CT ANGIOGRAPHY DELAYS GROIN PUNCTURE IN MECHANICAL THROMBECTOMY FOR LARGE VESSEL OCCLUSION IN STROKE
K. Atchaneeyasakul1, A. Tipirneni1, P. Khandelwal1, V. Saini1, R. Ronca1, S. Lord1, K. Ramdas1, L. Guada Delgado1 and D. Yavagal1
1University of Miami Miller School of Medicine, Neurology, Miami, USA
Abstract
Background: Thrombectomy in proximal anterior circulation occlusions has shown significant improvement in functional outcome over tPA alone. Recent trials have utilized CT angiography(CTA) for vascular imaging immediately following non-contrast CT(NCCT).Thin section NCCT with automated MIP reconstructions has high accuracy in showing occluding thrombus. However, multiple imaging modalities may delay time to groin puncture(GP).We hypothesized that CTA after NCCT increases time to GP compared to thin section NCCT alone.
Methods: This is a retrospective cohort study of consecutive patients receiving thrombectomy for anterior circulation occlusions at our tertiary-care academic medical center. All stroke NCCTs are thin section(0.625 mm) with software automated maximal intensity projection(MIP) reconstructions available within 2 minutes of CT images. When “hyperdense sign” was seen on thin section MIPs in anterior circulation, physician may forgo CTA and bring patient directly to angiography suite. We excluded all transfer patients, in-hospital stroke, and receiving stroke imaging other than NCCT or CTA prior to thrombectomy. NCCT-CTA and NCCT groups were compared for time from initiation of NCCT to GP(tNCCT-GP) and total imaging time prior to GP(tIMAGING).Time from imaging completion to GP was included in multivariate analysis as potential confounder increasing tNCCT-GP.
Results: From March 2008 through August 2015,289 patients underwent thrombectomy with 56 patients meeting inclusion/exclusion criteria(24 NCCT,32 NCCT-CTA group).tIMAGING was significantly lower in the NCCT group compared to NCCT-CTA group,3.2 ± 1.4vs56.9 ± 14.1 min (p < 0.001).Multivariate analysis showed significantly lower tNCCT-GP in NCCT only group,100 ± 22.1vs124.8 ± 16.1 min (p < 0.001).
Conclusions: Performing CTA after NCCT prior to thrombectomy does significantly delay time to groin puncture. Selecting LVO patients with thin section NCCT with MIPs showing hyperdense sign may significantly save time, brain, and further improve outcomes.
AS17-014
ACUTE ENDOVASCULAR TREATMENT: BEYOND THE TRIALS
Oral
IMPACT OF COMPLETE REPERFUSION (TICI 3) COMPARED TO NEAR COMPLETE REPERFUSION ON CLINICAL OUTCOME IN CAROTID-SYLVIAN ACUTE ISCHEMIC STROKE TREATED WITH MECHANICAL THROMBECTOMY
C. Dargazanli1, M. Barral1, B. Lapergue2, H. Redjem1, J.P. Desilles1, G. Ciccio1, S. Smajda1, P. Guedin3, P. Paraschakis1, H. Takezawa1, G. Rodesch3, R. Blanc1 and M. Piotin1
1Rothschild Foundation Hospital§, Interventional Neuroradiology, PARIS, France
2Foch Hospital, Neurology, Suresnes, France
3Foch Hospital, Neuroradiology, Suresnes, France
Abstract
Background: Successful reperfusion is a major predictor of good outcome following endovascular therapy for acute large vessel occlusions. Recent studies demonstrating the efficiency of mechanical thrombectomy considered TICI 2b (near-complete reperfusion) and TICI 3 (complete reperfusion) as technical success. The objective of this study was to compare the outcomes of patients with final TICI 2b and TICI 3 reperfusion status.
Methods: Data were extracted from a bicentric prospective register of consecutive patients treated by intravenous and/or mechanical thrombectomy for acute cerebral infarct between January 2012 and January 2015.
Inclusion criteria were: 1. MCA M1 or M2 segment and/or ICA occlusion, confirmed on cerebral MRI; 2. Mechanical thrombectomy achieving TICI 2b or TICI 3 reperfusion status. Baseline characteristics (age, NIHSS score, time to reperfusion, procedure time, ASPECTS, risk factors), rate of good outcome (mRS 0–2) and rate of very good outcome (mRS 0–1), intracranial haemorrhage and mortality were assessed. Patients with large ischemic score (DWI-ASPECTS < 6) were excluded.
Results: 199 patients (TICI 2b, N = 98, TICI 3, N = 101, Median NIHSS 15, median ASPECTS 8) were included. No differences in baseline characteristics were identified. Patients with TICI 3 status had higher rate of good outcome (73% vs 52%, p = 0.002), higher rate of very good outcome (61% vs 40%, p = 0.002), and lower haemorrhage rates (p = 0.003) as compared to TICI 2b.
Conclusions: Patients with TICI 3 reperfusion have better clinical outcomes as compared to TICI 2b. These results suggest to analyse TICI 2b and TICI 3 status separately in further studies focusing on thrombectomy efficiency.
AS09-017
ACUTE ENDOVASCULAR TREATMENT: BEYOND THE TRIALS
Oral
CLINICAL OUTCOMES IN ACUTE STROKE PATIENTS TREATED WITH MECHANICAL THROMBECTOMY: COMPARISON BETWEEN SOLUMBRA AND ADAPT TECHNIQUES
J. Delgado Almandoz1, Y. Kayan1, M. Young2, J. Fease1, J. Scholz1, A. Milner1, T. Hehr2, P. Roohani2, M. Mulder3 and R. Tarrel2
1Abbott Northwestern Hospital, Division of Neurointerventional Radiology, Minneapolis, USA
2Abbott Northwestern Hospital, Division of Vascular Neurology, Minneapolis, USA
3Abbott Northwestern Hospital, Division of Critical Care Medicine, Minneapolis, USA
Abstract
Background: Although the recently published randomized controlled trial results validated the use of intra-arterial (IA) therapy in combination with IV-tPA, the relative safety and efficacy of the different IA treatment modalities used in these stroke trials remained uncertain. The goal of this study was to compare the incidents of symptomatic intracranial hemorrhage (sICH) and good clinical outcome in a stroke cohort with emergent large vessel occlusions (ELVO) in the anterior circulation treated with either Solumbra or A Direct Aspiration first-Pass Thrombectomy (ADAPT) technique.
Methods: Baseline and procedural characteristics, clinical outcomes and safety were compared in subjects treated using Solumbra or ADAPT over a 38-month period. sICH was defined by the SITS-MOST criteria. Good clinical outcome was defined by modified Rankin Scale scores of 0–2 at 90 days.
Results: One hundred patients met study criteria, 55 with Solumbra and 45 with ADAPT. ADAPT patients presented with a higher mean NIHSS (19.2 vs 16.8, p = 0.02) and a greater number of internal carotid artery terminus occlusions than Solumbra patients (42.2% vs 20%, p = 0.03). Post-procedure, the ADAPT cohort tended to have a lower sICH rate than the Solumbra cohort (2.2% vs 12.7%, p = 0.07). Furthermore, ADAPT patients had better good clinical outcomes than Solumbra patients (55.6% vs 30.9%, p = 0.015). Use of ADAPT was an independent predictor of good clinical outcome at 90 days (OR 6 [95% CI 1.0 to 31.2], p = 0.049).
Conclusions: In this study, patients with stroke from anterior circulation ELVOs treated with ADAPT were associated with better clinical outcomes than those treated with Solumbra.
AS09-022
ACUTE ENDOVASCULAR TREATMENT: BEYOND THE TRIALS
Oral
ENDOVASCULAR THERAPY FOR ISCHAEMIC STROKE: SAVE A MINUTE - SAVE A WEEK
A. Meretoja1, M. Keshtkaran2, T. Tatlisumak3, G. Donnan4 and L. Churilov4
1Helsinki University Hospital, Department of Neurology, Helsinki, Finland
2RMIT University, School of Mathematical and Geospatial Sciences, Melbourne, Australia
3University of Gothenburg, Institute of Neuroscience and Physiology- Sahlgrenska Academy, Gothenburg, Sweden
4University of Melbourne, The Florey Institute of Neuroscience and Mental Health, Parkville, Australia
Abstract
Background: Achieving recanalisation in ischaemic stroke is highly time-critical, but long-term consequences of small reductions in endovascular treatment delays have not been reported. Our objective was to quantify the patient lifetime benefits gained from faster endovascular therapy.
Methods: We used observational prospective data of consecutive stroke patients treated with intravenous thrombolysis in Helsinki (1998 to September 2014; n = 2474) to provide distributions of age, sex, stroke severity, onset-to-treatment times, and 3-month modified Rankin Scale (mRS) in daily clinical practice. We applied treatment effects by time of endovascular therapy in large vessel occlusion over and above thrombolysis as reported by the MR-CLEAN study to model the shift in 3-month mRS distributions with reducing treatment delays, from which we derived the expected lifetime and level of long-term disability with incrementally faster treatment.
Results: Each minute reduction in onset-to-treatment time granted on average 4.2 days of extra healthy life, with a 95% prediction interval of 2.3 to 5.4. Women gained slightly more than men over their longer lifetimes. Patients less than 55 years of age with severe strokes of NIHSS above 10 gained more than a week of healthy life for each minute saved, or more than a year for every hour.
Conclusions: Realistically achievable small reductions in endovascular delays lead to significant and robust health benefits over patients’ lifetimes. Services need to be optimized to reduce all delays in endovascular therapy.
AS07-037
ACUTE ENDOVASCULAR TREATMENT: BEYOND THE TRIALS
Oral
VALUE OF NIHSS ITEM PROFILES AND PREHOSPITAL STROKE SCALES TO IDENTIFY PATIENTS WITH LARGE ANTERIOR VESSEL OCCLUSION DESPITE MODERATE STROKE SEVERITY - RESULTS FROM SITS-ISTR
J.F. Scheitz1, A.H. Abdul-Rahim2, R.L. MacIsaac2, C. Cooray3, H. Sucharew4, D.O. Kleindorfer4, P. Khatri4, J. Broderick4, H.J. Audebert1, N. Ahmed3, N. Wahlgren3, M. Endres1, C.H. Nolte1 and K.R. Lees2
1Charité - Campus Benjamin Franklin, Neurology, Berlin, Germany
2Stroke Research- Institute of Cardiovascular & Medical Sciences, University of Glasgow, Glasgow, United Kingdom
3Karolinska Institutet, Department of Clinical Neurosciences and Department of Neurology, Solna, Sweden
4UC Neuroscience Institute, Neurology and Rehabilitation Medicine, Cincinnati, USA
Abstract
Background: The National Institutes of Health Stroke Scale (NIHSS) is routinely used to select ischemic stroke patients for urgent neurovascular imaging to detect large anterior vessel occlusion (LAVO). However, the selection criteria based on current recommended cut-points of the NIHSS sum score may discriminate against patients with moderate stroke severity. We aimed to assess the associations of NIHSS item profiles and simplified NIHSS scores with the presence of LAVO in patients with moderate stroke.
Methods: Data from the Safe Implementation of Thrombolysis in Stroke International Stroke Thrombolysis Registry (2010-May 2014) were analyzed retrospectively. Patients with moderate stroke severity (NIHSS 6–11), who had complete breakdown of NIHSS scores and status of LAVO (internal carotid artery, carotid-terminus or M1 segment of the middle cerebral artery) were included. We assessed the association of NIHSS item profiles and prehospital stroke scales with LAVO.
Results: Among 2820 patients with moderate stroke, 6.3% (n = 178) had LAVO. There were two NIHSS item profiles representing total anterior circulation syndromes that had a 5–6-fold increased risk of LAVO compared to a non-specific clinical profile. Simplified NIHSS scores performed as well as the full NIHSS for detection of LAVO. Abnormal findings on all three FAST items identified LAVO with high sensitivity. Addition of abnormal gaze to FAST and high scores on prehospital stroke scales showed increased specificity.
Conclusions: In patients with moderate stroke severity, the NIHSS item profiles and simplified NIHSS scores may help to stratify patients’ risk of LAVO and to identify individuals who deserve urgent neurovascular imaging and consideration for thrombectomy.
AS09-038
ACUTE ENDOVASCULAR TREATMENT: BEYOND THE TRIALS
Oral
MECHANICAL THROMBECTOMY WITH THE EMBOLUS RETRIEVER WITH INTERLINKED CAGES IN ACUTE ISCHAEMIC STROKE: ERIC, THE NEW BOY IN THE CLASS
H. Steglich-Arnholm1, D. Kondziella1, A. Wagner2, M.E. Cronqvist2, K. Hansen1, T.C. Truelsen1, L.H. Krarup1, J.L. Højgaard1, S. Taudorf1, H.K. Iversen1, D.W. Krieger3 and M. Holtmannspötter2
1Rigshospitalet, Department of Neurology, Copenhagen, Denmark
2Rigshospitalet, Department of Neuroradiology, Copenhagen, Denmark
3Dubai Healtcare City, Clinic 2006, Dubai, United Arab Emirates
Abstract
Background: Introduction of the stent-retriever design was essential for the positive results of the recent randomized controlled thrombectomy trials in acute ischaemic stroke. However, further improvements in device designs could improve recanalization rates and reduce adverse events in more patients. The Embolus Retriever with Interlinked Cages (ERIC®) device is a novel and improved stent-retriever.
This study aims to compare the rates of recanalization, favourable clinical outcome, and procedural adverse events between the ERIC®-device and older stent-retrievers.
Methods: Retrospective single-centre propensity score matched analysis of patients treated between 2012 and 2015. From 257 patients treated with thrombectomy 231 patients were included in this study and 26 were excluded because of incomplete follow-up or missing data. Mean age was 68 years (±13), mean baseline NIHSS was 16 (±5), 128 (55%) were male, and ERIC® was used as the primary thrombectomy device in 42 (24%) patients. Patients were matched 1:1 for age, baseline NIHSS, anaesthetic management, and Charlson Comorbidity Index score.
Results: Preliminary analysis of 38 matched pairs suggests that patients treated with the ERIC®-device compared to older stent-retrievers had equal rates of recanalization (89% vs 74%, P = 0.074) and favourable clinical 3-months outcome (mRS0–2: 53% vs 32%, P = 0.063), and shorter groin-puncture-to-recanalization time (51 minutes vs. 80 minutes, P = 0.001), fewer thrombectomy passes (2.6 vs. 3.6, P = 0.026) and lower rate of procedural adverse events (21% vs. 42%, P = 0.048).
Conclusions: This study suggests that the ERIC®-device could improve procedural benchmarks compared to older stent-retrievers with at least equal rates of recanalization and 3-months clinical outcome.
AS09-041
ACUTE ENDOVASCULAR TREATMENT: BEYOND THE TRIALS
Oral
CLOT BURDEN SCORE: A MEANS FOR PATIENT SELECTION?
K.M. Treurniet1, O.A. Berkhemer1,2, H.F. Lingsma3, P.S.S. Fransen2, D. Beumer4, L.A. van den Berg5, W. van Zwam6, A. van der Lugt7, R.J. van Oostenbrugge4, Y.B.W.E.M. Roos5, D.W.J. Dippel2, H.A. Marquering1,8 and C.B.L.M. Majoie1
1Academic Medical Center- University of Amsterdam, Radiology, Amsterdam, Netherlands
2Erasmus Medical Center, Neurology, Rotterdam, Netherlands
3Erasmus Medical Center, Public Health, Rotterdam, Netherlands
4Maastricht University medical Center, Neurology, Maastricht, Netherlands
5Academic Medical Center- University of Amsterdam, Neurology, Amsterdam, Netherlands
6Maastricht University medical Center, Radiology, Maastricht, Netherlands
7Erasmus Medical Center, Radiology, Rotterdam, Netherlands
8Academic Medical Center- University of Amsterdam, Biomedical Engineering & Physics, Amsterdam, Netherlands
Abstract
Background: A lower clot burden score (CBS) is known to be associated with unfavourable outcome after acute ischemic stroke (AIS). The goal of this study was to assess whether CBS can aid in the identification of patients who will benefit from intra-arterial treatment (IAT) compared to usual care alone.
Methods: For all patients in the MR CLEAN study the CBS was determined. Patients without a CT Angiogram (CTA) were excluded. Univariate and multivariate ordinal logistic regression were used to assess the association between CBS (continuous or dichotomized (>6)) and modified Rankin Scale (mRS). Clinical baseline characteristics were included in the multivariate model. The odds ratios (OR) express the odds of improving one step on the mRS for each unit increase of the CBS. Models with and without an interaction term between CBS and treatment allocation were compared using the chi-square test to assess treatment effect modification by CBS.
Results: One patient was excluded because of the absence of baseline CTA. In the remaining cohort (n = 499) a higher CBS was statistically significantly associated with an improvement on the mRS, both on univariate (OR: 1.11, 95% CI 1.04–1.18, dichotomized OR: 1.67, 95%CI 1.13–2.48) and multivariate analysis (aOR: 1.12, 95% CI: 1.04–1.20, dichotomized aOR 1.67, 95% CI 1.12–2.51). No interaction was found between treatment allocation and continuous or dichotomized CBS (p-values: 0.60 and 0.18 respectively).
