
Abstract
Background:
Paroxysmal atrial fibrillation (PAF) is strongly associated with ischemic stroke. Continuous cardiac implantable electronic devices (CIEDs) can assess PAF episodes over prolonged periods. Studies that attempted to find a temporal association between PAF and ischemic stroke were inconclusive. Thus, we performed a systematic review and meta-analysis to assess this relationship.
Aims:
This study aimed to assess the temporal association between AF episodes and stroke within 30 days of the arrhythmic episode. The secondary outcome is a temporal association within a 90-day period.
Summary of review:
A total of 2804 studies that discussed the temporal relationship between PAF and ischemic stroke were screened, and 7 studies were included in the meta-analysis. Among the 4041 patients included in these studies, there were 138 patients with device detected PAF episodes and stroke. Four studies used a 30-day window for temporality and the pooled odds ratio (OR) showed a significant association (OR 4.11 (95% CI 1.03–16.40)). The three studies reporting on AF and stroke within a 90-day window did not find a significant temporal relationship (OR 0.43 (95% CI 0.13–1.41)). Finally, the pooled result of those seven studies did not show a significant association (OR 1.51 (95% CI 0.44–5.17)).
Conclusion:
This meta-analysis supports a temporal relationship between PAF and ischemic stroke within a 30-day window. Establishing this relationship is important for individualized risk prediction and targeted anticoagulation treatment.
Data access statement:
The data will be made available upon reasonable request.
Introduction
Atrial fibrillation (AF) affects 46.3 million people worldwide and is strongly associated with ischemic stroke and mortality.1–3 Both symptomatic and asymptomatic AF (occurring in up to 40% of patients), and permanent and paroxysmal AF increase stroke risk. 4 Continuous cardiac implantable electronic devices (CIEDs) allow clinicians to measure the presence and length of the episodes of AF over a prolonged period. Several studies using CIEDs have attempted to find a temporal association with stroke. A post hoc analysis of the ASSERT trial did not find a temporal relationship, whereas a recent case-crossover study found a strong association, especially within 30 days of an AF episode.1,2
These contradictory findings may be due to differences in study design, anticoagulation rate, the temporal window considered between the AF episode and stroke, and the duration of the AF episodes considered relevant. Establishing this temporal relationship is important to permit individualized risk prediction and targeted anticoagulation treatment.
Given these findings, we performed a systematic review and meta-analysis of the literature to assess whether there is a temporal relationship between episodes of AF and ischemic stroke.
Methods
Search strategy and selection criteria
We reported this systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. The search protocol was published at the International Prospective Register of Systematic Reviews (PROSPERO), ID CRD42022336171.
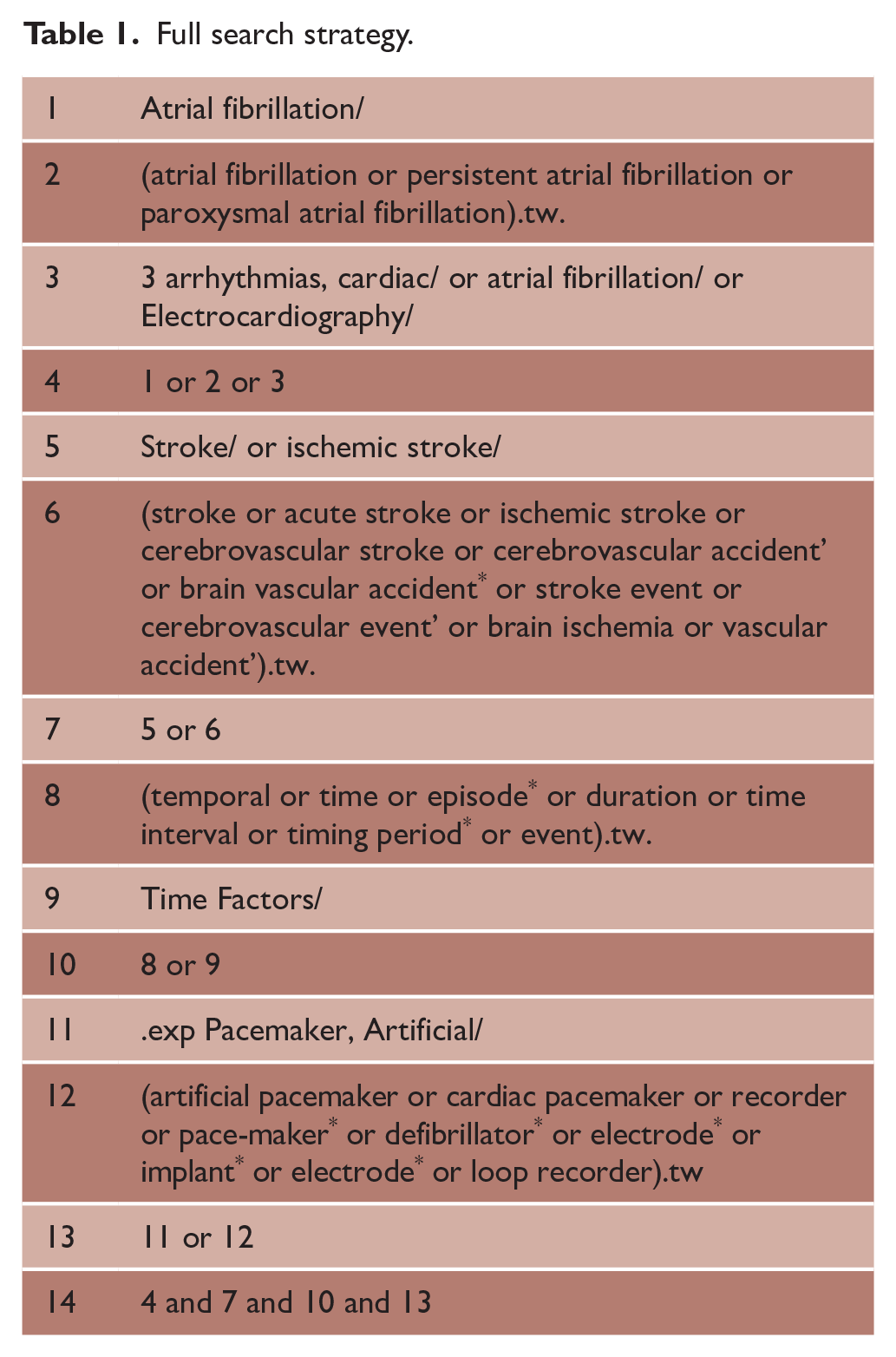
A comprehensive structured literature search was performed using MEDLINE (OVID), EMBASE (OVID), and Cochrane Database of Systematic Reviews from database inception to 7 June 2022. The search strategy included keywords relating to: atrial fibrillation, ischaemic stroke, temporality and long term cardiac monitoring devices (see Table 1).
Full search strategy.
Inclusion and exclusion criteria
