
Abstract
The European Stroke Organisation (ESO) guidelines on Moyamoya Angiopathy (MMA), developed according to ESO standard operating procedure and Grading of Recommendations, Assessment, Development and Evaluation (GRADE) methodology, were compiled to assist clinicians in managing patients with MMA in their decision making. A working group involving neurologists, neurosurgeons, a geneticist and methodologists identified nine relevant clinical questions, performed systematic literature reviews and, whenever possible, meta-analyses. Quality assessment of the available evidence was made with specific recommendations. In the absence of sufficient evidence to provide recommendations, Expert Consensus Statements were formulated. Based on low quality evidence from one RCT, we recommend direct bypass surgery in adult patients with haemorrhagic presentation. For ischaemic adult patients and children, we suggest revascularization surgery using direct or combined technique rather than indirect, in the presence of haemodynamic impairment and with an interval of 6–12 weeks between the last cerebrovascular event and surgery. In the absence of robust trial, an Expert Consensus was reached recommending long-term antiplatelet therapy in non-haemorrhagic MMA, as it may reduce risk of embolic stroke. We also agreed on the utility of performing pre- and post- operative haemodynamic and posterior cerebral artery assessment. There were insufficient data to recommend systematic variant screening of RNF213 p.R4810K. Additionally, we suggest that long-term MMA neuroimaging follow up may guide therapeutic decision making by assessing the disease progression. We believe that this guideline, which is the first comprehensive European guideline on MMA management using GRADE methods will assist clinicians to choose the most effective management strategy for MMA.
Introduction
Moyamoya angiopathy (MMA) is a chronic cerebrovascular disorder characterised by progressive bilateral steno-occlusion of the supraclinoid internal carotid artery (ICA) and its main branches, and the development of a collateral network of fragile vessels (named ‘moyamoya’ in Japanese language) in the deep areas of the brain.1,2 Despite its increasing recognition worldwide, MMA is still considered a rare disease. 3 It occurs more frequently in East-Asian countries, particularly in Japan (incidence rate up to 0.54 per 100,000) but the disease is 10 times less frequent in Western countries (0.047–0.086 per 100,000).4–7 However, MMA is probably underestimated outside East-Asia and may be an increasing health issue in Europe. 8 MMA is conventionally classified as Moyamoya disease (MMD), when it occurs as idiopathic disease or Moyamoya syndrome (MMS) when it is associated with inherited (i.e. Down syndrome, type I Neurofibromatosis or Sickle Cell Disease) or acquired conditions (i.e. head and neck radiotherapy).9–11 The most common clinical features are cerebrovascular events (transient ischaemic attacks – TIA, ischaemic and haemorrhagic strokes and subarachnoid haemorrhage – SAH) which originate respectively from the steno-occlusive process of intracranial ICAs bifurcation and from the rupture of fragile collateral vessels, leptomeningeal anastomosis or associated saccular aneurysms.9–13 The clinical presentation differs according to age and ethnicity: adults may present with transient or permanent cerebral ischaemic events and intracranial haemorrhages, children present mainly with ischaemic events whereas Western adults tend to present with a lower rate of haemorrhage than East-Asian patients.6,7,10–12,14–16 Cognitive deficits, migraine-like episodes, psychiatric and movement disorders are also common disease features.11,13 Although the clinical expression of the disease largely varies between patients, MMA can have a rapid progression leading to severe disabilities, mostly in paediatric cases but also in adults.10,17,18 The pathogenesis of MMA is still largely unknown, although an imbalance of angiogenic factors and genetic susceptibility are believed to be involved in the pathophysiology.9,10,19 The role of genetic factors is supported by several elements including the association of MMA with heritable disorders, the high familial rate in East Asia and the geographical distribution of the disease.19–21 Particularly, a variant of the RNF213 gene, p.R4810K with a strong founder effect was found in East-Asians with MMA but not in Western patients whereas the role of other RNF213 gene variants20,22 has apparently less association with the disease.23–30 The diagnosis of MMA is confirmed according to established angiographic diagnostic criteria,31,32 requiring the presence of a bilateral stenosis or occlusion at the terminal portion of the ICAs and/or at the proximal portion of the anterior and/or the middle cerebral arteries and the development of a network of fragile collateral vessels in the vicinity of the occlusive or stenotic lesions.31,32 In a variable proportion of MMA patients, posterior circulation (mainly posterior cerebral artery-PCA) may be involved. Although cerebral MRI and MRA are increasingly used to identify the main MMA neuroradiological hallmarks, cerebral digital subtraction angiography (DSA) is still performed for diagnostic confirmation but also for collaterals and vessel status evaluation. Patient diagnostic work up usually includes haemodynamic assessment by transcranial ultrasound examination and perfusion imaging evaluation by perfusion CT or MRI with or without acetazolamide (ACZ) and/or ACZ single photon emission computed tomography (SPECT) or quantitative H2[15O] positron emission tomography (PET).12,33,34 Although these techniques are currently used not only to assess the disease severity but also to establish indication to surgery, they are not validated, and no standardised indications are provided for pre-operative and outcome patient assessment.35–37
To date, no treatment limiting the progression of the occlusive arterial lesions is available for MMA patients and strategies aiming at reducing the risk of further cerebrovascular events employ surgical revascularization techniques.38–40 The surgical methods are mainly divided into direct revascularization, in which the superficial temporal artery (STA) – a branch of the external carotid artery (ECA) – is directly anastomosed with the middle cerebral artery (MCA) or the anterior cerebral artery (ACA), and indirect revascularization (synangiosis procedures) in which tissues encompassing ECA branches (dura mater, temporal muscle, galeal tissue, or superficial temporal artery) are placed in contact with the surface of the ischaemic brain. Potential indications for revascularization surgery include ischaemic symptoms, a decreased regional cerebral blood flow or a cerebrovascular reserve (CVR) decrease on perfusion imaging.41–44 Moreover, although recent meta-analyses suggest the efficacy of surgical revascularization in symptomatic MMA patients, the optimal surgical procedure as well as the timing of surgery remain controversial. Usually, decisions on the surgical approach depend on the neurosurgeon’s expertise and on the condition of the donor and recipient arteries.35,45 Therefore, although some care pathways have been proposed, 42 a consensus on management and treatment of MMA, especially in European patients, has never been achieved.
The aim of this guideline is to provide recommendations guiding stroke clinicians and researchers to ensure the best diagnostic and therapeutic management strategies when assessing patients with a diagnosis of MMA, with the final objective of reducing the risk of stroke recurrence and long-term disability.
Methods
Composition and approval of the Module Working Group
These guidelines were initiated by the European Stroke Organisation (ESO). Two chairpersons (AB and DH) were selected to assemble and coordinate the Guideline Module Working Group (MWG). The final group contained 10 experts (AB, NK, BF, FA, IC, ETL, PV, MZ, MK, DH). All 10 are experts in cerebrovascular disease with a special interest in MMA. MWG included six vascular neurologists, three neurosurgeons and one geneticist. Of the 10 MWG members, all are working in Europe. Two methodologists (SH, SL) supported the literature search as well as performed data extraction, risk of bias assessment and meta-analyses independently.
The ESO Guideline Board and Executive Committee reviewed the intellectual and financial disclosures of all MWG members and approved the composition of the group. The full details of all MWG members and their disclosures are included in Supplemental Materials-Table 1.
Development and approval of clinical questions
This guideline was prepared according to the ESO standard operating procedure (SOP), 46 which is based on the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) framework. 47 The MWG developed a list of topics and corresponding questions of greatest clinical interest. Questions were formatted using the PICO approach (Population, Intervention, Comparator and Outcome), and reviewed by two external reviewers as well as members of the ESO Guideline board and Executive Committee. The outcomes were rated by members of the MWG as: critical, important or of limited importance according to GRADE criteria. Final decision on outcomes used a Delphi approach. Results of the outcomes rating for each PICO question are included in Supplemental Materials-Table 2.
We considered as critical outcomes (defined as ‘critical for making decision’): any stroke (ischaemic or haemorrhagic), major stroke (resulting in moderate to severe disability defined by mRS 3-5) and disability. We identified as important outcomes (defined as ‘important but not critical for making the decision’): TIA, death and cognitive impairment. The term unfavourable clinical outcome (UCO) included all the critical and important outcomes.
Diagnostic criteria
For inclusion in the guidelines, MMD diagnosis should have been performed according to established angiographic diagnostic criteria31,32 including the presence of stenosis or occlusion at the terminal portion of the ICAs or the proximal segment of the ACAs or MCAs and abnormal vascular networks in the arterial territories near the occlusive or stenotic lesions. Patients were considered symptomatic when presenting with TIA, ischaemic or haemorrhagic stroke, headache, movement disorders or cognitive disturbances. Unilateral presentation was considered only in syndromic cases (MMS).
Selection of Population, Intervention, Comparator, and Outcome (PICO)
The MWG formulated nine PICO questions relevant for MMA management, with several sub-questions relating to the six different outcomes described above (if applicable), different subpopulations, as relevant to each PICO and described in the PICO header questions (Supplemental Materials-Table 2). The MWG decided to focus primarily on three types of intervention: imaging assessment, genetic testing and medical and surgical treatment. For PICO5 and PICO6 the adult population was differentiated from the paediatric population as the key factors affecting the benefit-risk balance differ in these two situations. Indeed, the expression of the MMA is mainly ischaemic in children, whereas it is also characterised by cerebral haemorrhage in adults. Revascularization techniques also differ due to anatomical factors related to the size of cerebral vessels and to the potential of neovascularization, which appear to be more efficient in children. For PICO8, a post-hoc change to the wording of the question was agreed to avoid any potential misunderstanding. The initial statement of this PICO was as follows: “In patients with MMA, does respecting the 8-week time interval from an acute cerebrovascular event to revascularization surgery compared to earlier and/or immediate surgery reduce the risk of an unfavourable clinical outcome?” We chose 8 weeks not as a fixed criterion, but as an average duration, to select all studies comparing early/immediate surgery with later time windows. This choice was made early in the process of defining the PICO, when the literature search had not yet been conducted. In practice, to ensure selection of all studies of interest, we did not include ‘8 weeks’ as a criterion for the literature search. The literature search found studies comparing early/immediate surgery with late surgery after a 6- or 12-week delay. This 6- or 12-week delay was close to the average delay of 8 weeks that we originally proposed, which is why we have included these studies in the manuscript. The module working group agreed to change the wording of the PICO as follows: In patients with MMA, does respecting a 6- or 12-week minimum time interval from an acute cerebrovascular event to revascularization surgery compared to earlier and/or immediate surgery reduce the risk of an unfavourable clinical outcome?
Literature search
For each PICO question, search terms were developed, tested, refined, and agreed among the overall MWG and guideline methodologists (SL and SH). Where a validated search strategy was available, it was used or adapted. Where there was a recent relevant systematic review on the question of interest, the corresponding search strategy and results were used and updated as necessary. Search strategies are described in Supplemental Materials-File 1. A systematic review of literature was done to collect evidence to answer each PICO question. This search was performed by the ESO Guideline methodologist. For each PICO question, the following databases were searched: PUBMED, EMBASE and Cochrane Library, from inception of each database to 02/2022. We also searched reference lists of review articles, the authors’ personal reference libraries, and previous guidelines for additional relevant records. The search results were loaded into the web-based Covidence platform (Health Innovation, Melbourne, Australia) for assessment by the MWG. Two or more MWG members were assigned to independently screen the titles and abstracts of publications registered in Covidence and then assess the full text of studies determined to be potentially relevant. All disagreements were resolved by discussion between the two reviewers or by a third MWG member. We prioritised randomised controlled trials (RCTs) but due to the limited data, we also considered health registry data analyses, large observational studies and systematic reviews or meta-analyses of observational studies. Only observational studies with more than 40 subjects for paediatric and more than 30 subjects for adult MMA were selected for evidence-based recommendation. These different thresholds were defined for obtaining a sample with a distribution that approximates what is observed in the general population (Central Limit Theorem) and for reducing, as much is possible, biases from small sample sizes. 48 This threshold was reduced to 20 participants for homogenous samples of MMS, taking into account the very limited data. We considered only studies in humans and where the full article was available in English. Conference abstracts (oral or poster) were excluded.
Data analysis
Data extraction and analysis was performed by the ESO methodologists (SH and SL) independently. DerSimonian and Laird (random-effects) method was used for conducting meta-analyses using Review Manager (RevMan) version 5.4.1 software (Cochrane). 49 We expected a high probability of heterogeneity in terms of population characteristics, intervention types, and settings, so, the random-effect model was chosen over the fixed-effect model. Meta-analyses findings were summarised with a summary effect estimate and associated 95% confidence intervals (CI). Statistical heterogeneity across studies was assessed using the I 2 statistic, and classified as moderate (I 2 ⩾ 30%), substantial (I 2 ⩾ 50%), or considerable (I2 ⩾ 75%). 50 Where appropriate, subgroup analyses were performed based on population (ischaemic or haemorrhagic MMD), and age group (adult or paediatric). The MWG members of each PICO independently evaluated the validity of the results of each meta-analysis.