Conclusions: A higher CBS is associated with favourable outcome after AIS. CBS does not influence the efficacy of IAT.
AS01-058
ACUTE ENDOVASCULAR TREATMENT: BEYOND THE TRIALS
Oral
TOWARDS PERSONALIZED TREATMENT CHOICE IN INTRA-ARTERIAL TREATMENT FOR ACUTE ISCHEMIC STROKE: DEVELOPMENT OF A CLINICAL DECISION AID
E. Venema1, M. Mulder2, H. Lingsma1, B. Roozenbeek2, O. Berkhemer3, E. Steyerberg1, Y. Roos4, R. van Oostenbrugge5, W. van Zwam6, C. Majoie3, A. van der Lugt7 and D. Dippel2
1Erasmus University Medical Center, Public Health, Rotterdam, Netherlands
2Erasmus University Medical Center, Neurology, Rotterdam, Netherlands
3Academic Medical Center, Radiology, Amsterdam, Netherlands
4Academic Medical Center, Neurology, Amsterdam, Netherlands
5Maastricht University Medical Center, Neurology, Maastricht, Netherlands
6Maastricht University Medical Center, Radiology, Maastricht, Netherlands
7Erasmus University Medical Center, Radiology, Rotterdam, Netherlands
Abstract
Background: Although intra-arterial treatment (IAT) proved to be overall beneficial in patients with acute ischemic stroke (AIS), heterogeneity of baseline risk and treatment effect can cause clinically relevant differences in absolute benefit.
Methods: We used the MR CLEAN trial data (n = 500) to identify characteristics that predict outcome (modified Rankin Scale (mRS) at 90 days after stroke) or treatment effect, using ordinal regression. Variables with a multivariable P-value <0.15 (main effect or interaction with treatment) were included in the final model. Internal validation was performed with bootstrapping and model performance was expressed as area under the curve (AUC).
Results: Eight variables were included in the final model, including age (OR 0.96 per year, p < 0.0001), NIHSS score at baseline (OR 0.93 per point, p < 0.0001), time from onset to randomization (OR 0.85 per hour delay, p = 0.0196) and CTA collateral score (OR 1.44, p = 0.0056). The internally validated AUC of the model was 0.732. Table 1 illustrates an example of two patients, with their predicted probabilities on favorable outcome (mRS score 0–2) with and without IAT. For patient 1 the model predicts no benefit of IAT, while for patient 2 the expected benefit is very large.
Conclusions: The presented model predicts absolute benefit of IAT for individual patients and - after external validation - can be used as a decision aid for personalized management in AIS.
AS21-056
ACUTE ENDOVASCULAR TREATMENT: BEYOND THE TRIALS
Oral
PERFORMING CT ANGIOGRAPHY IMMEDIATELY AFTER NCCT IS ASSOCIATED WITH SHORTER TIME TO STROKE INTERVENTION
O. Zaidat1, B. Mehta2, A. Yoo3, R. von Kummer4, P. Khatri5, R. Gupta6, D. Lopes7, D. Frei8, H. Shownkeen9, D. Meyer10, V. Bach10, H. Buell10, S. Kuo10, A. Bose10, S.P. Sit10 and J. Mocco11
1St Vincent Mercy Hospital, Endovascular Neurosurgery, Toledo, USA
2Memorial Neuroscience Center, Neuroradiology, Hollywood, USA
3Texas Stroke Institute, Neuroradiology, Plano, USA
4Universitätsklinikum Carl Gustav Carus, Neuroradiology, Dresden, Germany
5University of Cincinnati, Neurology, Cincinnati, USA
6WellStar Health System, Neuroradiology, Marietta, USA
7Rush University, Neurosurgery, Chicago, USA
8Swedish Medical Center, Neuroradiology, Englewood, USA
9Central DuPage Hospital, Neuroradiology, Winfield, USA
10Penumbra Inc., Clinical Affairs, Alameda, USA
11Mount Sinai Health System, Neurosurgery, New York, USA
Abstract
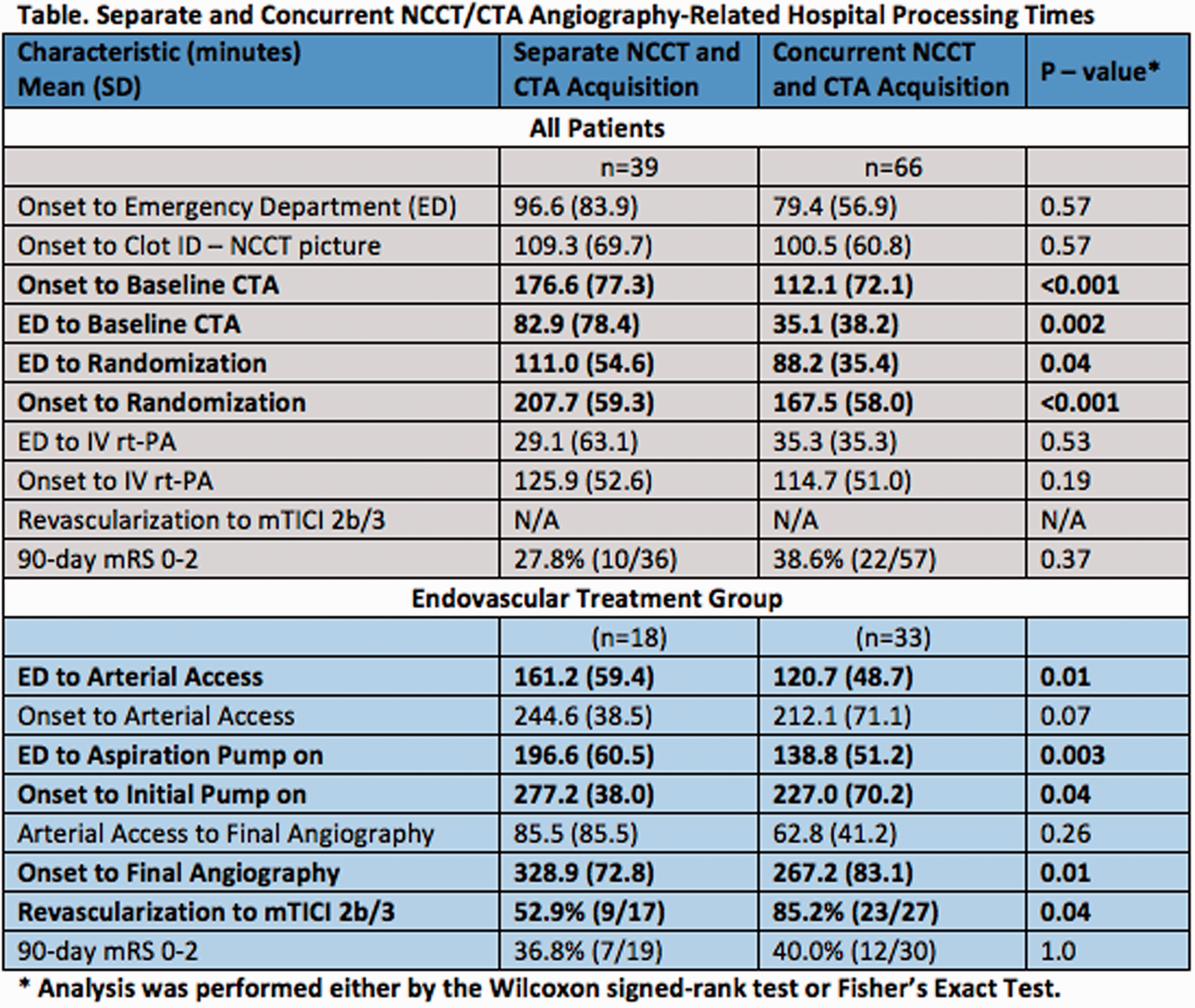
Background: CT angiography (CTA) is a critical test for identifying large vessel occlusions amenable to intra-arterial therapy (IAT). However, it is uncertain whether CTA performed immediately after NCCT delays IV rtPA in eligible patients. Herein are analysis of hospital workflow times in centers conducting separate and concurrent CTA and NCCT imaging to examine whether the schedule of imaging prolongs time to IV rtPA or delays IAT initiation.
Methods: The multicenter THERAPY trial randomized patients to either combined endovascular therapy or IV rtPA monotherapy. Centers enrolled were asked to identify their standard Emergency Department process as either 1) concurrent NCCT and CTA imaging or 2) NCCT with postponed acquisition of CTA. Times associated with each process from admission to reperfusion were analyzed and compared between the two groups.
Results: Analysis of present data yielded 105 patients treated across 36 centers. Sixty-six patients received concurrent imaging across 22 centers while 39 patients received separate NCCT and CTA imaging at 13 centers. In patients with concurrent NCCT and CTA, a statistically significant mean reduction from arrival to puncture of roughly 40 minutes (p = 0.01) and to aspiration of 60 minutes (p = 0.003) was observed in comparison to patients with separate imaging. There was no significant difference in the time from door to IV rtPA (Table).
Conclusions: Concurrent CTA and NCCT imaging was associated with improved time to IAT, without a significant delay in the delivery of IV rtPA. Study results support having concurrent CTA and NCCT imaging, potentially to increase efficiency and reduce downstream delays, leading to faster reperfusion.
URIC ACID THERAPY IN STROKE PATIENTS TREATED WITH MECHANICAL THROMBECTOMY: AN EXPLORATORY ANALYSIS OF THE URICOICTUS TRIAL
Á. Chamorro1, S. Amaro1, M. Castellanos2, L. San Román1, M. Gomis3, J. Blasco1, X. Urra1, J. Arenillas4, R. Muñoz5, D. Cánovas6, J. Marti-Fabregas7, J. Macho1 and E. Cobo8
1Hospital Clínic, Neurosciences Stroke Comprehensive Center, BARCELONA, Spain
2SERGAS, Neurology, A Coruña, Spain
3Hospital Germans Trias i Pujol, Neuroscience, Badalona, Spain
4Hospial Clinico, Neurology, Valladolid, Spain
5Hospital de Navarra, Neurology, Pamplona, Spain
6Hospital PArc Taulí, Neurology, Sabadell, Spain
7Hospital Santa Creu i Sant PAu, Neurology, Barcelona, Spain
8Campus Nord UPC, Statistics, Barcelona, Spain
Abstract
Background: We explored the effects of uric acid (UA) therapy in stroke patients treated with mechanical thrombectomy in the URICOICTUS Trial (NCT00860366).
Methods: Of 411 patients included in the Trial, 45 received mechanical thrombectomy because a CT-angiogram showed persistence of a proximal vessel occlusion following alteplase administration. In this subgroup, we compared the proportion of good functional outcome at 90 days (modified Rankin Score 0 to 2), full independence at 90 days (Barthel Index score 95 to 100), ischemic worsening during the first 72 hours, mortality at 90 days, and risks of intracerebral bleeding between the patients allocated to UA (n = 24) or placebo (n = 21).Adjusted odds ratios and 95% confidence intervals were estimated using logistic regression models adjusted by the stratification factors and baseline traits
Results: Good outcome was observed in 16 patients (67%) receiving UA, and in ten (48%) receiving placebo (adjusted odd ratio 6•12 [95% CI 1•06–34•56]. There were statistically significant differences between treatment groups with respect to full independence (16 [67%] patients who received UA vs nine [43%] who received placebo) (adjusted odd ratio 9.20 [95% CI 1•53–55•20], and ischemic stroke worsening within 72 hours (none [0%] vs four [19%]). No clinically relevant or statistically significant differences were reported between groups with respect to death (four [17%] patients who received UA vs four [19%] who received placebo), or symptomatic intracerebral hemorrhage (one [4%] vs none [0%]).
Conclusions: UA therapy was safe and more effective than placebo to improve functional outcome and daily living activities in stroke patients treated with mechanical thrombectomy.
OCCURRENCE AND CHARACTERISTICS OF INFARCT IN A NEW TERRITORY (INT) IN THE ESCAPE TRIAL OF ENDOVASCULAR STROKE TREATMENT
A. Ganesh1,2, M. Goyal1,3, M.D. Hill1,4, A. Demchuk1,3, M. Eesa1,3, B. Menon1,3,4 and O.B.O. the ESCAPE Trialists1
1University of Calgary, Calgary Stroke Program- Department of Clinical Neurosciences, Calgary, Canada
2University of Oxford, Centre for Prevention of Stroke and Dementia- Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
3University of Calgary, Department of Radiology, Calgary, Canada
4University of Calgary, Department of Community Health Sciences, Calgary, Canada
Abstract
Background: Infarct in a New Territory (INT) is a complication associated with endovascular procedures that has not been consistently reported in trial literature. We applied a recently-proposed methodology to identify and classify INTs in the ESCAPE trial of endovascular stroke treatment.
Methods: 151 patients in the interventional arm of ESCAPE underwent endovascular treatment. 150 of them received both baseline angiography and followup neuroimaging. The core lab reviewed all follow-up CT imaging and flagged all infarcts located outside the immediate territory of the originally occluded vessel. Each infarct was re-reviewed in the context of the anatomy of the Circle of Willis, the original occlusion site, the presence of other acute occlusions, and the endovascular procedure performed. Infarcts in a previously unaffected vascular territory following detailed assessment of vascular anatomy were determined to be INTs, and were classified into 3 types (I-III) and 2 subtypes (A or B) based on size and catheter manipulation across the vessel territory ostium, respectively.
Results: 32 infarcts were initially identified by the core lab as possibly being new infarcts. Following re-review, 18 of them were deemed to be explainable by baseline vascular anatomy or to be pre-procedural on comparison with baseline imaging. The remaining 14 infarcts were determined to be INTs: 1 Type I-A, 1 Type I-B (size ≤2 mm), 1 Type II-A, 6 Type II-B (size 2–20 mm), 1 Type III-A, and 4 Type III-B (size >20 mm).
Conclusions: Most apparent new infarcts after endovascular treatment are explainable by baseline vascular anatomy. Large INTs are infrequently seen.
ISCHEMIC STROKE SUBTYPE AND TREATMENT EFFECT IN AN ENDOVASCULAR THROMBECTOMY TRIAL
M. Gomis1, C. Castaño1, J. Pagola2, X. Urra3, L. Dorado1, P. Cardona4, D. Rodriguez Luna2, L. San Román3, L. Muñoz1, B. Lara4, A. Dávalos1 and T. Jovin5
1Hospital Germans Trias i Pujol, Neurosciences, Badalona. Barcelona, Spain
3Hospital Universitari Clínic i Provincial, Neurology, Barcelona, Spain
4Hospital Universitari de Bellvitge, Neurology, L´Hospitalet de Llobregat. Barcelona, Spain
5University of Pittsburgh Medical Center, Neurology, Pittsburgh, USA
Abstract
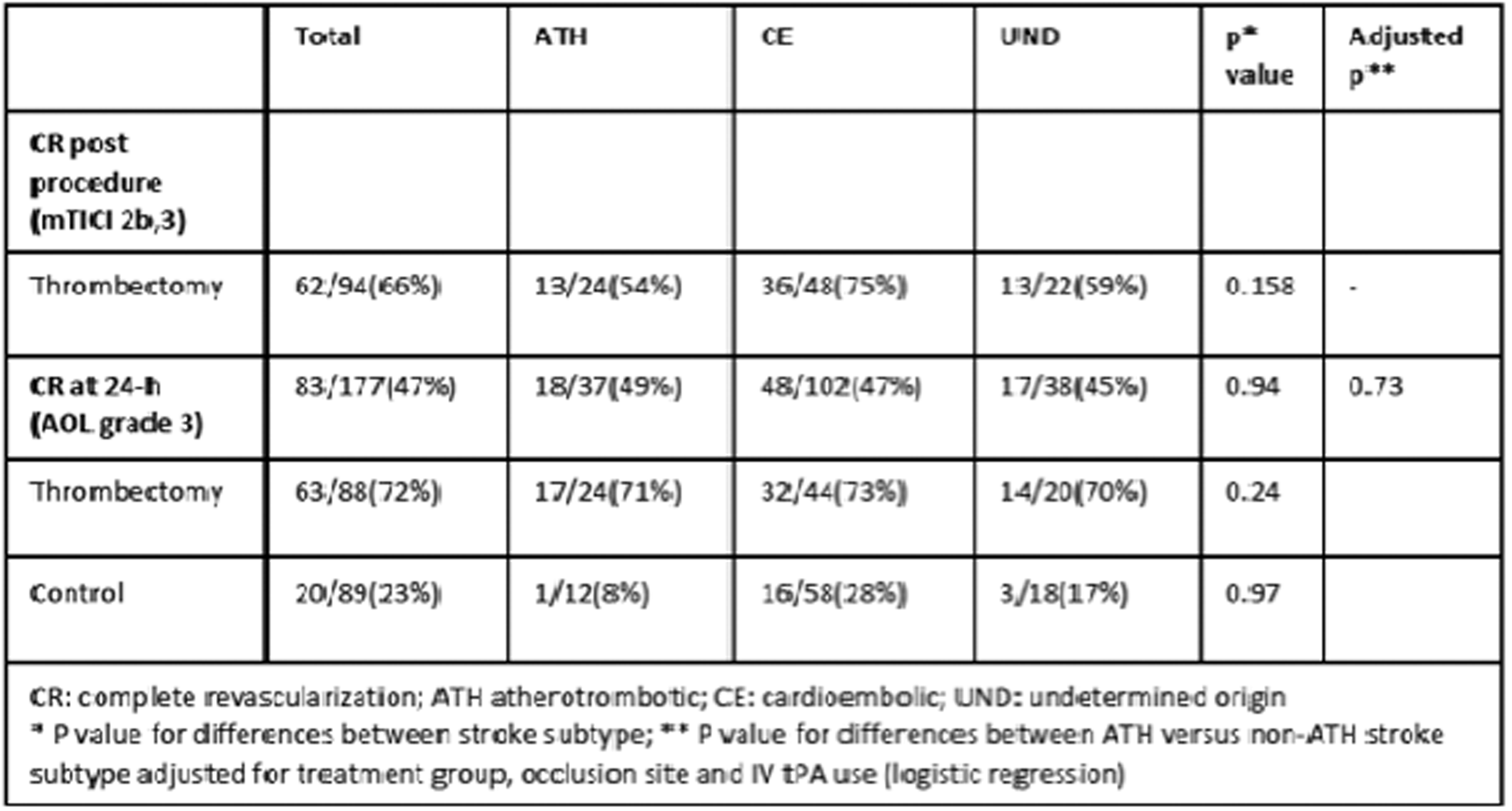
Background: To investigate whether stroke subtypes exhibit differential profile of revascularization and clinical outcome in REVASCAT trial.