To be eligible for inclusion, studies needed to be (1) written in English, (2) have participants ⩾ 18 years of age, (3) heart rhythm monitored with an implantable monitoring device (pacemaker (PM), implantable loop recorder (ILR), cardiac resynchronization therapy (CRT), implantable cardio defibrillator (ICD), (4) embolic event as the endpoint or outcome (ischemic stroke), and (5) recording of any duration of AF/Atrial tachycardia (AT)). Studies were excluded if they (1) reported on permanent AF, (2) were reviews, case reports, case studies, or research letters to editor unless containing original data, (3) did not discuss any temporal relationships between AF and stroke, or (4) if embolic events were exclusively systemic emboli- or cardiac- or pulmonary-related.
Study selection and data extraction
We used an online systematic review platform (Covidence, Veritas Health innovation Ltd, Melbourne Australia) to screen and extract data. Three investigators (A.M.B., T.S.R., and J.D.) identified potentially eligible studies while a fourth (V.T.) resolved any disagreements. Study selection was performed by the authors using a priori determined criteria.
The primary outcome for the meta-analysis was based on studies reporting a temporal association between AF episode and stroke within 30 days of the AF episode. The secondary outcome was a temporal association between AF episode and stroke within a 90-day time period. Additional variables analyzed included age, prior stroke, CHA2DS2-VASc score, and duration of AF.
Two reviewers (J.D. and A.M.B.) independently extracted the data from the selected studies after full-text revision. The data were then compared, and discrepancies were resolved by revision of the studies followed by consensus. Baseline characteristics were extracted from the overall population, including age, sex, CHADS2 and CHA2DS2-VASc scores, diagnosis of hypertension, heart failure, prior stroke or transient ischemic attack (TIA), diabetes mellitus, coronary artery disease, peripheral vascular disease, chronic obstructive lung disease, Charlson Comorbidity Index, and oral anticoagulation. The stroke subtypes (ischemic, hemorrhagic, or both), duration of follow-up, and anticoagulation at the end of the study were also noted. Regarding the method of AF detection, extracted data included the device type, atrial arrhythmia electrograms detection (bpm), AF threshold burden (minutes or hours), temporal window examined, number of AF/AT episodes, AF average daily burden, duration of last episode before stroke, and duration of the longest episode.
Risk of bias and quality assessment
The risk of bias was independently assessed by two investigators using the Risk of Bias In Non-randomized Studies—of Exposure tool (ROBINS-E) (Supplemental Table S1). 3
Statistical analysis
Individual study characteristics were summarized prior to quantitative analysis. Studies not meta-analyzed were included in the narrative synthesis. The effect size was measured using odds ratios (ORs) with corresponding 95% confidence intervals (CIs), and log OR and log CI were calculated from the original studies. We performed a random-effects analysis using restricted maximum likelihood (REML) with the Hartung–Knapp adjustment to estimate the between-study heterogeneity. This model was used to allow for study-specific effects rather than considering a common effect across studies. Results were presented in Forest plots. The statistical heterogeneity was estimated using the I2 statistic and considered low if the I2 was less than 25%, moderate if around 50%, and high if greater than 75%. Publication bias (small-study effect) was evaluated using funnels plots with Egger’s test for asymmetry.
