
Abstract
Aims:
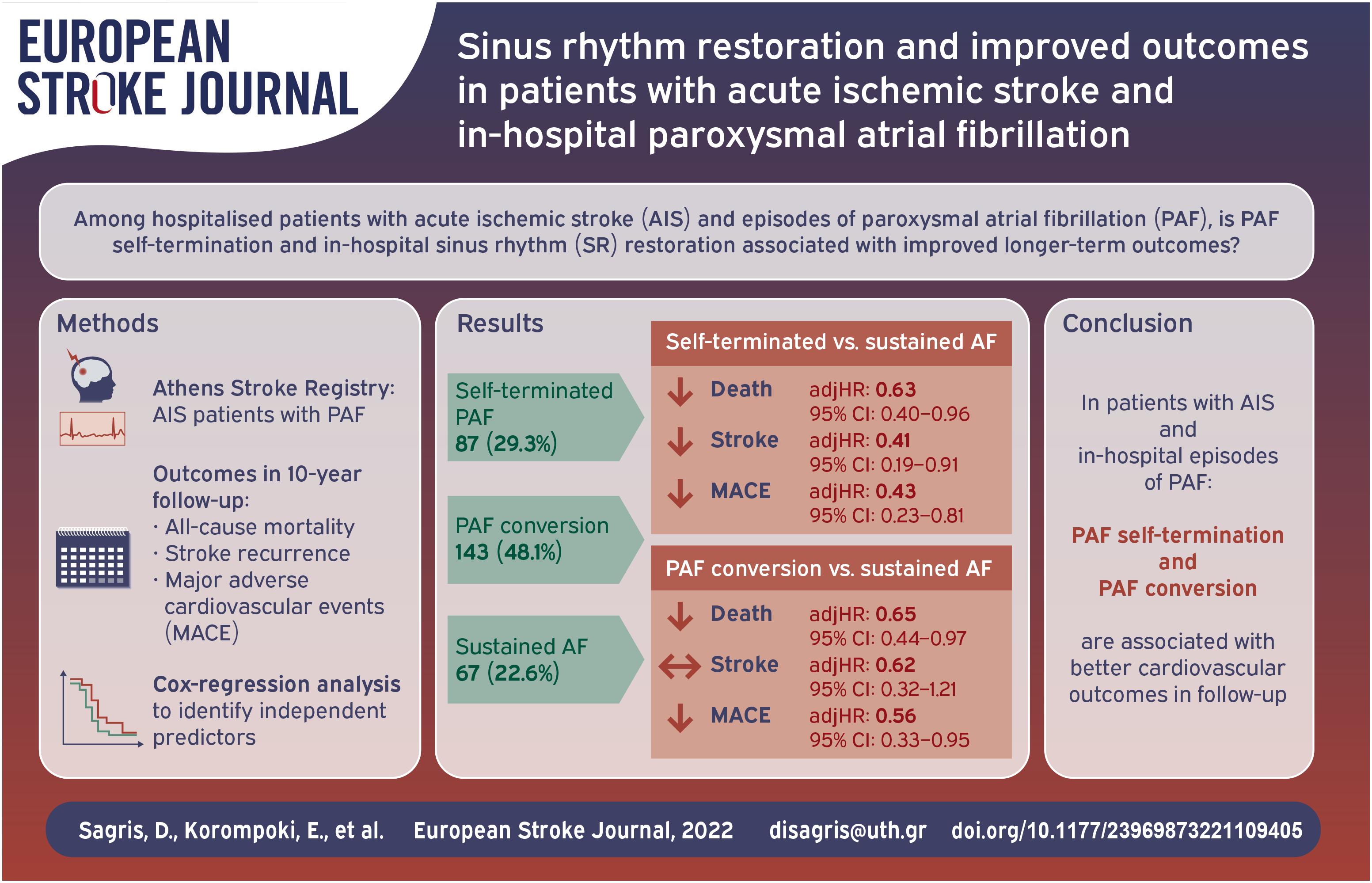
It is unclear whether early cardiac rhythm control is beneficial in patients with acute ischemic stroke and paroxysmal atrial fibrillation (PAF). We sought to investigate whether PAF self-termination and in-hospital sinus rhythm (SR) restoration is associated with improved outcome in ischemic stroke patients with PAF, compared to those with sustained atrial fibrillation (AF).
Methods:
Consecutive patients with first-ever acute stroke and confirmed PAF during hospitalization were followed for up to 10 years after the index stroke or until death. We investigated the association of in-hospital self-terminated PAF and PAF conversion to SR compared to sustained AF with 10-year all-cause mortality, stroke recurrence, and major adverse cardiovascular events (MACE). Cox regression analysis was performed to identify independent predictors of each outcome.
Results:
Among 297 ischemic stroke patients with in-hospital PAF detection, PAF was self-terminated in 87 (29.3%) patients, while 143 (48.1%) patients received antiarrhythmic medication in order to achieve PAF conversion to SR. During a median (Interquartile range, IQR) period of 28 (4–68) months, among patients with self-terminated PAF there were 13.5 deaths, 3.6 stroke recurrences, and 5.3 MACE per 100 patient-year while in patients who underwent medical PAF conversion there were 11.7 deaths, 4.6 stroke recurrences, and 5.8 MACE per 100 patient-year. Patients with sustained AF experienced 23.8 deaths, 8.7 stroke recurrences, and 13.9 MACE per 100 patient-years. In multivariable analysis, compared to patients with sustained AF, PAF self-termination was associated with significantly lower 10 years-risk of death (adjusted hazards ratio (adjHR): HR: 0.63, 95% Confidence interval: 0.40–0.96), stroke recurrence (adjHR: HR: 0.41, 95% CI: 0.19–0.91), and MACE (adjHR: 0.43, 95% CI: 0.23–0.81), while PAF medical conversion to SR was associated with lower 10 years-risk of death (adjHR: 0.65, 95% CI: 0.44–0.97) and MACE (adjHR: 0.56, 95% CI: 0.33–0.95).
Discussion:
This study showed that in-hospital PAF self-termination was associated with lower risk of 10-year mortality, stroke recurrence, and MACE, potentially attributed to the lower burden of AF, whereas in-hospital PAF conversion to SR was associated with lower risk of 10-year mortality and MACE.
Conclusion:
Early restoration of sinus rhythm is associated with improved survival and MACE in patients with acute ischemic stroke and PAF.
