
Abstract
Introduction:
The aim of our study was to determine whether the severity of the COVID-19 pandemic affected the quality of acute care of stroke.
Methods:
Data from the stroke register at the National Health Information Centre were analysed. Clinical data from two time periods (the first wave: March–April 2020; the second wave: October–November 2020) were compared using an independent sample t-test and the Wilcoxon-Mann-Whitney two sample rank-sum test.
Results:
The total number of patients admitted with stroke during the second wave of COVID-19 was 1848, versus 1698 in the first wave. The proportion of patients treated by IVT was similar in both waves (275 (20.7%) vs 333 (22.1%), p = 1, difference in location: −0,0003, 95% CI: −5.0 to 5.95). We found no difference in time from the onset of symptoms to treatment (median = 130 min in both waves, p = 0.52, difference in location: 3.99, 95% CI: −6.0 to 14.0), nor in the door-to-needle time (median = 29 vs 30 min, p = 0.08, difference in location: −2.99, 95% CI: −5.0 to 0.008) between the first and the second waves of the pandemic. We found no difference in NIHSS (median = 3 vs 4, p = 0.51, difference in location: 0.00007, 95% CI: −0.9 to 0.000006) and mRS (median = 3 in both waves, p = 0.60, difference in location: −0.00004, 95% CI: −0.00004 to 0.00003) at discharge from hospital between the two periods.
Conclusion:
The severity of the COVID-19 outbreak did not affect the quality of acute stroke care in Slovakia.
Introduction
Since the onset of the COVID-19 pandemic, several groups have reported a decreased number of patients admitted to hospital with acute ischaemic stroke.1–4 Most of them collected information from a single clinical site or from a larger region,1,2,5,6 but the findings from country-level data are scarce. Thanks to the mandatory stroke register for all 43 hospitals included in the network for acute stroke treatment in Slovakia, we were able to perform a national, multi-centre study during the first wave of COVID-19 pandemic (March–April 2020) and we found a reduction in the number of stroke patients admitted to hospital during the COVID-19 outbreak in Slovakia, but no evidence of a change in the quality of acute stroke care. 4 This was explained by the low incidence of COVID-19 positive patients in the first wave (1375 positive patients from the population of 5.458 million inhabitants). Unfortunately, during the second wave (October–November 2020), Slovakia was one of the countries with the highest incidence of positive patients (90,943 positive patients), which allowed us to compare whether the severity of the COVID-19 pandemic affected the acute care of stroke patients.
Methods
This retrospective cohort study analysed data from the stroke register at the National Health Information Centre and was approved by Ethics Committee of P.J. Šafárik University, Medical Faculty, Kosice. All patients brought to 1 of 43 hospitals for acute stroke care are entered into the register. This applies to both ischaemic stroke and TIA, as well as to intracerebral and subarachnoid haemorrhage. As the national stroke register allows only monthly reports to be extracted, the data from March and April 2020 were used as data from the first wave of the COVID-19 pandemic and data from October and November 2020 as data from the second wave of the COVID-19 pandemic. The information obtained from the stroke register includes the total number of patients admitted to hospitals with a final diagnosis of any stroke, ischaemic stroke and TIA, the number of patients treated with IV thrombolysis (IVT) and mechanic thrombectomy (MT); the average door-to-needle time (DNT) and average onset-to-needle time (ONT) for each hospital and for each evaluated time period. DNT is the time from arrival at the hospital to reperfusion therapy, and ONT is the time from first symptoms to reperfusion therapy. The severity of the stroke was measured using the NIHSS (National Institutes of Health Stroke Scale) score and the mRS (modified Rankin Scale) at discharge from hospital and mortality rate. Written informed consent was waived due to the retrospective character of the investigation.
Statistical analysis
Clinical variables of interest were described separately for each wave. Continuous variables were assessed for normality by visual inspection of histograms and were described using mean, standard deviation and median with the interquartile range (IQR), as appropriate. Categorical variables were summarised using frequencies.
An independent sample t-test was used to compare the means of normally distributed data. Non-normally distributed data were compared using the Wilcoxon-Mann-Whitney two sample rank-sum test.