Evaluation of the quality of evidence and formulation of recommendations
The risk of bias was assessed independently by the methodologists with the Cochrane Collaboration risk of bias tool (RoB 2) for randomised trials and ROBINS-I tool for non-randomised studies.51,52
The results of data analysis were imported into the GRADEpro Guideline Development Tool (McMaster University, 2015; developed by Evidence Prime, Inc.). For each PICO question, and each outcome, the following were considered: risk of bias based on the type of available evidence (randomised or observational studies); considerations on inconsistency of results; indirectness of evidence, imprecision of results, and other possible bias. GRADE evidence profiles/summary of findings tables were generated and used to prepare recommendations. 47 ‘Evidence-based Recommendations’ were based on the GRADE methodology. The direction, strength and formulation of the recommendations were determined according to the GRADE evidence profiles and the ESO-SOP.46,47
Finally, Expert Consensus Statements were added whenever the PICO group considered that there was insufficient evidence available to provide Evidence-Based Recommendations and where practical guidance is needed for routine clinical practice. The Expert Consensus Statements were based on voting by all expert MWG members. The geneticist ETL, due to personal professional experience, was not involved in voting on clinical relevant questions. Importantly, these Expert Consensus Statements should not be regarded as evidence-based recommendations. Expert Consensus Statements are summarised in Supplemental Materials-Table 3.
Drafting of the document, revision and approval
Each PICO question was addressed in distinct sections, in line with the updated ESO SOP. 46 First, ‘Analysis of current evidence’ summarised current pathophysiological considerations followed by a summary and discussion of the results of the identified RCTs and other studies. Second, ‘Additional information’ was added when more details on the studies referred to in the first section were needed to provide information on key subgroup analyses of the included studies, on ongoing or future RCTs, and on other studies which can provide important clinical guidance on the topic. Third, an ‘Expert consensus statement’ paragraph was added whenever the MWG considered that insufficient evidence was available to provide evidence-based recommendations for situations in which practical guidance is needed for everyday clinical practice. The Synoptic Table (Table 1) includes all recommendations and Expert Consensus Statements. The Guideline document was reviewed several times by all MWG members and recommendations and consensus expert statement wording was modified using a Delphi approach until agreement was reached. The final submitted document was peer-reviewed by two external reviewers, two members of the ESO Guideline Board and one member of the Executive Committee.
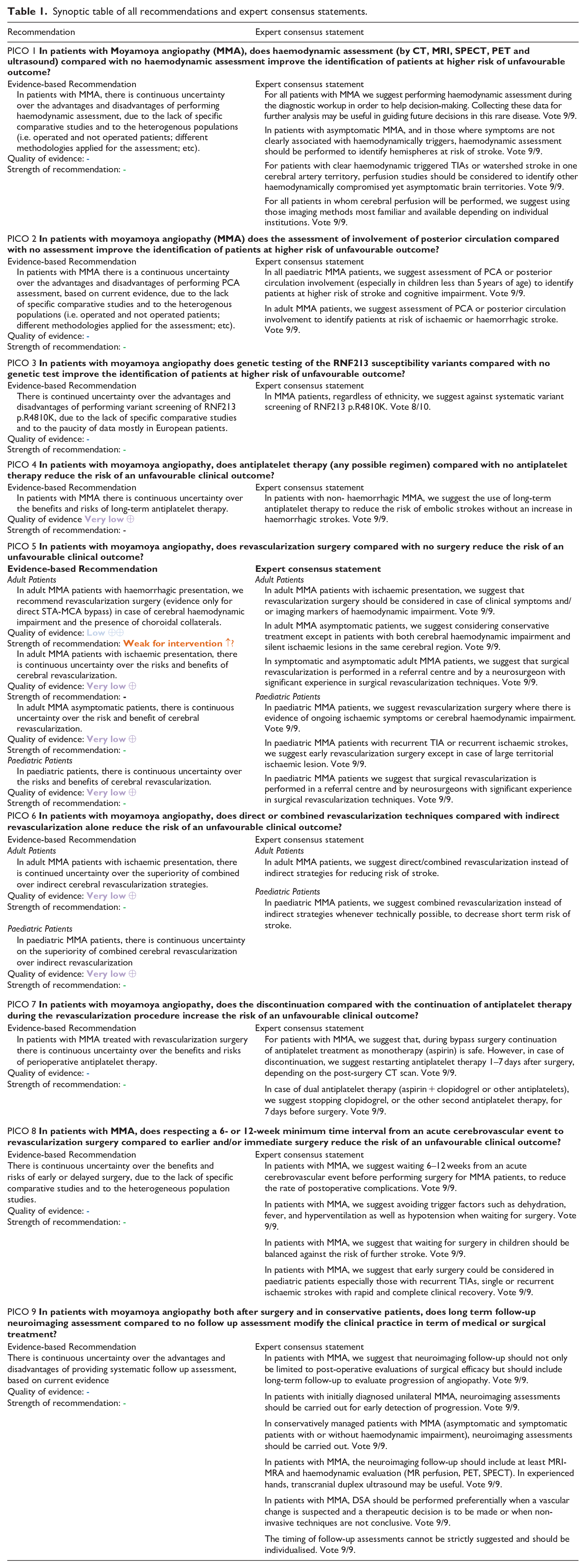
Synoptic table of all recommendations and expert consensus statements.
Results
PICO 1: In patients with MMA, does haemodynamic assessment by (CT, MRI, SPECT, PET and ultrasound) compared with no haemodynamic assessment improve the identification of patients at higher risk of unfavourable outcome?
Analysis of current evidence
The literature search identified no RCT and no comparative studies specifically evaluating the effectiveness of the assessment versus no assessment of haemodynamic status (by CT perfusion, MRI perfusion, PET, SPECT or Doppler sonography) in identifying patients at higher risk of unfavourable clinical outcome (UCO).
Additional information
Scientific data on the natural course of MMA are scarce in East Asians and even more rare in Caucasian populations, especially in Europeans. Previous retrospective studies from the United States and Germany showed a risk of recurrent cerebrovascular event after a first stroke of 80%–82% within 5 years53,54 where this value was only 10.2% over a time frame of 3.7 years in a prospective study of 49 adult patients with more than half having a stroke at baseline. 55 Perfusion studies have been shown to identify MMA patients at risk of haemodynamic stroke in numerous retrospective studies.56–61 Hervé et al. prospectively followed 90 multi-ethnic patients with MMD and MMS conservatively treated, for a period of 42.8 months. 43 In these patients, impairment of CVR assessed by Acetazolamide-99mTc-HMPAO-SPECT, along with East Asian origin and history of TIA, were identified as independent predictors of stroke increasing the annual risk for stroke or silent ischaemic or haemorrhagic lesion from 0.5% to 20%. 43 Other retrospective data suggested the utility of cerebral perfusion imaging to identify patients at risk of stroke, even in the absence of symptom or imaging marker of haemodynamic impairment, such patients presented with headache only or with ischaemic lesions outside the watershed areas.62–65
Regarding asymptomatic MMA, natural history data are available from only few studies and biased by inconsistent definition of ‘asymptomatic’ and short follow up periods. 66 In a small cohort study of 40 East Asian asymptomatic patients, perfusion studies (Xenon CT, SPECT, PET) detected cerebral haemodynamic impairment in 40% of hemispheres but it was not related to disease progression in conservatively treated patients. 67 Another study on East Asian ‘asymptomatic’ subjects (defined as without ischaemic event or cerebral lesion) found a significant association between TIA and decreased CVR (p < 0.001, log-rank test) on 99mTc-HMPAO-SPECT 66 whereas Yang et al. 62 found a significant relationship between initial CVR decrease and disease progression (p = 0.05) in 42 asymptomatic MMD patients followed-up during a mean period of 37.3 months. Disease progression was defined in this study as the occurrence of any neurological symptom or silent lesions on MRI or CVR worsening during the follow-up.
MMA is also responsible for haemorrhagic stroke. In a cohort of 200 Caucasian European patients, 9.5% of the patients had an haemorrhagic presentation. 14 CVR decrease on SPECT was prospectively found to be an independent risk factor (HR 5.37, 95% CI 1.07–27.02) for subsequent haemorrhage in a supplementary analysis of the Japan Adult Moyamoya (JAM) trial. 61 In East Asia, bleeding risk recurrence was also found to be associated with decreased basal perfusion measured by 99mTc-HMPAO-SPECT. 68 However, since haemorrhages in MMA are mostly caused by the fragile collateral system, perfusion studies alone are not always reliable predictors of outcome.69,70
Regarding the impact of haemodynamic impairment on cognition, long-standing hypoperfusion in specific brain regions measured by SPECT was found to be associated with impairment of several cognitive domains (p < 0.01) in 53 Japanese patients. 71 In European Caucasian patients, Roder et al. found a significant correlation between dysexecutive cognitive syndrome and an impairment of CVR detected in H215OPET with ACZ challenge for the right MCA territory. 72 In mainly European Caucasian patients, psychoticism assessed in Symptom Checklist-90-R was significantly more frequent in cases where perfusion deficits on PET imaging were observed in left (0.0124) or right (p = 0.0145) MCA territory. 73
Numerous studies demonstrated improvement of perfusion assessments after bypass surgery for almost all methods of haemodynamic assessment including CT perfusion, Xenon CT, perfusion-weighted imaging (PWI), Acetazolamide-99mTc-HMPAO-SPECT and PET with ACZ challenge, both in East Asian and Caucasian patients.57,58,74–77 Transcranial Doppler sonography with inhalation of hypercapnic normoxic gas to assess vasomotor reactivity is also known to reflect CVR, allowing pre- and postoperative haemodynamic assessment in MMA.54,57,78
Overall, based on current literature, it is not yet possible to identify the best haemodynamic evaluation technique for MMA risk stratification and each available perfusion imaging modality has its strengths and weakness. PET using H215O, 15O2 or C15O2 as tracers, seems to have greatest clinical utility as it allows quantitative assessment and could be used to evaluate oxygen extraction fraction (OEF), cerebral metabolic rate of oxygen (CMRO2) and CVR capacity.79–81 Routine and widespread use of this modality is limited by availability of the hardware, high cost and length of measurement time. SPECT using 99mTc-ECD, 99mTc-HMPAO and 123I-IMP as tracers is also considered as a reference standard technique to assess the regional CBF and the CVR capacity to CO2 or acetazolamide challenge but this perfusion modality was found, in one study, to be less efficient than PET for detection of impaired CVR. 56 The other perfusion imaging modalities used in the management of MMD such as ASL, CT perfusion, PWI, resting-state fMRI, and transcranial doppler ultrasound are more available. Even where they have been compared to SPECT and PET, their predictive value regarding the clinical course of the disease have not yet been prospectively verified.82–85
PICO 2: In patients with MMA does the assessment of involvement of posterior circulation compared with no assessment, improve the identification of patients at higher risk of unfavourable outcome?
Analysis of current evidence
The literature search identified no comparative studies specifically evaluating the benefit of assessment versus no assessment of posterior circulation involvement in MMA patients.
Additional information
Although MMA is more often considered a disease of the anterior circulation, involvement of the posterior circulation, mainly posterior cerebral artery (PCA), has increasingly become a point of interest due to its relevance in terms of cerebral haemodynamic and clinical outcome.
Posterior circulation is an important collateral pathway that helps to compensate and supply blood flow to the anterior circulation in MMA. In this PICO, paediatric and adult MMA were separately addressed to review the published data on assessment of involvement of posterior circulation and the role of this feature either on ischaemic or haemorrhagic stroke outcomes. Six papers on PCA involvement in the paediatric population were found according to the predefined literature search.86–91
In an East Asian cohort of both adult and paediatric MMA patients PCA involvement was found to significantly predict cerebral infarction. 90 PCA involvement especially in the younger age group (<4 years of age) resulted in a high prevalence of ischaemic strokes. 89 Araki et al. 86 in 2021 emphasised age (early onset moyamoya, age <5 years) to be an independent risk factor also for early post-operative stroke. In this age group PCA involvement was a relevant characteristic frequently observed.
In a study of a mainly European paediatric MMA cohort PCA involvement was observed in 35% of cases. 88 Early age at symptom onset (<2 years of age) and PCA involvement was observed to be an important risk factor for a higher overall stroke burden with an unfavourable neurological and clinical outcome tested on the paediatric stroke outcome score and modified Rankin score (mRS). Similarly, PCA involvement has also been shown to be a risk factor for poorer non-verbal IQ and processing speed measured at baseline and pre-operatively with a battery of neurodevelopmental testing. 91 Additionally, long-term social outcome, that is testing for education and occupation history has also been shown to be unfavourable in patients with PCA involvement 10 years after revascularization surgery. 87
Although hemorrhagic stroke is less common in children than in adult MMA patients (3% vs 25%-60% respectively), the involvement of PCA and the development of choroidal anastomosis seem to be the main cause of hemorrhage in these patients. 92
Information about PCA involvement in the adult population was derived from four papers.44,60,93,94 Hishikawa et al. 44 compared long-term outcomes in adult patients with posterior circulation involvement versus those without, after cerebral revascularization. The prevalence of stroke presentation was significantly higher among patients with posterior circulation involvement than in patients without PCA involvement (67% vs 15%, p = 0.006). The mRS score was also significantly higher in these patients both in the preoperative and in the postoperative period. In another long-term (>5 years) follow up of MMA patients (62% adults) after combined direct and indirect surgery, 93 symptomatic disease progression affecting PCA occurred 0.5–15 years after initial surgery (mean 5.4 ± 4.4 years) suggesting late disease progression and hence highlighting the need for longer follow up periods after bypass surgery.
