
Abstract
Background and purpose:
To evaluate the association of genetic liability to migraine with functional outcome after ischemic stroke using Mendelian randomization.
Methods:
Genetic proxies for migraine were obtained from the largest genome-wide association study meta-analysis of 102,084 migraine cases and 771,257 controls. Genetic associations with functional outcome after ischemic stroke were obtained from the Genetics of Ischemic Stroke Functional Outcome network study (N = 6021). Poor functional outcome after ischemic stroke was defined as a score of 3–6 on the modified Rankin scale at 3 months (N = 2280). The inverse-variance weighted method was used to estimate the association of genetic liability to migraine with functional outcome, and we performed sensitivity analyses to assess the robustness of results.
Results:
Genetic liability to migraine was associated with poor functional outcome after ischemic stroke (odds ratio of poor functional outcome per doubling in migraine odds 1.22, 95% confidence interval 1.02–1.45, p = 0.031). This association remained directionally consistent across sensitivity analyses.
Conclusions:
This study provides genetic support that migraine is associated with poor functional outcome after ischemic stroke. These findings warrant further follow-up and, if replicated, may have clinical implications for post-stroke recovery.
Introduction
Migraine is a primary headache disorder that affects up to 20% of the population worldwide and is ranked as the second most common cause of disability globally.1,2 A meta-analysis of prospective cohort studies showed that migraine was associated with increased risk of ischemic stroke. 3 However, few studies have investigated the association of migraine with post-stroke outcome.4,5 Establishing causality between liability to migraine and post-stroke outcome could have significant clinical implications, with a positive association suggesting that migraine treatment may improve post-stroke recovery.
Mendelian randomization (MR) is a statistical method that utilizes genetic variants robustly related to exposures to examine causal effects of the exposure on outcomes.6,7 With available genome-wide association study (GWAS) data for migraine and post-stroke outcome,8,9 MR provides an opportunity to evaluate the causal effect of migraine on post-stroke outcome. Thus, we conducted this two-sample MR study to test the effect of genetic liability to migraine on functional outcome after ischemic stroke. We hypothesized that genetic liability to migraine would associate with poor functional outcome after ischemic stroke.
Methods
Study design
We performed a two-sample MR analysis, which leverages summary statistics for migraine (exposure) and functional outcome after ischemic stroke (outcome) obtained from two independent, non-overlapping populations. Analyses were restricted to individuals of European descent to reduce bias owing to population stratification.
Genetic proxies for migraine
Genetic proxies for migraine were obtained from the largest GWAS meta-analysis of 102,084 migraine cases and 771,257 controls. 8 This GWAS meta-analysis included five study collections: IHGC2016 (International Headache Genetics Consortium) without 23andMe, 23andMe, UK Biobank, GeneRIS, and HUNT (Nord-Trøndelag Health Study). 8 These cohorts included a mixture of self-reported cases as well as cases that were clinically diagnosed using The International Classification of Headache Disorders (ICHD) criteria (the IHGC2016 and HUNT cohorts). 8 Prior investigations have found that self-reported migraine has a high sensitivity and specificity for clinically diagnosed migraine, thus supporting the combination of the two ascertainment methods in one genetic sample. 10 This GWAS was adjusted for sex, age and population structure. There were 121 autosomal lead variants showing significant associations with migraine in this meta-analysis (p < 5 × 10−8). We clumped these 121 variants for independence based on the 1000 Genomes European samples data and identified 100 independent (r2 < 0.001; 10,000 kb window) variants associated with migraine. We identified 9 of 100 migraine-associated variants to be associated with smoking initiation or insomnia (p < 0.05/100),11,12 two risk factors for post-stroke outcome identified in previous MR studies.13,14 After removing these nine potentially pleiotropic variants, we used the remaining 91 genetic variants in MR analyses (Supplemental Table 1). In addition, we also evaluated the association of different migraine subtypes (migraine with aura (4 SNPs) and migraine without aura (15 SNPs)) with post-stroke outcome.
