
Abstract
Stroke continues to be one of the main causes of death in the developed countries and the incidence in pregnancy appears to be increasing. Pregnancy-related stroke has a relatively high mortality rate of 10% and so clinicians need to be mindful of appropriate investigations and referral of a pregnant woman with suspected stroke, so they can receive timely treatment. In this review we address the risk factors associated with stroke, diagnosis and appropriate management of the different stroke types. We also discuss implications for care around pregnancy and delivery as well as reviewing how a pregnancy with previous stroke should be managed.
Introduction
Stroke is currently one of the leading causes of death and disability in developed countries. 1 The risk amongst women of childbearing age is low but pregnancy appears to increase this risk particularly in the peripartum period. 2 Furthermore, the incidence of stroke in pregnancy and the puerperium appears to be increasing. 3 This is likely to be explained by women delaying pregnancy until older ages and by increasing rates of obesity, diabetes and hypertension. A recent systematic review and meta-analysis of stroke and pregnancy that included 11 studies estimated that stroke affects 30 out of 100,000 pregnancies, this figure being three times higher than for young adults overall.4,5 The incidence of stroke is highest in the third trimester and puerperium, and increased in older women and those with hypertensive disorders in pregnancy.2,6,7 If stroke is suspected in pregnancy it is essential that prompt referral and timely investigations are undertaken so that women receive appropriate treatment. Data from a large retrospective study showed that although the rate of ischaemic stroke is higher than that of haemorrhagic stroke in pregnancy (being 11 versus nine per 100,000 deliveries 8 ), actually haemorrhagic stroke is relatively more common in pregnancy than outside, where the ratio of haemorrhage to infarct in the general population in Europe is 15–85%.
Further data from the United Kingdom Obstetric Surveillance System (UKOSS) also demonstrated that for strokes that occurred in the antenatal period the rate of non-haemorrhagic strokes was 0.9 versus 0.5 for haemorrhagic stroke per 100,000 deliveries. 7 The mortality following pregnancy-related stroke is around 10%, although this figure may be greater for antenatal stroke. 8 Clinicians should be mindful that from the most recent Confidential Enquiry into maternal deaths in the United Kingdom stroke accounted for 26 maternal deaths between 2011 and 2013 with a rate of 0.75 per 100,000 deliveries.9,10
Diagnosis
As with the non-pregnant population if stroke is suspected it is essential that the diagnosis is confirmed in a timely manner as this may influence treatment strategies. Neuroimaging will help to differentiate an ischaemic versus a haemorrhagic stroke and computerised tomography (CT) or magnetic resonance imaging (MRI) should be undertaken. MRI is usually the preferred imaging modality in pregnancy and has a greater sensitivity at identifying small infarcts, cerebral venous thrombosis (CVT) and structural problems such as cavernomas. 11 MRI scanning is safe in all trimesters and historically whilst there may have been some concern regarding teratogenicity there are no human data to demonstrate this. Indeed recent guidance from the American College of Obstetricians and Gynaecologists supports the use of appropriate diagnostic imaging in pregnancy. 12 CT is often more accessible and readily available in most acute settings and should not be withheld (as the fetal dose exposure to ionising radiation is incredibly low and shielding can be undertaken) if an MRI scan cannot be undertaken in a timely fashion. Perfusion CT and angiography CT can also be undertaken in pregnancy as they may guide appropriate interventional therapies. For instance, CTA is typically undertaken when thrombectomy is a possible option. Presently, there is less evidence for CT perfusion as a technique for decisions around stroke management and should not be done performed in view of the additional burden of radiation. Scanning with contrast is rarely needed for the initial diagnosis and management but gadolinium-enhanced MRI has previously been avoided because of concerns regarding fetal safety, although recent data suggest that these concerns may be unfounded. 13 As imaging is mandatory to make a diagnosis of stroke it should be noted that positioning of the mother to allow displacement of the gravid uterus to reduce aortocaval compression should be undertaken, especially in the third trimester.
