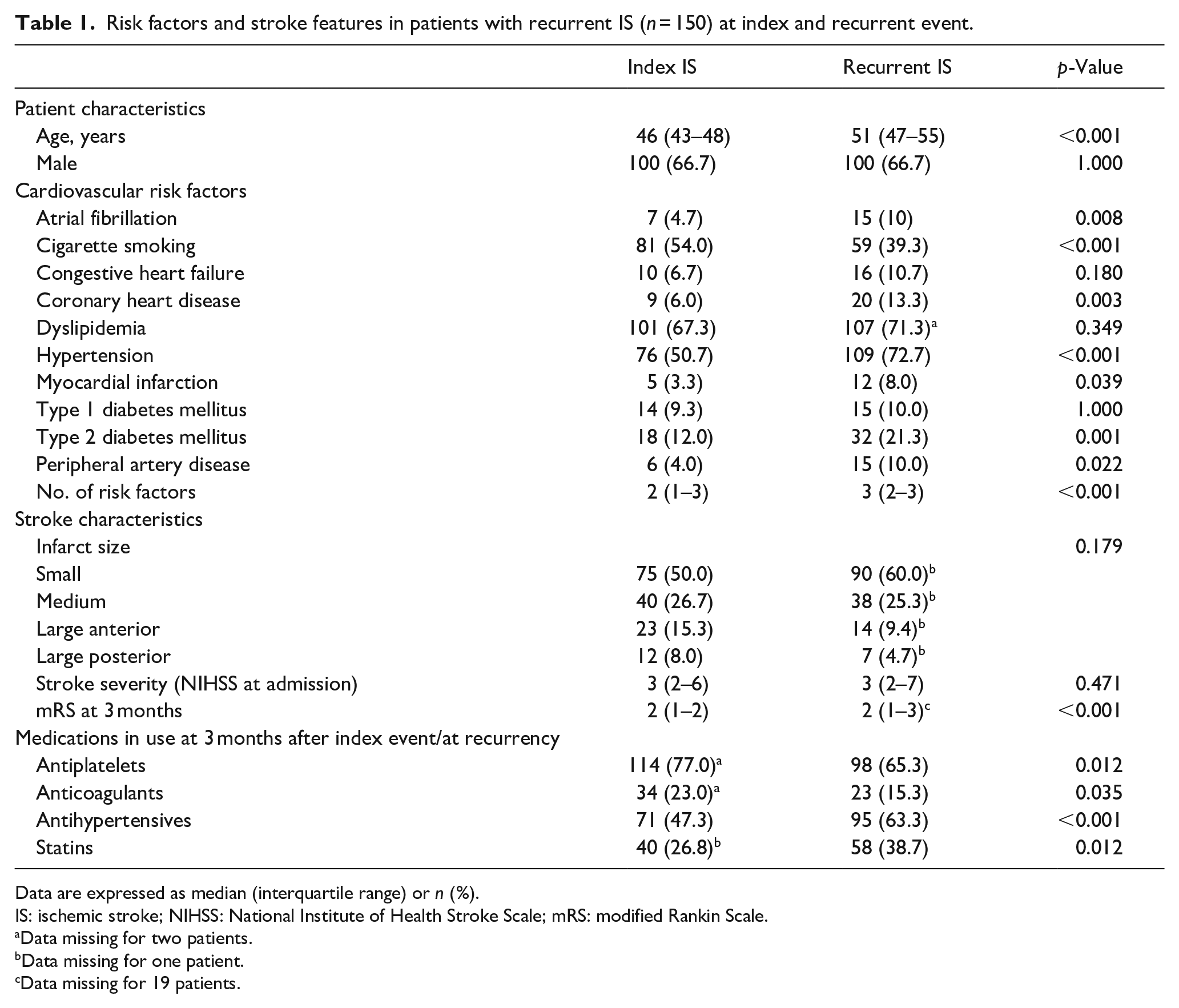
Data are expressed as median (interquartile range) or n (%).
IS: ischemic stroke; NIHSS: National Institute of Health Stroke Scale; mRS: modified Rankin Scale.
Data missing for two patients.
Data missing for one patient.
Data missing for 19 patients.