Methods: Stroke subtype was prospectively adjudicated by local investigators in 95/103 patients in Solitaire and 98/103 in medical arm as cardioembolic (CE), atherothrombotic (ATH) and undetermined origin (UND). Independent corelab adjudicated complete revascularization (CR) after thrombectomy (mTICI 2b,3), at 24-h post randomization on CT/MR angiography (Arterial Occlusive Lesion grade 3) and 24-h infarct volume were analyzed. Treatment effect by stroke subtype on distribution of mRS scores at 90 days was analysed by ordinal logistic regression.
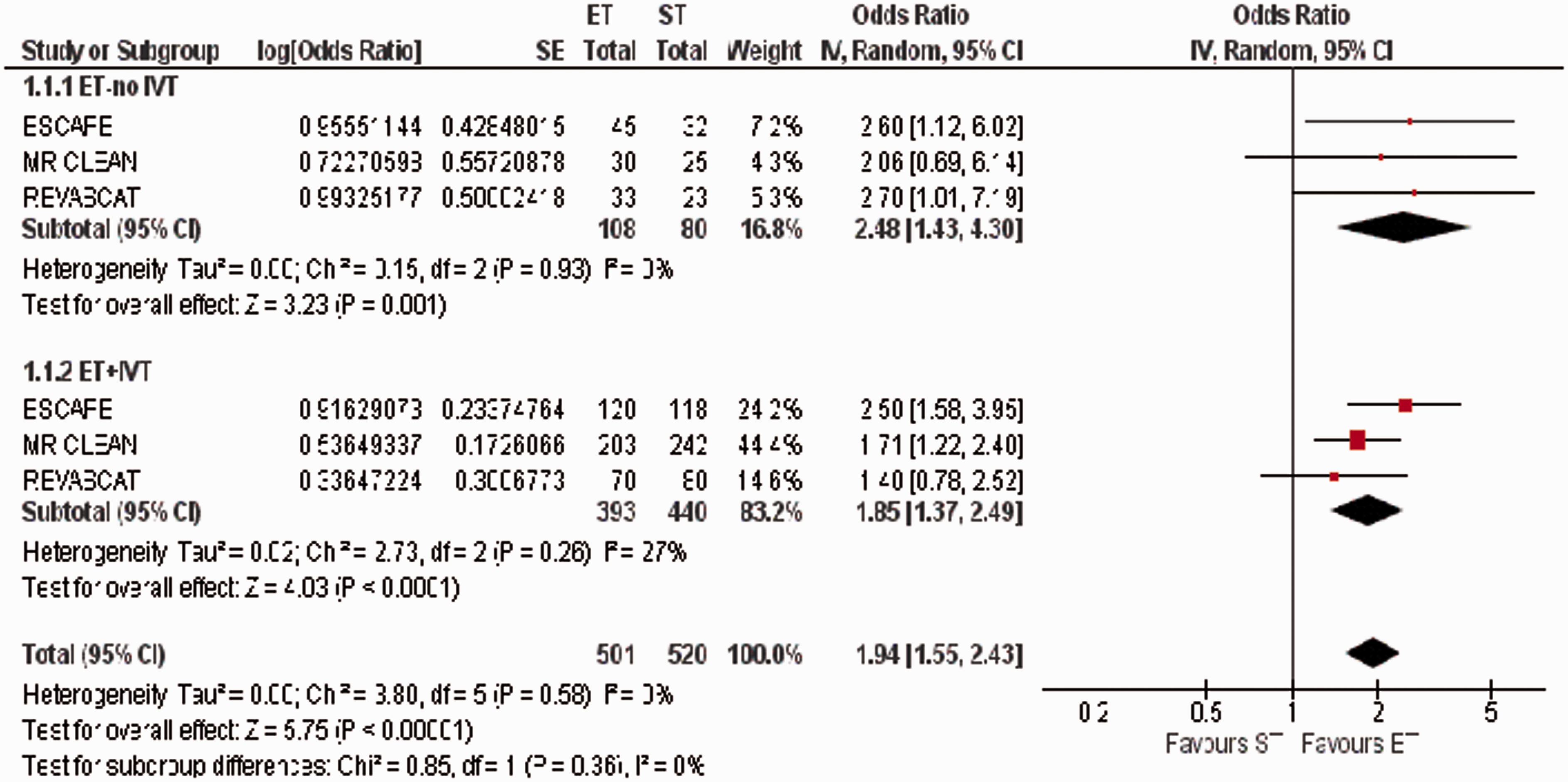
Results: Frequency of stroke subtypes was comparable in the two treatment groups. CR rate after thrombectomy and at 24 hours in the overall patients was not different by stroke subtypes (Table). UND subtype was associated with larger infarct volume compared to AT and CE combined (adjusted mean increased volume, 14.7 cc; 95%CI, 3.4 – 26.0). There was interaction between treatment and stroke subtype on outcome (p < 0.01). AT group showed the highest effect because of higher odds ratios favouring thrombectomy in patients with atherosclerotic tandem occlusions (Figure).
Conclusions: Thrombectomy in proximal arterial occlusions may have distinct treatment effects by stroke subtype.
MECHANICAL THROMBECTOMY WITH AND WITHOUT EMERGENCY CAROTID ARTERY STENTING: RISKS AND CLINICAL OUTCOME IN A STANDARDIZED VASCULAR APPROACH
J. Hensler1, J. Meyne2, A. Binder2, O. Jansen1 and F. Wodarg1
1Universitätsklinikum Schleswig-Holstein- Campus Kiel, Klinik für Radiologie und Neuroradiologie, Kiel, Germany
2Universitätsklinikum Schleswig-Holstein- Campus Kiel, Klinik für Neurologie, Kiel, Germany
Abstract
Background: Mechanical thrombectomy has become an important therapy in patients with acute intracerebral artery occlusion. In up to 20% of cases an additional occlusion of the extracranial carotid artery complicates the endovascular access. Acute carotid artery stenting (CAS) requires anti-platelet therapy and might increase post ischemic hemorrhages. This study compares risk and outcome of mechanical thrombectomy with or without emergency CAS in a retrospective single center analysis.
Methods: We screened our database for patients who underwent mechanical thrombectomy with and without CAS between 2009 and 2015. The rate of symptomatic intracerebral hemorrhage (sICH) was compared in both groups as well as clinical parameters including National Institutes of Health Stroke Scale (NIHSS) and modified Rankin Scale (mRS) at discharge and 90-day-follow-up.
Results: Based on a total of 367 patients with mechanical thrombectomy 63 (21%) were treated with additional emergency CAS. There was no significant difference in NIHSS (14 vs. 14; p = 0.39) on admission, mRS at discharge (3 vs. 4; p = 0.07) or good clinical outcome (mRS ≤ 2) on 90day-follow-up (48.2% vs. 37.4%; p = 0.13). Symptomatic ICH appeared in 17.5% of patients treated with emergency CAS, compared to 6.9% of those treated with mechanical thrombectomy alone (p < 0,01).
Conclusions: Emergency CAS for endovascular stroke treatment is an effective and safe procedure. This analysis showed no significant difference in good clinical outcome between patients treated with and without emergency CAS, despite a significant higher rate of sICH following CAS. Due to a standardized endovascular approach this study offers a good comparability between the two groups.
ENDOVASCULAR TREATMENT IMPROVES COGNITIVE OUTCOME AT 3 MONTHS AND 1 YEAR AFTER STROKE. RESULTS FROM REVASCAT TRIAL
E. López-Cancio1, M. Jiménez1, R. García1, E. Palomeras1, E. Sanjuan2, S. Boned2, P. Cardona3, B. Lara3, X. Urra4, L. Llull4, T. Jovin5 and A. Dávalos1
1Hospital Universitari Germans Trias i Pujol, Neurosciences, Badalona, Spain
4Hospital Clinic i Provincial, Neurology, Barcelona, Spain
5Stroke Institute UPMC, Neurology, Pittsburgh, USA
Abstract
Background: Endovascular treatment has demonstrated reduction in disability after stroke but the effect on cognitive outcomes has not been established. We aim to investigate the effect of endovascular treatment on cognitive function in a randomized clinical trial
Methods: REVASCAT randomized 206 stroke patients with proximal arterial occlusion of anterior circulation within 8 h from onset to thrombectomy or best medical treatment. Patients with established dementia were excluded from enrollment. Executive cognitive function was assessed in person with Trail Making tests (TMT) parts A and B at 3 months and 1 year after randomization. TMT measures attention, processing speed, working memory, visuospatial ability and set shifting. Tests must be completed in <5 minutes. Time of completing each test and errors were recorded. Multivariate analyses were adjusted by age and affected hemisphere
Results: TMT was performed in 82/84 thrombectomy and in 86/87 control patients alive at 3 months and in 71/79 thrombectomy and in 72/78 control patients alive at 1 year. Rates of TMTA completion were similar in both treatment arms; thrombectomy was associated with higher rates of in time TMTB completion (adjusted OR 2.6[1.3–2.1] at 3months and 2.9[1.3–6.3] at 1year). Control patients required longer times to complete TMTA-1y, TMTB-3 m and TMTB-1y (adjusted p < 0.05). Errors in TMTA were more frequently detected in control patients than in thrombectomy patients (adjusted OR 2.4[1.1–5.5] at 3 m and 2.6[1.0–6.5] at 1y)
Conclusions: These results suggest that thrombectomy improves cognitive function at 3 months and 1 year after stroke
BASELINE BLOOD PRESSURE, FUNCTIONAL OUTCOME AND EFFECT OF INTRA-ARTERIAL TREATMENT FOR ACUTE ISCHEMIC STROKE. A MR CLEAN SUBSTUDY
M. Mulder1, S. Ergezen2, O. Berkhemer3, P. Fransen1, D. Beumer4, V.D.B. Lucie5, H. Lingsma6, Y. Roos5, R. Van Oostenbrugge4, W.H. Van Zwam7, C. Majoie3, A. Van der Lugt8 and D. Dippel2
3Academic Medical Center, Radiology, Amsterdam, Netherlands
4Maastricht University Medical Center, Neurology, Maastrich, Netherlands
5Academic Medical Center, Neurology, Amsterdam, Netherlands
6Erasmus MC, Public Health, Rotterdam, Netherlands
7Maastricht University Medical Center, Radiology, Maastrich, Netherlands
8Erasmus MC, Radiology, Rotterdam, Netherlands
Abstract
Background: Little is known about the effect of blood pressure on the functional outcome and occurrence of symptomatic intracranial hemorrhage (SICH) after intra-arterial treatment (IAT) for acute ischemic stroke (AIS). Our aim was to describe the relationship between baseline blood pressure and functional outcome and occurrence of SICH.
Methods: All 500 MR CLEAN patients were included. Blood pressure was measured before treatment. We estimated the effect of systolic- (SBP) and diastolic blood pressure (DBP) on the shift on the modified Rankin Scale (mRS) with ordinal logistic regression analysis, and on the occurrence of SICH. Furthermore we tested for interaction of blood pressure with intra-arterial treatment (IAT).
Results: Median DBP was 80 (IQR:70–90) and SBP was 143 mmHg (IQR:130–160) with SBP exceeding 180 mmHg in 41 patients (8.2%). Relationship on outcome was strongest with SBP. After adjustment for age, baseline NIHSS and collateral score, every 10 mmHg increase in SBP resulted in poorer mRS (OR = 0.89 [95% CI:083.-0.95]), but SBP did not interact with IAT (p = 0.748). SICH occurred in 18 (7.7%) of 233 intervention patients and in 17 (6.4%) controls. Patients with higher SBP had an increased risk of SICH (OR = 1.23 [95% CI: 1.08–1.41], but again there was no interaction with treatment (p = 0.979).
Conclusions: High blood pressure in patients with acute ischemic anterior circulation stroke caused by intracranial large vessel occlusion leads to an increased risk of developing SICH and of poor outcome on the mRS. However, we observed no interaction of baseline blood pressure with treatment.
COMPARISON OF GENERAL VERSUS NON-GENERAL ANESTHESIA ON OUTCOME OF ACUTE ISCHEMIC STROKE AFTER ENDOVASCULAR TREATMENT WITH THE SOLITAIRE STENT RETRIEVER
A. Slezak1, L. Oppliger1, R. Kurmann1, A. Broeg-Morvay1, J. Gralla2, G. Schroth2, P. Mordasini2, H. Mattle1, M. Arnold1, U. Fischer1, S. Jung3, R. Greif4, F. Neff4 and M.L. Mono1
2University Hospital Bern, Diagnostic and Interventional Neuroradiology, Bern, Switzerland
3University Hospital Bern, Neurology and Diagnostic and Interventional Neuroradiology, Bern, Switzerland
4University Hospital Bern, Anesthesiology and Pain medicine, Bern, Switzerland
Abstract
Background: Recent data suggests a non-favourable effect on outcome of general anesthesia (GA) versus non-general anesthesia (NGA) in endovascular treatment (EVT) of acute ischemic stroke (AIS). However, confounding factors like different thrombolytics have to be considered as potential bias. We therefore compared outcome of GA- and non-GA AIS-patients with anterior circulation stroke (ACS) treated with the SOLITAIRE-device.
Methods: Four-hundred-and-two consecutive AIS patients treated with a SOLITAIRE stent retriever for ACS were included in this study. 3-months-outcome was assessed by the modified Rankin Scale (mRS).
Results: One-hundred-and-three patients (26%) underwent EVT in NGA and 279 patients (74%) in GA. The GA-group showed a higher initial NIHSS (17vs. 13, p = 0.000) and had more often an internal-carotid-artery occlusion (44.4% vs. 12.1%, p = 0.000). Other baseline characteristics (e.g. time to treatment (TTT)) did not differ between groups. Favourable outcome (mRS 0–2) was more frequent in NGA-patients (46.3% vs 32.3%; p = 0.01) in univariate, but not multivariate analysis. Independent predictors of favourable outcome were younger age (OR 0.953;95% CI:0.935–0.972; p = 0.000), lower NIHSS (OR 0.889;95% CI:0.851–0.921; p = 0.000), shorter TTT (OR 0.998;95% CI:0.996–0.999; p = 0.011), diabetes mellitus (OR 0.462;95% CI: 0.258 to 0.827, p = 0.009) and symptomatic intracranial hemorrhage (ICH) (OR 0.108;95% CI:0.028–0.426, p = 0.001), but not NGA. Furthermore, GA was not associated with death.
Conclusions: In our study, outcome did not differ between GA- and NGA-treated patients and TTT was not longer in the GA-group. The decision between GA and NGA should be mainly driven by individual patients’ factors with the focus on minimizing TTT with the best comfort and highest safety for patients.
K.M. Treurniet1, O.A. Berkhemer1,2, P.S.S. Fransen2, D. Beumer3, L.A. van den Berg4, H.F. Lingsma5, W.H. van Zwam6, A. van der Lugt7, R.J. van Oostenbrugge3, D.W.J. Dippel2, Y.B.W.E.M. Roos4, H.A. Marquering1,8 and C.B.L.M. Majoie1
1Academic Medical Center- University of Amsterdam, Radiology, Amsterdam, Netherlands
2Erasmus Medical Center, Neurology, Rotterdam, Netherlands
3Maastricht University Medical Center, Neurology, Maastricht, Netherlands
4Academic Medical Center- University of Amsterdam, Neurology, Amsterdam, Netherlands
5Erasmus Medical Center, Public Health, Rotterdam, Netherlands
6Maastricht University Medical Center, Radiology, Maastricht, Netherlands
7Erasmus Medical Center, Radiology, Rotterdam, Netherlands
8Academic Medical Center- University of Amsterdam, Biomedical Engineering & Physics, Amsterdam, Netherlands
Abstract
Background: While intra-arterial treatment (IAT) for acute ischemic stroke (AIS) is a safe and effective treatment modality, complications do occur. One potential complication is infarction in new territory (INT) after catheterisation of the occluded artery. The aim of this study is to assess the incidence of INT after standard care or standard care with IAT in the MR CLEAN study.
