
Abstract
Introduction:
Balance and postural control impairments are common in stroke patients, increasing fall risk and limiting their daily and social activities. Current research lacks comprehensive studies evaluating the efficacy and long-term effects of task-specific training on balance and postural control among stroke patients, especially when considering biomechanical and posturographic assessments.
Patients and Methods:
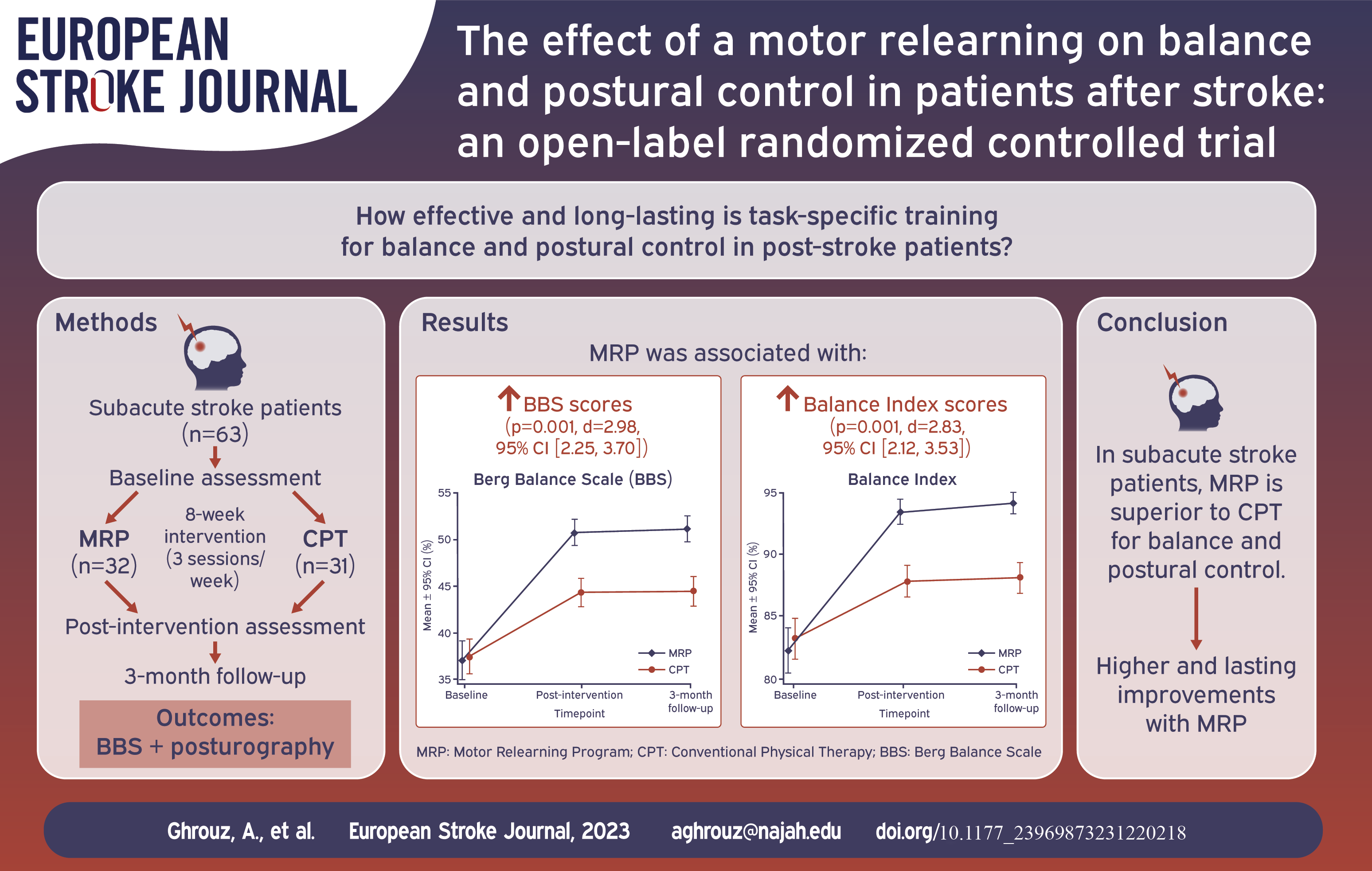
A randomized controlled trial included 63 subacute stroke patients recruited from the outpatient rehabilitation department. Participants were randomly assigned to the MRP group (n=32), receiving task-specific training based on MRP, or the CPT group (n=31), receiving conventional physical therapy. Both groups completed an 8-week intervention (3 sessions/week; 1 h./session). Balance and postural control were assessed at baseline, post-intervention, and 3-month follow-up using the Berg Balance Scale (BBS) and posturography.
Results:
The MRP group exhibited significantly larger improvements than the CPT group in both BBS scores (p=0.001, d=2.98, 95% CI [2.25, 3.70]) and Balance Index scores (p=0.001, d=2.83, 95% CI [2.12, 3.53]) after the intervention. These improvements were sustained at 3-month follow-up.
Discussion:
The findings suggest that task-specific training based on MRP is more effective than CPT for improving balance and postural control. The MRP intervention may enhance the motor learning and neural plasticity of the patients, leading to better functional outcomes. However, the study’s open-label design represents a limitation, and further research with adequate blinding is needed.
Conclusion:
Task-specific training based on MRP was superior to CPT for improving balance and postural control in subacute stroke patients. Participants undergoing MRP exhibited significant and clinically relevant improvements that were sustained at follow-up.
