
Abstract
Introduction:
Although stroke patients in Slovakia had been treated according to European recommendations, no network of primary and comprehensive stroke centers had been officially established; the ESO recommended quality parameters had not been fulfilled. Therefore, the Slovak Stroke Society decided to change the stroke management concept and introduced mandatory evaluation of quality parameters. This article focuses on key success factors of the change in stroke management in Slovakia and presents the 5-year results and perspectives for the future.
Material and methods:
We processed data from the stroke register at the National Health Information Center, which is mandatory in Slovakia for all hospitals designated as primary and secondary stroke care centers.
Results:
Since 2016, we have started to change stroke management. New National Guideline for Stroke Care was prepared in 2017 and published in 2018 as a Recommendation of the Ministry of Health of the Slovak Republic. The recommendation included pre-hospital as well as in-hospital stroke care, a network of primary stroke centers (hospitals administering intravenous thrombolysis – 37), and secondary stroke centers (hospitals treating with intravenous thrombolysis + endovascular treatment (ET) – 6). A stroke priority was instituted, having equally high priority as myocardial infarction. More efficient in-hospital workflow and pre-hospital patient triage shortened the time to treatment. Prenotification became mandatory in all hospitals. Non-contrast CT, and CT angiography is mandatory in all hospitals. In patients with suspected proximal large-vessel occlusion the EMS stays at the CT facility in primary stroke centers until the CT angiography is finished. If LVO is confirmed, the patient is transported to an EVT secondary stroke center by the same EMS. From 2019 all secondary stroke centers offer endovascular thrombectomy in a 24/7/365 system. We consider the introduction of quality control one of the most critical steps in stroke management. The result of these activities is 25.2% of patients treated with IVT and 10.2% by endovascular treatment, and median DNT 30 min. Number of patients screened for dysphagia increased from 26.4% in 2019 to 85.9% in 2020. In the most of the hospitals the proportion of ischemic stroke patients discharged with antiplatelets and in case of AF with anticoagulants was >85%.
Discussion:
Our results indicate that it is possible to change stroke management at a single hospital and national level. For continuous and further improvement, regular quality monitoring is necessary; therefore, the results of stroke hospital management are presented regularly once a year at national and international level. Collaboration with the “Second for Life” patient organization is very important for the “time is brain” campaign in Slovakia.
Conclusion:
Due to the change in stroke management over the last 5 years, we have reduced the time for acute stroke treatment and improved the proportion of patients with acute treatment, and in this area, we have achieved and exceeded the goals of the Stroke Action Plan for Europe for 2018–2030. Nevertheless, we still have many insufficiencies in stroke rehabilitation and post-stroke nursing that need to be addressed.
Keywords
Introduction
Stroke is a major public health issue due to its high incidence rates, high case fatality rates, residual physical and neuropsychological disability risks, and direct and indirect costs.
Therefore, the European Stroke Organisation (ESO) updated its 2008 recommendations for Stroke Management to include the establishment of primary (PCS) and comprehensive (CSC) stroke centers, recommendations for acute treatment, as well as primary and secondary stroke prevention. The MR CLEAN, SWIFT, ESCAPE, and EXTEND-1A trials published in 2015 confirmed mechanical thrombectomy’s superiority on top of thrombolysis for acute stroke treatment; this is why interventional management of stroke patients for 24 h, 7 days per week is an essential requirement for CSCs.
Although stroke patients in Slovakia had been treated according to European recommendations, no network of primary and comprehensive stroke centers had been officially established; the ESO recommended quality parameters had not been fulfilled. Therefore, the Slovak Stroke Society decided to change the stroke management concept and introduced mandatory evaluation of quality parameters. This article focuses on key success factors of the change in stroke management in Slovakia and presents the 5-year results and perspectives for the future.