In a retrospective analysis of 574 angiograms, PCA involvement was present in 30% of East Asian adult MMA patients with haemorrhage being the most common presentation. Additionally the risk of posterior circulation infarction was seen to be significantly higher in patients with PCA involvement compared to those without. 94 Noh et al. 60 evaluated 104 adult MMA patients with ischaemic stroke or TIA, followed up for a median 29 months. Revascularization surgery was performed in 45 patients. PCA stenosis (HR = 17.53, 95% CI 2.02–152.43) was identified as predictor of ischaemic stroke recurrence (1.6% in the first year and 11.8% in the fifth year) in non-surgically treated MMA patients, but not in the surgically treated MMA, suggesting a protective role of surgical revascularization.
Moreover, PCA involvement appears to be an independent factor for posterior haemorrhage through development of fragile thalamo-perforator and choroidal collaterals. 95 Additionally posterior haemorrhage is a significant predictor of rebleeding in MMA. 96 Funaki et al. 97 in a supplementary analysis of the JAM Trial on 75 haemorrhagic hemispheres in 75 patients showed PCA involvement in 24 (32%) haemorrhagic hemispheres and found this feature to be associated with posterior haemorrhage in both univariate and multivariate analyses. In addition, the presence of choroidal anastomosis was associated with posterior haemorrhage, with a good topographical correspondence between bleeding points and the anatomical distribution of the choroidal arteries.
In addition to being an important risk variable for stroke and poor clinical outcome at baseline, involvement of PCA is also important while planning revascularization surgery. Park et al. showed PCA involvement to be an independent risk factor for peri- and postoperative stroke (within 15 days of surgery) in adult patients who additionally had preoperative stroke and TIAs. 98 Muraoka et al. showed the same to be true for children. 99
PICO 3: In patients with MMA does genetic testing of the RNF213 susceptibility variants compared with no genetic test improve the identification of patients at higher risk of unfavourable outcome?
Analysis of current evidence
The literature search did not find any study specifically comparing genetic test versus no genetic test for genetic variants of RNF213 gene in order to improve the identification of patients at higher risk of UCO.
Additional information
An association between MMD and a locus at 17q25.3 100 and particularly with a single missense mutation in RNF213 gene (p.R4810K or p.R4859K) has been reported in Japanese patients. 101 This p.R4810K (c.14576G>A) variant was detected in 95.1% of familial MMD cases and 79.2% of sporadic MMD cases, with an OR of 259 (p < 0.001). 101 The exact pathophysiological mechanism by which the RNF213 gene is involved in MMA pathogenesis remains unknown. However, p.R4810K has been found also in about 20% of intracranial major artery stenosis as well as in 0.4%–2% of Japanese controls. 102 Previous authors found that homozygous carriers of this variant had more frequently an early onset, infarction as initial presentation and change with PCA involvement. 101 In another study, these patients had also more frequently a familial history of MMA, an early onset (<5 years), cerebral infarction at diagnosis and cognitive impairment at 1 year follow-up. 103 Although we did not find comparative studies evaluating a possible benefit of genetic testing, available studies did not show any association between RNF213 heterozygous p.R4810K variants and any outcome. Particularly, three papers were evaluated but not considered in the analysis. The first paper from Hara et al. investigated the role of p.R.4810K variant in a retrospective study on 129 Japanese patients with paediatric-onset MMD (onset age ⩽15 years). 104 Homozygous or heterozygous or RNF213 p.R4810K variants were present in almost 80% of patients. The authors did not find any significant association between heterozygous p. R4810K genotype and clinical surgical and non-surgical outcomes, after 1-year follow-up. Patients with homozygosity and heterozygosity for the p.R.4810K variant had more frequent good surgical outcomes as compared to wild type but the difference was not significant (90.9% vs 92.2% vs 76.5%; p = 0.166). Another retrospective cohort study on 94 MMD Japanese patients undergoing direct or combined bypass for revascularization evaluated the relationship between the p.R4810K genotype and outcome after a follow up of 100 months (30–219 months). 105 The p.R4810K (c.14429G>A) variant of RNF213 gene was detected in 69 (73.4%) of the 94 patients with MMD. The homozygous (A/A) and the heterozygous variant (A/G) were identified in 5 and 64 patients respectively. The authors did not observe differences between the genotype regarding baseline features except for a slightly higher frequency of TIA in A/G compared to G/G patients. All patients underwent surgical revascularization. There weren’t significant differences among these genotypes in terms of perioperative and follow up stroke occurrence or in the stroke survival rate and frequency of poor functional condition. Finally, Wang et al., evaluated retrospectively the genotype of 2545 Chinese MMD patients treated with surgical revascularization (median of follow-up duration: 32 months). Of these 627 (24.63%) patients were GA and 10 (0.39%) patients were AA p.R4810K genotype. They did not find, using multivariate Cox analysis, any association between p.R4810K variant and stroke or poor neurologic outcome at the last follow-up visit.
In Western MMA patients the p.R4810K RNF213 variant is absent, 102 but other RNF213 susceptibility variants located in the E3 ligase domain have been associated with MMA. Their penetrance is unknown and there is a lack of evidence regarding the influence of these variants on clinical outcome. However, de novo RNF213 gene mutations located in the E3 ligase have recently been reported in several severe infant onset MA cases.27–29,106 Liver, kidney and skin clinical manifestations are often associated with cerebrovascular manifestations in those infants leading to diagnosis delay and unneeded investigations.
PICO 4: In patients with MMA, does antiplatelet therapy (any possible regimen) compared with no antiplatelet therapy reduce the risk of an unfavourable clinical outcome?
Analysis of current evidence
The literature search identified no RCT specifically analysing the effects of antiplatelet therapy compared with no antiplatelets. However, we found observational studies providing relevant information to this PICO.
Antiplatelets are often prescribed in two scenarios in MMA: in non-operated MMA patients with the aim to reduce ischaemic events, and in surgically treated patients to decrease the potential risk of periprocedural complications as well as ischaemic strokes in the long-term follow-up. However, MMA may also present with cerebral haemorrhage and this is one of the main fears for prescribing antiplatelet drugs, as shown in different surveys among international experts.107–109
Few studies have evaluated the risk of any stroke in patients treated with antiplatelet therapies. No meta-analysis was possible for this outcome due to the heterogeneity in the population data provided (individual cerebral hemispheres were assessed by Pang et al. 110 and patients were assessed by Ye et al. 111 ). The first study found no significant differences in the risk of cerebral infarction (2.3% in the antiplatelet group vs 2.3% in the conservative group) or haemorrhage (5.9% in the antiplatelet groups vs 7.8% in the conservative group) after a mean follow-up of 62 months. 110 On the other hand, Ye et al. 111 reported significantly fewer ischaemic strokes in the group of patients treated with antiplatelets (5.6%) as compared to conservative or surgical treatment (8.4%) after propensity score matching and an average follow-up period of 33 months. 111 Additional cohort studies have addressed the influence of antiplatelet agents on the risk of recurrent stroke. The Registry Study of Research Committee on Moyamoya Disease in Japan found no influence of antiplatelets on the rates of stroke recurrence in a cohort of 344 MMD patients with an initial TIA or cerebral infarction within 10 years prior to enrolment (2.9%/5 years vs 1.6%/5 years). 112 Interestingly, there were significantly more haemorrhagic stroke recurrences in the group of non-antiplatelet therapy (4.2%/5 years vs 0%/5 years). 112 On the other hand, the International Paediatric Stroke Study, in a retrospective analysis of an international multicentre registry which included a total of 174 children >28-days old with MMD (90% of them initially presented with ischaemic strokes), reported 20% of stroke recurrence over a median follow-up of 13 months, without any difference in antiplatelet therapy among those with or without a stroke recurrence. 113
With regard to disability (defined by mRS > 2–5), Ye et al. found no significant differences in the group of patients treated with antiplatelet therapy as compared to conservative/surgical groups (22.6% vs 26.4%) after a mean follow-up of 33 months. 111 The J-ASPECT study, in a propensity-matched analysis from a nationwide registry in Japan, concluded that pre-hospital antiplatelet use was significantly associated with good functional status (defined by mRS 0–1) on hospital admission of non-haemorrhagic MMA patients (OR adjusted for covariates 3.82; 95% CI 1.22-11.99). 114
Finally, only two studies provided data related to the mortality outcomes in MMA patients treated with antiplatelet therapy compared to no antiplatelet therapy.111,115 Ye et al. found a trend of higher frequency of deaths in the group treated with antiplatelets (3.77%) as compared to a group of conservative or surgically treated patients (0.94%) without antiplatelet after a mean follow-up period of 33 months. 111 Seo et al. in a larger and longer study, concluded that antiplatelet therapy was associated with a reduced risk of death in a multivariate model after a total follow-up of 163,347 person-years (HR 0.77; 95% CI 0.70-0,84). 115 However, our meta-analysis (Figure 1), including 2870 MMD patients, found no significant effect of antiplatelet therapy on the risk of mortality with a pooled relative risk of 1.07 (95% CI: 0.22–5.36).111,115 The certainty evaluated by GRADE in this estimate was very low due to concern on the risk of bias, heterogeneity and imprecision in the effect estimate (Table 2; Figure 1 and Supplemental Materials-Table 4).

Meta-analysis (for PICO 4) showing the risk of mortality among antiplatelet users compared to non-users.
GRADE evidence profile for PICO 4, In patients with moyamoya angiopathy, does antiplatelet therapy (any possible regimen) compared with no antiplatelet therapy reduce the risk of an unfavourable clinical outcome?
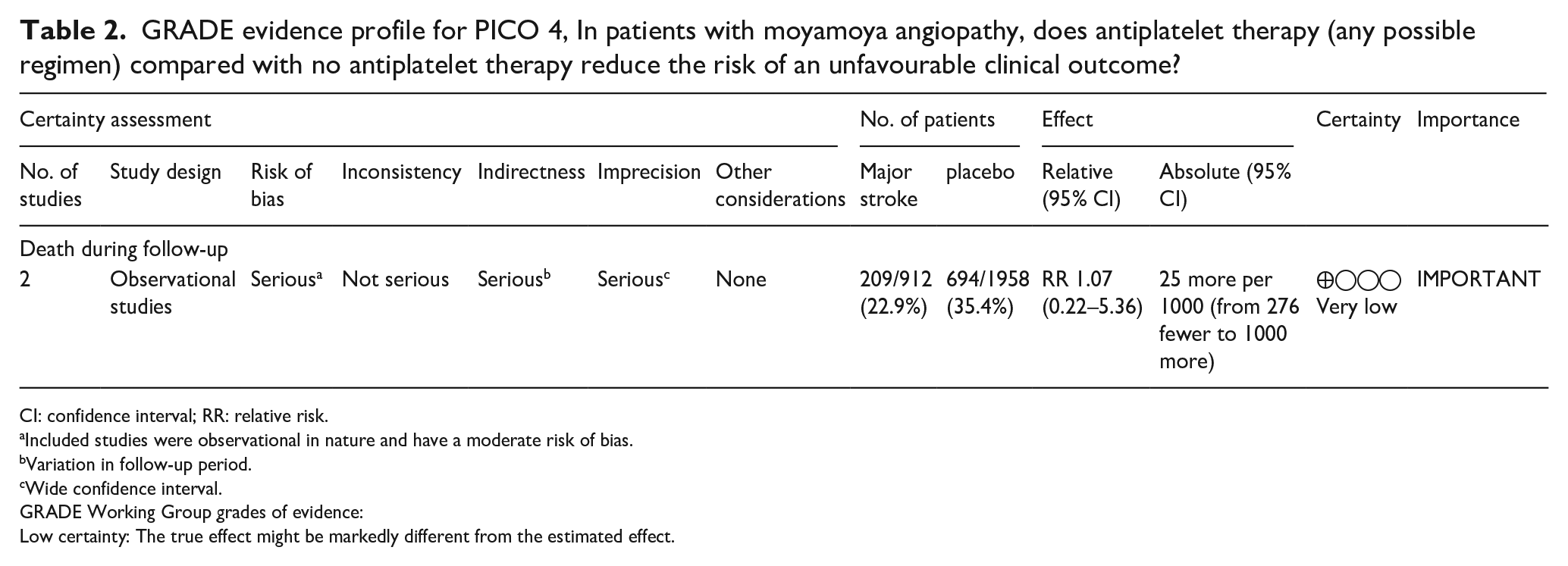
CI: confidence interval; RR: relative risk.
Included studies were observational in nature and have a moderate risk of bias.
Variation in follow-up period.
Wide confidence interval.
GRADE Working Group grades of evidence:
Low certainty: The true effect might be markedly different from the estimated effect.
Additional information
In the therapeutic strategy for MMA three major risks have to be balanced: haemodynamic ischaemic events, risk of bleeding due to fragile moyamoya vessels and embolic stroke. Regarding the latter, there are some studies describing the finding of microembolic signals (MES) or high intensity transient signals (HITS) using transcranial Doppler in patients with MMA,116–118 which could represent embolic risk. 119 One retrospective study in a small population of MMA observed a reduction of MES after antiplatelet administration or regimen change. 120 Direct embolism has been even also visualised during surgery in a MMA patient. 121 Evaluating the type of antiplatelet drugs, the most commonly used agents in the studies included in this analysis were aspirin, clopidogrel or cilostazol as monotherapy, with only a minority of patients receiving dual antiplatelet therapy.93,110,115 Since the literature search for this PICO question was focused on the comparison between antiplatelet versus no antiplatelet therapy, we did not retrieve any randomised clinical trial with a comparative efficacy focus. Some of the observational studies provided subgroup analysis stratified by the antiplatelet drug used, with some studies reporting no differences in outcomes related to the drug potency 110 whilst others suggested a greater reduction in mortality with cilostazol than with other antiplatelet drugs. 115
Only one of the studies included in this analysis specifically analysed the effect of antiplatelet therapy in a cohort of 5308 MMD patients initially presenting with cerebral haemorrhage, 4008 of them were treated with antiplatelet drugs. 115 Interestingly, the Cox regression analysis showed a reduced odds of long-term mortality in the cohort of patient with prior haemorrhagic stroke with the use of aspirin (0.49; 95% CI 0.32–0.75), cilostazol (0.40; 95% CI 0.30–0.53) or clopidogrel (0.57; 95% CI 0.46–0.71) as compared to no antiplatelet therapy. 115
PICO5: In patients with MMA, does revascularization surgery compared with no surgery reduce the risk of an unfavourable clinical outcome?
