
Abstract
Introduction
Systemic contraceptives increase the risk of ischemic stroke but little is known about the characteristics, mechanisms and long-term outcome post stroke of patients on hormonal contraception. We sought to To assess characteristics and outcome of acute ischemic stroke (AIS) in young women using systemic hormonal contraceptives (SHC) and compare them to strokes in non-contraceptive users.
Patients and methods
Using the Acute STroke Registry and Analysis of Lausanne (ASTRAL), we analyzed demographics, risk factors, clinical, radiological and treatment data of consecutive female patients of <50 years between 2003 to 2015. We compared groups with and without SHC in a logistic regression analysis.
Results
Of the 179 female patients of <50 years during the observation period, 57 (39.6%) used SHC, 71.9% of whom, a combined oral contraceptive pill. On logistic regression contraceptive users were significantly younger but had comparable stroke severity. They had less migraine with aura and tobacco use, and more hyperlipidaemia. Also, contraceptive users had significantly less intra and extracranial stenosis and occlusion on arterial imaging, but more focal hypoperfusion on CT-perfusion. Undetermined mechanism of stroke was more frequent with SHC users, whereas rare mechanisms were more frequent in non-users. The contraceptive user group had a more favourable adjusted 12-month outcome with significantly fewer ischemic recurrences after stopping systemic contraception in all.
Conclusion
Contraceptive users with ischemic strokes are younger and have lesser tobacco use and migraine with aura and more hyperlipidemia. Their stroke mechanism is more often undetermined using a standardised work-up, and their adjusted long-term outcome is more favourable with less stroke recurrence.
Keywords
Background
Stroke in young women is rare with an estimated incidence of 6–20 per 1,00,000 women below age 35. 1 Oral contraceptive pills are a reliable and easy means of contraception, with around 151 million users worldwide, but female sterilization is still the most prevalent method. 2
It is well established that contraceptives increase the risk of venous thromboembolism. 3 In addition, oral contraceptives increase the risk for ischemic stroke and subarachnoid haemorrhage.4,5 A Cochrane review showed that systemic hormonal contraceptive users had a 1.6 times higher relative risk for ischemic stroke and myocardial infarction, and more so with higher doses of oestrogen. 6 These observations are not only relevant for preventing a first stroke in young women, but also to make informed decisions regarding contraception after a first ischemic event.
The mechanisms by which SHC increase the risk of stroke may be related to prothrombotic and proinflammatory effects. 7 On the other hand, research in animals showed that oestrogen reduces the extent of stroke, making it a candidate for neuroprotection after stroke in humans.7–9 In addition, there is some evidence that progesterone may be a neuroprotective agent after traumatic brain injury. 10
There is scarce information on the clinical and risk factor profile of woman having acute ischemic stroke (AIS) while taking SHC. 11 Therefore, we aimed to describe the risk factor profile, demographic and clinical characteristics, stroke mechanism, and long-term course of young women on SHC having AIS in a consecutive series of AISs and compare them to young women not taking SHC.
Subjects and methods
We retrospectively analysed all consecutive female patients aged 18 – 50 years on SHC (oral, injectable, transdermal patch and intrauterine contraceptive implants) at the time of their stroke from the Acute STroke Registry and Analysis of Lausanne (ASTRAL) between 01/2003 and 12/2015. As the control group, we selected all female patients in the same age category who were not using SHC.
The ASTRAL registry includes all patients admitted to the stroke unit and/or intensive care unit of the Lausanne University Hospital with a main discharge diagnosis of AIS, including recurrent AIS. 12 In summary, we collected the following parameters in a prespecified manner and then analysed them: demographics (age, gender), medical history and cardiovascular risk factors (hypertension, diabetes mellitus, dyslipidaemia, smoking, atrial fibrillation, documented coronary artery disease, mechanical or biological valves, low ejection fraction <35%, symptomatic peripheral artery disease, oncological disease, migraine with and without aura, alcohol abuse), current medications (antiplatelets, anticoagulants, antihypertensives, lipid-lowering drugs, insulin and oral antidiabetics). We also registered vascular territory, the National Institutes of Health Stroke Severity scale (NIHSS) and time from stroke onset to hospital arrival.