Introduction
Stroke is a prevalent cause of long-term disability, with a rising global incidence. 1 Stroke patients commonly experience impaired balance and postural control, which limits their daily activities and quality of life. 2 Rehabilitation programs aim to promote functional recovery in stroke survivors by improving their balance and posture. 3
Balance and postural control are essential for maintaining stability and controlling body movements. Balance refers to the ability to maintain the body’s center of mass (COM) over its base of support (BOS), while postural control involves maintaining a stable posture in response to external disturbances. Both require constant adjustment of the center of pressure (COP), which moves around the COM to keep it within the limit of stability (LOS). 4 Balance and postural control depend on the integration of sensory and motor systems by the central nervous system, which assigns different weights to sensory inputs from vision, somatosensory, and vestibular systems depending on the task and environment. 5
Stroke can cause a range of impairments, with balance dysfunction affecting approximately 83% of stroke patients. 6 This can lead to gait problems and an increased risk of falling, with falls occurring in around 37%–73% of patients within the first 6 months post-stroke. 7 Stroke can impair both the sensory system (disrupted sensory organization and integration) and the motor system (spasticity and weakness) involved in balance control, leading to deficits in balance control.8,9
The motor relearning program (MRP) is a rehabilitation approach for stroke patients that aims to improve motor control through specific motor task practice and training in controlled muscle action and movement components. It is based on learning principles, biomechanical movement analysis, and the importance of functional tasks in rehabilitation. The program involves repetitive and intense training, gradually increasing in difficulty with feedback, to regain lost functions. The MRP incorporates four factors for motor skill learning: eliminating unnecessary muscle activity, providing feedback, practicing, and integrating postural adjustments. This approach stimulates brain recovery by emphasizing cognitive function and learning. It requires the patient’s active participation and conscious movement control awareness, progressing to more automatic levels of practice.10,11
Limited clinical trials have explored the effectiveness of MRP on balance and postural control. Chan et al. 12 found that MRP significantly improved functional recovery and balance compared to conventional therapy, while Mufidah et al. 13 discovered that MRP was more effective than the Bobath Method in enhancing standing balance. Despite promising outcomes for post-stroke patients, more rigorous research is required to validate MRP’s efficacy. Large-scale RCTs are notably scarce, often hindered by small sample sizes. Long-term effects of MRP are underexplored, with existing research mainly focusing on immediate or short-term outcomes. Moreover, there is a significant research gap in using comprehensive outcome measures, especially those using biomechanical balance and posturography variables. Current evidence predominantly relies on traditional clinical measures, and studies investigating the impact of MRP using these instrumental evaluation tools are scarce or non-existent. Incorporating these evaluation tools can provide more objective and detailed information about the biomechanical balance outcomes and enhance our understanding of MRP’s impact on stroke rehabilitation.
To address these gaps, this study aimed to evaluate the effectiveness and long-term outcomes of task-specific training based on MRP on balance and postural control in post-stroke patients. This study provides comprehensive evidence for the effectiveness and value of the MRP as a rehabilitation approach for stroke patients. It also intends to bridge the current knowledge gap in rehabilitation and exercise recommendations in the stroke population.
Methods
Study design and setting