Material and methods
We processed data from the stroke register at the National Health Information Center, which is mandatory in Slovakia for all hospitals designated as primary and secondary stroke care centers. The change in stroke management in Slovakia also resulted in a change in the structure of the register; thus, the parameters obtained were comparable to the quality parameters set by ESO, 1 as well as with other international registers, especially the SITS (Safe Implementation of Thrombolysis in Stroke) 2 and later the RES-Q (Registry of Stroke Care Quality) registries. 3 At the beginning of the registry in 2010, the following parameters were collected: recanalization rate, treatment time <3 and <6 h, risk factors and treatment at discharge. Since 2015 we have started to add “time data” (stroke onset, time of arrival at the hospital, time of CT examination, time of IVT, so that we can calculate onset-to-treatment time – ONT, door-to-needle time – DNT, etc.) to be compatible with the SITS register. With the introduction of the Angels (Acute Networks Striving for Excellence in Stroke) project in 2016, a healthcare initiative that supports hospitals worldwide to be “stroke-ready” in order to treat acute stroke patients based on international guidelines, we have harmonized the evaluated parameters also with Angels criteria. As ESO has endorsed this initiative, the main quality parameters are those of the ESO Action Plan for stroke 2018–2030 (% of patients treated with door to needle (DNT) <60 min, <45 min, % recanalization procedure rate out of total stroke incidence in the hospital, % of all suspected stroke patients undergoing a CT or MRI imaging procedure, % of all stroke patients undergoing dysphagia screen, % of ischemic stroke patients discharged with antiplatelets, % of atrial fibrillation related stroke patients discharged with anticoagulants, stroke patients treated in a dedicated stroke unit or an ICU during their hospital stay). 4 In 2016 was launched also The Registry of Stroke Care Quality (RES-Q) by ESO-EAST (Enhancing and Accelerating Stroke Treatment) to provide a tool for monitoring the quality of stroke care primarily at Central and Eastern Europe hospitals, but at present, RES-Q is open for users from across the world. In order to be able to compare the data from the national register with other countries, the IT experts of both registers solved the method of sending data from Slovakia to the RES-Q register. Aggregate data for the whole year from the Slovak register are sent to RES-Q once a year in March of the following year.
Results
Organization
