
Abstract
Rationale
Restoration of adequate standing balance after stroke is of major importance for functional recovery. POstural feedback ThErapy combined with Non-invasive TranscranIAL direct current stimulation (tDCS) in patients with stroke (POTENTIAL) aims to establish if cerebellar tDCS has added value in improving standing balance performance early post-stroke.
Methods
Forty-six patients with a first-ever ischemic stroke will be enrolled in this double-blind controlled trial within five weeks post-stroke. All patients will receive 15 sessions of virtual reality-based postural feedback training (VR-PFT) in addition to usual care. VR-PFT will be given five days per week for 1 h, starting within five weeks post-stroke. During VR-PFT, 23 patients will receive 25 min of cerebellar anodal tDCS (cb_tDCS), and 23 patients will receive sham stimulation.
Study outcome
Clinical, posturographic, and neurophysiological measurements will be performed at baseline, directly post-intervention, two weeks post-intervention and at 15 weeks post-stroke. The primary outcome measure will be the Berg Balance Scale (BBS) for which a clinical meaningful difference of six points needs to be established between the intervention and control group at 15 weeks post-stroke.
Discussion
POTENTIAL will be the first proof-of-concept randomized controlled trial to assess the effects of VR-PFT combined with cerebellar tDCS in terms of standing balance performance in patients early post-stroke. Due to the combined clinical, posturographical and neurophysiological measurements, this trial may give more insights in underlying post-stroke recovery processes and whether these can be influenced by tDCS.
Keywords
Introduction and rationale
Impaired standing balance after stroke is common and has a significant impact on fall events, independence in activities of daily living and perceived disability.1,2 Prospective cohort studies suggest that most improvements in standing balance and walking ability occur within the first five to eight weeks post-stroke.3,4 There is strong evidence of enhanced homeostatic forms of neuroplasticity during this time window, including upregulation of gene expression of growth promoting factors, such as brain derived nerve growth factors (BDNF) followed by growth inhibiting factors. 5 Human motor learning in this critical time window may be facilitated by transcranial direct current stimulation (tDCS) which is believed to specifically target synapse-based learning by enhancing the turnover of the secretion of BDNF. 6 tDCS is thought to induce polarity-driven alterations of membrane potentials and efficacy modulations of specific neuronal receptors in the underlying brain tissue. 6 These dynamic neural modulations are evident not only in motor performance,7–9 but also in intrinsic functional network connectivity that manifest in neurophysiological recordings of cortical brain activity. 10 Neural changes while performing balance tasks are mostly reflected by a change in theta (4–7 Hz), and alpha power (7.5–12.5 Hz).11,12 A higher alpha power reflects increased learning speed and an optimal concentration level. 13 Decreased alpha activity is also generally seen in patients after stroke. 14 Theta power activity is associated with an emerging state of concentration and optimal error control and found to increase with increasing complexity of balance tasks.11,15 Although a general deceleration of EEG signals is associated with poor functional outcome after stroke, conflicting results regarding a correlation of increased theta power activity with post-stroke function are found.16–18 Next to an alteration in power spectral density, asymmetry between the hemispheres (low Brain Symmetry Index) has been associated with poor clinical function and disability six months post-stroke and is believed to reflect the clinical neurological condition of acute stroke patients.19,20 To study these changes in cortical activation patterns in post-stroke recovery, and the potential influence tDCS may have on these processes, repetitive EEG measurements in both a resting state and during postural balance tasks are required.21–23
The cerebellum with its distinct role in feedback-based learning could be a promising target for tDCS.8,24 The cerebellum is involved in motor adaptation via long-term depression-like plasticity of Purkinje cells mediated by activation of predominantly climbing fibers.25–27 Via cortico-cerebellar connections, it is involved in optimization of timing of movements by comparing a copy of efferent and afferent information, which may be enhanced by tDCS.28–31 From a detailed anisotropic head model study a known optimal configuration to apply cerebellar tDCS (cb_tDCS) is available. 32
We recently found an instantaneous positive effect of a postural feedback-based tracking task combined with anodal cb_tDCS on standing balance performance in a small group of patients with a chronic stroke (N = 15) when stimulated on the ipsi-lesional cerebellar hemisphere as compared to sham. 33 Moreover, it has been proposed that anodal cb_tDCS may counteract the effect of crossed cerebellar diaschisis, which induces a disbalance in cerebellar brain inhibition by a decrease in activity of Purkinje cells. 34 Anodal cb_tDCS might positively interfere with this process when applied early.34,35
“POstural feedback ThErapy combined with Non-invasive TranscranIAL direct current stimulation in patients with stroke” (POTENTIAL) aims to establish whether virtual reality-based postural feedback training (VR-PFT) combined with anodal cb_tDCS is more effective than VR-PFT with sham cb_tDCS in improving standing balance, starting within five weeks post-stroke. Clinical measurements are needed to establish the clinical relevance of cb_tDCS, while posturographical and neurophysiological measurements are required to gain understanding into underlying mechanisms of standing balance performance and recovery post-stroke. 36 We hypothesize that: patients receiving VR-PFT+cb_tDCS will show a clinically meaningful improvement of 6 points or more on the Berg Balance Scale (BBS) at 15 weeks post-stroke when compared to patients receiving VR-PFT + sham. A significantly larger decrease over time in center of pressure (CoP) parameters is expected after VR-PFT+cb_tDCS as compared to VR-PFT+sham. We also hypothesize that these posturographical improvements will be accompanied by neurophysiological changes evident in normalization in EEG-based theta and alpha power spectral density and cortical asymmetries between hemispheres.