We compiled comorbidities according to Charlson and Elixhauser indexes,13,14 vital signs (skin temperature, blood pressure, heart rate) and metabolic and haematological parameters (glucose, creatinine, total cholesterol, white blood cells, haematocrit, platelet count) on admission (usually in the emergency room).
Acute brain imaging on admission was mostly CT-based and included CT angiography (CTA) and CT-perfusion whenever possible. We obtained at least one arterial study of cervical and cerebral arteries within 24 hours of stroke onset, mainly CTA with multidetector-array technology in helicoidal mode. We considered stenosis of ≥50% and occlusion as significant and recorded it for all arterial segments as published in detail elsewhere.15,16 We classified this arterial pathology as being intracranial or extracranial, and inside or outside the ischemic territory.
We designated stroke pathophysiology according to TOAST, 17 with dissections, PFO-related stroke (in the presence of a RoPE score ≥7, 18 embolic strokes of undetermined origin (ESUS), 19 and multiple causes recorded as additional mechanisms.
We performed general stroke management and secondary prevention according to hospital criteria at the time of admission, which followed national, 20 European 21 and American guidelines.22,23 This included the advice to stop hormonal contraception after the first ischemic stroke. According to our in-hospital investigational protocol for ischemic stroke, patients below age 55 routinely underwent admission testing for thrombin time, activated partial thrombin time, international normalized ratio, full blood count, antiphospholipid antibodies and homocysteine levels. If one of these values was abnormal, further testing was done according to hematology consultation. Although this is somewhat controversial, we did not systematically screen for thrombophilic states such as factor V Leiden, prothrombin deficiency, protein C/S deficiency etc. because international recommendations are considering such testing of “unknown usefulness”. 23 We defined recurrence as any new neurological event including ischemic and haemorrhagic stroke and transient ischemic attacks (TIA) in the first year after stroke. We evaluated long-term outcome at 12 months using the modified Rankin scale (mRS) either during outpatient cerebrovascular consultations or in a telephone interview using a validated questionnaire. 24
Statistical analysis and ethical considerations
We compared patients taking hormonal contraceptives (contraceptive group - CG) to patients who were not (non-user group - NU). We first performed a univariable logistic regression analysis and calculated the odds ratios and confidence intervals in addition to p values. We then chose variables based on clinical significance and/or with a p < 0.2 to perform a multivariable logistic regression analysis (LRA) in order to identify independent variables (predictors) associated with the CG. The outcome and cerebrovascular recurrence at 12 months were adjusted with variables significantly different in the LRA, and with parameters known to influence long-term outcome. 25 We performed analyses using Stata (StataCorp. 2011. Stata Statistical Software: Release 12. College Station, TX: StataCorp LP).
ASTRAL is registered as a clinical and research databank in our institution. Before analysis, we anonymised the data using the principles of the Health Insurance Portability and Accountability Act (HIPAA) Safe Harbour Privacy Rule. 26 We respected any patient decision to opt out of scientific use of their routinely collected clinical data. As we analysed anonymised data only in this project, there was no need for patient consent or ethics commission approval according to the current national laws. We applied the STROBE method (Strengthening the Reporting of Observational Studies in Epidemiology) to report results. 27 The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Results
From 2003 to 2015, we identified 179 women aged 50 years or less accounting for 10.3% of all women (n = 1742) registered in ASTRAL, of which 57 (39.6%) were on hormonal contraception. We list the detailed demographic and risk factor data in Table 1 and Supplemental Table 1. The 7 preceding events consisted of 3 recent events in acute cervical artery dissection (2 strokes and 1 TIAs), 3 remote events in PFO patients (1 stroke, 2 TIAs), and a stroke one month earlier in a patient with a biological aortic valve.
Contraceptive user group and control group (non-user) patient characteristics.