This study is a two-armed randomized controlled clinical trial (RCT) of parallel design, conducted at the Department of Physical Medicine and Rehabilitation in two hospitals of the Parc de Salut Mar Consortium (Hospital de l’Esperança and Centre Fòrum-Hospital del Mar) in Barcelona, Spain. The study employed standardized clinical outcome measures and posturography to assess improvements in balance and postural control. The study protocol was published, 14 and the study adhered to the Consolidated Standards of Reporting Trials (CONSORT) reporting guidelines. The study’s CONSORT flow chart is presented in Figure 1.
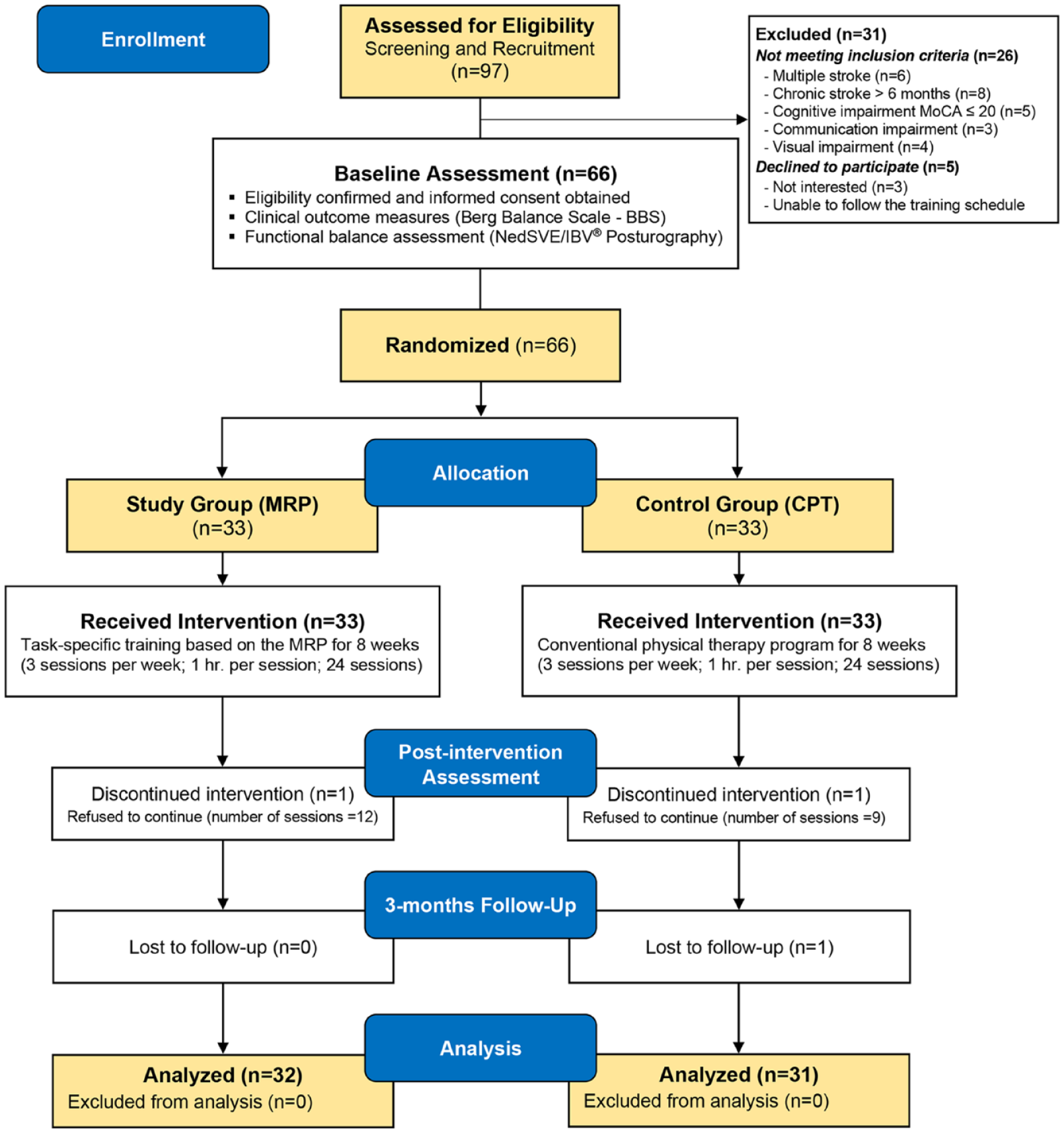
CONSORT flow chart of the study.
Participants
The study included subacute stroke patients aged 18–85, admitted to an outpatient rehabilitation department. Inclusion criteria were: first-ever subacute stroke (1–6 months), ability to provide informed consent, hemiparesis with lower-limb muscle power of 2–4 on the Medical Research Council (MRC) Muscle Scale on the affected side, independent standing for at least 1 min, and ambulation of 25 feet/10 m (with or without assistive device). Exclusion criteria were: post-stroke patients with major cognitive deficits (Montreal Cognitive Assessment-MoCA score ⩽ 20) and/or communication impairments preventing them from following directions (e.g. deafness, aphasia), visual impairments (e.g. visuospatial neglect, diplopia), receiving other related therapy that may affect the study’s efficacy, medical contraindications to start rehabilitation (e.g. severe uncontrolled hypertension, unstable angina), and history of disability related to neurological deficits other than stroke.
Recruitment and consent
The study was conducted from October 2021 to January 2023. Participants were recruited from the outpatient rehabilitation department through referrals from specialist physicians. The principal investigator (PI) screened and obtained consent from eligible participants before the baseline assessment. Participants who completed the assessment were then randomly assigned to intervention groups. Assessments and interventions conducted at the Functional and Movement Analysis Laboratory at Centre Fòrum-Hospital del Mar.
Randomization and blinding
Participants were randomly assigned to two groups using a web-based tool with a block size of 4 and a 1:1 allocation ratio. The PI conducted the randomization using sealed envelopes and informed participants of their assigned intervention group. The study involved an exercise-based intervention with active participation from therapists and participants, making blinding after assignment unfeasible. The PI, who also served as the outcome assessor, was involved in most interventions. Therefore, the study was an open-label trial, except for the person responsible for data analysis.
Interventions
Participants from both groups completed an 8-week, (3 sessions per week; 1 h. per session; 24 sessions) of either task-specific training based on the MRP or conventional physical therapy (CPT). The interventions were delivered face-to-face and individually. The interventions in the two groups were as follows:
Study group (MRP)
The participants received task-specific training based on the MRP, designed and implemented by the PI, following MRP approach that incorporates motor learning principles, such as feedback, variability, and specificity. The MRP aims to enhance balance and postural control by improving the sensory, motor, and central systems involved in maintaining stability.10,11 Each MRP session included five tasks: (1) bed mobility and sitting up: exercises for trunk rotation, bridging, single-leg bridge, and transitioning from supine to sitting at the edge of the bed; (2) balanced sitting: activities for trunk lateral flexion, rotation, and multidirectional reaching while seated; (3) standing up and sitting down: transitioning from a seated position on a firm flat surface with no arm rests to standing with upright posture and feet placed backward, followed by sitting down by bending the hips, knees, and ankles; (4) balanced standing: practicing multidirectional reaching activities, heel and toe raises, single leg standing, and knee extension with heel strike; and (5) walking practice: starting with practice of walking components, progressing to backwards, sideways, and braiding walking, then heel-to-toe walking (tandem walking), and finally walking with head turns and tilts. For a demonstration, description, and progression of the MRP training program’s exercises, see Supplemental 2.