Risk factors
Ischaemic stroke
Pre-eclampsia and eclampsia
Pregnancy-associated stroke is more common in women with pre-eclampsia and eclampsia. 14 Pre-eclampsia is a multisystem disorder characterised by hypertension, proteinuria and generalised oedema with vascular endothelial dysfunction. Eclampsia is defined as pre-eclampsia with concomitant seizures. In the 2006–2008 Confidential Enquiry into maternal deaths in the United Kingdom over three quarters of the deaths from severe pre-eclampsia and eclampsia were from cerebral causes. 15 A recent North American study showed that in women with pre-eclampsia who went on to have a stroke, those with more severe pre-eclampsia and eclampsia, as well as those who had evidence of intercurrent infections, were at greatest risk of pregnancy-associated stroke. 16
Migraine
Migraine is common and affects up to a quarter of women of childbearing age 17 Analysis of hospital discharge data from the United States demonstrated migraine was strongly associated with stroke (odds ratio of 15.8) between migraine and ischaemic stroke; 18 but causality could not be established. 6 Similarly data from a retrospective cohort UKOSS study demonstrated that women with migraine had an odds ratio of antenatal stroke of 8.5 (95% CI 1.5–62.1). 7 The overall number of confirmed strokes during pregnancy in this study was small and so the findings from this study should be interpreted with caution. In addition, migraine is often misdiagnosed as a transient ischaemic attack, which may have led to an overestimation of the association.
Hypercoagulability and antiphospholipid syndrome
Increased levels of activated protein C, fibrinogen and other clotting factors, coupled with decreased levels of protein S culminate in a hypercoagulable state in pregnancy and the puerperium. In addition, specific thrombophilias increase the risk of stroke. Outside pregnancy, data from a prospective observational study showed that over a 10-year period in patients with Antiphospholipid Syndrome (APS) the risk of stroke was 5.3%. The overall incidence of APS in pregnancy is largely unknown but probably <1%, although antiphospholipid antibodies are present in approximately 15% of women with recurrent miscarriage. 19 Outside pregnancy in a cohort of 1000 patients with APS stroke was reported in almost 20% of cases although this may relate to case ascertainment. 20 APS is particularly pro-thrombotic in pregnancy, and even when women are treated with aspirin and low molecular weight heparin for a history of prior ischaemic stroke in one study the rate of recurrence in pregnancy was 10.7%. 21
Cardiac disease
Mechanical heart valves
The risk of cardioembolic stroke in pregnancy in women with metal heart valves varies between 0.005 and 7%.22,23 Women appear to be at particular risk during the point at which their anticoagulation regime is converted from Vitamin K antagonists to low molecular weight heparin so as to reduce the risk of warfarin embryopathy. This risk appears greatest if women are not referred to specialists who can provide appropriate multidisciplinary care. 22 In selected cases in women with mechanical heart valves, particularly those with multiple prostheses, or with concurrent atrial fibrillation or in those with previous thromboembolic complications, it may be advisable to continue warfarin in pregnancy, notwithstanding the increased risks of miscarriage, stillbirth and embryopathy, since the risk of valve thrombosis is lower with warfarin.
Patent foramen ovale (PFO) and atrial septal defect (ASD)
A PFO is an embryological anomaly caused by lack of fusion of primum and secundum septum that normally occurs after birth, when left atrial pressure rises above right atrial pressure. It is common and may affect almost 30% of the population. 24 Whilst uncommon a recent review reported that the majority of women with stroke associated with PFO have a good neurological outcome 25 The desire for pregnancy alone would, however, not typically be seen as a reason to close a PFO. This has been supported by the findings from a meta-analysis of studies in individuals with prior stroke and PFO that failed to show such closure ensures any benefit over medical therapy. 26 Nevertheless, these studies did not include pregnant women in their analysis. However in women who have had a prior stroke, data from three recent randomised trials demonstrate a lower rate of stroke recurrence in individuals who had closure of a PFO versus medical therapy long term.27–29 Closure prior to a planned pregnancy needs to be an individualised decision. Closure of a PFO during pregnancy is not routinely recommended but use of low-dose aspirin should be considered for secondary stroke prevention. ASD is a less common congenital defect with a prevalence reaching 0.1%. 30 Closure of a known ASD can reduce the incidence of complications such as stroke. 31 For women who present with embolic stroke in pregnancy a bubble echocardiogram is an important investigation, since finding of a shunt (PFO/ASD) would be an indication for anticoagulation with low molecular weight heparin since it should be assumed that the paradoxical stroke arose from a deep venous thrombosis in the absence of another obvious cause. Despite the lack of published evidence bubble echocardiograms are generally viewed as safe in pregnancy as there is no theoretical reason why the use of agitated saline would be harmful in pregnancy. It is an important assessment tool and should not be withheld in pregnancy.