Introduction
Atrial fibrillation (AF) is highly prevalent in patients with ischemic stroke. 1 In a pursue to reduce this burden in primary and secondary prevention of AF-related strokes, recent guidelines support an holistic approach to AF management taking in account novel anticoagulants and rhythm control strategies in patients with AF and several comorbidities. 2
Atrial fibrillation is a common finding in ischemic stroke patients, ranging from 7.7% to 23.7%, based on the detection method.1,3 Although it is still unclear whether there is a temporal association between ischemic stroke and new onset AF, there might be a stronger association with longer episodes close to the index event. 4 Several observational studies proposed the hypothesis of neurogenic post-stroke AF as a result of brain damage, especially in patients with cryptogenic stroke, generating a discussion on whether post-stroke AF serves as cause or consequence in this population. 5 Regardless of the pathogenesis of AF after stroke, recent studies have shown that post-stroke AF shares similar stroke outcomes or even higher mortality compared to those with known AF.6,7
Observational population-based studies have shown a significant reduction of stroke in patients with AF who underwent rhythm control management compared to rate control, regardless of anticoagulant treatment.8,9 Recently, the Early Treatment of Atrial Fibrillation for Stroke Prevention Trial (EAST-AFNET 4) showed that patients with AF benefit from early rhythm-control as this therapeutic approach significantly reduced the risk of future stroke compared to the standard care. 10 Whether the reduction of AF burden by sinus rhythm restoration which was achieved in EAST-AFNET 4 applies also in the acute phase of ischemic stroke is unknown as these patients were not included in the trial.
In the latest AF guidelines, remains unclear whether patients with acute ischemic stroke and episodes of in-hospital paroxysmal AF (PAF) after stroke should undergo rhythm control therapy during hospitalization in order to restore SR. 2
In this report from the Athens Stroke Registry, we sought to investigate whether in-hospital PAF self-termination and medical PAF conversion to SR in patients with acute ischemic stroke and in-hospital PAF is associated with future outcomes.
Methods
Study population
The study included prospectively collected data from consecutive first-ever acute stroke patients over a period of 20 years (January 1993–December 2012), who were admitted to the Alexandra University Hospital within 24 h after the onset of symptoms. Details about the prospective Athens Stroke Registry were published elsewhere. 11 The study was approved by the institutional Ethics Committee.
In this study we included patients with a first-ever ischemic stroke and at least one episode of PAF which was detected on admission or during hospitalization. Patients with known medical history of permanent or paroxysmal AF which was not confirmed during hospitalization were excluded from the analysis. Patients with AF which was detected for the first time on admission and was not restored during hospitalization were excluded from the analysis, as these patients may had permanent AF, which had never been detected. Patients with previous medical history of PAF were included in the study only if they had at least one episode of PAF detected during hospitalization. Patients with PAF episodes were categorized into three groups: (i) those with self-terminated PAF, (ii) those who received antiarrhythmic medication in order to convert PAF and restore SR, and (iii) those with sustained AF. The decision to treat each patient with specific antiarrhythmic medication was individualized, based on the judgment of the treating physician, depending on patient’s profile, comorbidities, and contraindications.
Atrial fibrillation documentation
AF was diagnosed and documented prospectively by admission and repeated standard 12-lead ECGs, continuous ECG monitoring for 1 week or until discharge for patients treated in the acute stroke unit and 24-h Holter ambulatory ECG monitoring during hospitalization. An ECG recording of
Outcomes and follow-up
Patients were prospectively followed-up at 1, 3, and 6 months after discharge and yearly thereafter for up to 10 years after stroke or until death. Follow-up was routinely performed at the outpatient clinic, at the patient’s residence or during a telephone interview. Death, cause of death, stroke recurrence, and major adverse cardiovascular event (MACE) were further ascertained by using death certificates, patient records, information from general practitioners, and family physicians’ records. The outcomes assessed in the analysis were overall mortality, ischemic stroke recurrence, and MACE defined as recurrent stroke, new myocardial infarction or unstable angina, peripheral embolism, and sudden cardiac death with or without resuscitation.
Statistical analysis
Continuous variables are presented as mean value (±standard deviation, SD) or median (Inter quartile range, IQR) and categorical covariates as absolute numbers and proportion (%). For patients lost during follow-up, survival data were censored at the last time known to be alive. Patients who experienced more than one MACE were censored at the time of the first event. Student’s t-test was applied for continuous variables; chi-square or Fisher’s exact test was applied for categorical variables. The Kaplan-Meier product limit was used to estimate the cumulative probability of each outcome according to whether patients had self-terminated PAF, received antiarrhythmic medication to restore SR, or remained in sustained AF. Differences in Kaplan-Meier curves were evaluated with the log-rank test. Cox-regression analyses were performed to assess whether PAF self-termination and PAF conversion to SR are independent predictors of outcomes in patients with PAF and acute stroke, compared to patients with sustained AF. We performed univariable cox-regression analyses, for each outcome using the variables age, sex, NIHSS on admission, days from admission to first episode of AF, hypertension, diabetes mellitus, smoking, dyslipidaemia, coronary artery disease, TIAs, heart failure, insular involvement, in-hospital treatment (thrombolysis, antithrombotics, antiarrhythmics), and antithrombotic treatment at discharge. Among them, only variables reaching the statistical significance level of p < 0.1 for each outcome, were finally included in the multivariable cox regression analysis. For the univariable analysis, the level of significance was set at 0.1 to reduce the risk of a type II error. Additionally, apart from variables which reached the statistical significance level of p < 0.1, in the multivariable cox-regression analysis for each outcome we included CHA2DS2-VASc score, “anticoagulation at discharge” and the variables “first detection of AF” and “days from admission to first episode of AF,” which can serve as surrogates for AF burden. In the final multivariable analysis, the level of significance was set at 0.05. Associations are presented as hazard ratios with their corresponding 95% confidence interval (95% CI). Additionally, we performed a time dependent cox-regression analysis to assess whether PAF self-termination and PAF conversion to SR were associated with the outcomes in patients with PAF and acute stroke, compared to patients with sustained AF at 3 months, 1 year, and 5 years. Statistical analyses were performed with the Statistical Package for Social Science (SPSS Inc, version 25.0 for Windows; Chicago, IL).
Results
Baseline characteristics
From the original study cohort of 3304 acute stroke patients, we identified 297 cases of ischemic stroke patients with paroxysmal AF detected after the ischemic stroke (Figure 1). The cohort population consisted of 162 (51.9%) men and 135 (48.1%) women. SR was restored in 230 (77.4%) patients with PAF. Among them, PAF was self-terminated in 87 (29.3%) patients, while 143 (48.1%) patients received antiarrhythmic medication in order to achieve PAF conversion to SR. Among the included patients’ previous medical history of PAF was mentioned in 53 (17.8%). PAF was detected after a median (IQR) of 2 (1–4) days from the admission while PAF was documented for the first time in 244 (82.2%) patients, in similar proportion between the compared study groups (Table 1). Seventy-three (24.6%) patients experienced more than one episode of PAF and among patients who finally remained in sustained AF 17.9% experienced more than one episode. Baseline cha-racteristics and therapeutic interventions are summarized in Table 1.