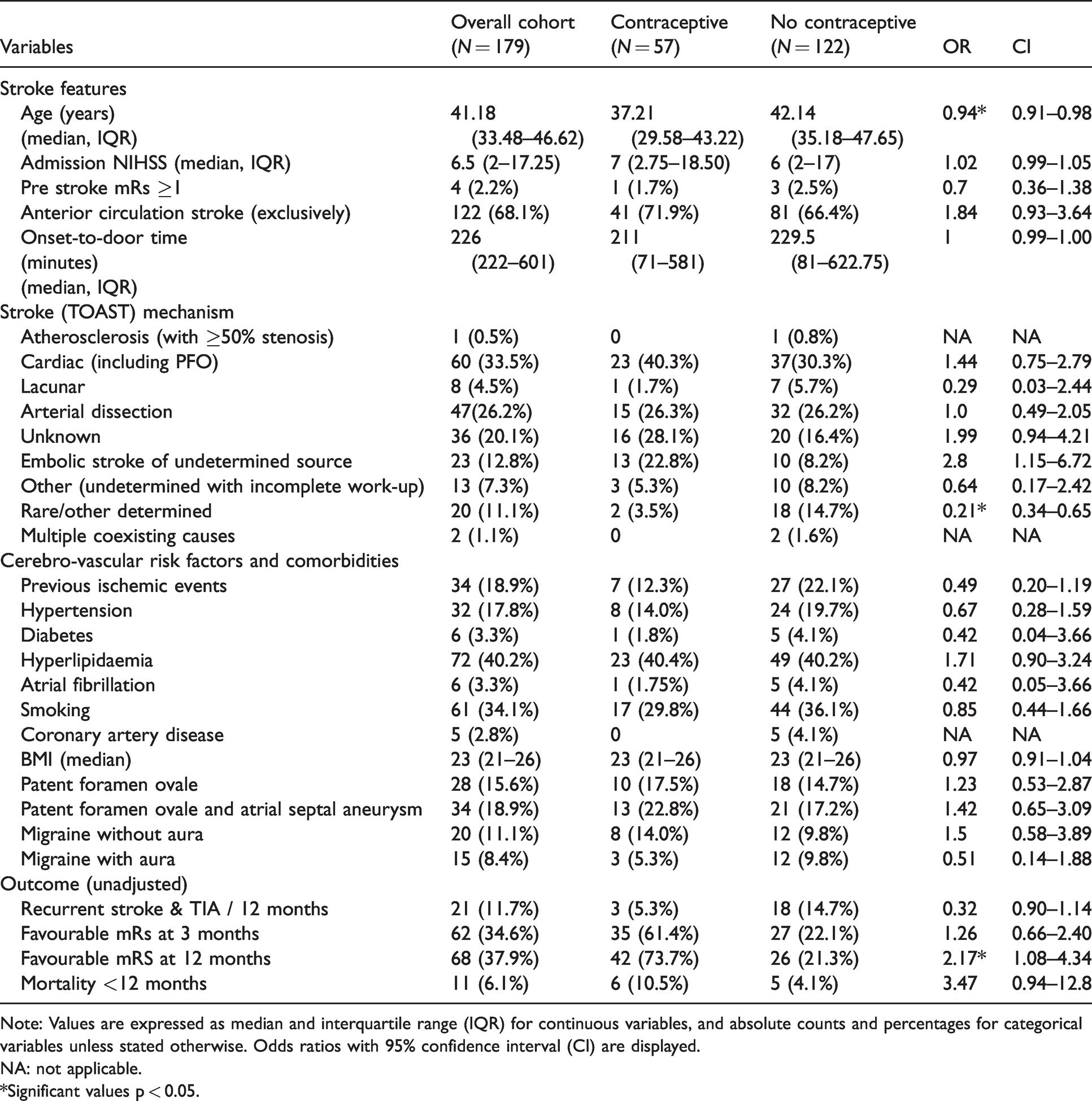
Note: Values are expressed as median and interquartile range (IQR) for continuous variables, and absolute counts and percentages for categorical variables unless stated otherwise. Odds ratios with 95% confidence interval (CI) are displayed.
