
Abstract
We aimed to provide practical recommendations for the screening of subclinical atrial fibrillation (AF) in patients with ischaemic stroke or transient ischaemic attack (TIA) of undetermined origin. These guidelines are based on the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) methodology. Five relevant Population, Intervention, Comparator, Outcome questions were defined by a multidisciplinary module working group (MWG). Longer duration of cardiac rhythm monitoring increases the detection of subclinical AF, but the optimal monitoring length is yet to be defined. We advise longer monitoring to increase the rate of anticoagulation, but whether longer monitoring improves clinical outcomes needs to be addressed. AF detection does not differ from in- or out-patient ECG-monitoring with similar monitoring duration, so we consider it reasonable to initiate in-hospital monitoring as soon as possible and continue with outpatient monitoring for more than 48 h. Although insertable loop recorders (ILR) increase AF detection based on their longer monitoring duration, comparison with non-implantable ECG devices for similar monitoring time is lacking. We suggest the use of implantable devices, if feasible, for AF detection instead of non-implantable devices to increase the detection of subclinical AF. There is weak evidence of a useful role for blood, ECG and brain imaging biomarkers for the identification of patients at high risk of AF. In patients with patent foramen ovale, we found insufficient evidence from RCT, but prolonged cardiac monitoring in patients >55 years is advisable for subclinical AF detection. To conclude, in adult patients with ischaemic stroke or TIA of undetermined origin, we recommend longer duration of cardiac rhythm monitoring of more than 48 h and if feasible with IRL to increase the detection of subclinical AF.
Keywords
Introduction
Ischaemic stroke is among the leading causes of disability and death worldwide, 1 with a high risk of recurrence. Transient ischaemic attack (TIA), although itself not disabling, increases healthcare burden and causes anxiety to patients because of the elevated future risk of stroke. Establishing the most likely stroke aetiology forms the cornerstone for rational and effective secondary prevention. However, the aetiology cannot be determined in about one quarter of stroke patients despite adequate diagnostic evaluation (frequently termed ‘cryptogenic stroke’), including vessel and cardiac imaging studies, electrocardiogram (ECG), in-hospital cardiac telemetry and/or 24-to-48-h Holter-ECG monitoring. 2 Atrial fibrillation (AF) is the most common cardiac arrhythmia, affecting 1%–2% of the European population3,4 and is a frequent cause of ischaemic stroke, with increasing prevalence and incidence worldwide, especially in older patients. 4 Up to 25% of ischaemic strokes can be attributed to AF, either previously known or detected during the diagnostic in-hospital work-up or later ECG monitoring. Identification of AF is critical because oral anticoagulation is highly effective for prevention of ischaemic stroke recurrence. Moreover, ischaemic strokes due to AF are usually more severe compared to other stroke aetiologies.5,6 Stroke of undetermined origin is defined according to varying concepts; the definition of embolic stroke of undetermined source (ESUS) has acquired a prominent role, and specifically implies a proximal (often cardiac) embolic mechanism. 7 In patients with a stroke of undetermined origin prolonged cardiac rhythm monitoring is likely to increase the detection rate of subclinical AF,5,8–10 with potentially important therapeutic implications.
Anticoagulant treatment for the prevention of recurrent stroke and TIA due to AF is indicated only if AF is proven and documented by ECG; the decision to recommend anticoagulant treatment cannot be based on cerebral and neurovascular imaging alone.11,12 Therefore, identification of subclinical AF in patients with an ischaemic stroke or TIA of undetermined origin, who are likely to benefit from anticoagulant treatment, is an important goal. Given its frequently asymptomatic and paroxysmal occurrence, AF can be difficult to capture by traditional short-term monitoring approaches. Currently, there are several strategies for detection of subclinical AF, including: ECG at hospital admission; serial in-hospital ECGs; in-hospital continuous non-ambulatory and ambulatory monitoring (telemetry); inpatient or outpatient Holter monitoring; and the use of external ambulatory ECG recorders, varying from short repeated intermittent ECG (e.g. thumb-ECG) to continuous wearable recorders or implantable loop recorders that can be utilised for long-term monitoring lasting for weeks to years. 12
The aim of this Guideline document is to provide recommendations for physicians treating patients with an ischaemic stroke or TIA of undetermined origin in their management decisions regarding the detection of subclinical AF.
Methods
Composition and approval of the module working group
These guidelines were initiated and endorsed by the European Stroke Organisation (ESO) and supported by the Stroke Council of the European Society of Cardiology. A Module Working Group (MWG) was established, consisting of 10 members with relevant expertise: eight neurologists (AA, AMT, CHN, DJW, JP, KA, MP, MR), one cardiologist (RBS) and one research fellow in biomedical informatics (DZ). The composition of this group was approved by the ESO Guidelines Board and the ESO Executive Committee, based on a review of the intellectual and financial disclosures of the proposed members. The research and publication record on the guideline topic of the MWG members was also taken into account before approval.
Development and approval of clinical questions
The guidelines were developed using Grading of Recommendations, Assessment, Development and Evaluation (GRADE) methodology 13 and the ESO Standard Operating Procedure, 14 as described previously. 15 In brief, the MWG developed and agreed on a list of topics, and corresponding outcomes of clinical interest. The outcomes were rated as critical, important or of limited importance according to GRADE criteria.13,15 A series of PICO (Population, Intervention, Comparator, Outcome) questions related to the global list of outcomes were then developed by group consensus and approved by the ESO Guidelines board and the ESO Executive Committee.
Literature search
As suggested by the ESO Guidelines Board, these guidelines were specifically focussed on screening of subclinical AF in patients with stroke or TIA of undetermined origin. Therefore, studies focussing on all stroke subtypes were discarded during the literature search. For each question, systematic searches of the PubMed, Embase and Cochrane databases, covering the period from the inception of each database to 30 November 2021 were conducted by an ESO Guidelines methodologist, Avtar Lal (AL). AL, SL (ESO Guidelines Methodologist), MR and MP agreed on the search terms for each PICO question. Search terms and their corresponding Medical Subject Heading (MeSH) terms used to identify the articles are described in the Online Supplemental File. Groups of authors independently screened the titles and abstracts of publications identified from the searches and assessed the full text of potentially relevant studies. Two votes were required for each article and both literature selection steps.
For each question, a group of three MWG members (a ‘PICO group’) was formed to evaluate the available evidence. Meta-analyses of randomised-controlled trials (RCTs) or observational studies with a control group were performed using RevMan 5.4. When all studies that were meta-analysed together provided compatible effects estimates, those were used for meta-analyses. Otherwise, raw data was used.
Meta-analyses of AF detection rates in observational single arm studies were performed using MetaXL, a MicroSoft Excel tool allowing the meta-analysis of this kind of data. For these meta-analyses, when values were available for any AF or AF lasting at least 30 s, the latter was used since it is the most accepted threshold for treatment allocation and based on a consensus statement. 16 All meta-analyses were performed using random effects, yielding a pooled odds ratio (OR) or hazard ratio (HR). Forest plots were generated using R studio. The risk of selection, performance, detection, attrition and reporting biases in each RCT was assessed using the Cochrane Collaboration’s tool, 17 and heterogeneity across studies was assessed using Cochran’s Q (reported as a p value) and I2 statistics. 18 For each PICO question and each outcome, the quality of evidence was rated using the GRADE system as high, moderate, low or very low. 14 The relevant PICO group was responsible for reviewing the available data and formulating an evidence-based recommendation according to the GRADE evidence profiles and the ESO standard operating procedure. Given the low number of RCTs found in the literature search, the quality of evidence was selected by that corresponding with the most relevant outcome for the MWG, rate of detection of subclinical AF. The strength of the recommendation was derived from data from RCT. In addition, it was recommended by the ESO Guidelines committee that only one level of recommendation should be provided for each PICO, even if the strength was different for the diverse outcomes. An Expert Consensus Statement, based on voting by all MWG members, was presented where the PICO group considered that not enough evidence was available to provide evidence-based recommendations for situations in which practical guidance was needed for everyday clinical practice. Importantly, these Expert Consensus Statements should not be regarded as evidence-based recommendations since they only reflect the opinion of the MWG.
The Guidelines document was reviewed several times by all MWG members and modified using a Delphi approach until consensus was reached. The document was further reviewed and approved by two external reviewers, members of the ESO Guideline Board, and Executive Committee.
Results
The working group identified five areas relevant to clinical practice for which PICO questions were formulated: (i) longer duration of cardiac rhythm monitoring compared to a shorter duration; (ii) the addition of out-patient cardiac rhythm monitoring compared to in-hospital cardiac rhythm monitoring alone; (iii) implantable monitoring devices compared to any non-implantable external monitoring device; (iv) the presence of potential blood, echocardiographic, ECG or heart and brain imaging biomarkers, compared to their absence; (v) implantable monitoring devices, compared to any non-implantable external monitoring device in patients with patent foramen ovale (PFO).
The working group identified 14 outcomes of interest, of which AF detection (any duration) and recurrent ischaemic stroke were considered the most relevant outcomes (Table e2 in the Supplemental File). Relevance of the outcomes was determined by Delphi vote, ranging from 0 to 10. A mean score of the voting of all MWG members was calculated, and only outcomes with a score higher than 7 were considered for the literature search.
The study selection process for each of the PICO questions is outlined in Online Figures e1 to e5 and Tables e3 to e8 of the Supplement File.
Outcome: Detection of subclinical AF
Analysis of current evidence
The 30-day Cardiac Event Monitoring Belt for Recording Atrial Fibrillation After a Cerebral Ischaemic Event (EMBRACE) study randomly assigned 572 patients 55 years of age or older, without known AF, who had had a cryptogenic stroke or TIA within the previous 6 months (cause undetermined after standard tests, including 24-h ECG), to undergo additional non-invasive ambulatory ECG monitoring with either a 30-day event-triggered recorder (intervention group) or a conventional 24-h monitor (control group). The primary outcome was newly detected AF lasting 30 s or longer within 90 days after randomisation. AF lasting 30 s or longer was detected in 45 of 280 patients (16.1%) in the intervention group, whereas AF was detected in 9 of 277 (3.2%) in the control group (absolute difference, 12.9% points; 95% CI 8.0–17.6; p < 0.001). The number needed to screen was 8 (i.e. it was needed to perform prolonged cardiac monitoring in eight patients to detect one subclinical AF). 9
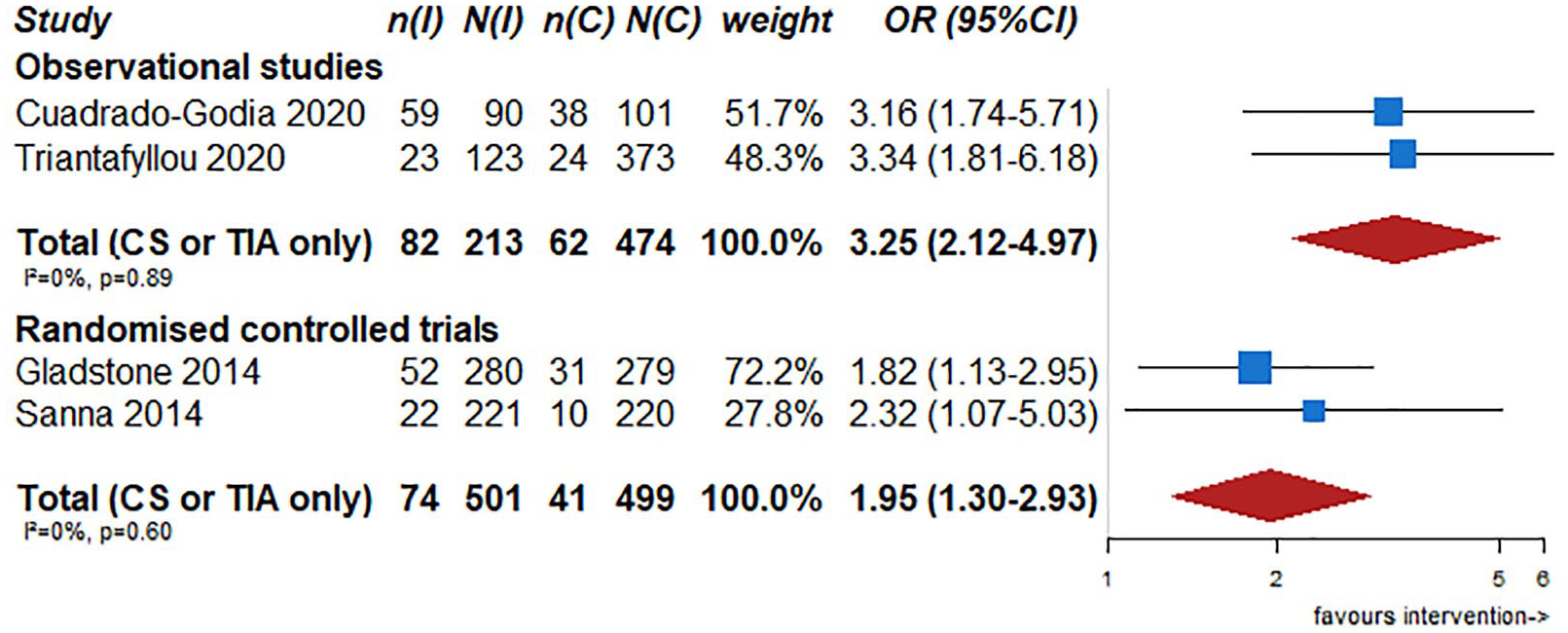
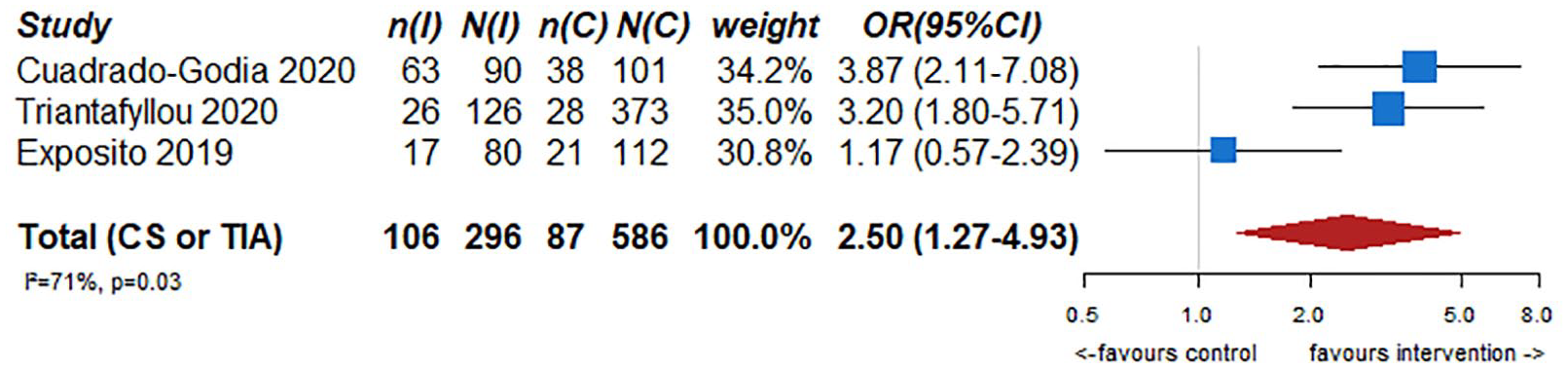
The Continuous Cardiac Monitoring to Assess Atrial Fibrillation After Cryptogenic Stroke (CRYSTAL AF) investigators conducted a randomised, controlled study of 441 patients to assess whether long-term monitoring with an insertable cardiac monitor was more effective than conventional follow-up (control) for detecting AF in patients with cryptogenic stroke. Patients 40 years of age or older with no evidence of AF over at least 24 h of ECG monitoring underwent randomisation within 90 days after the index event. The primary end point was the time to first detection of AF (lasting >30 s) within 6 months. The secondary end points included the time to first detection of AF within 12 months. Data were analysed according to the intention-to-treat principle. By 6 months, AF had been detected in 8.9% of patients in the implantable monitoring group (19 patients) versus 1.4% in the control group (three patients) (HR 6.4; 95% CI 1.9–21.7; p < 0.001). By 12 months, AF had been detected in 12.4% of patients in the implantable device group (29 patients) versus 2.0% in the control group (four patients) (HR 7.3; 95% CI 2.6–20.8; p < 0.001). At 36 months of follow-up, the rate of detection of AF was 30% in the implantable monitoring group versus 3% in the control group. 10 Age is considered one of the strongest predictors of subclinical AF; the mean age of the patients in the EMBRACE study was 72.5 years compared to 61.6 years in the CRYSTAL AF study, and this may partially explain the rate differences. A pooled analysis of these two randomised trials evidenced that longer ECG monitoring was superior to the standard practice of short-term ECG monitoring for the detection of AF (duration at least 30 s) in patients with a stroke or TIA labelled as cryptogenic (OR 6.4; 95% CI 3.5–11.7) (Figure 1). Furthermore, a pooled analysis of observational studies with a control group demonstrated that longer ECG monitoring was superior to the standard practice of short-term ECG monitoring for the detection of AF (any duration) in patients with cryptogenic stroke or TIA (OR 3.8; 95% CI 2.4–5.9)19–23 (Figure 2).