Methods
Study design
POTENTIAL is a double-blind randomized controlled trial, with 15 intervention sessions of 1 h during three weeks and a follow-up period until 15 weeks post-stroke. Forty-six patients with a first-ever ischemic stroke will be enrolled within five weeks post-stroke. The study has been approved by the local Medical ethical committee (NL52021.029.15), is registered in the Dutch trial register (NTR5261) and designed according to the criteria of the CONSORT 2010 statement.
37
A flowchart of the study procedures can be found in Figure 1.
Flowchart of the patient inclusion and study procedures. BBS: Berg Balance Scale; MMSE: Mini Mental State Examination; HADS: Depression Scale.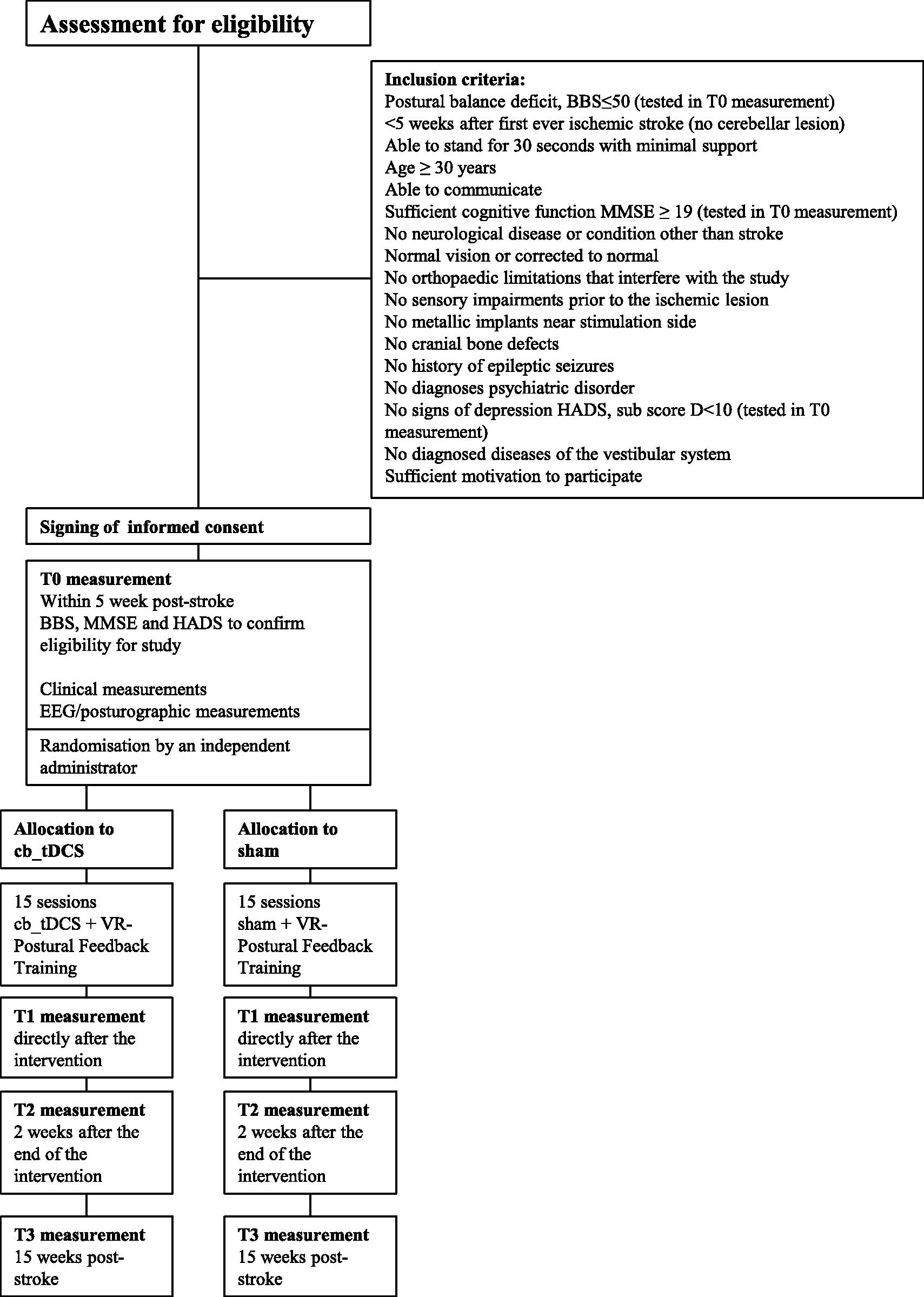
Patient population
Inclusion criteria are displayed in Figure 1.