Peripartum and other dilated cardiomyopathies
Peripartum cardiomyopathy is rare but characterised by marked cardiac dysfunction at the end of pregnancy or within several months of birth when no other explanation for heart failure is present. Pre-existing but unrecognised dilated cardiomyopathy may also present in pregnancy due to the increased cardiac demands. Either can lead to the formation of cardiac thrombi and subsequent embolism. 32 In women who present with new stroke and marked global impairment of systolic function this diagnosis should be considered.
Carotid and vertebral artery dissection
Dissection of the carotid or vertebral artery is uncommon in women of childbearing age, but recent data suggest that they occur more commonly in the postpartum period, but diagnosis may be delayed because of a low index of suspicion. 33 Early diagnosis is key as it may prevent complete vessel occlusion and the thromboembolic sequelae. In a small cases series and literature review of 27 cases, advanced maternal age (mean age 34 years) appeared to be the only common risk factor. Interestingly, raised maternal blood pressure and a prolonged period of pushing (Valsalva) were not associated with arterial dissection. 33 For women with a prior history of dissection, a recent European observational study did not suggest a high rate of recurrence in pregnancy with a prior history of dissection, 34 although women need to be counselled about the possibility of recurrence.
Thrombotic thrombocytopenic purpura (TTP) and haemolytic uraemic syndrome (HUS)
TTP and HUS are acute syndromes with abnormalities in multiple organ systems that demonstrate microangiopathic haemolytic anaemia and thrombocytopenia. Neurologic manifestations can include coma, confusion, seizure, transient ischaemic attack and stroke. There is an association between TTP and pregnancy. 35
Amniotic fluid embolism (AFE)
AFE occurs when there is a breach in the maternal–fetal physiological barrier during labour and a subsequent proinflammatory response. Definitive diagnosis is challenging as there are no universally accepted diagnostic criteria. Nevertheless, maternal stroke has been attributed to AFE. In an Australian cohort study of over 600,000 deliveries there were 20 cases of AFE; 36 in these 20 women there were four recorded cases of cerebral infarction. The authors of this study felt that the association was related to the hypercoagulable state resulting from AFE. 36
Intracranial and subarachnoid haemorrhage
Intracranial haemorrhage that includes subarachnoid bleeds is uncommon and usually related to an underlying aneurysm or vascular abnormality. Registry data from Germany showed that overall incidence of non-traumatic subarachnoid haemorrhage was 11.3 per 100,000 years. 37 Intracranial haemorrhage is one of the crises that can occur in pre-eclampsia and eclampsia 38 and indeed remains the commonest cause of death in women with pre-eclampsia. 39 Subarachnoid bleeds are usually a consequence of aneurysmal rupture in pregnancy and occur most frequently in the third (55%) and second trimesters (31%). Outside of pregnancy the estimated incidence of subarachnoid haemorrhage is about 2–22 per 100,000 people.40,41 Overall pregnancy probably does not increase the risk of bleeding from aneurysmal subarachnoid vessels.
Although intracranial haemorrhage is less common than ischaemic stroke mortality is higher. Retrospective data from a large UK series demonstrated that mortality from intracranial haemorrhage was the single greatest cause of maternal death from stroke. 7
Underlying vascular anomalies
Arteriovenous malformations (AVMs) are rare with a reported prevalence of 18 per 100,000. 42 In a review of nearly 60,000 deliveries there were 11 reported haemorrhagic strokes of which four were due to rupture of an AVM. 43 It is not clear whether pregnancy increases the risk of haemorrhage from an AVM. A retrospective review of 154 cases of spontaneous intracerebral haemorrhage during pregnancy noted that 23% of cases were attributable to AVM rupture. They noted that aneurysms and AVMs bled more frequently with increasing gestational age. Of 13 women undergoing surgery with ruptured AVMs, there was a 23% maternal mortality rate. Of 22 women who were observed with ruptured AVMs, there was a 32% maternal mortality rate. A smaller more recent study from a single centre showed that haemorrhage was higher in a cohort of women specifically during pregnancy at 8.1% with a hazard ratio for haemorrhage of 7.9 versus 1.1% during the study period. 44 Management for an unruptured AVM in pregnant women should be individualised with women being referred for expert preconception counselling.