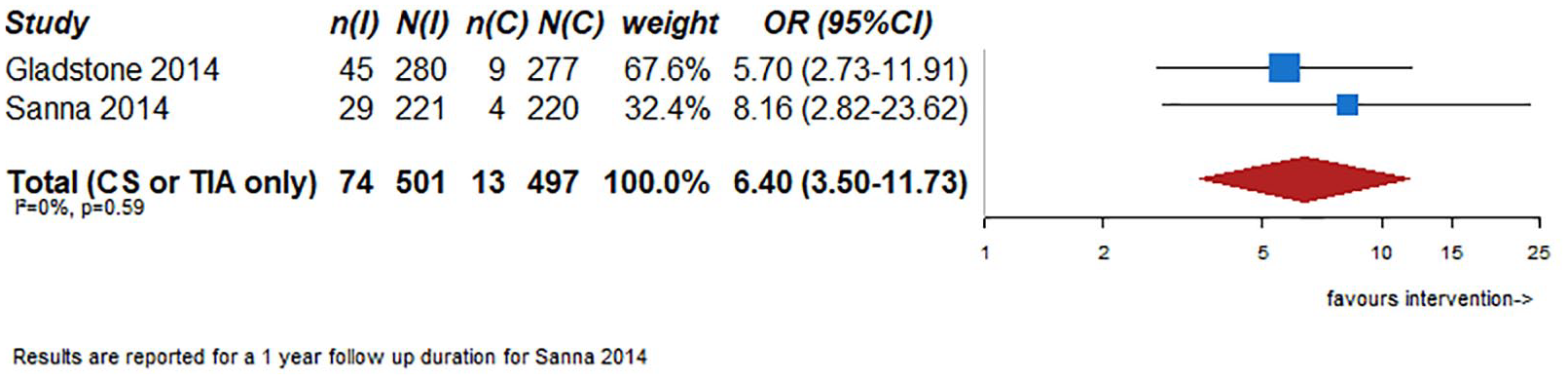
AF detection lasting at least 30 s in RCTs (1-year follow-up).
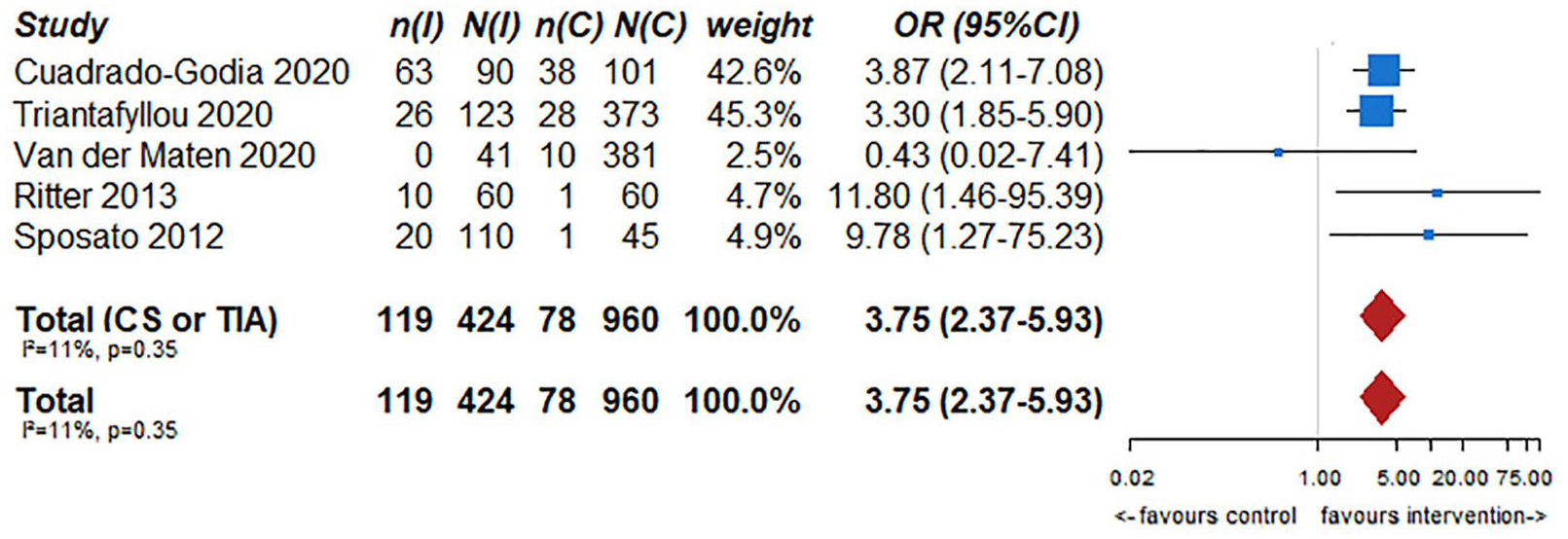
Any AF detection in observational studies with control group.
Additional information
The optimal duration of monitoring for subclinical AF after acute ischaemic stroke or TIA remains a matter of debate. Multiple studies have been published using both invasive and non-invasive monitoring strategies for different monitoring periods. The data from these studies provide evidence that a longer monitoring strategy beyond 24 h is associated with higher detection rates of AF. A pooled analysis of published single arm studies demonstrated that the rate of detected AF increases with the duration of monitoring, from about 8.9% at 1 month to 17.9% at 6 months, 22.3% at 12 months and 25.2% at 36 months (Figures 3–6).24–73
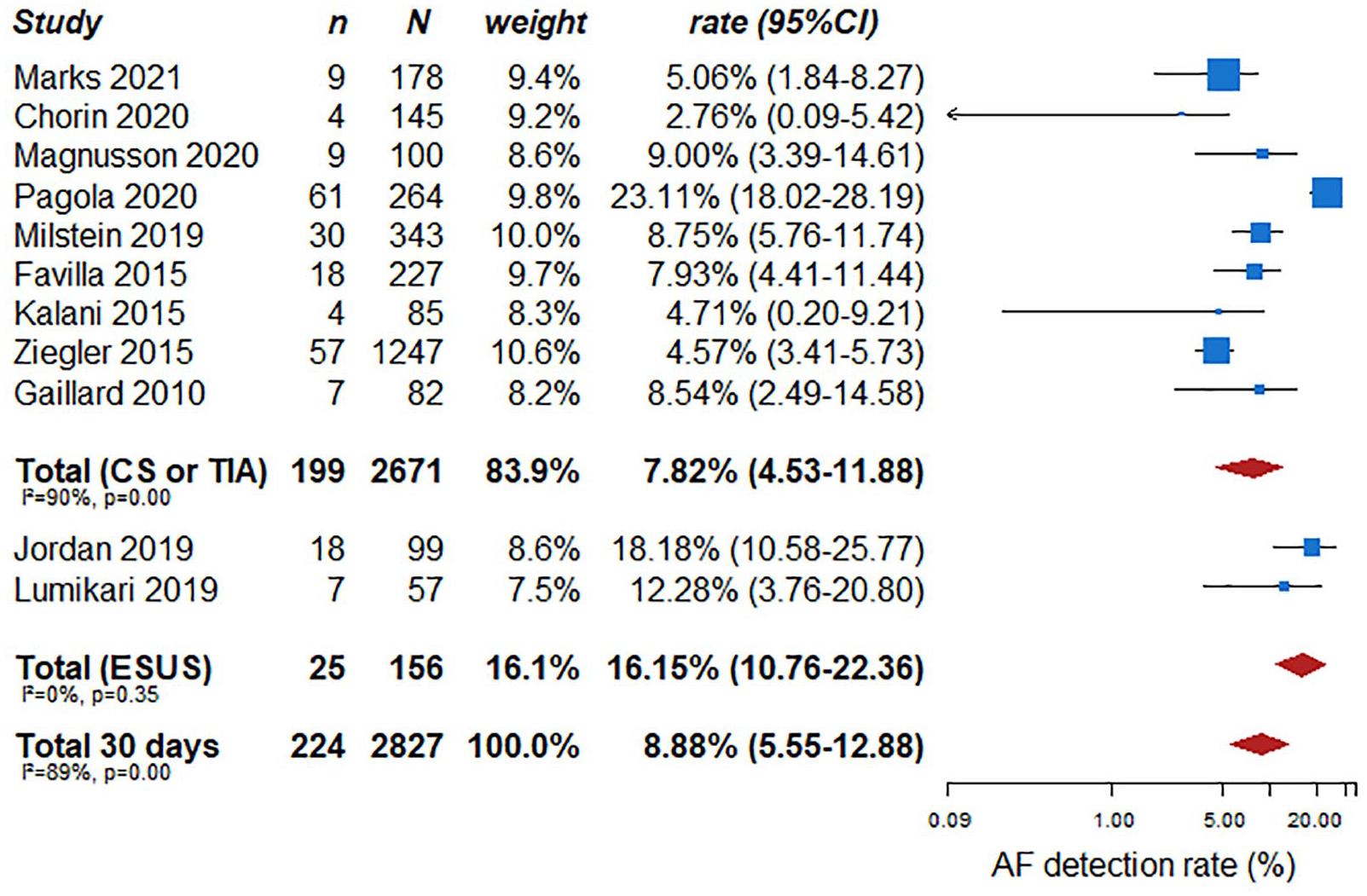
AF detection rate in single arm studies (30-day follow-up).
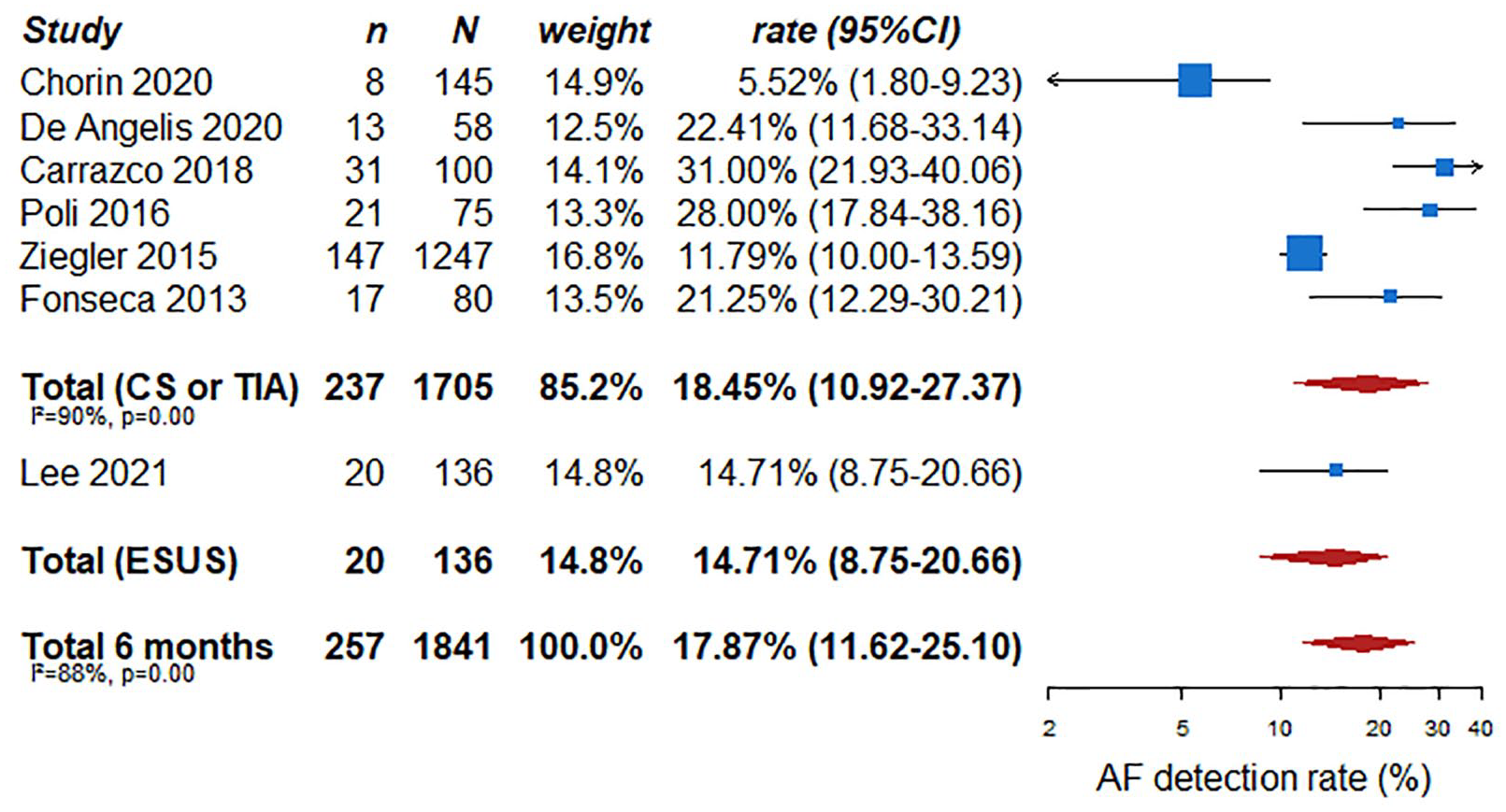
AF detection rate in single arm studies (6 months follow-up).
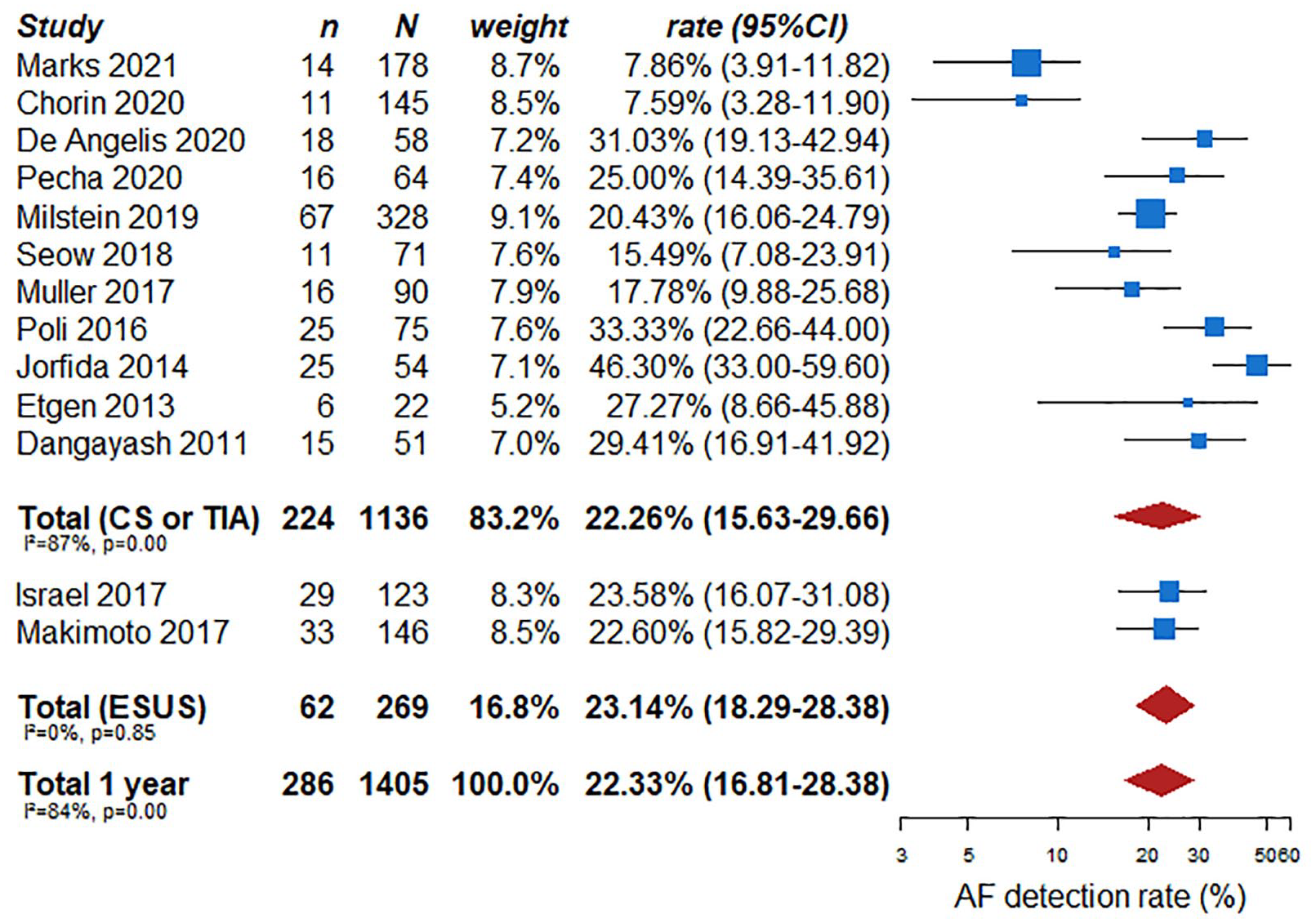
AF detection rate in single arm studies (1-year follow-up).
