
Abstract
Introduction
Research has suggested that delivery is associated with an increased risk of stroke in women; however, there is a lack of contemporary estimates on the incidence of stroke in and after pregnancy compared with the baseline risk in women of childbearing age in Sweden.
Patients and methods
All women aged 15–49 years with live births/stillbirths in 1992–2011 were identified from the Swedish Medical Birth Registry linked with the National Patient Registry. First stroke during the study period was identified. Incidence rates per 100,000 person-years and adjusted incidence rate ratios (IRRs) were calculated for antepartum, peripartum and early and late postpartum periods, compared with all other available follow-up time (time before pregnancy and after postpartum) using Poisson regression adjusted for maternal age, education attainment and calendar time.
Results
Of 1,124,541 women, 3094 had a first incident stroke (331 occurred during pregnancy or first 12 weeks postpartum), about half having ischaemic stroke. The incidence was 15.0 per 100,000 person-years (95% confidence interval 14.5–15.6) in non-pregnant time. The incidence was lower antepartum (7.3/100,000 person-years, 6.0–8.9; adjusted IRR = 0.7, 0.5–0.8) but higher peripartum (314.4/100,000 person-years, 247.5–399.5; adjusted IRR = 27.3, 21.4–34.9) and early postpartum (64.0/100,000 person-years, 54.1–75.7; adjusted IRR = 5.5, 4.6–6.6). The increased risk in peripartum was more evident for intracerebral haemorrhage than other types of stroke.
Conclusion
Overall risk of stroke was low in women of childbearing age, but stroke risk peaks in the peripartum and early postpartum periods. Future work should address factors that contribute to this increased risk in order to develop approaches to attenuate risk.
Introduction
Stroke is a major cause of death and disability in Sweden and worldwide. While the risk of stroke increases with age, it is increasingly recognised that stroke also occurs in younger populations. 1 Due to the wider impacts of disability on family, children, work and society, the burden of stroke in younger people is an increasing global problem. In addition, it is widely known that pregnancy is associated with an increased risk of stroke, and a recent report detailed maternal deaths from neurological disease including stroke and subarachnoid haemorrhage (SAH). 2 There are pathophysiological reasons for increases in the risk of both ischaemic stroke (IS) and haemorrhagic stroke in pregnancy. 3 Although less common than IS, haemorrhagic stroke is relatively more common in pregnancy 4 and carries a greater risk of morbidity.5,6 In particular, hypertensive diseases of pregnancy such as pre-eclampsia/eclampsia and rupture of vascular malformations and aneurysms can lead to SAH or intracerebral haemorrhage (ICH). 7 The recent 2015 Global Burden of Disease reported hypertensive disorders of pregnancy (HDP) the second highest cause of maternal deaths behind haemorrhage. 8 The risk of venous thrombosis increases in pregnancy and this therefore could increase the risk of IS due to paradoxical emboli or cerebral venous thrombosis. 9 As well as being a prothrombotic state, pregnancy is also associated with relative hyperlipidaemia and hypertension. However, most previous literature is limited to small retrospective case series and/or has failed to distinguish risks between different time periods around pregnancy.10,11 This is crucial as risk factors and treatment may differ between time periods. Previous population-based studies from Sweden have found increased risks of stroke around delivery and in the early postpartum period; however, the studies used data between 1987 and 1995 and did not report risk for the early trimesters.12,13
In this study, we aimed to quantify incidence rates of ischaemic, ICH and SAH stroke during pregnancy and the postpartum compared with background rates among women of childbearing age in the Swedish population using more recent data. We linked the Swedish Birth Registry with over 1 million women who had deliveries between 1992 and 2011 to nationwide data on stroke obtained from the Swedish National Patient Registry (NPR).