Control group (CPT)
The control group received a CPT training program, implemented by the PI and modeled after conventional stroke rehabilitation.15,16 Each CPT session comprised five training components: (1) gradual progressive stretching of the shoulder, elbow, forearm, wrist, hamstrings, and calf; (2) active-assisted range of motion for the affected upper and lower limbs, including the hip, knee, ankle, shoulder, elbow, forearm, and wrist; (3) strengthening exercises of the hip abductors, quadriceps, and hamstrings; (4) balance training, including reaching beyond arm’s length while sitting and standing; and (5) walking training that involves a dynamic balance challenge (e.g. overground walking and obstacle courses). For a demonstration, description, and progression of the CPT training program’s exercises, see Supplemental 3.
Assessments and outcomes
The assessment variables for this study included the patients’ demographic information, clinical characteristics, and posturography data. Patients from both groups were assessed at baseline, post-intervention, and 3-month follow-up. The study outcomes were as follows:
Berg Balance Scale (BBS)
The primary outcome was the BBS, a widely used clinical performance measure to assess functional balance ability. It consists of 14 predetermined tasks that evaluate both static and dynamic balance, with tasks of varying difficulty. Each task is scored on a 5-point scale, ranging from 0 to 4, resulting in a total score range of 0–56. Higher scores indicate better performance. 17 The BBS is considered reliable, valid, and responsive in measuring balance impairment in post-stroke patients. 18 The minimal detectable change for clinically important differences is 6 BBS points, providing 90% confidence in genuine change for stroke patients. 19
Posturography assessment
The functional balance assessment was conducted using the NedSVE/IBV® system, a computerized posturography software. This system utilizes data from a dynamometric platform to analyze balance disorders, comparing them to normal patterns (based on age and sex). The assessment comprises two tests: static posturography tests to evaluate sensory input and postural control tests, including limits of stability (LOS) and rhythmic and directional control (RDC). The overall balance assessment (balance index) is a weighted average of the test scores, expressed as a percentage of normality. A score of 90%–100% indicates normal balance, 80%–89% indicates slight impairment, and below 79% indicates functional impairment.20,21
The static balance assessment involved four 30-s Romberg tests on a dynamometric platform, manipulating sensory input (visual, proprioceptive, and vestibular) necessary to maintain balance. The tests were: Romberg with eyes open (ROA), Romberg with eyes closed (ROC), Romberg with eyes open on foam cushion (RGA), and Romberg with eyes closed on foam cushion (RGC). The system recorded postural oscillation, indicating COP displacement, during these tests (Figure 2(a)). Moreover, the system calculated four indices to assess the contributions of the somatosensory, visual, and vestibular systems to balance.
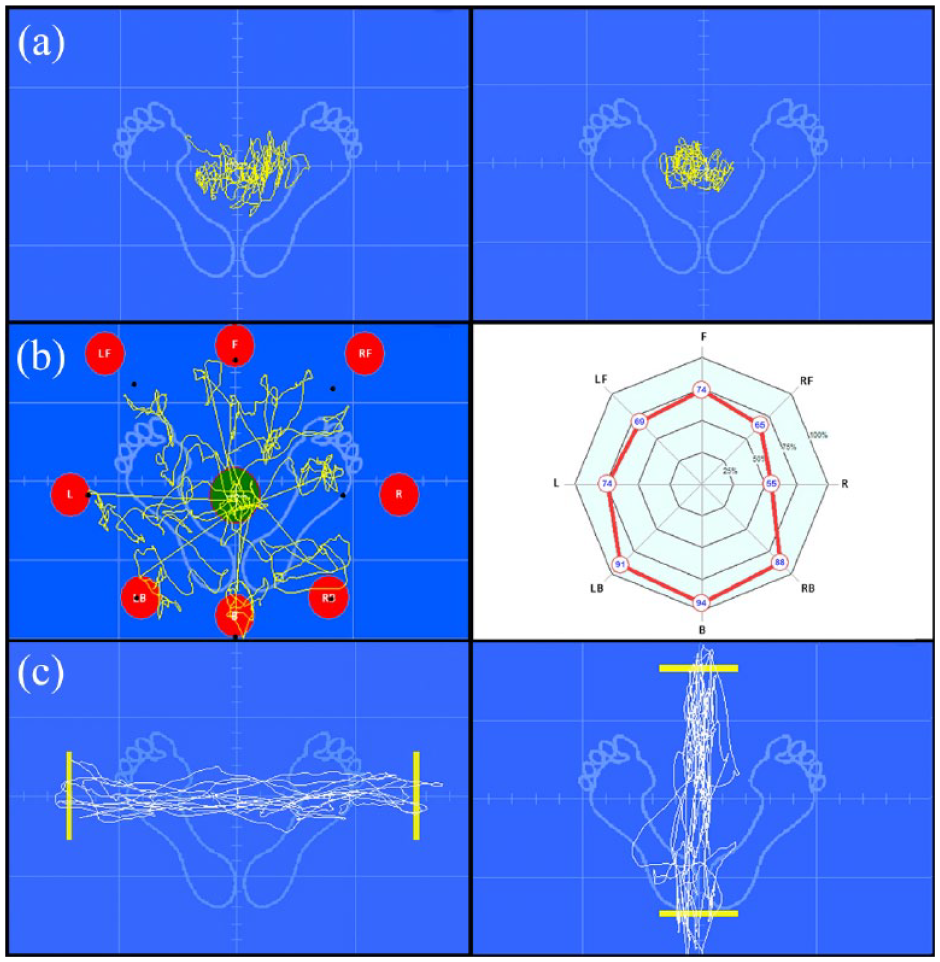
(a) Postural oscillation recording with dynamometric platform. (b) LOS analysis test with COG displacement toward targets. Yellow traces and black points denote direction and maximum ranges of each limit. Graphical representation of scores for each stability limit direction is also shown. (c) Mediolateral and anteroposterior rhythmic and directional control tests with COG trajectory tracking.