Since 2016, we have started to change stroke management. After many discussions, a new National Guideline for Stroke Care was prepared in 2017 and published in 2018 as a Recommendation of the Ministry of Health of the Slovak Republic, according to § 45 par. 1 letter (b) of Act No. 576/2004 Coll. On Health Care, Health Care-related Services, and amendments to certain acts. 5 The recommendation included pre-hospital as well as in-hospital stroke care, a network of primary stroke centers (hospitals administering only intravenous thrombolysis – 37), and secondary stroke centers (hospitals treating with intravenous thrombolysis + endovascular treatment (ET) – 6) (Figure 1).
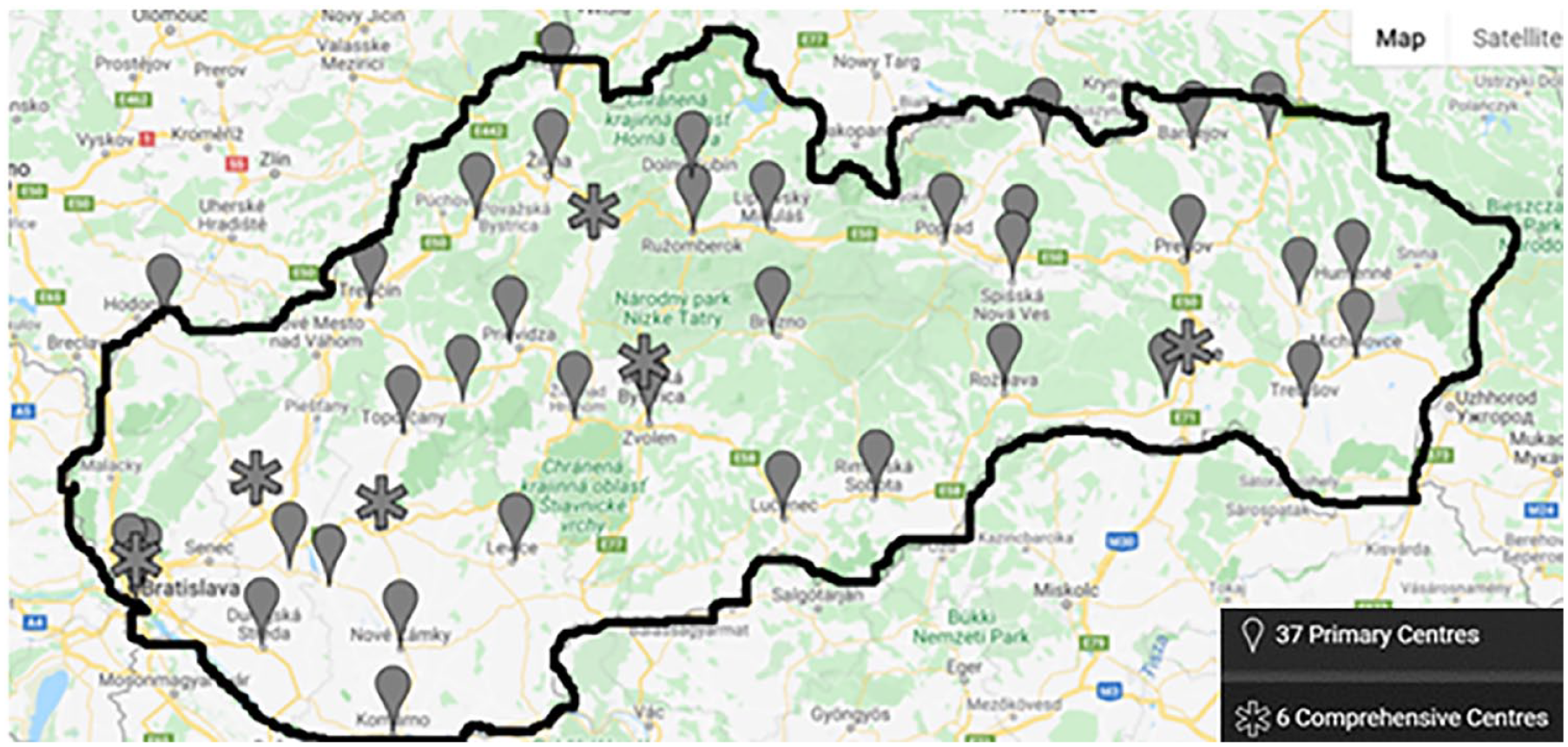
Primary stroke centers (centers for IVT) and secondary stroke centers (centers for IVT and ET).
Management
We started with systematic education of emergency call centers and emergency medical services (EMS). A stroke priority was instituted, having equally high priority as myocardial infarction. More efficient in-hospital workflow and pre-hospital patient triage shortened the time to treatment. This increased the proportion of eligible patients for specialized treatments limited by the strict therapeutic window. In the beginning, we prepared a “stroke-card” with all critical information in collaboration with EMS. Part of the card was the G-FAST score, a pre-hospital scheme for identifying stroke symptoms, and in all hospitals, we started to use “stroke mobile phones” for prenotification. Later, a smartphone application was developed (Figure 2), and prenotification became mandatory in all hospitals. The application prenotification includes all important data from the patient’s history, so a patient’s data can be entered into the hospital information system before arrival. Part of pre-hospital management was also a change of the patient’s delivery to the hospital. Before, the EMS used to bring patients to an emergency department or neurology department. The delivery of a stroke patient directly to CT became the standard in most hospitals. The only problem with the application is that due to the GDPR (General Data Protection Regulation), the patient identification data cannot be entered into the application. Still, the doctor must call the EMS crew during transport to the treating hospital so it does not affect the overall transport time. The application enables the GPS location of the ambulance to be monitored so that the stroke team can prepare for the arrival of the patient accordingly. The application is also used in communication between primary and secondary centers.