Etiology between index and recurrent ischemic stroke using the TOAST classification
Classified with TOAST, the proportion of true cryptogenic ISs decreased (16.7% vs 6.7%, p = 0.003), while the proportion of patients with incomplete evaluation (5c) increased (9.3% vs 19.3%, p = 0.015) between the index and recurrent IS. The proportion of other TOAST phenotypes 1–3 remained the same (Table 2, Figure 2(a)). The etiologies of index and recurrent IS were exactly the same in 11 of 18 (61.1%) index ISs caused by LAA, 20 of 27 (74.1%) caused by cardioembolism, 23 of 37 (62.2%) caused by SVD, 13 of 26 (50.0%) caused by other causes, 1 of 3 (33.3%) caused by multiple possible etiologies, 6 of 25 (24.0%) index cryptogenic ISs, and 5 of 14 (35.7%) ISs with incomplete evaluation. PFO alone was diagnosed in 8 (5.3%) patients both at index and at recurrent IS. The median RoPE Score was 8.0 (IQR 7.0–8.3) at index versus 6.0 (IQR 4.3–7.8) at recurrent event. Furthermore, at index IS, 2 (1.3%) patients had PFO with ASA.
Etiologies of IS at index and recurrent event by modified TOAST classification (n = 150).
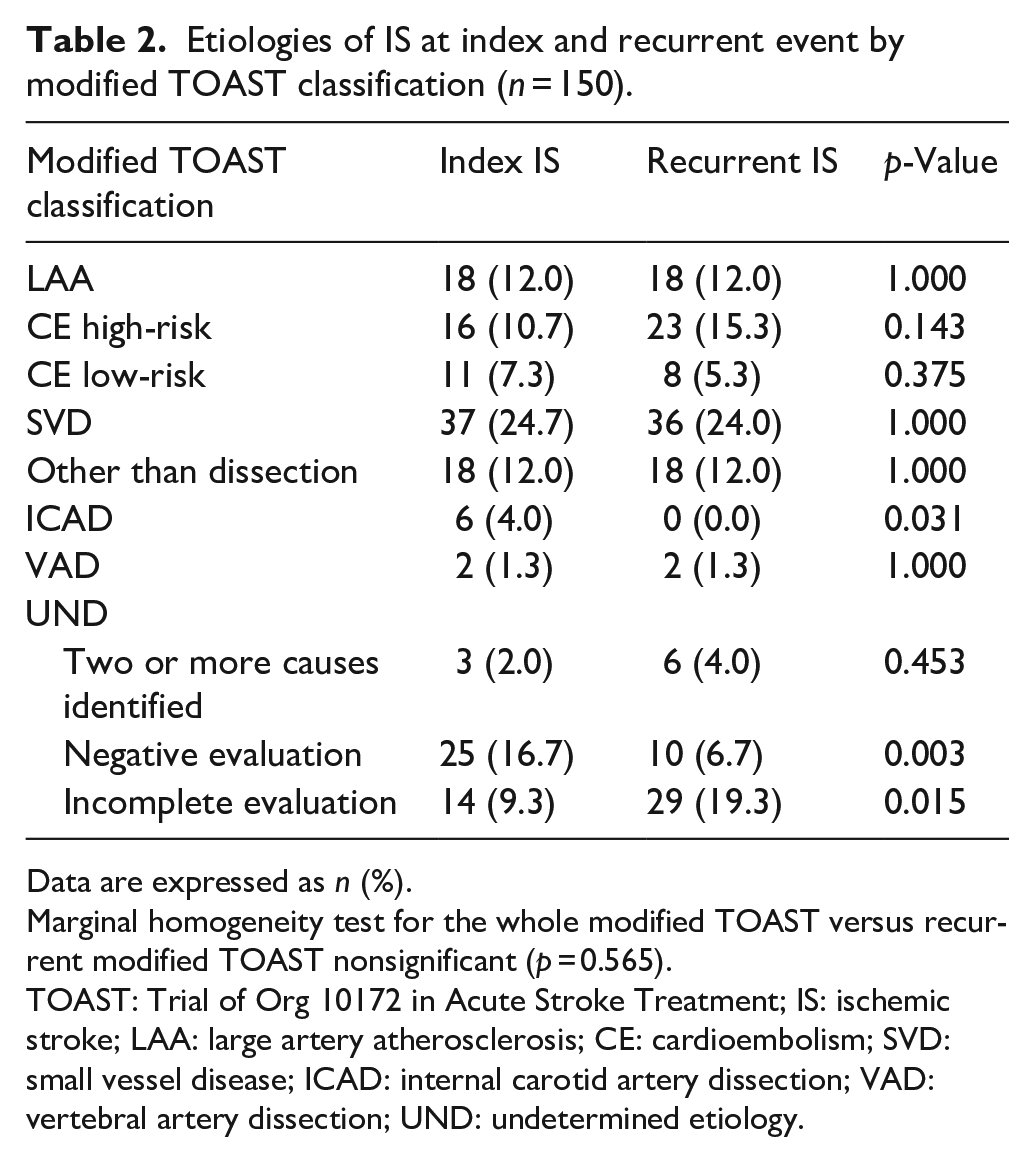
Data are expressed as n (%).