Methods
Dataset and study population
We included all women aged 15–49 years who experienced a pregnancy ending in live birth or stillbirth between 1 January 1992 and 31 December 2011 from the Swedish Medical Birth Registry (MBR). The MBR contains information on more than 97% of deliveries occurring in Sweden with approximately 100,000 births occurring each year.14,15 The MBR has been subjected to numerous quality checks in the past, and the birth data recorded have been validated against birth data at Statistics Sweden. 14
The outcome of this study was first incident stroke during the study period. Stroke was identified from the NPR hospital inpatient data. Each resident in Sweden is assigned a personal identity number at birth or upon becoming a resident, 16 which allows the MBR data to be linked with the NPR at an individual level. 17 The NPR began in 1964 but became nationwide in 1987. The diagnoses are coded using International Classification of Disease (ICD) codes. Both ICD-10 and ICD-9 codes were used during the study period and therefore both used to extract the stroke diagnosis, regardless of its hierarchal position in the diagnostic filed (primary or secondary). Based on previous research, 12 diagnoses of stroke identified not from the primary or the first two secondary diagnoses were excluded since these were more likely to be historical events. We also included stroke events that had resulted in death and may have only been diagnosed post-mortem from the Cause of Death Registry which contains all deaths among Swedish residents. The Cause of Death Registry started in 1951–1952 and has been complete since 1961. 18 Women with stroke were classified as having IS, ICH or SAH. Women with unspecified stroke were included in a separate category. For women firstly admitted to the internal medicine clinic and then transferred to the neurology clinic within the same hospitalisation, the primary diagnosis from the neurology clinic was used to identify the stroke type.
The start of follow-up was 1 January 1992 or the woman’s 15th birthday whichever came later and the end of follow-up was 31 December 2011, the day before the woman’s 50th birthday, the date of death or emigration or the date of first stroke diagnosis whichever came earliest. Women’s follow-up time was divided into antepartum (the date of conception until three days before the date of delivery), peripartum (two days before until one day after delivery), postpartum (from two days after delivery until the end of 12 weeks postpartum) and ‘non-pregnant time’ including all other available follow-up time excluding the antepartum, peripartum and postpartum periods. The postpartum period was subdivided into individual weeks and also into early (first 6 weeks) and late (7–12 weeks) postpartum.
Statistical analysis
We assessed the rates of stroke per 100,000 person-years and 95% confidence intervals (CIs) for different time periods. We stratified the analysis by maternal age (in five-year age bands), education attainment in 2012 in five categories, calendar time (in 1992–1996, 1997–2001, 2002–2006 and 2007–2012) and different types of stroke. We calculated the incidence rate ratios (IRRs) for each pregnancy and postpartum time period using the non-pregnant time as the comparison group, with adjustment for maternal age, education attainment and calendar time. Since by using the current definition we might include women with stroke history (rather than first incident stroke), we conducted a sensitivity analysis by excluding women with stroke identified from secondary diagnoses in NPR.
The study was approved by Stockholm Ethical Review Board (Ref: 2015/1686-31/2) on 21 October 2015. The Review Board deemed that none of the participants should to be contacted due to the strict registry-based nature of the study. 18
Results
Incidence rates (per 100,000 person-years) of stroke in antepartum, postpartum and non-pregnant time (N = 1,124,541 women).