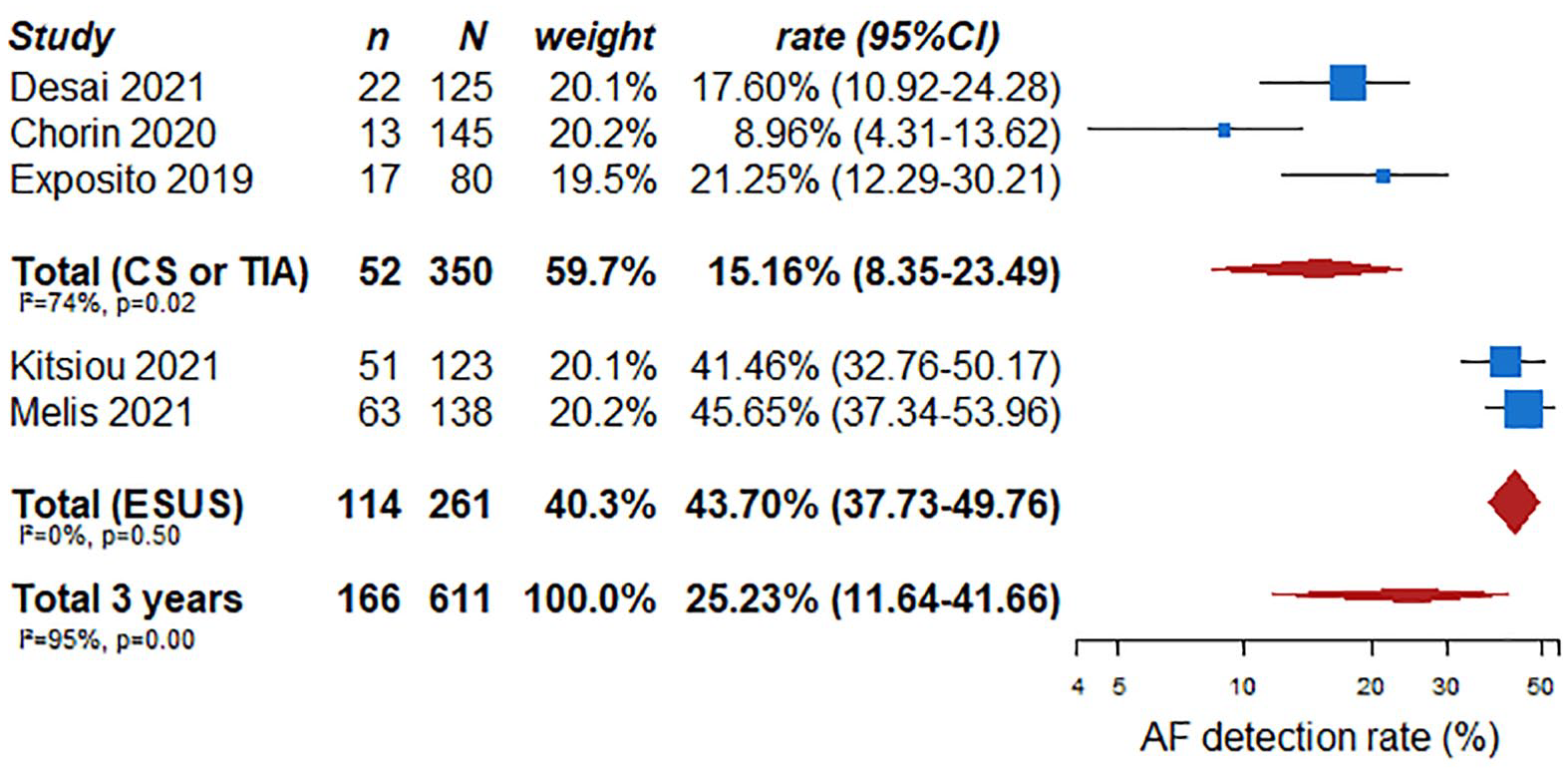
AF detection rate in single arm studies (3 years follow-up).
In addition, data from RCT including different stroke subtypes also demonstrate that longer cardiac monitoring increases the rate of subclinical AF detection. FIND-AF (Finding Atrial Fibrillation in stroke patients, NCT01855035) 74 was a RCT that included patients with ischaemic stroke of any aetiology admitted to four German hospitals (without known AF, one-half of patients suffering a stroke of undetermined origin). Patients underwent three sets of 10 days of ECG-Holter monitoring at baseline (median time of 4 days after stroke onset), and after 3 and 6 months compared with conventional monitoring (24 h ECG monitoring). The rate of AF detection in the intervention group was significantly higher (14% vs 5%, absolute difference 9.0%: 95% CI 3.4–14.5, p = 0.002). The STROKE-AF trial (Stroke of Known Cause and Underlying Atrial Fibrillation, NCT02700945) included patients with stroke attributed to large or small vessel disease, who were randomised to long-term cardiac monitoring through an implantable loop recorder versus conventional ECG monitoring. Patients in the intervention group presented with a higher rate of subclinical AF after 12 months (27 patients (12.1%) vs 4 patients (1.8%); HR 7.4 (95% CI 2.6–21.3); p < 0.001). 75 Finally, PER-DIEM (Post-Embolic Rhythm Detection with Implantable vs External Monitoring, NCT02428140) included 300 patients with ischaemic stroke, 66% defined as stroke of undetermined origin. Patients were randomised 1:1 to 1 month of external-loop recorder versus 1 year of ILR. The primary outcome was the development of definite AF or highly probable AF (adjudicated new AF lasting ⩾2 min within 12 months of randomisation) and was observed in 15.3% (23/150) of patients in the implantable loop recorder group and 4.7% (7/150) in the external loop recorder group (between-group difference, 10.7% (95% CI 4.0–17.3); RR 3.3 (95% CI 1.5–7.4); p = 0.003). 76
Furthermore, limited data suggest that an earlier start of prolonged ECG monitoring might result in higher yield of AF compared to a later start of monitoring 31 and that with short-term continuous monitoring lasting for 4 weeks soon after stroke, a higher yield might be obtained within the first weeks from stroke. 42 However, a meta-analysis that investigated the duration of implantable cardiac monitoring and the yield of AF detection in ischaemic stroke patients showed that in multivariate meta-regression analyses only monitoring duration (coefficient = 0.009; 95% CI 0.003–0.015; p = 0.006) and mean patient age (coefficient = 0.037; 95% CI 0.013–0.062; p = 0.007) were independently associated with the proportion of AF detection. The rate of AF detection was identical (23%) in patients with implantation occurring within the first month of stroke symptom onset and in patients with implantation occurring after the first month of stroke symptom onset. 77 As existing studies varied widely in their design, methods of monitoring, study population, stroke characteristics, total duration of monitoring, timing of monitoring since stroke and the definition of AF, future studies should focus on optimising these characteristics for effective AF monitoring following an acute ischaemic stroke or TIA.
Outcome: Rate of anticoagulation
Analysis of current evidence
When AF is detected, anticoagulation is strongly advised to reduce the risk of stroke recurrence in clinical practice. In the EMBRACE study, at randomisation, most patients were receiving antiplatelet therapy, as expected. After monitoring, most of the patients with AF received anticoagulant therapy. At 90 days, the proportion of patients treated with anticoagulants was significantly higher in the intervention group compared to the control group: 18.6% (52 of 280 patients) versus 11.1% (31 of 279), for an absolute treatment difference of 7.5 percentage points (95% CI 1.6–13.3; p = 0.01). In the intervention group, 38 of 280 patients (13.6%) switched from antiplatelet to anticoagulant therapy, compared to 13 of 279 (4.7%) in the control group: a difference of 8.9% points (95% CI 4.2–13.6; p < 0.001). 9 In the CRYSTAL AF study, the rate of oral anticoagulant use was 10.1% in the longer duration cardiac rhythm monitoring group, versus 4.6% in the control group at 6 months (p = 0.04) and 14.7% versus 6.0% at 12 months (p = 0.007). 10 Furthermore, in a pooled analysis of randomised and observational studies with a control group, longer ECG monitoring in patients with cryptogenic stroke or TIA was associated with an increased rate of anticoagulation compared to a shorter duration (Figure 7).
Increase of anticoagulation rate in observational studies with a control group or randomised clinical trials.
Outcome: Rates of recurrent stroke or systemic embolism, mortality, intracranial haemorrhage and major haemorrhage (intracranial or extracranial)
Analysis of current evidence
In the CRYSTAL AF study, ischaemic stroke or TIA occurred in 11 patients (5.2%) in the longer duration of cardiac rhythm monitoring group, compared to 18 patients (8.6%) in the control group, during the first 6 months after randomisation and in 15 patients (7.1%) versus 19 patients (9.1%) during the first 12 months. 10 No published data to date are reported from stroke recurrence in the EMBRACE study.
Furthermore, longer ECG monitoring was not statistically superior to the standard practice of short-term ECG monitoring for the reduction of mortality (OR 1.0; 95% CI 0.2–4.3) (Figure 8). These results derived from subgroup analyses of two randomised trials, both of which aimed to investigate whether longer duration of cardiac rhythm monitoring may be better than a shorter duration in detecting AF in patients with cryptogenic stroke or TIA. The studies were not powered to detect any difference regarding the risk of recurrent stroke or mortality. Nevertheless, point estimates for reductions of stroke recurrence at both 6 months and 1 year were less than 1, pointing towards a statistically non-significant advantage of longer ECG monitoring. Furthermore, the two studies did not report data regarding other endpoints such as systemic embolism, intracranial haemorrhage, major haemorrhage (intracranial or extracranial) or functional outcome.
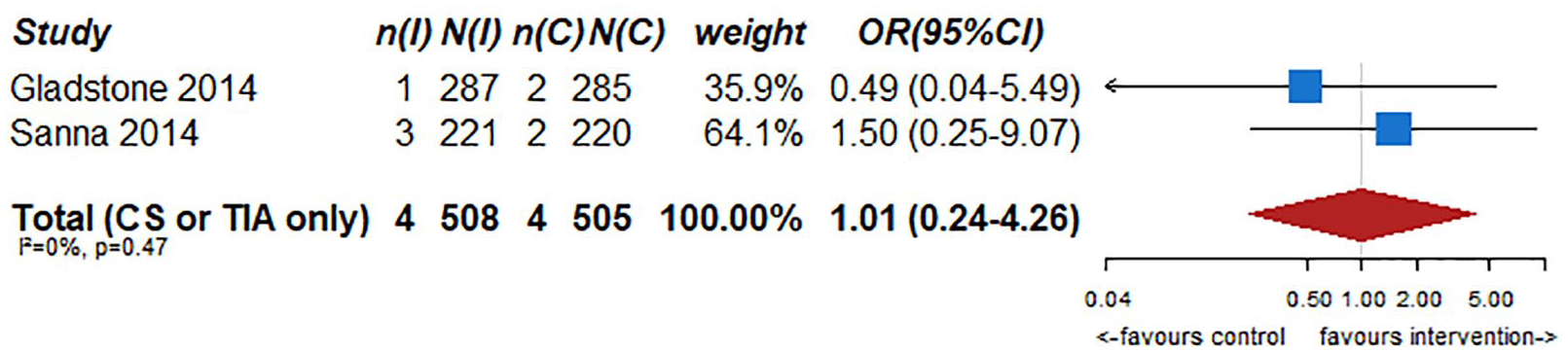
Longer ECG monitoring was not superior to the standard practice of short-term ECG monitoring for the reduction of mortality.
The effects of longer duration of cardiac rhythm monitoring compared to shorter duration of cardiac rhythm monitoring for all the outcomes are summarised in Table 1.
The effects of longer duration of cardiac rhythm monitoring compared to shorter duration of cardiac rhythm monitoring for all the outcomes in patients with stroke of undetermined origin (PICO 1).
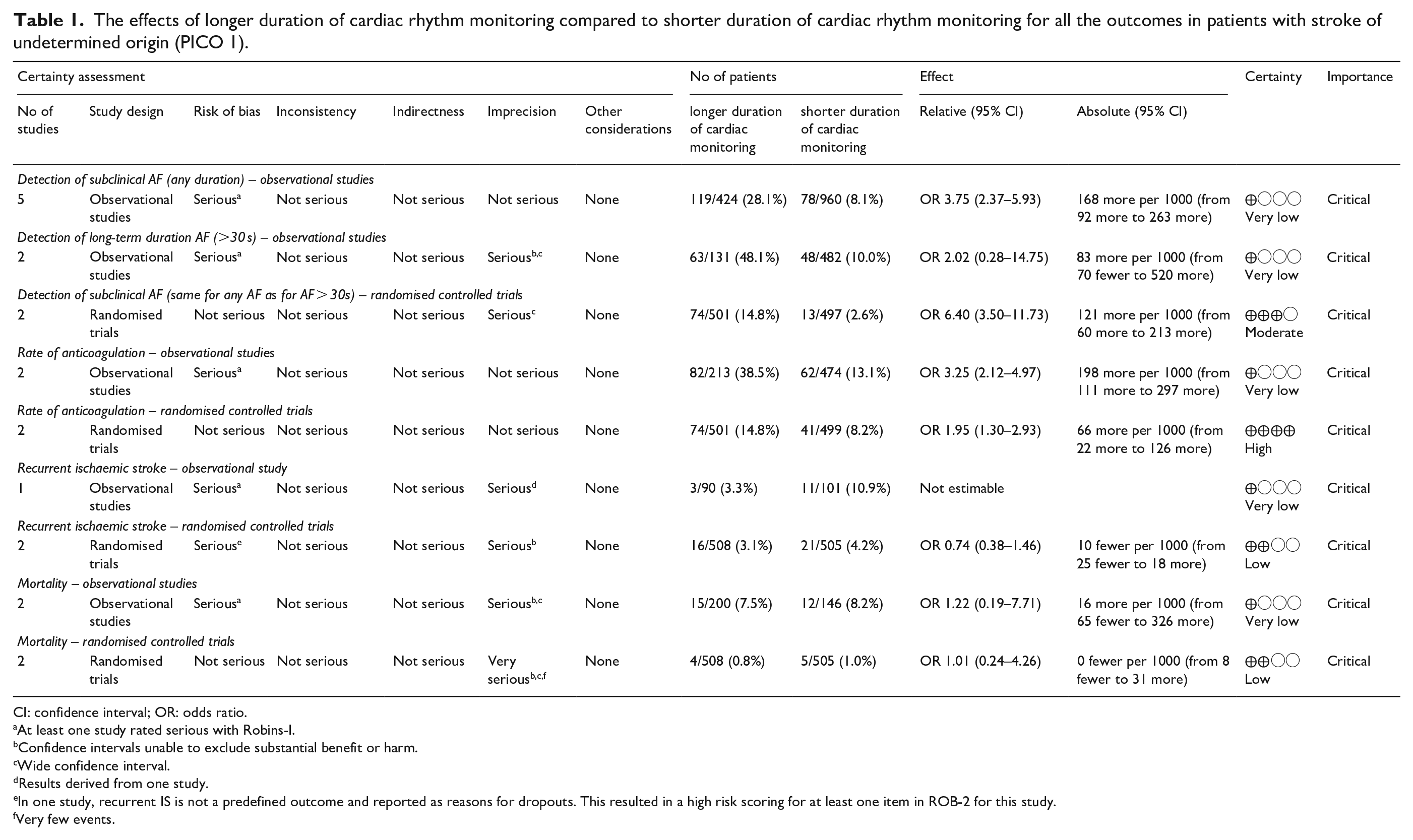
CI: confidence interval; OR: odds ratio.
At least one study rated serious with Robins-I.
Confidence intervals unable to exclude substantial benefit or harm.
Wide confidence interval.
Results derived from one study.
In one study, recurrent IS is not a predefined outcome and reported as reasons for dropouts. This resulted in a high risk scoring for at least one item in ROB-2 for this study.
Very few events.
The graphics of risk of bias of RCTs are reported in Figures e6 to e9 of the Supplemental File.
Additional information
The risk of stroke in patients with subclinical paroxysmal AF does not appear to differ to that in patients with chronic or persistent AF. 78 For this reason, patients with subclinical AF detected with ECG monitoring should be eligible for secondary stroke prevention with oral anticoagulants using vitamin K antagonists or non-vitamin K antagonists, as recommended by the ESO guidelines. 79 An important issue of uncertainty is the minimal clinically relevant duration of paroxysmal AF episodes. A meta-analysis of 10,016 patients with cardiac implantable electronic devices evaluated device-detected atrial tachyarrhythmias and thromboembolic risk in patients with paroxysmal or persistent AF. In this analysis, the rate of ischaemic stroke or TIA was low, ranging from 0.3 per 100 person-years for having 0 to fewer than 5 total minutes to 0.5 per 100 person-years for having 23 or more total hours of AF. After adjusting for the CHADS2 score and the receipt of oral anticoagulation at entry, increasing time in AF was associated with a higher risk of stroke as a continuous measure (HR 1.0 h; 95% CI 1.0–1.1) and using prespecified cut-offs of 1 h or longer (HR 2.1; 95% CI 1.2–3.6) and 5 min or longer (HR 1.8; 95% CI 1.0–3.0). 80 In the Asymptomatic Atrial Fibrillation and Stroke Evaluation in Pacemaker Patients and the Atrial Fibrillation Reduction Atrial Pacing Trial (ASSERT) including 2580 patients with a pacemaker or implantable cardioverter defibrillator and no prior AF or atrial flutter, asymptomatic atrial tachyarrhythmias lasting longer than 6 min during a 3-month monitoring period were associated with a higher adjusted rate of ischaemic stroke or systemic embolism (HR 2.5; 95% CI 1.3–4.8). 81 The current consensus definition of paroxysmal AF applies an arbitrary cut-off of ⩾30 s, 16 yet in clinical practice cryptogenic stroke patients with paroxysmal AF duration of <30 s might not be excluded from anticoagulation therapy. Some studies have demonstrated an association between AF burden and stroke risk. The electrophysiological definition of AF burden is the amount of time the patient is in AF out of the total monitored time. A systematic review found the AF burden exceeding different thresholds was associated with an increased risk of ischaemic stroke. However, the review did not provide a definite threshold for AF burden at stroke risk. 82 A meta-analysis found that AF burden >5 min was associated with a higher stroke risk, but it was not associated with an increase in all-cause mortality. 83
Liantinioti et al. 84 found that duration of paroxysmal AF was not associated with baseline stroke severity and early outcomes in patients with cryptogenic stroke and should not influence anticoagulation decision in these patients. The results of a UK survey among cardiologists and stroke physicians that sought to assess current management of patients with atrial arrhythmia of <30 s duration detected on ambulatory ECG, found that when asked whether they would anticoagulate eight hypothetical patients with non-diagnostic paroxysms of AF, there was a mean agreement of responses of 78.6%, with up to 94.1% agreement for high-risk patients including patients with previous stroke. 85
Outcome: Detection of subclinical AF
Analysis of current evidence
Screening for AF is usually initiated during the in-hospital stay after acute ischaemic stroke. Typically, a minimum of 24-h ECG monitoring by continuous telemetry within the Stroke Unit, or a 24-h Holter ECG without AF detected are required to define a patient as having a stroke of undetermined origin. 86 Indeed, 24 h is also the minimum ECG monitoring period required for the diagnosis of ESUS. 7 However, further in-hospital or outpatient ECG monitoring beyond 24 h is frequently performed, 87 so we aimed to assess if addition of out-patient cardiac rhythm monitoring compared with in-hospital monitoring alone may improve the rates of our pre-defined outcomes.