Randomization and blinding procedure
Patient, assessors, and therapists will be blinded to treatment allocation. Block randomization per participating center with blocks of six (last block of four) will be used. Concealed allocation will be effectuated with an online randomization tool (Julius Center, Utrecht, The Netherlands) performed by an independent administrator who will convey the randomization into the tDCS software per patient. The group allocation is secured by a code only known to the independent administrator.
Intervention
Training and measurements will take place at the rehabilitation facility where patients reside or receive outpatient therapy. Fifteen VR-PFT sessions, applied five days per week for 1 h will be started within five weeks post-stroke, in addition to usual care. Subjects will be randomized by an independent administrator, into either VR-PFT plus active cb_tDCS (N = 23) or VR-PFT plus sham (N = 23). VR-PFT will be given by trained physical therapists on a balance workstation (Motek, Amsterdam, The Netherlands). The balance workstation consists of a customized software setup with a computer and 42 inch flat screen TV on a frame. VR software applications will be implemented in which visual feedback is given regarding center of gravity or trunk movements during several tasks requiring active control of posture and balance in a virtual environment (D-flow, Motek, Amsterdam, The Netherlands), see Supplementary Table 1.
Cb_tDCS application
tDCS will be applied starting 5 min before and during the first 20 min of each training session. The stimulation will be delivered by a portable stimulator (Starstim®, Neuroelectrics, Barcelona, Spain) through a pair of 3.14 cm2 electrodes filled with a conducting gel, see Figure 2.
Head cap with portable wireless tDCS stimulator.
The anodal electrode will be placed 3 cm lateral of the inion towards the affected leg side, the cathodal electrode over the buccinator muscle. A 1.5 mA constant current will be applied in the cb_tDCS-group for 25 min with a ramp up and down phase of 30 s. The sham-group will receive a 0.5 mA ramp up of 30 s followed by a ramp down of 30 s, 24 min of 0 mA current ending with a 0.5 mA ramp up of 30 s and a ramp down of 30 s. Sham stimulation is a common procedure in tDCS research as an effective and reliable blinding method. 38
Measurement outline
Assessments will be carried out prior to treatment allocation (baseline assessment, T0) as well directly after the intervention (T1), repeated two weeks after the end of the intervention (T2) and at 15 weeks post-stroke (T3). The clinical measures are performed by the researchers according to recommended guidelines 39 covering the three domains of the International Classification of Functioning, Disability and Health (ICF). 40
Primary outcome measure
The main outcome parameter is the BBS, which assesses balance performance and consists of 14 test items in which the patient is asked to maintain a number of standing positions and to perform a number of balance tasks of increasing difficulty. The test is reliable and valid in stroke patients. 41 A 6-points change is considered a clinical relevant difference. 42
Secondary outcome measures
The secondary measures performed are: Fugl-Meyer Motor Scale lower extremity, 43 Motricity Index arm and leg, 44 Erasmus modifications to the Nottingham Sensory Assessment of both legs, 45 Fall history, 10-m walk test, 46 Falls Efficacy Scale, 47 Nottingham Extended Activities of Daily Living, 48 and Stroke Impact Scale version 3.0. 49
Patient descriptors: age, date of stroke, affected side, Bamford classification, comorbidities, handedness, and smoking habits will be recorded at T0.
Posturographic assessment
Ground reaction forces will be measured to assess standing balance performance, see Figure 3 for the complete setup. A monitor providing VF is positioned at eye-height in front of two force platforms, one foot positioned on each plate (Motek, Amsterdam, The Netherlands).