Marginal homogeneity test for the whole modified TOAST versus recurrent modified TOAST nonsignificant (p = 0.565).
TOAST: Trial of Org 10172 in Acute Stroke Treatment; IS: ischemic stroke; LAA: large artery atherosclerosis; CE: cardioembolism; SVD: small vessel disease; ICAD: internal carotid artery dissection; VAD: vertebral artery dissection; UND: undetermined etiology.
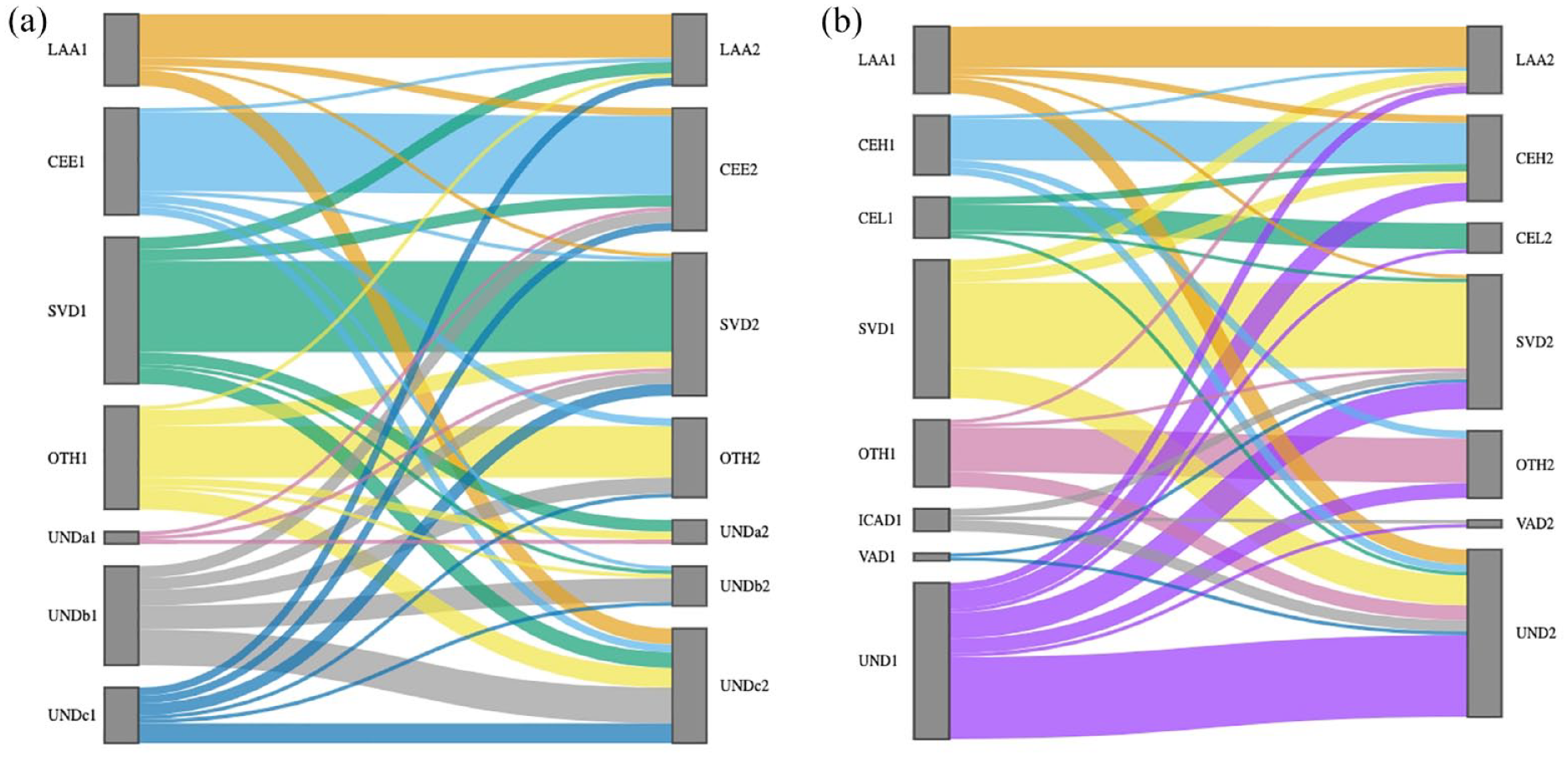
The change of etiology from the index to the recurrent event in (a) TOAST and (b) modified TOAST classification system by Sankey diagram.