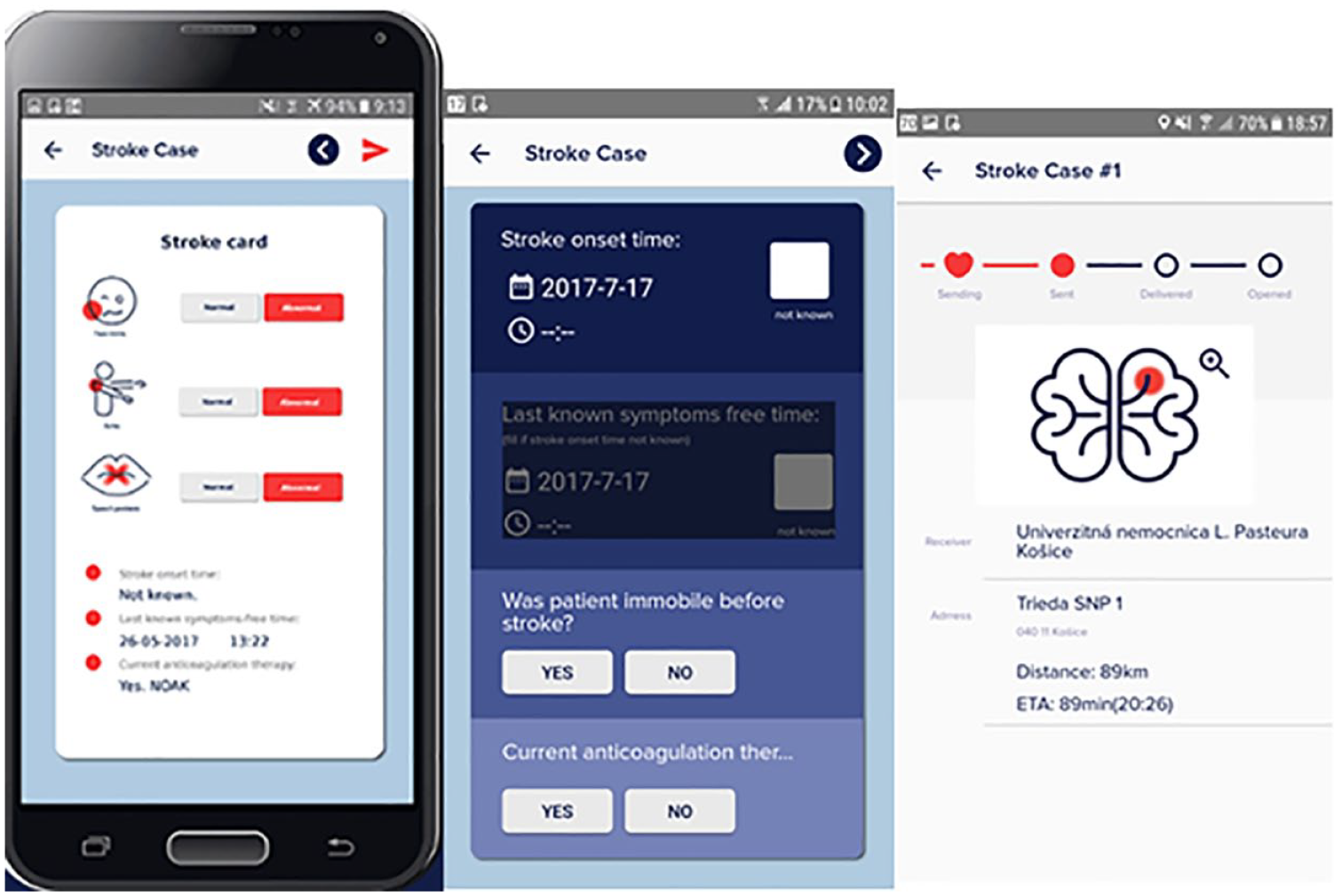
Application for stroke prenotification.
The neurologist does a physical examination, history data check before non-contrast CT, and CT angiography is mandatory in all hospitals. A radiologist and neurologist immediately interpret the CT. If the patient meets the criteria for thrombolysis, the alteplase bolus is administered on the CT table, and then IVT continues, or it starts at the stroke unit when the distance is very short.
Blood samples are drawn from all patients; the only laboratory tests affecting treatment decisions are blood glucose and coagulation status in patients on anticoagulants.
In patients with a confirmed proximal large-vessel occlusion (LVO), interventional radiology is activated immediately and thrombectomy starts as soon as possible. The EMS stays at the CT facility in primary stroke centers until the CT angiography is finished. If LVO is confirmed, the patient is transported to an EVT secondary stroke center by the same EMS. This shortens the onset to recanalization time (door-to-groin puncture time). From 2019 all secondary stroke centers offer endovascular treatment in a 24/7/365 system.
Quality control
We consider the introduction of quality control one of the most critical steps in stroke management. Outcomes and performance of individual centers are presented at various cerebrovascular seminars and conferences. This regular benchmarking creates an opportunity for the members of the stroke team to improve treatment processes internally by comparing their performances and/or externally with other teams. These results are also sent once a year to hospital directors and presented to the public over the last 3 years.