Cavernomas are composed of dilated, thin-walled capillaries encompassed in a simple endothelial lining with no elastic or smooth muscle fibres in the vessel wall and are most commonly sited in the cerebellum. They usually present with epilepsy or ICH. Pregnancy may cause an increase in size of a cavernoma which then may logically increase the risk of bleeding. However, data from a Canadian study suggest that pregnancy and delivery do not increase the haemorrhage risk from a cavernoma. 45 Pregnant women with a known cavernoma with no symptoms can be managed expectantly; but in cases where there is bleeding or intractable seizures, surgery may need to be considered.
Untreated vascular malformations are prone to rebleeding whether or not the patient becomes pregnant. Data from an American study examining recurrent haemorrhage in women with a known brain AVM estimated the incidence to be 31% in the first year following an initial haemorrhage and 6% in subsequent years. 46 It is logical therefore that vascular malformations should be definitively treated if possible, by surgical excision or endovascular embolisation, in women before attempting pregnancy. Women with AVMs that are not easily amenable to surgical management should be counselled that pregnancy may increase their risk of an intracranial haemorrhage. (For mode of delivery see section below.)
Reversible cerebral vasoconstriction syndrome (RCVS)
RCVS describes a clinical and radiographic syndrome that includes many aetiologies (including pregnancy and pre-eclampsia). The syndrome includes the entities that represent the same vasospastic disorder, namely postpartum angiopathy, drug-induced cerebral vasospasm and benign cerebral angiopathy. It usually presents with abrupt onset severe headache, with or without focal neurological deficit and seizures. Neuroimaging shows multifocal vasoconstriction in large and medium-sized vessels and can be associated with haemorrhagic or ischaemic stroke. In pregnancy the majority of cases develop in the postpartum period, with many cases being associated with vasoactive drugs. 47 Headache can be treated with calcium channel blockers (nimodipine), but symptoms may resolve without treatment, especially if any precipitant is removed. 48
Cerebral venous sinus thrombosis
Pregnancy and the puerperium are associated with an increased risk of venous thrombotic events both in cerebral and non-cerebral territories. The incidence estimates for CVT during pregnancy and the puerperium range from one in 2500 deliveries to one in 10,000 deliveries in Western countries,49,50 with the highest risk periods for CVT being the third trimester and early postpartum period. Headache is the most typical presenting feature and can precede other symptoms or signs by many days. This can be accompanied by encephalopathy, focal signs and/or seizures. Neuroimaging may reveal venous infarction with or without haemorrhage. Unenhanced CT imaging may demonstrate hyperdensity in the sagittal sinus due to occlusion from thrombus often referred to as the ‘delta’ or ‘dense triangle sign’. In contrast, the ‘empty delta sign’ is also a CT sign (CT with contrast) of thrombosis of the superior sagittal sinus, where contrast outlines a triangular filling defect (thrombus). MRI in combination with MR venography remains the most sensitive imaging methodology for CVT. 51 However, CT venography also provides good visualisation, is quicker and often more readily available than MR venography. Treatment aims to recanalise any venous/sinus occlusion and prevent propagation of the thrombus through the use of anticoagulation, although definitive evidence for this is lacking. Nevertheless in a non-randomised non-pregnant case–control study of over 400 patients with CVT who received LMWH compared to unfractionated heparin showed that a greater proportion of those that received LMWH were independent at six months follow-up. 52 Thrombophilia screening should be conducted six weeks postpartum to exclude any underlying thrombophilia.
Management of ischaemic stroke
Initial stroke management of pregnant women does not differ from that of the non-pregnant patient, with care focused on adequate oxygenation, maintaining circulatory integrity and euglycaemia. Further management is then directed to confirm whether the stroke is ischaemic or haemorrhagic as this will determine whether thrombolysis/clot retrieval is appropriate. In young patients presenting with ischaemic stroke, typically those of less than 45 years of age, antiphospholipid antibody testing is recommended, as well as echocardiography, to exclude a paradoxical embolus or other cardiac cause. Extracranial imaging is also appropriate to assist in determining the underlying cause of the stroke if the initial tests fail to reveal a cause.