The LOS test evaluates the participant’s stability limits in eight directions by matching their COG to a cursor on a screen (Figure 2(b)). Targets appear sequentially for 8 s each, and the participant must reach and hold each target without changing their base of support. Evaluation is determined by weighting parameters referring to normality patterns, including maximum displacement, directional control, and reaction time to reach the target. The RDC tests assess the participant’s ability to rhythmically sync their COG with a screen target. The target moves either mediolateral (ML) or anteroposterior (AP) at different speeds. The participant tracks the target with their COG projection on the screen (Figure 2(c)).
Sample size
The trial’s sample size was calculated based on the Berg Balance Scale (BBS) as the main indicator, with an expected mean effect size of d = 0.65 from previous studies.12,13,22 Using G*power Software (version 3.1; Heinrich-Heine-Universität Düsseldorf, Germany), 23 with an alpha level (α) of 0.05 and power (1–β) of 0.80, a sample size of 30 patients in each group was determined. Taking into account a 10% drop-out rate, the total sample size for this study was approximately 66 patients randomized to either the study or control groups.
Statistical analysis
Descriptive statistics included the mean and standard deviation for continuous variables, and a frequencies table for categorical variables showing absolute numbers and percentages. Statistical tests used were the Chi-square or Fisher exact tests for categorical variables, and the Mann-Whitney U test for continuous variables. The non-parametric option of the Mann-Whitney U test was chosen due to violations of the normality assumption for a significant number of continuous variables.
Between-group differences (MRP vs CPT) were tested using Mann-Whitney U tests. For within-group differences, the Wilcoxon signed-rank test was used to calculate differences between time points within each group. Cohen’s d effect sizes were reported to assess differences between and within groups. Cohen’s d values were interpreted as follows: very small effect (<0.2), small effect (0.2–0.4), medium effect (0.5–0.7), and large effect (⩾0.8). 24 Statistical significance was set at p-values less than 0.05 with 95% confidence intervals (CI). The statistical analysis was conducted using STATA version 15.1 (StataCorp, College Station, TX, USA).
Results
Participant flow
Out of 97 screened stroke patients, 31 were excluded or declined. The remaining 66 were randomized into study (n = 33) or control (n = 33) groups. Two participants withdrew, and one was lost to follow-up. The final analysis included 32 in the study group and 31 in the control group. Figure 1 displays the participant flow.
Baseline characteristics
The MRP and CPT groups had comparable baseline characteristics (p > 0.05) (Table 1). Age, gender distribution, stroke type, and time since stroke onset were similar between the groups. The mean BBS score, indicating impaired balance and fall risk, did not significantly differ between the groups. The posturography assessment showed no significant differences in various measures of postural control, except for ML rhythmic and directional control, which was lower in the MRP group (p = 0.041). However, the overall postural control assessment score and balance index global score did not significantly differ between the groups, indicating impaired balance in both. Supplementary 1 Table 1 provides additional balance assessment data at baseline.
Participants’ characteristics at baseline.
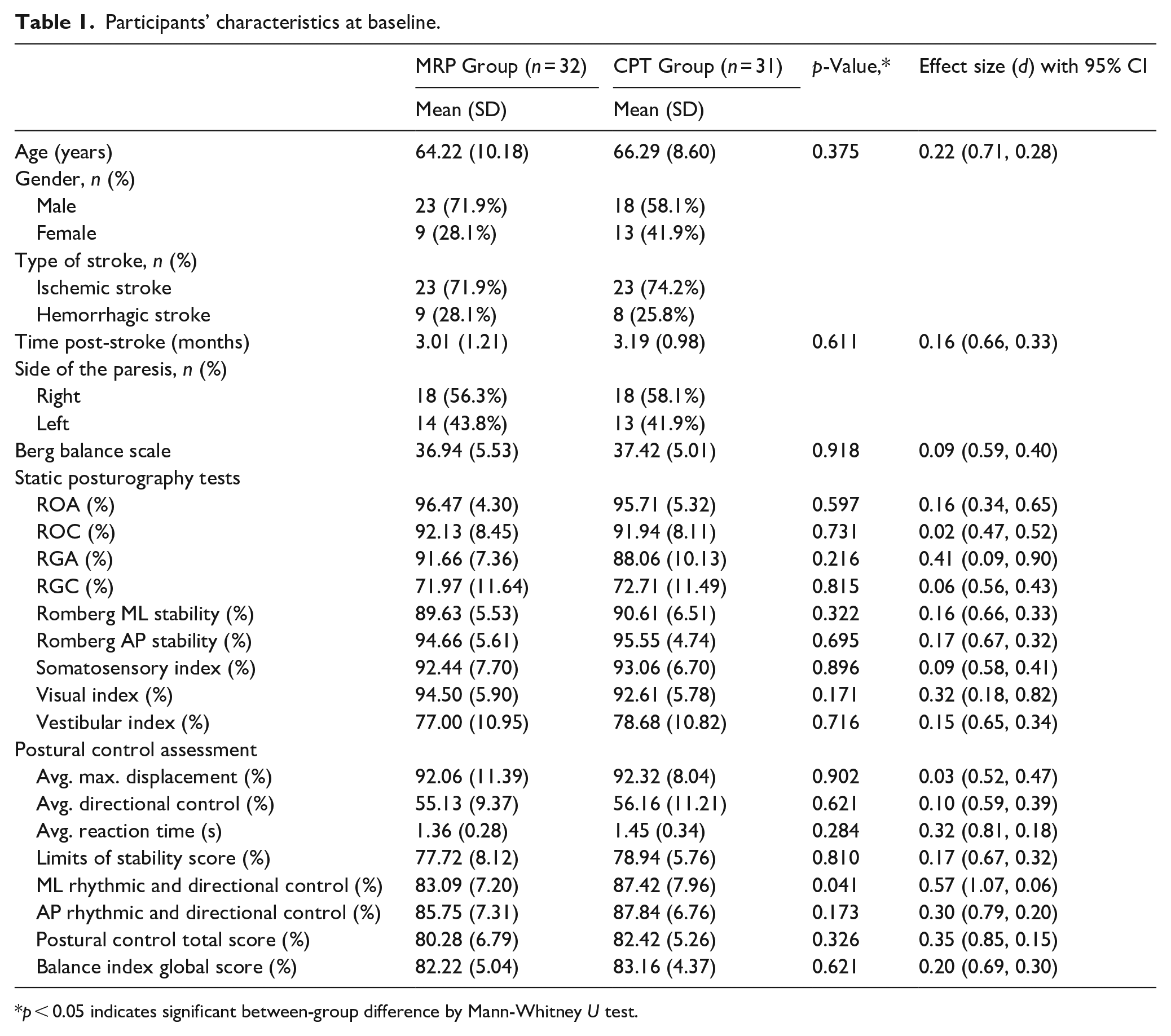
p < 0.05 indicates significant between-group difference by Mann-Whitney U test.