Baseline characteristics of the study population according to sinus rhythm restoration.
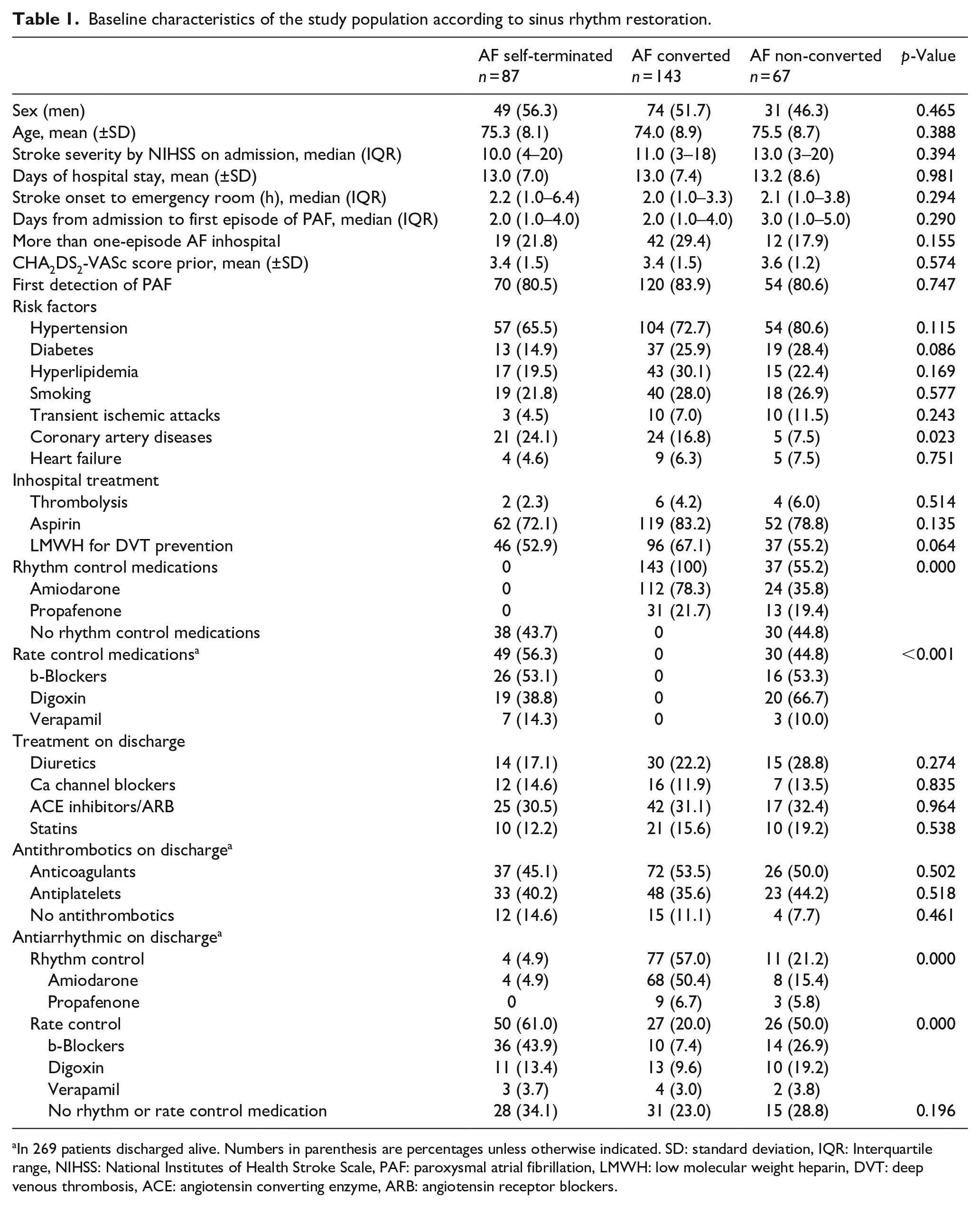
In 269 patients discharged alive. Numbers in parenthesis are percentages unless otherwise indicated. SD: standard deviation, IQR: Interquartile range, NIHSS: National Institutes of Health Stroke Scale, PAF: paroxysmal atrial fibrillation, LMWH: low molecular weight heparin, DVT: deep venous thrombosis, ACE: angiotensin converting enzyme, ARB: angiotensin receptor blockers.
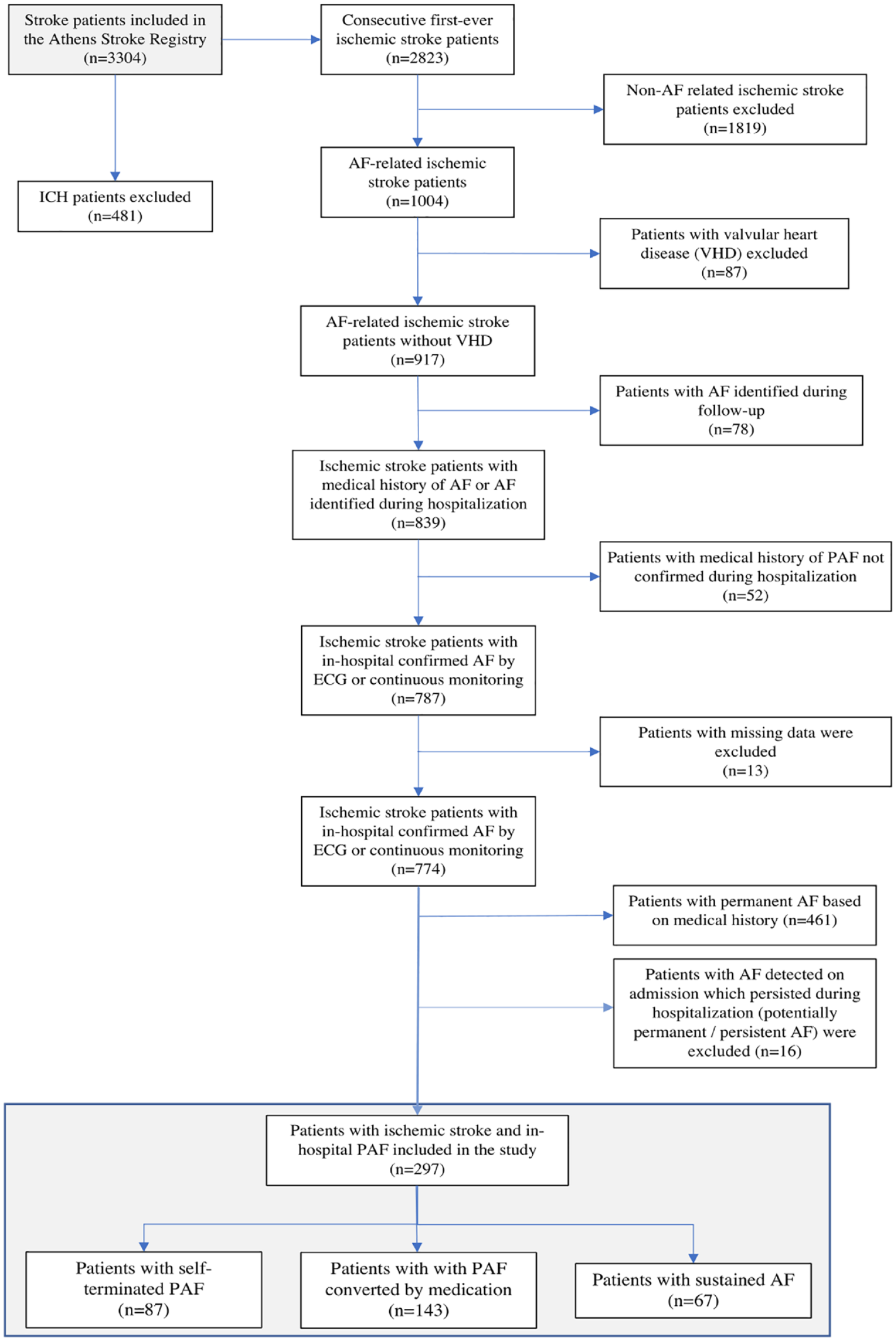
Study flow chart for identification of inhospital paroxysmal atrial fibrillation.