Methods: INT was defined as a new infarct in a territory not supplied by the primary occlusive lesion and was identified by comparing 1–7 day follow-up non-contrast CT with baseline non-contrast CT and CTA. Cases were excluded from this study if baseline or follow-up imaging was missing or if scans were of insufficient quality. The incidence of INT was compared between both arms using the chi-square test.
Results: Of the 500 patients included in the trial, 23 did not have follow-up imaging available and 4 had scans of insufficient quality. In the intervention arm, 31 of the remaining 223 patients (13.9%) had confirmed INT compared to 25 of the remaining 250 (10%) patients in the control arm. The difference was not statistically significant (p = 0.19).
Conclusions: INT does not occur more often in AIS patients treated with IAT compared to treatment with usual care alone. It is likely that other factors than catheter manipulation, such as malignant oedema or new emboli, cause INT and these should be considered when assessing this phenomenon in patients treated with IAT.
TIMING OF THE DELIVERY OF INTRA-ARTERIAL TREATMENT IN THE MR CLEAN TRIAL
E. Venema1, N. Boodt2, O. Berkhemer3, H. Lingsma1, W.H. van Zwam4, R. van Oostenbrugge5, A. van der Lugt6, Y. Roos7, C. Majoie3 and D. Dippel2
1Erasmus University Medical Center, Public Health, Rotterdam, Netherlands
2Erasmus University Medical Center, Neurology, Rotterdam, Netherlands
3Academic University Medical Center, Radiology, Amsterdam, Netherlands
4Maastricht University Medical Center, Radiology, Maastricht, Netherlands
5Maastricht University Medical Center, Neurology, Maastricht, Netherlands
6Erasmus University Medical Center, Radiology, Rotterdam, Netherlands
7Academic University Medical Center, Neurology, Amsterdam, Netherlands
Abstract
Background: Clinical outcome and effect of intra-arterial treatment (IAT) for acute ischemic stroke are time-dependent. We investigated treatment delay in the MR CLEAN trial and estimated the additional benefit of treatment within a specific benchmark time.
Methods: We used multivariable linear regression analyses to evaluate the effect of inter-hospital transfer and clinical variables on time intervals in the MR CLEAN trial (n = 500). To assess the effect of in-hospital treatment delay on outcome we defined a benchmark time of 50 minutes between CTA and groin puncture.
Results: Factors with a significant effect on time between CTA and start of treatment were inter-hospital transfer (beta = −33 p < 0.001) and inclusion on weekend days (beta = 19, p = 0.012). Although transfer from a primary stroke center to an intervention center increased time between onset of stroke and CTA with 97 minutes, the subsequent time interval from CTA to start of treatment was 31 minutes shorter compared to non-transferred patients (Figure 1). The benchmark time was reached in only 11% of the patients. If all patients in the MR CLEAN trial would have been treated within benchmark time, disability could have been further reduced with 6.2% (95% CI: 5.5% to 7.0%).
Conclusions: Only few patients in the MR CLEAN trial received IAT within the benchmark time. Reduction of time to treatment by avoiding transfer- and in-hospital-delay would significantly improve clinical outcomes.
AS01-002
ACUTE STROKE TREATMENT: BEYOND REPERFUSION
Oral
EARLY ISCHEMIC WORSENING AS A TARGET FOR NEUROPROTECTIVE THERAPIES: INSIGHTS FROM THE URICO-ICTUS TRIAL
S. Amaro1, C. Laredo1, M. Castellanos2, T. Segura3, J. Arenillas4, J. Martí-Fàbregas5, J. Gállego6, J. Krupinski7, M. Gomis8, D. Cánovas9 and Á. Chamorro1
1Hospital Clinic de Barcelona, Comprehensive Stroke Center- Department of Neuroscience., Barcelona, Spain
2Hospital Universitario Doctor Josep Trueta, Department of Neurology, Girona, Spain
3Complejo Hospitalario Universitario de Albacete, Department of Neurology, Albacete, Spain
4Hospital Clínico Universitario- Universidad de Valladolid, Stroke Unit- Department of Neurology and Medicine, Valladolid, Spain
5Hospital de la Santa Creu i Sant Pau IIb Sant Pau, Department of Neurology, Barcelona, Spain
6Hospital de Navarra, Department of Neurology, Pamplona, Spain
7University Hospital Mutua Terrassa, 7Cerebrovascular Diseases Unit- Department of Neurology, Terrassa, Spain
8Hospital Universitario Germans Trias i Pujol- Universidad Autónoma de Barcelona, Department of Neurosciences, Barcelona, Spain
Background: We aimed to evaluate whether uric acid (UA) is superior to placebo for reducing the rate of early ischemic worsening (EIW) in acute stroke patients receiving alteplase.
Methods: Patients were part of the URICO-ICTUS trial (NCT00860366), a randomized double-blind study that compared the administration of UA versus placebo in 411 stroke patients treated with alteplase within 4.5 hours of onset. The effect of therapy on the rate of EIW within 72 hours was assessed with multivariate models adjusted by variables associated with EIW on univariate analysis. Pretreatment collateral status was assessed in 127 patients who had a baseline CT-angiogram.
Results: EIW occurred in 25 (6%) patients and was associated with older age, hypertension, smoking, atrial fibrillation, higher baseline glucose and stroke severity, as well as with poor outcome at 90 days (OR = 7.07, CI95% = 1.64–30.44). Compared to placebo, UA therapy resulted in lower rates of EIW (3.3% versus 9.0%; adjusted-OR = 0.4, CI95% = 0.14–0.88, p = 0.03). UA/Placebo therapy interacted significantly with pretreatment glucose levels (p = 0.04), sex (p = 0.05) and baseline collateral status (p = 0.04) in the prediction of EIW. Thus, UA was significantly superior to placebo in reducing the rate of EIW in patients with hyperglycemia (adjusted-OR = 0.21, 95%CI = 0.05–0.83, p = 0.03) and in females (adjusted-OR = 0.19, CI95% = 0.05–0.71, p = 0.01), and near-significantly in patients with good collaterals (OR = 0.35, CI-95% = 0.11–0.14, p = 0.08).
Conclusions: UA therapy was associated with a reduced rate of EIW in stroke patients receiving alteplase, particularly in females and in patients with pretreatment hyperglycemia and good collaterals. A larger confirmatory trial is justified to establish the neuroprotective efficacy of UA in acute stroke.
AS02-006
ACUTE STROKE TREATMENT: BEYOND REPERFUSION
Oral
PARACETAMOL (ACETAMINOPHEN) IN STROKE 2 (PAIS2): RESULTS FROM A RANDOMIZED, DOUBLE-BLIND PLACEBO-CONTROLLED CLINICAL TRIAL
I. de Ridder1, H. den Hertog2, H.B. Van de Worp3, M. van Gemert4, T. Schreuder5, A. Ruitenberg6, L. Maasland7, R. Saxena8, J. van Tuijl9, B. Jansen9, R. van den Berg-Vos10, F. Vermeij11, P. Koudstaal1, J. Kappelle12, A. Algra13 and D. Dippel1
1Erasmus MC University Medical Center, Neurology, Rotterdam, Netherlands
3Rudolf Magnus Institute for Neuroscience- University Medical Center Utrecht, Rudolf Magnus Institute for Neuroscience- University Medical Center Utrecht, Utrecht, Netherlands
4Meander Medical Center, Neurology, Amersfoort, Netherlands
5Atrium Medical Center, Neurology, Heerlen, Netherlands
6Admiraal de Ruyter Hospital, Neurology, Goes, Netherlands
12Rudolf Magnus Institute for Neuroscience- University Medical Center Utrecht, Neurology and neurosurgery, Utrecht, Netherlands
13University Medical Center Utrecht, Julius Center for Health Sciences and Primary Care, Utrecht, Netherlands
Abstract
Background: Subfebrile body temperature and fever in the first days after stroke are strongly associated with unfavorable outcome. We assessed the effect of prevention of subfebrile temperatures and fever with high-dose paracetamol on functional outcome in patients with acute stroke and a body temperature of 36.5°C or above.
Methods: PAIS 2 was a multicenter, randomized, double-blind, placebo-controlled clinical trial. We aimed to include 1,500 patients with acute ischemic stroke or intracerebral hemorrhage within 12 hours of symptom onset. Patients were treated with paracetamol in a daily dose of 6 g or matching placebo for 3 consecutive days. The primary outcome was improvement on the modified Rankin Scale score at 3 months, assessed with multivariable ordinal logistic regression. PAIS 2 was registered, NTR2365. Due to lack of funding the study was stopped prematurely.
Results: We included 255 patients, of whom 136 (53%) were allocated to paracetamol. Two patients were lost to follow-up. Mean age was 69 years in both groups. Baseline characteristics did not differ, except for sex (paracetamol 50% men; placebo 63% men). Treatment with paracetamol did not influence functional outcome at 3 months (OR 0.97; 95% CI: 0.62–1.49). After adjustment for age, stroke severity (NIHSS at admission) and stroke type this finding did not change. There was no difference in serious adverse events (paracetamol 16 (12%) versus placebo 16 (14%), OR 0.86; 95%CI: 0.41–1.81).
Conclusions: Treatment with high-dose paracetamol was safe. The study was underpowered to detect a difference in functional outcome after stroke.
AS02-012
ACUTE STROKE TREATMENT: BEYOND REPERFUSION
Oral
CAN A NURSE-INITIATED INTERVENTION TO MANAGE FEVER, HYPERGLYCAEMIA AND SWALLOWING POST STROKE REDUCE LONG-TERM MORTALITY? FOLLOW-UP RESULTS FROM THE QASC TRIAL
S. Middleton1, G. Mnatzaganian2, K. Coughlan1, C. D’Este1, N. Low Choy3, A. Jammali-Blasi1, J. Grimshaw3, C. Levi4, N.W. Cheung5, J. Ward6, D. Cadilhac7, P. McElduff8 and S. Dale1
1Nursing Research Institute- Australian Catholic University, SVHA & ACU Nursing Research Institute, Sydney, Australia
2Australian Catholic University, Faculty of Health Sciences, Melbourne, Australia
3Australian Catholic University- School of Physiotherapy, Faculty of Health Sciences, Brisbane, Australia
3Clinical Epidemiology Program, Ottawa Health Research Institute, 1053 Carling Avenue, Administration Building, Room 2-017,Department of Medicine, University of Ottawa, 451 Smyth Road, Ontario K1H 8M5, Canada
4Centre for Translational Neuroscience and Mental Health, University of Newcastle/Hunter Medical Research Institute
5Centre for Diabetes and Endocrinology Research, Westmead Hosp
ital and University of Sydney, Westmead NSW 2145, Australia
6Department of Epidemiology and Community Medicine, University of Ottawa, 451 Smyth Road, Ottawa, Ontario K1H 8M5, Canada
7Translational Public Health Unit, Stroke and Ageing Research, Southern Clinical School, Monash University, Clayton 3168, Australia. Public Heath, Stroke Division, The Florey Institute of Neuroscience and Mental Health, Heidelberg, Australia
8School of Medicine and Public Health The University of Newcastle, University Drive, Callaghan, Newcastle NSW 2300, Australia
Abstract
Background: The Quality in Acute Stroke Care (QASC) CRCT (2005–2010) conducted in 19 NSW acute stroke units demonstrated that management of fever, hyperglycaemia and swallowing dysfunction decreased death and disability 90-days post-stroke.
Aim: To assess the impact of the QASC intervention on longer term all-cause mortality.
Methods: All-cause mortality was ascertained through linkage with Australia’s National Death Index. Cox proportional hazards regression was used to compare time to death adjusting for correlation of outcomes within stroke units. Primary analyses included treatment group only, with secondary analyses also including age, sex, marital status, education, and Los Angeles Motor stroke severity Scale (LAMS).
Results: A total of 1,076 participants (Intervention n = 600; control n = 476) were followed for a median of 4.1 years (range 38–70 months), of which 264 (24.5%) had died. Preliminary analyses showed that those in the QASC intervention group, relative to the control group had better overall survival: unadjusted hazard ratio (HR): 0.79, 95% CI 0.7–0.9, P = 0.006; adjusted HR: 0.76, 95% CI 0.6–0.9, P = 0.013). Older age and increasing LAMS were associated with poorer survival, while being married was associated with better survival (HR: 0.71, 95% CI 0.5–0.9, P = 0.03).
Conclusions: Multidisciplinary supported evidence-based protocols initiated by nurses for the management of fever, hyperglycaemia, and swallowing dysfunction has a sustained effect in reducing long-term mortality after discharge from stroke units.
AS02-020
ACUTE STROKE TREATMENT: BEYOND REPERFUSION
Oral
PREHOSPITAL INTIATION OF NEUROPROTECTION FOLLOWED BY IN-HOSPITAL THROMBOLYSIS
Y. Hovhannisyan1, N. Sanossian2, M. Kim-Tenser2, S. Starkman3, D. Liebeskind4, R. Conwit5, S. Hamilton6 and J. Saver3
1Yerevan State Medical University, Comprehensive Stroke Center, Yerevan, Armenia
2University of Southern California, Neurology, Los Angeles, USA
3University of California Los Angeles, Stroke Center, Los Angeles, USA
4University of California Los Angeles, Neurovascular Imaging Research Core, Los Angeles, USA
5National Institutes of Health, National Institute of Neurological Disorders and Stroke, Bethesda, USA
6Stanford University, Neurology, Palo Alto, USA
Abstract
Background: Prehospital initiation of neuroprotectant followed by in-hospital thrombolysis is a promising strategy in ischemic stroke, leading to longer exposure prior to thrombolysis. Magnesium may improve outcomes and reduce hemorrhagic transformation (HT) after thrombolysis.
Methods: We selected all cases of intravenous thrombolysis in the Field Administration of Stroke Therapy Magnesium (FAST-MAG) clinical trial, an NIH-funded phase 3 study of prehospital treatment with magnesium vs. placebo initiated <2 hours from symptom onset. We describe duration of study drug exposure prior to thrombolysis and the effect of magnesium therapy in long-term outcome and symptomatic HT.
Results: There were 1700 cases, age 69 (SD14), 43% women, 78% white race (13%African-American,8% Asian) and 24% Latino. Final diagnosis was cerebral ischemia in 73%, ICH in 23% and 4% mimic. Subjects were evaluated by paramedics 24 (IQR15–43) minutes, received study agent 44 (IQR34–59) minutes and arrived to emergency department (ED) 56 (45–73) minutes after onset. There were 455 subjects (27% of total and 36% of cerebral ischemia) who where treated with IV TPA 79 (IQR62–104) minutes after arrival. Patients were exposed to study agent for 92 (SD33) minutes before thrombolysis. In thrombolysed cases, magnesium was not associated with improvement in 3-month Rankin (median 3 vs 3, p = 0.408) or good outcome (mRS 0–2, OR 1.042,95%CI 0.558–1.945). Symptomatic HT rates were not different (6%vs8%, OR 0.695, 95%CI 0.334–1.45).
Conclusions: Prehospital initiation leads to over 90 minutes of neuroprotectant exposure prior to thrombolysis. Magnesium in combination with thrombolysis was not associated with improved 90-day outcomes or significant reduction in the rate of HT.
AS17-073
ACUTE STROKE TREATMENT: BEYOND REPERFUSION
Oral
EARLY INITIATION OF STATIN TREATMENT AND OUTCOME AFTER ACUTE ISCHEMIC STROKE
J.F. Scheitz1, R.L. MacIsaac2, A.H. Abdul-Rahim2, B. Siegerink1, P. Bath3, M. Endres1, K.R. Lees2 and C.H. Nolte1
1Charité - Center for Stroke Research Berlin, Neurology, Berlin, Germany
2Stroke Research- Institute of Cardiovascular & Medical Sciences, University of Glasgow, Glasgow, United Kingdom
3Stroke Trials Unit- Division of Clinical Neuroscience, University of Nottingham, Nottingham, United Kingdom
Abstract
Background: Guidelines recommend statin treatment in ischaemic stroke patients. However, there is paucity of data on the effects of early statin treatment on functional outcome. Therefore, we aimed to analyse whether early initiation of statins among statin-naïve patients improves outcome at three months.
Methods: Data were sought from the Virtual International Stroke Trials Archive (VISTA). Multivariate ordinal regression was applied to estimate odds ratios for the distribution of modified Rankin Scale (mRS) at day 90 associated with early statin exposure (initiated within 3 days post stroke) compared to patients without early or without any statin exposure. Multivariable Cox proportional-hazard-models were applied to estimate hazard ratios for mortality at day 90. A propensity-matched design, matching based on relevant clinical covariates (age, sex, stroke severity, diabetes, hypertension, myocardial infarction, and initiation of co-medication post-stroke) was used to reduce potential for confounding.