The percentage of patients treated with IVT is commonly used in the literature to document improved evidence-based care processes for patients with stroke. The rising numbers of patients treated with IVT and MT and DNT shortening (Figures 3 and 4) confirm that the quality of care has improved significantly since 2018. The recommended door-to-needle time in literature is below 1 h. In Slovakia, quality indicators from RES-Q show that in all 43 hospitals, more than 75% of patients had a DNT <60 min, and in 42 hospitals, more than 50% of patients had a DNT <45 min; some hospitals even achieved a DNT <20 min and median DNT in 2021 was 30 min. After achieving a higher proportion of patients treated with endovascular treatment, we focused on reducing the time to the start of endovascular treatment (door-to-groin puncture time). In 2020 the percentage of patients treated with a door-to-groin time <120 min was more than 75% in 38 primary hospitals (door here means the door of the primary care center).
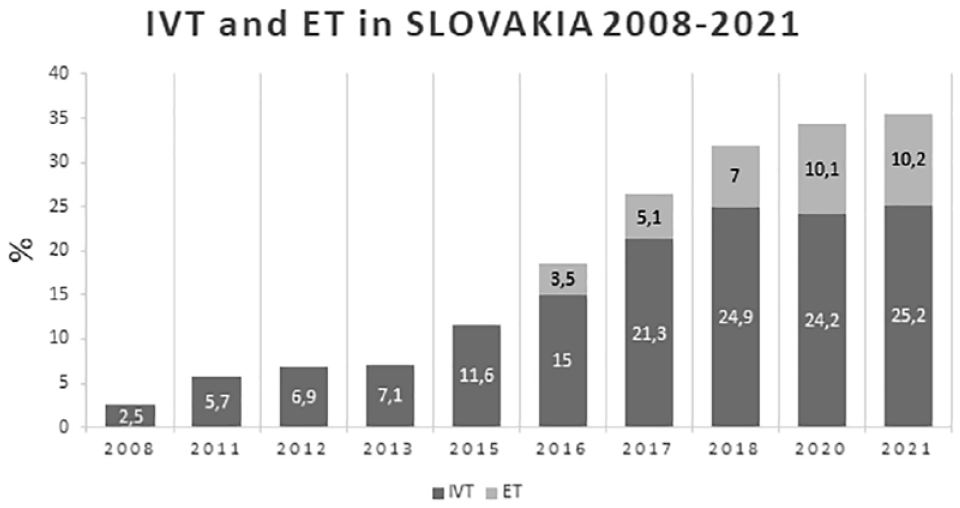
IVT: intravenous thrombolysis; ET: endovascular treatment.
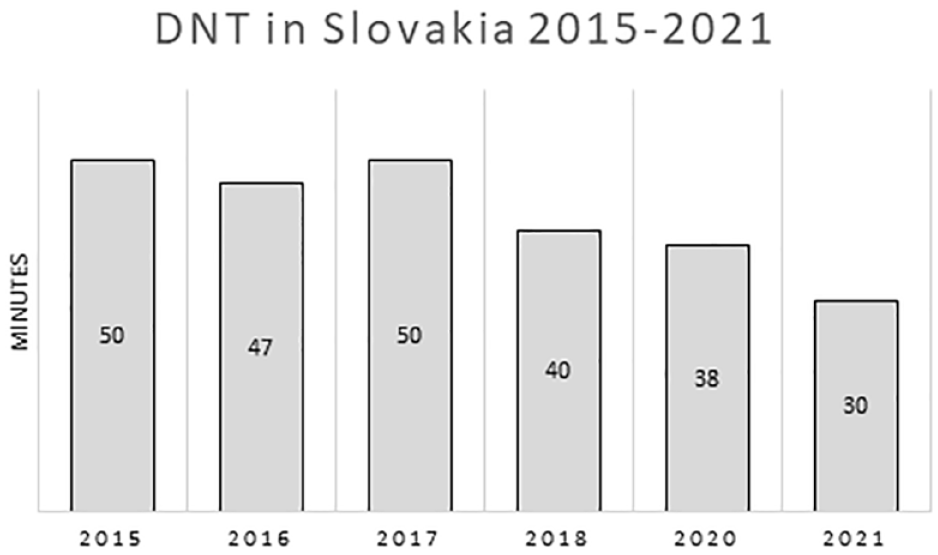
Door-to-needle time (DNT) and *DNT was not calculated before 2015.
The advantage of the mandatory stroke register is that every year we have quality data from all 43 hospitals with stroke for the entire previous year.