Etiology between index and recurrent ischemic stroke using the modified TOAST classification
Using the modified TOAST classification, the prevalence of ISs caused by internal carotid artery dissection (ICAD) decreased (4.0% vs 0.0%, p = 0.031) while it remained unchanged for ISs caused by vertebral artery dissection (VAD) or ISs caused by other defined etiologies (Table 2, Figure 2(b)). Similarly, the prevalence of CE high-risk and CE low-risk remained the same (10.7% vs 15.3%, p = 0.143 and 7.3% vs 5.3%, p = 0.375, respectively). Of the 25 patients with an index cryptogenic IS (TOAST 5b), 1 had a recurrent IS due to vertebral artery dissection, 1 due to low-risk causes of CE, namely PFO, 2 due to high-risk causes of CE, 3 due to SVD, 3 due to other causes than dissection, namely 2 due to vasculitis and 1 due to APC resistance, 9 had incomplete evaluation, and 6 remained cryptogenic despite routine examinations.
In the 6 (5.2%) patients with fatal record-verified recurrences, 3 (50.0%) were due to high-risk sources of cardioembolism, 2 (33.3%) due to LAA and 1 (16.7%) due to other causes than dissection. Furthermore, of the 150 patients with a recurrent IS, multiple recurrences were verified in 26 (17.3%) patients (median 2, IQR 2–3). The majority of the second recurrences (n = 26) were undetermined ISs (34.6%) or ISs caused by rare causes other than dissection (30.8%). These rare syndromes included cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL, n = 2), primary angiitis of the central nervous system (PACNS, n = 3), one patient with secondary central nervous system vasculitis associated with systemic lupus erythematosus (SLE), one patient with severe anemia and hypovolemia, and one patient with polycytemia vera, heterozygous Factor V Leiden mutation and warfarin below therapeutic level. Eight patients experienced up to three recurrent ISs during the follow-up, five of which were due to a rare cause: one CADASIL, two PACNS, one vasculitis associated with SLE, and one patient with a thrombosed basilar artery aneurysm.
Finally, in the 815 patients with no recurrent IS, the most frequent etiology was undetermined (34.7%), followed by SVD (12.5%), other than dissection (10.6%), VAD (10.1%), CE low-risk (9.9%), CE high-risk (8.8%), ICAD (7.9%), and LAA (5.5%).
Etiology between index and recurrent ischemic stroke using the A-S-C-O classification
Table 3 shows the overall distribution of grade of certainty for each etiological subgroup according to A-S-C-O in both index and recurrent IS. Definitely a potential cause (A-S-C-O grade 1) could be verified in 76 index ISs, compared to 89 recurrences. At the time of the index IS, atherosclerosis was the most frequent definite cause (A = 1, 13.3%), followed by SVD (S = 1, 12.7%). In contrast, in recurrent ISs, definite SVD (S = 1, 18%) and cardioembolism (C = 1, 18%) were the largest groups, while atherosclerosis remained unchanged (A = 1, 13.3%). Recurrent events were more often due to definite cardioembolism compared to index ISs (18.0% vs 10.7%, p = 0.013) (Table 4). Compared to patients with recurrent IS, in the 815 patients with no recurrence, the most frequent definite etiology was other defined cause (O = 1, 23.1%), followed by cardioembolism (C = 1, 8.8%), SVD (S = 1, 6.3%), and atherosclerosis (A = 1, 5.8%).