NA: not applicable.
*Significant values p < 0.05.
Radiological and metabolic data appear in Table 2.
Radiological and laboratory values and clinical outcomes.
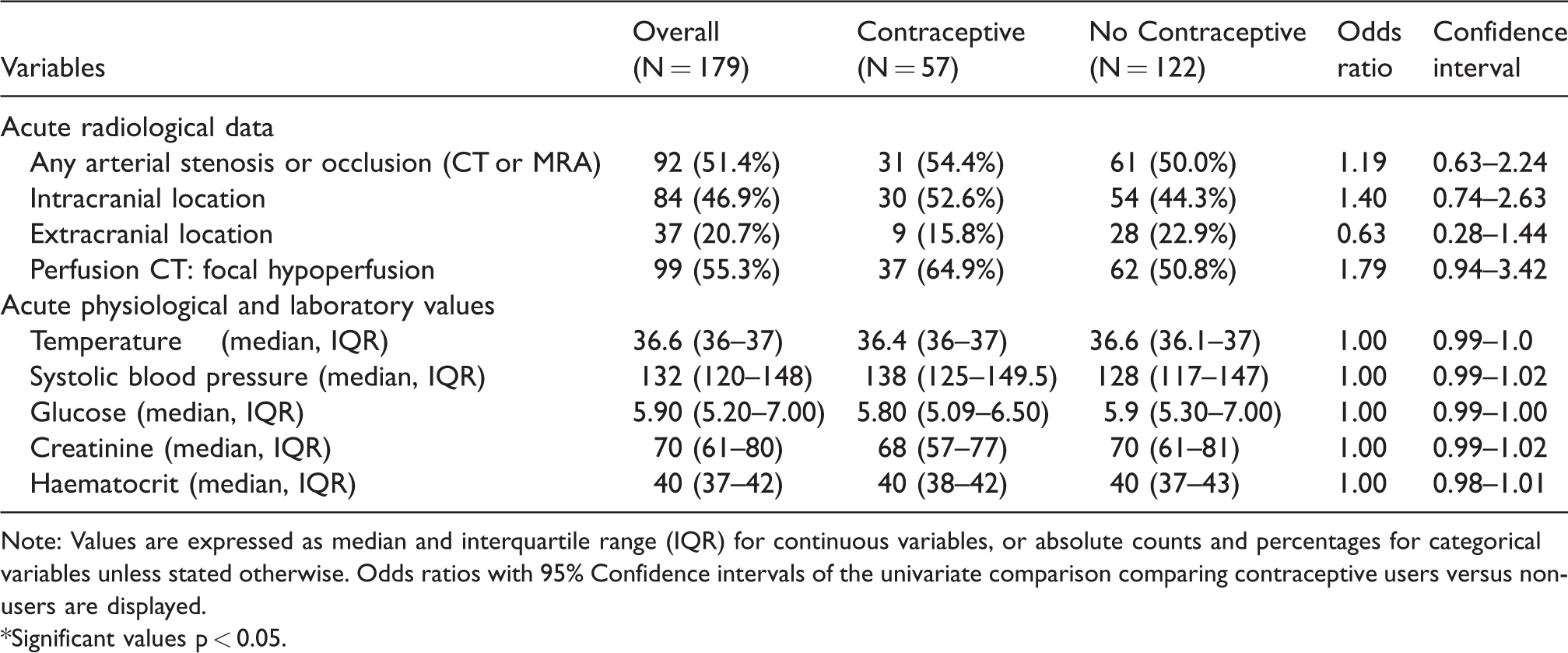
Note: Values are expressed as median and interquartile range (IQR) for continuous variables, or absolute counts and percentages for categorical variables unless stated otherwise. Odds ratios with 95% Confidence intervals of the univariate comparison comparing contraceptive users versus non-users are displayed.
*Significant values p < 0.05.
Women in the contraceptive group most frequently used new generation combined oral contraceptive pills amounting to 71.9% of cases (Supplemental Table 2). The other methods used included medroxyprogesterone acetate injections, progesterone-only pills, progesterone implant and combined contraceptive patches. All patients in the CG stopped hormonal contraception in the first 12 months after the index stroke.