Changes from baseline to post-intervention
After the intervention, both groups showed significant improvement in all study outcomes (p < 0.05) (Table 2). The MRP group had higher improvements in mean BBS score (13.78, SD = 2.85, d = 4.84 vs 6.90, SD = 1.56, d = 4.43; p < 0.001, d = 2.98) and posturography assessment tests (global score: 11.19, SD = 2.89, d = 3.87 vs 4.61, SD = 1.52, d = 3.03; p = 0.001, d = 2.83) compared to the CPT group. Supplemental 1 Table 2 provides additional balance assessment data at post-intervention.
Changes from baseline to post-intervention.
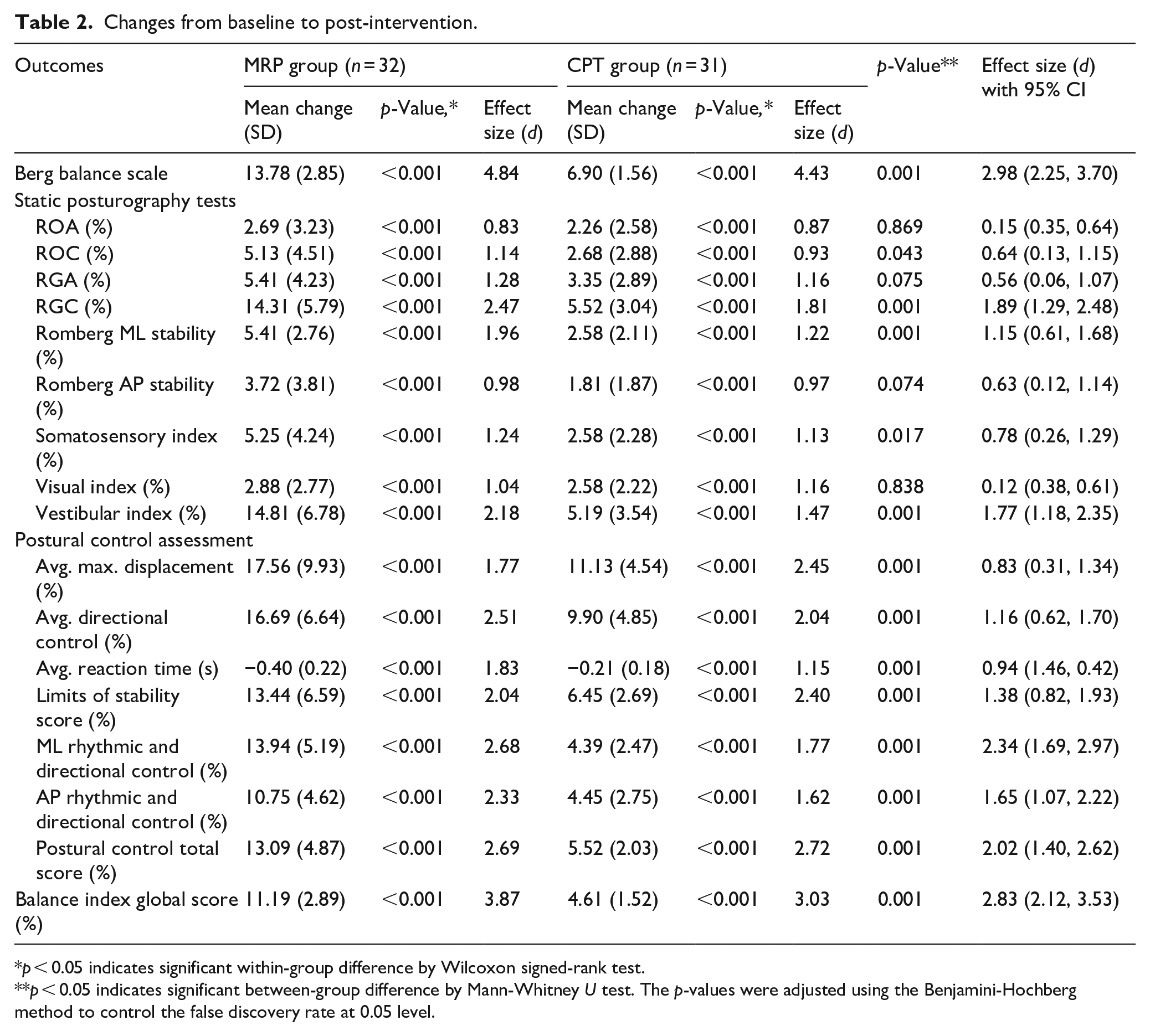
p < 0.05 indicates significant within-group difference by Wilcoxon signed-rank test.
p < 0.05 indicates significant between-group difference by Mann-Whitney U test. The p-values were adjusted using the Benjamini-Hochberg method to control the false discovery rate at 0.05 level.