Pre-specified meta-regression analysis was performed to assess for potential contributors for the observed effect size. The variables used in our random-effects meta-regression with analysis were age, prior stroke, CHA2DS2-VASc score, and duration of AF. We considered a p-value less than 0.05 to be significant. All statistical analyses were performed using Stata 17.BE (StataCorp, College Station, Tx, USA).
Results
The online search yielded 3704 citations from date of inception to 30 June 2022 from MEDLINE, EMBASE, and Cochrane. Hand searching yielded an additional one citation. Of these, 901 duplicates were removed, and 2602 citations were excluded as they did not meet the inclusion criteria. A total of 201 studies were identified for full-text review, and after removal of 186 studies, 15 were included in the final analysis and 7 in the meta-analysis (see Figure 1). Among the 15 included studies, there were a total of 11,878 patients with a mean age of 75.6 years. A history of stroke was present in 2913 patients. Eight studies were observational,2,4–10 two were randomized control trials,11,12 and two used a case-crossover design.1,13 One study used a prospective cohort design, 14 one was a case–control study, 15 and one was a cohort study. 16 The devices used in the studies of this review include dual-chamber PM, ICD, implantable cardiac monitors, biomonitors, and ILR.
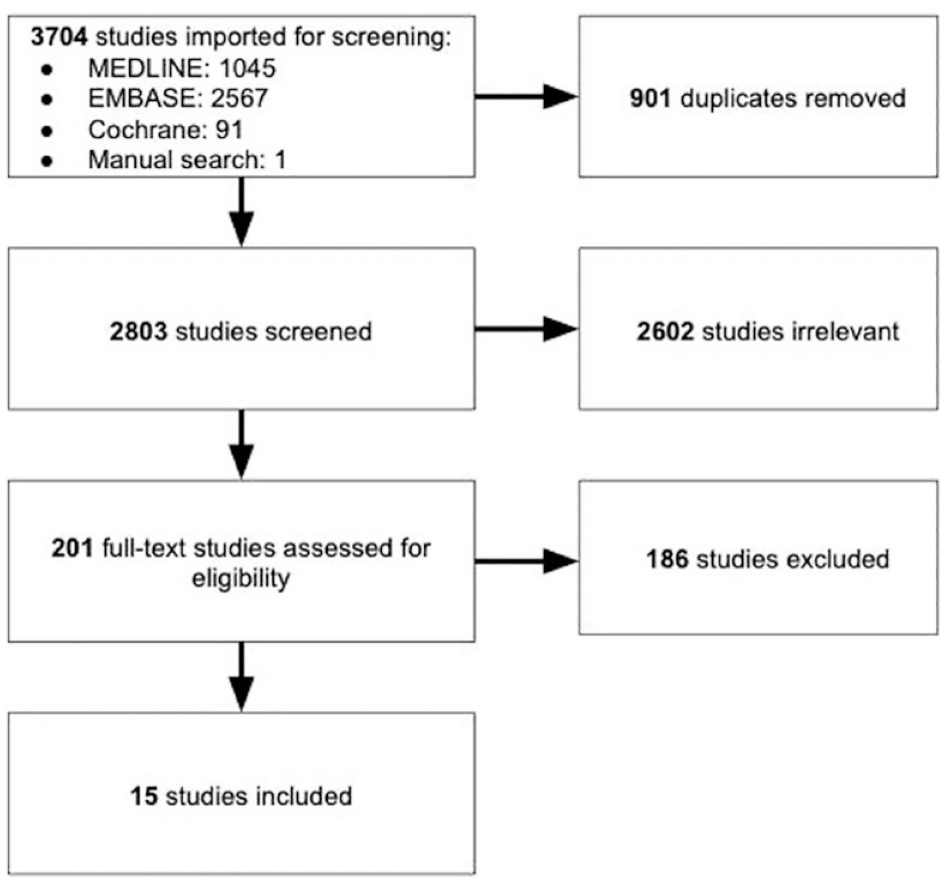
PRISMA flow diagram.
Baseline characteristics
The baseline characteristics of participants are included in Table 2. The median age of participants was 74.3 years, and the median CHA2DS2-VASc score of 4.5 was provided by 11 of the 15 studies included. Hypertension was a common comorbidity of patients included, with 78.44% reported at the time of study inclusion. In addition, 28.68% of included participants experienced a prior stroke or TIA.
Baseline characteristics.