Results
The total number of patients with any type of stroke (ischaemic stroke, intracerebral and subarachnoid haemorrhage) admitted to hospitals during the second wave of the COVID-19 pandemic was 1848, versus 1698 in the first wave (a 9% increase). The main characteristics of the samples from the two waves are summarised in Table 1. The proportion of patients treated by IVT was similar in both waves (275 patients, 20.7% vs 333 patients, 22.1%, p = 0.53, difference in location: —0,0003, 95% CI: −5.0 to 5.95), and the proportion of patients treated by mechanical thrombectomy (MT) on the country level did not significantly differ (p = 0.64, difference in location: −6.8, 95% CI: −25 to 7.0) between wave 1 (117 patients, 10.2%) and wave 2 (153 patients, 11.7%), though some regional differences were observed. The number of MTs in some hospitals doubled during the second wave (Figure 1).
Main clinical characteristics of the sample in the first and the second wave of the COVID-19 pandemic.
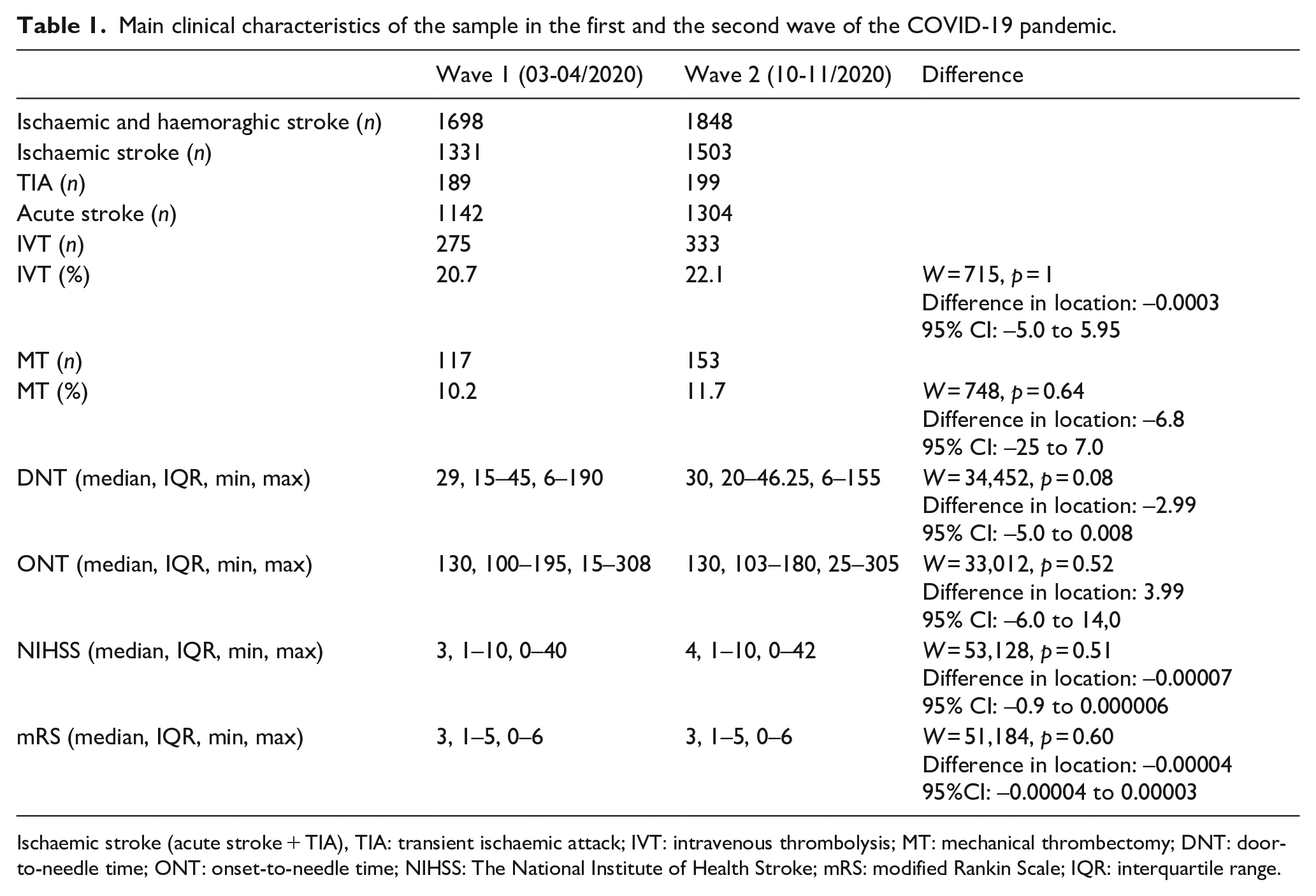
Ischaemic stroke (acute stroke + TIA), TIA: transient ischaemic attack; IVT: intravenous thrombolysis; MT: mechanical thrombectomy; DNT: door-to-needle time; ONT: onset-to-needle time; NIHSS: The National Institute of Health Stroke; mRS: modified Rankin Scale; IQR: interquartile range.