Adult patients
Analysis of current evidence
We identified one completed RCT, the JAM trial, addressing PICO 5 which compared direct revascularization with best medical treatment in adult MMD with haemorrhagic presentation. 122 It was a multicentre, randomised control, open label study (Table 3, GRADE profile and Table 4, risk of bias assessment). Adult patients functionally independent, aged between 16 and 65 years and with a history of intracerebral, intraventricular or subarachnoid haemorrhage that occurred within 12 months before inclusion were eligible. Patients with diastolic blood pressure >110 mm Hg or treated with extracranial-intracranial bypass surgery before enrolment were excluded. The JAM trial included 80 patients and randomly allocated participants to either conservative medical care or extracranial-intracranial direct bypass on both sides (each side to be performed within 3 months of inclusion). The intention-to-treat population comprised 42 patients in the surgical group and 38 patients in the conservative group. There was one protocol violation in the surgical group with one patient receiving direct bypass on one side and indirect bypass on the other side. To increase the number of events and power, the primary outcome was a composite endpoint defined by recurrent bleeding, completed stroke causing significant morbidity, mortality or significant morbidity from other medical causes or requirement for extracranial-intracranial bypass for a nonsurgical patient. The primary composite endpoint occurred in 6 (14.3%) patients in the surgical group and 13 (34.2%) patients in the nonsurgical group during a mean follow-up period of 4.32 years (HR: 0.39 [95% CI, 0.15–1.03], p = 0.057). The log-rank test revealed that the surgical group was at significantly lower risk than the nonsurgical group for the primary endpoint (3.2%/y vs 8.2%/y; p = 0.048). These differences in results could be related to the small sample size included in the study. The sample size initially calculated (n = 160) was based on the assumption that the incidence of adverse neurological events would be 8%/y in the non-surgical group and 4%/y in the surgical group (to detect a difference between the two groups with a significance level of 0.05). Due to the lower number of eligible patients than expected, the sample size was finally set at 80 (based on an event rate in the surgical group <2.8%). Perioperative complications were observed in eight patients (9.5%) and included hyperperfusion syndrome, TIA, seizure, scalp bedsore and tear of subcutaneous drainage tube. All but one of these complications were transient. This low rate of perioperative complications, including mainly transient events, may be related in part to the experience in extracranial-intracranial bypass in MMD of all centres participating in the trial and suggest the importance of sufficient training in the field.
GRADE evidence profile for PICO 5, In adult patients with moyamoya angiopathy, does revascularization surgery compared with no surgery reduce the risk of an unfavourable clinical outcome?
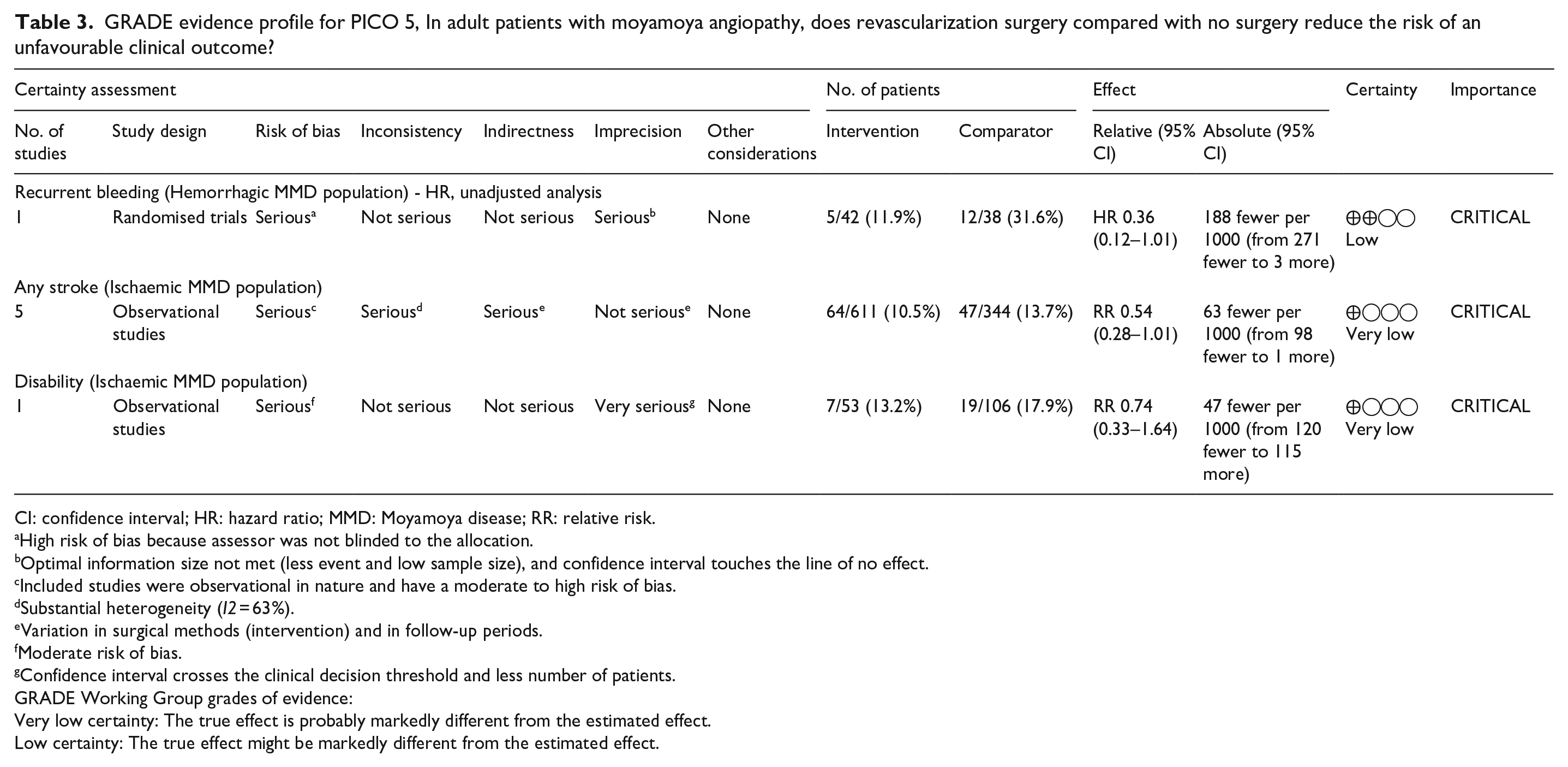
CI: confidence interval; HR: hazard ratio; MMD: Moyamoya disease; RR: relative risk.
High risk of bias because assessor was not blinded to the allocation.
Optimal information size not met (less event and low sample size), and confidence interval touches the line of no effect.
Included studies were observational in nature and have a moderate to high risk of bias.
Substantial heterogeneity (I2 = 63%).
Variation in surgical methods (intervention) and in follow-up periods.
Moderate risk of bias.
Confidence interval crosses the clinical decision threshold and less number of patients.
GRADE Working Group grades of evidence:
Very low certainty: The true effect is probably markedly different from the estimated effect.
Low certainty: The true effect might be markedly different from the estimated effect.
Risk of bias of randomised controlled trial for PICO 5.
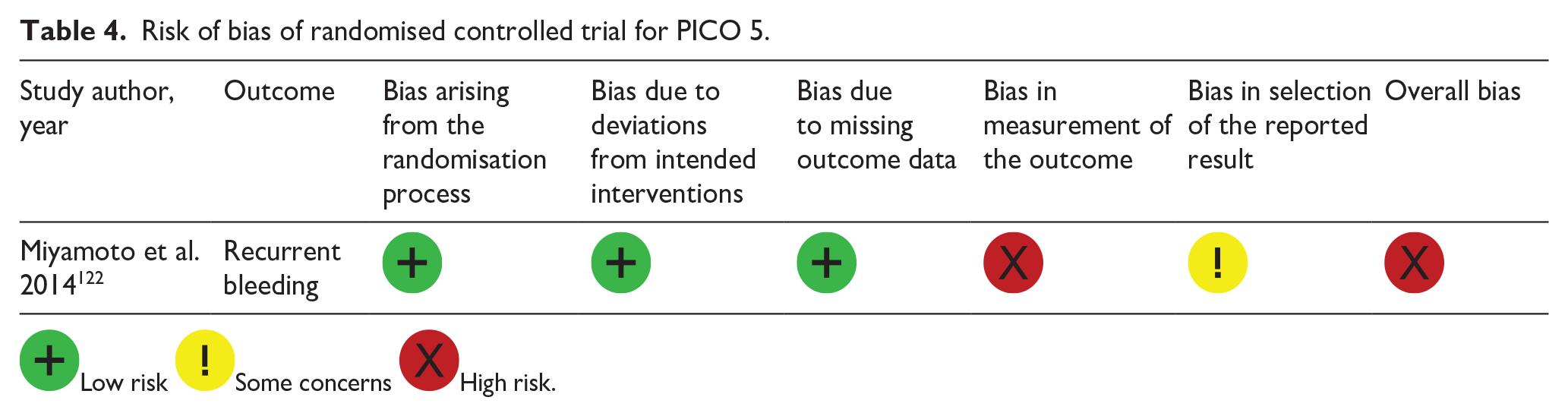
 Low risk
Low risk  Some concerns
Some concerns  High risk.
High risk.
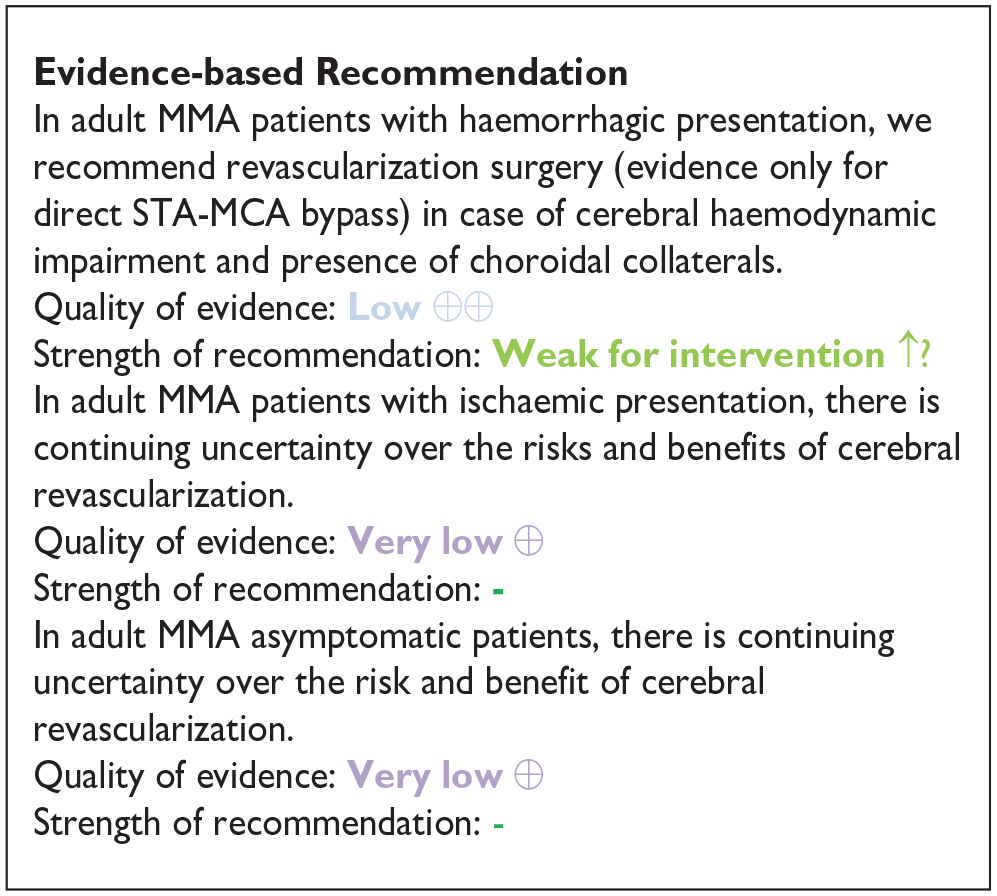
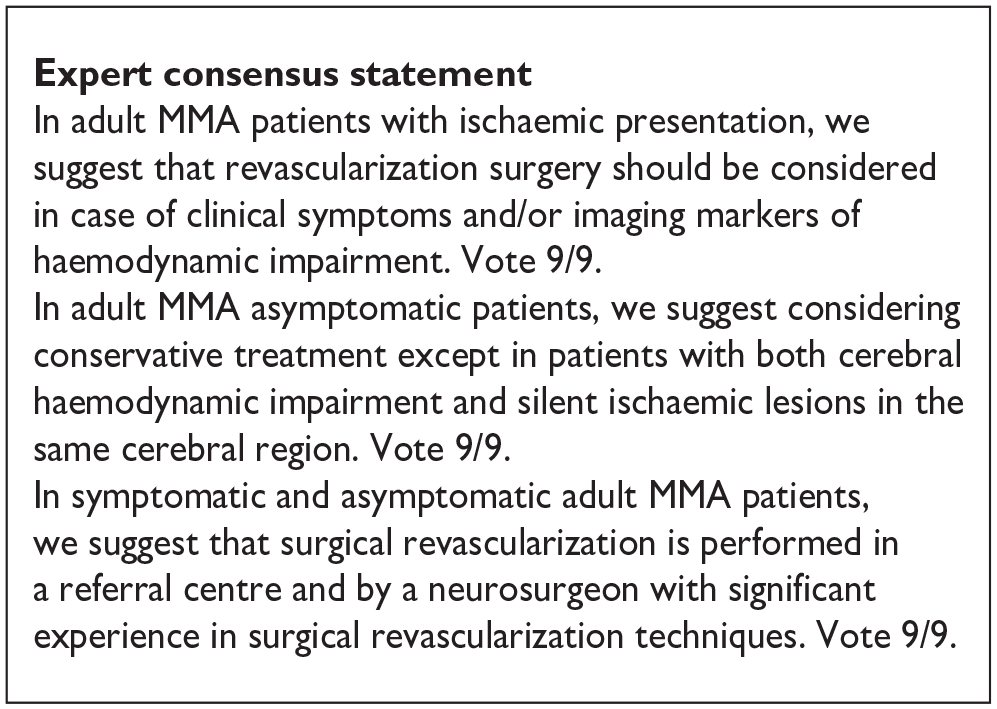
In patients with ischaemic presentation, our systematic review identified no randomised data on the efficacy and safety of revascularization surgery. Only five comparative observational studies, with usable data for meta-analysis in this subgroup of patients, were found.60,111,123–125 A reduction in any stroke was found in MMD adult patients with ischaemic onset who underwent revascularization surgery compared to conservative treatment with a pooled relative risk of 0.54 (95% CI: 0.28–1.01), p = 0.06) (Figure 2). However, it is important to consider that most of these studies were retrospective, conducted at a single centre, and lacked matched control groups. The indication for surgery was at the discretion of each surgeon and based on variable clinical or imaging parameters, explaining why demographic and clinical characteristics differed in all studies between surgical and conservative groups. In addition, revascularization procedure and conservative treatment as well as follow-up were not standardised. These facts underline the level of evidence to be considered when interpreting the data (Table 3, GRADE profile, Supplemental Materials-Table 5).
