
Abstract
Background:
Despite multiple effective secondary prevention strategies, the risk for stroke recurrence remains remarkable, and further ways to mitigate it are warranted. The results of the Cardiovascular Outcomes for People Using Anticoagulation Strategies (COMPASS) trial could generate the hypothesis that the addition of low-dose oral anticoagulation to the standard antiplatelet treatment could be beneficial for the prevention of stroke recurrence among patients with acute ischemic stroke who have no indication for oral anticoagulation. We aimed to assess this hypothesis with a systematic review and meta-analysis of currently available evidence from randomized controlled trials.
Methods:
Following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) reporting guidelines for systematic reviews and meta-analyses, we systematically reviewed MEDLINE, Scopus, and ClinicalTrials.gov until 14 January 2025. Eligible studies included randomized controlled trials including participants with acute ischemic stroke or high-risk transient ischemic attack with no indication for oral anticoagulation, who were randomized to a combination strategy of oral anticoagulation with antiplatelets versus antiplatelets alone. The outcomes studied included recurrent stroke, major hemorrhage, their combination (net clinical benefit outcome), any stroke, and magnetic resonance imaging (MRI)-detected covert brain infarct.
Results:
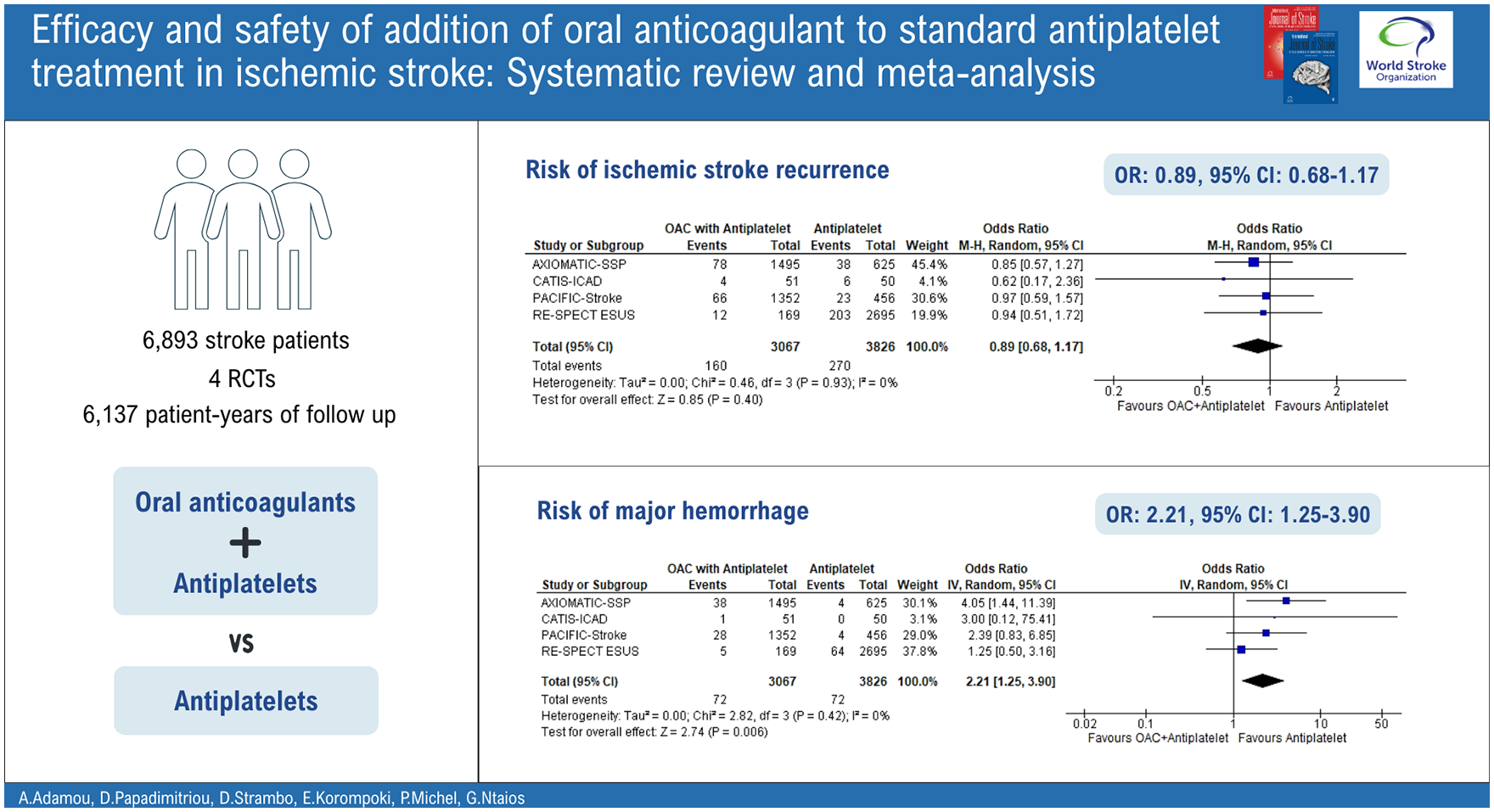
Among 1850 screened studies, 4 were eligible including 6893 patients (50.4% women). There were 430 stroke recurrences during an overall follow-up period of 6137 patient-years. Compared to patients assigned to standard antiplatelet treatment, those assigned to the combination strategy had a similar risk of ischemic stroke recurrence (odds ratio (OR) = 0.89, 95% confidence interval (CI) = 0.68–1.17), net clinical benefit outcome (OR = 1.12, 95% CI = 0.88–1.43), any stroke (OR = 0.88, 95% CI = 0.65–1.18), covert brain infarct (OR = 1.06, 95% CI = 0.86–1.31), but a higher risk of major hemorrhage (OR = 2.21, 95% CI = 1.25–3.90).
Conclusion:
The strategy of combination of oral anticoagulation with antiplatelet treatment should not be chosen in patients with acute ischemic stroke and no indication for oral anticoagulation, unless the results of ongoing trials like the LIBREXIA-Stroke and OCEANIC-Stroke yield different conclusions.
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.