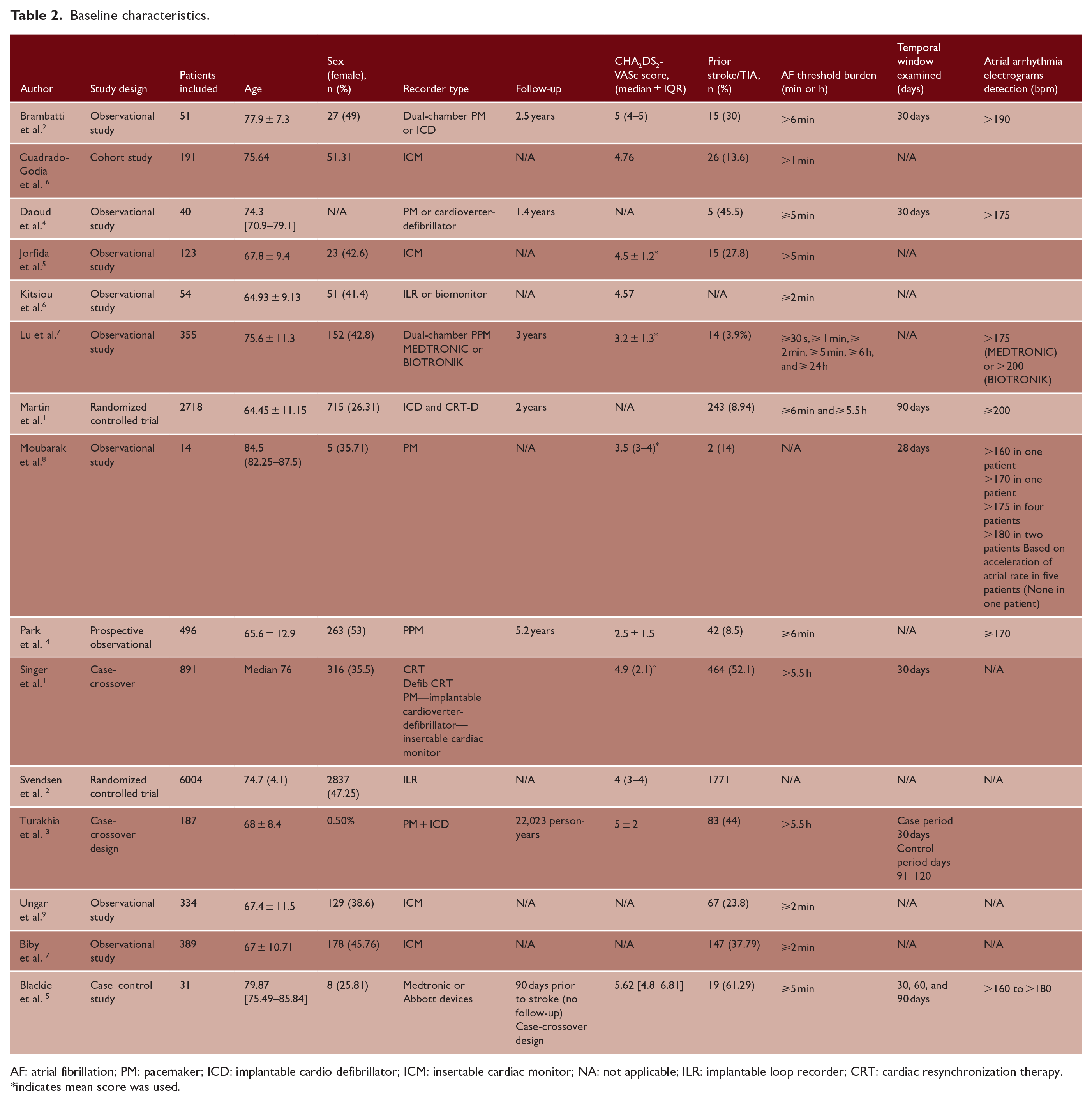
AF: atrial fibrillation; PM: pacemaker; ICD: implantable cardio defibrillator; ICM: insertable cardiac monitor; NA: not applicable; ILR: implantable loop recorder; CRT: cardiac resynchronization therapy.
indicates mean score was used.
Temporal relationship
Among the seven studies that discussed a temporal relationship between AF and stroke, four reported on stroke within 30 days and three reported on stroke within 90 days (Figure 2). When assessing the four studies using a 30-day window for temporality, the pooled OR is 4.11 (95% CI 1.03–16.40). The studies reporting on AF within 90 days did not find a significant relationship. The pooled result for the seven studies did not find a significant association (OR 1.51 (95% CI 0.44–5.17)). The statistical heterogeneity was high for the three analyses, as shown on Figure 2.
