
Abstract
Introduction:
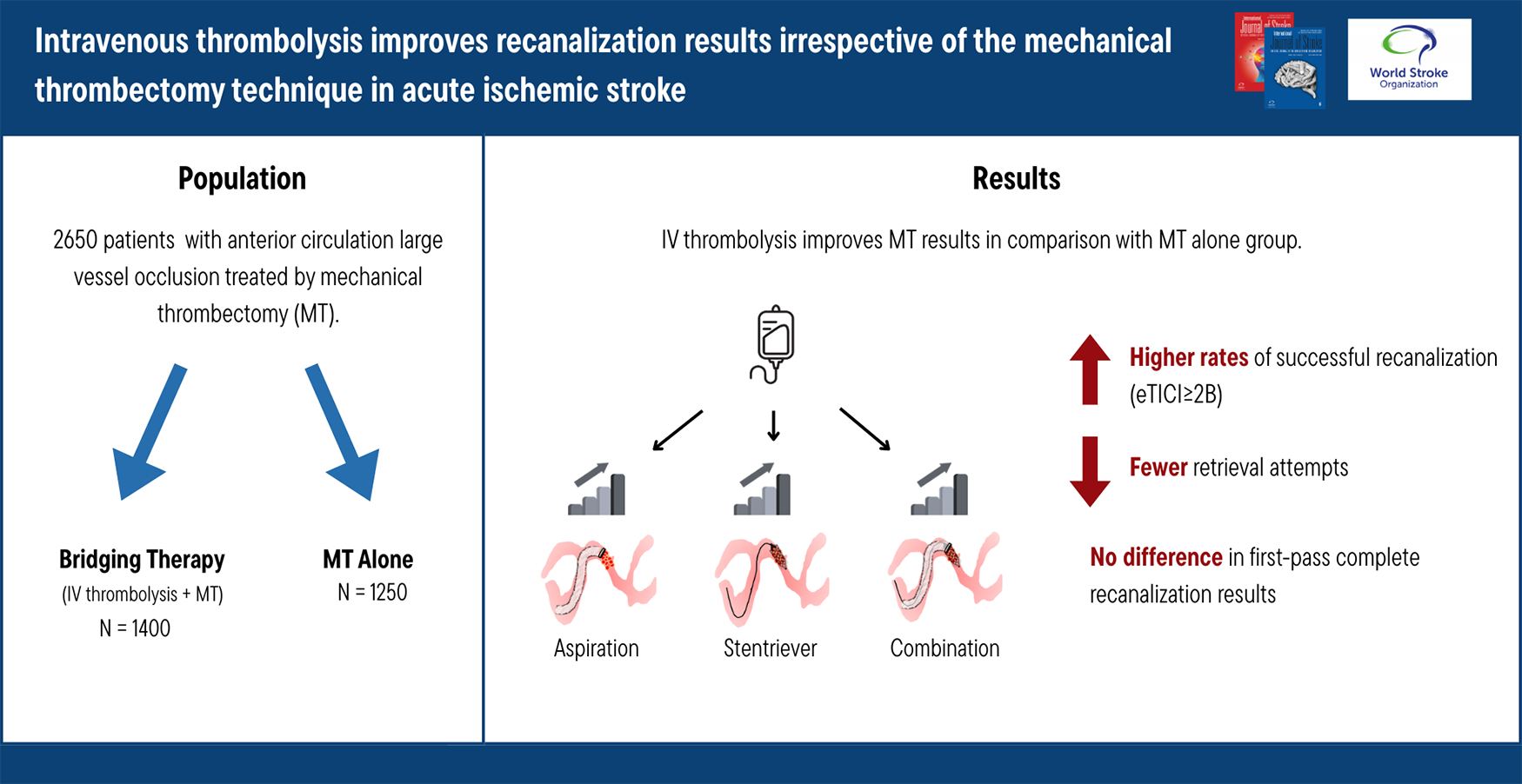
Post hoc analysis of recent trials comparing bridging therapy to endovascular therapy (EVT) alone reported improved recanalization results with bridging therapy. It remains uncertain whether the positive effect of prior intravenous thrombolysis (IVT) is consistent across all mechanical thrombectomy first-line techniques (aspiration, stent-retriever, or combination of both) currently in use. In this study, we aimed to evaluate the consistency of IVT’s beneficial impact on different mechanical thrombectomy techniques.
Methods:
Data were extracted from prospective registries, including consecutive acute ischemic stroke patients treated with EVT between January 2015 and October 2022. Patients included had anterior circulation large vessel occlusion and were treated with EVT, with or without prior IVT. A propensity score-weighted analysis was performed to measure the effect of IVT on recanalization results across different EVT techniques.
Results:
A total of 2650 patients (mean age 70 ± 15 years, 47% males) were included, 1400 in the bridging group and 1250 in the EVT alone group. Bridging group demonstrated higher rates of successful recanalization (eTICI ⩾ 2B) (odds ratio (OR) = 1.78, 95% confidence interval (CI): [1.52–2.1]). This result was consistent across all EVT first-line techniques: aspiration (OR = 1.81; 95% CI: [1.3–2.6], p = 0.01); stent-retriever (OR = 1.64; 95% CI: [1.2–2.2]) and combined technique (OR = 1.94; 95% CI: [1.6–2.4]). In addition, fewer retrieval attempts were needed in the bridging group (OR = 1.26, 95% CI: [1.04–1.4]), with a consistent effect across different EVT techniques.
Conclusion:
IVT significantly improves recanalization results of EVT in patients with acute ischemic stroke, regardless of employed mechanical thrombectomy technique.
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.