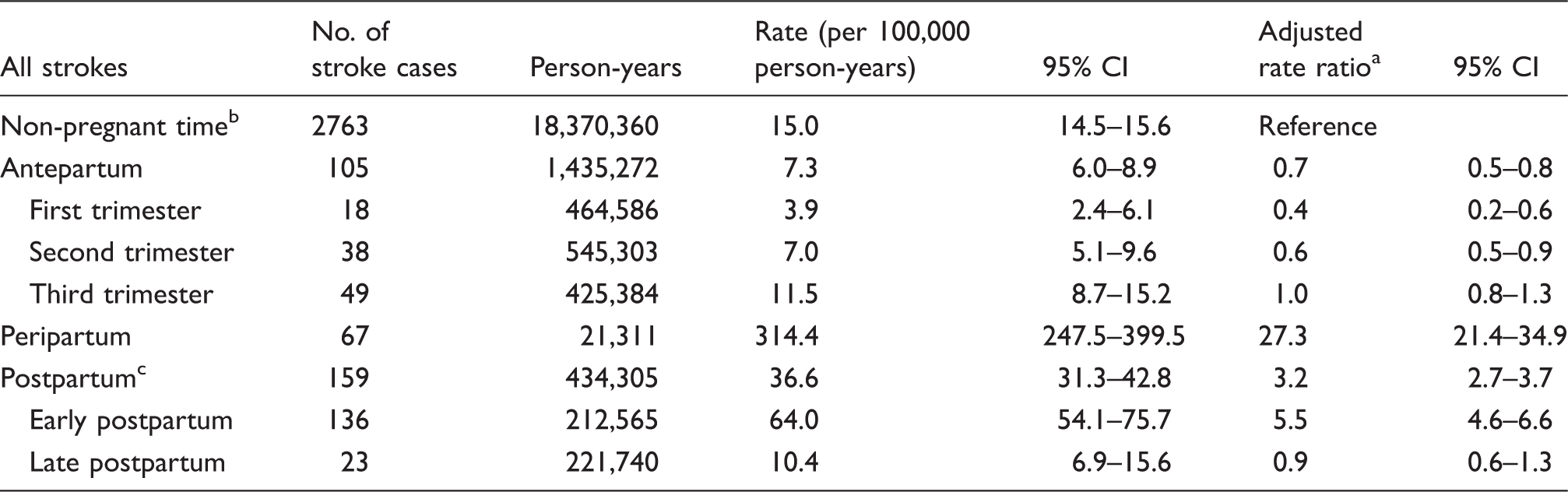
Rate ratio adjusted for maternal age, education attainment and calendar time.
Excluding the first 12 weeks postpartum.
The first 12 weeks postpartum.
Incidence rates (per 100,000 person-years) of different types of stroke in antepartum, postpartum and non-pregnant time (N = 1,124,541 women).
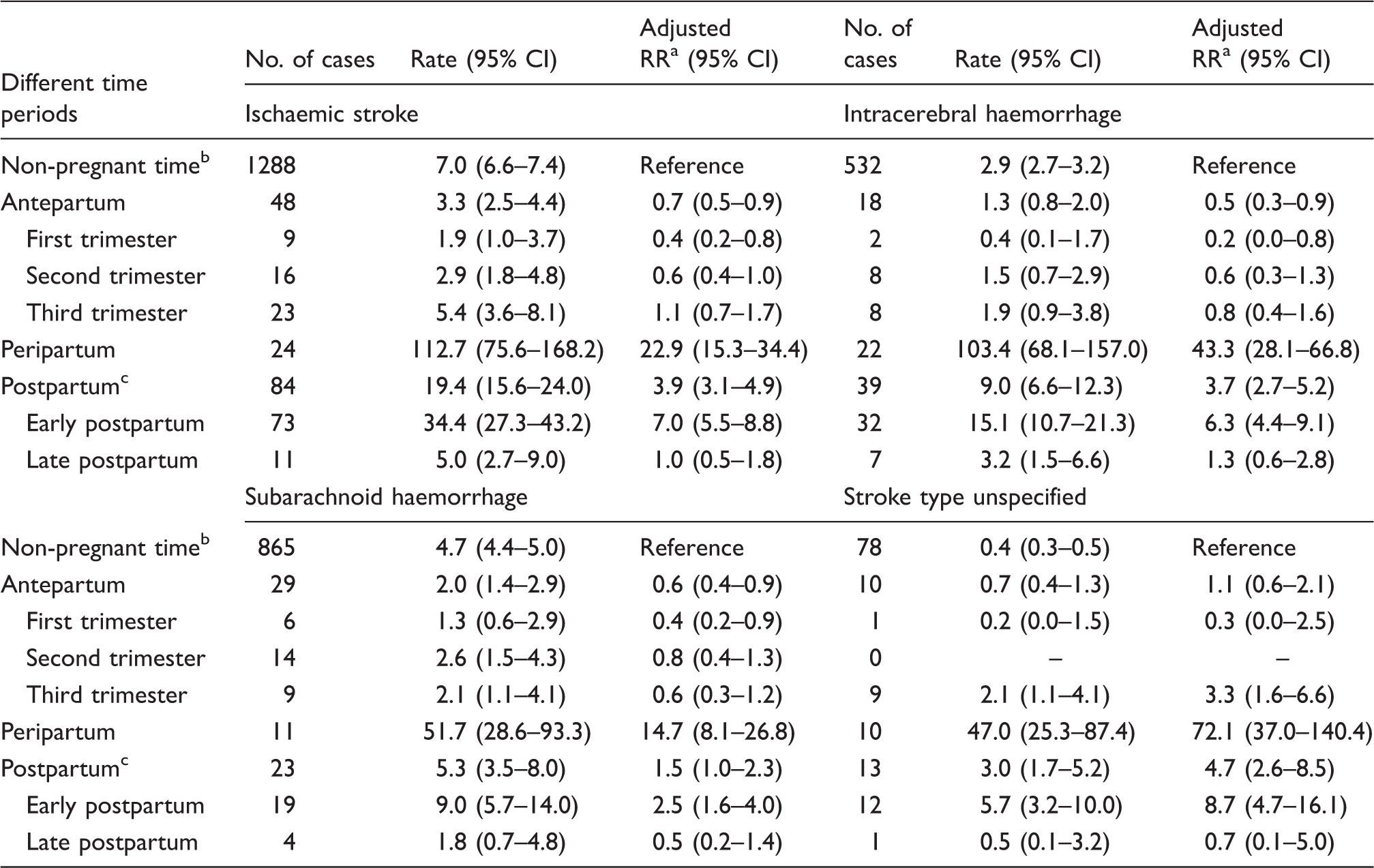
Rate ratio adjusted for maternal age, education attainment and calendar time.
Excluding the first 12 weeks postpartum.
The first 12 weeks postpartum.
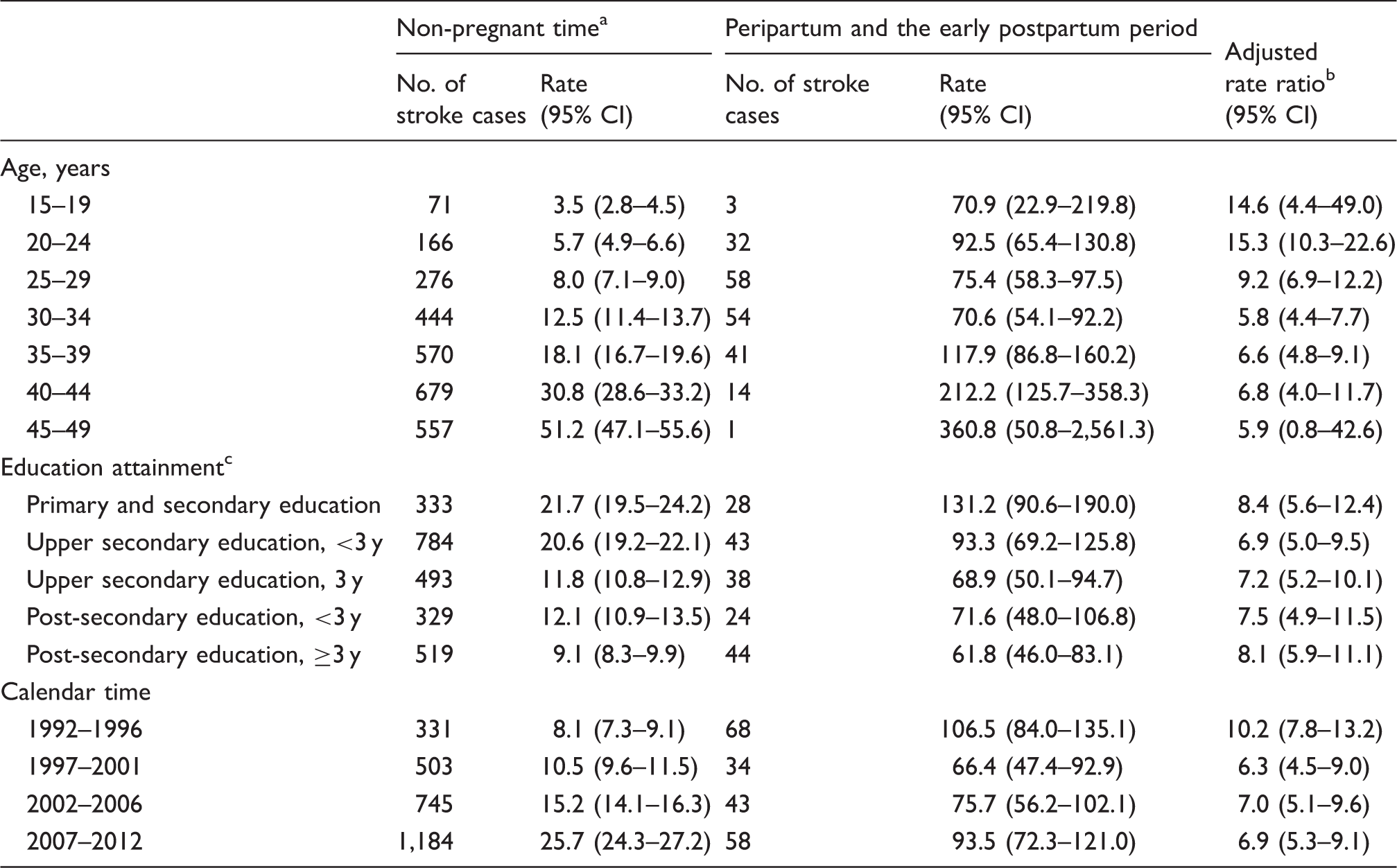
The incidence rate in the non-pregnant time increased with age and calendar time, but decreased by women’s education attainment (Figure 1 and Table 3). The pattern however was not so evident in the peripartum or the early postpartum