The majority of the patients (58.9%) experienced the first episode of PAF on admission or the during the first 2 days of hospitalization (Figure 2). Coronary artery disease was less common among patients with sustained AF (7.5%), compared to those with self-terminated episodes and those who underwent SR restoration (16.8% and 24.1% respectively, p = 0.023). No significant differences were observed in other cardiovascular risk factors, antithrombotic, and thrombolytic treatment during hospitalization (Table 1) and vascular location on imaging studies (Supplemental Table 1).
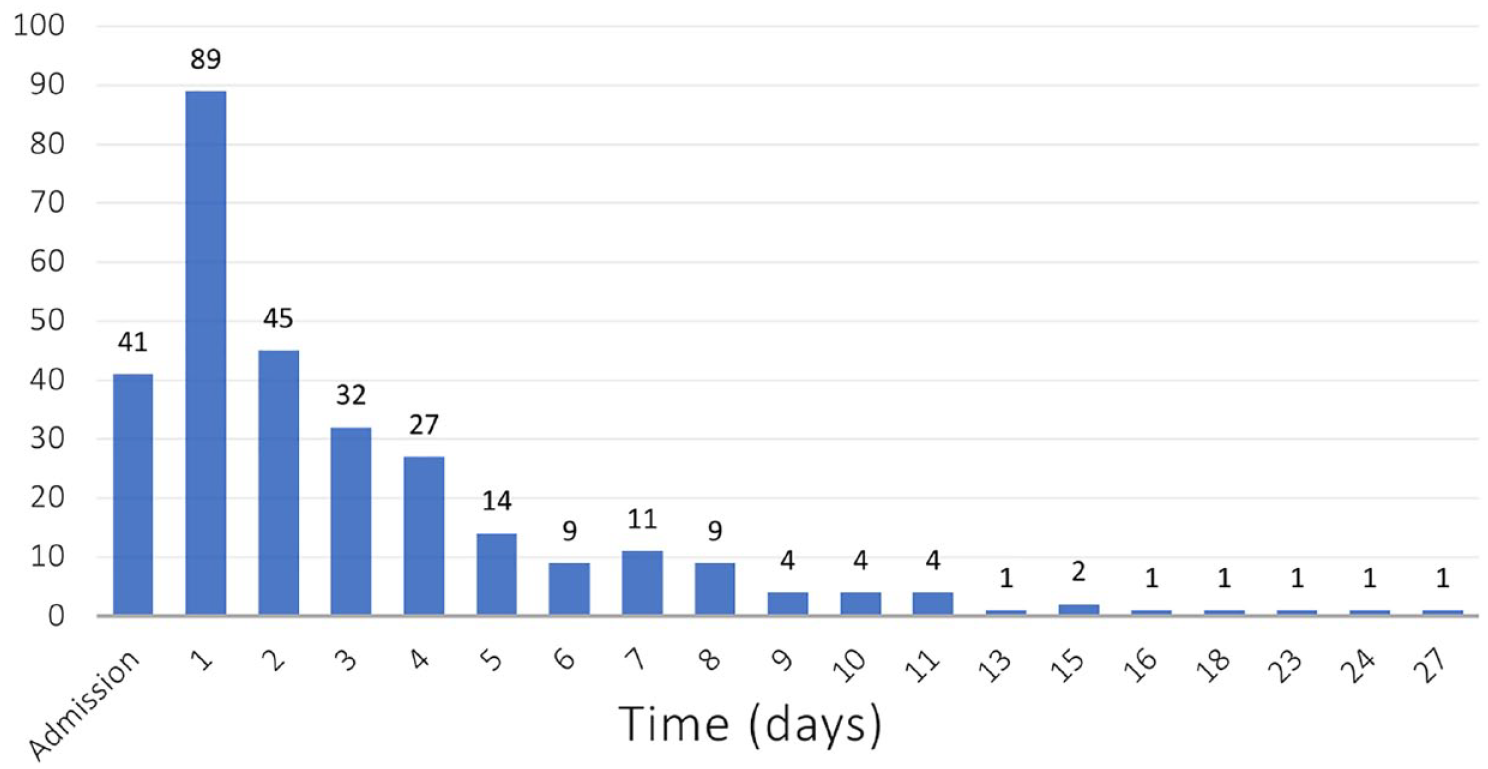
Distribution of days of inhospital paroxysmal atrial fibrillation detection during the hospital stay.