We could not identify a RCT addressing this specific issue. As commented in PICO 1, both interventional and control groups in CRYSTAL AF and EMBRACE received outpatient monitoring for AF detection. In EMBRACE the additional monitoring was performed in the intervention group by a 30-day event-triggered recorder and compared with repeated conventional 24-h monitoring (control group). In CRYSTAL AF the interventional group of cryptogenic stroke and TIA patients received outpatient monitoring by implantable loop-recorders, and the control group repeated ECG recordings performed in the scheduled, and non-scheduled, outpatient clinical visits. Therefore, no specific comparison with in-hospital monitoring was performed.
Conversely, the randomised, open-label MonDAFIS study (Systematic monitoring for detection of AF in patients with acute ischaemic stroke) 88 recruited patients with any aetiologic subtype of TIA and ischaemic stroke without previously known AF and tested two different in-hospital monitoring strategies. Patients were allocated to conventional monitoring (including 24 h stroke-unit cardiac telemetry) versus intensive monitoring with additional 7-day Holter-ECG. The rate of AF detection was significantly higher in the intensive monitoring group: 5.8% versus 4% (HR 1.4; 95% CI 1.0–2.0; p = 0.024).
Several observational single-arm studies,20,28,31,35–37,42,44,45,48,54–59,62,64,65,67–70,73,89–91 have studied additional outpatient ECG monitoring, with a wide range of monitoring initiation, duration and type of monitoring systems (Figure 9). The median rate of any AF detection in patients with cryptogenic stroke or TIA with out-patient AF screening was 19.2% (95% CI 15–23.8). For ESUS patients, out-patient monitoring in single arm studies detected AF in a 22.6% of cases (95% CI 12.5–34.6). Conversely, we could only find one observational study focussed on in-hospital monitoring for AF screening (after ruling-out the minimum 24-h ECG monitoring). The CHALLENGE ESUS/CS (Mechanisms of Embolic Stroke Clarified by Transoesophageal Echocardiography for Embolic Stroke of Undetermined Source/Cryptogenic Stroke) 92 is a multicentre registry of patients admitted with an acute ischaemic stroke in seven centres in Japan. All patients had a complete work-up, including 24-h cardiac rhythm monitoring before inclusion, and a transoesophageal echocardiography. In addition, the 677 patients included in the study underwent a 12-lead ECG, continuous cardiac rhythm monitoring, and a 24-h Holter ECG. The aim of the study was to identify differences in the rates of early or late (⩽4 or >4 days) AF detection (median monitoring time: 17 days). AF was detected in 64 patients (9.5% of cases), 37/64 (58%) of them within the first 4 days.
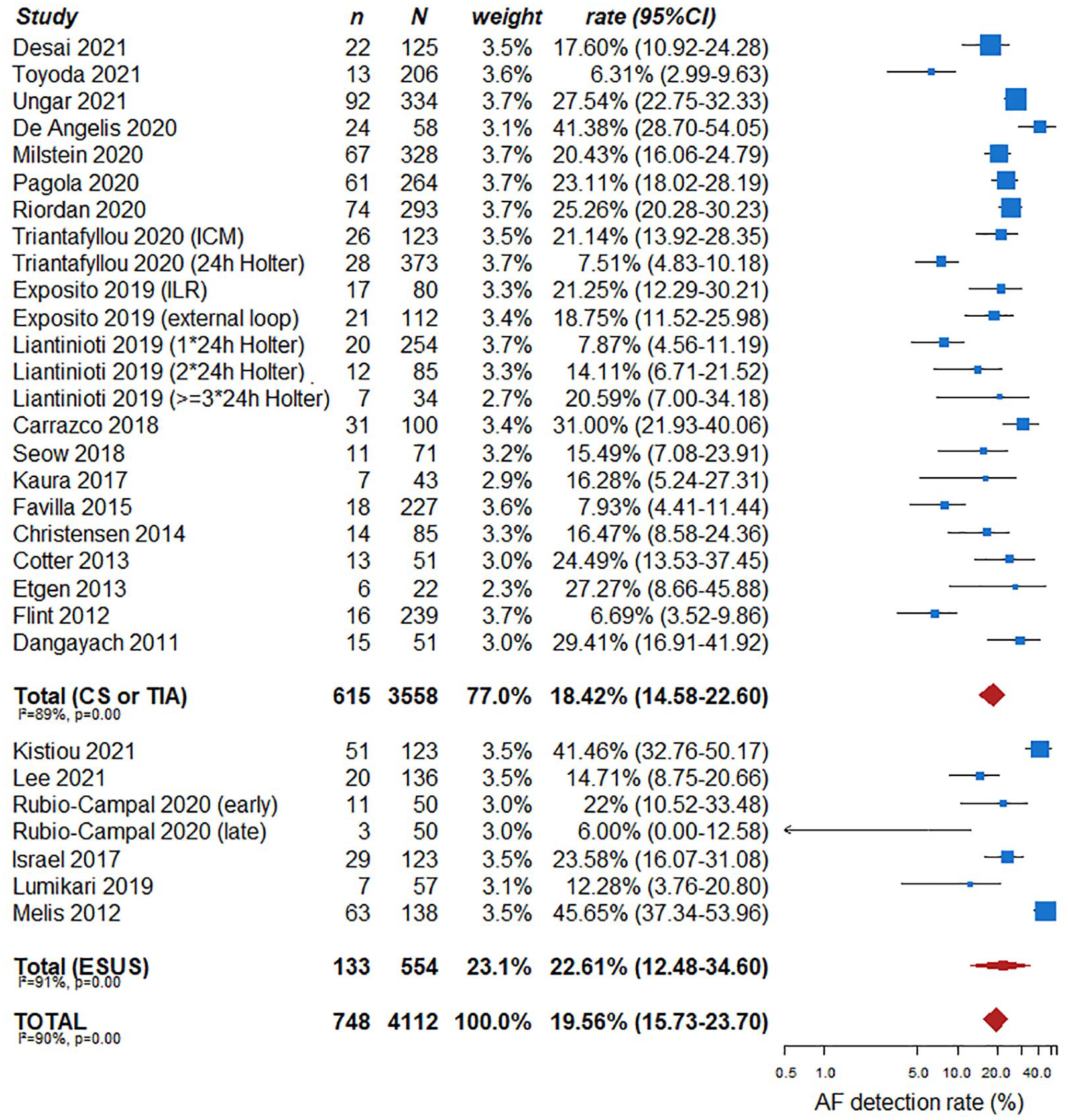
AF detection rate with outpatient devices in single arm studies.
Additional information
The available data show an increased AF detection rate by adding outpatient monitoring. The increased detection rate appears to be explained by the prolonged time duration of monitoring than the outpatient setting. Whether in-hospital and outpatient monitoring would differ with respect to AF detection rate if the duration of monitoring was identical is not known. Potentially, outpatient monitoring could increase AF detection because patients may be more physically active after discharge, which might induce AF in some patients (i.e. autonomic-triggered AF). 93 Conversely, the early initiation of ECG monitoring during the in-hospital stay may also increase AF detection 31 especially in patients with higher AF burden. In the multicentre CRYPTO-AF (PI15/02265) registry 35 AF monitoring by a textile-wearable Holter was started within the first 3 days after a cryptogenic stroke (diagnosed after a 24 h ECG monitoring without AF detection). The rates of AF detection were as follows: from 0 to 3 days 5.6% (8/142), from 4 to 15 days 16.2% (23/142) and from 16 to 28 days 14.8% (21/142). In the CHALLENGE ESUS/CS registry, AF was detected within the first 4 days in 5.5% of cases. 94 In FIND-AF, the relevant increase in AF detection occurred within the baseline 10-day period of monitoring (18 patients, as compared to 6 in the second and only 1 in the third 10-day period of ECG-Holter monitoring). 74 These results suggest that the lower rates of AF detected in RCTs as CRYSTAL AF or EMBRACE may be in part related to the later start of out-patient AF monitoring (within 90 days or 6 months of the index event, respectively).
Outcome: Rate of anticoagulation
Analysis of the current evidence
Detection of subclinical AF, lasting at least 30 s, usually prompts initiation of anticoagulation. As commented in PICO 1, CRYSTAL AF and EMBRACE studies only provide the rates of anticoagulation with out-patient monitoring, with an increase in the rate of anticoagulation in both studies in the interventional arm, given the higher rate of AF detection (10.1% vs 4.6% and 18.6% vs 11.1%, respectively).9,10 There is lack of information regarding rate of anticoagulation for in-patient monitoring in CHALLENGE ESUS/CS. In MonDAFIS, the rate of anticoagulation did not differ between both arms after 1 year of follow-up (OR 1.2 (95% CI 0.9–1.5); p = 0.13) 88 despite the increased rate of AF detection in the longer monitoring group.
Outcome: Rate of recurrent stroke or systemic embolism, intracranial haemorrhage, any major haemorrhage, mortality and improve functional outcome
Analysis of the current evidence
In CRYSTAL AF, with out-patient monitoring, the rates of ischaemic stroke recurrence and mortality did not statistically differ between the interventional and control arms. Information regarding systemic embolism, intracranial haemorrhage or functional outcome is not reported. The only data available for in-hospital ECG monitoring originates from MonDAFIS that was not focussed on strokes of undetermined origin; the composite outcome of recurrent stroke, major bleeding, myocardial infarction or death after 24 months did not differ in the longer monitoring versus the conventional monitoring group (13.5% vs 14.5%; HR 0.9 (0.8–1.1); p = 0.43).9,10,88
The effects of additional out-patient cardiac rhythm monitoring compared with in-hospital cardiac rhythm monitoring alone for all the outcomes in adult patients with stroke or TIA of undetermined origin are summarised in Table 2.
The effects of adding out-patient monitoring to in-hospital monitoring for all the outcomes in patients with stroke of undetermined origin (PICO 2).
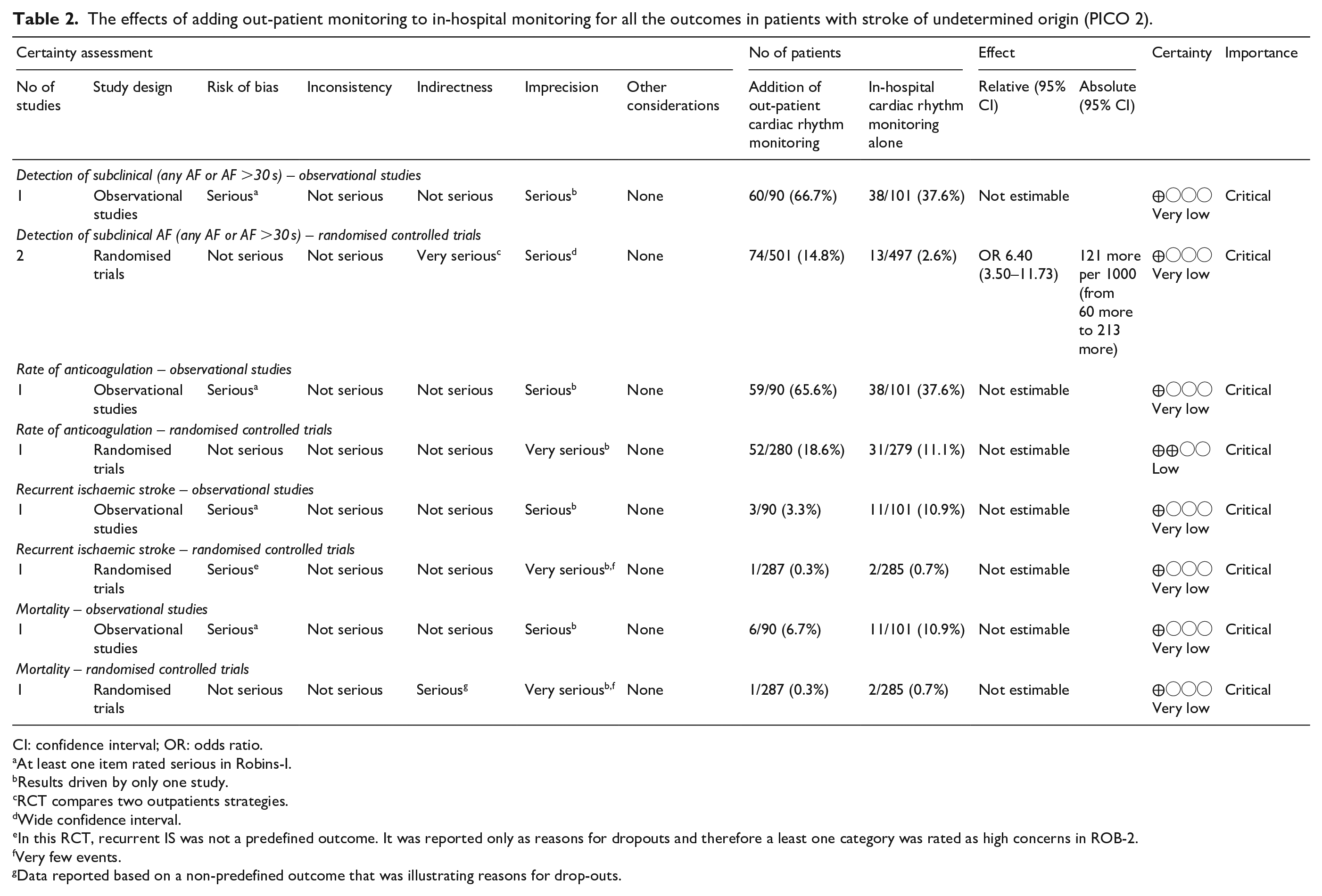
CI: confidence interval; OR: odds ratio.
At least one item rated serious in Robins-I.
Results driven by only one study.
RCT compares two outpatients strategies.
Wide confidence interval.
In this RCT, recurrent IS was not a predefined outcome. It was reported only as reasons for dropouts and therefore a least one category was rated as high concerns in ROB-2.
Very few events.
Data reported based on a non-predefined outcome that was illustrating reasons for drop-outs.
Outcome: Detection of subclinical AF
Analysis of the current evidence
In recent years, the development of implantable monitoring devices has led to a breakthrough in the opportunities for prolonged screening for AF. Implantable monitors allow very long monitoring, up to more than 3 years, without the need for patient collaboration and with very few implant complications. Furthermore, the newer implantable devices only require an injection for implantation, greatly facilitating their use. 95 The main drawback is the cost of the devices, which prevents their widespread application in all healthcare systems. Furthermore, additional arrangements are needed to ensure swift review and interpretation of transmissions prompted by the device that frequently tend to be false alarms. 96
As commented in PICO 1, only CRYSTAL AF compared AF detection using an implantable device as the intervention; patients in the control group instead received only ECG recordings in scheduled and non-scheduled medical visits according to the recommendation of the treating stroke physician, but not a non-implantable external monitoring device. The inclusion criteria included patients with a cryptogenic stroke in the previous 6 months, with a complete work-up including a 24-h Holter-monitoring. Patients in the interventional group showed AF lasting 30 s or longer in 8.9% in the intervention group, as compared with 1.4% in the control group after 6 months of monitoring (HR 6.4; 95% CI 1.9–21.7; p < 0.001). At 12 months, the rate of AF detection was 12.4% versus 2% in the control group (HR 7.3; 95% CI 2.6–20.8; p < 0.001). 10 A sub-study of CRYSTAL AF 97 selected those patients fulfilling ESUS criteria according to NAVIGATE-ESUS (Rivaroxaban vs Aspirin in Secondary Prevention of Stroke and Prevention of Systemic Embolism in Patients With Recent Embolic Stroke of Undetermined Source) 98 and RESPECT-ESUS (Randomised, double-blind, Evaluation in secondary Stroke Prevention comparing the EfficaCy and safety of the oral Thrombin inhibitor dabigatran etexilate vs acetylsalicylic acid in patients with Embolic Stroke of Undetermined Source) 99 trials. The rate of AF detection in these patients was 5.6% and 3.5% at 30 days (conventional monitoring: 1.0% and 0.8%) and 35.8% and 33.6% at 3 years (conventional monitoring: 3.4% and 2.8%, p > 0.001). The OR was 18.8 (95% CI 7.9–44.5) favouring implantable device monitoring for AF detection in patients fulfilling ESUS criteria.