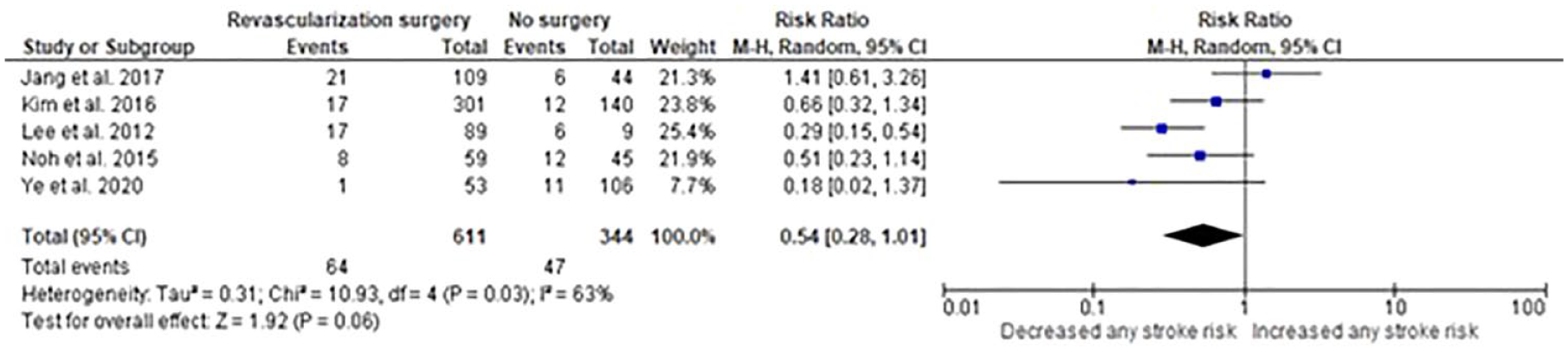
Meta-analysis (for PICO 5) showing the risk of any stroke in adult MMD patients with ischaemic presentation who underwent revascularization surgery compared to standard of care.
Regarding MMD patients without history of TIA or stroke, our systematic review of the literature identified only one observational comparative study with a distinct dataset for adults. Among 40 patients, 36 patients were conservatively treated, and 4 patients underwent indirect surgical revascularization. During a median follow-up of 32 months, no patient had a stroke and 3 conservatively treated patients had a TIA which was associated with decreased CVR on SPECT imaging. 66 Natural history, clinical and imaging predictors of worsening and potential benefit of surgical revascularization remain to be clarified in asymptomatic patients with MMD. The ongoing Japanese AMORE registry might clarify the long-term prognosis of this subgroup of patients 126
Additional information
Few predictive studies have been conducted prospectively on non-operated patients to identify subgroups of patients at higher risk of cerebrovascular complications to help decision making for surgical revascularization. Regarding patients with haemorrhagic presentation, an ancillary prospective cohort study of the JAM trial using 5-year follow-up data on 37 patients included in the non-surgical arm has suggested that choroidal anastomosis could be an independent predictor of rebleeding in haemorrhagic MMD 127 In this study, the incidence of rebleeding was significantly higher in the choroidal anastomosis-positive group (13.1% /year) than in the negative group (0.3%/year, p = 0.008). Moreover, in the positive group, the haematoma was located in the choroidal artery territory in 7 of 10 patients suggesting a causal association between the presence of choroidal anastomosis and the occurrence of rebleeding. Another supplementary analysis in the same cohort, used SPECT imaging before (resting state) and after ACZ challenge to evaluate the impact of cortical haemodynamic failure on rebleeding. 61 Multivariate analyses were adjusted for several potential confounders including the presence of choroidal collaterals. Among 72 non-surgical hemispheres, 34 (47.2%) had no haemodynamic impairment and 38 (52.8) had a CVR decrease associated or not with a decrease of baseline blood flow. The presence of haemodynamic failure was found to be an independent predictor of rebleeding (HR 5.37, 95% CI 1.07–27.02). Patients with cerebral haemodynamic impairment may not only be at greater risk of rebleeding but also be those for whom surgery is more effective. Indeed, in the same study, whereas the occurrence of rebleeding was significantly reduced in the presence of CVR decrease in the surgical arm compared with the conservative arm (HR 0.15, 95% CI 0.04–0.57), there was no significant difference between the two arms in the absence of cerebral haemodynamic impairment (HR1.56, 95% CI 0.22–11.10). Regarding patients with ischaemic presentation, cerebral haemodynamic impairment seems also to be one of the major predictors of poor prognosis. A first prospective study failed to establish a significant association between the occurrence of stroke during follow-up and cerebral regional oxygen extraction fraction which presumably increases at the cerebral tissue level when autoregulation is exceeded. 55 However, the limited number of patients included in these studies, low event rate and large number of censored cases due to the decision to pursue revascularization surgery might explain these negative results. A recent predictive study used a global approach wherein several parameters were tested as potential predictors of clinical or cerebral tissue changes in 90 adult patients with MMD or MMS, including more than 60% of ischaemic presentation. 43 In this cohort, the detection of regional alterations in CVR (HR: 4.4, 95% CI 1.2–16.1), a history of TIAs (HR: 4.18, 95% CI 1.37–12.75) and East Asian origin (HR: 2.63, CI 1–6.94) were independently associated with an increased risk of stroke or incidence of ischaemic or haemorrhagic lesions on MRI. The predictive value of cerebral haemodynamic status in ischaemic MMD is reinforced by the low risk of stroke occurrence observed in a prospective cohort of ischaemic MMD adult patients without misery cerebral perfusion on PET imaging.128,129 The incidence of further ischaemic events was only 6% per 5 years of follow-up in this population of patients having no cerebral area with abnormally elevated oxygen extraction fraction (OEF).
Less data is available on the predictors of surgical complications. A grading system has been proposed to stratify the individual risk of perioperative complications in adult MMD. 130 This scale is based on the following three imaging key parameters: 1/ the degree of steno-occlusive lesions and the development of intracranial and extracranial collaterals on conventional angiography (1–3 points), 2/ the absence or presence of ischaemic or haemorrhagic lesion on MRI (0 or 1 point) and 3/ the CVR capacity (>−5% = 0 point, <−5% = 2 points). MMD, grade I referred to 1–2 points, grade II to 3–4 points and grade III to 5–6 points. This grading system was first evaluated in 37 MMD patients treated by a bilateral and one-staged revascularization approach. 74 The differentiation of MMD according this grading system was correlated with the occurrence of post-operative cerebral ischaemic events (grade I: 0%, grade II: 9%, grade III: 16%, p < 0.05). The predictive value of this grading system has been replicated in an independent Japanese dataset of 89 adult patients treated by unilateral combined revascularization strategy. 131 Perioperative ischaemic and haemorrhagic complications occurred in 14.6% of operated hemispheres and the grading was related to their occurrence (p < 0.001).
Paediatric patients
Analysis of current evidence
Our systematic review identified no RCT and only one observational study on children with MMA, comparing surgical treatment to conservative treatment for the outcomes selected in these guidelines. In this retrospective multicentre study, 282 paediatric patients were retrospectively analysed. 132 Among them, 214 patients underwent surgical revascularization (direct bypass, combined bypass or indirect bypass) and 68 were treated conservatively. During a mean follow-up period of 41 (9–145) months, a significant reduction in any stroke was found in MMD paediatric patients who underwent revascularization surgery (2.8%) compared to conservative treatment (13.2%) with a relative risk of 0.21 (95% CI: 0.08–0.57) (Table 5, GRADE profile, Supplemental Materials-Table 5). In addition, at the end of the follow-up period, a significant reduction in disability was found in patients who underwent revascularization surgery (2.8%) compared to conservative treatment (20.6%), with a relative risk of 0.14 (95% CI: 0.05–0.34).
GRADE evidence profile for PICO 5, In paediatric patients with moyamoya angiopathy, does revascularization surgery compared with no surgery reduce the risk of an unfavourable clinical outcome?
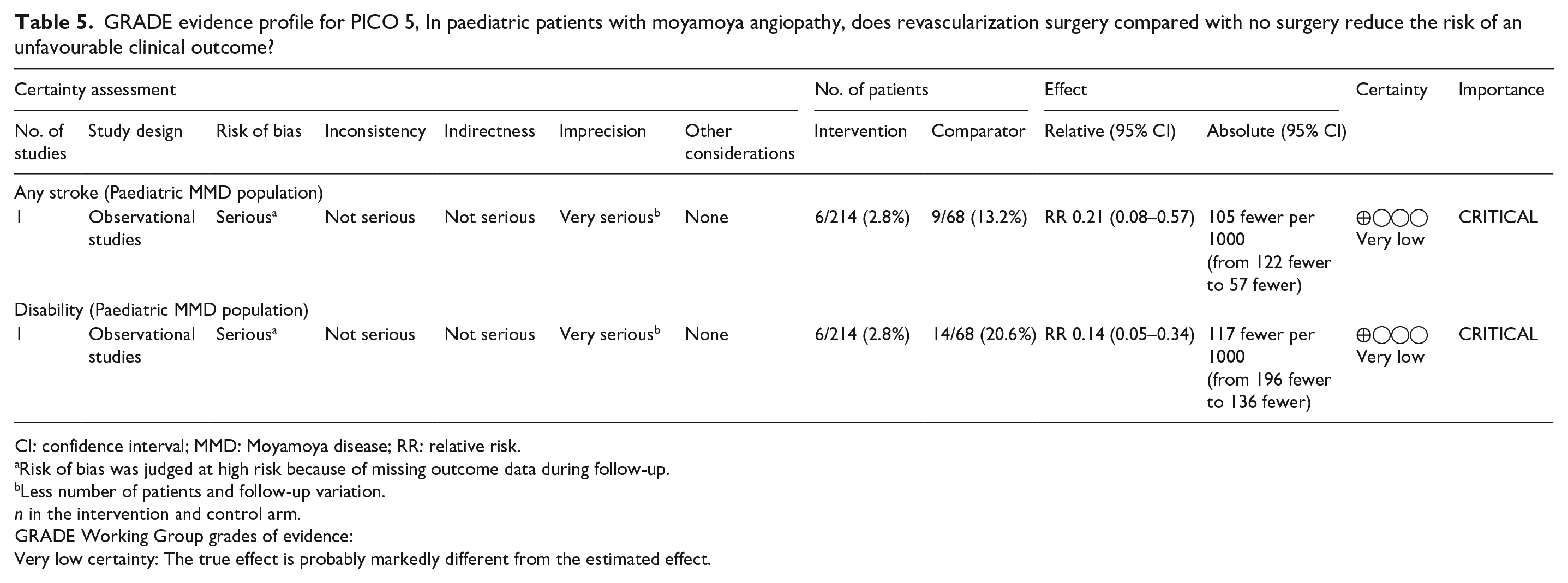
CI: confidence interval; MMD: Moyamoya disease; RR: relative risk.
Risk of bias was judged at high risk because of missing outcome data during follow-up.
Less number of patients and follow-up variation.
n in the intervention and control arm.
GRADE Working Group grades of evidence:
Very low certainty: The true effect is probably markedly different from the estimated effect.