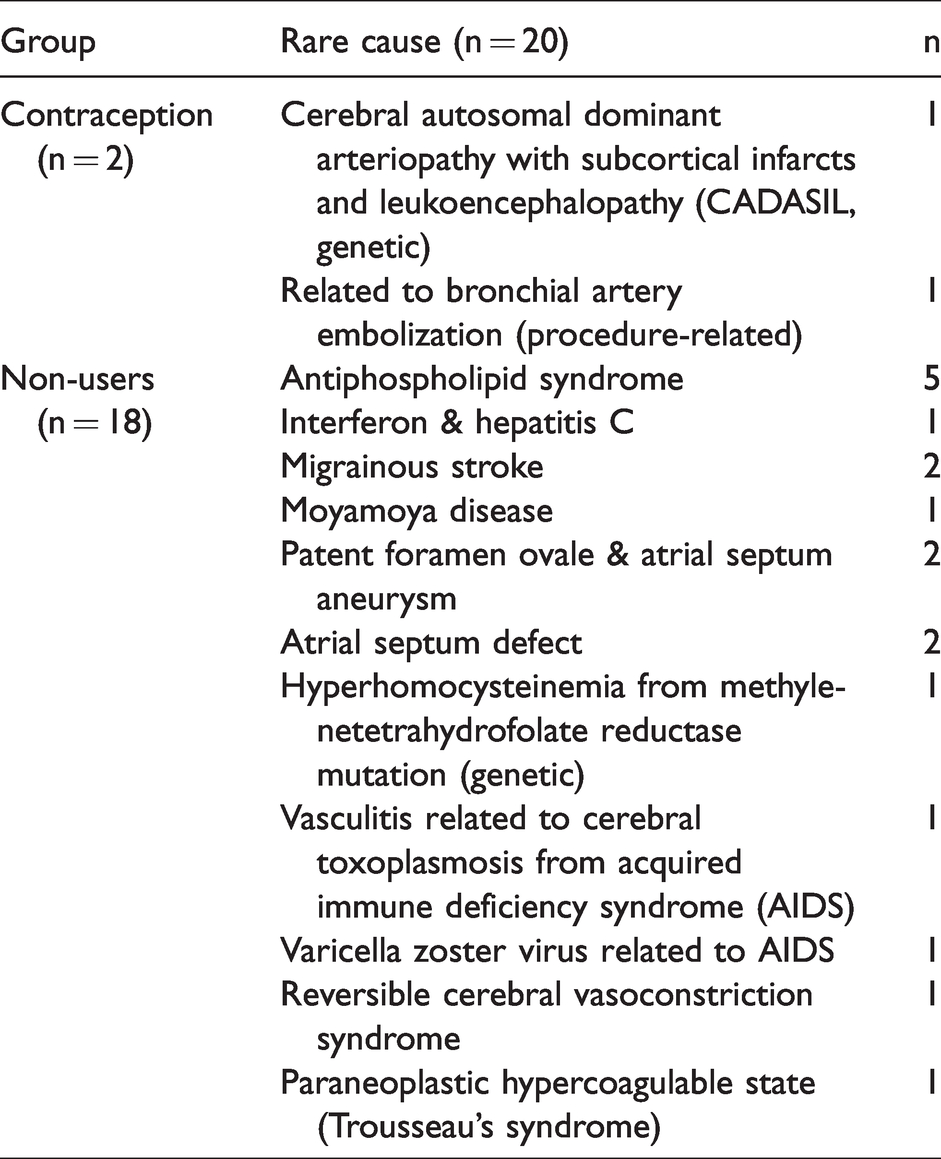
As shown in the multivariable LRA in Table 3, women in the contraceptive group were significantly younger compared to NU women (median age of 37 vs. 42 years). The CG patients had a lower prevalence of smoking and migraine with aura, but a higher prevalence of hyperlipidaemia. They also had a higher proportion of unknown stroke mechanism, with many cases fulfilling ESUS criteria (Table 1). Although stroke attributable to PFO was more frequent in the univariate analysis (40.3% vs. 31.9%, odds ratio (OR)1.44, confidence interval (CI) 0.75–2.79), this finding was no more significant in the LRA. In the radiological LRA (Table 4), CG patients had a higher rate of focal hypoperfusion on acute perfusion CT and significantly less intra- or extracranial pathology. Conversely, other determined (rare) causes of stroke were less frequent in the CG, as listed in Table 5. No patient in the contraceptive group had hyperhomocysteinemia, and one in the control group. One patient in the contraceptive group (with a PFO) had an elevated anti-phospholipid antibody titers in the acute stage which normalized during follow-up testing.