period (Figure 1 and Table 3). Compared to the non-pregnant time, the incidence rates of stroke in the peripartum and the early postpartum periods were consistently higher across all different groups (Table 3).
Incidence rates (per 100,000 person-years) of stroke by age (women<20 or ≥40 years old were excluded since there were few stroke cases in pregnant-related time periods). Incidence rates (per 100,000 person-years) of stroke in pregnant and non-pregnant time by maternal age, education attainment and calendar time. Excluding the first 12 weeks postpartum. Rate ratio mutually adjusted for maternal age, education attainment and calendar time. 37,709 (3.4%) women with missing information.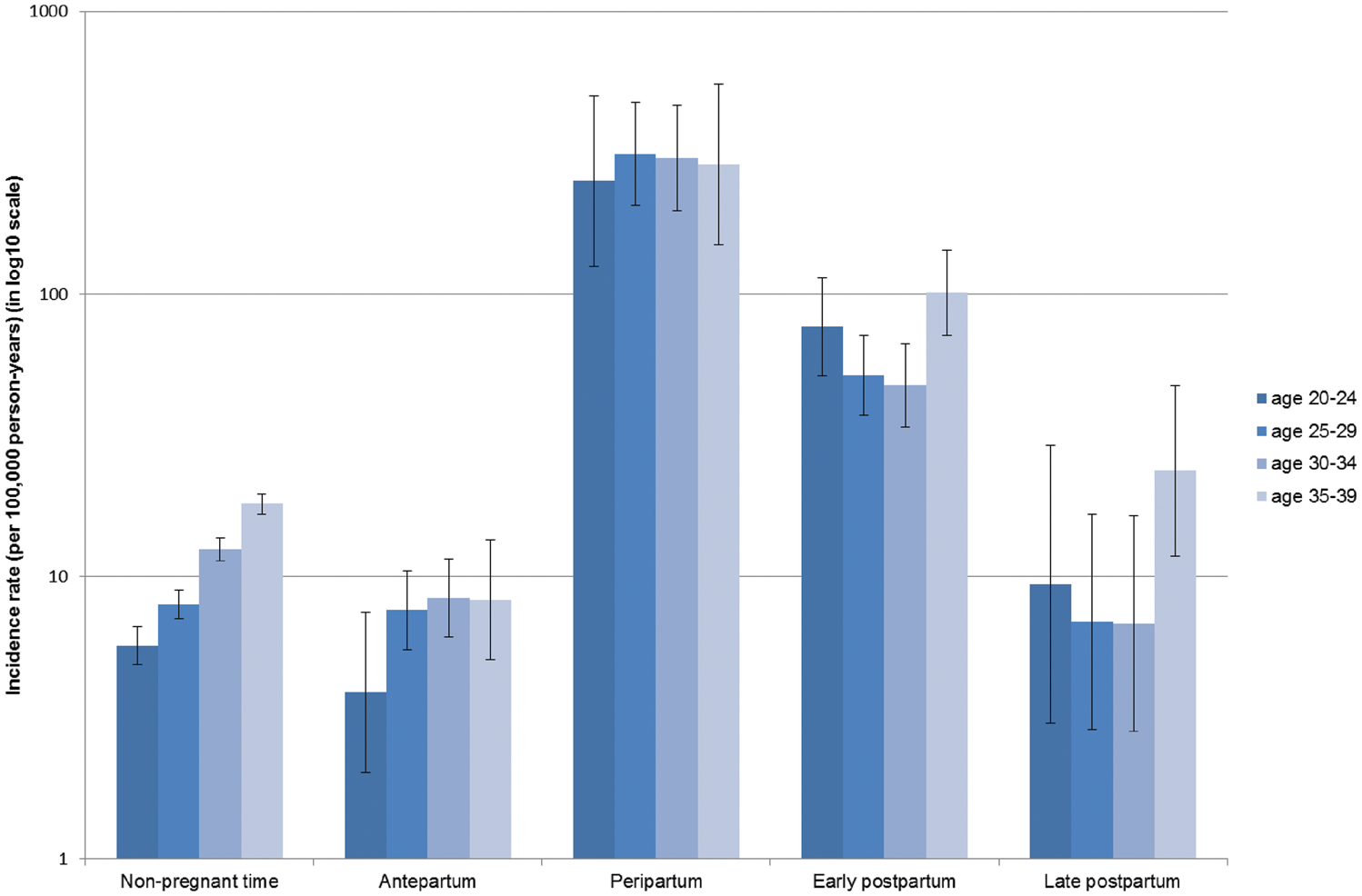