Additional information
One historical comparative study of children with MMD compared outcomes in terms of activities of daily living (ADL) (1–5 grades) of a total of 88 MMA patients (48 paediatric) with and without surgery at a follow-up period of 6–86.4 months. In the 33 patients with surgery, ADL improved in 61% versus only 26% in the non-surgical group. This improvement was more prominent in the paediatric group. 133 These results reflect the particularly severe natural course of the disease in children compared with adults resulting in an increased burden of stroke and long-term disability. Recent single centre studies with 100 and 73 paediatric MMA patients respectively and a multicentre study of 63 MMA patients, all of mainly European ethnicity, confirmed the high risk of progression with recurrent strokes in MMA children and more so in the younger age groups as well as in those showing PCA involvement.88,134,135 In an older publication with East Asian paediatric MMD patients, Kim et al. reiterated this aggressive clinical course. 136 In a recent follow-up study of 415 paediatric MMD patients, the same authors showed a favourable clinical outcome in 81% of the patients about 3 years after revascularization surgery. Good results of surgical revascularization in paediatric MMA on short- and long-term prognosis has been shown in several other studies to date.137,138
PICO6 In patients with MMA, does direct or combined revascularization techniques compared with indirect revascularization alone reduce the risk of an unfavourable clinical outcome?
In surgical practice, three different revascularization strategies are applied: indirect, direct, and combined revascularization. For MMD patients, indirect and combined are the most frequently applied strategies. Currently, there is still no consensus about the best type of revascularization surgery. To answer this question, we first analysed the overall data on indirect versus direct revascularization strategies. In a second step, we differentiated the adult population from the paediatric population as the key factor affecting the benefit-risk balance, that is the efficacy of indirect revascularization, differs in these two situations. Children may be characterised by a higher plasticity and angiogenic activity of their cerebrovascular system. In contrast, in adults the cerebrovascular system displays a reduced angiogenic activity as a function of age. Thus, indirect techniques may result in better vessel growth rates in the paediatric population, providing better results than in adults. Of note, in our analysis, we did not differentiate among the different indirect techniques described in the literature.
Adult patients
Analysis of current evidence
Our analysis identified no RCT and 7 observational study on adults with MMA, comparing combined with indirect revascularization strategies for the outcomes selected in these guidelines. Of seven studies, five studies125,139–142 reported any stroke and three studies125,143,144 assessed disability as outcome parameter.
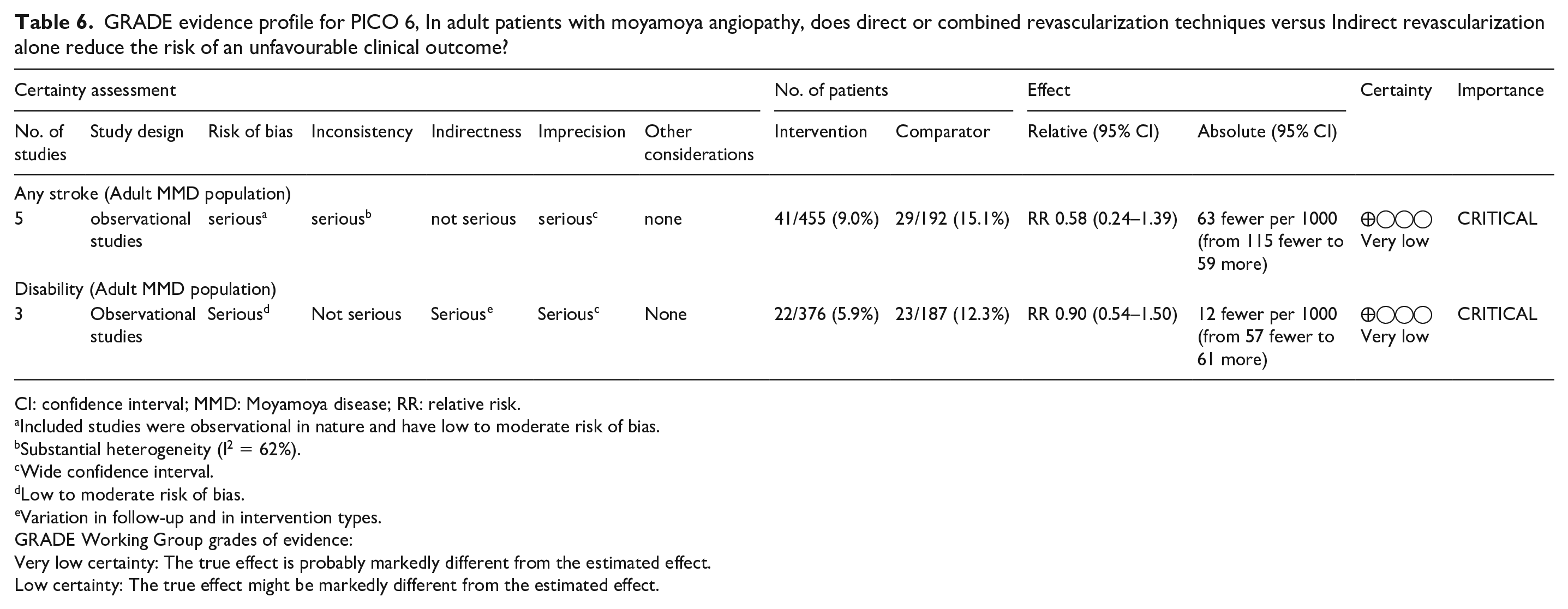
Bang et al., 139 reported 65 patients with MMA undergoing either indirect or combined revascularization. The authors used combined STA-MCA bypass with a variety of indirect techniques encephalo-myo-synangiosis (EMS), encephalo-duro-arterio-synangiosis (EDAS), encephalo-duro-arterio-myo-synangiosis (EDAMS). The mean age was 35.0 ± 12.4 years (range: 16–65 years), thus, only including adult patients. Mean follow-up time was 63.8 ± 29.7 months (range: 18–139 months). This study supported a trend for superiority of the combined technique over the indirect technique in preventing any form of stroke (2% vs 14%, RR 0.11 [95% CI: 0.01-1.18]). A smaller patient cohort was reported by Choi et al. 140 Here, 17 patients were revascularized by combined means, while 18 patients received an indirect bypass. Again, only adult patients were studied with a mean age of 43.6 ± 8.5 years. Mean follow-up was 54.4 ± 23.8 months. The stroke incidence for the combined revascularization group was 12%, while 22% suffered stroke following indirect bypass alone (RR 0.53 [95% CI: 0.11-2.53]). The largest study was published recently by Gao et al. 141 Here, 281 patients underwent combined/direct revascularization strategies and 90 patients received an indirect bypass. Only adult patients were reported with a mean age of 39.0 ± 11.1 years. The mean follow-up time accounted to 41.5 ± 23.0 months, with a wide range of 6.1–83.4 months. This study demonstrated superiority of the combined/direct approach over indirect revascularization strategies with an OR of 0.49 (stroke events in 7% and 14%, respectively, during the observation period). The fourth study 142 is characterised by a heterogenous patient cohort and included patients with typical MMD as well as patients with atypical unilateral MMA and MMS. The study focussed on adult patients with a mean age of 39.2 ± 12.2 years. Patients were observed for a mean of 2.7 years. The sample size of the two groups was small, with 29 patients receiving a combined intervention and 13 patients an indirect bypass. Despite this heterogeneity this study supported a trend for superiority of combined techniques over indirect techniques for stroke prevention (7% vs 23%; RR 0.30 [95% CI: 0.06-1.58]). In contrast to these four studies favouring combined techniques over indirect technique, the fifth study 125 revealed better results with indirect techniques. Here, a total of 124 patients were reported, 67 receiving a combined revascularization strategy and 57 being treated with an indirect revascularization strategy. Similar to the other studies, only adult patients were included (mean age 43.1 ± 10 years) and the mean observation time was comparable with 55 ± 19.2 months. The combined bypass group comprised a standard STA-MCA bypass and encephalo-duro-galeo (periosteal)-synangiosis (EDAGS), using inverted STA-galeal flap and STA-galeal pedicle, the latter being a somewhat unusual indirect strategy. In the indirect group, different strategies were applied, including EDAS, EMS, and EDAGS, making the indirect strategy for both groups hard to compare. The incidence of stroke in the combined bypass group was 24% and in the indirect group only 12% (RR 1.94 [0.86-4.39]). Our meta-analysis of these five studies (Figure 3) revealed a non-significant reduction in the risk of developing any stroke in MMD patients who underwent direct or combined revascularization surgery compared to indirect revascularization surgery [RR 0.58 (95% CI: 0.24–1.39)]. The certainty evaluated by GRADE in this estimate was very low due to concern on the risk of bias, substantial heterogeneity and limited precision in the effect estimate (Table 6, GRADE profile, Figure 3, Supplemental Materials-Table 6).

Meta-analysis (for PICO 6) showing the risk of any stroke in adult MMD patients who underwent direct or combined revascularization surgery compared to indirect revascularization surgery.
GRADE evidence profile for PICO 6, In adult patients with moyamoya angiopathy, does direct or combined revascularization techniques versus Indirect revascularization alone reduce the risk of an unfavourable clinical outcome?
CI: confidence interval; MMD: Moyamoya disease; RR: relative risk.
Included studies were observational in nature and have low to moderate risk of bias.
Substantial heterogeneity (I 2 = 62%).
Wide confidence interval.
Low to moderate risk of bias.
Variation in follow-up and in intervention types.
GRADE Working Group grades of evidence:
Very low certainty: The true effect is probably markedly different from the estimated effect.
Low certainty: The true effect might be markedly different from the estimated effect.
The three studies focussing on disability as primary outcome (mRS > 2–5) failed to reveal a clear superiority of any of the bypass strategies. This is most likely because an unfavourable, peri- or postoperative course leading to disability is fortunately a very rare event. Gao et al. 141 had also studied the disability for their 371 patients. Accordingly, out of the 281 patients undergoing combined revascularization only 1% and out of the 90 patients undergoing indirect revascularization only 2% had a disabling outcome. The study by Kim et al. 143 focused only on outcome as measured by the mRS. Fifty-one patients were treated with a combined and 45 patients with an indirect bypass. All patients were adults with a mean age of 38 years (range: 18–68). The follow-up period only covered the perioperative period up to 6 weeks following surgery, rather reflecting the risk and complications of the bypass strategies. During this early postoperative time, 10% of the combined group and 7% of the indirect group were categorised as disabled (RR 1.47 [0.37-5.81]). However, these data have to be interpreted carefully due to the short follow-up period and the bias that some patients were already disabled prior to surgery as a consequence of their strokes. Lai et al. 144 in contrast, followed up their patients at least 6 months, which is still relatively short. They included a total of 96 patients, 44 treated by combined and 52 treated by indirect revascularization strategies. Patients were all adults with a mean age of 42 ± 11 years (range: 18–69). In this study, the disability rate was comparable, but surprisingly high among the groups, with 30% and 35% for combined and indirect techniques, respectively (RR 0.85 ([0.47-1.54]). Analysing these three studies together was hampered by the large heterogeneity of follow-up periods and frequencies for patients presenting with disability. The meta-analysis findings (Figure 4) revealed a non-significant association between direct or combined revascularization surgery versus indirect revascularization surgery in reducing the disability risk in patients with MMD (p = 0.68). The certainty evaluated by GRADE was low due to low to moderate risk of bias, heterogeneity and imprecision in the summary estimate (Table 6, GRADE profile, Supplemental Materials-Table 6).

Meta-analysis (for PICO 6) showing disability risk in adult MMD patients who underwent direct or combined revascularization surgery compared to indirect revascularization surgery.
Additional information
Indirect revascularization relies on neovascularization of the cortical surface via angiogenic mechanisms from pedicle-based grafts. The variability of techniques and tissues used as vascularised grafts is huge. Several variations of indirect revascularization have been developed: EMS, encephalo-arterio-synangiosis (EAS), encephalo-myo-arterio-synangiosis (EMAS), encephalo-duro-synangiosis (EDS), EDAS, EDAMS, EDAGS, as well as various combinations of these. The variety of indirect techniques is large, and it remains unknown which, if any, of these techniques is superior to the others. In general, indirect techniques are easier to perform since they do not include a direct anastomosis. Moreover, cerebral revascularization, along with the haemodynamic protection of the brain, may take months to develop.
All studies agree that the perioperative complication rates do not differ between direct/combined versus indirect revascularization techniques: Kim et al.143,145 confirm that procedures that include a direct intervention are not more risky with respect to stroke, irreversible/transient ischaemic neurological deficit, haemorrhage, skin necrosis, and infection. Deng et al. 146 comparing direct versus indirect revascularization among adults, also did not detect any significant increase in perioperative complications by direct revascularization techniques. Furthermore, another meta-analysis that focused on perioperative complications in adults demonstrated that despite a higher incidence of haemorrhagic complications in the direct bypass group, direct and combined revascularization techniques were superior in providing long-term favourable outcome. 147 Here, the beneficial effects of combined revascularization techniques (via the direct bypass component) outweighed the higher complication rate.