Etiologies of IS at index and recurrent event by A-S-C-O classification (n = 150).
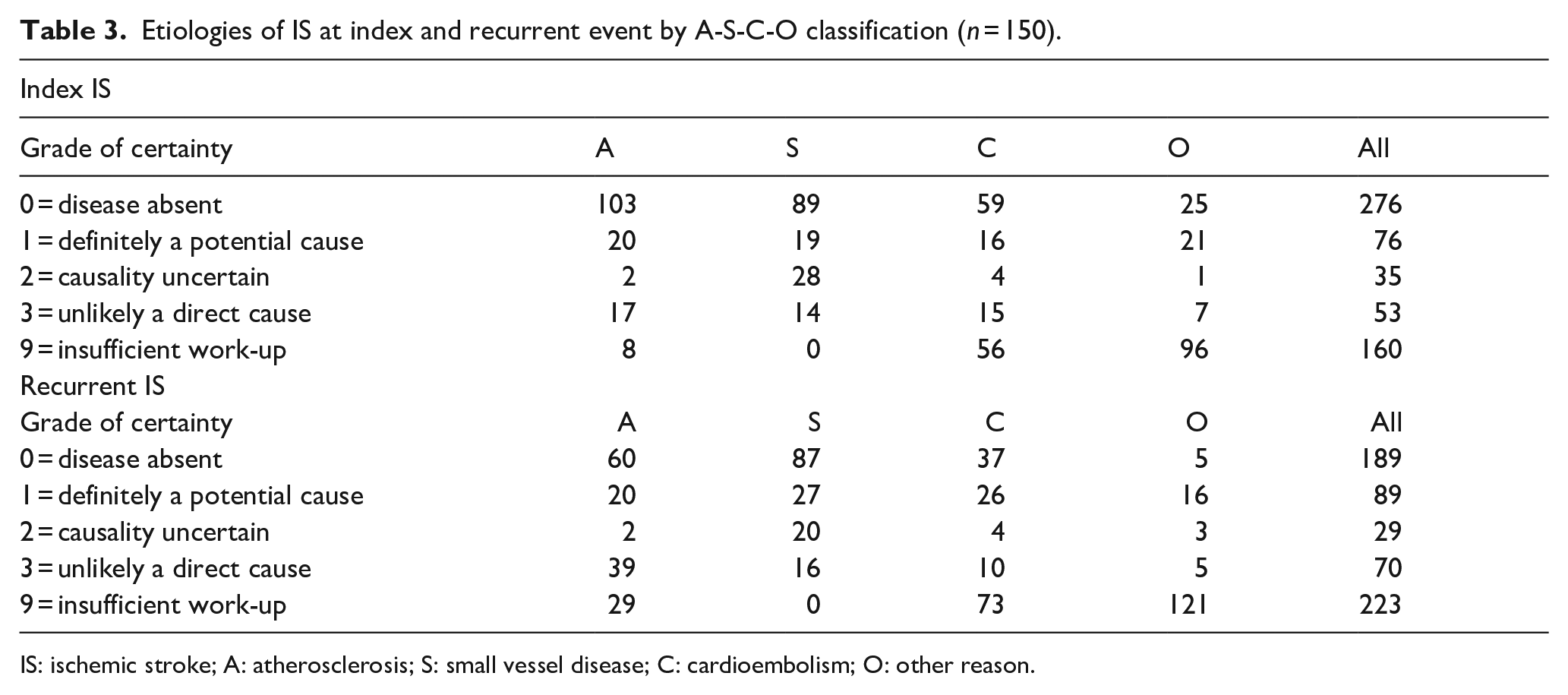
IS: ischemic stroke; A: atherosclerosis; S: small vessel disease; C: cardioembolism; O: other reason.
Comparison of definite A-S-C-O between index and recurrent event.