Results: Among 7116 statin-naïve patients registered within the VISTA Acute repository, 626 patients with early initiation of statins were identified. Before propensity matching a significant relationship between early statin exposure and both favourable distribution of mRS (ORunadjusted 1.63, 95%CI 1.41–1.89; ORadjusted 1.20, 95%CI 1.03–1.40) and mortality by day 90 was observed (HRunadjusted 0.49, 95%CI 0.38–0.62; HRadjusted 0.68, 95%CI 0.52–0.88). Within the propensity-matched cohort the relationship with mRS d90 attenuated (ORPPM 1.21, 95%CI 0.98–1.50) but the relationship with mortality remained consistent (HRPPM 0.67, 95%CI 0.46–0.97).
Conclusions: We found evidence that initiation of statin treatment within three days post ischaemic stroke is associated with lower mortality and probably with improved functional outcome at 90 days.
AS09-032
ACUTE STROKE TREATMENT: BEYOND REPERFUSION
Oral
NO BENEFITS OF HYPOTHERMIA IN PATIENTS TREATED WITH HEMICRANIECTOMY FOR LARGE ISCHEMIC STROKE
H. Schneider1, P. Krüger2, A. Algra3,4, J. Hofmeijer5, H.B. Van de Worp3, E. Jüttler6, K. Vahedi7, G. Schackert8, H. Reichmann1 and V. Puetz1
1University Hospital- TU Dresden, Department of Neurology and Dresden University Stroke Center, Dresden, Germany
2Klinikum Dortmund gGmbH, Department of Anesthesiology, Dortmund, Germany
3Brain Center Rudolf Magnus- University Medical Center Utrecht, Department of Neurology and Neurosurgery, Utrecht, Netherlands
4Julius Centre for Health Sciences and Primary Care, Department of Epidemiology, Utrecht, Netherlands
5Rijnstate Hospital, Department of Neurology, Arnhem, Netherlands
6Ostalb-Klinikum Aalen and University of Ulm, Department of Neurology, Aalen/Ulm, Germany
7Générale de Sante- Hôpital Privé d’Antony- Antony- and AP-HP- Hôpital Lariboisière, Neurology Centre, Paris, France
8University Hospital- TU Dresden, Department of Neurosurgergy, Dresden, Germany
Abstract
Background: To evaluate the benefit of therapeutic hypothermia in patients with space-occupying cerebral infarction treated with hemicraniectomy within 48 h of stroke onset.
Methods: Patients aged 18–60 years with space-occupying cerebral infarction treated with hemicraniectomy within 48 h and hypothermia (33–34°C) were selected from a single university hospital between 2001 and 2010 (n = 53). Patients treated with hemicraniectomy alone served as comparison group (n = 58), originating from three randomized controlled trials evaluating the effects of early decompressive surgery (DECIMAL, DESTINY, HAMLET).
Primary outcome was the score on the modified Rankin scale (mRS) at 12 months dichotomised between mRS 0–3 and mRS 4–6. Secondary outcome measures were mRS score 0–4 and survival. Risk ratios were adjusted with Poisson regression.
Results: Mean patient age was 48 years. Median time from stroke onset to hemicraniectomy was 23.5 h in both treatment groups. Treatment with hypothermia had no effect on the primary outcome (mRS 0–3 vs. 4–6 [13/53 (25%) vs. 24/58 (41%)]; adjusted risk ratio [ARR] 0.66, 95% CI 0.38 – 1.13). Fewer patients treated with hypothermia had a mRS score of 0–4 (21/53 [40%] vs. 42/58 [72%]; ARR 0.53, 95% CI 0.37 – 0.76) and fewer patients survived (26/53 [49%] vs. 46/58 [79%]; ARR 0.60, 95% CI 0.44 – 0.82).
Conclusions: In our single-center cohort of younger patients with space-occupying cerebral infarction, treatment with hypothermia had no additional benefit on functional outcome compared with treatment with hemicraniectomy alone.
AS06-046
ACUTE STROKE TREATMENT: BEYOND REPERFUSION
Oral
ANTIBIOTIC THERAPY FOR PREVENTING INFECTIONS IN PATIENTS WITH ACUTE STROKE: A META-ANALYSIS
J.D. Vermeij1, W.F. Westendorp1, D.W. Dippel2, D. van de Beek1 and P.J. Nederkoorn1
1Academic Medical Center University of Amsterdam, Neurology, Amsterdam, Netherlands
2Erasmus MC Rotterdam, Neurology, Rotterdam, Netherlands
Abstract
Background: Infections often occur in stroke patients and are associated with unfavorable outcome. Preventive antibiotic therapy in the acute phase may reduce infection rate and improve functional outcome. Two large phase III RCTs (PASS and STROKE-INF) have been published in 2015; warranting an update of our previous Cochrane meta-analysis.
Methods
Objectives: To assess whether preventive antibiotics reduce infections and improve functional outcome in acute stroke patients.
Search: We performed a systematic review using Cochrane methodology and searched CENTRAL, MEDLINE and EMBASE for RCTs on preventive antibiotics in acute stroke.
Data collection and analysis: Two authors independently assessed included studies. Study authors were contacted to obtain missing data when required. We calculated relative risks (RRs) for dichotomous outcomes, assessed heterogeneity, and performed subgroup analyses on study quality.
Results: We included seven studies involving 4225 patients. Study population, design, type of antibiotic and definition of infection differed considerably. Mortality rates were similar in the intervention and control group (348/2111 (16%) versus 332/2114 (16%), RR 1.03, 95%-CI 0.84 to 1.26). Preventive antibiotic therapy reduced post-stroke infection rate in patients with acute stroke from 25% to 18% (367/2049 (18%) versus 516/2041 (25%), RR 0.67, 95%-CI 0.54 to 0.83). The number of dependent patients in the preventive antibiotic group was similar (1070/2071 (52%) versus 1099/2064 (53%), RR 0.96, 95%-CI 0.85 to 1.08). No major side-effects were reported.
Conclusions: Preventive antibiotic therapy reduces the risk of post-stroke infection, but does not improve functional outcome. A Cochrane update will be published during 2016.
AS05-029
ACUTE STROKE TREATMENT: BEYOND REPERFUSION
Oral
PREDICTION OF STROKE-ASSOCIATED INFECTION IN THE PREVENTIVE ANTIBIOTICS IN STROKE STUDY (PASS)
W. Westendorp1, J.D. Vermeij1, M. Brouwer1, A. Algra2, H.B. Van de Worp3, D. Dippel4, D. van de Beek1 and P. Nederkoorn1
1Academic Medical Center University of Amsterdam, Neurology, Amsterdam, Netherlands
2UMC Utrecht, Neurology & Neurosurgery and Julius Center, Utrecht, Netherlands
3UMC Utrecht, Neurology, Utrecht, Netherlands
4Erasmus MC, Neurology, Rotterdam, Netherlands
Abstract
Background: Stroke-associated infections occur frequently and are associated with unfavourable outcome. In two recent large randomized trials (PASS and STROKE-INF) preventive antibiotics did reduce infections but did not improve functional outcome in all acute stroke patients. Here, we aim to develop a prediction model for stroke-associated infection to allow identification of patients at the highest risk of such infection.
Methods: Data were used from PASS, a multicentre trial with a PROBE design comparing preventive ceftriaxone in addition to standard stroke care vs. standard stroke care in 2550 patients. Infections were categorized as diagnosed by the clinician, and as judged by a blinded adjudication committee. Possible predictors for stroke-associated infection were selected based on literature. Backward elimination logistic regression analysis was used to construct a prediction model.
Results: Stroke-associated infections (N = 177) were predicted by age per year (OR 1.05; 95%CI 1.02–1.08,), stroke severity per point on the NIHSS (1.07; 1.01–1.12), female sex (2.2; 1.2–3.9), dysphagia (3.6; 1.8–7.0) and use of bladder catheter (5.2; 2.9–9.3). Pneumonia (N = 87) was predicted by age per year (1.05; 1.02–1.08), NIHSS (1.11; 1.05–1.18), female sex (1.9; 1.10–3.31) and dysphagia (4.2; 2.2–8.1). A prediction-chart will be presented after appropriate shrinking of regression coefficients for over-optimism as well as discrimination and calibration measures of the shrunk model.
Conclusions: Age, stroke severity, sex and dysphagia predict stroke-associated infections. The PASS prediction-chart for stroke-associated infection and pneumonia is to be used for clinical management and design of future trials, after external validation.
AS02-027
ACUTE STROKE TREATMENT: BEYOND REPERFUSION
Oral
INFLUENCE OF STENT DESIGN AND USE OF PROTECTION DEVICES ON OUTCOME OF CAROTID ARTERY STENTING - A POOLED ANALYSIS OF INDIVIDUAL PATIENT DATA
F. Wodarg1, E. Turner2, J. Dobson2, P.A. Ringleb3, G. Fraedrich4, J.P. Becquemin5, M.M. Brown6, A. Algra7, J.L. Mas8, O. Jansen1 and L.H. Bonati9
1University Hospital Kiel, Department of Radiology and Neuroradiology, Kiel, Germany
2London School of Hygiene and Tropical Medicine, Department of Medical Statistics, London, United Kingdom
3University Hospital Heidelberg, Department of Neurology, Heidelberg, Germany
4Medical University, Department of Vascular Surgery, Innsbruck, Austria
5Université Paris XII, Institut Vasculaire Paris Est HPPE Champigny, Paris, France
6Queen Square, Stroke Research Group- UCL Institute of Neurology, London, United Kingdom
7University Medical Center Utrecht, Brain Center Rudolf Magnus- Department of Neurology and Neurosurgery and Julius Center for Health Sciences and Primary Care, Utrecht, Netherlands
8Hôpital Sainte-Anne- Université Paris-Descartes- INSERM U894- DHU Neurovasc-Paris Sorbonne, Department of Neurology, Paris, France
9University Hospital Basel, Department of Neurology and Stroke Unit, Basel, Switzerland
Abstract
Background: Carotid artery stenting is an alternative to endarterectomy for treatment of carotid stenosis. We pooled individual patient data from three large randomised trials comparing stenting versus endarterectomy in patients with symptomatic carotid stenosis (ICSS, SPACE, EVA–3S) to investigate the influence of technical aspects, such as stent design or the use of an endovascular protection device on the risk of procedural stroke or death in patients treated with stents.
Methods: The per-protocol analysis included 1557 patients treated with stents in whom information on stent types and protection device use was available. The primary outcome event was any procedural stroke or death occurring within 30 days after stenting.
Results: 962 patients (61.8%) were treated with closed-cell stents and 595 (38,2%) with open-cell stents. Protection devices were used in 950 patients (61.0%); most protection devices were of the distal filter type (87.3%). Procedural stroke or death occurred significantly more often in patients treated with open-cell stents (61, 10.3%) than in those treated with closed-cell stents (58, 6.0%; p = 0.002). The primary outcome event occurred in 76 patients (8.0%) treated with protection devices and in 43 (7.1%) treated without protection devices (p = 0·67). The effect of protection devices did not differ significantly between patients treated with open-cell and those treated with closed-cell stents.
Conclusions: The use of stents with a closed-cell design is independently associated with a lower risk of procedural stroke or death compared with open-cell stents. Protection devices do not appear to reduce stroke risk, independently of the type of stent used.
AS01-004
ACUTE THROMBECTOMY TRIALS - IMAGING PREDICTORS OF OUTCOME
Oral
RELATIVE-CEREBRAL BLOOD VOLUME PREDICTS COLLATERAL STATUS AND INFARCT GROWTH IN HYPERACUTE ISCHEMIC STROKE PATIENTS IN SWIFT PRIME
J.F. Arenillas1, E. Cortijo1, P. García-Bermejo1, E.I. Levy2, R. Jahan3, M. Goyal4, J.L. Saver5 and G.W. Albers6
1Hospital Clínico Universitario. University of Valladolid, Stroke Program. Department of Neurology, Valladolid, Spain
2State University of New York at Buffalo, Neurosurgery, Buffalo- New York, USA
3University of California Los Angeles, Division of Interventional Neuroradiology, Los Angeles- California, USA
4University of Calgary, Departments of Radiology and Clinical Neurosciences, Calgary- Alberta, Canada
5David Geffen School of Medicine at the University of California Los Angeles, Department of Neurology and Comprehensive Stroke Center, Los Angeles- California, USA
6Stanford University School of Medicine, Department of Neurology and Neurological Sciences, Stanford- California, USA
Abstract
Background: We aimed to identify perfusion imaging markers of collateral circulation status (CCS) and evaluate their capacity to predict infarct growth in anterior circulation acute ischemic stroke (AC-AIS) patients included in SWIFT PRIME study.
Methods: Patients with baseline CT perfusion (CTP) scans were included. RAPID software was used to calculate baseline ischemic core volume (based on relative CBF maps), relative cerebral blood volume (rCBV) in regions with Tmax > 6 s perfusion lesions and the Tmax10s/Tmax6s hypoperfusion ratio (HIR). Blind core-lab assessment of CCS was based on CT angiography (CTA) in the full sample (tPA alone and the tPA plus endovascular group) and on cerebral angiography (CAng) in the endovascular group. Reperfusion was assessed on 27-hour CTP, infarct volume assessed on 27-hr MRI/CT scans. Linear regression models assessed the relationship between perfusion parameters, collateral status and infarct growth.
Results: One hundred fifty-eight patients were included. Both rCBV and HIR were associated with good vs. poor CTA-assessed CCS (p = 0.03 and p = 0.04 respectively) and also with CAng-defined CCS. A gradual improvement in rCBV was observed with increasing collateral grades on CAng (p = 0.01). Baseline and 27-hr follow-up CTP was available in 112 patients, of whom 71 (63%) achieved successful reperfusion. Among patients who reperfused, higher rCBV was associated with smaller infarct growth (p = 0.03).
Conclusions: rCBV and HIR are associated with CCS in AC-AIS. In successfully reperfused patients, rCBV is a predictor of infarct growth. The benefit of early cerebral reperfusion is enhanced by good CCS, which can be non-invasively assessed with CTP.
AS22-003
ACUTE THROMBECTOMY TRIALS - IMAGING PREDICTORS OF OUTCOME
Oral
DEGREE OF COLLATERAL FLOW AT BASELINE ASSOCIATED WITH FOLLOW UP INFARCT VOLUME AFTER INTRA-ARTERIAL THERAPY IN MR CLEAN
A. Boers1,2,3, I. Jansen1,3, O. Berkhemer1, P. Fransen4, D. Beumer5, L.A. van den Berg6, H. Lingsma7, W.H. van Zwam8, R. van Oostenbrugge5, A. van der Lugt9, D. Dippel4, Y. Roos6, H. Marquering3 and C. Majoie1
1Academic Medical Center University of Amsterdam, Radiology, Amsterdam, Netherlands
2University of Twente, Robotics & Mechatronics, Enschede, Netherlands
3Academic Medical Center University of Amsterdam, Biomedical Engineering & Physics, Amsterdam, Netherlands
4Erasmus MC University Medical Center, Neurology, Rotterdam, Netherlands
5Maastricht University Medical Center, Neurology, Maastricht, Netherlands
6Academic Medical Center University of Amsterdam, Neurology, Amsterdam, Netherlands
7Erasmus MC University Medical Center, Public Health, Rotterdam, Netherlands
8Maastricht University Medical Center, Radiology, Maastricht, Netherlands
9Erasmus MC University Medical Center, Radiology, Rotterdam, Netherlands
Abstract
Background: Collateral flow is a strong treatment effect modifier of intra-arterial therapy (IAT) for stroke, with improved clinical outcomes on mRS (90 days) for patients with high collateral grades. However, the effect of collateral flow on final infarct volume (FIV), an important quantifiable surrogate marker for clinical outcome, has not yet been studied. We aimed to investigate the association of collateral flow on FIV and IAT in MRCLEAN.
Methods: Infarctions were segmented on 5–7 day follow-up non-contrast CT (or 1 day if not available), whereafter FIV was calculated. Baseline CTA collaterals were graded from 0 (absent) to 3 (excellent). Mann-Whitney-U test was used to compare FIV’s between IAT and control group per collateral grade.
Results: Four-hundred-thirty-two scans were included. FIV difference for IAT vs. controls was significant with medians of resp. 51 vs. 80 mL (p = 0.01) for the total population and 25 vs. 49 mL for grade 3 (p = 0.01), and 42 vs. 70 mL for grade 2 (p = 0.01). No statistically significant difference was found for grade 1 collaterals (115 vs. 145 mL (p = 0.19)) and for grade 0 (339 vs. 212 mL (p = 0.26)).
Conclusions: In this study, a significant reduction of FIV between treatment groups was found for collateral grade 1 and 2. The largest reduction was in patients with excellent collaterals. For patients with absent or poor collaterals no significant FIV difference was found.