Paediatric patients
Analysis of current evidence
Our systematic review identified no RCT and only two observational studies on children with MMA, comparing combined revascularization and indirect revascularization strategies for the outcomes selected in these guidelines. Ishikawa et al. 38 analysed their series of 64 paediatric patients with a mean age of 7.6 ± 3.6. A large proportion of patients was thus below 5 years of age. In 48 patients, the authors succeeded to realise an STA-MCA anastomosis in combination with an EDAGS. In 16, they failed to do so and ended up with an indirect revascularization strategy only, using EDAGS again. The incidence of stroke during the observation period of 6.6 ± 3.8 years was remarkably low for both groups, that is 0% in both groups, which is markedly lower than observed for adults. Similarly, Sadashiva et al. 148 reported their series of 108 paediatric MMA patients undergoing combined (58 patients) or indirect (50 patients) revascularization strategies. Noteworthy, their patient cohort was older with a mean age of 13.8 years. During the mean follow-up period of 15.9 months (3–62 months), again only a limited number of patients experienced stroke after revascularization. Following combined revascularization, the stroke incidence was 5% and following indirect revascularization, only 2%. Taken together, these results suggest that the superiority of combined revascularization strategies over indirect techniques is not obvious in the paediatric population.
Additional information
A high level of plasticity and angiogenic potential of the brain tissue and vasculature are required for the success of indirect revascularization techniques. The cerebrovascular plasticity in patients with MMD seems to be age dependent, with indirect revascularization procedures showing a higher success rate in children compared with adults.130,149 On the other hand, direct revascularization strategies carry relevant advantages over indirect techniques. 145 Thus, they provide an immediate increase of cerebral blood flow and improvement of CVR capacity while indirect techniques depend on an ingrowth of collateral blood vessel into the brain pial surface and provide a delayed increase of cerebral blood flow and improvement of CVR capacity only. Even in children, this delay may last up to 3–6 months leaving especially haemodynamically unstable children unprotected for several weeks or months and exposing them to an increased short-term risk for stroke. In addition, the surgical approach for a direct revascularization strategy is less invasive since indirect techniques depend on a large exposure of the brain surface for covering the cortex with the pedicle graft.
PICO 7: In patients with MMA, does discontinuation compared with continuation of antiplatelet therapy during the revascularization procedure increase the risk of an unfavourable clinical outcome?
Analysis of current evidence
The literature search did not identify any RCT or prospective comparative studies specifically analysing the effects of continuation versus no continuation of antiplatelet therapy during the revascularization procedure.
Additional information
It has been reported that MMA patients are more prone to develop acute thrombogenesis at the anastomotic site just after extracranial-to-intracranial bypass surgery, as compared to similar neurosurgical procedures in non-MMA patients. 150 Symptomatic or asymptomatic cerebral infarction may occur in up to 14% of MMA patients treated with indirect revascularization surgery, half of them within the first day after surgery. 151 Despite these findings, the role of antiplatelets in the perioperative period and whether withholding or continuing them before surgery remained to be elucidated.107,109
In a large retrospective analysis of the factors associated with perioperative complications, Schubert et al. reported that preoperative single antiplatelet therapy was not associated with increased haemorrhagic complications, and that postoperative single antiplatelet treatment was associated with improved outcomes (defined as the absence of any new neurologic deficit) at the time of discharge. 152 However, the authors did not specifically analyse the outcomes of patients who discontinued antiplatelets at the time of surgery. Kanamori et al. evaluated a total of 74 surgical procedures who either received or did not receive aspirin, 52 of them in patients previously treated with aspirin. 153 They found a significantly lower rate of white thrombus at the anastomosis site and a higher initial bypass patency in patients treated with aspirin, without differences in the rate of ischaemic or haemorrhagic complications. However, the authors did not report separately the outcomes of the 20 cases who continued with aspirin, the 26 who stopped aspirin 3 days before and the 6 who stopped aspirin just on the operation day. 153
Two retrospective studies have specifically addressed the effects and safety of aspirin administered postoperatively but results regarding the effect of aspirin on bypass patency were conflicting. Zhao et al. reported no significant differences in bypass patency (95.5% vs 96.1%) after an unadjusted analysis in patients postoperatively treated with aspirin (59 hemispheres) versus no aspirin (138 hemispheres). 154 Lu et al. reported in a retrospective study on 217 patients with ischaemic-onset MMA undergoing STA-MCA bypass that the continuation of aspirin within the first month after surgery was associated with a higher bypass patency rate (98.7% vs 89.7%; HR 1.57; 95% CI 1.106–2.235; p = 0.012). 155 None of these two studies found significant differences in the incidence of ischaemic or haemorrhagic events between aspirin users and non-users. However, other factors potentially influencing thrombus formation and bypass patency such as duration of neurosurgical procedure were not analysed systematically.
In patients who discontinue antiplatelet therapy 7 days before the revascularization surgery, there is uncertainty about the timing for restarting it, with both early (day 1–3) or late (day 4–7) timing possibilities described. 156 In a retrospective study, Kraemer et al. analysed the safety of early (day 1–3) or late (day 4–7) restarts of antiplatelet therapy showing no difference in the incidence of subdural haematoma. 156 Bypass patency was 100% at day 4 as well as after 3 months despite paused antiplatelet therapy in the majority of the cohort. 156 However, small silent ischaemic lesions were found on MRI at 6 days post-surgical follow-up in 10.9% of patients, 86% of whom were older than 40 years old.
For Japanese experts, discontinuation of antiplatelets after bypass surgery ‘for a certain period’ of time is a common behaviour 108 reflecting different opinions between East Asian and non-Asian experts as it was emphasised by a worldwide survey of experts on the use of antiplatelet therapy in MMA. 107
PICO8: In patients with MMA, does respecting a 6- or 12-week minimum time interval from an acute cerebrovascular event to revascularization surgery compared to earlier and/or immediate surgery reduce the risk of an unfavourable clinical outcome?
Analysis of current evidence
The literature search did not find any RCT or prospective comparative study specifically analysing the effects of respecting a 6- or 12-week minimum time interval (from an acute cerebrovascular event to revascularization surgery) in comparison to early surgery.
Additional information
Timing of surgical revascularization after the last cerebrovascular event remains controversial in MMA patients. Although early surgery may be ideally beneficial in ischaemic MMA, patients operated early after a stroke might suffer from a higher rate of post-operative complications, related to: (1) hyperperfusion syndrome with or without intracranial haemorrhage,157–160 (2) the risk of haemorrhagic transformation related to acute ischaemic stroke, (3) a more significant haemodynamic instability at risk of further ischaemic events in the early post-operative period, 161 (4) higher risk of systemic complications, particularly in the setting of significant neurological deficits after a stroke. 162 In addition, there is a lack of consensus regarding the definition of what can be considered ‘early’ or ‘late’ and the required delay between the time of the last cerebrovascular event and the time of surgery.
Our systematic review identified only two publications considering a time interval of 90 days and 6 weeks respectively.163,164 The first of these is a retrospective case control study that evaluated 57 MMA patients undergoing standard superficial temporal artery-to-middle cerebral artery (STA-MCA) bypass combined with EDAMS. 163 Patients were classified among two groups, whether the surgery was performed early (<90 days, n = 28) or late (⩾90 days, n = 29). Initial ischaemic manifestations were significantly more frequent in the early group compared to the late group (43% vs 17%; p = 0.035), while haemorrhagic presentation was more frequent in the late group (62% vs 36%; p = 0.047). Despite the low number of cases, the authors concluded that their data supported later revascularization strategy, as there was a significant higher rate of post-operative complication in the early group compared to the late group (39.3% vs 13.8%, p = 0.029). However, patients in the late group were at non-significantly higher risk of experiencing a second stroke or a clinical deterioration compared to the early group (31% vs 11%, p = 0.06). The results of this study were not adjusted for type of presentation (haemorrhagic or ischaemic) and age. In the latter study, Kim et al. performed a retrospective analysis of 170 indirect revascularization procedures in 90 children with ischaemic MMD and investigated several potential risk factors for ischaemic complications during the 2 weeks following surgery. 164 A delay of less than 6 weeks between the last ischaemic event and surgery was found to be associated with post-operative ischaemic complications. However, this association was no longer seen in multivariate analysis.
PICO 9: In patients with MMA, both after surgery and with conservative management, does long-term follow-up neuroimaging assessment compared to no follow up assessment modify the clinical practice in term of medical or surgical treatment?
Analysis of current evidence
The literature search identified no RCT or prospective comparative studies specifically examining whether long-term follow-up with neuroimaging assessment modifies medical or surgical treatment.
Additional information
Our systematic review identified several studies which have followed up MMA patients either with unilateral angiopathy,165–167 asymptomatic initial presentation, 67 or ischaemic initial presentation without cerebral misery perfusion. 168 Patients undergoing cerebral revascularization are usually followed for evaluation of surgical efficacy, yet few long-term studies were also available for review.93,169
Regarding patients with unilateral disease, while information on the incidence of progression of unilateral MMD varies in literature to date, Park et al. in 2011 showed a 59% rate of bilateral progression (on MRI-MRA or angiography) in an East Asian paediatric MMD cohort (n = 40/259) where a younger age (age <8 years, FU:14.18 months and age >8, FU: 22.38 months) at first diagnosis demonstrated a faster rate of progression. 167 In Smith and Scott, mainly Caucasian cohort, 30% of unilateral paediatric MMA patients also showed angiographic progression over an average time of 2.2 years. 170 In a cohort of mainly adult Caucasians, 165 angiographic progression from unilateral to bilateral disease was seen in 38.9% of patients at a mean follow-up of 12.7 months, 71% of these patients had adult onset MMA with 57% of patients thereafter undergoing surgical intervention. In another study of adult and mainly East Asian operated and non-operated MMD patients, the incidence of disease progression was 20% over a mean follow-up time of 73.6 months. 171 This progression was seen in both uni- and bilateral MMD and also in the anterior and posterior circulation. In more than 50% of these patients the progression of disease was related to a clinical event, that is ischaemic or haemorrhagic stroke. In summary, these observational, single arm studies have shown that neuroimaging assessments of patients with unilateral angiopathy is essential for early detection of progression and treatment thereof. While this is more frequent and rapid in the paediatric population, it is also observed in the adult patients. Female sex and presence of angiographic changes on the contralateral side seem to be predictive indicators of progression. MRI-MRA were almost always performed, and progression was then confirmed on angiography.
A multicentre, nation-wide Japanese prospective survey followed-up asymptomatic MMA patients (age range 13–59 years) over an average time of 44 months and found cerebrovascular episodes including TIAs in 21% of patients and an annual risk of ischaemic or haemorrhagic stroke of 3.2%. The angiographical stage of disease was also more advanced with age. Onset of ischaemic symptoms and deterioration of CVR also related to angiographic disease progression. 67 Similar findings were observed in a prospectively analysed cohort of East Asian MMA patients where the incidence of angiographic disease progression was 12% for 5 years in medically treated adult MMD patients with initial ischaemic symptoms but without cortical ischaemic lesion on MRI nor cerebral misery perfusion. 168 Patients with further ischaemic events always exhibited angiographic disease progression. Cerebral perfusion was reduced in patients with angiographic disease progression even when further ischaemic events did not occur. Since, in these studies, onset of symptoms with deterioration in cerebral haemodynamic has been shown to be related to angiographic progression over time, even in initially asymptomatic patients and patients with ischaemic symptoms but without hypoperfusion, follow-up assessment in these subsets of patients also seems to be warranted.
Regarding the course of the disease after revascularization surgery, 93 patients (paediatric and adults) were followed up in a prospective study to 10.5 ± 4.4 years after combined revascularization surgery for the MCA territory. 93 While late morbidity, that is haemorrhage was seen only in one adult patient 9.5 years after surgery (0.10% per patient-year), progression of angiopathy in the contralateral carotid or the PCA occurred on MRA in 1.5% per patient-year within an interval of 0.5–15 years from first surgery. The authors concluded that longer follow-ups, that is 10 years post-surgery are essential to detect disease progression and prevent late cerebrovascular events. 93
The question of ‘progression’ of MMA is an important one, whether this is observed on MRA or conventional angiography or on haemodynamic testing, whether in symptomatic and medically treated or asymptomatic patients, whether in initial unilateral presentation or even surgically treated patients. The MWG agreed about the therapeutic consequence related to the assessment of disease progression. Most of the papers reviewed were not comparative studies (i.e. those specifically referring to follow-up assessment vs no assessment groups), but they do present important observations and highlight the value of serial testing leading to clinically relevant therapeutic decision making. In addition to MRA, non-invasive transcranial duplex ultrasound can be used to follow up bypass patency and progression of vasculopathy in experienced hands.75,172,173
Discussion
Although the incidence of MMA is increasing worldwide, 3 data on disease natural history are poor and fragmented, especially in European countries. The incomplete knowledge on the natural course of MMA, as well as the unknown pathophysiology and the heterogeneity of the disease, especially between East Asians and Western populations, has limited, so far, the development of shared management strategies.9,10,19,35–37 Surgical revascularization is considered the only treatment able to prevent ischaemic and haemorrhagic strokes.38,40 However, indication on the best type of revascularization and the timing of surgery as well as on patient management in the presurgical and follow-up phases are lacking.