In-hospital sinus rhythm restoration and outcomes during follow-up
Study patients were followed-up for up to 10 years with a median (IQR) follow-up period of 28 (4–68) months. Forty-five patients (15.2%) patients were lost to the scheduled follow-up (from 6 to 75 months). During the study period 148 (49.8%) deaths occurred. The cumulative 10-year probability of mortality in patients with self-terminated PAF was 66.8% (95% CI: 52.9–80.7), 62.6% (95% CI: 51.7–72.8) in patients with medical PAF conversion to SR and 79.8% (95% CI: 66.7–92.9) in those with sustained AF, corresponding to 13.5 deaths per 100 patient-years among patients with self-terminated PAF, 11.7 deaths per 100 patient-year among patients underwent PAF conversion, and 23.8 per 100 patient-years in those with sustained AF (Table 2 and Supplemental Table 1). Patients with self-terminated PAF and PAF converted by medication had significantly lower risk of 10 years-mortality compared to those with sustained AF (HR: 0.66, 95% CI: 0.40–0.95 and HR: 0.56, 95% CI: 0.38–0.82, respectively) (Figure 3(a)), a finding which remained consistent from the first year of the follow-up (Supplemental Table 3). Cardiovascular death occurred in significantly lower proportion of patients with self-terminated PAF and converted PAF compared to those who remained in sustained AF (3.9 per 100 patient-years in patients with self-terminated and medical PAF conversion, compared to 9.8 per 100 patient-years respectively, p = 0.016). In the multivariable cox-regression analysis, after adjusting for age, stroke severity (NIHSS), first detection of PAF, day of PAF detection, CHADS2DS2-VASc, and anticoagulation at discharge, compared to patients with sustained AF, the 10 years-risk of death was lower in patients with self-terminated episodes of PAF (HR: 0.63, 95% CI: 0.40–0.96) and those who underwent PAF conversion (HR: 0.65, 95% CI: 0.44–0.97) (Table 3).
Outcomes during follow-up.
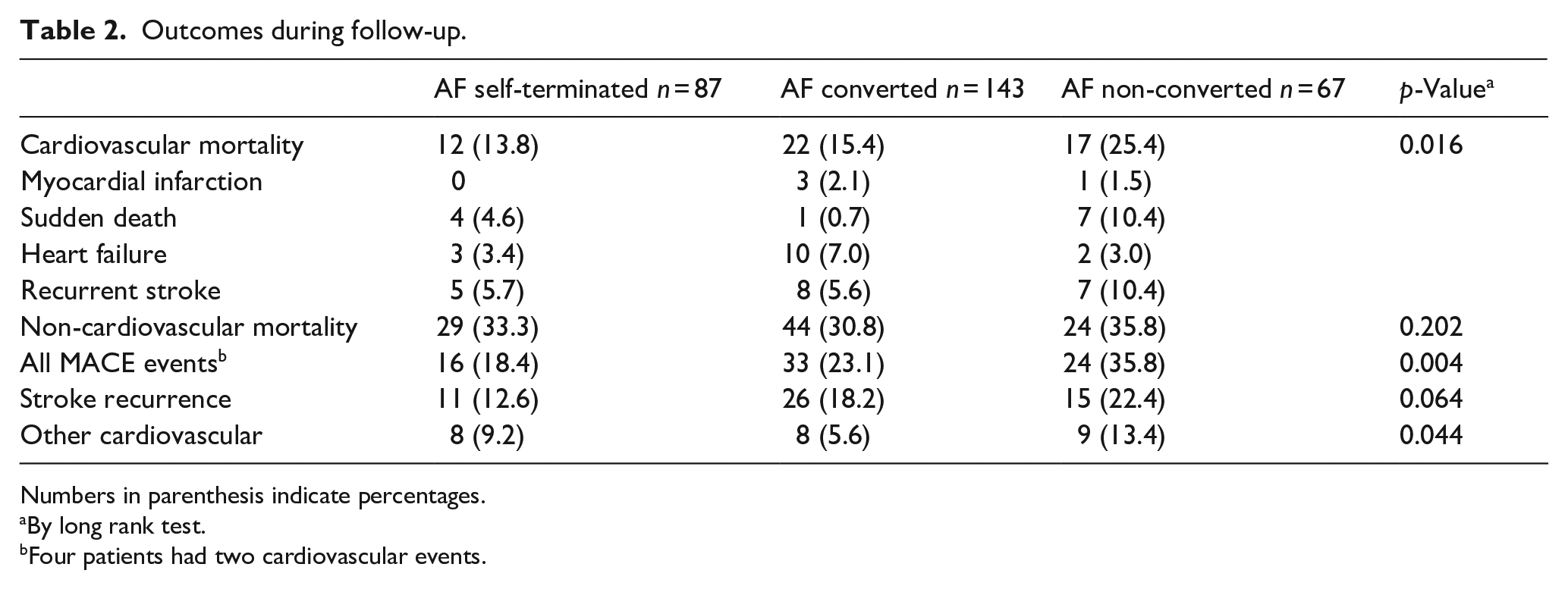
Numbers in parenthesis indicate percentages.
By long rank test.
Four patients had two cardiovascular events.
Multivariable cox regression analysis determining the effect of various factors on mortality, stroke recurrence, and cardiovascular events.