Thrombolytic therapy
Stroke thrombolysis improves outcome for ischaemic stroke for individuals presenting up to 4.5 h after onset of symptoms.53,54 Historically pregnancy was considered a relative exclusion for thrombolysis in ischaemic stroke, as pregnant women were not included in the original trials involving recombinant tissue plasminogen activator (tPA). 55 However, in more recent times there has been a shift to consider thrombolysis in pregnancy because published data appear to suggest positive outcomes; indeed outcomes from pregnant women receiving thrombolysis are comparable to non-pregnant women. 56 Recent registry data from the United States showed that in a cohort of young women aged 18–44 years, pregnant women and those in the postpartum period were less likely to receive thrombolytic therapy. 56 They also demonstrated that the rate of symptomatic intracranial haemorrhage following thrombolysis was greater in the pregnant or postpartum group of women who received tPA, although this was not significant; but importantly there was no significant difference between pregnant or postpartum women and non-pregnant women for rates of in-hospital death, discharge to home or independent ambulation at home. Whilst this study is retrospective and small, management needs to be individualised with clear discussion between the patient, neurology/stroke and obstetric teams. The risks of maternal haemorrhage or abruption both of which could lead to preterm labour must be balanced against the fact that half of women who suffer a pregnancy-related stroke will go on to suffer some residual neurological deficit. The most recent American Heart/American Stroke Association Guidelines from 2015 consider pregnancy as one of the relative exclusions from thrombolytic therapy, but state that in certain circumstances, particularly when it is felt that morbidity from stroke would be reduced by thrombolysis, it should be considered. 57 In the UK the advice is that pregnancy and the postpartum start should NOT be a contraindication to thrombolysis. 9
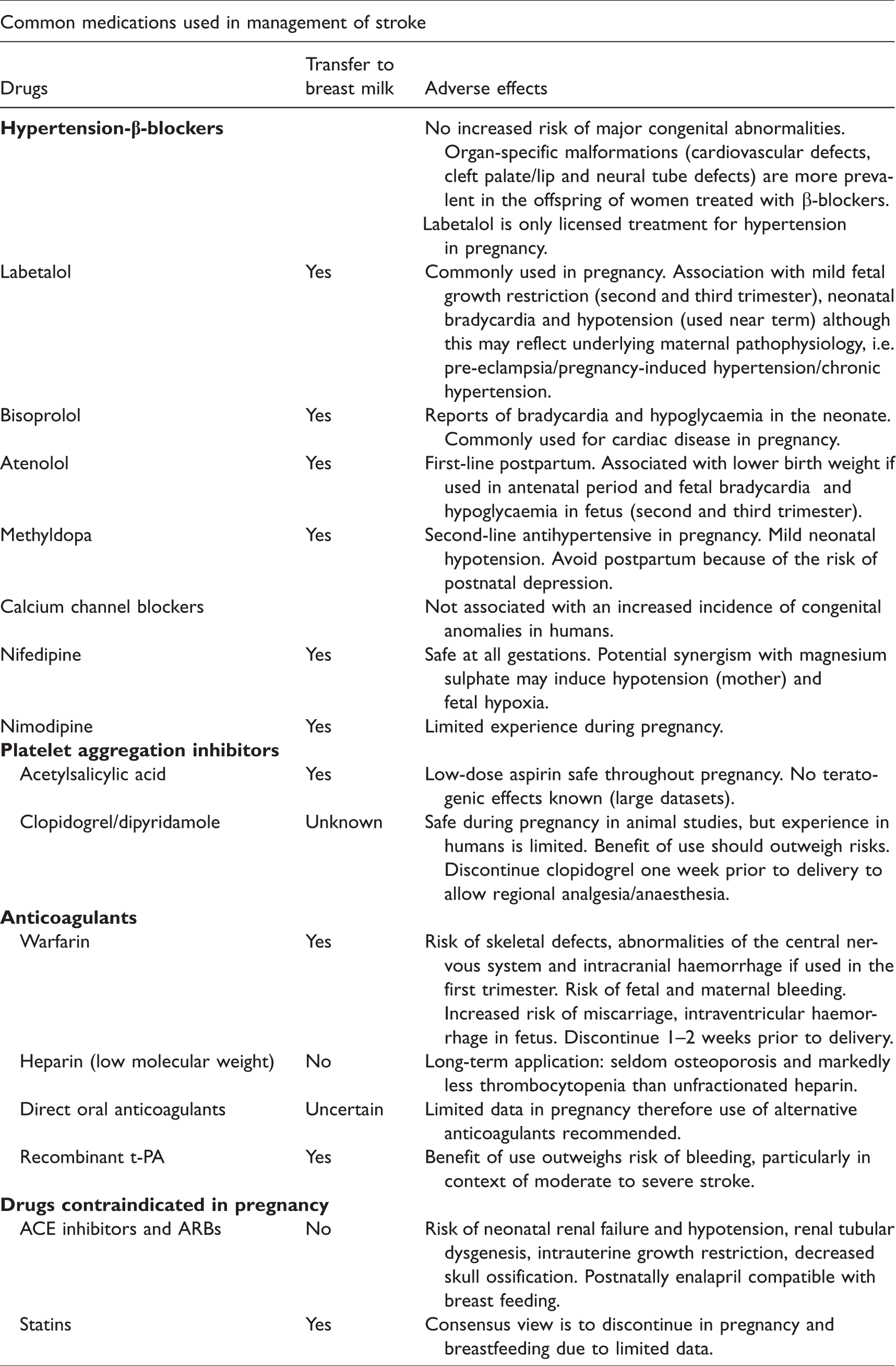
If a pregnant patient receives tPA then aspirin should be started 24 h following thrombolysis to reduce the risk of recurrent stroke. Aspirin can be safely continued throughout pregnancy; data from the CLASP study demonstrated a tendency to a greater need for blood transfusion in the group of women treated with aspirin, but there were no other adverse maternal or fetal effects. 58 Table 1 lists some of the common medications used in stroke medicine and during pregnancy.