This article is the first comprehensive European guideline on the management of MMA using GRADE methods.47,174 The aims of our WG was to conduct a methodologically rigorous and extensive analysis of the available evidence and data and to provide evidence based recommendations, or when not possible, Expert Consensus Statements which may be helpful for clinical decision in diagnostic work up, management and care of MMA worldwide. Recommendations and Expert Consensus Statement are based on the work of a group with broad expertise on MMA and on PICO questions, spanning disciplines (neurology with clinical and research areas, neurosurgery, genetic and methodologists) and several European countries (Italy, France, Germany, Spain, Switzerland). This last point was specifically important for this guideline since most of guidelines are provided by Japanese groups. 41
The literature search performed to answer our PICO questions, found a marked paucity of high-quality papers and most of our data were derived from observational studies since no specific RCTs were available, except the JAM trial, comparing bilateral direct revascularization to the best medical treatment in adult MMD with haemorrhagic presentation. 169 Therefore, in adult MMA patients with haemorrhagic presentation we recommended (PICO5), with ‘low quality’ of evidence, direct-bypass surgery, after assessing the haemodynamic and choroidal collateral status. The recommendation was ‘weak for intervention’ since it was supported by only one small sized RCT. Data from five comparative observational studies (Figure 2 and Table 3)60,93,123–125 led experts to suggest with very low grade of evidence, revascularization surgery in adults and children with ischaemic MMA, when supported by the presence of clinical symptoms or imaging markers of haemodynamic failure, if performed in referral centres with neurosurgical expertise. The quality of evidence was very low since most studies were retrospective, conducted at a single centre level, suffering from bias in control population selection and variable indication to surgery.
Regarding the type of surgery, different revascularization strategies are being applied in current practice (indirect, direct, and combined revascularization). Although direct and combined are the most frequently used techniques, especially in adults, the best type of revascularization surgery is still unknown. For this question (PICO6), no RCT was available, and data were provided by seven observational studies with a relatively long follow-up (up to 84 months and 64 months respectively). The results of these studies supported the Expert Consensus statement that direct/combined is preferable to indirect cerebral revascularization strategies in adult MMA patients and in children, to reduce the risk of stroke. However, these findings could be influenced by the different indirect techniques applied in the included studies (i.e. EMS, EAS, EMAS, EDS, EDAS, EDAMS, EDAGS) which were not individually differentiated or specifically evaluated. This could be of particular importance since the indirect technique is easier and particularly relevant to children due to their high vessel plasticity and angiogenic activity. Therefore, further larger studies, especially RCTs may be useful to assess whether one of these techniques, direct or indirect could be recommended as well as how to deal asymptomatic patients.
Our expert group also stated that it might be reasonable to wait 6–12 weeks (PICO8) from an acute cerebrovascular event before performing surgery, although data were available from only two retrospective comparative observational studies with a relatively small sample size. Patients operated on in the early period after acute events might suffer from a higher rate of post-operative complications such as cerebral hyperperfusion syndrome with or without haemorrhage, early haemorrhagic transformation of an acute ischaemic stroke or peri- or postoperative ischaemic events.157–161
Results from studies on large series,110,111,115 and registries112,114 were also not conclusive on the benefits and risk of long-term antiplatelet therapy in non-haemorrhagic MMA (PICO7). Therefore, for these patients we could develop only an Expert Consensus statement suggesting the safe long-term use of antiplatelets in these patients, although Asian physicians do not routinely use antiplatelet in MMA. 107 Conversely, we did not have enough data to formulate statements on haemorrhagic MMA patients. Given the lack of data, we can also not provide any recommendation or expert consensus statement on bridging with heparins during discontinuation of antiplatelet. Moreover, since the analyses were based on data from Japanese studies, environmental or specific susceptibility factors (i.e. resistance to antiplatelet) could limit the translation of these findings in Western countries. Due to the lack of specific comparative studies and to the heterogeneity of the study populations (i.e. operated and not operated patients; different methodologies applied for assessment; etc) we could not provide a recommendation but only an Expert Consensus statement on the advantages of haemodynamic studies and PCA assessment to identify the risk of stroke (PICO1 and 2). However, we have to take into account that it could be difficult to implement RCTs on this topic, due to ethical problems and common clinical practice.
We had also no evidence to support the clinical utility of performing the genetic screening of p.R.4810K include’ variant of RNF213 gene’ (PICO3), despite the fact that it could be useful to look for other variants in the RNF213 gene in children with a very early onset and severe disease.27–29,112 Since it has been observed that MMA steno-occlusive lesions progress over the years conditioning ischaemic and haemorrhagic clinical events and that unilateral MMA may evolve to bilateral conditions, the MWG agreed in suggesting the neuroimaging assessment of disease progression (MRI, MRA, cerebral perfusion imaging and DSA), based on the potential need for a therapeutic decision (PICO9). However, also in this case most of the papers reviewed were not comparative studies (i.e. those specifically referring to follow-up assessment vs no assessment groups), and the analysis was limited by the different imaging approaches used as well as by the dyshomogeneous time periods studied.75,172,173 Therefore, given the relevance for therapeutic decision, the implementation of specific studies addressing this question should be encouraged.
The limitations of our work is mostly related to the lack of RCTs and by the observational and retrospective nature of most of the studies evaluated, allowing us to provide mostly Expert Consensus rather than recommendations. Moreover, the small sample sizes of most studies further reduce the certainty of our findings. For some PICOs there was significant heterogeneity between included populations, outcomes as well as duration of follow-up or methodologies applied. Another important limitation may be the fact that we did not specifically separate East Asian patients from American and European series for the analysis. We are aware that it is possible that patients with MMA in East Asia and Europe have different characteristics and need to be managed differently. However, we do not have enough data, mainly in European MMA patients, to support the idea that MMA could be considered as a different entity in Europe. Also, more specific analyses focusing on different perfusion imaging techniques, different surgical or antiplatelet strategies were not performed and could be useful, but this is beyond the scope of the present study.
In conclusion, the diagnostic work up as well as the clinical and surgical management of MMA continues to evolve. Although there are still several unmet needs and lack of evidence, we believe that our work, by providing detailed information on the available findings on this field can be useful in guiding clinicians in choosing the most effective treatment and management strategy for MMA. Moreover, by identifying research gaps and unresolved questions regarding MMA diagnosis and therapy, these guidelines may also contribute to the implementation of further research such as RCTs or rigorously conducted observational studies.
Plain language summary
Moyamoya disease (MMD) is a rare disorder of the vessels that carry blood to the brain. The blood vessel at the base of the skull become narrowed over time, resulting in an inadequate supply of blood, and therefore oxygen, to the brain.
The disease affects all populations but is much more common in East Asia. Moyamoya disease mainly affects children but can also occur in adults. The problems associated with MMD vary greatly from one person to another. In both children and adults, the disease usually manifests as strokes. Strokes occur when an area of the brain is suddenly cut off from blood flow (called an ischaemic stroke) or when a blood vessel bursts and blood spills into the brain (called haemorrhagic stroke). Children with moyamoya may also suffer from severe headaches, dizziness and learning difficulties.
When the first symptoms appear, a brain magnetic resonance imaging (MRI) scan is often performed. This painless examination gives precise images of the brain and can show signs of brain damage (haemorrhage or infarction). However, the examination that confirms the diagnosis of moyamoya is cerebral angiography. This is a radiological examination, which assesses blood vessels with X-rays, after injection an X-ray dye. This allows a better visualisation of the blood vessels than MRI.
The exact cause of MMD is unknown. Our limited understanding of the disease is one of the reasons we have no tablets that can prevent or reverse moyamoya blood vessel changes. Surgery is used to limit damage from moyamoya. However, brain surgery comes with a risk of complications. The decision to perform surgery is difficult and is made in concert with the patient, the family and the medical team. Decisions on the suitability for surgery usually depend on the patient’s age, condition of the blood vessels and symptoms.
In our guideline, having assessed all the evidence, we recommend surgical intervention in patients with moyamoya who have bleeding type strokes. We also suggest that any surgery is performed in highly specialised centres. Surgery should be delayed after a stroke to avoid complications. We support that specialised brain scans are used to assess whether the moyamoya blood vessel changes are worsening over time. Finally, we suggest that blood thinning medications (antiplatelets) be used for some people on a long-term basis and during the perioperative period.
Supplemental Material
sj-docx-1-eso-10.1177_23969873221144089 – Supplemental material for European Stroke Organisation (ESO) Guidelines on Moyamoya angiopathy: Endorsed by Vascular European Reference Network (VASCERN)
Supplemental material, sj-docx-1-eso-10.1177_23969873221144089 for European Stroke Organisation (ESO) Guidelines on Moyamoya angiopathy: Endorsed by Vascular European Reference Network (VASCERN) by Anna Bersano, Nadia Khan, Blanca Fuentes, Francesco Acerbi, Isabella Canavero, Elisabeth Tournier-Lasserve, Peter Vajcoczy, Maria Luisa Zedde, Salman Hussain, Sabrina Lémeret, Markus Kraemer and Dominique Herve in European Stroke Journal
Supplemental Material
sj-docx-2-eso-10.1177_23969873221144089 – Supplemental material for European Stroke Organisation (ESO) Guidelines on Moyamoya angiopathy: Endorsed by Vascular European Reference Network (VASCERN)
Supplemental material, sj-docx-2-eso-10.1177_23969873221144089 for European Stroke Organisation (ESO) Guidelines on Moyamoya angiopathy: Endorsed by Vascular European Reference Network (VASCERN) by Anna Bersano, Nadia Khan, Blanca Fuentes, Francesco Acerbi, Isabella Canavero, Elisabeth Tournier-Lasserve, Peter Vajcoczy, Maria Luisa Zedde, Salman Hussain, Sabrina Lémeret, Markus Kraemer and Dominique Herve in European Stroke Journal
Supplemental Material
sj-docx-3-eso-10.1177_23969873221144089 – Supplemental material for European Stroke Organisation (ESO) Guidelines on Moyamoya angiopathy: Endorsed by Vascular European Reference Network (VASCERN)
Supplemental material, sj-docx-3-eso-10.1177_23969873221144089 for European Stroke Organisation (ESO) Guidelines on Moyamoya angiopathy: Endorsed by Vascular European Reference Network (VASCERN) by Anna Bersano, Nadia Khan, Blanca Fuentes, Francesco Acerbi, Isabella Canavero, Elisabeth Tournier-Lasserve, Peter Vajcoczy, Maria Luisa Zedde, Salman Hussain, Sabrina Lémeret, Markus Kraemer and Dominique Herve in European Stroke Journal
Supplemental Material
sj-docx-4-eso-10.1177_23969873221144089 – Supplemental material for European Stroke Organisation (ESO) Guidelines on Moyamoya angiopathy: Endorsed by Vascular European Reference Network (VASCERN)
Supplemental material, sj-docx-4-eso-10.1177_23969873221144089 for European Stroke Organisation (ESO) Guidelines on Moyamoya angiopathy: Endorsed by Vascular European Reference Network (VASCERN) by Anna Bersano, Nadia Khan, Blanca Fuentes, Francesco Acerbi, Isabella Canavero, Elisabeth Tournier-Lasserve, Peter Vajcoczy, Maria Luisa Zedde, Salman Hussain, Sabrina Lémeret, Markus Kraemer and Dominique Herve in European Stroke Journal
Supplemental Material
sj-docx-5-eso-10.1177_23969873221144089 – Supplemental material for European Stroke Organisation (ESO) Guidelines on Moyamoya angiopathy: Endorsed by Vascular European Reference Network (VASCERN)
Supplemental material, sj-docx-5-eso-10.1177_23969873221144089 for European Stroke Organisation (ESO) Guidelines on Moyamoya angiopathy: Endorsed by Vascular European Reference Network (VASCERN) by Anna Bersano, Nadia Khan, Blanca Fuentes, Francesco Acerbi, Isabella Canavero, Elisabeth Tournier-Lasserve, Peter Vajcoczy, Maria Luisa Zedde, Salman Hussain, Sabrina Lémeret, Markus Kraemer and Dominique Herve in European Stroke Journal
Supplemental Material
sj-docx-6-eso-10.1177_23969873221144089 – Supplemental material for European Stroke Organisation (ESO) Guidelines on Moyamoya angiopathy: Endorsed by Vascular European Reference Network (VASCERN)
Supplemental material, sj-docx-6-eso-10.1177_23969873221144089 for European Stroke Organisation (ESO) Guidelines on Moyamoya angiopathy: Endorsed by Vascular European Reference Network (VASCERN) by Anna Bersano, Nadia Khan, Blanca Fuentes, Francesco Acerbi, Isabella Canavero, Elisabeth Tournier-Lasserve, Peter Vajcoczy, Maria Luisa Zedde, Salman Hussain, Sabrina Lémeret, Markus Kraemer and Dominique Herve in European Stroke Journal
Footnotes
Acknowledgements
We would like to acknowledge Guillaume Turc and Terry Quinn (the chair and co-chair of the ESO guidelines board) for reviewing the final text. We would also like to acknowledge Yvonne Brüchert and Sabrina Lémeret for providing administrative support. We are particularly grateful to Vijeya Ganesan who contributed to the PICOs drafting and literature search. We finally thank Dena Zera, who contributed to draft PICOs and search term definition
Correction (March 2023)
Article updated online to correct “0.13-1.01” to “0.15-1.03” on page 66, line 38, PICO 5.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the development of these guidelines was provided by the European Stroke Organisation, Basel, Switzerland. The author(s) did not receive financial support for the development, writing and/or publication of this guideline
Ethical Approval
Ethical approval was not necessary for the work described in this paper.
Informed consent
Not applicable.
Guarantor
AB and DH as MWG chairs are the guarantor of the guidelines
Contributorship
AB and DH drafted the PICO questions, which were refined by all authors (AB,DH, NK, BF, FA, IC, ETL, PV, MLZ, MK, SL). SL and SH conducted the literature search, conducted data extraction and performed meta-analyses. AB, DH coordinated the whole MWG activities, drafted and revised the manuscript. All authors (AB, DH, NK, BF, FA, IC, ETL, PV, MLZ, MK, SL, SH) participated in the writing of the first draft of the manuscript. All authors reviewed and edited the manuscript for important intellectual content and approved the final version of the manuscript
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.