Outcome data
The primary outcome was poor functional outcome after ischemic stroke, defined as a modified Rankin scale (mRS) score of 3–6 (range, 0 (no symptoms) to 6 (death)), at 3 months after stroke onset. 9 GWAS summary statistics for post-stroke outcome were obtained from the Genetics of Ischaemic Stroke Functional Outcome (GISCOME) network which included 12 cohorts of European ancestry. 9 The primary analyses of mRS 3–6 (n = 2280) versus 0–2 (n = 3741) included 6021 ischemic stroke cases. Genetic associations with mRS 3–6 versus 0–2 were obtained using logistic regression with adjustment for sex, age, ancestry, and baseline NIH Stroke Scale. 9
Evaluating the association of genetic liability to migraine with risk of ischemic stroke
Collider bias is a potential source of bias that may affect MR analyses of disease prognosis. 15 To exclude this bias, we evaluated the association of genetic liability to migraine with risk of ischemic stroke. We obtained summary statistics for ischemic stroke from the GIGASTROKE consortium including 62,100 cases and 1,234,808 controls of European descent. 16 For the five instrumental SNPs that were not available in the ischemic stroke outcome dataset, we used the proxy SNPs (r2 > 0.8) to replace them. 17
Statistical analysis
MR effect estimates for individual SNPs were calculated using the Wald ratio and standard errors were approximated using the delta method. 18 We pooled individual SNP MR estimates using the random-effect inverse-variance weighted (IVW) method. 18 We assessed the heterogeneity of causal estimates using the p value for the Cochran’s Q statistic.
Four methods were performed as sensitivity analyses. The MR-Robust adjusted profile score (MR-RAPS) method can produce robust causal estimates when many weak instruments exist. 19 The weighted median estimator provides unbiased estimates even if up to 50% of the instruments are invalid. 20 The MR-Egger method can provide an unbiased estimate with adjustment for unbalanced, directional pleiotropy. 21 The intercept term estimated from the Egger method can provide a statistical test for directional pleiotropy (statistical significance set at p < 0.05). 21 Finally, MR-PRESSO (MR pleiotropy residual sum and outlier) method was used to detect, remove, and re-estimate causal effects excluding pleiotropic genetic proxies for migraine. 22 To facilitate interpretation of effect estimates, the odds ratio (ORs) with 95% confidence intervals (95% CIs) for poor functional outcome were rescaled to increase in odds of poor functional outcome per doubling odds of migraine (by multiplying betas and standard errors by the natural logarithm of 2). 23
All statistical analyses were conducted using R version 4.0.2 and the R packages TwoSample MR, 24 MendelianRandomization, 25 mr.raps, 19 and MR-PRESSO. 22
Results
In the primary analysis, genetic liability to migraine was significantly associated with poor functional outcome after ischemic stroke (mRS 3–6 vs 0–2, OR 1.22 per doubling odds of migraine, 95% CI 1.02–1.45, p = 0.031; Table 1). Results were directionally consistent using all alternative MR methods (MR-RAPS, weighted median, and MR-Egger). The scatter plot of SNP effect on migraine versus post-stroke outcome was presented in Supplemental Figure 1. We found no evidence for significant heterogeneity (p for Cochran’s Q = 0.18; Table 1), which further supports the absence of bias due to pleiotropy. Furthermore, the MR-Egger intercept indicated that there was no evidence of directional pleiotropy (p for intercept = 0.81; Table 1). In addition, no outlier SNPs were identified using the MR-PRESSO method. We found no evidence of associations between genetic liability to different migraine subtypes and post-stroke outcome, although confidence intervals were wide (Supplemental Table 2).
Mendelian randomization (MR) estimates for the association of genetic liability to migraine with 3-month functional outcome after stroke and with ischemic stroke risk.