Common medication used in the management of stroke.
Thrombectomy
Mechanical thrombectomy is licensed for use in selected patients that present within 6 h of new onset of stroke symptoms and is of particular benefit to those who present with an arterial occlusion in the proximal anterior circulation. Indeed more recent data would suggest benefit up to 24 h after onset of symptoms. 59 A variety of different mechanical devices are in use although again the trials that were conducted prior to their implementation excluded pregnant patients.60,61 Most patients also received bridging tPA prior to thrombectomy but pregnancy may be an indication for withholding this and going straight to thrombectomy. In theory these treatments may be preferable in women where obstetric haemorrhage is a concern, such as women with a placenta praevia or those at particular risk of bleeding. There are few case reports that describe use of these devices in pregnancy although it is likely the numbers will increase. 62 Currently, not all centres providing specialist stroke services offer mechanical thrombectomy and only approximately 10% of patients with acute ischaemic stroke have a proximal large artery occlusion in the anterior circulation and present early enough to qualify for this treatment.
Management of haemorrhagic stroke
Initial management of haemorrhagic stroke involves both medical and, if necessary, surgical intervention. Medical therapy should be targeted towards management of hypertension. Blood pressure management following haemorrhagic stroke requires careful assessment as marked elevations in blood pressure may cause haemorrhage expansion. 63 Conversely an increased mean arterial blood pressure maybe required to maintain cerebral perfusion in some patients, and so a fall in systolic blood pressure may cause ischaemia and worsen neurologic injury. 64 Hyperglycaemia has been shown to be associated with poorer outcomes and the use of insulin may need to be considered. 65 Outside pregnancy in patients with limited mobility, the use of intermittent pneumatic calf compression has been shown to lower rates of venous thromboembolism. 66 All antiplatelet and anticoagulation medication should be stopped immediately and if on warfarin this requires pharmacological reversal. Whilst NOACs are not recommended for use in pregnancy, reversal agents can be used should women suffer a haemorrhagic stroke. 67 Measures to reduce intracranial pressure with osmotic diuretics may be required and should be undertaken for maternal benefit and, if warranted, surgical evacuation of haematomas also. Seizures can elevate intracranial pressure and so anti-epileptic medication may be indicated. Newer anti-epileptic agents such as levetiracetam, do not have the dose-dependent side effects of fetal congenital malformations seen with older agents such as valproate. 68
Specific pregnancy considerations
Blood pressure management during pregnancy
Women with hypertension are at greater risk of stroke during pregnancy and so treatment of hypertension is important. The most commonly used agents in pregnancy are methyldopa, labetalol and nifedipine all of which are safe. The Control of Hypertension in Pregnancy Study evaluated the management of moderate hypertension in pregnancy (diastolic blood pressure between 85 and 105 mm Hg) comparing tight versus less tight control and demonstrated that in women assigned tight control (DBP 80–85) there was a lower incidence of severe hypertension. 69 However, the study failed to show any reduction in the incidence of primary outcomes such as perinatal death or still birth between the two groups. For women with a prior history of stroke blood pressure control is vital. Hypertension should be managed in the same way as it would be outside of pregnancy, but with the use of agents mentioned above. In women with haemorrhagic stroke blood pressure control should be addressed in relation to intracranial pressure; intravenous labetalol and hydralazine can be safely used for acute blood pressure management. Previous older data suggesting an association between beta blockers and fetal growth restriction related to larger doses than currently employed were subject to confounding by indication. NICE recommends labetalol as first-line agent to treat hypertension in pregnancy. 70
Pharmacotherapy
Statins
Statins have a well-established use for secondary stroke prevention but their use in pregnancy is usually not warranted. Currently, statins are considered to be contraindicated in pregnancy due to higher rates of birth defects. 71 However when the authors corrected for cofounding factors such as age and diabetes the detrimental effects of statins were not apparent. For those already on statins for secondary prevention a short interruption for the duration of pregnancy is unlikely to cause any harm. Lipids should not be measured during pregnancy as interpretation of results is unreliable since there is a physiological increase in both cholesterol and triglycerides.