Balance workstation with double force platforms, visual feedback with concurrent EEG.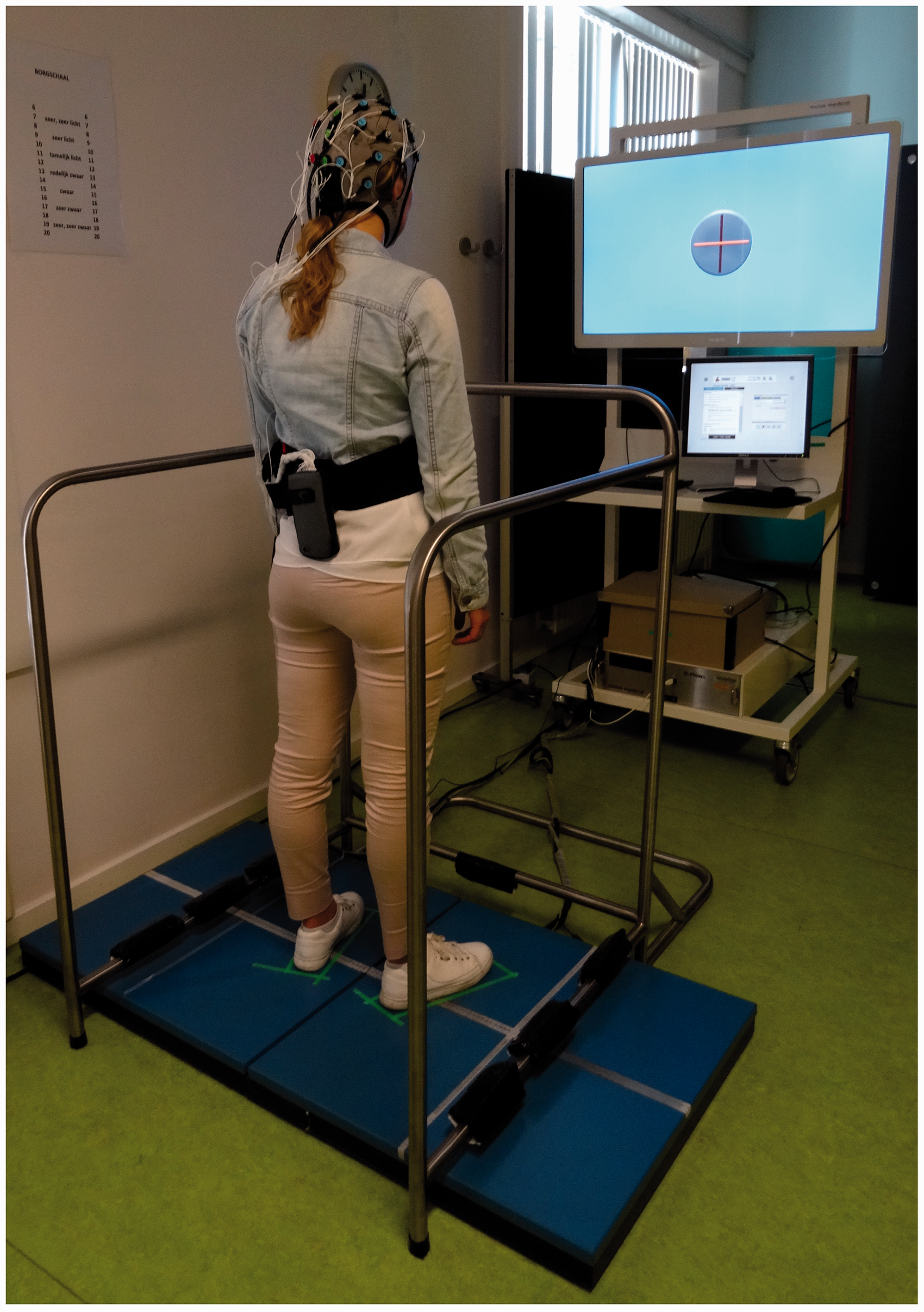
The following conditions will be tested:
Sit eyes open: to obtain the resting state activity of the brain, four times 60 s of EEG will be recorded while the patient is seated and is asked to look at a dot in front of him/her. Two minutes will be recorded at the beginning and 2 min at the end of the session. Quiet stance eyes-open/ eyes-closed: the patient will be asked to stand on the force platforms. Five trials with eyes open and five trials with eyes closed will be recorded for 60 s. Tandem stance: the patient is asked, to hold the most difficult position that is feasible to perform for minimally 30 s. Five trials will be performed. Anterior-posterior and medio-lateral limits of stability: the patient is asked to shift his/hers CoP forward-backward and sideways as much as possible shown by a moving dot on a video screen while maintaining the same foot position.