Changes from post-intervention to 3-month follow-up
At the 3-month follow-up, both groups improved in the BBS score, but only the MRP group had a significant change (p = 0.024). The MRP group also significantly improved in the balance index global score (p < 0.001), while the CPT group did not. However, there were no significant differences between the groups in either outcome (see Supplemental 1 Table 3).
Discussion
Following a stroke, individuals commonly experience difficulties with balance and postural control, which increase fall risk and limit daily activities. Addressing these issues is crucial for effective stroke rehabilitation. This study aims to evaluate the effectiveness and long-term outcomes of task-specific training based on MRP for improving balance and postural control in subacute stroke patients.
The study group received task-specific training based on MRP, while the control group received conventional physical therapy. Both groups completed 24 rehabilitation sessions over 8 weeks. This intensity aligned with international guidelines for stroke rehabilitation.15,25 Therefore, the study interventions were in line with the current best practice recommendations for stroke rehabilitation.
This study used standardized and objective outcome measures to evaluate balance and postural control impairments in subacute stroke patients. The primary measure was the BBS, a widely used and validated tool for assessing balance impairment. However, the BBS has limitations, including a ceiling effect, low sensitivity to change, and poor correlation with other functional outcomes. 26 Therefore, it might not capture the full extent of the impact of MRP on balance and postural control. To address this concern, the study also utilized posturography, a biomechanical balance assessment that provides more detailed and objective information about balance performance and stability. Posturography can detect subtle changes that may not be captured by the BBS. By using a combination of standardized and objective measures, the study improved the reliability, validity, and consistency of its findings. This highlights the importance of considering both clinical and biomechanical measures when evaluating the effectiveness of rehabilitation programs in stroke rehabilitation.
The MRP and CPT groups were comparable at baseline, with no significant differences (p > 0.05), indicating that any observed differences in outcomes are more likely due to the interventions. This strengthens study validity and enhances the generalizability of the findings. After the intervention, the MRP group showed a significantly greater mean improvement (13.78 vs 6.90) and a larger effect size in the BBS score. This suggests the superiority of the MRP intervention in improving balance and reducing fall risk. These findings are consistent with previous studies that have demonstrated the effectiveness of MRP in stroke patients, as measured by the BBS.12,13,27
The MRP intervention outperformed CPT in improving static balance control under various sensory conditions and contributions from somatosensory, visual, and vestibular inputs. This was evident through greater mean changes and effect sizes, suggesting an enhanced ability to utilize multiple sensory cues for balance maintenance. The superior impact of the MRP intervention on integrating sensory information and sensory reweighting for post-stroke balance control is crucial for maintaining stability in complex environments. This difference could be attributed to the fact that the MRP intervention involved more sensory stimulation and challenge, requiring participants to use different sensory systems to maintain balance, while the CPT intervention involved less sensory variation and did not activate different sensory systems as much.
The MRP group exhibited significantly greater improvements than the CPT group in postural control assessment, including LOS and rhythmic/directional control tests. These findings suggest the effect of the MRP intervention on enhancing postural control during weight shifting, which is important for fall prevention and functional task performance. The MRP intervention’s advantage can be attributed to its incorporation of more dynamic and complex balance tasks that challenged participants to move their COG closer to their LOS, and more dynamic and directional movements that challenged participants’ balance in various directions. The CPT intervention, on the other hand, used more static and simple balance tasks.
Considering the balance index global score, the MRP group exhibited significantly greater improvements compared to the CPT, as evidenced by larger mean changes and effect sizes. This suggests the superior effectiveness of the MRP intervention in enhancing functional balance performance. This difference could be attributed to the MRP intervention’s incorporation of more functional and task-specific balance exercises that simulate real-life situations, whereas the CPT intervention involved general and non-specific exercises. These findings emphasize the importance of specificity and relevance in balance rehabilitation after stroke.
At the 3-month follow-up, both groups maintained their improvements. The MRP group improved significantly in BBS and posturography, while the CPT group did not. However, there was no significant difference between the groups. This suggests that MRP had a greater impact on maintaining and promoting functional balance over time, highlighting its potential long-term benefits for stroke patients. The long-term maintenance of MRP effects could be attributed to its emphasis on cognitive, associative, and autonomic processes that promote motor learning, leading to better consolidation and retention of motor skills after practice. 28 MRP incorporates factors such as practice variability, specificity, and feedback, which enhance the consolidation and retention of motor skills in stroke patients, leading to long-lasting functional improvements. This makes MRP a preferable approach for stroke rehabilitation, effectively enhancing functional balance recovery.