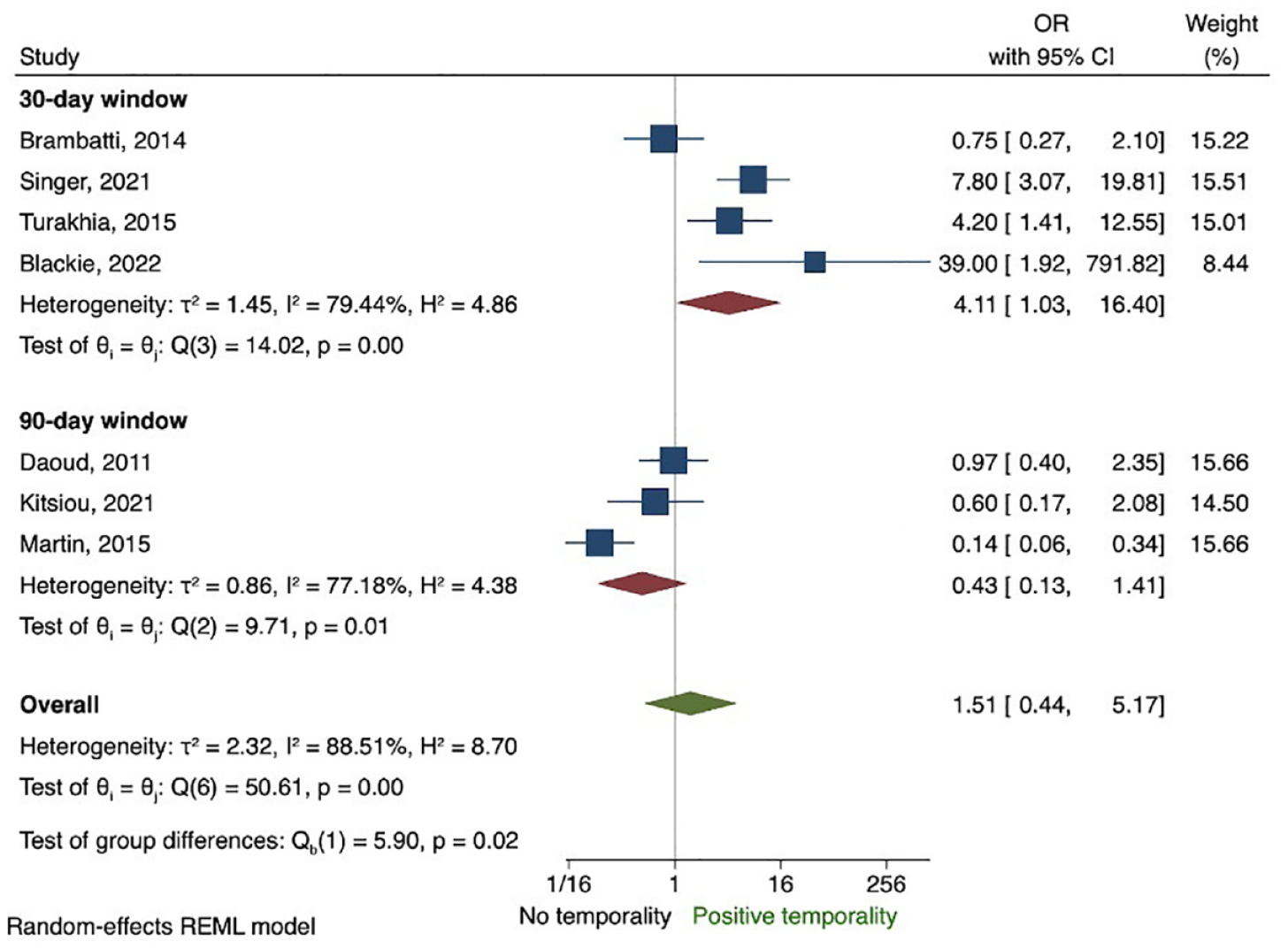
Forest plot analyzing the temporal relationship between episodes of AF and stroke within 30 and 90 days.
Meta-regression
In the linear meta-regression, we identified a linear and significant (p < 0.05) association between the variables of CHA2DS2-VASc score, duration of AF, and percentage of participants with a prior stroke (Figure 3). A non-significant association was indicated for participant age (coefficient 0.17, 95% CI −0.03 to 0.36, p > 0.05).
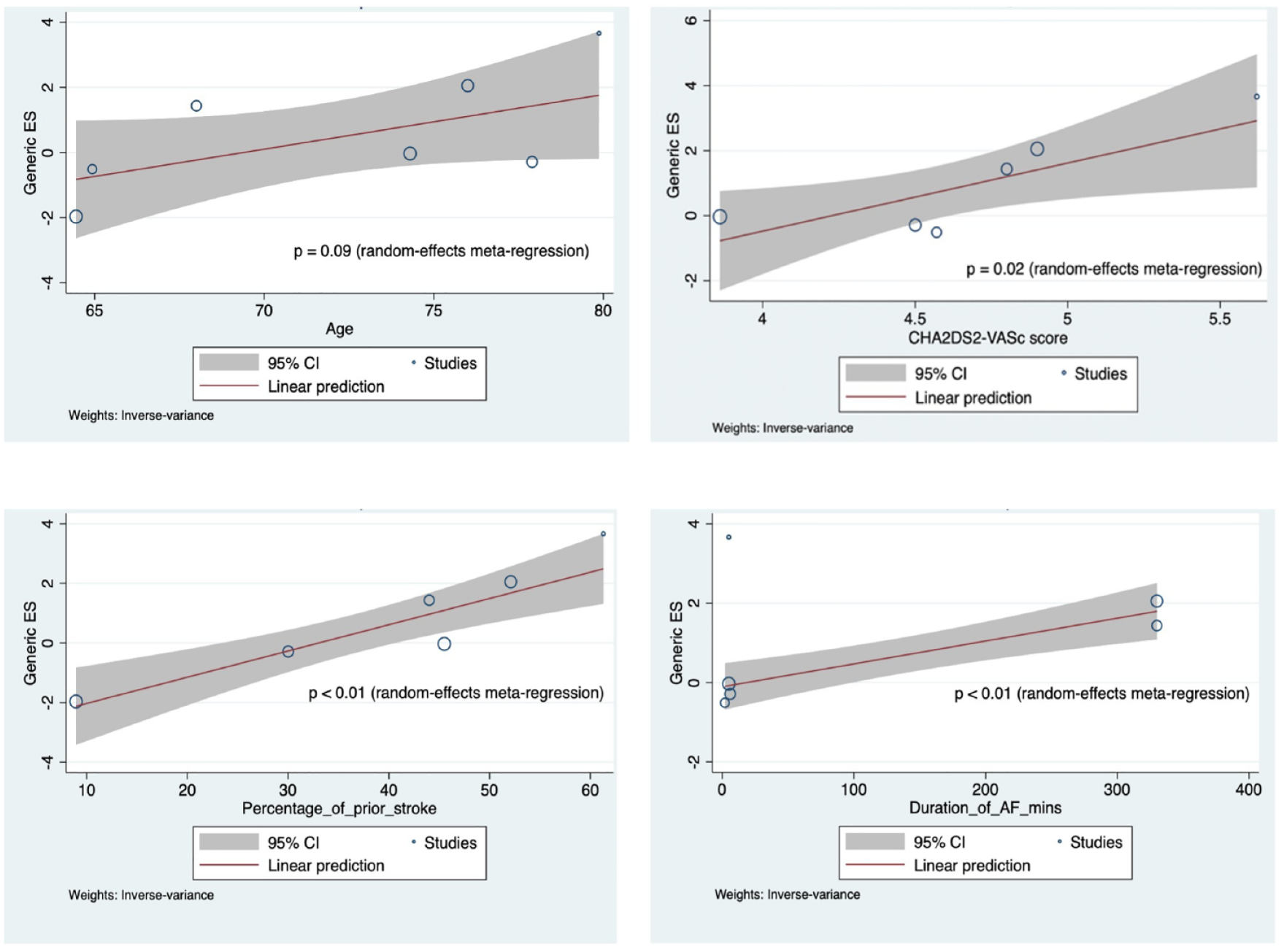
Bubble plot of meta-regression variables (age, duration of AF, CHA2DS2-VASc score, duration of AF, and percentage of participants with a prior stroke).
Publication bias
Risk of publication bias was assessed by inspection of an Egger’s test for funnel plot asymmetry which yielded a p-value of 0.09, indicating a low risk of publication bias in this meta-analysis (Figure 4).