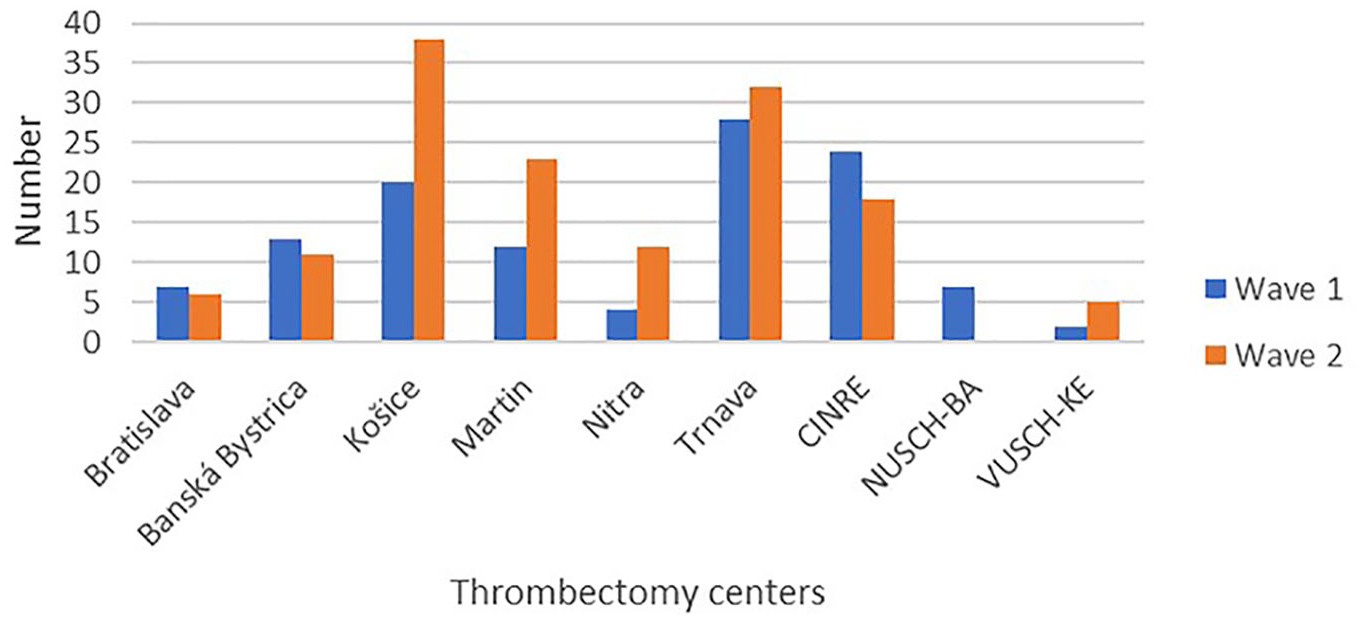
Number of thrombectomies in wave 1 and wave 2 of COVID-19 pandemic in Slovakia.