This study holds significant clinical implications for stroke rehabilitation. It suggests that task-specific training based on MRP is superior to CPT in enhancing balance and postural control for stroke patients. MRP targets functional tasks relevant to daily life, addressing specific impairments and challenges faced by stroke survivors. Moreover, MRP enables stroke survivors to practice movements in context, facilitating more efficient and meaningful recovery. Therefore, MRP stands as a recommended and effective approach to address balance impairments in a task-specific manner. Healthcare professionals should consider integrating MRP into their clinical practice and stroke rehabilitation protocols to optimize functional outcomes and achieve better long-term results. Furthermore, this study contributes to existing literature by providing further evidence supporting the benefits of the MRP in improving functional balance.
Limitations
The study has certain limitations to acknowledge. It only includes first-ever stroke patients in the subacute phase, with mild to moderate lower-limb weakness, who can stand and walk independently. This excludes many post-stroke patients with different recovery phases and stroke severities, affecting its generalizability. Future research should recruit a wider and more diverse range of post-stroke patients, including those in the acute and chronic phases or with severe impairments.
Another limitation is the lack of blinding, as it was an open-label trial, with participants and outcome assessors aware of the intervention received. This could introduce biases and reduce the internal validity of the study. Future research should implement a double-blind design, where neither the participants nor the therapist or outcome assessor are aware of the intervention allocation.
Conclusions
Task-specific training based on MRP was superior to CPT for improving balance and postural control in subacute stroke patients. Participants who received MRP exhibited significant and clinically relevant improvements in balance and postural control and maintained these improvements at follow-up. However, the study’s open-label design represents a limitation, and further research with adequate blinding is needed.
Supplemental Material
sj-docx-1-eso-10.1177_23969873231220218 – Supplemental material for The effect of a motor relearning on balance and postural control in patients after stroke: An open-label randomized controlled trial
Supplemental material, sj-docx-1-eso-10.1177_23969873231220218 for The effect of a motor relearning on balance and postural control in patients after stroke: An open-label randomized controlled trial by Amer Ghrouz, Anna Guillen-Sola, Andrea Morgado-Perez, Elena Muñoz-Redondo, Cindry Ramírez-Fuentes, Yulibeth Curbelo Peña and Esther Duarte in European Stroke Journal
Supplemental Material
sj-pdf-2-eso-10.1177_23969873231220218 – Supplemental material for The effect of a motor relearning on balance and postural control in patients after stroke: An open-label randomized controlled trial
Supplemental material, sj-pdf-2-eso-10.1177_23969873231220218 for The effect of a motor relearning on balance and postural control in patients after stroke: An open-label randomized controlled trial by Amer Ghrouz, Anna Guillen-Sola, Andrea Morgado-Perez, Elena Muñoz-Redondo, Cindry Ramírez-Fuentes, Yulibeth Curbelo Peña and Esther Duarte in European Stroke Journal
Supplemental Material
sj-pdf-3-eso-10.1177_23969873231220218 – Supplemental material for The effect of a motor relearning on balance and postural control in patients after stroke: An open-label randomized controlled trial
Supplemental material, sj-pdf-3-eso-10.1177_23969873231220218 for The effect of a motor relearning on balance and postural control in patients after stroke: An open-label randomized controlled trial by Amer Ghrouz, Anna Guillen-Sola, Andrea Morgado-Perez, Elena Muñoz-Redondo, Cindry Ramírez-Fuentes, Yulibeth Curbelo Peña and Esther Duarte in European Stroke Journal
Supplemental Material
sj-pdf-4-eso-10.1177_23969873231220218 – Supplemental material for The effect of a motor relearning on balance and postural control in patients after stroke: An open-label randomized controlled trial
Supplemental material, sj-pdf-4-eso-10.1177_23969873231220218 for The effect of a motor relearning on balance and postural control in patients after stroke: An open-label randomized controlled trial by Amer Ghrouz, Anna Guillen-Sola, Andrea Morgado-Perez, Elena Muñoz-Redondo, Cindry Ramírez-Fuentes, Yulibeth Curbelo Peña and Esther Duarte in European Stroke Journal
Supplemental Material
sj-pdf-5-eso-10.1177_23969873231220218 – Supplemental material for The effect of a motor relearning on balance and postural control in patients after stroke: An open-label randomized controlled trial
Supplemental material, sj-pdf-5-eso-10.1177_23969873231220218 for The effect of a motor relearning on balance and postural control in patients after stroke: An open-label randomized controlled trial by Amer Ghrouz, Anna Guillen-Sola, Andrea Morgado-Perez, Elena Muñoz-Redondo, Cindry Ramírez-Fuentes, Yulibeth Curbelo Peña and Esther Duarte in European Stroke Journal
Footnotes
Acknowledgements
Sincere gratitude to Dr. Esther Duarte, the study director, for her support, insights, and comments that helped complete this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. This research study is an essential requirement for Amer Ghrouz doctoral study (PhD) in Physical Medicine and Rehabilitation at Universitat Autònoma de Barcelona, Spain and not funded by any party or agency.
Ethical approval
The Research Ethics Committee of the Hospital del Mar Research Institute, Barcelona, Spain, has approved the study (REC No: 2021/9986/I).
Informed consent
Participants were verbally informed about the study and provided with an information sheet. Written informed consent was obtained from all participants before the study commenced.
Guarantor
AG.
Contributorship
AG contributed to the trial design, procedures, content development, and drafted the manuscript. ED was responsible for the critical revision of the article for important intellectual content, provided feedback on the trial design, and managed the project. AG-S also contributed to the critical revision of the article. AM-P, EM-R, CR-F, and YGCP contributed feedback on assessments and data collection. All authors revised and approved the final version of the manuscript.
Trial registration
The study was registered on ClinicalTrials.gov with registration number (NCT05076383).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.