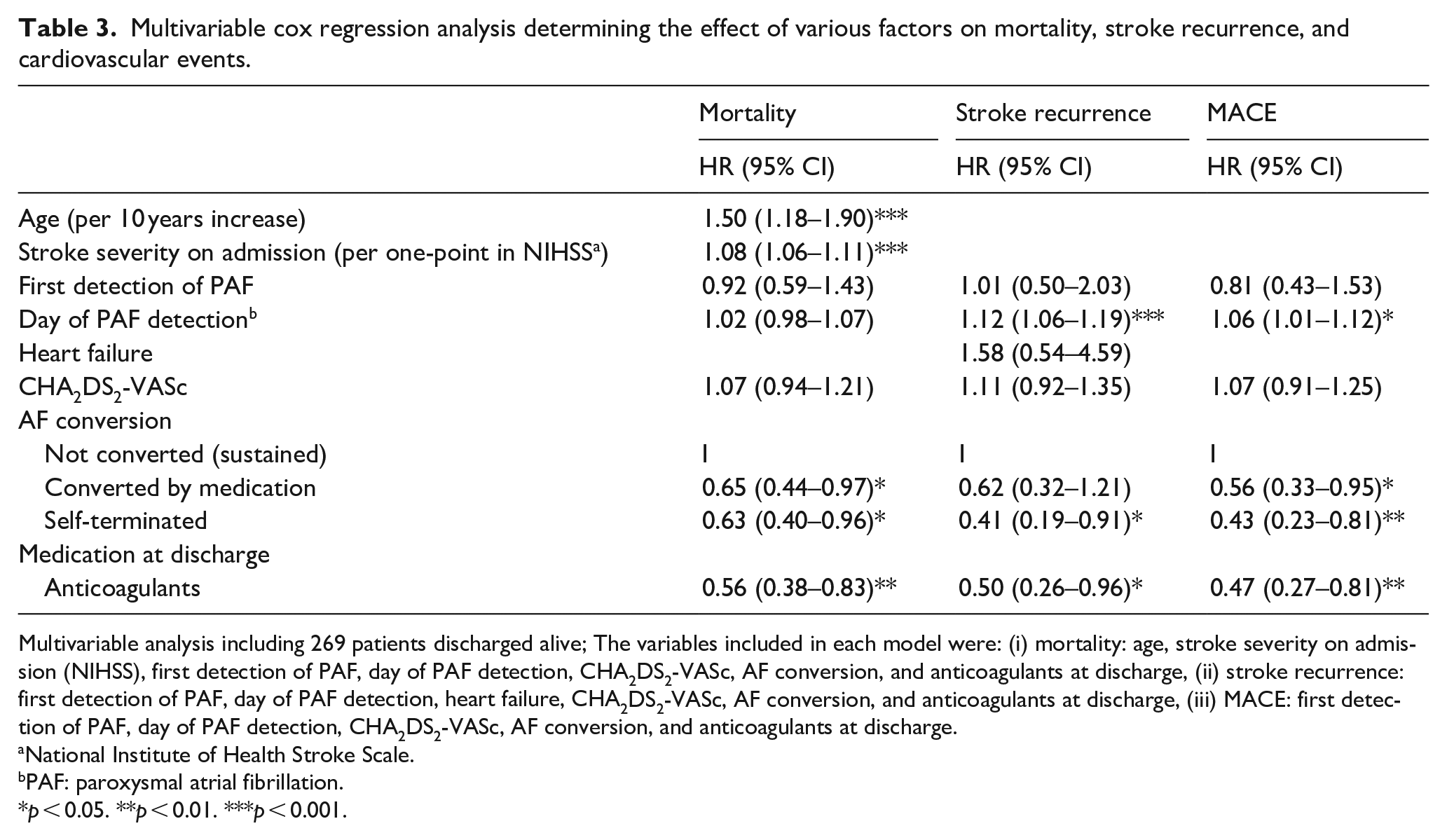
Multivariable analysis including 269 patients discharged alive; The variables included in each model were: (i) mortality: age, stroke severity on admission (NIHSS), first detection of PAF, day of PAF detection, CHA2DS2-VASc, AF conversion, and anticoagulants at discharge, (ii) stroke recurrence: first detection of PAF, day of PAF detection, heart failure, CHA2DS2-VASc, AF conversion, and anticoagulants at discharge, (iii) MACE: first detection of PAF, day of PAF detection, CHA2DS2-VASc, AF conversion, and anticoagulants at discharge.
National Institute of Health Stroke Scale.
PAF: paroxysmal atrial fibrillation.
p < 0.05. **p < 0.01. ***p < 0.001.
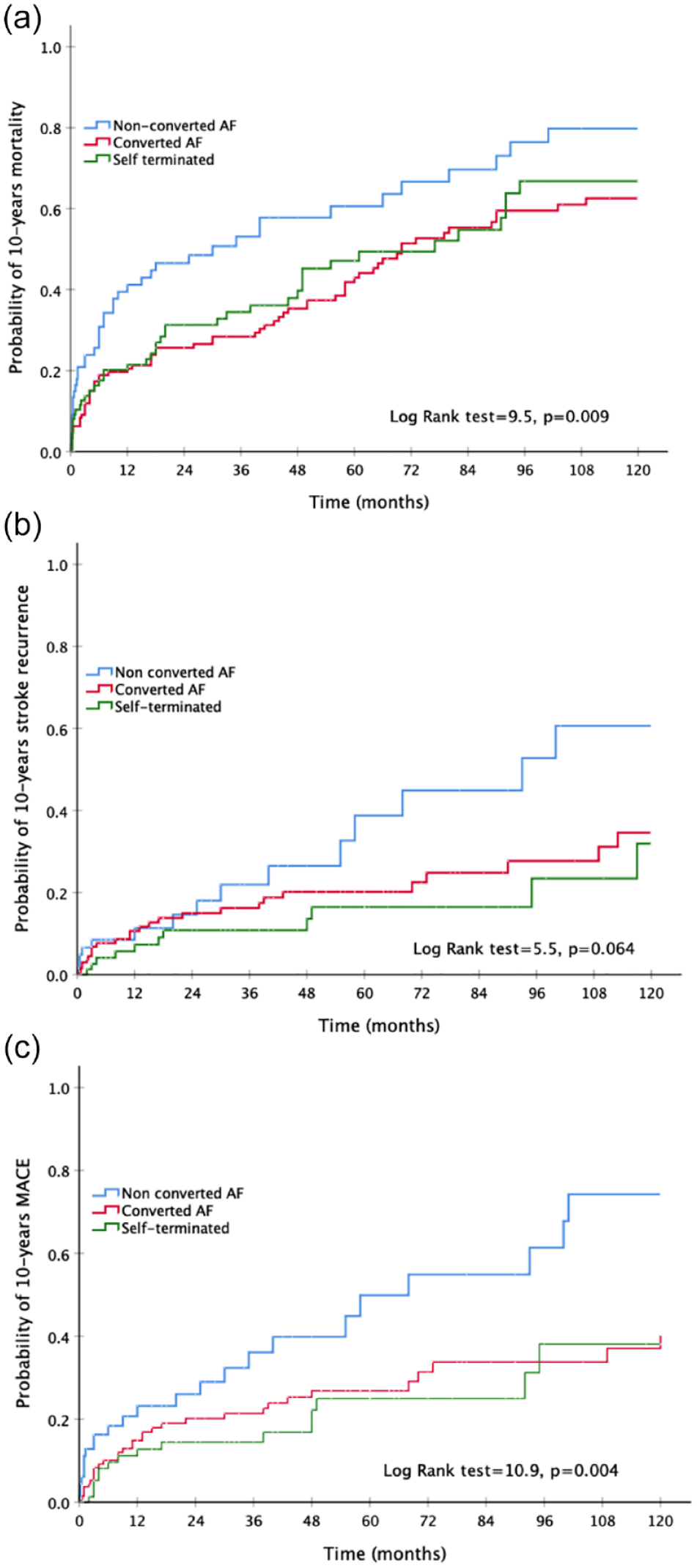
Cumulative risk for stroke mortality (a), stroke recurrence (b), and MACE (c) according to inhospital paroxysmal atrial fibrillation conversion.