Posturographic outcome measures
CoP time series will be used to calculate qualitative measures of standing balance performance. For the quiet stance conditions we will determine: mean amplitude, amplitude variability, range, velocity, variability of the velocity and a composite-score of the above-mentioned parameters representing standing balance performance.33,50 The anterior-posterior and medio-lateral limits will be used to determine the area of the patients limits of stability.
Neurophysiological assessment and outcome measures
During the quiet stance conditions and sitting task, 32-channel EEG will be recorded. Electrodes will be placed onto the skull using a head cap according to the international 10-20 system (TMSI International, Enschede, The Netherlands). Line noise will be reduced via bandpass filters and artefacts will be removed by an independent component analysis approach. 51 The Fieldtrip toolbox for MEG and EEG analysis will serve to estimate power spectral densities. 52 Spectral power in the theta band (4–7 Hz), alpha band (7.5–12.5 Hz), and the beta band (12.5–30 Hz) will be calculated. Asymmetry between hemispheres will be quantified with the Brain Symmetry Index.19,53
Sample size calculation
Sample size of this phase II study was calculated using a two-sided alpha of 0.2 with a power of 80% to correctly identify a potentially beneficial intervention.54,55
Previous studies among (sub)acute ischemic stroke patients have reported BBS values with a mean of (M):10, standard deviation (SD):1056 and median (med):12, interquartile range (IQR):2–22. 57 VR-PFT+cb_tDCS provides benefit over VR-PFT if the improvement on the BBS over time is 6 points larger at 15 weeks post-stroke. 42 In order to find a 6-points difference in improvement, with a SD of 11, 19 patients per group are needed. Using a 15% inflation to allow for non-parametric testing, and allow for a 10% loss to follow-up, we will need to enroll 23 patients per group.
Statistical analysis
The BBS as the main outcome parameter of this study will be analyzed with a Mann-Whitney U test to establish a possible difference between the cb_tDCS and the sham group. The null hypothesis will be rejected if the cb_tDCS group shows a larger increase in BBS score between T0 and T3, as compared to the sham group with a probability value lower than 0.05. The difference between the groups need to be 6 points or larger to be clinically meaningful.
Secondary outcome measures will be analyzed using a mixed-model approach to establish statistical differences over time and between stimulation groups. This model will include factor time (T0, T1, T2, T3) and stimulation group (cb_tDCS versus sham) for which T0 and sham will be used as contrast. The distribution of the data or residuals of the models will be tested for normality using the Shapiro–Wilk test and by visual inspection of the histogram when appropriate. When normality of the residual is not met or in case of ordinal data and transformation to meet these criteria do not apply, a non-parametric equivalent will be used. The null hypothesis will be rejected if the corresponding probability value in the cb_tDCS group in measurement T3 is lower than 0.05 for the BBS as the main outcome parameter of this study.
Study organization and funding
Patients will be included in Reade rehabilitation centre Amsterdam and Vogellanden rehabilitation centre Zwolle, the Netherlands. Research coordination and analyses will be conducted at Amsterdam UMC. The study is funded by the Brain Foundation of the Netherlands.
Discussion
This trial will contribute to further understanding of underlying post-stroke recovery processes and whether these can be influenced by tDCS. Thereby it will add to a current lack of translational models of preclinical to human studies which are needed for instance to explain the large individual variability previously observed in tDCS studies.33,58,59 As has been recommended by the series of rehabilitation roundtable papers of the leading experts in the field, we will combine clinical, posturographical and neurophysiological measurements, and conduct the follow-up measurement at a fixed time point to enhance understanding of post-stroke recovery.21,22,60–63
Summary and conclusions
This proof of concept double blind, sham controlled trial will show whether VR-PFT combined with anodal cb_tDCS is more effective than VR-PFT with sham in improving standing balance, measured with the BBS, started within the critical time window for homeostatic neuroplasticity within five weeks post-stroke.
Supplemental Material
Supplemental material for The effect of cerebellar transcranial direct current stimulation to improve standing balance performance early post-stroke, study protocol of a randomized controlled trial
Supplemental Material for The effect of cerebellar transcranial direct current stimulation to improve standing balance performance early post-stroke, study protocol of a randomized controlled trial by Sarah B Zandvliet, Carel GM Meskers, Rinske HM Nijland, Andreas Daffertshofer, Gert Kwakkel and Erwin EH van Wegen in International Journal of Stroke
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: a fellowship of the Brain Foundation of the Netherlands (Hersenstichting), awarded to Dr EEH van Wegen. Grant no: F2013(1)-41.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.