Other quality parameters are evaluated in the structure required by the ESO only in recent years in collaboration with the ESO Angels Initiative. Based on the agreement, we then send them to the RES-Q register in March for international comparison. While in 2019, the proportion of all stroke patients undergoing dysphagia screening was 26.4%, in 2020, after educational training of nurses organized by the Angels, this was 85.9%. In 36 out of 43 hospitals, the proportion of ischemic stroke patients discharged with antiplatelets was >85%. In 40 hospitals, the proportion of atrial fibrillation-related stroke patients discharged with anticoagulants was >85%, and in 29 of them >90%. In total, 58% of stroke patients are treated in a dedicated stroke unit. Most of the remaining stroke patients with acute stroke are treated in multidisciplinary intensive care units, where not only stroke patients are hospitalized. The most important procedures for improving stroke care in Slovakia are shown in Figure 5.
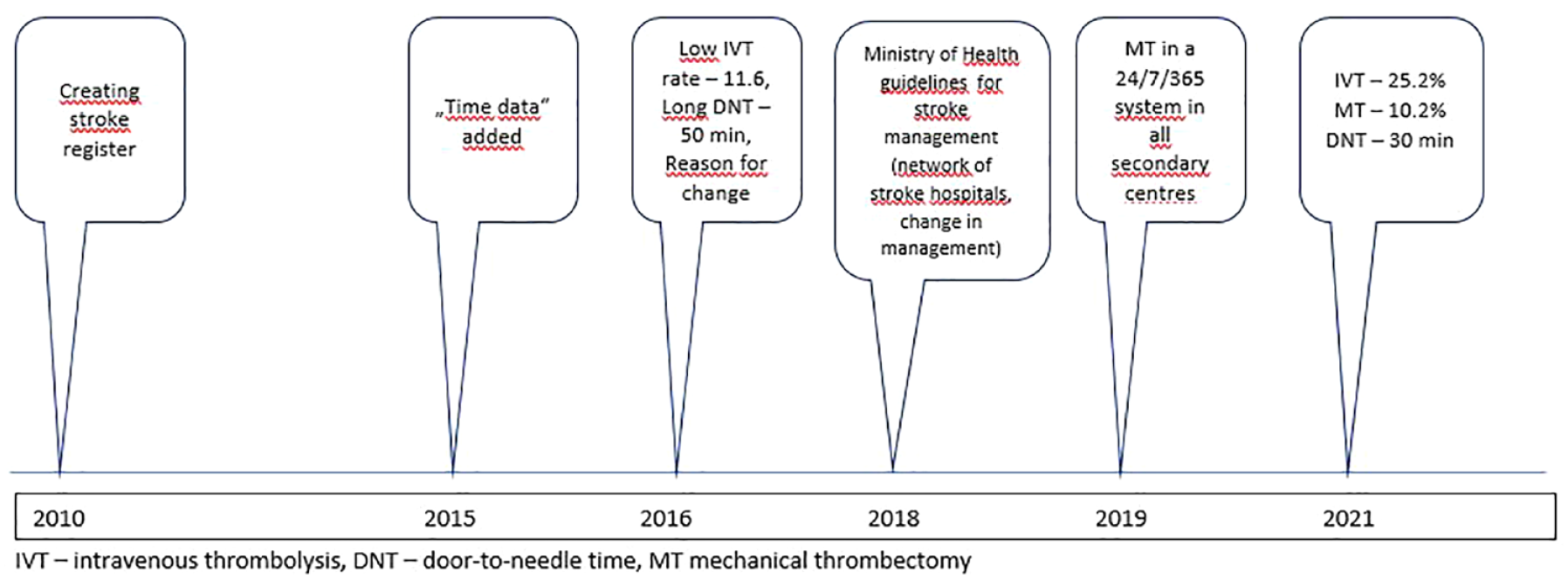
The most important procedures for improving stroke care in Slovakia.
Education and collaboration with the Angels Initiative
To expand knowledge to the nurses and raise motivation, the Angels Initiative supported educational training courses for nurses, with the topics of early rehabilitation, positioning, and the psychological aspect of working with stroke patients and their relatives.
The international Angels Initiative improved the education of emergency services in Slovakia, providing training courses in pre-hospital management on the national and regional levels and implementing quality monitoring in pre-hospital stroke care by involving the EMS providers in the EMS Angels Awards program, which is based on data collection and enables the acknowledgment of the best performing pre-hospital stroke care providers.