Four observational clinical studies compared AF detection by implantable devices with a control group of patients undergoing routine care. In a study, 22 61 patients with a cryptogenic stroke received an implantable device after a median of 14 days after the ischaemic event. All patients also received 7-day Holter-monitoring. 7-day Holter monitoring revealed AF only in one patient (1.7%; 95% CI 0–5), as compared to 10 patients (17%; 95% CI 7–26) who received an implantable device. A Spanish study 68 tested a ‘progressive’ strategy: 119 cryptogenic stroke or TIA patients with a complete diagnostic work-up including a minimum of 72 h in-hospital monitoring were included. All received a 24-h Holter-ECG, which detected AF in 5/119 (4.2%) patients. The remaining 112 patients received an external-loop recorder for 14 days, which detected AF in 21 additional patients (18.7%). The last 80 patients who had not shown AF in the previous recordings, received an implantable device, which revealed AF in a further 17 patients (21%). Another Spanish study 19 compared implantable devices with serial ECG and 24-h Holter monitoring, showing an AF detection rate of 58.5% in the implantable device group compared with 21.3% in the control group. Finally, another study 20 included cryptogenic stroke or TIA patients with a complete work-up including in-hospital 24-h Holter ECG over 8 years; from 2013 to 2017 patients received repeated 24-h ambulatory Holter ECG monitoring at the discretion of the treating stroke physicians (n = 373), while after 2017 patients received an implantable device (n = 123). After 3 years of follow-up, AF detection was significantly higher in the implantable device group (21.1% vs 7.5%, p < 0.001). A meta-analysis of these observational studies shows an OR of 2.8 (95% CI 1.4–5.6) favouring the implantable devices monitoring for AF detection after cryptogenic stroke or TIA (Figure 10). Also investigating AF lasting at least 30 s, a meta-analysis of Cuadrado-Godía, Triantafyllou and Exposito showed an OR of 2.5 for AF detection ⩾30 s, (95% CI 1.3–4.9)2,19,68 (Figure 11).
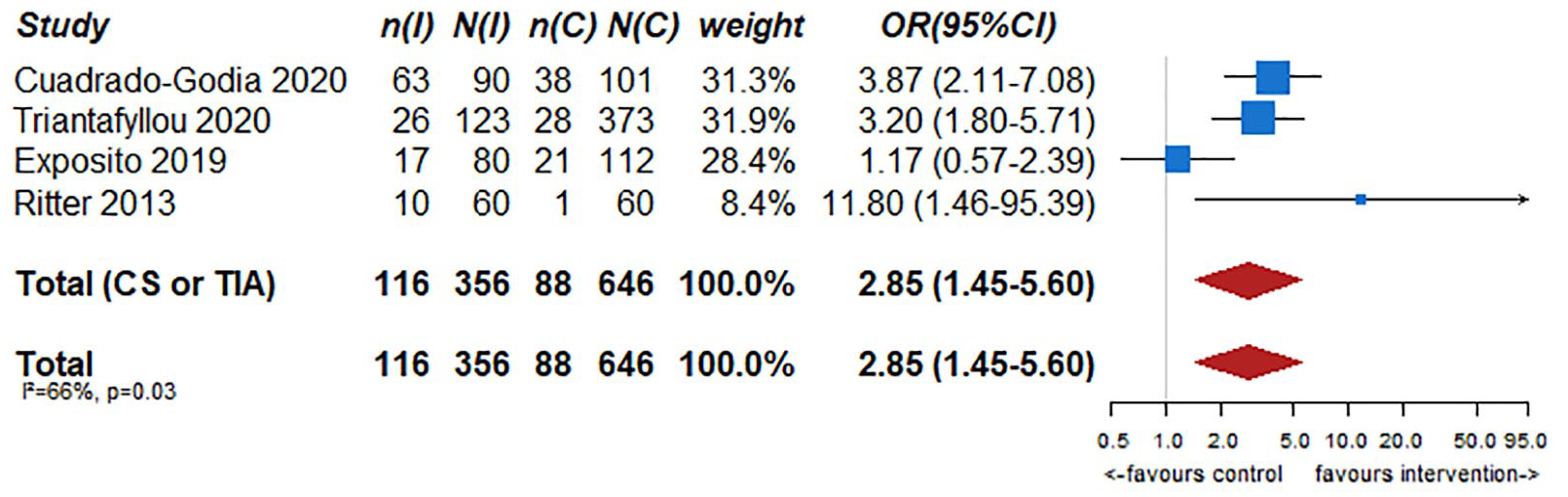
Any AF detection in observational studies with a control group.
Detection of AF lasting at least 30 s in observational studies with a control group.
In addition, there are several reports of single-arm studies using implantable monitoring devices with different monitoring duration times (Figure 12). The pooled rate of AF detection after cryptogenic stroke or TIA in these studies was 24.2% (95% CI 20.4–28.2), with a wide range from 11.7% to 46.3%. In patients who fulfilled the criteria of ESUS, the pooled rate of AF detection was 26.9% (95% CI 18.3–36.5). Globally, the pooled rate of AF detection with implantable devices was 25.0% (95% CI 21.4–28.7). In contrast, the rate of AF detection in reports from single-arm studies using any non-implantable device was 11.9% (95% CI 8.8–15.4) for cryptogenic stroke and TIA patients. For ESUS patients, the pooled rate was 13.5% (95% CI 6.5–22.6), and globally, the AF detection with non-implantable devices was 12.3% (95% CI 9.4–15.4).32,33,36,39,43–46,48–54,56–67,69,70,100
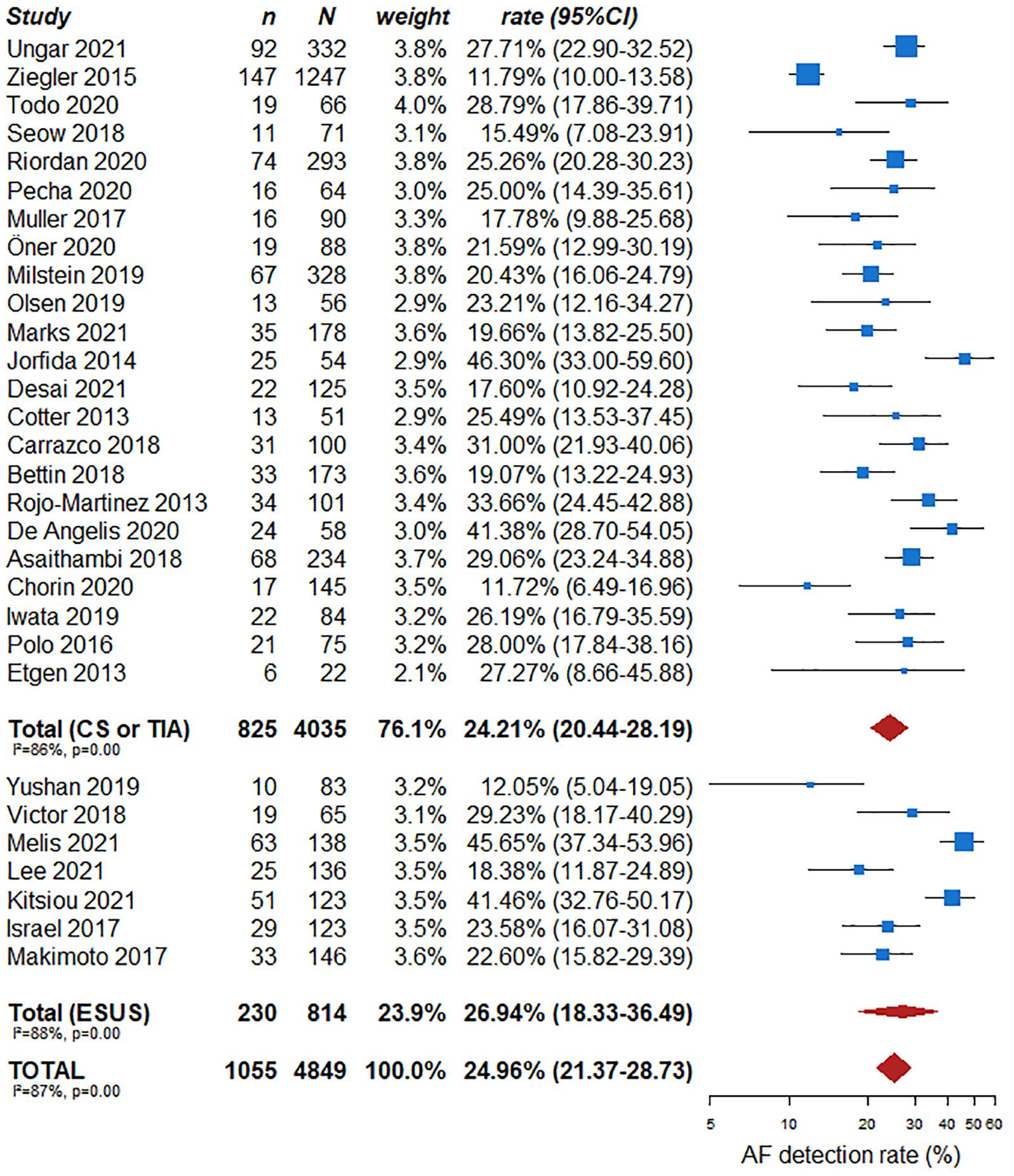
AF detection rates with implantable devices in single arm studies.
Additional information
The provided data identify an increased detection of AF with the use of implantable monitoring devices as compared with non-invasive strategies. However, the difference is probably related to the duration of the monitoring, which is much longer with the implantable devices, rather than the technology used. In a recently published meta-analysis 101 the proportion of AF detection was independently associated with the monitoring duration (coefficient = 0.015; 95% CI 0.005–0.024). However, given the inherent characteristics of implantable loop recorders, which are able to monitor for years, it is unrealistic to consider a direct comparison between implantable and non-implantable strategies with the same monitoring duration. In fact, in the two available RCTs of undetermined stroke prolonged cardiac monitoring, the rate of AF detection in EMBRACE at 90 days with non-invasive prolonged monitoring for 1 month was 16.1%, as compared with 8.9% at 180 days (6 months) in CRYSTAL AF, which used implantable devices. This is probably related to different inclusion criteria and not the different technologies.9,10
In PER-DIEM, patients with any ischaemic stroke without known AF were randomised to 1 month of external loop recorder versus 1 year of an implantable loop recorder. 76 As commented in PICO 1, patients with the implantable recorder showed higher rate of subclinical AF detection after 1 year. A post hoc analysis compared group differences in the proportion of patients who received AF diagnoses within 30 days. There were 7 (4.7%) new AF diagnoses in the implantable loop recorder group and 5 (3.3%) in the external loop recorder group (between-group difference, 1.3% (95% CI −3.1–5.8); p = 0.77). Another study, the LOOP trial (Patients at Risk Long-Term Monitored with Implantable Loop Recorder, NCT02036450) included persons with stroke risk factors but without AF, who were recruited from the general population to undergo screening with an implantable loop recorder. 102 Simultaneous monitoring strategies (i.e. single 10-s ECG, twice-daily 30-s ECGs for 14 days, single 24-, 48-,and 72-h, 7-day or 30-day continuous monitoring) were tested, and the authors showed that the diagnostic yield increased with duration, dispersion and number of non-implantable devices screenings, although all strategies had low yield compared with the implantable loop recorder.
In addition, some authors23,68,88 suggest progressive monitoring strategies, starting with non-invasive longer monitoring through external loop-recorders, followed by implantable devices in patients without AF detection. However, the efficacy and efficiency of this strategy for AF detection, compared to other approaches, is unknown. In fact, some cost-effectiveness models show a more efficient profile with the direct implantable monitoring strategies, although they are associated with increased health care costs, and the opportunity cost of wide scale implementation must be considered.103–105
Outcome: Rate of anticoagulation
Analysis of the current evidence
CRYSTAL AF studied the rate of anticoagulation in an implantable device monitored group as compared with conventional monitoring. The authors found a rate of oral anticoagulant use of 10.1% with implantable devices compared with 4.6% in the control group at 6 months (p = 0.04) and 14.7% versus 6.0% at 12 months (p = 0.007). 10
A meta-analysis of Cuadrado-Godía and Tryantafillou, as commented in PICO 1, showed a rate of anticoagulation significantly higher in the intervention group (OR 3.3; 95% CI 2.1–5)19,20 (Figure 7).
Outcome: Rate of recurrent stroke or systemic embolism, intracranial haemorrhage, any major haemorrhage, mortality and improve functional outcome
Analysis of the current evidence
In CRYSTAL AF the rate of ischaemic stroke or TIA recurrence was similar between groups receiving an implantable device or conventional monitoring at 6 months (5.2% vs 8.6%) and 12 months (7.1% vs 9.1%). No information regarding systemic embolism, functional outcome or mortality were reported. 10 However, in the three observational studies of implantable monitoring devices with a control group, a lower stroke recurrence was reported in the intervention group (OR 0.3; 95% CI 0.14–0.66) (Figure 13). No data about systemic embolism or mortality were provided.19,20,68
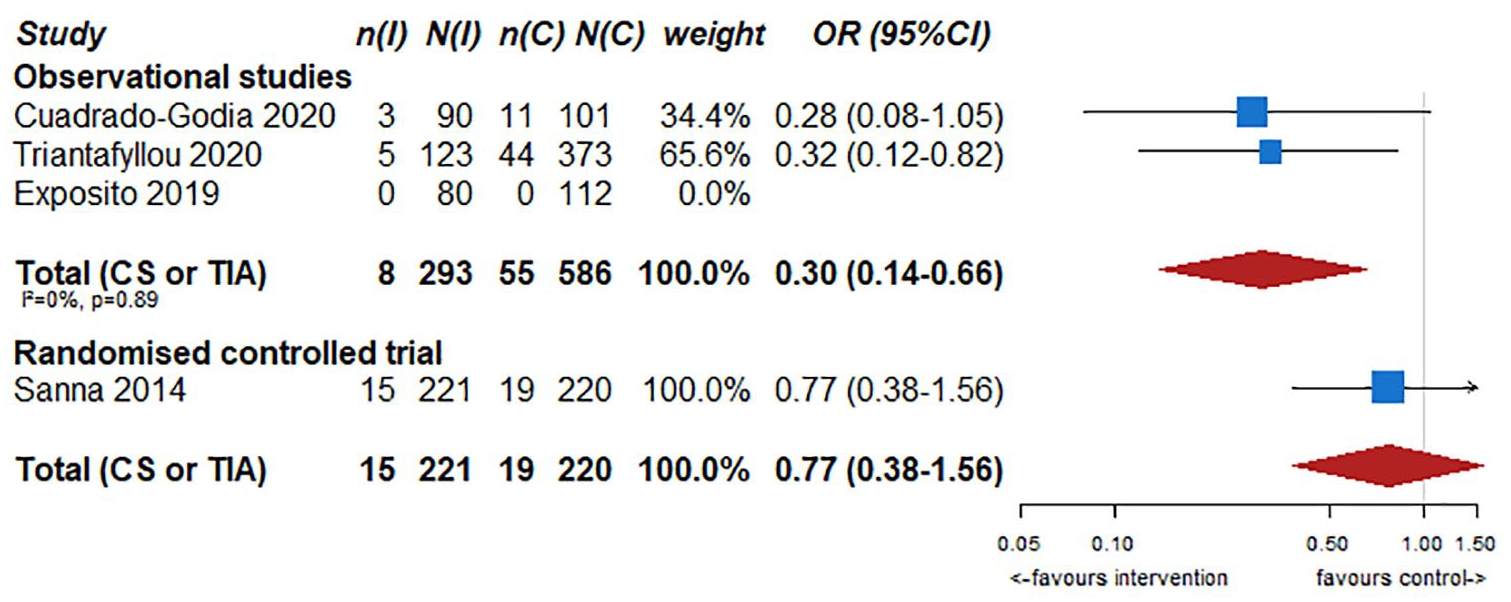
Reduction of stroke or TIA recurrence in observational studies or randomised clinical trial.
Additional information
Oral anticoagulation treatment substantially reduces the rate of recurrent stroke or systemic embolism in patients with AF. Therefore, it is plausible that strategies that lead to an increase detection, and an increase of anticoagulation initiation would also lead to a reduction in these outcomes. However, the RCTs available to date were not designed or powered to detect these differences. Nevertheless, a recent meta-analysis including patients with ESUS, cryptogenic stroke or ischaemic stroke of any aetiology (excluding severe symptomatic extra- or intracranial stenosis) showed a reduced rate of recurrent stroke in the group of patients receiving prolonged ECG-monitoring (RR 0.45; 95% CI 0.21–0.97). 77
The effects of additional implantable monitoring devices compared to any non-implantable external monitoring device for all the outcomes in adult patients with stroke or TIA of undetermined origin are summarised in Table 3.
The effects of implantable monitoring devices compared to any non-implantable external monitoring device for all the outcomes in patients with stroke of undetermined origin (PICO 3).