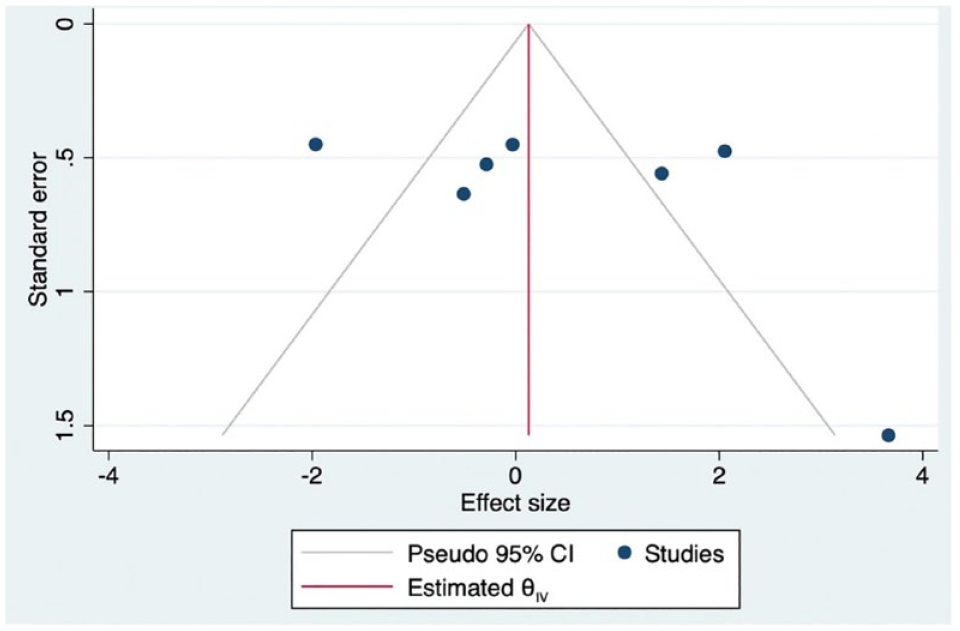
Risk of publication bias assessed via inspection of Egger’s test.
Discussion
Detected AF is highly prevalent in patients with CIEDs, and its relationship with ischemic stroke has been widely examined. There are, however, inconsistent findings within the literature regarding this temporal relationship. Due to this, there is limited utility within clinical settings and uncertainty regarding its implications and therapeutic direction. This systematic review and meta-analysis demonstrate that there is a pooled OR 4.11 (95% CI 1.03–16.40) suggesting an increase in the risk of developing a stroke after an episode of AF of any duration within 30 days. This risk decreases when the time window is extended to 90 days with the overall OR 1.51 (95% CI 0.44–5.17).