AS09-003
ACUTE THROMBECTOMY TRIALS - IMAGING PREDICTORS OF OUTCOME
Oral
ASSOCIATION OF THROMBUS CHARACTERISTICS ON CT IMAGING WITH OUTCOME AND EFFICACY OF INTRA-ARTERIAL TREATMENT IN PATIENTS WITH ACUTE ISCHEMIC STROKE IN MR CLEAN
J. Borst1, O. Berkhemer2, E. Santos3, A. Yoo4, M. den Blanken3, P. Fransen5, D. Beumer6, L.A. van den Berg7, Y. Roos7, E. van Bavel3, W.H. Zwam8, R. van Oostenbrugge6, H. Lingsma9, A. van der Lugt10, D. Dippel5, H. Marquering3 and C. Majoie2
1Academic Medical Center, Amsterdam, Netherlands
2Academic Medical Center, Radiology, Amsterdam, Netherlands
3Academic Medical Center, Biomedical Engineering and Physics, Amsterdam, Netherlands
4Texas Stroke Institute, Radiology, Texas, USA
5Medical Center Rotterdam, Neurology, Rotterdam, Netherlands
6Maastricht University Medical Center, Neurology, Maastricht, Netherlands
7Academic Medical Center, Neurology, Amsterdam, Netherlands
8Maastricht University Medical Center, Radiology, Maastricht, Netherlands
9Medical Center Rotterdam, Department of Public Health, Rotterdam, Netherlands
10Medical Center Rotterdam, Radiology, Rotterdam, Netherlands
Abstract
Background: CT thrombus imaging characteristics have been associated with outcome after IAT for acute ischemic stroke. Our objective was to study the association of CT thrombus characteristics with outcome and treatment effect in patients with acute ischemic stroke.
Methods: We included 199 of the 500 MR CLEAN patients for whom thin-slice NCCT and CTA within 30 minutes from each other were available. The following CT thrombus characteristics were assessed: location, distance from ICA-T to thrombus (DT), length, volume, absolute and relative density on NCCT, and thrombus perviousness measures including: attenuation increase, void fraction, and absolute and relative density on CTA. Associations of thrombus characteristics with outcome were estimated with univariable and multivariable ordinal logistic regression as an odds ratio (OR) for a shift toward better outcome on the mRS. Secondary outcomes were final infarct size and recanalization. Interaction between thrombus characteristics and treatment effect was investigated using multivariable ordinal logistic regression.
Results: Distance to thrombus and the thrombus perviousness measures were univariable associated with functional outcome. Relative density on CTA was an independent predictor of functional outcome; adjusted common OR of 1.21 per 10%(95%CI:1.02–1.43)(P = 0.029). The absolute NCCT thrombus density showed a significant interaction with treatment effect (P = 0.048); with increasing NCCT thrombus density the treatment effect of IAT was larger.
Conclusions: Only distance to thrombus and thrombus perviousness are associated with functional outcome. Relative density on CTA is the only independent predictor of functional outcome. In our study cohort intra-arterial therapy is more effective for thrombi with a higher density on NCCT.
AS01-014
ACUTE THROMBECTOMY TRIALS - IMAGING PREDICTORS OF OUTCOME
Oral
CT PERFUSION IMAGING PROFILES AND RESPONSE TO ENDOVASCULAR REPERFUSION IN POOLED ANALYSIS OF RANDOMIZED TRIALS OF ENDOVASCULAR STENT THROMBECTOMY
B.C.V. Campbell1, C.B.L.M. Majoie2, M.D. Hill3, A. Demchuk3, L. San Román4, T.G. Jovin5, J.L. Saver6, D.W.J. Dippel7, M. Goyal8 and P.J. Mitchell9
1Royal Melbourne Hospital and The University of Melbourne, Department of Medicine and Neurology, Melbourne, Australia
2Academic Medical Center, Department of Radiology, Amsterdam, Netherlands
3Hotchkiss Brain Institute- Cumming School of Medicine- University of Calgary- Foothills Hospital, Department of Clinical Neurosciences, Calgary, Canada
4Hospital Clínic, Department of Radiology, Barcelona, Spain
5University of Pittsburgh Medical Center, Stroke Institute- Department of Neurology-, Pittsburgh, USA
6David Geffen School of Medicine at the University of California- Los Angeles, Department of Neurology and Comprehensive Stroke Center, Los Angeles, USA
7Erasmus University Medical Center, Department of Neurology, Rotterdam, Netherlands
8University of Calgary- Foothills Hospital, Department of Radiology, Calgary, Canada
9Royal Melbourne Hospital and The University of Melbourne, Department of Radiology, Melbourne, Australia
Abstract
Background: The role of CT-perfusion imaging in selection of patients for endovascular thrombectomy has been controversial. We pooled data to investigate the association of CT-perfusion imaging profiles in 5 recent randomized trials of endovascular stent-thrombectomy.
Methods: Patient-level imaging data from the MR CLEAN, ESCAPE, EXTEND-IA, SWIFT PRIME and REVASCAT trials were pooled (HERMES Collaboration). CT-perfusion data were uniformly reprocessed using RAPID software (non-commercial research version, Stanford University) as used in the EXTEND-IA and SWIFT PRIME trials. Irreversibly injured ischemic core was defined using a relative cerebral blood flow threshold<30% of normal brain. Tissue at risk of infarction (ischemic penumbra) was estimated using a Tmax threshold >6 seconds. The association between pre-treatment ischemic core and mismatch volumes and the 90 day modified Rankin scale (mRS) was examined by treatment status and reperfusion status. The number needed to treat (NNT) to achieve at least 1 unit improvement in the mRS with endovascular treatment versus control was calculated as a function of ischemic core volume as a continuous variable. A similar analysis was performed for the NNT to achieve an extra patient with independent outcome (mRS 0–2).
Results: The results will be presented at the conference and are expected to include over 400 patients with pre-treatment CT-perfusion imaging.
Conclusions: This analysis will comprise the largest series examined to date with CT-perfusion imaging prior to endovascular therapy using current technology. The resulting insights into whether CT-perfusion parameters are prognostic, treatment effect modifying or both will be highly relevant to clinical practice.
AS01-028
ACUTE THROMBECTOMY TRIALS - IMAGING PREDICTORS OF OUTCOME
Oral
CORTICAL VEIN ASYMMETRY IS ASSOCIATED WITH INTRA-ARTERIAL TREATMENT BENEFIT IN PATIENTS WITH PROXIMAL ANTERIOR CIRCULATION STROKE INCLUDED IN MR CLEAN
I. Jansen1, A. van Vuuren2, W.H. van Zwam3, O. Berkhemer1, R. van Oostenbrugge4, D. Dippel5, L.A. van den Berg6, P. Fransen5, I. van den Wijngaard7, D. Beumer4, H. Lingsma8, A. van der Lugt9, M. van Walderveen7, Y. Roos6, H. Marquering10, C. Slump11, C. Majoie1 and R. van den Berg1
1Academic Medical Center University of Amsterdam, Radiology, Amsterdam, Netherlands
2Free University Amsterdam, Biomedical Sciences, Amsterdam, Netherlands
3Maastricht University Medical Center, Radiology, Maastricht, Netherlands
4Maastricht University Medical Center, Neurology, Maastricht, Netherlands
5Erasmus Medical Center Rotterdam, Neurology, Rotterdam, Netherlands
6Academic Medical Center University of Amsterdam, Neurology, Amsterdam, Netherlands
7Leiden University Medical Center, Radiology, Leiden, Netherlands
8Erasmus Medical Center Rotterdam, Public Health, Rotterdam, Netherlands
9Erasmus Medical Center Rotterdam, Radiology, Rotterdam, Netherlands
10Academic Medical Center University of Amsterdam, Biomedical Engineering & Physics, Amsterdam, Netherlands
11University of Twente, Technical Medicine, Enschede, Netherlands
Abstract
Background: During balloon test occlusion of the internal carotid artery, symmetrical opacification of the cortical veins indicates tolerance of vessel occlusion. We hypothesized that asymmetry in venous drainage reflected by poor opacified veins is associated with reduced intra-arterial therapy (IAT) treatment benefit.
Methods: From the MR CLEAN study patients with adequate baseline CTA images were included. Opacification of the vein of Labbé, sphenoparietal sinus, and superficial middle cerebral vein was graded as 0 (not visible), 1 (faint opacification), or 2 (full opacification). The Cortical Vein Ratio (COVER) was calculated by dividing the sum of opacified veins of the affected hemisphere with the contralateral side. Results were dichotomized into 0 and >0, with 0 representing complete absence of venous opacification in the affected hemisphere. Primary outcome was the modified Rankin Scale score at 90 days (mRS). IAT benefit was estimated with ordinal logistic regression as a common odds ratio, adjusted for pre-specified prognostic factors. We tested for interaction of COVER with treatment effect.
Results: One hundred and one patients with suboptimal scan-timing were excluded from analysis, leaving 399 patients for assessment. The acOR was 1.1 [CI95% 0.6–2.0] for COVER 0 (n = 162) and 2.5 [CI95% 1.6–4.1] for COVER > 0 (n = 237). Interaction of COVER with treatment was statistically significant (p = 0.042).
Conclusions: Patients with complete absence of vein opacification in the affected hemisphere (COVER 0) had no benefit of IAT. If venous flow was observed, a strong benefit was seen. Venous drainage assessment appears to be a promising approach to select patients for intra-arterial stroke treatment.
AS16-047
ACUTE THROMBECTOMY TRIALS - IMAGING PREDICTORS OF OUTCOME
Oral
PREDICTORS OF INFARCT GROWTH AFTER 24 HOURS IN PATIENTS WITH ACUTE ISCHEMIC STROKE
H. Marquering1, A. Bucker2, M. Boers3, J. Bot4, O. Berkhemer5, D. Beumer6, H. Lingsma7, L.A. van den Berg8, P. Fransen9, A. Yoo10, W.H. van Zwam11, R. van Oostenbrugge6, A. van der Lugt12, D. Dippel9, Y. Roos8 and C. Majoie2
1Academic Medical Center- University of Amsterdam, Radiology, Amsterdam, Netherlands
2Academic Medical Center, Radiology, Amsterdam, Netherlands
3University of Twente, Department of Robotics and Mechatronics, Enschede, Netherlands
4Free University Medical Center, Radiology, Amsterdam, Netherlands
5Academic Medcial Center, Radiology, Amsterdam, Netherlands
6MUMC, Neurology, Maastricht, Netherlands
7Erasmus MC, Public Health, Rotterdam, Netherlands
8Academic Medical Center, Neurology, Amsterdam, Netherlands
9Erasmus MC, Neurology, Rotterdam, Netherlands
10Texas Stroke Institute, Radiology, Texas, USA
11MUMC, Radiology, Maastricht, Netherlands
12Erasmus MC, Radiology, Rotterdam, Netherlands
Abstract
Background: Infarct growth in acute ischemic stroke is associated with unfavorable outcome. We aim to identify risk factors for infarct growth after 24 hours in patients with acute ischemic stroke as identified on non-contrast computed tomography (NCCT).
Methods: From the MRCLEAN population, we retrospectively selected 281 patients who received a 24 h and 5–7 days NCCT scan. Lesion volume in NCCT at 24 hours was compared with 5–7 day follow-up NCCT lesion volume. Growth was defined as an increase of lesion volume exceeding 30%. Between groups differences of patients with and without growth were tested in univariate analysis. Multivariate logistic regression analysis was performed to identify independent associations of patient characteristics with lesion growth.
Results: Hundred-and-forty-seven patients were included. Mean age was 66 (range 26–85) years, median admission NIHSS was 17 (range 4–29), 132 (90%) patients received intravenous thrombolysis and 67 (46%) were randomized for intra-arterial treatment (IAT). Median lesion volume was 35.4 (IQR:19.3–88.0) mL and 56.3 (IQR:29.9–116.4) mL at 24 hours and at 5–7 day follow-up respectively. Seventy patients (48%) showed relative growth of lesion volume. In multivariate analysis a left affected hemisphere side and a high collateral grade on CTA at baseline were associated with an increase of relative lesion growth after 24 hours, with an OR of respectively 2.7 (p = 0.006, 95%CI:1.9–4.7) and 1.7 (p = 0.012, 95%CI:1.2–2.8).
Conclusions: Good collateral capacity and left sided arterial occlusion are associated with relative infarct growth after 24 hours. Good collateral capacity also was associated with smaller infarcts, which may explain the more frequent relative growth.
AS01-038
ACUTE THROMBECTOMY TRIALS - IMAGING PREDICTORS OF OUTCOME
Oral
VESSEL PATENCY AT 24 HOURS AND ITS RELATIONSHIP WITH CLINICAL OUTCOMES AND 24 HOURS INFARCT VOLUME IN REVASCAT TRIAL
M. Millan1, S. Remollo1, H. Quesada2, A. Renú3, A. Tomasello4, N. Pérez de la Ossa1, M. Rubiera4, L. Llull3, P. Cardona2, M. Hernández-Pérez1, E. Cobo5, T. Jovin6 and A. Dávalos1
1Germans Trias i Pujol Hospital, Neuroscience, Badalona, Spain
2Bellvitge Hospital, Neurology, Hospitalet del Llobregat, Spain
5Universitat Politecnica de Catalunya, Statistics, Barcelona, Spain
6UPMC, Stroke Institute, Pittsburg, USA
Abstract
Background: We aimed to assess 24-hour revascularization rates by treatment groups and occlusion site as they related to clinical outcome and 24 hour infarct volume in REVASCAT.
Methods: Independent corelab adjudicated vessel status according to AOL (Arterial Occlusive Lesion) classification at 24 h on CT/MR (94.2%/5.8%) angiography and 24 h infarct volume on CT were studied in 95/103 patients in Solitaire arm and 94/103 in control arm. Complete revascularization (CR) was defined as AOL grade 3. Its effect on clinical outcome (distribution of mRS scores at 90 days) was analyzed by ordinal logistic regression.
Results: CR was achieved in 70.5% of the Solitaire group and in 22.3% of the control group (p < 0.0001). Table outlines differences in CR between Solitaire and control groups by baseline vessel occlusion location and t-PA treatment. CR was associated with improved outcome in both Solitaire (adjusted OR, 6.6; 95%CI, 2.7 to 16.1) and control groups (aOR, 2.7; 1.1 to 6.6). Significant differences were found in median infarct volume when revascularization included AOL 2&3 (12 vs 92 cc in Solitaire and 14 vs 58 cc in controls) with a non-significant trend in patients with CR (14.3 vs 17.7 cc and 18.1 vs 42.2 cc respectively).
Conclusions: CR at 24 hours is a powerful predictor of favorable clinical outcome while revascularization of any type resulted in reduced infarct volume in both thrombectomy and control groups.
AS01-045
ACUTE THROMBECTOMY TRIALS - IMAGING PREDICTORS OF OUTCOME
Oral
CLINICAL-IMAGING MISMATCH VERSUS PERFUSION IMAGING MISMATCH SELECTION FOR STROKE PATIENTS UNDERGOING MECHANICAL THROMBECTOMY: A POST-HOC ANALYSIS OF THE SWIFT PRIME TRIAL
R.G. Nogueira1, D.C. Haussen2, G.W. Albers3, C. Cognard4, D.S. Liebeskind5, T.G. Jovin6, H.P. Mattle7, D.R. Yavagal8, M. Goyal9 and J.L. Saver10
1Grady Memorial Hospital- Emory University School of Medicine, Department of Neurology, Atlanta, USA
2Marcus Stroke and Neuroscience Center- Grady Memorial Hospital/Emory University School of Medicine, Department of Neurology, Atlanta, USA
3Stanford University School of Medicine, Department of Neurology and Neurological Sciences, Stanford, USA
4University Hospital of Toulouse, Department of Diagnostic and Therapeutic Neuroradiology, Toulouse, France
5University of California Los Angeles, Neurovascular Imaging Research Core and UCLA Stroke Center, Los Angeles, USA
6University of Pittsburgh Medical Center, Department of Neurology, Pittsburgh, USA
7Inselspital- University of Bern, Department of Neurology, Bern, Switzerland
8University of Miami Miller School of Medicine / Jackson Memorial Hospital, Department of Neurology and Neurosurgery, Miami, USA
9University of Calgary, Departments of Radiology and Clinical Neurosciences, Calgary, Canada
10David Geffen School of Medicine at the University of California Los Angeles, Department of Neurology and Comprehensive Stroke Center, Los Angeles, USA
Abstract
Background: The optimal approach to select patients for acute stroke reperfusion therapy remains elusive. We compared the treatment effects of endovascular therapy vs. best medical treatment applying different selection modalities in the SWIFT Prime trial cohort.
Methods: Patients were classified as matching vs. not-matching three selection methods: (A)Perfusion-Imaging Mismatch (PIM, all criteria must be fulfilled): (1)Core Lesion ≤ 50 cc, (2)Severe hypoperfusion lesion (Tmax > 10 sec) < 100 cc, (3)Mismatch (Tmax > 6 sec lesion – core lesion) ≥ 15 cc and ratio > 1.8; (B)Clinical-Core Mismatch (CCM, one of the following criteria): (1)NIHSS ≥ 10 and core infarct<31 cc(age < 80years),(2)NIHSS ≥ 20 and core infarct < 51 cc (age < 80years), (3)NIHSS ≥ 10 and core infarct<21 cc (age ≥ 80 years); (C)Clinical-ASPECTS Mismatch (CAM): NIHSS ≥ 10 and ASPECTS > 5.The treatment effect of endovascular therapy was analyzed across the different groups.