A Mann-Whitney U test showed no difference in the time from onset of symptoms to treatment (median = 130, IQR = 100–195 min in the first wave vs median = 130, IQR = 103–180 min in the second wave, p = 0.52, difference in location: 3.99, 95% CI: −6.0 to 14.0), nor in the door-to-needle time (p = 0.08, difference in location: −2.99, 95% CI: −5.0 to 0.008) between the first (median = 29, IQR 15–45 min) and the second wave (median = 30, IQR 20–46 min). NIHSS at discharge from hospital did not differ significantly (p = 0.51, difference in location: 0.00007, 95% CI: −0.9 to 0.000006) between the first (median = 3, IQR = 1–10) and second wave (median = 4, IQR = 1–10), which corresponded to the similar median modified Rankin Scale score at discharge in stroke patients in both periods (median = 3, IQR = 1–5 vs median = 3, IQR = 1–5, p = 0.60, difference in location: −0.00004, 95% CI: −0.00004 to 0.00003). Mortality for all types of stroke was 9.3% in the first wave and 7.8% in the second wave.
Discussion
The aim of the current study was to determine whether the severity of the COVID-19 pandemic affected the quality of acute care of stroke patients. In the second wave of the COVID-19 pandemic, with a significantly higher number of positive patients in comparison with the first wave, a mild increase in hospitalised patients with stroke (ischaemic, intracerebral, subarachnoid) was observed, but the quality of acute stroke treatment did not change. The proportion of patients treated with IVT and MT did not decrease; it even increased slightly, and there was no prolongation of the time to acute treatment.
In the first wave of the pandemic, we recorded a decrease (by 28%) in the number of patients hospitalised for a stroke, 4 which was similar to the situation in the Czech Republic (14%), 3 the Amsterdam area of the Netherlands (24%) 1 and in the Akershus region of Norway (32%), 2 though with no evidence of a change in the quality of acute stroke care. Contrary, in cross-sectional survey in early phase of the COVID-19 pandemic, including 375 stroke care providers from Europe, only 23% respondents considered that all stroke patients in their centres were still receiving the usual acute and post-acute care. 7 During the second wave, the number of patients admitted with stroke in Slovakia was slightly higher than in the first wave, which was comparable to the situation in Germany 8 or at a single centre in Liberec, Czech Republic. 9 In contrast to our results, the authors from a tertiary care hospital in Saxony, Germany, found a 25% decline in stroke admissions during the second wave period, when Saxony was among the most severely affected regions in Germany, while it was barely affected by the first wave. 10 They explained the drop in the number of stroke admitted patients by the regional variability of SARS-CoV-2 incidence in Germany and by an avoidance to seek hospital treatment during the increasing intensity of lockdown measures. This is also confirmed by the fact that the country level data in Germany showed a slight increase in the number of patients admitted to hospitals in the second wave in comparison with the first one .8,10
No difference in the number of stroke patients between the first and the second wave was found in three tertiary care hospitals in Greece, although the severity of the pandemic during the second wave was stronger in Greece. The authors did not note a repeating of the reduction in the number of admissions of younger patients during the second wave, which was observed in the first wave. 11
During the first pandemic wave, there was a great fear of acquiring a SARS-CoV-2 infection during a hospital stay 12 therefore, one explanation for the slight increase of hospitalised patients with stroke observed, although speculative, may be that a reduction in the fear of contracting SARS-CoV-2 infection might be attributed to the smaller decline in AIS hospitalisations during the second wave period. 8 The equally reduced number of stroke patient admissions in both waves in Greece in comparison with the pre-COVID time period is explained by the lockdowns in both waves. 11 The conclusions from other studies indicate that the reduced number of patients with stroke during the COVID-19 pandemic may be explained by a lower number of patients with TIAs avoiding hospitals out of fear of infection with SARS-CoV-2.1,13–15 We found no difference in the proportions of patients with TIA during the first wave of the pandemic when compared to the period March–April 2019. 4 The same trend was observed in the second wave.