The Angels Initiative and the patients’ association implemented in the country the Fast Heroes campaign supported by the World Stroke Organization (WSO), which aims to raise awareness of key stroke symptoms among children, encouraging them to share the knowledge with their relatives. In the first year of the Fast Heroes campaign in Slovakia, 143 schools with more than 5500 children were enrolled, and 300 teachers were involved. As a result, 90% of parents expressed higher confidence about what to do if somebody has a stroke.
Discussion
Our results indicate that it is possible to change stroke management (reduce DTN time for thrombolysis, increase the proportion of patients treated by thrombolysis and thrombectomy) at a single hospital and national level.
Previous unsatisfactory results, especially the low rate of recanalization and longer time to treatment in patients with acute stroke, led the Slovak Stroke Society to change the management of stroke.
Implementing the changes was not easy. Most of the changes were achieved thanks to the enthusiasm of doctors, nurses, paramedics, and emergency services, without significant support from state authorities or the Ministry of Health. Engagement was identified as a key facilitator for improving stroke care, and the Slovak Stroke Society has developed a network of hospitals for primary and secondary stroke care. Still, it took 2 years to be officially recognized by the Ministry of Health, together with National Guideline for Stroke Care.
Creating a network of stroke centers was crucial to improving cooperation with emergency services so that crews could transport patients directly to a stroke-ready hospital. The second key moment was the introduction of prenotification, which made it possible to obtain essential data about a patient before his or her arrival at the hospital and to enter a patient’s individual data into the hospital information system. We relied on proven procedures, such as the Helsinki6,7 or Czech model of stroke care, 8 such as cooperation with the emergency medical service, prenotification, hospital stroke team education and achieving CT priority.
It was challenging to convince radiologist that each stroke patient requires non-contrast CT and CT angiography. Nowadays, we are in the process of explaining the need for CT perfusion to extend the window for IVT and/or EVT. The administration of alteplase bolus on the CT table reduced the DNT, especially during regular working hours. Before becoming a routine action, it had been topic of repeated discussions with CT staff and nurses.
Despite all our activities, seminars, and lectures at conferences, reducing the door-to-needle time and increasing the rate of intravenous thrombolysis to the required level was achieved only in some hospitals, and significant inter-hospital differences persisted. And far too many stroke patients still arrive to hospitals outside of the time window for acute treatment.
We presented data on the differences between hospitals at professional events, but this did not significantly improve either management or data entry, which was still insufficient in some hospitals. In cooperation with the patient organization “Second for Life,” the situation changed when we began to present the register results at press conferences. Since then, data entry has improved, which was impossible several years before. At the same time, hospitals have begun to address their internal problems in stroke management.
For continuous and further improvement, regular quality monitoring is necessary; therefore, the results of stroke hospital management are presented regularly once a year. At the same time, they are entered into the international register for comparing the quality of management at the international level. Slovakia has become part of the ESO Angels initiative, which aims to increase the number of patients treated in stroke-ready hospitals and optimize the quality of treatment in all existing stroke centers. To date, each hospital in Slovakia has received at least the ESO Angels gold award, and many have repeatedly won the highest diamond award.
In the future, we would like to improve the quality and accuracy of the collected data, so we are working to ensure that the data is transferred directly from the structured discharge report, thus ensuring that really all patients are reported and reducing the error rate that can always be present at rewriting the data in the register. The program is already ready and the Ministry of Health has promised to support this project.
The achievement of a structured organization of acute stroke management was confirmed during the Covid-19 pandemic. During the first wave, when Slovakia had a low incidence of Covid-19, as well as during the second wave when Slovakia was among the countries in the world with the highest incidence of Covid-19, the acute stroke management stroke did not differ.9,10
The challenges of pre-hospital stroke management can be divided into two main groups: the patients themselves and their families and the emergency medical services team. Cooperation with EMS has improved significantly; therefore, we decided to spread knowledge of stroke among the population. Stroke educational campaigns were one solution for improving patients’ and families’ awareness of stroke symptoms and the correct response in the case of stroke. We started the “time is brain” campaign, which is well known in other countries, collaborating with the “Second for Life” patient organization. However, such campaigns have been shown to have a short-term impact, and constant repetition of their message is a central precondition for their success. After each campaign, we registered a higher number of patients who arrived on time; therefore, public education efforts are worthwhile, and future efforts should focus more strongly on specific target groups, such as the elderly, minorities, neighbors, people who have survived a stroke, medical students and even children (who may be future relatives, patients, or doctors). Finally, the previously mentioned Angels Initiative was implemented.