Logistic regression analysis showing the demographic and clinical differences between contraceptive users and non-user groups.
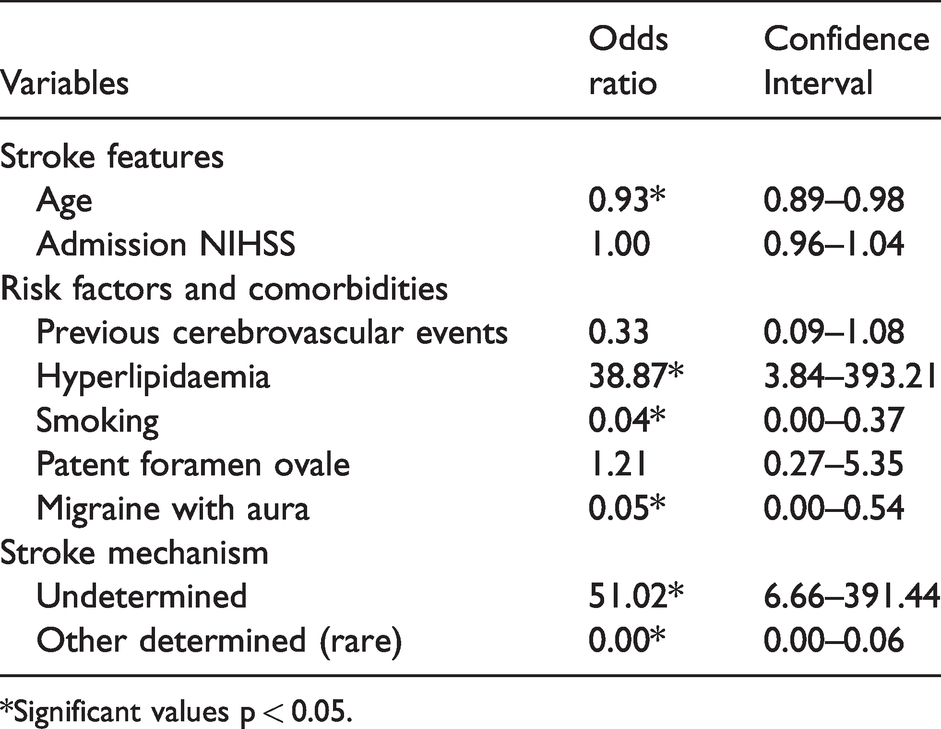
*Significant values p < 0.05.
List of rare causes of stroke in contraceptive users and non-users.
Logistic regression analysis showing radiological differences between contraceptive users and non-user groups.
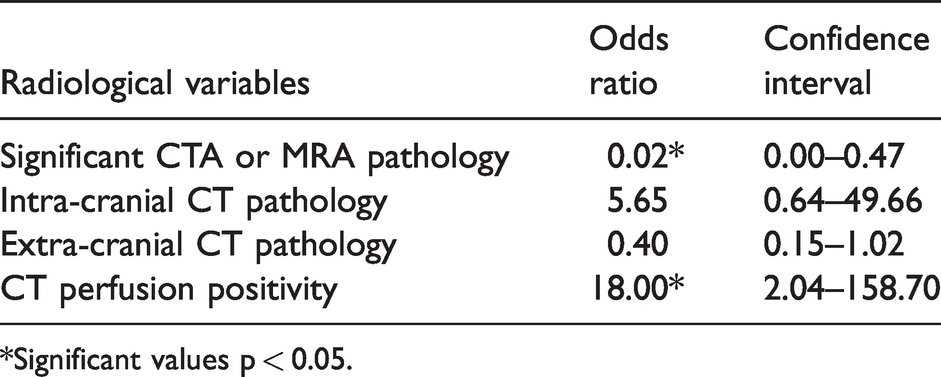
*Significant values p < 0.05.