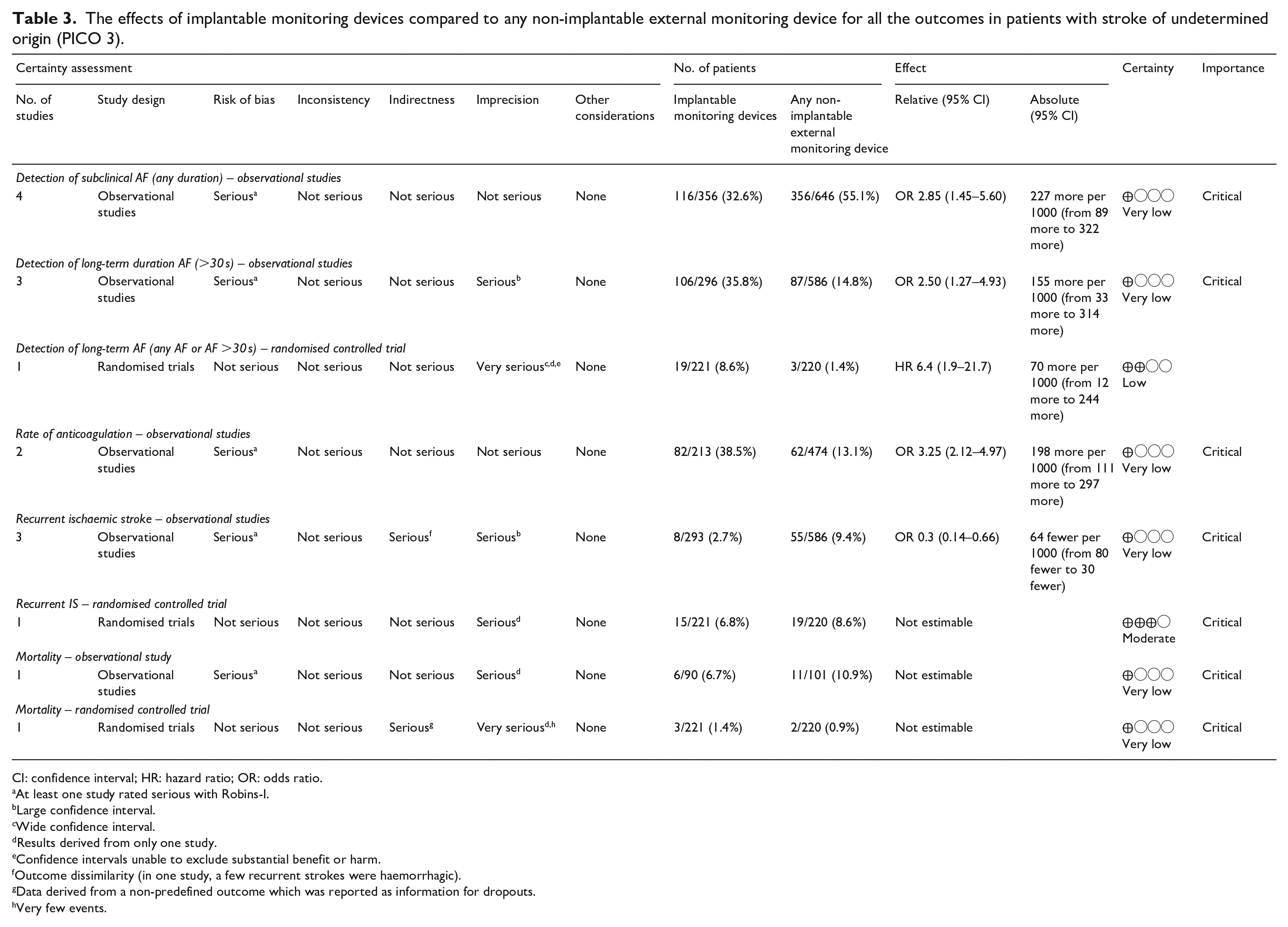
CI: confidence interval; HR: hazard ratio; OR: odds ratio.
At least one study rated serious with Robins-I.
Large confidence interval.
Wide confidence interval.
Results derived from only one study.
Confidence intervals unable to exclude substantial benefit or harm.
Outcome dissimilarity (in one study, a few recurrent strokes were haemorrhagic).
Data derived from a non-predefined outcome which was reported as information for dropouts.
Very few events.
Outcome: Detection of subclinical AF
Analysis of the current evidence
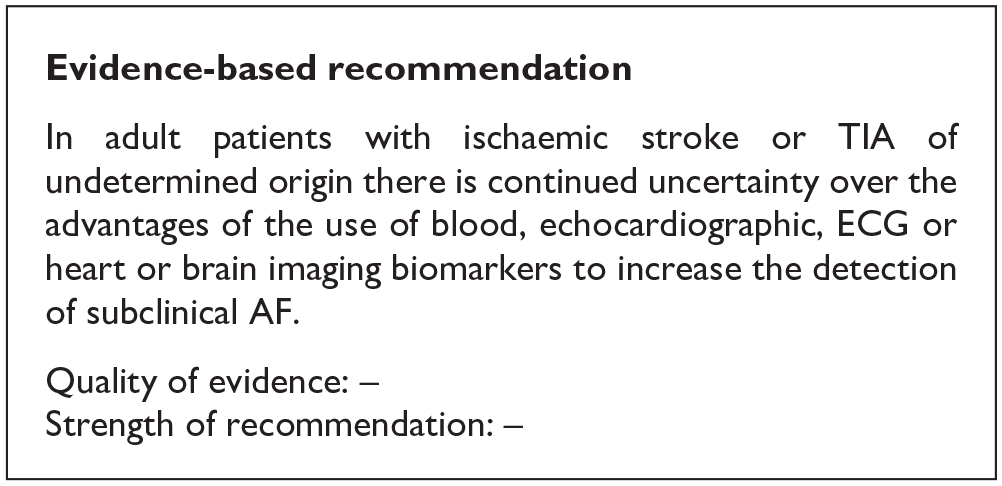
As commented in PICO 1, it has been demonstrated that the longer the monitoring, the higher the probability of detecting subclinical AF. However, longer monitoring incurs burden in terms of healthcare work and costs. This additional burden could overstrain some healthcare systems; to minimise this, the resources used for monitoring should not outweigh the health benefits. Therefore, the identification of biomarkers that can potentially increase the diagnostic yield (and thus cost-effectiveness) of AF screening in patients with stroke or TIA of undetermined origin has been intensively researched.88,106,107 However, we found no RCTs available to date specifically comparing the use of biomarkers to increase the AF detection after stroke or TIA of undetermined origin.
Additional information
Some sub-studies of AF screening RCTs and observational studies have identified predictive variables of subclinical AF.46,64,73,108
Age remains one of the strongest predictors of subclinical AF detection after stroke of undetermined origin in several studies.20,37,56,61,62,64,67,100,109–113 Clinical features including cortical branch occlusion syndromes, past cardiac medical history, 114 or vascular risk factors, including those included in the AF stroke risk prediction score CHA2DS2-VASc20,52,56,61,112 have also been related to the rate of AF detection. Potentially predictive AF biomarkers derived from blood, cardiac investigations or brain imaging are summarised in Table 4 and below.
Presence of potential blood, echocardiographic, ECG or heart and brain imaging biomarkers compared to their absence for increase the detection of subclinical atrial fibrillation in patients with stroke or TIA of undetermined origin.
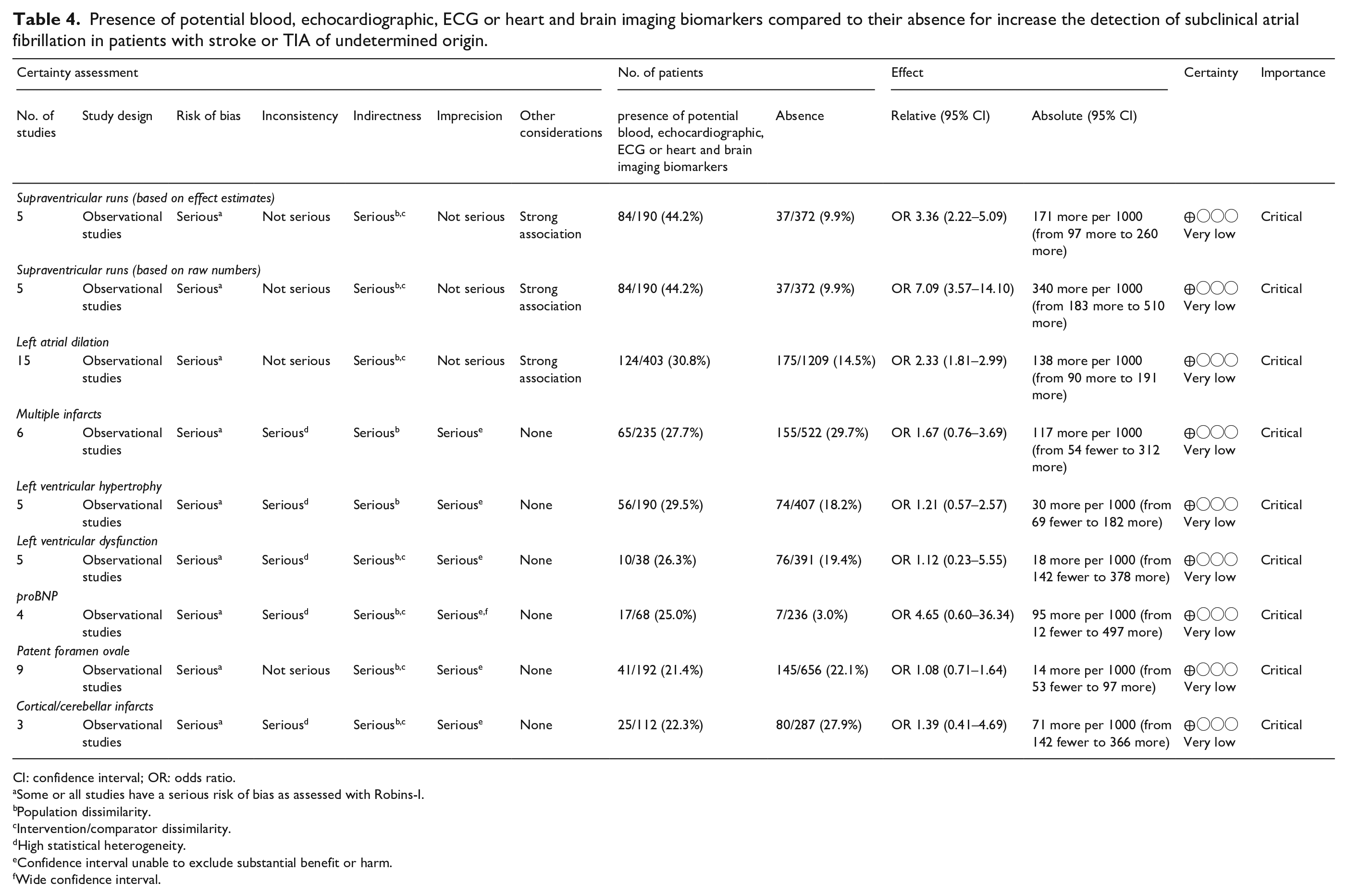
CI: confidence interval; OR: odds ratio.
Some or all studies have a serious risk of bias as assessed with Robins-I.
Population dissimilarity.
Intervention/comparator dissimilarity.
High statistical heterogeneity.
Confidence interval unable to exclude substantial benefit or harm.
Wide confidence interval.
Blood biomarkers
Blood biomarkers previously related to heart failure or myocardial injury (including acute coronary syndromes) are associated with an increased yield of AF detection in patients with ischaemic stroke of undetermined origin. Inflammation and haemodynamic stress trigger the production of natriuretic peptides by cardiomyocytes, which both occur with AF and thrombus formation. Both B-type natriuretic peptide (BNP) or N-terminal pro-BNP (NT-proBNP) have been related to the rate of AF detection after undetermined stroke25,35,47,73,115,116 (Figure e10 of the Supplemental File). Thresholds and accuracies differ between studies, but a recently published meta-analysis 117 suggest a better accuracy for NT-proBNP in AF prediction. Elevated high sensitivity troponin T has also been identified as a biomarker for AF detection in a few studies.25,112,118 Midregional Proatrial Natriuretic Peptide (MRproANP) is a newly biomarker providing additional prognostic information after stroke. Higher MRproANP levels seems to be associated with cardioembolic stroke aetiology and, even more strongly, AF.119,120
Echocardiographic biomarkers
Multiple studies have detected an association between left atrial (LA) dilation and AF occurrence. Different definitions and thresholds, including volume and diameter measures, and sex differences, have been reported20,41,45,48,61,94,121–124 (Figure 14).
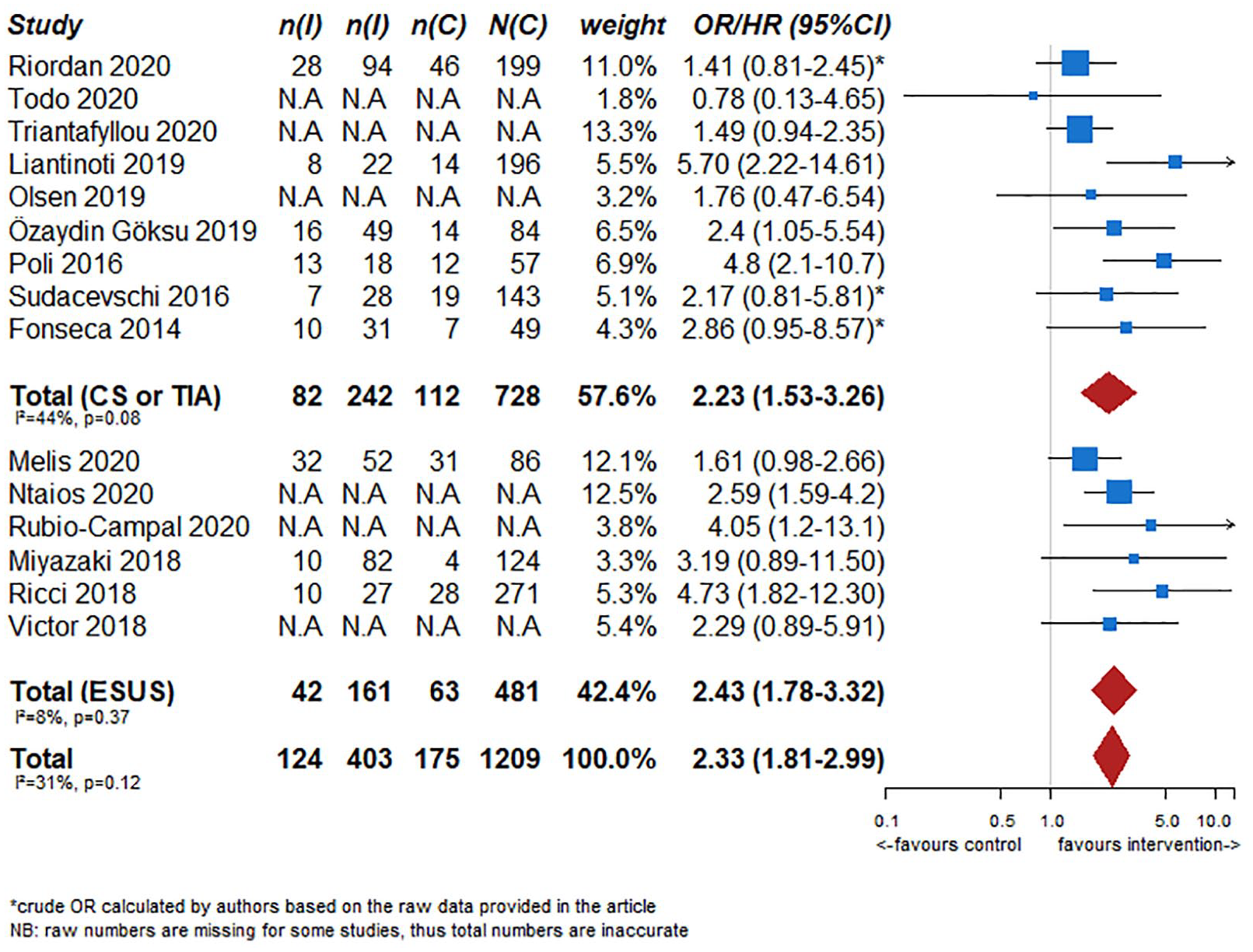
Association between presence of left atrial dilation and atrial fibrillation detection in observational studies.
Perlepe et al. 125 studied 675 ESUS patients from three multicentre European registries (Acute STroke Registry and Analysis of Lausanne, the Athens Stroke Registry and the Larissa Stroke Registry). After testing several thresholds, they found that a 40 mm LA diameter yielded the highest Youden’s J-statistic for AF detection of 0.35 with sensitivity 0.69, specificity 0.66, positive predictive value (PPV) 0.27 and negative predictive value (NPV) 0.92.
In addition to size, other echocardiographic biomarkers of left atrial dysfunction have been related to a higher risk of AF detection in patients with stroke of undetermined origin, including: LA strain,35,59 total atrial conduction time assessed by tissue Doppler imaging, 52 LA emptying fraction measured with 2D echocardiography or lower A′ velocities in ventricular (5.9 ± 2.2 vs 7.2 ± 1.6, p¼ 0.010) and atrial septa (4.8 ± 1.4 vs 5.9 ± 1.4, p¼ 0.013). 122
Furthermore, left ventricular abnormalities (left ventricular ejection fraction depression, left ventricular hypertrophy) have been also related with a higher risk of AF detection, probably because of the known relationship between previous cardiac disease and subclinical AF67,110 (Figures e11 and e12 in the Supplemental File).
Electrocardiographic biomarkers
Abnormalities in ECG or 24-h Holter monitoring related to LA dysfunction have been associated with an increased yield of AF detection during prolonged monitoring of patients with TIA or stroke of undetermined origin. These include premature atrial complexes on ECG,29,43,61,73,100,110,126,127 excessive supraventricular electric activity, 70 atrial ectopic burden, 48 P terminal force in the precordial lead V1, 128 P wave dispersion >40 ms, 32 increased maximum P-wave duration, 52 sinus bradycardia, 31 prolonged PR interval 62 and interatrial conduction block 100 (Figure e13 in the Supplemental File).