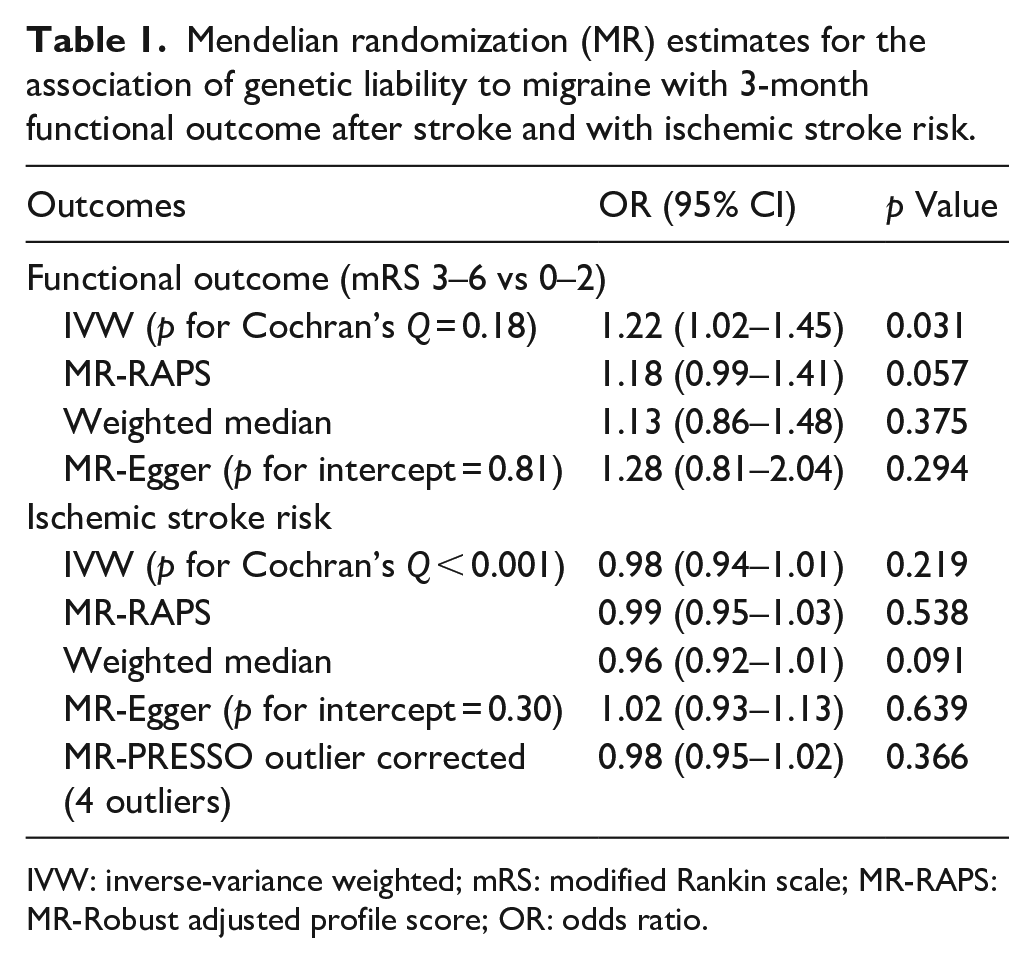
IVW: inverse-variance weighted; mRS: modified Rankin scale; MR-RAPS: MR-Robust adjusted profile score; OR: odds ratio.
Across all MR methods, we found no evidence for a causal effect of genetic liability to migraine on overall ischemic stroke risk, providing evidence to support that their association with functional outcome may not be attributed to collider bias (Table 1). There was evidence of significant heterogeneity in this analysis (p for Cochran’s Q < 0.001), however, we did not find evidence for directional pleiotropy (p for intercept = 0.30).
Discussion
To our knowledge, we performed the first MR analysis to evaluate the effect of genetic liability to migraine on functional outcome after ischemic stroke. We found that genetic liability to migraine was associated with worse post-stroke outcome. This result did not appear to be driven by collider bias or horizontal pleiotropy.
Prior observational analyses examining the association of migraine with post-stroke outcome have been inconclusive. A multicenter ischemic stroke cohort study (n = 600) did not find a significant association between migraine and poor functional outcome, albeit with wide confidence intervals (RR = 0.60; 95% CI = 0.30–1.20). 4 Another prospective multicenter study included 2492 patients with ischemic stroke was similarly inconclusive due to wide confidence intervals (RR = 1.30; 95% CI = 0.9–1.7). 5 Furthermore, findings from observational studies are potentially confounded by reverse causality and confounding. The present MR-analysis overcomes these limitations by using randomly assorted genetic variants, thereby reducing the impact of confounding and reverse causality.