Results: 155 patients qualified. PIM, CCM, and CAM were present in 84.5%(n = 131), 87.1%(n = 135), and 88.4%(n = 137) of the patients, respectively. There were no significant differences across the CCM+/CCM- vs. PIM+/PIM-(p = 0.49), CCM+/CCM- vs. CAM+/CAM-(p = 0.56), and PIM+/PIM- vs. CAM+/CAM-(p = 0.35) groups. Numerically, PIM had the lowest number of qualifying patients and the highest disagreement (15 PIM+/CCM-; 19 PIM-/ CCM+; 18 PIM+/CAM-; 24 PIM-/ CAM+; 5 CCM+/CAM-; 7 CCM-/ CAM+). All methods demonstrated a significant treatment effect in mismatch+ patients(Table). CCM had a trend toward the largest treatment gradient across mismatch+ vs. mismatch- patients (gradient %absolute difference/OR: CCM:16.2%/1.3 vs. PIM:6.9%/0.62 vs. CAM:-3.5%/-0.79).
Conclusions: Clinical outcomes and endovascular treatment effects in SWIFT PRIME did not differ based on clinical-imaging and perfusion-imaging mismatch selection criteria.
AS01-061
ACUTE THROMBECTOMY TRIALS - IMAGING PREDICTORS OF OUTCOME
Oral
IMPACT OF HYPERDENSE CLOT LENGTH ON OUTCOMES AFTER INTRA-ARTERIAL THROMBECTOMY IN THE THERAPY TRIAL
A. Yoo1, J. Mocco2, O. Zaidat3, P. Khatri4, R. Gupta5, D. Frei6, D. Lopes7, H. Shownkeen8, O. Berkhemer9, D. Meyer10, M. Chauke10, S. Hak10, S. Kuo10, H. Buell10, A. Bose10, S.P. Sit10 and R. von Kummer11
1Texas Stroke Institute, Radiology, Plano, USA
2Mount Sinai Health System, Neurosurgery, Neurosurgery, USA
3St. Vincent Mercy Hospital, Endovascular Neurosurgery & Stroke, Toledo, USA
4University of Cincinnati, Neurology, Cincinnati, USA
5WellStar Health System, Neuroradiology, Marietta, USA
6Swedish Medical Center, Neuroradiology, Englewood, USA
7Rush University, Neurosurgery, Chicago, USA
8Central DuPage Hospital, Neuroradiology, Winfield, USA
9Academic Medical Center Amsterdam, Radiology, Amsterdam, Netherlands
10Penumbra Inc., Clinical Affairs, Alameda, USA
11Universitätsklinikum Carl Gustav Carus, Neuroradiology, Dresden, Germany
Abstract
Background: Increasing clot length reduces the chance of recanalization after IV thrombolysis. Limited data are available for intra-arterial therapy (IAT). The benefits of aspiration thrombectomy relative to IV rtPA may be greater at longer clot length.
Methods: THERAPY was a randomized controlled trial of aspiration thrombectomy plus IV rtPA versus IV rtPA alone in large vessel stroke patients with hyperdense clot length (HCL) ≥8 mm. Uni- and multivariate analyses assessed the association of clot length with primary and secondary trial endpoints. In multivariate ordinal regression for 90-day mRS, multiplicative interaction was assessed between treatment allocation and HCL.
Results: For 108 patients, occlusion locations were 28% ICA, 62% MCA M1, and 10% MCA M2. Median HCL was 14.0 mm (IQR 9.7–19.5). Longer HCL was associated with higher 90-day mRS (p = 0.02) and worse clinical outcomes for all dichotomized endpoints (all p < 0.05, except mRS 0–2). Longer HCL had higher rates of serious adverse events (p = 0.03), mortality (p = 0.04) and longer procedural time (rho = 0.36, p < 0.05). There was no significant relationship with mTICI 2b-3 reperfusion.
With increasing clot length, there was a greater relative benefit of IAT over IV rtPA alone (interaction term p = 0.03; figure). This was related to a stronger adverse effect of increasing HCL on 90-day mRS for IV rtPA (rho = 0.39, p = 0.009) compared to IAT (rho = 0.19, p = 0.19).
Conclusions: Greater hyperdense clot length is a negative prognostic marker in stroke patients with large vessel occlusion. This effect is less pronounced with intra-arterial treatment, leading to a greater relative benefit of IAT over IV rtPA alone with increasing clot length.
AS18-008
ATRIAL FIBRILLATION
Oral
PREDICTORS OF HIGHER ARRHYTMIC LOAD IN PATIENTS WITH CRYPTOGENIC STROKE AND COVERT ATRIAL FIBRILLATION DETECTED BY IMPLANTABLE LOOP RECORDERS
M. de Lera1, G. Largaespada2, E. Cortijo1, M. Sandín2, A. Calleja1, E. García2, E. Rojo1, L. López-Mesonero1, P. García-Bermejo1, M. Usero1, A. Juanatey1, L. Bautista1, J. Rubio2 and J.F. Arenillas1
1Hospital Clínico Universitario de Valladolid, Servicio de Neurología, Valladolid, Spain
2Hospital Clínico Universitario de Valladolid, Servicio de Cardiología, Valladolid, Spain
Abstract
Background: Implantable loop recorders (ILR) may allow detection of covert paroxysmal atrial fibrillation (cpAF) in patients with embolic strokes of undetermined source (ESUS). Arrhythmic load (AL) may help establish a causal relationship between cpAF episodes and ESUS. We aimed to identify baseline predictors of a higher AL in ESUS patients undergoing ILR monitoring.
Methods: We studied consecutive ischemic stroke patients fulfilling ESUS criteria who underwent ILR after complete diagnostic work-up. Baseline variables included clinical, neuroimaging, cerebral large-artery atherosclerosis status, EKG, echocardiography measures and 24 hour-Holter-EKG parameters. Long-term clinical and online follow-up was performed to detect >2 min cpAF episodes. We looked for predictors of repeated vs. single AF episodes as an estimation of a higher AL.
Results: Between October 2010 and May 2015, we included 163 ESUS patients (mean age 67 years, 55% men). Mean follow-up after device implantation was 616 ± 340 days. Confirmed cpAF episodes were detected in 69 (42%) patients, of whom 48 presented repeated AF episodes, vs. 21 who had isolated AF events. Adjusted logistic regression models revealed that female sex (OR 8.4 [1.1–6.4], p = 0.04), shorter time to first event detection (OR 0.9 [0.98–0.99], p = 0.016) and number of supraventricular paroxysmal tachycardia events on 24 hour Holter-EKG (OR 2.1 [1.1–3.1]; p = 0.015) were predictors of a higher AL.
Conclusions: Female sex, precocity of first cpAF event detection and a higher number of supraventricular paroxysmal tachycardia events on 24-hour Holter-EKG, emerged as predictors of a higher AL in ESUS patients studied with ILR.
AS06-012
ATRIAL FIBRILLATION
Oral
DETECTION OF ATRIAL FIBRILLATION AMONG PATIENTS WITH STROKE DUE TO LARGE OR SMALL VESSEL DISEASE: A META-ANALYSIS
J. Demeestere1, M. Lansberg2 and R. Lemmens1
1Catholic University of Leuven, Neurology, Leuven, Belgium
2Stanford University of Medicine, Stanford Stroke Center-, Stanford, USA
Abstract
Background: Recent trials have demonstrated that extended cardiac monitoring increases the yield of paroxysmal AF detection in patients with cryptogenic stroke. The utility of extended cardiac monitoring is uncertain in patients with stroke caused by small and large vessel disease. We conducted a meta-analysis to estimate the yield of AF detection in this population.
Methods: We searched Pubmed for studies on AF detection in stroke patients and excluded studies reporting exclusively on findings in cryptogenic stroke patients. From the included studies, we abstracted the AF detection rates for three populations grouped by stroke etiology: large vessel stroke, small vessel stroke or undefined stroke etiology.
Results: Our search yielded 21 studies (n = 5983), nine (n = 3175) reported rates of AF detection according to stroke subtype; the other twelve (n = 2808) reported the rate of AF detection in aggregate for the overall stroke population (i.e. undefined stroke etiology). AF detection rates were similar in patients with large vessel (3.5%, 95%CI 1.1–7.4) and small vessel stroke (2.4%, 95%CI 0.2–6.8). The yield of AF detection among patients with undefined stroke etiology was higher (10.0%; 95%CI 7.7–12.6) compared to patients with small vessel stroke (p = 0.01) and patients with large vessel stroke (p = 0.03).
Conclusions: Studies of AF detection show similar rates of AF detection in patients with small and large vessel strokes (2.4 – 3.5%). Randomized controlled trials are needed to examine the utility of AF detection with long-term cardiac monitoring (>7 days) in patients with presumed small and large vessel disease stroke.
AS06-016
ATRIAL FIBRILLATION
Oral
ATRIAL FIBRILLATION PATTERN MIGHT INFLUENCE THE RISK OF ISCHAEMIC STROKE AN UPDATED META-ANALYSIS
F. Fortuni1, F. Angelini2 and V. Caso1
1University of Perugia- Santa Maria della Misericordia Hospital, Stroke Unit and Division of Internal and Cardiovascular Medicine, Perugia, Italy
2University of Perugia, Faculty of Medicine, Perugia, Italy
Abstract
Background: Atrial fibrillation (AF) pattern has not been taken into account for the choice of stroke prophylaxis, as it remains unclear whether patients with persistent or permanent AF (SAF) are at higher risk compared to those with paroxysmal AF (PAF).
Aim: to detect if AF pattern has an impact on the risk of ischaemic stroke and systemic embolic events (SSE).
Methods: We systematically searched PubMed for recent studies that had analysed the influence of different AF patterns on occurrence of ischaemic stroke or SEE as primary objective. To be included, these studies had to report on event rates related to the AF pattern as classified by the ACC/AHA/ESC 2006 Guidelines.
Results: 6 studies fully met our inclusion criteria. Overall, 12,723 patients with PAF and 46,622 patients with SAF were studied according to use of oral anticoagulants.
The risk of ischaemic stroke and SEE was lower for patients with PAF than for those with SAF in all analyses (OR = 0.77; 95% CI 0.67 – 0.89 with OAC; OR = 0.58; 95% CI 0.49- 0.70 without OAC).
Conclusions: Based on this meta-analysis, patients with PAF bear a lower risk than those with SAF. However, this is likely due to a lower global risk profile, more common in patients with PAF. In fact, PAF has been identified as first stage of a progressive disease by some authors.
AS13-021
ATRIAL FIBRILLATION
Oral
TRENDS IN THE PREVALENCE AND MANAGEMENT OF PRE-STROKE ATRIAL FIBRILLATION
V. Jain1, I. Marshall2, C.D.A. Wolfe2,3
1King's College London, School of Medicine and Life Sciences, London, United Kingdom
2King's College London, Division of Health and Social Care Research, London, United Kingdom
3National Institute for Health Research Comprehensive Biomedical Research Centre, Guy’s & St. Thomas’ NHS Foundation Trust and King’s College London, London, United Kingdom
Abstract
Background: Anticoagulation is widely recommended in atrial fibrillation (AF), over antiplatelet. This study sought to examine changes in the quality of management of AF prior-to-stroke over time, and reasons for suboptimal treatment.
Methods: The South London Stroke Register (SLSR) is an ongoing population-based register recording first-in-a-lifetime stroke. Of 5041 patients, 816 (16.2%) were diagnosed with AF before their stroke. Trends in the prevalence of AF, and antithrombotic medication prescribed before stroke, were investigated from 1995 to 2014. Multivariable logistic regression analyses were conducted to investigate factors associated with inappropriate management.
Results: The proportion of patients diagnosed with AF prior to stroke significantly increased from 1999 to 2014 (p = 0.003). Black ethnic patients comprised an increasing proportion of AF-related stroke, from 5% in 1995–1998 to over 25% by 2011–2014 (p < 0.001). Anticoagulant prescription in those at high-risk of stroke (CHADS2 score [≥2]) increased from 9% (1995–1998) to 32% (2011–2014) (p < 0.001). Antiplatelet prescription was more common throughout all time periods. Elderly patients (>65) were significantly less likely to be prescribed an anticoagulant (Table 1). Alcohol consumption (≥8 units/week) and past TIA were associated with antiplatelet prescription (OR 1.67 [95% CI 0.97–2.88] and OR 2.36 [95% CI 1.51–3.69] respectively).
Conclusions: Despite modest improvements over time, most AF-related strokes still occur in people who could have been identified as high-risk before their stroke, yet were not prescribed optimal preventative treatment.
AS18-023
ATRIAL FIBRILLATION
Oral
POPULATION-BASED PROGNOSTIC STUDY OF A POLICY OF NON-ANTICOAGULATION OF TIA/STROKE PATIENTS WITH BRIEF EPISODES OF ATRIAL FIBRILLATION ON 5-DAY HOME-MONITORING
S.M. Lyons1, M.M. Kubiak1, G. Lau1, L. Li1, N. Lovett1, G.S. Yiin1 and P.M. Rothwell on behalf of the Oxford Vascular Study
1
1Stroke Prevention Research Unit, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
Abstract
Background: Atrial fibrillation (AF) is a risk factor for recurrent stroke. However, the clinical relevance of brief episodes of paroxysmal AF (pAF) detected on monitoring is uncertain. In particular, the appropriate thresholds for anticoagulation in terms of frequency and duration of pAF have not yet been determined. We therefore assessed the prognosis of patients with recent TIA and non-disabling stroke who had brief pAF (<2 min) on 5-day monitoring.
Methods: In a population based study (Oxford Vascular Study), consecutive eligible consenting patients underwent 5-day outpatient cardiac rhythm monitoring (Novacor R-Test) at one-month follow-up. Patients with AF < 2 minutes were not anticoagulated unless there were other factors suggestive of cardio-embolic cause (multi-territory infarct or echocardiographic abnormality). Patients were followed for recurrent TIA/stroke/death.
Results: Among 627 patients (mean/range age = 68.7/21–98) who underwent monitoring, 109 (17%) had recurrent neurovascular events (30 stroke; 79 TIA only) and 31 died during 1663 patient-years of follow-up. pAF was detected in 115 (18.3%), with longest episode <2 minutes in 72 (62.2%). Of these 72, 8 had other evidence of likely cardioembolism and were anticoagulated. The risk of recurrent stroke in the remaining 64 non-anticoagulated patients with pAF < 2-mins was no greater than in patients without pAF (stroke - HR = 0.68, 95%CI 0.23–2.03; stroke/TIA - 0.91, 0.47–1.77; death - 0.76, 0.26–2.23).
Conclusions: Managing patients with monitoring-detected pAF < 2 minutes without anticoagulation did not confer a clearly increased risk of recurrent stroke or death. Such a policy is therefore feasible and ethical for larger prognostic studies and for placebo-controlled randomised trials of anticoagulation.
AS18-028
ATRIAL FIBRILLATION
Oral
EMBOLIC STROKE OF UNDETERMINED SOURCE AND DETECTION OF ATRIAL FIBRILLATION ON FOLLOW-UP: HOW MUCH CAUSALITY IS THERE?
G. Ntaios1, V. Papavasileiou2, G. Lip3, H. Milionis4, K. Makaritsis1, A. Vemmou5, E. Koroboki5, E. Manios5, K. Spengos6, P. Michel7 and K. Vemmos5
1University of Thessaly, Department of Medicine, Larissa, Greece
2Salford Royal NHS Foundation Trust- Manchester Academic Health Sciences Centre- Salford Royal Foundation Trust, Comprehensive Stroke Centre, Manchester, United Kingdom
3University of Birmingham- City Hospital, Centre for Cardiovascular Sciences, Birmingham, United Kingdom
4Department of Internal Medicine, University of Ioannina, Ioannina, Greece
5Alexandra Hospital, Department of Clinical Therapeutics, Athens, Greece
6Eginition Hospital- University of Athens Medical School, Department of Neurology, Athens, Greece
7Centre Hospitalier Universitaire Vaudois and University of Lausanne, Stroke Center- Neurology Service, Lausanne, Switzerland
Abstract
Background: Strokes related to atrial fibrillation (AF) are more severe than strokes of other etiologies. In this context, we aimed to compare stroke severity between patients with embolic stroke of undetermined source (ESUS) diagnosed with AF during follow-up and those who were not; we hypothesized that, if AF episodes detected during follow-up are indeed causally associated with the index event, stroke severity in the AF group should be higher than the non-AF group.
Methods: Dataset was derived from the Athens Stroke Registry. ESUS was defined by the Cryptogenic Stroke/ESUS International Working Group criteria. Stroke severity was assessed with the NIHSS score. Cumulative probabilities of recurrent stroke or peripheral embolism in the AF and non-AF ESUS groups were estimated by Kaplan–Meier analyses.
Results: Among 275 ESUS patients, AF was detected during follow-up in 80 (29.1%), either during repeated ECG monitoring (18.2%) or during hospitalization for stroke recurrence (10.9%). NIHSS was similar between the two groups [5 (2–13) vs. 5 (2–14), p = 0.998].
More recurrent strokes or peripheral embolisms occurred in the AF group compared to the non-AF [42.5% vs. 13.3%, p = 0.001].
In a sensitivity analysis including only patients discharged on antiplatelet, Kaplan-Meier analysis and the Cox-regression analysis (HR: 3.37, 95%CI: 1.77–6.43) gave similar results.