It has been reported that IVT use was affected by the pandemic on a global level during the first pandemic wave.16–18 This was not the case in Slovakia, and the use of IVT and MTs did not decrease even during the second wave, which was stronger in terms of the incidence of COVID-19 positive patients. The proportion of patients treated by IVT as well as by MT in Slovakia was similar in both waves. In Germany, there was a decrease in the proportion of patients treated with IVT in the second wave, which was probably due to a reduction in the number of intensive care units but also due to an increase in the total number of patients admitted with acute stroke. 10 In contrast, the use of MT was consistently higher throughout 2020 when compared to 2019, and it is probably part of Germany’s steadily rising MT rate over past years.8,19,20 An increase in the total number of patients admitted with acute stroke in the second wave of the COVID-19 pandemic was also referred to in the Madrid health region with one endovascular centre and seven hospitals with ISUs (intensive stroke units). Consistent with our results, the proportion of patients undergoing reperfusion therapy in Madrid was similar in both waves, as were the time metrics. We cannot explain unequivocally why the number of MTs doubled in three hospitals in Slovakia. The hospital in Košice has the largest catchment area (10 stroke units and 1.5 million inhabitants), and this may be related to the consistently growing number of MTs since 2018, when the number of invasive radiologists was increased and began operating in a 24/7 regime. In the city of Martin, the increase can be explained by almost doubling the number of admissions with stroke in the second wave compared to the first wave, probably due to the regional reorganisation of admissions during the second wave of the COVID-19 pandemic. In the third hospital, in Nitra, the lower number of MTs during the first wave in comparison with the standard numbers was likely caused by temporary staffing problems at the department performing MT.
We found no difference in the time from onset of symptoms to treatment, nor in the door-to-needle time between the first and the second wave of pandemic, similar to the Madrid health region and Germany.8,21 Data from Germany and Slovakia comparing stroke management during the first and second waves across the country, as well as data from Madrid health region confirmed that with a well-organised stroke care system, even a higher incidence of COVID-19 infection during the second wave did not worsen the quality of acute stroke care in hospitalised patients.8,21 This is in line with the conclusions of a prospective multicentre cohort study based on data from the TRISP (Thrombolysis in Ischaemic Stroke Patients) registry from the first wave of the COVID-19 pandemic, that the stability of acute stroke care results may be explained by the resilience of acute cerebrovascular care services during the lockdown, at least in well-established European stroke centres, and implies quick and sufficient adaptation by these centres to the new situation. 22
Thanks to the mandatory stroke register in Slovakia, we have data about patients’ NIHSS scores and mRS at discharge from hospital. The NIHSS score did not differ significantly in the first (median = 3) and second wave (median = 4), which corresponded to the similar median modified Rankin Scale score at discharge in stroke patients in both periods (in both median = 3). Our nationwide study has limitations. First, data collection was retrospective, but thanks to the mandatory register the number of patients with incomplete or missing data is low. However, it is possible that some data from the COVID departments are missing. Second, we have no data about stroke patients with concomitant COVID-19 disease for the whole country. We have no data on NIHSS and mRS 90 days after stroke. The strength of our study is the collection of data from the whole country.
Mortality rate for all types of stroke was similar in the first and the second waves of pandemic, but it is possible that some patients with stroke who died in the COVID ward were not reported to the registry.
In conclusion, neither during the first wave of the COVID-19 pandemic, when Slovakia was one of the countries with a low prevalence of COVID-19 disease, nor during the second wave of the pandemic, when Slovakia was one of the countries with the highest incidence of COVID-19, was a worsening of acute care for stroke patients found. Our data confirmed the conclusions of other countries from the first wave 22 that the quality of acute stroke care can be preserved with a well-organised stroke care system. These findings are very important for stroke care during the COVID-19 pandemic, and we must do everything we can to maintain them. Patients with stroke should be constantly encouraged to seek medical care immediately (e.g. the ‘do not stay at home with stroke’ campaign).
Footnotes
Acknowledgements
The authors wish to acknowledge the colleagues from all 43 departments who contributed to the register. This article was supported by the Irene Cost Action CA18118 ‘Implementation Research Network in Stroke Care Quality’, there was no financial and material support.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ZG received honoraria for lectures from Boehringer-Ingelheim and serves as a member of the European Academy of Neurology Stroke Management Panel, other authors do not have conflict of interest in relation to this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by Ethics Committee of P.J. Safárik University, Medical Faculty, Kosice.
Informed consent
Informed consent was not sought for the present study due to the retrospective character of the investigation.
Guarantor
ZG.
Author contributions
Study concept and designs: Gdovinova, Vitkova. Acquisition, analysis and interpretation of data: All authors. Drafting of the article: Gdovinova. Critical revision of the article for important intellectual content: All authors. Statistical analysis: Vitkova.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.