Antiplatelet agents
Decision making for antiplatelet medications in pregnancy should be individualised to the patient and should be multidisciplinary. In women who are already taking an antiplatelet other an aspirin for a prior stroke, then a discussion should be had regarding switching to low-dose aspirin throughout the pregnancy. In circumstances where a specific antiplatelet may need to be continued, such as clopidogrel for a coronary stent or post-PFO closure, management should be individualised. Clopidogrel is safe in pregnancy but should be discontinued 10 days prior to delivery to allow regional analgesia and anaesthesia.69,72 Low-dose aspirin does not need to be withdrawn for delivery or breast feeding.
Mode of delivery
In women who have had a prior ischaemic stroke vaginal delivery can be encouraged providing there is no obstetric contraindication. Women who have received prior treatment for an AVM or an aneurysm can also be reassured that vaginal delivery is appropriate. In cases of ruptured aneurysm, untreated or partially treated AVMs and very recent neurosurgery, the most appropriate mode of delivery is less clear. At present there are no data, even from large series, to suggest whether a caesarean section is preferable to vaginal delivery and so management should be individualised. No studies have compared caesarean section against vaginal delivery in women with untreated AVMs. Vaginal delivery, with epidural and consideration for shortened second stage, maybe preferable as this reduces fluctuations in maternal blood pressure and carries a lower risk of obstetric haemorrhage than caesarean delivery.
Risk of recurrent stroke and stroke in future pregnancies
The overall rate of recurrence of stroke associated with a subsequent pregnancy is small. In a French multicentre study of women aged 15–40 years presenting with cerebrovascular events over a five-year period, the absolute recurrence rate outside of pregnancy was 0.5% and during was 1.8%. 73 The two strokes that recurred in pregnancy were associated with rare stroke causes, essential thrombocythaemia and antiphospholipid syndrome. Pregnancy complications in women with a prior stroke appear to be greater but this may represent the underlying maternal pathophysiology. 74 Women who are taking aspirin following an initial stroke can be reassured that they may continue with this in any future pregnancy. Data from a systematic review demonstrated that the overall risk of subsequent fatal and non-fatal strokes after a pregnancy complicated by pre-eclampsia is RR 1.81 (CI 1.45–2.27) compared to women who never developed pre-eclampsia. 75 This risk appears even greater if the woman was diagnosed with pre-eclampsia prior to 37 weeks (RR 5.08 (CI 2.09–12.35)). This has implications for counselling given to and cardiovascular screening of women who have had pre-eclampsia, particularly with regard to modifying other vascular risk factors.
Conclusion
Stroke during pregnancy has a significant maternal morbidity and mortality and may have long-lasting consequences. Pregnancy itself should not be a barrier to timely diagnosis and treatment and multidisciplinary working can ensure favourable outcomes. Despite the rising incidence of stroke it will remain rare in pregnancy and so will require the expertise of multidisciplinary specialised tertiary units which may not be co-located with hyperacute stroke units.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MC, AR and CNP are all an employee of Guy’s and St Thomas’ NHS Foundation Trust. CNP has received professional fees from Alliance Pharmaceuticals, UCB Pharmaceuticals, LEO Pharmaceuticals, Sanofi Aventis and Warner Chilcott. These do not relate to this submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not sought for this article because it is a review article.
Informed consent
Informed consent was not sought for this article because this is a review article.
Guarantor
MC
Contributorship
MC conceived the idea for the manuscript and wrote the first draft, this was reviewed and revised by CNP and AR. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Acknowledgements
None.