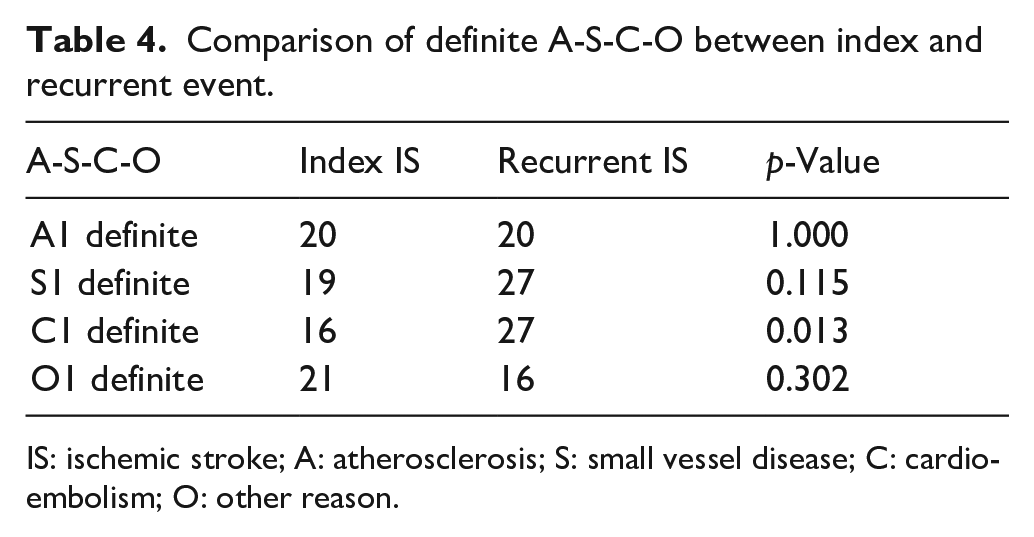
IS: ischemic stroke; A: atherosclerosis; S: small vessel disease; C: cardioembolism; O: other reason.
Discussion
In our retrospective cohort study, we found that in a significant number of 150 recurrent ISs in young adults, the etiologies remained mostly the same as in the index event. Up to 17% of patients with recurrent ISs experienced more than one recurrent event. Only the number of definitive cardioembolic strokes increased and the number of cryptogenic strokes decreased, however, including more cases with incomplete diagnostic work-up at the time of recurrence.
To our knowledge, this is the first study among young stroke patients to investigate differences in the etiologies of index and recurrent ISs. Among an older patient population looking at etiologies using the A-S-C-O classification, definite cardioembolic strokes were also more frequent at the recurrent event. 8 In that study, the etiological work-up at recurrency, especially regarding cardiological investigations, were less frequent, tallying with our observations. 8
In a recent meta-analysis on recurrence of IS involving patients over 18 years of age, recurrence rates were higher with LAA and cardioembolic strokes, where the etiology remained mostly the same as in recurrency. 18 On the contrary, the meta-analysis found that among ISs caused by SVD, the etiology in recurrent IS was more versatile. 18 In our study, most patients with LAA IS, cardioembolic and SVD infarcts had the same etiology at recurrence, while cryptogenic strokes decreased, and incomplete diagnostic work-up increased at recurrence.
Also, compliance with secondary preventive medication seems to be poor in the long run, with less than 40% of patients using statins at recurrence, although over 70% had dyslipidemia. The same trend applies to antihypertensives, indicating the need for better secondary preventive medication strategies and follow-up. According to our previous findings in a shorter follow-up, the use of antihypertensives was suboptimal in one third of patients in whom antihypertensives were initially prescribed. 19 Also, less than half of young IS patients used statins at end of follow-up in 2012 (vs ischemic stroke 1994–2007). 20 Similarly, the use of antiplatelets (65.3%) and anticoagulants (15.3%) was low at recurrency in the longer follow-up, possibly due to poor compliance, but hypothetically it could also be due to, for instance, hemorrhagic complications, and thus the patients’ inability to use medications as prescribed. Recurrent ISs should be avoided, especially since the mRS was higher after recurrent events than the mRS after the index event, leading to greater residual symptoms.
Both the A-S-C-O and TOAST classifications have weaknesses, but a comprehensive classification system for IS is not yet available. A-S-C-O has relatively strict and specific rules for classification for the required etiological work-up. 6 However, during the years, etiological work-up schemes have evolved and, for instance, prolonged rhythm monitoring to screen for atrial fibrillation is performed more systematically than in the past. 21 It can also be debated whether lumbar puncture is necessary for all patients with otherwise unknown etiology in A-S-C-O classification, as this is not done in routine practice unless an inflammatory etiology is clinically suspected. Similarly, the most widely used TOAST classification has its weaknesses. It does not give detailed requirements on investigations needed for specific etiologies, nor does it indicate if there are multiple etiologies, the etiologies found. Also, for instance, the classification of PFO-related strokes is not given in detail.