Only one patient in the CG group was discharged on oral anticoagulation because her stroke occurred on anticoagulation for a recent deep vein thrombosis after appendicectomy; this treatment was continued after the stroke and then stopped when her PFO was closed 2.5 months later.
After adjusting for multiple variables (see Supplemental Table 3), clinical outcome at 12 months was significantly more favourable in the CG (adjusted odds ratio (ORadj) 3.68, 95% confidence interval (95%CI) 1.26–10.74, p = 0.02). The CG patients also had a significantly lower adjusted stroke and transient ischemic attack recurrence rate over 12 months (ORadj 0.04, 95%CI 0.00–0.55, p = 0.02, Supplemental Table 4).
Discussion
Our retrospective analysis of consecutive young female AIS patients showed that systemic hormonal contraceptive users were significantly younger, had less tobacco use and migraine with aura, but more hyperlipidaemia than non-users. On neuroimaging, they had significantly less overall (intracranial and extracranial) CT or MR angiography-based atheromatosis but more often focal hypoperfusion on CT perfusion studies. Undetermined mechanism of stroke was more frequent with use of contraception, and rare stroke mechanisms were less frequent. At 12 months, contraceptive users had a better functional outcome and less stroke recurrence than the comparison non-user group.
The fact that well-known risk factors such as age, tobacco use and migraine with aura were less frequent, and stroke etiology of undetermined cause more prevalent, indirectly confirms that oral contraceptives were an important independent risk factor for ischemic stroke in these cases. This confirms findings from large epidemiological6,28,29 and a recent study from our group investigating the risk factor profile of ischemic stroke in patients without established vascular risk factors. 30 The design of our study, which is not population based, does not allow to draw firm conclusions on associations of hormone use with other stroke risk factors.
As regards the etiology of stroke in the contraceptive group, the lesser intracranial and extracranial atheromatosis and higher incidence of focal hypoperfusion on CTP in our study allowed us to classify many of these strokes as ESUS. 19 The lower rate of strokes of other determined origin, and a similar rate of PFOs in contraceptive users and non-users, suggests that the predominant stroke mechanism in systemic hormonal contraception is an arterial prothrombotic state rather than paradoxical embolization or accelerated atherosclerosis.
Still, the absolute risk of stroke will of course depend largely on the patient’s baseline stroke risk and therefore on established cerebrovascular risk factors, including migraine with aura.31,32 Therefore, potential users of SHC have to be informed about both their absolute and relative risk for ischemic stroke. 33 This increased relative risk of hormonal contraception is also present in new generation lower-dose combined contraceptives, 34 but not in progestin-only contraceptives. 35
Interestingly, hyperlipidaemia was independently associated with use of contraception in ischemic stroke patients. Women using combined oral contraceptives are at increased risk of myocardial infarction and stroke and should be advised about this risk. 36 Routine screening of lipid profiles before prescription of SHC is however not recommended.33,37 On the contrary, non-hormonal contraceptive methods should be proposed to women with LDL cholesterol levels more than 160 mg/L (4 mmol/L) or multiple cardiovascular risk factors. 38
Our cohort of contraceptive users had a better functional long-term outcome after adjustment for age, stroke mechanism and multiple other prognosis-related factors. 25 This may be partially related to less stroke recurrence, which could be explained by the fact that contraceptive users in our study stopped using systemic hormonal contraception after stroke, as recommended.20–23 This change seems to have removed an important risk factor for stroke and recurrence in such women.