Recurrent ischemic stroke occurred in 52 (17.5%) patients in the overall population during follow up. The cumulative 10-year probability of recurrent ischemic stroke in patients with self-terminated PAF was 31.9% (95% CI: 10.5−53.3), 34.6% (95% CI: 13.3−55.9) in patients with PAF conversion to SR by antiarrhythmic medication and 60.6% (95% CI: 36.7−84.5) in those with sustained AF, corresponding to 3.6 stroke recurrences per 100 patient-year among patients with self-terminated AF, 4.6 per 100 patient-year among patients underwent PAF conversion and 8.7 per 100 patient-years in those with sustained AF (Table 2 and Supplemental Table 2). Patients with self-terminated PAF had significantly lower rates of 10 years ischemic stroke recurrence compared to those with sustained AF (HR: 0.42, 95% CI: 0.19–0.91), while patients with PAF converted by medication had a non-significant trend toward lower ischemic stroke recurrence compared to those with sustained AF (HR: 0.58, 95% CI: 0.31–1.09) (Figure 3(b)). In the multivariable cox-regression analysis, after adjusting for first detection of PAF, day of PAF detection, heart failure, CHADS2DS2-VASc, and anticoagulation at discharge, self-terminated PAF was associated with a significant reduction of 10 years-risk of ischemic stroke recurrence compared to patients with sustained AF (HR: 0.41, 95% CI: 0.19–0.91), while medical PAF conversion did not significantly affect the risk of stroke recurrence (HR: 0.62, 95% CI: 0.32–1.21) (Table 3).
There were 77 (25.9%) MACE comprised of 52 recurrent ischemic strokes, 13 myocardial infarction or unstable angina not leading to death, 2 cases of peripheral embolism, and 10 cases of sudden cardiac death. Four patients experienced more than one vascular event during the follow-up period. The cumulative 10-year probability of MACE in patients with self-terminated PAF was 38.1% (95% CI: 18.7−57.5), 40.4% (95% CI: 27.3–53.5) in patients with PAF conversion to SR by antiarrhythmic medication and 74.2% (95% CI: 56.4–93.9) in those with sustained AF, corresponding to 5.3 MACE per 100 patient-year among patients with self-terminated AF, 5.9 per 100 patient-year among patients underwent PAF conversion and 13.9 per 100 patient-years in those with sustained AF (Table 2 and Supplemental Table 1). Patients with self-terminated PAF and PAF converted by medication had significantly lower risk of 10 years-MACE compared to those with sustained AF (HR: 0.40, 95% CI: 0.21–0.76 and HR: 0.40, 95% CI: 0.29–0.82, respectively) (Figure 3(c)), a finding which remained consistent after the first year of the follow-up (Supplemental Table 3). In multivariate cox-regression analysis, after adjusting for first detection of PAF, day of PAF detection, CHADS2DS2-VASc, and anticoagulation at discharge, compared to patients with sustained AF, patients with self-terminated episodes of PAF and those who underwent AF conversion had significantly lower risk of MACE (HR: 0.43, 95% CI: 0.23–0.81 and HR: 0.56, 95% CI: 0.33–0.95, respectively) (Table 3).
In the multivariable analysis, treatment with anticoagulants at discharge was associated with significantly lower risk of all-cause mortality, stroke recurrence, and composite MACE independently of the SR restoration (HR: 0.56, 95% CI: 0.38–0.83; HR: 0.50, 95% CI: 0.26–0.96; and HR: 0.47, 95% CI: 0.27–0.81, respectively) (Table 3). Late detection of PAF during hospitalization was associated with increased risk of stroke recurrence and future MACE (HR: 1.12, 95%CI: 1.06–1.19 and HR: 1.06, 95% CI: 1.01–1.12, respectively per day to PAF detection) (Table 3 and Figure 2).
Discussion
The present study shows that restoration of sinus rhythm in acute ischemic stroke patients with in-hospital episodes of paroxysmal AF, is associated with better cardiovascular outcomes during a long-term follow-up. Both self-terminated episodes of PAF and medically converted PAF were associated with lower mortality and MACE, while self-terminated PAF episodes were associated with lower risk of ischemic stroke recurrence.
Although several observational studies have shown that post-stroke AF did not affect the risk of stroke recurrence compared to those with known AF,12,13 others showed that post-stroke AF was related to higher risk of recurrent stroke and mortality on follow-up compared to those with known AF. 6 A nationwide cohort analysis found that early initiation of rhythm control was associated with a lower risk of adverse cardiovascular outcomes, compared to rate control amongst patients with recently diagnosed AF. 14
Our analysis showed that self-terminated episodes of PAF in acute ischemic stroke patients were associated with 42% reduction of mortality, 57% reduction in ischemic stroke recurrence, and 58% reduction of the risk of MACE compared to patients with sustained AF. Rhythm control therapy, resulting in PAF conversion, was associated with 33% reduction in mortality risk and 43% reduction in the risk of MACE compared to sustained AF, while PAF conversion was associated with a 34% non-significant reduction of recurrent ischemic stroke risk. However, given the large effect estimate for the outcome of ischemic stroke recurrent in ischemic stroke patients treated to restore sinus rhythm, we cannot exclude a potential effect of medical sinus rhythm restoration in the reduction of ischemic stroke recurrence. In line to our results, the EAST-AFNET 4 trial recently showed that a rhythm control strategy in patients with AF and previous stroke or AF and increased risk for cardiovascular events, significantly reduced stroke risk and cardiovascular death, a finding which remained significant also in the subgroup of patients with previous stroke. 10 Recently, the Risk and Benefits of Urgent Rhythm Control of Atrial Fibrillation in Patients With Acute Stroke (RAFAS) randomized trial recently showed that early rhythm control strategy in patients with acute ischemic stroke and AF decreased the risk of recurrent stroke within 12 months (HR: 0.215, 95% CI: 0.05–0.89), without an increase in the composite adverse outcomes. 15
The association of SR restoration, either due to PAF self-termination or due to the medical conversion PAF, with improved outcomes of patients with acute stroke and PAF could be attributed to several factors. The development of PAF during the acute phase of stroke could cause hemodynamic instability because of the irregular ventricular rate, the loss of atrial contribution to the ventricular filling, the lower blood pressure with consequent reduction in the cerebral blood flow. 16 AF is also associated with an increase in blood pressure variability which is a poor prognostic factor in the acute phase of stroke.16,17 Even short-term episodes of PAF may contribute to the formation of thrombi in the left atrium and therefore increase the risk of stroke recurrence. 18 Permanent AF after stroke is associated with increased risk of stroke recurrence, while pathophysiological and epidemiological evidence suggest an increasing risk of sudden cardiac death.19–21 In line with these results, we showed that in the acute phase of ischemic stroke, compared to patients with sustained AF, patients with self-terminated PAF or those who underwent medical SR restoration, had lower risk of cardiovascular events and mortality. Interestingly, self-terminated PAF was associated with numerically lower cardiovascular event rates during follow-up compared to those underwent medical SR restoration. This finding is potentially attributed to a lower AF burden and subsequently lower burden of atrial cardiopathy, as seen in patients with PAF, which in turn is associated with lower risk of stroke recurrence and mortality.19,22–24 Thus, in our study, self-termination of PAF or the potential response to medical SR restoration in patients with PAF after ischemic stroke may reflect patients’ AF burden and the underlying atrial changes, which correlate to lower cardiovascular events.