In acute care, we have already achieved and exceeded the quality parameters set by the Stroke Action Plan for 2018–2030. 4 Nevertheless, even in acute care, it is necessary to improve the technical and personnel equipment, which we are trying to address with the Ministry of Health in the ongoing health care reform.
In the Helsingborg Declaration of 2006, the goal for 2015 was that all stroke patients in Europe would have access to a continuum of care, from acute management to appropriate rehabilitation, delivered in dedicated stroke units. The Action Plan for 2018–2030 for Rehabilitation includes occupational, physical, and speech and language therapy, with input from psychologists and social workers. This should involve a multidisciplinary approach in a comprehensive stroke team and an ordered plan after discharge from the hospital, with documented responsibility for continuing rehabilitation needs in the community. In this area, we still have many deficiencies, and the improvement of rehabilitation and post-stroke care in all its areas is the subject of the ongoing health care reform. 4
The strengths of the presented results are (1) that we have achieved changes throughout Slovakia in all stroke hospitals, (2) there is now a mandatory stroke register in Slovakia, and as a result, we have available data on monitored quality parameters for all hospitals, and (3) data from our register are compatible with the international register.
A limitation of the presented study is the quality of the registry data since the stroke physicians themselves enter all the data in addition to their working duties, which may result in inaccuracies. Our goal is to automatically transfer the data from patient records in the hospital information system into the registry.
Conclusion
Due to the change in stroke management over the last 5 years, we have reduced the time for acute stroke treatment and improved the proportion of patients with acute treatment, and in this area, we have achieved and exceeded the goals of the Stroke Action Plan for Europe for 2018–2030. Nevertheless, we still have many insufficiencies in stroke rehabilitation and post-stroke nursing that need to be addressed.
Supplemental Material
sj-tiff-1-eso-10.1177_23969873221115457 – Supplemental material for How stroke care has changed in Slovakia in the last 5 years
Supplemental material, sj-tiff-1-eso-10.1177_23969873221115457 for How stroke care has changed in Slovakia in the last 5 years by Zuzana Gdovinova, Michal Kovačik and Diana Urbani in European Stroke Journal
Supplemental Material
sj-tiff-2-eso-10.1177_23969873221115457 – Supplemental material for How stroke care has changed in Slovakia in the last 5 years
Supplemental material, sj-tiff-2-eso-10.1177_23969873221115457 for How stroke care has changed in Slovakia in the last 5 years by Zuzana Gdovinova, Michal Kovačik and Diana Urbani in European Stroke Journal
Supplemental Material
sj-tiff-3-eso-10.1177_23969873221115457 – Supplemental material for How stroke care has changed in Slovakia in the last 5 years
Supplemental material, sj-tiff-3-eso-10.1177_23969873221115457 for How stroke care has changed in Slovakia in the last 5 years by Zuzana Gdovinova, Michal Kovačik and Diana Urbani in European Stroke Journal
Supplemental Material
sj-tiff-4-eso-10.1177_23969873221115457 – Supplemental material for How stroke care has changed in Slovakia in the last 5 years
Supplemental material, sj-tiff-4-eso-10.1177_23969873221115457 for How stroke care has changed in Slovakia in the last 5 years by Zuzana Gdovinova, Michal Kovačik and Diana Urbani in European Stroke Journal
Footnotes
Acknowledgements
Acknowledgments belong to all doctors and nurses who take part in the care of stroke patients in Slovakia and who give data to the stroke register. Our thanks belong to Dr. A. Barakova, MD and Dr. A. Cvopová, MD for keeping the stroke register and data processing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The ethics committee of Faculty of Medicine P. J. Safarik University approved using data from stroke registry.
Informed consent
Informed consent was not required. Anonymized data from the mandatory stroke register were used.
Guarantor
ZG.
Contributorship
ZG and MK researched literature and conceived the study, ZG processed data from the register, ZG and MK described the development of stroke care in Slovakia, DU documented the activities of the Angels initiative. ZG wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.