Limitations of our study are its retrospective, non-randomized nature, and a predominantly Caucasian, Western population. Although most of our patients used a combined estrogen-progestin pill, the limited number of eligible AIS patients does not allow a more detailed analysis of the specific classes of hormonal treatments. The small number of patients on hormonal contraception led to wide confidence intervals and a potential to miss additional associations. Still, the identified associations were sufficiently strong that adjusted analyses led to several statistically significant results. Also, we did not collect data regarding the duration of contraceptive use before the stroke. The lower prevalence of women with a history of smoking and migraine with aura in the contraceptive group could also be affected by bias resulting from prescriptions based on international guidelines which deter the initiation of hormonal contraceptive methods in this group of women. Finally, a complete work-up for more rare coagulopathies was not performed despite potential associations with hormonal contraception in AIS, 33 because their impact on further management is uncertain. 23
In conclusion, ischemic stroke in young women taking hormonal contraceptives is frequently due to unknown, embolic stroke mechanisms, suggesting a hormone-induced prothrombotic state. Their association with hyperlipidaemia may suggest that monitoring and treatment of lipid parameters in these women could further decrease their stroke risk. Our findings reiterate the importance of careful evaluation of cardiovascular risk factor profile before starting hormonal contraception and having a low threshold to prescribing lipid profile evaluation especially in high-risk women. The women have a better long-term outcome with little recurrence if they stop hormonal contraception post stroke.
Supplemental Material
sj-pdf-1-eso-10.1177_23969873211019586 - Supplemental material for Ischemic stroke on hormonal contraceptives: Characteristics, mechanisms and outcome
Supplemental material, sj-pdf-1-eso-10.1177_23969873211019586 for Ischemic stroke on hormonal contraceptives: Characteristics, mechanisms and outcome by P Correia, S Machado, I Meyer, M Amiguet, A Eskandari and P Michel in European Stroke Journal
Supplemental Material
sj-pdf-2-eso-10.1177_23969873211019586 - Supplemental material for Ischemic stroke on hormonal contraceptives: Characteristics, mechanisms and outcome
Supplemental material, sj-pdf-2-eso-10.1177_23969873211019586 for Ischemic stroke on hormonal contraceptives: Characteristics, mechanisms and outcome by P Correia, S Machado, I Meyer, M Amiguet, A Eskandari and P Michel in European Stroke Journal
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Pamela Correia (PC)- Reports no conflict of interest. Sara Machado (SM)- Reports no conflict of interest. Ashraf Eskandari(AE)- Reports no conflict of interest. Ivo Meyer (IM)- Reports no conflict of interest. Michael Amiguet (MA) - Reports no conflict of interest. Patrik Michel (PM) received research grants from the Swiss National Science Foundation, the Swiss Heart Foundation and the ERISTA program (BMS/Pfizer) within the last 2 years; and consulting fees from Medtronic. All this support goes to his institution and is used for stroke education and research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a Swiss Government Excellence Scholarship and a Swiss Heart Foundation Grant, both obtained by PC. PM has received within the last 2 years research grants from the Swiss National Science Foundation, the Swiss Heart Foundation and the ERISTA program (BMS/Pfizer); and consulting fees from Medtronic. All this support goes to his institution and is used for stroke education and research.
Informed consent
The ethical standards committee for research on humans of the Canton of Vaud (CER-VD) approved the use of anonymized data from the Acute Stroke Registry and Analysis of Lausanne (ASTRAL) registry for scientific purposes without requiring individual informed consent because of the retrospective nature of this study.
Ethical approval
This study was conducted under the auspices of the ethical standards committee for research on humans of the Canton of Vaud (CER-VD). No experiments were performed on human participants.
Trial registration
Not applicable.
Guarantor
PM.
Contributorship
PC, SM, PM: Conceived the manuscript, analyzed the data, drafted the initial manuscript, agreement to be accountable for all aspects of the work, IM, AE, MA: Acquisition and interpretation of clinical data, critically revised the manuscript, agreement to be accountable for all aspects of the work.
Acknowledgements
We thank Ms. Melanie Price Hirt for critical comments on the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.