An interesting finding in our study was that the detection of PAF later during hospitalization was associated with increased risk of stroke recurrence and MACE. There has been extensive discussion about whether post-stroke PAF is a consequence of neurogenic mechanisms related to brain damage or is the cause of stroke. Several studies support the hypothesis that ischemic stroke, especially with insular involvement, impairs the autonomic regulation and may cause short and potentially “benign” PAF episodes, mainly in the early days after the ischemic stroke. 25 “Neurogenic” PAF may serve as a potential explanation of the lower or similar risk of stroke recurrence compared to patients with known AF.1,7,13 In our study PAF was detected in most of the cases during the first days of hospitalization and taking into account that later PAF detection was associated with higher risk of recurrent stroke and MACE, we cannot exclude the possibility that episodes especially early after the index event may be related to the index stroke. This finding supports the notion of the stroke-related heart syndrome, although without providing any evidence on the potentially “benign” nature of these episodes. On the contrary, in this study patients who were treated with anticoagulants at discharge, irrespective of SR restoration, had a significant reduction in stroke recurrence and MACE risk compared to those who were not discharges on anticoagulants, a finding which indicates the effectiveness of anticoagulant therapy in PAF detected both in the early and late phase after the index event. A quarter of our patients did not restore SR and were discharged with sustained AF, which implies a potential underlying pathology of the cardiac atria. Additionally, although more than 60% in every group had an ischemic stroke with insular involvement, this finding was similar in patients with and without restored sinus rhythm.
Study limitations
This was a single-center prospective observational hospital-based registry with some additional data gathered retrospectively representing a potential selection bias and confounding by indication, although the two groups, patients with SR restoration or not did not differ regarding baseline characteristics. Although PAF was identified prospectively in the majority of the included patients, in some patients it was documented retrospectively, and some cases may have been missed. Echocardiography was not applied universally to all patients. Echocardiographic and markers of atrial cardiopathy (such as P wave terminal force in lead V1 or natriuretic peptide) which could provide further pathophysiologic insights on the effect of atrial cardiopathy in those patients, were not included in the analysis. Treatment choices were based on the decision of the treating physician taking into account patient’s comorbidities and stroke severity, while the time of initiation of antiarrhythmic treatment and time to SR restoration were not documented. In-hospital rhythm monitoring was not universally documented in our study and thus may have affected AF detection rates and the association of AF burden with SR restoration and cardiovascular outcomes. Despite that our patients followed up regularly, we did not perform systematic screening for AF on follow-up, and this may have led to poor documentation of AF relapse in patients with SR restoration. Finally, compliance and adherence to treatment after discharge was not universally documented and may have affected the outcomes of the study.
Conclusion
In patients with first-ever acute ischemic stroke and in-hospital episodes of PAF, self-termination of AF and medical sinus rhythm restoration was associated with better cardiovascular outcomes in follow-up. These findings support the importance of a rhythm control strategy in this patient group, but large randomized controlled studies are needed to provide more solid evidence.
Supplemental Material
sj-docx-1-eso-10.1177_23969873221109405 – Supplemental material for Sinus rhythm restoration and improved outcomes in patients with acute ischemic stroke and in-hospital paroxysmal atrial fibrillation
Supplemental material, sj-docx-1-eso-10.1177_23969873221109405 for Sinus rhythm restoration and improved outcomes in patients with acute ischemic stroke and in-hospital paroxysmal atrial fibrillation by Dimitrios Sagris, Eleni Korompoki, George Ntaios, Stylianos Tzeis, Efstathios Manios, John Kanakakis, Haralampos Milionis, Panagiotis Papanagiotou, George Andrikopoulos, Gregory YH Lip and Konstantinos Vemmos in European Stroke Journal
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. D. Sagris reports no disclosures, Dr. E. Korompoki reports no disclosures, Dr. G. Ntaios reports speaker fees/advisory boards/research support from: Abbott; Amgen; Bayer; BMS/Pfizer; Boehringer-Ingelheim; Elpen; Galenica. All fees are paid directly to his institution (University of Thessaly), Dr. S. Tzeis reports no disclosures, Dr. E. Manios reports no disclosures, Dr. J. Kanakakis reports no disclosures, Dr. H. Milionis reports speaker fees/advisory boards/research support from: Alexion, Amgen, AstraZeneca, Bayer, Elpen, Genesis Pharma, MSD, Pfizer, Sanofi, Servier, Viatris, Winmedica, Dr. P. Papanagiotou: reports no disclosures, Dr. G. Andrikopoulos reports speaker fees/advisory boards/research support from: AstraZeneca, Abbot, Bard, Bayer Healthcare, Boehringer Ingelheim, Boston Scientific, Bristol-Myers Squibb, ELPEN, Galenica, Lilly, Medtronic, Menarini, MSD, Pfizer, Sanofi, Servier, StJude, Unifarma, and Vianex, Dr. GY Lip: consultant and speaker for BMS/Pfizer, Boehringer Ingelheim and Daiichi-Sankyo. No fees are received personally, Dr. K. Vemmos: reports speaker fees/advisory boards from: Amgen; Bayer; BMS/Pfizer; Boehringer-Ingelheim; Elpen.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Alexandra Hospital ethics committee.
Informed consent
Written informed consent was obtained from all subjects before the study.
Guarantor
KV.
Contributorship
Dr. Sagris: data acquisition, statistical analysis and interpretation, manuscript preparation. Dr. Korompoki: data acquisition, statistical analysis and interpretation, manuscript preparation. Dr. Ntaios: interpretation, manuscript preparation, and critical revision of the manuscript. Dr. Tzeis: interpretation, manuscript preparation, and critical revision of the manuscript. Dr. Manios: data acquisition, interpretation, and critical revision of the manuscript. Dr. Kanakakis: interpretation and critical revision of the manuscript. Dr. Milionis: interpretation and critical revision of the manuscript. Dr. Papanagiotou: interpretation and critical revision of the manuscript. Dr. Andrikopoulos: interpretation and critical revision of the manuscript. Dr. Lip: interpretation and critical revision of the manuscript. Dr. Vemmos: study concept and design, data acquisition, statistical analysis and interpretation, manuscript preparation, study supervision.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.