In the sensitivity analysis, we excluded 518 women with incidence of stroke identified from secondary diagnoses. The overall incidence rate of stroke decreased considerably, especially in peripartum (112.6 per 100,000 person-years, 95% CI 75.5–168.1), but the rate was still higher compared to the non-pregnant time (adjusted IRR = 11.3, 95% CI 7.5–16.9).
Discussion
In this nationwide population-based study of more than 1 million pregnant women, we identified around 3000 stroke episodes, of which 331 occurred in pregnancy or the first 12 weeks postpartum. This is equal to approximately 17 women with stroke per 100,000 deliveries. The highest incidence rates were seen during the days around delivery, consistent with earlier data. 12 This pattern was seen across all ages, calendar time periods and education levels, although we noted lower absolute risks in highly educated women.
Overall, the absolute rate of stroke has increased over calendar years. This is in line with data in Sweden that show the rate of stroke increasing in young people. 19 However, the relative rate of stroke around delivery or early postpartum seems to have decreased after early 1990s. In addition, compared with previous research in Sweden, 12 we found fewer episodes of ICH around the time of delivery, but more episodes of IS. This reduction may relate to improvements in antenatal care, for example, highlighting the need for aggressive treatment of blood pressure to prevent stroke in pre-eclampsia. 9 However, caution is needed when interpreting comparisons with previous data, as the recent change from ICD-9 to ICD-10 may have implications on stroke subtyping.