Our study has limitations. First, due to the long period of inclusion of patients, the etiologic work-up protocols have varied over time, and due to the retrospective study design, protocols have varied between patients. Then again, this better reflects the real-life situation. Also, for instance, the introduction of direct oral anticoagulants for non-valvular atrial fibrillation has changed treatment strategies in stroke patients. Second, with more advanced imaging techniques, such as high-resolution vessel wall imaging, for example, the proportion of undetermined IS and SVD might decrease and the proportion of LAA might increase, as was the case in a recent Chinese study. 22 Also, there might still be unidentified etiologies constituting now the undetermined group, such as the newly suggested clonal hematopoiesis of indetermined potential (CHIP). 23 Cancer screening was rarely done routinely, only in cases with high clinical suspicion, although it is a possible etiology of IS. 24 Third, A-S-C-O-D is a newer classification system that takes into account arterial dissection as a separate group, but also includes other changes compared to the previous A-S-C-O classification system. 25 As our cohort study already used the older A-S-C-O classification, we did not switch to A-S-C-O-D but considered vertebral and carotid arterial dissections in the modified TOAST classification as separate groups. Similarly, for PFO-related ISs, we only graded the RoPE score but did not have all the information needed for doing the newer and more extensive PFO-Associated Stroke Causal Likelihood grading. 26 We were unable to report in more detail whether the diagnostic work-up for recurrent IS actually had an impact on secondary prevention or outcome. Finally, some very early recurrences may have been missed because those who died within 30 days were excluded.
Nevertheless, there are strengths in our study. We have a large cohort consisting of solely young IS patients with a long follow-up time and a significant number of recurrent events. The coverage (90%), sensitivity (95%–97%) and positive predictive value (87%–93%) of stroke diagnoses have been rated as good in the Care Register for Health Care, from which the recurrent ISs were primarily retrieved. 27 We had the possibility to verify the etiologies from original patient records and not only rely on ICD codes or registry data. The TOAST and A-S-C-O classifications can be difficult to use, and the inter-rater agreement rate is not always good enough from a clinical point of view, although in one study it was rated high, 28 which led us to double-check the classifications and reach a consensus in difficult cases.
Conclusions
Our study showed that most etiologies remained unchanged in the index and recurrent IS also among young adults. In the future, prospective studies are needed to systematically determine the etiologies of recurrent ISs. Our study also emphasizes that etiological work-up should be systematically repeated also in recurrent ISs to avoid mistargeting of tertiary prevention efforts.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241238508 – Supplemental material for Etiologic subtypes of first and recurrent ischemic stroke in young patients using A-S-C-O and TOAST classification criteria: A retrospective follow-up study
Supplemental material, sj-docx-1-eso-10.1177_23969873241238508 for Etiologic subtypes of first and recurrent ischemic stroke in young patients using A-S-C-O and TOAST classification criteria: A retrospective follow-up study by Karoliina Aarnio, Nicolas Martinez-Majander, Elena Haapaniemi, Eeva Kokkola, Jenna Broman, Lauri Tulkki, Markku Kaste, Turgut Tatlisumak and Jukka Putaala in European Stroke Journal
Footnotes
Acknowledgements
We are indebted to Anu Eräkanto, Research Secretary, for her invaluable assistance in preparing the language editing for the manuscript.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TT serves/has served on advisory boards for Astra Zeneca, Bayer, Bristol Myers Squibb, Inventiva, and Portola Pharm. The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: K.A.: Academic research funding from Maire Taponen Foundation and N.M.M.: Academic research funding from Finnish Medical Foundation. T.T.: Academic research funding from the European Union, University of Gothenburg, Sahlgrenska University Hospital, and Wennerström’s Foundation.
Ethical approval
A regional Ethics Committee approved the study.
Informed consent
According to the Finnish legislation, a written informed consent is not needed in a registry-based study without direct patient contacts.
Guarantor
JP.
Contributorship
KA and NMM* designed the study, acquired and analyzed the data and prepared the first version of the manuscript.
EH, MK, TT, and JP designed the study and acquired the data.
EK, JB, and LT acquired the data.
All authors reviewed and edited the manuscript and approved the final version of the manuscript.
*shared first authorship.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.