Brain imaging biomarkers
Whether defined ischaemic patterns detected by neuroimaging (frequently magnetic resonance imaging, MRI) can identify patients with the higher probability of subclinical AF detection after a TIA or an undetermined ischaemic stroke remains theoretically highly plausible but controversial in practice. Different studies have shown conflicting findings: a sub-study of CRYSTAL AF 129 was not able to detect any acute infarction pattern in the baseline neuroimaging that related to subsequent subclinical AF diagnosis, although chronic brain infarctions (15.8% vs 7.0%; HR 2.84; 95% CI 1.13–7.15; p = 0.02) and leukoaraiosis (18.2% vs 7.9%; HR 2.94; 95% CI 1.28–6.71; p < 0.01) were associated with AF detection in this sub-study.
Conversely, observational studies have shown associations between AF detection and the presence of multiple acute diffusion-weighted imaging MRI lesions,29,130 including cortical-subcortical 62 or bilateral infarct patterns 60 (Figures e14 and e15 in the Supplemental File). Chronic presumed ischaemic lesions have also been related to AF, including cortical or cerebellar lesions 37 or white matter lesions on brain magnetic resonance imaging, 110 as have combined acute and chronic ischaemic lesions together. 130 In addition, recent studies suggest a strong association between intracranial large-vessel occlusion and subsequent AF detection.92,113
The previously described blood, cardiac and neuroimaging biomarker have been identified as promising independent predictors of AF detection in patients with TIA or stroke of undetermined origin. However, the huge variability in the different studies in terms of populations, adjustment for confounding variables, thresholds and imaging definitions preclude their routine use as biomarkers of AF detection in clinical practice. Furthermore, their practice as a selection tool for prolonged monitoring is also debatable, as they have insufficient negative predictive value to avoid missing subclinical AF in patients with a lower but still clinically important chance of detecting it. The MWG identified this as an area for future research.
Outcome: Rate of anticoagulation
Analysis of current evidence
Given the higher probability of AF detection in patients with the previously described potential biomarkers, it is reasonable to suspect that they would increase the rate of anticoagulation when AF is detected. However, the available data are derived from observational studies which were not designed to investigate this question.
Outcome: Rate of recurrent stroke or systemic embolism, intracranial haemorrhage or major haemorrhage and mortality or improve functional outcome
Analysis of the current evidence
There are no data regarding the influence of the addition of potential AF biomarkers on outcomes in patients with stroke or TIA of undetermined origin.
Additional information
RE-SPECT ESUS and NAVIGATE-ESUS were two RCTs aimed to demonstrate the benefit of non-vitamin K antagonist oral anticoagulants (NOAC) in patients with ESUS.98,99 The rationale of both studies assumed that a high proportion of ischaemic strokes would be caused by subclinical AF. The studies were not designed to search for AF detection by longer monitoring and only the basic work-up for AF to meet the ESUS definition was required (i.e. 24 h-monitoring). The negative ESUS trial results discourage treatment with anticoagulation based on brain and vascular imaging only, supporting a more intensive and prolonged monitoring for AF detection. The results also raise the question of whether adding potential AF prediction biomarkers could allow better selection of patients who might benefit from oral anticoagulation. There is increasing evidence of the relevance of atrial cardiomyopathy in patients with undetermined stroke or TIA, even in the absence of AF. 131 Atrial cardiomyopathy has been defined as an atrial disorder characterised by clinically relevant manifestations related to complex structural, architectural, contractile and electrophysiological changes. A simple definition or quantification system has not been established. 132 Two RCTs have included different AF biomarkers of atrial cardiomyopathy to select patients for NOAC treatment in patients with ESUS. ATTICUS (Apixaban for Treatment of Embolic Stroke of Undetermined Source, NCT02427126) included patients with a high risk profile for cardiac embolism (i.e. at least one of the following criteria: LA size >45 mm, spontaneous echo contrast in LA appendage, LA appendage flow velocity ⩽0.2 cm/s, atrial high-rate episodes, CHA2DS2-VASc score ⩾4, PFO), who were randomised to apixaban versus aspirin. Patients received long-term ECG monitoring by an implantable device. The study was recently stopped due to futility. The rate of AF detection was 23%, while the rate of stroke recurrence after 12 months was documented at 6.8%. Nevertheless, final details are still lacking at the time of writing this guideline. 133 Another study, ARCADIA (AtRial Cardiopathy and Antithrombotic Drugs In Prevention After Cryptogenic Stroke, NCT03192215) is now randomising ESUS patients with atrial cardiomyopathy (P-wave terminal force >5000 µV × ms in ECG lead V1, serum NT-proBNP > 250 pg/mL and LA diameter index ⩾3 cm/m2 on echocardiogram) for treatment with apixaban or aspirin. The primary efficacy outcome is recurrent stroke and primary safety outcomes are symptomatic intracranial haemorrhage or non-intracranial major haemorrhages. 134 The MidregiOnal Proatrial Natriuretic Peptide to Guide SEcondary Stroke Prevention (MOSES) trial is addressing the question if a biologically distinct subgroup of ischaemic stroke patients without known atrial fibrillation at admission, selected by a cut-off level of MRproANP concentration, which represents a underlying increased risk of cardiac thrombogenicity, benefits from direct oral anticoagulation versus antiplatelets as preventive treatment (NCT03961334).
Final results from these trials may increase the evidence of the relevance of biomarkers for AF detection, anticoagulation treatment and outcomes.
Outcome: Detection of subclinical AF
Analysis of the current evidence
The percutaneous closure of PFO is considered a safe and effective option as secondary prevention for patients with cryptogenic stroke aged <60 years. 135 An underlying subclinical newly diagnosed AF may question the indication for PFO closure or even render PFO closure unnecessary, especially in patients older than 60 years.
Currently, there have not been any RCTs that have compared implantable monitoring devices to any non-implantable external monitoring devices to detect subclinical AF in patients with PFO.
Additional information
In an observational study, 136 62 patients older than 55 years with cryptogenic stroke and high risk PFO (permanent right-to-left shunt and one or more of the following risk factors: atrial septal aneurysm, prominent Eustachian valve, recurrent brain ischaemia, previous deep vein thrombosis, thrombophilia not requiring oral anticoagulation) had an implanted loop recorder; 28 patients underwent percutaneous PFO closure. Before implantation, all patients underwent a 12-lead ECG, 48-h in-hospital continuous telemetry and 24-h Holter monitoring. Among the 28 patients who underwent closure, prolonged monitoring led to a 6-month paroxysmal AF (>5 min) detection rate of 14.3% (4/28) compared to 0% in the remaining 34 medically treated patients. Regarding clinical events at follow-up (mean duration 18.9 ± 11.9 months), 1 (1.4%) patient had a recurrent stroke, whereas 1 (1.4%) had bleeding.
Another study that included patients with cryptogenic stroke <55 years observed paroxysmal AF (>30 s) in two patients (7.4%) out of 27 patients with PFO over a 3-week period of Holter monitoring. Before this monitoring, all the patients had undergone 24-h Holter monitoring. 25
Finally, a third study, 69 enrolling 22 patients (mean age 65 ± 9 years) with ESUS and PFO, reported paroxysmal AF (>2 min) in nine patients (40.9%) after ILR implantation (36 months of follow-up). Prior to implantation, all the patients had undergone serial 12-lead ECGs, 24-h Holter monitoring and continuous stroke unit ECG monitoring for >72 h. Furthermore, another observational study 56 recorded five patients (22.7%) with paroxysmal AF lasting >2 min after ILR implantation (mean follow-up 12.7 ± 5.5 months) in 22 consecutive patients with ESUS and PFO.
In a pooled analysis of these studies in patients with PFO, the paroxysmal AF rate detection was 18.4% (10.6% in patients with cryptogenic stroke and 31.6% in patients with ESUS) after the implantation of monitoring devices (Figure e16 in the Supplemental File).
In addition to our data, a recent meta-analysis found that the presence of PFO is associated with a lower risk of AF detection in patients with ischaemic stroke or TIA. 137 Another study by Yasaka et al. found that risk of AF was higher in PFO patients who were older. For these reasons, in younger patients with stroke, the presence of PFO may prevent prolonged cardiac rhythm monitoring, especially when the patient has not risk factors for AF (uncontrolled hypertension or diabetes, congestive heart failure. . .) and/or the clinical stroke and anatomical PFO characteristics (large right-to-left shunt, associated atrial septal aneurism. . .) suggest a PFO-related embolism.138,139 On the contrary, prolonged cardiac monitoring should also be considered in young patients. However, in older patients, we consider that prolonged cardiac monitoring should be performed similarly in patients with or without PFO. As commented in PICO 1, the maximum duration recommended for this monitoring is unknown. PFO closure has demonstrated reduction of recurrent stroke in patients until 60 years. Other considerations, in addition to prolonged cardiac monitoring, like clinical stroke characteristics or anatomical PFO features should lead the multidisciplinary decision of PFO closure in older patients. A recently published European position paper suggests that all patients with cryptogenic stroke and PFO should undergo a routine 12 lead ECG and either in-patient cardiac telemetry or 24-h Holter monitoring. 139 In patients older than 55 years, prolonged monitoring is recommended for more than 48 h, preferably with an implantable loop recorder. They also suggest that the device evaluation period should last at least 6 months before deciding on PFO closure or oral anticoagulation. A comment about the indication for oral anticoagulation in this group of patients is also provided: paroxysmal AF episodes lasting more than 30 s detected with intermittent recordings or more or equal than 5 min during implantable cardiac monitoring can be considered sufficient to evaluate patients for oral anticoagulation.
Outcome: Rate of anticoagulation
Analysis of the current evidence
To date, there have not been any RCTs that have compared implantable monitoring devices with any non-implantable external monitoring devices for the detection of subclinical AF and increase in the rate of anticoagulation in patients with PFO; there is therefore continued uncertainty over the risks and benefits of oral anticoagulation.
Outcome: Rates of recurrent stroke or systemic embolism, mortality, intracranial haemorrhage and major haemorrhage (intracranial or extracranial)
Analysis of the current evidence
There have not been any RCTs that have compared the use of implantable monitoring devices to any non-implantable external monitoring devices to reduce the rates of recurrent stroke or systemic embolism, mortality, intracranial haemorrhage and major haemorrhage (intracranial or extracranial) in patients with PFO; therefore, there is therefore continued uncertainty over reduction of recurrent stroke or systemic embolism, mortality, intracranial haemorrhage and major haemorrhage.
All recommendations are summarised in Table 5.
Synoptic table of all recommendations and expert consensus statements.
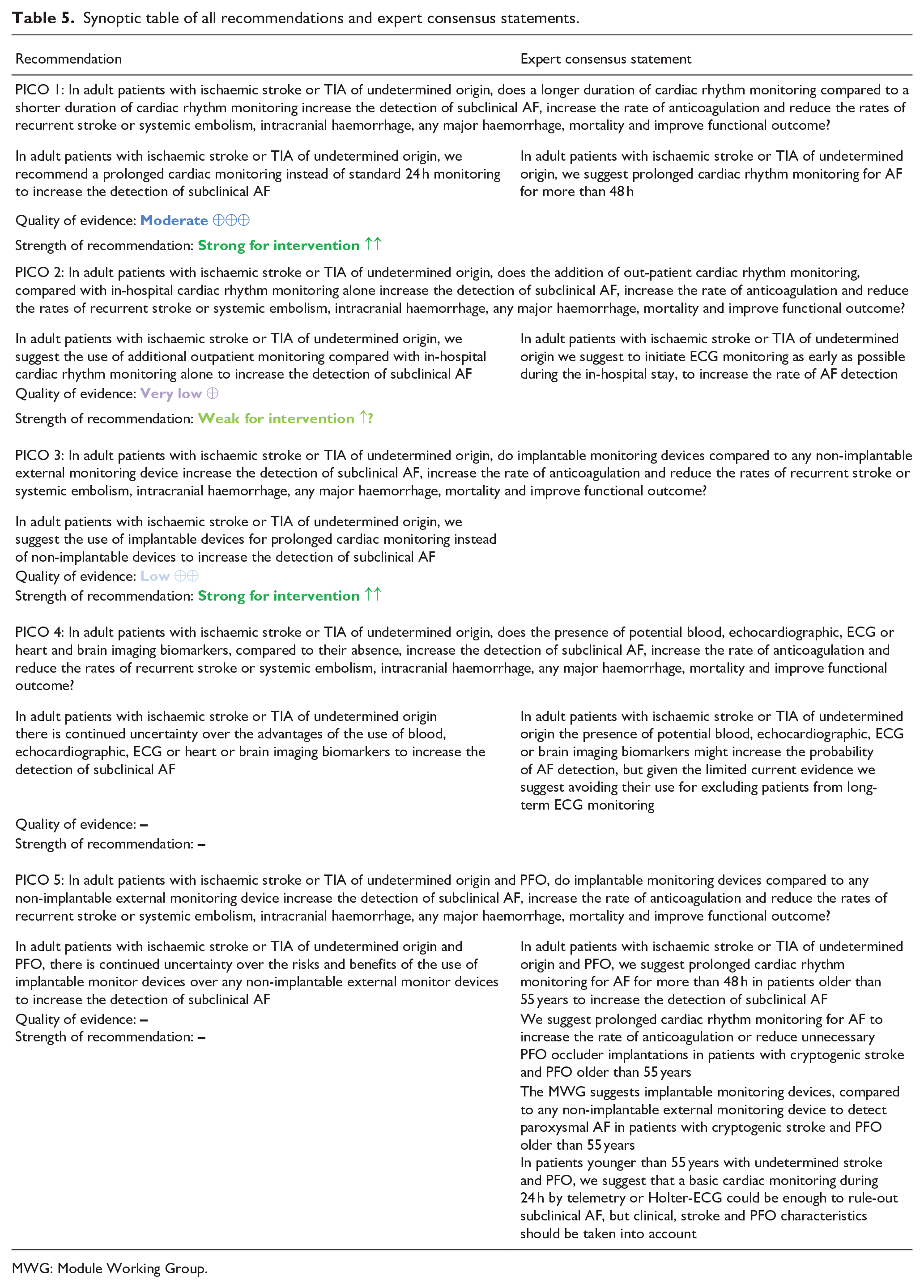
MWG: Module Working Group.
Discussion
This guideline document was conceived according to the GRADE methodology and aims to provide evidence-based recommendations on screening for subclinical AF after stroke or TIA of undetermined origin. A limitation of the guidelines is that they are focussed on screening of AF in patients with TIA or stroke or undetermined origin, but not all stroke subtypes. Therefore, studies aimed at other stroke aetiologies have not been included in the main analysis, but whenever the data was considered relevant, we included them as additional information.
First, we defined a set of outcomes relevant for the Guidelines theme, and grading was performed according to Delphi voting. Even if clinical outcomes were considered theoretically the most relevant, discussion between the MWG raised the concern (later-on confirmed) that few clinical outcomes would probably be found in the literature search. Therefore, subclinical AF detection was considered a good surrogate marker for clinical outcome and obtained the higher score during Delphi voting. We organised our PICO questions to determine the effects of cardiac rhythm monitoring duration, setting (in-hospital vs outpatient), monitoring device type (implantable vs non-implantable) and according to patient phenotype (with and without a PFO). We also assessed potential biomarkers that could help to predict the likelihood of detecting subclinical AF. In every PICO we prioritised evidence collected from RCTs or meta-analyses of RCTs, when these were available, rather than observational studies. However, where no RCT evidence was available we considered appropriate observational data for expert consensus statements.
Based on the result of RCTs, we strongly recommend a longer duration of cardiac rhythm monitoring (i.e. more than 48 h), instead of no-monitoring or standard 24 h-monitoring to increase the detection of subclinical AF. Although there are currently no RCT data directly comparing shorter versus longer cardiac rhythm monitoring with anticoagulation initiation as the primary outcome, we also advise longer duration cardiac rhythm monitoring to increase the rate of anticoagulation once AF is detected (as shown from subgroup analyses of RCT and observational studies). Other questions remain outstanding. First, the optimal maximal duration of monitoring for subclinical AF remains uncertain; the yield clearly increases with increasing duration of cardiac rhythm monitoring, but existing studies – with different designs and durations of monitoring – do not yet allow a clear definition of the upper time limit. Indeed, few studies have monitored for more than 6 months so whether an upper time limit exists beyond this is undefined; very prolonged monitoring may have resource and cost-effectiveness implications with diminishing returns beyond a certain extended duration. Another issue is whether detection of AF late after stroke implies that the previous stroke is caused by the subclinical AF. The probability of having AF increases with age; if individuals without stroke, matched for age and risk factors, did a long-term monitoring, probably a high rate of subclinical atrial fibrillation would be found. Second, the minimum duration of AF that should be considered causal and lead to anticoagulation remains unclear; although we prespecified a minimum duration of ⩾30 s, there is no definitive evidence that patients with paroxysmal AF duration of <30 s should be excluded from anticoagulation therapy.
We did not identify RCTs or observational studies directly addressing whether adding outpatient monitoring to in-hospital cardiac rhythm monitoring might increase subclinical AF detection. Any increased yield from outpatient monitoring might be simply because of a longer screening period, rather than any difference due to the setting. On the other hand, patients might be more physically active after hospital discharge, which could induce the extent of detectable AF, but this hypothesis remains unproven. Considering the limited high-quality evidence available, and the usual stroke clinical care pathway, our expert consensus recommendation is to initiate in-hospital monitoring as soon as possible after acute ischaemic stroke or TIA and complete it with outpatient monitoring in order to practically achieve longer duration cardiac rhythm monitoring, as was shown to increase the rate of AF detection in PICO 1.