One of the major strengths of our paper is our population-based study design. We used the MBR to define stroke in relation to pregnancy. The registry has high-quality 15 data that are collected by dedicated antenatal midwives/nurses. The large number of pregnant women, and with that the large number of stroke outcomes, allowed us to calculate precise estimates with narrow confidence intervals. Furthermore, it allowed us to examine subgroups of pregnant women and also specific outcomes such as IS, ICH and SAH. This is important as different forms of stroke have different risk factors and hence different temporal patterns in relationship to delivery. In addition, we included women up until 2012, and the latest calendar period encompassed the period 2007–2012. Our data therefore represent modern-day management of pregnancy.
The Swedish NPR was used to identify stroke diagnosis. When the validity of this registry was evaluated, the positive predictive values of most diagnoses were between 85% and 95%. 17 The NPR also has a high sensitivity for stroke. In a comparison with the National Quality Registry for stroke, 20 the NPR identified 96% of all stroke incidents, 17 and when Stegmayr and Asplund 21 examined 3732 cases of non-fatal strokes, 3492 (93.6%) were identified in the NPR. 21 This is important as it means we are unlikely to have underestimated the incidence risk of stroke.
Through the unique personal identity number assigned to all residents in Sweden, we were able to add other data, including education attainment. This is important, as stroke has been linked to socioeconomic status as many risk factors are more prevalent with increased deprivation, and our study did find a lower risk of stroke among highly educated women. Our results are in agreement with others who have confirmed that stroke risk is independently related to education. 22 However, medical termination of pregnancy and spontaneous abortion are not routinely recorded in the MBR and therefore not available for our study. Some of these early ending of pregnancy may be related to a stroke, and consequently, the true incidence of stroke during early pregnancy could have been underestimated.
Given the substantial increased risk of stroke around the time of delivery, it is imperative that health professionals are aware of this risk in order that stroke may be recognised and optimally treated. Future research should investigate potential causative factors to enable focus on prevention strategies to reduce this hazard. Unfortunately, we were not able to study co-morbidities and risk factors other than age and education in this study. These would include traditional cardiovascular risk factors such as hypertension, smoking, hyperlipidemia, diabetes and obesity, but should also include factors related to pregnancy such as pre-eclampsia, thrombophilia and delivery. This would be important in future research, as it would have implications for targeted prevention approaches.
A systematic review assessing the accuracy of utilising registry coding for stroke in epidemiological studies concluded that linking hospital registers with other data sets, such as primary care, would yield additional information and increase quality but is seldom performed. 23 Unfortunately, we did not have access to primary care data. In addition, despite the markedly increased risk of stroke around delivery, most strokes in these young women were unrelated to pregnancy. Assessment of risk factors and primary prevention programs are needed to halt the worrying trend of increased risk of stroke in young people.
In conclusion, this population-based study found that risk of stroke was increased significantly at the time of delivery and in the early postpartum period. Future work should address the multiple factors that may contribute to this increased risk in order to develop appropriate approaches to attenuate the risk.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CNP has received consultancy fees from Alliance Pharmaceuticals, UCB and lecturing fees from UCB, Sanofi and Leo-Pharma. There are no other conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: LB received funding from the University of Nottingham to visit the Karolinska Institutet where the data management and analysis were conducted. OS was supported by the Swedish Research Council (grant 2013-2429). PMB is Stroke Association Professor of Stroke Medicine, and is a National Institute of Health Research Senior Investigator.
Ethical approval
The study was approved by Stockholm Ethical Review Board (Ref: 2015/1686-31/2) on 21 October 2015.
Informed consent
Not applicable.
Guarantor
JFL.
Contributorship
LJT, LB, NS, AAS, CNP, PMB, OS and JFL contributed to conception and design of the study. LB and AAS contributed to data management and analysis of the study. NS, CNP, JFL and LB drafted the manuscript and LB, NS, AAS, CNP, PMB, OS, LTJ and JFL commented and edited the manuscript. All authors read and approved the final version. JFL supervised the study and is guarantor.