Length of the temporal window: 30 versus 90 days
Among the 15 studies initially extracted from the original screening process, 7 were used for the meta-analysis. Many studies lacked data relating to the temporal relationship between episodes of AF and stroke and instead reported only first AF episode detected, longest AF episode, or time from implantation to first episode.7,15 Most studies did not provide justification for the temporal window chosen for analysis while some cited periods > 30 days would be an unlikely source of cardiac thrombi as it would likely undergo dissolution or fibrosis. 12
Among the seven studies included in the meta-analysis, three studies had OR values > 1 and four studies had values < 1. Among these studies, three examined the relationship between AF and stroke occurrence within a 30- to 90-day window. All reported OR values < 1, indicating no association between AF during that 90-day period and the incidence of stroke. The other four studies focused on the association between AF and stroke within a 30-day window, with three reporting OR values > 1. The study by Brambatti et al. was the only one in this subgroup with an OR value < 1. Notable differences across these studies included the proportion of female participants and the study designs; the latter study was observational, while the others were case-crossover or case–control studies. Variables such as the age of participants, CHA2DS2-VASc scores, and types of recorders used were similar across the studies.
The overall trend of increasing OR as the time window decreased suggests that there is a stronger temporal relationship when the duration between AF and stroke is reduced. Blackie et al. examined the OR in windows of 30, 60, and 90 days. Their work supports this hypothesis as the OR decreased as the time windows after the AF episode increased, with OR 39 (95% CI 1.92–791.45), 20.65 (95% CI 1.00–427.66), and 6.07 (95% CI 0.94–39.04), respectively. 14 Furthermore, a recently published registry-based retrospective study showed that 5.5% of included patients had ischemic stroke temporally associated with AF, defined as stroke occurring 30 days prior to 30 days after a new-onset AF diagnosis. 18 Interestingly, this study found that 80.1% of those strokes were recorded in 0–30 days after AF.
Two studies used a case-crossover study design assigning a period of analysis from days 1 to 30 prior to stroke and using a control days 90–120 days pre-stroke. However, episodes of AF occurred in both the control and analysis periods making it difficult to determine if there is a true temporal relationship or it is the effect of ongoing AF.1,12 The meta-regression suggests that there is a stronger association in the temporal relationship between stroke and AF in patients with a higher CHA2DS2-VASc score, duration of AF, and percentage of participants with a prior stroke.
Atrial cardiomyopathy and AF
Growing evidence suggests the inconsistencies in the OR values could be attributed to or explained by atrial cardiomyopathy in which the atrium is predisposed to thrombus formation in the absence of AF. 16 It is suggested that AF may be a marker of stroke risk rather than a causative agent and that AF itself is a presentation of left atrial functional and structural abnormalities. 18 The recently published The Atrial Cardiopathy and Antithrombotic Drugs in Prevention After Cryptogenic Stroke (ARCADIA) trial compared the efficacy of anticoagulation with apixaban to antiplatelet therapy with aspirin for preventing recurrent stroke in 1015 adults with cryptogenic stroke and atrial cardiopathy. 19 After a mean follow-up of 1.8 years, there was no significant difference between the studied groups and the trial was stopped for futility after interim analysis. The relationship between AF, stroke, and atrial cardiomyopathy, however, remains unclear, and further research is warranted to investigate this relationship.
Variations in anticoagulation, AF threshold burden, and duration and patient demographics
Most studies had inconsistencies in the criteria oral anticoagulation (OAC) use or did not report the percentage of patients currently on OACs. This is likely to have impacted the study results as OAC use has been shown to reduce the risk of stroke by 64% in patients with AF. 20 Varying study AF detection rates and duration of AF recorded were prevalent among the studies included. This may have contributed to the inconsistencies within the results as some studies had minimum AF detection thresholds from > 5.5 min while other studies only included AF episodes greater than > 5.5 h. Short threshold burdens may increase the risk of false positives, incidental AF or clinically irrelevant AF. However, this should be balanced with longer durations as it risks underreporting the significance of shorter episodes of AF.
The studies analyzed had varying patient populations and devices used for monitoring periods of AF. Some studies excluded patients who had prior episodes of AF or atrial flutter and used either a dual-chamber PM, ILR, or ICD while other studies included patients who had documented AF prior to enrollment. Analysis of patient characteristics did not reveal any associations between the type of monitoring device and a temporal relationship.2,4,6
Only one study specified that patients with permanent AF were excluded in their criteria; however, other studies did not specify its nature. Categorizing episodes of AF particularly in stroke can help guide future monitoring and anticoagulation for patients. 21 In addition, patient demographics, such as a history of prior stroke, had a strong association to the temporal relationship between ischemic stroke and AF (Figure 3). The percentage of patients with a prior stroke varied greatly from 8.9% 11 to 61.9%, 15 and results from the meta-analysis suggest that a history of prior stroke has a stronger temporal association between stroke and AF.