The mechanisms underlying the association between migraine and post-stroke outcome remain unclear and are not informed by the present analysis. One possible mechanism is cortical spreading depolarization (SD). SDs are waves of neuronal and glial depolarization and has been implicated in the pathophysiology of migraine. 26 During cerebral ischemia, multiple SDs can lead to a reduction of cerebral blood flow and potentiate ischemic injury.27–29 In addition, SDs can initiate a cascade that disrupts the blood brain barrier, malignant edema, and increased risk for hemorrhage.26,30 In keeping with this hypothesis, mice carrying the familial hemiplegic migraine type 1 mutation had larger infarcts and worse neurological outcomes after stroke. 31
Our MR-designed investigation is less prone to bias due to confounding and reverse causality but also has limitations. First, although we found no evidence of the associations between genetic liability to different migraine subtypes and post-stroke outcome, we cannot exclude the possibility of the associations between migraine subtypes and post-stroke outcome owing to the few available variants to proxy the migraine subtypes. Second, we cannot evaluate sex-specific effects of migraine on post-stroke outcome due to no available sex-specific GWAS data for both the exposure and the outcome. Third, an important issue of MR investigations of disease prognosis is collider bias, 15 whereby the exposure (in this case, migraine) is also associated with onset of disease (in this case, ischemic stroke). To clarify the association of migraine with risk of ischemic stroke, we performed an updated MR analysis, using a larger sample size for ischemic stroke and more instrumental variables compared with three previous MR studies of migraine in relation to ischemic stroke.32–34 Consistent with the previous MR findings, we also found no significant association of migraine with risk of overall ischemic stroke (although previous studies report associations with the large artery subtype of ischemic stroke which we did not investigate), suggesting that the risk of collider bias in the present analysis is low.32–34 Fourth, we were not able to test the associations of migraine with post-stroke outcome across ischemic stroke subtypes, as the GISCOME GWAS did not have available data for functional outcome after different ischemic stroke subtypes. Finally, this study only included individuals of European ancestry which may limit the generalizability of our findings to other ancestry groups.
In summary, this MR analysis provides evidence that genetic liability to migraine is associated with worse post-stroke outcome. Future studies are warranted to replicate and confirm our findings in larger samples with different patient subgroups.
Supplemental Material
sj-docx-1-eso-10.1177_23969873231164728 – Supplemental material for Genetic liability to migraine and functional outcome after ischemic stroke
Supplemental material, sj-docx-1-eso-10.1177_23969873231164728 for Genetic liability to migraine and functional outcome after ischemic stroke by Mengmeng Wang, Iyas Daghlas, Zhizhong Zhang, Dan Ye, Shun Li and Dandan Liu in European Stroke Journal
Footnotes
Acknowledgements
The authors want to thank the GISCOME (Genetics of Ischaemic Stroke Functional Outcome) network, ISGC Cerebrovascular Disease Knowledge Portal, GIGASTROKE consortium, and GWAS catalog for making summary data publicly available.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Mengmeng Wang has received funding from Young Talent Development Plan of Changzhou Health Commission (No. CZQM2022001) and Changzhou Sci&Tech Program (Grant No. CJ20210084). Dan Ye was supported by Changzhou Sci&Tech Program (Grant No. CJ20220093).
Informed consent and ethical approval
This MR study was based on public summary data from published GWAS that had already obtained informed consent and ethical review board approvals. This study was completed in accordance with the Helsinki Declaration as revised in 2013.
Guarantor
Mengmeng Wang.
Contributorship
Mengmeng Wang, Iyas Daghlas, and Dandan Liu conceived and designed the study; Mengmeng Wang was involved in data collection, statistical analysis, and drafting the manuscript; Iyas Daghlas, Dan Ye, Shun Li, Zhizhong Zhang, and Dandan Liu revised the manuscript; Each author approved the version to be published.
Trial registration
Not applicable.
Data availability statement
This study was based on publicly available summary-level data. GWAS summary statistics for 3-month mRS after ischemic stroke were accessed through the GISCOME network and ISGC Cerebrovascular Disease Knowledge Portal. Summary statistics for overall ischemic stroke are available in the GWAS Catalog (GCST90104540). The genetic instruments for migraine are available as Supplemental Material.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.