When considering monitoring devices, implantable devices show an increased AF detection rate when compared to external loop-recorders, but this difference seems to be explained by a longer monitoring duration rather than an increased AF detection capacity related to the type of device. There remains a lack of RCTs focussing on a direct comparison between different monitoring strategies controlling for monitoring duration, but given the capability of implantable loop recorders to monitor for years, a RCT comparing with other technologies is unrealistic. Implantable monitoring strategies also show increased anticoagulation therapy in interventional groups, and reduction of recurrent stroke in observational studies. Therefore, we suggest their use, and if possible, as a first line strategy. Although some studies suggest a progressive strategy, evidence supporting it is lacking. In fact, economic models recommend the direct implantation of a loop recorder over other prolonged non-implantable monitoring because of its efficiency; whether this can be assumed in all health-care systems is a matter of debate. Furthermore, other cost-effectiveness models suggest benefit also from shorter monitoring periods (7–10 or 30 days) with external devices, with some suggesting even cost savings. 140
In this guideline we also investigated potential biomarkers of AF detection to identify patients at higher risk of having AF which could allow targetted screening to increase its cost effectiveness. We did not find any RCTs to support the use of biomarkers. Our group consensus was that the role of blood, echocardiographic, ECG or brain imaging biomarkers remains uncertain, but there is weak evidence supporting their promise to identify patients most appropriate for prolonged cardiac rhythm monitoring. Echocardiographic findings, such as increased left atrial diameter and left ventricular abnormalities, have been related to a higher risk of AF detection, as have several abnormalities in ECG, blood biomarkers (such as NT-proBNP or Troponin) and brain imaging findings (as multiple territories infarcts or cortico-subcortical infarcts). However, evidence is currently not sufficient to support the routine use of these biomarkers during investigation for subclinical AF. Therefore, even if these biomarkers of AF are not detected, prolonged monitoring should not be avoided. We identified the value of biomarkers to predict AF as an important area for future research.
In the specific subgroup of patients with PFO we found insufficient evidence for the use of implantable monitor devices over any non-implantable external monitor device to increase the detection of subclinical AF based on RCT. However, based on limited observational evidence in patients with PFO older than 55 years, our expert consensus was that it is reasonable to monitor these patients for more than 48 h, if possible, with implantable devices and initiate, if AF is detected, oral anticoagulants. However, further data, ideally from RCTs, are needed to confirm the value of this approach.
This guideline has both strengths and limitations. Strengths include a systematic approach to searching the literature and a structured process for generating recommendations according to the GRADE methodology. A limitation of our study is that for observational studies, we did not implement the variance-stabilising double arcsine transformation before pooling the prevalence of AF detection from each study and before the synthesis of proportions for the studies aimed for prolonged monitoring for AF detection.
Our search identified RCT data for the PICO related to comparing a longer versus a shorter cardiac rhythm monitoring to increase the rate of detection of subclinical AF and anticoagulation initiation, but not for the remaining clinically relevant outcomes, although there was strong consensus in the MWG that detecting AF should plausibly lead to improved outcomes. A very recent metaanalysis, published after the literature search and data analysis of the present guidelines and including patients with stroke or TIA of different aetiologies, also shows that prolonged post-stroke cardiac monitoring increases AF detection and anticoagulant initiation. Data from observational studies also suggests a reduction of stroke recurrence, but this has not been confirmed by RCT. 141
Our findings indicate a research need for RCTs and high-quality observational studies to directly determine whether different monitoring strategies or biomarkers can influence key clinical outcomes including the rates of anticoagulation, recurrent ischaemic stroke or systemic embolism, intracranial haemorrhage, any major haemorrhage, mortality or improved functional outcome.
Another relevant question that remains to be clarified with RCT data is the use of prolonged ECG monitoring in patients with PFO older than 55 years. Finally, it is necessary to clarify the minimum duration of paroxysmal AF duration that increases stroke risk.
As technology develops, prolonged monitoring is likely to become more widely available. There is an increasing number of certified wearable devices which could greatly increase the ease of prolonged monitoring in the community, yet also posing challenges such as assessing diagnostic accuracy and optimising the collection and analysis of the large amount of rhythm data generated.12,142 For example, ongoing clinical trials using smartwatches (e.g. HEARTLINE (NCT04276441)) aim to assess whether accurate and early AF diagnosis reduces the risk of thromboembolic events.
Future research must also focus on defining the optimal selection of patients for intensive cardiac rhythm monitoring strategies. Better predictive ability could improve the identification of patients who would most benefit from long duration monitoring, improving diagnostic yield and cost-effectiveness. In 2014, the concept of ESUS was defined, considering that it would identify patients in whom anticoagulation would lead to reduction of stroke recurrence. A minimum set of work-up for stroke patients to diagnose ESUS was required. However, the neutral results from RCTs using the simple clinical and radiological criteria for ESUS – including RE-SPECT ESUS and NAVIGATE-ESUS – further highlight the need of a more extensive diagnostic workup in patients with stroke of undetermined origin. A non-depreciable proportion of ESUS are probably related to aetiologies without indication for anticoagulation, and therefore prolonged cardiac monitoring should be a requirement in these patients. Whether redefinition of the ESUS concept including a wider workup is needed, or its actual lack of usefulness compared with the previous aetiological stroke categories, is again another matter of debate.143,144
A clear pragmatic message from these guidelines is that to maximise AF detection, clinicians should perform the longest possible cardiac rhythm monitoring, starting as soon as possible, in patients with stroke or TIA of undetermined origin. The longer the period of monitoring, the greater the diagnostic yield of AF. However, our search identified the need for RCTs to definitively determine if increased AF detection improves important clinical outcomes.
Plain language summary
Ischaemic stroke occurs when an artery of the brain is occluded by a thrombus, and it is the main cause of adult disability in our society. If the patient recovers without sequelae and without a lesion in the brain within 24 h, we term the event a transient ischaemic attack (TIA). TIAs, although not in themselves disabling, are also relevant because they imply a high risk of having a new ischaemic stroke later. In almost 25% of cases, despite a complete work-up, we cannot find the aetiology of the ischaemic stroke or TIA, and we defined these cases as ‘stroke of undetermined origin’.
Atrial fibrillation (AF) is the most frequent alteration of the rhythm of the heart (arrythmia). It can induce clot (thrombus) formation in the left atrium (a chamber in the heart), and these thrombi can travel through the blood and block (occlude) an artery in the brain (a process calls ‘embolism’), causing what we term a ‘cardioembolic stroke’. Anticoagulant (‘inhibition of blood clotting’) treatment effectively prevents thrombus formation in AF, and it is the treatment of choice in these patients to avoid stroke or embolisms to other parts of the body. However, AF is frequently subclinical and paroxysmal (in other words it does not cause symptoms and the rhythm of the heart varies from AF to normal (sinus) rhythm), so it is difficult to diagnose. Stroke specialists suspect that a high proportion of stroke of undetermined origin are caused by subclinical AF. The only way to detect subclinical AF is by monitoring the rhythm of the heart with different devices based on recording a heart trace called an electrocardiogram (ECG). Finding AF in patients with stroke of undetermined origin has crucial implications for choosing the most effective drugs to prevent thrombus formation (anticoagulants or antiplatelet drugs, collectively termed antithrombotic agents) and new strokes. This guideline is aimed to provide recommendations for the screening for subclinical AF in stroke or TIA of undetermined origin.
To develop the guideline, a group of experts selected by the European Stroke Organization (ESO) joined in a module working group (MWG) and selected five relevant questions for the management of patients with stroke or TIA of undetermined origin regarding AF screening. Relevant outcomes were also selected, and the MWG looked for the evidence in previous studies to recommend actions for clinicians treating these patients.
First, the MWG found evidence that prolonged ECG monitoring compared to shorter ECG monitoring increases the detection of subclinical AF. It also appears to increase the initiation of anticoagulant therapy, but we could not prove that prolonged monitoring reduces the risk of new strokes or other complications of AF. Therefore, we recommend prolonged ECG monitoring, and the MWG considers reasonable for more than 48 h in patients with TIA or stroke of undetermined origin. If AF is found, and it lasts at least 30 s, anticoagulation should be initiated. It is reasonable to initiate the ECG monitoring early, if possible, during the in-hospital stay, besides we recommend adding outpatient ECG monitoring to increase the monitoring-time, and therefore, the rate of AF detection. Different devices have been developed to monitor ECG. Implantable loop recorders (ILR) are placed subcutaneously close to the heart, and they allow ECG monitoring during several months (up to about 3 years), but they are expensive. We recommend use of ILR to prolong ECG monitoring in some patients with undetermined stroke to increase the monitoring time and AF detection, but it is reasonable to perform a progressive screening strategy, starting with safer and less expensive non-implantable devices followed by (if necessary), an ILR. Several characteristics in blood samples, heart scans (echocardiograms), ECG or scans imaging of the brain have been associated with an increased risk of subclinical AF (‘biomarkers’), but we could not confirm the advantages of their use in patients with stroke of undetermined origin, and we do not recommend excluding patients from prolonged ECG monitoring if they are not found. Finally, patent foramen ovale (PFO) is a communication between both atria in the heart that has been associated with ischaemic stroke, especially in young patients; it can be closed by a heart catheterisation procedure which reduces the risk of stroke recurrence. In patients with undetermined stroke and PFO, we could not find evidence of the advantages of ILR for AF detection over any non-implantable device. However, we consider reasonable prolonged ECG-monitoring for more than 48 h, if feasible, with ILR, for screening for subclinical AF in PFO patients older than 55 years. If AF lasting 30 s or more is detected, anticoagulation therapy should be initiated.
In conclusion, prolonged ECG monitoring in patients with stroke or TIA of undetermined origin increases the detection of subclinical AF, and it may increase the initiation of anticoagulant therapy in patients who should benefit from this treatment.
Supplemental Material
sj-docx-1-eso-10.1177_23969873221099478 – Supplemental material for European Stroke Organisation (ESO) guideline on screening for subclinical atrial fibrillation after stroke or transient ischaemic attack of undetermined origin
Supplemental material, sj-docx-1-eso-10.1177_23969873221099478 for European Stroke Organisation (ESO) guideline on screening for subclinical atrial fibrillation after stroke or transient ischaemic attack of undetermined origin by Marta Rubiera, Ana Aires, Kateryna Antonenko, Sabrina Lémeret, Christian H Nolte, Jukka Putaala, Renate B Schnabel, Anil M Tuladhar, David J Werring, Dena Zeraatkar and Maurizio Paciaroni in European Stroke Journal
Supplemental Material
sj-pdf-2-eso-10.1177_23969873221099478 – Supplemental material for European Stroke Organisation (ESO) guideline on screening for subclinical atrial fibrillation after stroke or transient ischaemic attack of undetermined origin
Supplemental material, sj-pdf-2-eso-10.1177_23969873221099478 for European Stroke Organisation (ESO) guideline on screening for subclinical atrial fibrillation after stroke or transient ischaemic attack of undetermined origin by Marta Rubiera, Ana Aires, Kateryna Antonenko, Sabrina Lémeret, Christian H Nolte, Jukka Putaala, Renate B Schnabel, Anil M Tuladhar, David J Werring, Dena Zeraatkar and Maurizio Paciaroni in European Stroke Journal
Footnotes
Acknowledgements
The authors would like to thank Yvonne Bruchert and Sabrina Mutter for assistance and guidance. They also would like to thank Simona Sacco and Guillaume Turc, Chairs of the ESO Guidelines Board, for the advice and extremely useful revision of the final draft of the guidelines. Finally, we acknowledge the Board of the Stroke Council of the European Society of Cardiology for their support to this Guidelines
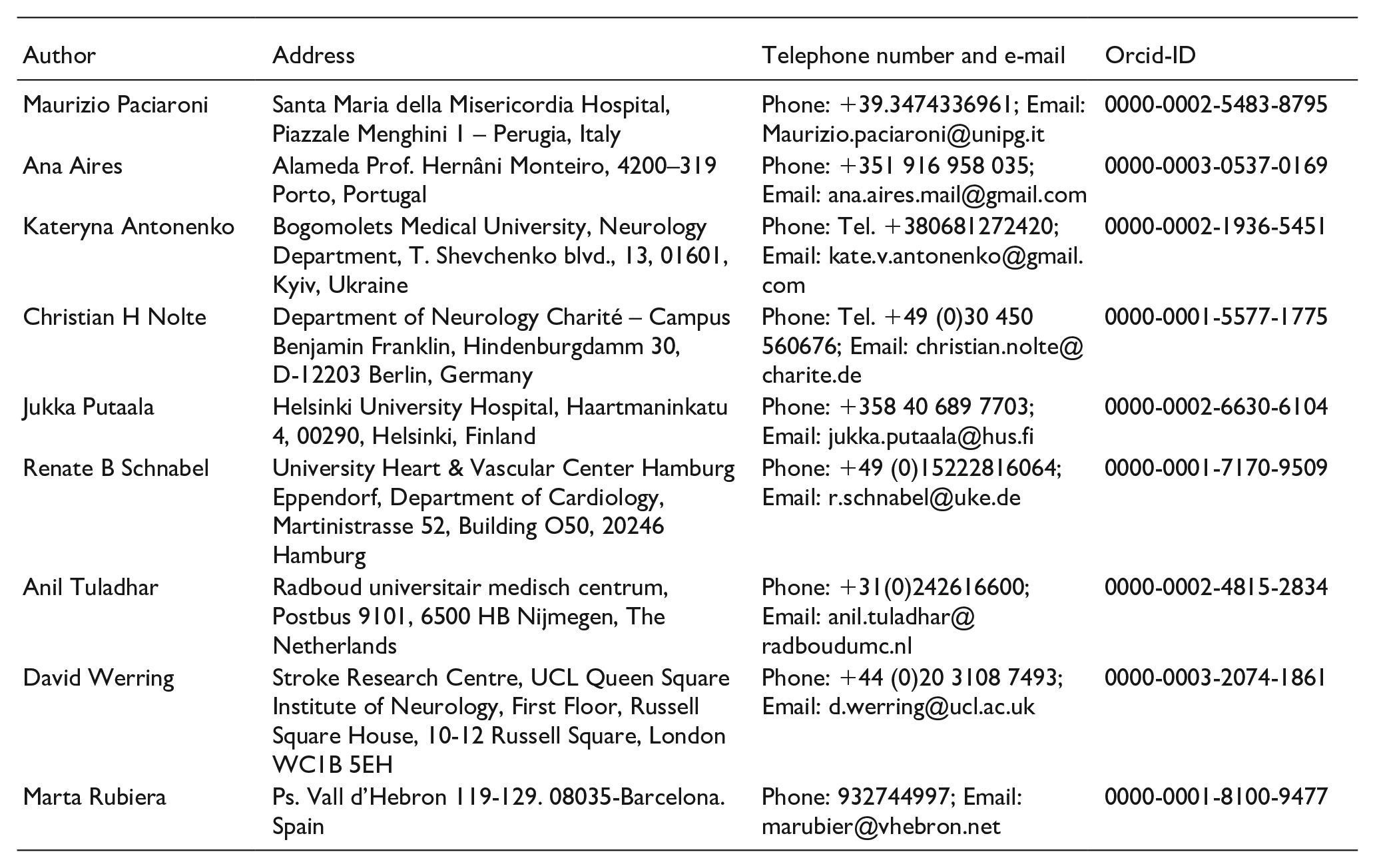
| Author | Address | Telephone number and e-mail | Orcid-ID |
|---|---|---|---|
| Maurizio Paciaroni | Santa Maria della Misericordia Hospital, Piazzale Menghini 1 – Perugia, Italy | Phone: +39.3474336961; Email: |
0000-0002-5483-8795 |
| Ana Aires | Alameda Prof. Hernâni Monteiro, 4200–319 Porto, Portugal | Phone: +351 916 958 035; Email: |
0000-0003-0537-0169 |
| Kateryna Antonenko | Bogomolets Medical University, Neurology Department, T. Shevchenko blvd., 13, 01601, Kyiv, Ukraine | Phone: Tel. +380681272420; Email: |
0000-0002-1936-5451 |
| Christian H Nolte | Department of Neurology Charité – Campus Benjamin Franklin, Hindenburgdamm 30, D-12203 Berlin, Germany | Phone: Tel. +49 (0)30 450 560676; Email: |
0000-0001-5577-1775 |
| Jukka Putaala | Helsinki University Hospital, Haartmaninkatu 4, 00290, Helsinki, Finland | Phone: +358 40 689 7703; Email: |
0000-0002-6630-6104 |
| Renate B Schnabel | University Heart & Vascular Center Hamburg Eppendorf, Department of Cardiology, Martinistrasse 52, Building O50, 20246 Hamburg | Phone: +49 (0)15222816064; Email: |
0000-0001-7170-9509 |
| Anil Tuladhar | Radboud universitair medisch centrum, Postbus 9101, 6500 HB Nijmegen, The Netherlands | Phone: +31(0)242616600; Email: |
0000-0002-4815-2834 |
| David Werring | Stroke Research Centre, UCL Queen Square Institute of Neurology, First Floor, Russell Square House, 10-12 Russell Square, London WC1B 5EH | Phone: +44 (0)20 3108 7493; Email: |
0000-0003-2074-1861 |
| Marta Rubiera | Ps. Vall d’Hebron 119-129. 08035-Barcelona. Spain | Phone: 932744997; Email: |
0000-0001-8100-9477 |
Declaration of conflicting interests
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the development of these guidelines was provided by the European Stroke Organisation, Basel, Switzerland. The author(s) did not receive financial support for the development, writing and/or publication of this guideline.
Ethical approval
Ethical approval was not necessary for the work described in this paper.
Guarantor
A specific guarantor does not exist. The working group has jointly developed the manuscript.
Author contributions
Marta Rubiera and Maurizio Paciaroni wrote the first draft of the manuscript. Sabrina Lémeret conducted the statistical analyses. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.