Variation in methodology
Study population recruitment in some studies occurred from identification within stroke populations and subsequent cross-linking to CIED registries. 15 While this enables identification of individuals that experienced a stroke and had an implantable monitoring device, it does not provide information on populations with monitoring devices who did not experience a stroke. Without comparison between the two populations, it is difficult to ascertain a true temporal relationship between AF and stroke.
The statistical heterogeneity was high for the 30-day window, 90-day window, and overall analyses, highlighting the high degree of variation among the included studies. The main differences include study design, sample size, population characteristics, and outcomes measured. First, sample size ranged from 40 to more than 2700 subjects. The mean or median age of those samples ranged between 64 and 80 years old. The significance of this difference lies in the fact that AF prevalence increases markedly with age: it affects 6.4% of adults aged 65–69 years, in contrast to 28.5% of those aged 85 years. 22 Furthermore, the percentage of females included in the study samples ranged from 26% to 49%, a significant observation as mounting evidence indicates that female gender constitutes an additional risk factor for stroke. 23 Significant variations among the studies include the research design and the type of recorder used. Moreover, there was inconsistency in the measured outcomes regarding the AF duration threshold (ranging from 2 min to 5.5 h), the AF detection rate threshold (ranging from 160 to 200 beats per minute), and the duration of the monitoring period (with five studies using a 30-day window and two studies using a 90-day window).
Study population recruitment in some studies occurred from identification within stroke populations and subsequent cross-linking to CIED registries. 14 While this enables identification of individuals that experienced a stroke and had an implantable monitoring device, it does not provide information on populations with monitoring devices who did not experience a stroke. Without comparison between the two populations, it is difficult to ascertain a true temporal relationship between AF and stroke.
Translation into clinical practice
AF has been associated with an increased risk of stroke with clinicians prescribing OACs for the prevention of thromboembolic events. However, there is mixed evidence in relation to when clinicians should prescribe oral anticoagulation, and what duration of AF should warrant medication. There appears to be little distinction between paroxysmal AF and asymptomatic AF in relation to anticoagulation advice as there are no set guidelines of what determines a “clinically relevant” episode of AF. 24 The meta-regression identified a positive linear relationship for the risk of stroke and CHA2DS2-VASc score. Identifying these patients may guide clinicians on anticoagulant use, helping determine in which patients thromboembolic prophylaxis would be useful and where oral anticoagulation may not. Individualizing drug treatments to patients can maximize treatment outcomes and tailor strategies to reduce AF thromboembolic consequences on the individual risk profile. Another potential implication of defining the temporal relationship between AF and stroke is its role in the reduction of adverse events after surgery. Patients who experience an episode of AF may have an increased risk of post-operative complications after surgery compared to those without AF prior to surgery. Further research is warranted to categorize the type of AF and quantify the temporal relationship to surgical outcomes. In future, this may guide timing of elective surgical procedures based on periods of high and low risk determined by episodes and duration of AF. 25
Recommendations for future research
To determine if there is a true temporal relationship between AF and stroke, future studies need to adopt consistent methodologies to enable accurate detection. Temporal windows of analysis, control for anticoagulation use, and AF threshold and duration should be made consistent among studies to allow studies to accurately determine the temporal relationship between stroke and AF. In addition, sampling the study population should include population with/without CIEDs and strokes to allow comparison between both populations and avoid inherent bias.
Limitations
Within the included studies, there was no distinction between AF/AT as many studies grouped both episodes together. In addition, there was very little information relating to anticoagulant use, despite its importance. Without this, we were unable to conduct an analysis on this and its subsequent implications on the temporal relationship. In addition, there was limited information on the burden of AF over time, limiting analysis on the frequency and total number of episodes experienced by patients. Furthermore, it should be noted that a potential reason for the inconclusive relationship between AF and ischemic stroke was that patients with stroke causes other than cardio-embolic associated with AF were not excluded. Finally, articles were limited to the English language.
Conclusion
There is increasing evidence to suggest there is a temporal relationship between AF and stroke, particularly within a 30-day window. However, future research is warranted to ensure consistencies in anticoagulation use, AF duration, and detection threshold. Furthermore, future studies should examine the role of atrial cardiomyopathy and its implications within AF and stroke.
Supplemental Material
sj-jpg-1-wso-10.1177_17474930241253482 – Supplemental material for Temporal association between atrial fibrillation and ischemic stroke: Systematic review and meta-analysis
Supplemental material, sj-jpg-1-wso-10.1177_17474930241253482 for Temporal association between atrial fibrillation and ischemic stroke: Systematic review and meta-analysis by Jessica D’lima, Vincent Thijs, Han S Lim, Thalys Sampaio Rodrigues and Ann-Marie Beaudoin in International Journal of Stroke
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: V.T. receives consulting fees from Medtronic and lecture, and consulting fees from Boehringer Ingelheim and Bayer. H.S.L. reports having received research support from St Jude Medical (now Abbott).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.