Conclusions: Stroke severity is similar between ESUS patients who were diagnosed with AF during follow-up and those who were not. Given that AF-related strokes are more severe than strokes of other etiologies, this finding challenges the assumption that the association between ESUS and AF detected during follow-up is as frequently causal as regarded.
AS17-056
ATRIAL FIBRILLATION
Oral
RISK STRATIFICATION FOR RECURRENCE AND MORTALITY IN EMBOLIC STROKE OF UNDETERMINED SOURCE
G. Ntaios1, K. Vemmos2, G. Lip3, A. Rodríguez-Campello4, E. Giralt-Steinhauer4, V. Arnao5, V. Caso5, M. Paciaroni5, E. Diez-Tejedor6, B. Fuentes6, A. Arauz7, S.F. Ameriso8, M. Hawkes8, F. Bandini9, A. García Pastor10, J. Putaala11, T. Tatlisumak12, M. Barboza13, G. Athanasakis1 and V. Papavasileiou14
1University of Thessaly, Department of Medicine, Larissa, Greece
2Alexandra Hospital, Department of Clinical Therapeutics, Athens, Greece
3University of Birmingham, Institute of Cardiovascular Sciences, Birmingham, United Kingdom
4Hospital del Mar. Neurovascular Research Group- IMIM-Hospital del Mar Institut Hospital del Mar d'Investigacions Mèdiques- Universitat Autònoma de Barcelona, Stroke Unit- Department of Neurology, Barcelona, Spain
5University of Perugia, Stroke Unit, Perugia, Italy
6La Paz University Hospital - Autónoma University of Madrid- IdiPAZ Health Research Institute, Department of Neurology and Stroke Center, Madrid, Spain
7Instituto Nacional de Neurología y Neurocirugía Manuel Velasco Suárez, Stroke Clinic, Mexico city, Mexico
8Institute for Neurological Research- FLENI-, Department of Neurology, Buenos Aires, Argentina
9S. Paolo Hospital, Department of Neurology, Savona, Italy
10Hospital General Universitario Gregorio Marañón- IiSGM Health Research Institute- Universidad Complutense de Madrid, Vascular Neurology Section- Stroke Center, Madrid, Spain
11Helsinki university Central Hospital and University of Helsinki, Department of Neurology, Helsinki, Finland
12Sahlgrenska University Hospital, Department of Neurology, Gothenburg, Sweden
13Hospital Dr. Rafael A. Calderón Guardia- CCSS. University of Costa Rica, Neurosciences Departmen, Costa Rica, Costa Rica
14Salford Royal NHS Foundation Trust- Manchester Academic Health Sciences Centre- Salford Royal Foundation Trust, Comprehensive Stroke Centre, Manchester, United Kingdom
Abstract
Background: The risk of stroke recurrence in patients with embolic stroke of undetermined source (ESUS) is high and the optimal antithrombotic strategy for secondary prevention is not clear.
Methods: We pooled datasets of 11 stroke registries from Europe and America. ESUS was defined according to the Cryptogenic Stroke/ESUS International Working Group. Cox-regression analyses were performed to investigate if pre-stroke CHADS2 and CHA2DS2-VASc scores were independently associated with the risk for ischemic stroke/TIA recurrence or death. The Kaplan–Meier product limit method was used to estimate the cumulative probability of ischemic stroke/TIA recurrence and death in different strata of the CHADS2 and CHA2DS2-VASc scores.
Results: 159 (14.5%) ischemic stroke/TIA recurrences and 148 (13.5%) deaths occurred in 1095 patients (median age 68 years) followed-up for a mean of 36 months.
Compared to CHADS2 = 0, patients with CHADS2 = 1 and CHADS2 > 1 had higher risk for ischemic stroke/TIA recurrence (HR: 2.38, 95%CI: 1.41–4.00 and HR: 2.72, 95%CI: 1.68–4.40, respectively) and death (HR: 3.58, 95%CI: 1.80–7.12, and HR: 5.45, 95%CI: 2.86–10.40, respectively). Compared to low-risk CHA2DS2-VASc, patients with high-risk CHA2DS2-VASc had higher risk for ischemic stroke/TIA recurrence (HR: 3.35, 95%CI: 1.94–5.80) and death (HR: 13.0, 95%CI: 4.7–35.4).
Conclusions: The risk of recurrent ischemic stroke/TIA and death in ESUS is reliably stratified by CHADS2 and CHA2DS2-VASc scores. Compared to the low-risk group, patients in the high-risk CHA2DS2-VASc group have much higher risk of ischemic stroke recurrence/TIA and death, approximately 3-fold and 13-fold respectively.
AS18-040
ATRIAL FIBRILLATION
Oral
DURATION OF PAROXYSMAL ATRIAL FIBRILLATION IN CRYPTOGENIC STROKE IS NOT ASSOCIATED WITH STROKE SEVERITY AND EARLY OUTCOMES
C. Liantinioti1, K. Tympas2, M. Chondrogianni1, C. Zompola1, G. Papadimitropoulos1, A. Papa1,3, A. Katsanos1,4, S. Triantafyllou1, A. Roussopoulou1,5, K. Voumvourakis1, J. Parissis2 and G. Tsivgoulis1
1School of Medicine - University of Athens, Second Department of Neurology, Athens, Greece
2School of Medicine - University of Athens, Second Department of Cardiology, Athens, Greece
3School of Medince - University of Thessaly, Department of Neurology, Larissa, Greece
4School of Medicine - University of Ioannina, Department of Neurology, Ioannina, Greece
5“Evangelismos” General Hospital, Department of Neurology, Athens, Greece
Abstract
Background: The current AHA definition of PAF requires an arbitrary cut-off of >30 sec of AF, but in clinical practice cryptogenic stroke (CS) patients with PAF duration of ≤30 sec are not usually excluded from anticoagulation therapy. We sought to evaluate the clinical relevance of short-duration (≤30 sec) PAF in CS.
Methods: Consecutive CS patients (defined using TOAST criteria) with no prior AF history and sinus-rhythm on baseline-ECG were prospectively evaluated over a three-year period. Baseline stroke severity was assessed by NIHSS-scores. All patients underwent 24-hour Holter-electrocardiography during hospitalization. ECG recordings were analyzed by two blinded investigators using dedicated analysis software. Total time in AF was calculated as the sum of each individual AF episode for patients with multiple episodes during monitoring. Patients were dichotomized in two groups using PAF total duration (≤30 sec & >30 sec). Early recurrent stroke and favorable functional outcome (FFO, defined as mRS-grades of 0–1) were evaluated during a three-month follow-up period.
Results: A total of 184 patients (66% men, mean age 57 ± 11years) with CS (median NIHSS-score 4, IQR: 2–7) were evaluated. PAF of any duration was detected in 23 individuals (13%; 95%CI:8%-18%). Among these patients the prevalence of brief PAF was 57% (n = 13). The two groups did not differ (p > 0.2) in terms of demographics, vascular risk factors and NIHSS-scores. Early recurrent stroke and FFO rates were similar (p > 0.4) in the two groups.
Conclusions: Duration of PAF is not associated with baseline stroke severity and early outcomes in patients with CS and should not influence anticoagulation decision in these patients.
AS18-048
ATRIAL FIBRILLATION
Oral
ATRIAL FIBRILLATION DETECTION RATES IN PATIENTS WITH CRYPTOGENIC STROKE: A COMPARISON OF THE CRYSTAL-AF AND EMBRACE TRIALS
T. Sanna1, R. Bernstein2, J. Brachmann3, H.C. Diener4, V. Di Lazzaro5, C. Morillo6, R. Passman7, M. Rymer8, V. Thijs9, S. Liu10 and P. Ziegler11
1Catholic University of the Sacred Heart, Institute of Cardiology, Rome, Italy
2Northwestern University Feinberg School of Medicine, Davee Department of Neurology, Chicago, USA
4University Hospital Essen, Department of Neurology and Stroke Center, Essen, Germany
5Campus Bio-Medico University, Institute of Neurology, Rome, Italy
6Population Health Research Institute- McMaster University, Cardiology, Hamilton, Canada
7Northwestern University Feinberg School of Medicine, Bluhm Cardiovascular Institute, Chicago, USA
8University of Kansas Medical Center, Neurology, Kansas City, USA
9Florey Institute of Neuroscience and Mental Health, Neurology, Heidelberg, Australia
10Medtronic, Cardiac Rhythm Heart Failure, Mounds View, USA
11Medtronic, Diagnostics and Monitoring Research, Mounds View, USA
Abstract
Background: Detection rates of atrial fibrillation (AF) in cryptogenic stroke patients depend on many factors, making direct comparisons between studies difficult. We compared AF detection rates between the intervention arms of CRYSTAL-AF and EMBRACE after adjusting for differences in age, minimum AF episode duration, and follow-up duration.
Methods: Patients ≥55 years from the insertable cardiac monitor (ICM) arm of CRYSTAL-AF were included in this analysis. AF detection rates were computed at 90 days and 3 years using Kaplan-Meier estimates. Published AF detection rates at 90 days from the event monitor arm of EMBRACE (all ≥55 years) were used for comparison. The ICM is capable of detecting AF episodes lasting ≥2 minutes and therefore was compared to a secondary endpoint definition of 2.5 minutes in EMBRACE.
Results: A total of 158 patients (65% male, age 67 ± 8 years) from CRYSTAL-AF and 284 patients (54% male, age 73 ± 9 years) from EMBRACE were included. AF detection rates at 90 days were 10.0% and 9.9% in the intervention arms of CRYSTAL-AF and EMBRACE, respectively. By 3 years, the AF detection rate was 33.5% in this subset of CRYSTAL-AF patients, while no data were available beyond 90 days in the EMBRACE study.
Conclusions: AF detection rates were remarkably similar over the short-term in the intervention arms of CRYSTAL-AF and EMBRACE after adjusting for differences in age, AF definition, and follow-up duration. Whether the long-term monitoring capabilities afforded by ICMs can result in improved clinical outcomes compared to shorter-term event recorders in cryptogenic stroke patients requires further evaluation.
AS17-016
CEREBRAL HAEMORRHAGE 2
Oral
HAEMORRHAGE LOCATION INFLUENCES QUALITY OF LIFE AND DISABILITY AFTER INTRACEREBRAL HAEMORRHAGE IN THE INTERACT2 STUDY
C. Delcourt1, S. Sato1, E. Sandset2, D. Zheng1, X. Chen1, M. Hackett1, H. Arima1, E. Heeley1, Y. Huang3, R. Al Shahi-Salman4, T. Robinson5, P. Lavados6, R. Lindley1, C. Stapf7, J. Chalmers8 and C. Anderson1
1The George Institute, Neurology and Mental Health, Sydney, Australia
2Oslo University Hospital, Department of Medicine, Oslo, Norway
3Peking University First hospital, Department of Neurology, Beijing, China
4University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
5University of Leicester, Department of Cardiovascular Sciences and NIHR Biomedical Research Unit for Cardiovascular Diseases, Leicester, United Kingdom
6Clinica Alemana- Universidad del Desarrollo- Universidad de Chile, Neurology, Santiago, Chile
7University of Montreal, Department of Neurosciences- CRCHUM, Montreal, Canada
8The George Institute, Cardiovascular, Sydney, Australia
Abstract
Background: The influence of location of intracerebral haemorrhage (ICH) on outcome is uncertain. We investigated associations between ICH location and death/disability or health-related quality of life (HRQoL) in the Intensive Blood pressure Reduction in Acute Cerebral haemorrhage Trial (INTERACT2).
Methods: In patients with baseline brain CT, we assessed associations between ICH location and death/disability (modified Rankin Scale score) or HRQoL (European Quality of Life Scale [EQ-5D]) at 90 days after randomisation in logistic regression models (adjusted for clinically relevant factors), using odds ratios (OR) and 95% confidence intervals (CI).
Results: Among 2,066 patients, posterior limb of internal capsule was associated with death/disability (OR 2.10, 95%CI 1.65–2.68) and disability alone (OR 1.82, 95%CI 1.45–2.27); thalamic ICh was associated with death/disability (OR 2.24, 95%CI 1.40–3.57) and death alone (OR 1.98, 95%CI 1.19–3.29). Posterior limb of the internal capsule, thalamus, and infratentorial locations were associated with poor HRQoL utility score (≤0.7) (OR 2.04, 95%CI 1.27–3.29; OR 1.94, 95%CI 1.51–2.49; OR 2.75, 95%CI 1.49–5.07, respectively). ICH in posterior limb of internal capsule was strongly associated with all HRQoL domains, though thalamus and infratentorial locations were associated with poor HRQoL domains of mobility, self-care and usual activity.
Conclusions: ICHs in the posterior limb of the internal capsule, thalamus, and infratentorial locations are associated with death/disability or poor HRQoL at 90 days.
AS27-005
CEREBRAL HAEMORRHAGE 2
Oral
PREDICTORS OF OUTCOME IN ANEURYSMAL SUBARACHNOID HAEMORRHAGE (aSAH) PATIENTS: OBSERVATIONS FROM A LARGE, CONTEMPORARY MULTI-CENTRE DATASET
H. Patel1, J. Galea2 and L. Dulhanty1
1University of Manchester, Department of Neurosurgery, Manchester, United Kingdom
2Ninewells Medical School, Division of Neurosciences, Dundee, United Kingdom
Abstract
Background: The mortality and morbidity following aSAH has improved because of better diagnosis and early treatment to secure the aneurysm. In light of these improvements in care, it is not clear if the independent predictors of a negative outcome have changed.
The aim of this study was to identify the independent predictors of an unfavourable outcome (Glasgow Outcome Score 1, 2 & 3) in aSAH patients.
Methods: Univariate and multivariate analysis of prospectively collected data on patients presenting with aSAH was performed. Outcome was assessed at discharge. Data was collected from 14 centres in the United Kingdom over a period of 4 years (September 2011–2015).
Results: The mean age (SD) of presentation of 3489 patients with aSAH was 55.3 (0.4). Most patients were female (69%), presented in good grade (2397 (70%)) (World Federation of Neurological Surgeons (WFNS) grade 1&2), and were treated by endovascular coiling (72%).
The independent predictors of outcome were age (p < 0.001), WFNS grade (p < 0.001) re-bleeding (p < 0001) need for CSF diversion (p < 0.001) and DCI (p < 0.001).
Conclusions: These data suggest that potentially modifiable risk factors of re-bleeding (OR 0.1 CI 0.01–0.15 p < 0.001) and DCI (0.55 OR CI 0.44–0.70 p < 0.001) remain barriers to favourable outcomes. Understanding the reasons why patients requiring CSF diversion have an almost 7-fold higher adjusted odds (OR 0.95 CI 0.95–0.96 p < 0.001) of a poor outcome needs to be studied.
ESOC6-1465
CEREBRAL HAEMORRHAGE 2
Oral
CLEAR III: PATTERNS OF EXTERNAL VENTRICULAR DRAINAGE UTILIZATION RELATE TO IVH REMOVAL AND ICP CONTROL
I. Awad1, W. ziai2, B. Gregson3, D. Mendelow4, K. Lees5, J. Dawson5, A. Mould2, K. Lane2, N. McBee2, P. Keyl2, J. Betz6, E. Sugar6, G. Yenokyan6, S. Harnof7, M. Rosenblum6, R. Thompson6 and D. Hanley2
1University of Chicago, Neurosurgery, Chicago, USA
2Johns Hopkins University, Neurology, Baltimore, USA
3Newcastle University, Neurosurgery, Newcastle Upon Tyne, United Kingdom
4Newcastle University, Neurosurgery, Newcastle, United Kingdom
5University of Glasgow, Neurology, Glasgow, United Kingdom
6Johns Hopkins University School of Public Health, Biostatistics, Baltimore, USA
7Sheba Medical Center, Neurosurgery, Ramat Gani, Israel
Abstract
Background: CLEAR III, a randomized, double-blinded, placebo-controlled trial, demonstrated benefits of extraventricular drainage (EVD) plus alteplase for intraventricular hemorrhage (IVH) removal and intracranial pressure (ICP) control to improve outcome in patients with severe IVH and small ICH. This report focuses on the mediation of mRS benefits at 365 days via IVH clot reduction.
Methods: ESO and AHA ICH Guidelines regarding utilization of ventricular catheters (levels 2 & 3) and ICP/CPP control were followed. Consented subjects received saline or alteplase Q8H via the EVD until at least the 3rd and 4th ventricles cleared (end of treatment (EOT)). Sites were encouraged to attempt >80% clot removal with protocolized options for multiple catheters and dosing up to 12 doses.
Results: Among patients receiving alteplase, significantly lower EOT volume was achieved with an EVD placed ipsilateral to the dominant IVH (p = 0.004) and when multiple EVDs were used in subjects with IVH ≥ 20 mL (diff. dual vs single p = 0.005). ICP and CPP events were independently associated with D30 and D180 mortality (p = 0.001; p = 0.04) and D30 poor functional outcome (CPP only; p = 0.04). In both groups, contralateral EVDs were less likely associated with ICP elevation (p = 0.049) in the adjusted models; but, in the alteplase group, the proportion of ICP/CPP events did not differ between ipsi and contra EVD (p = 0.63/p = 0.26).
Conclusions: Improved strategies for controlling ICP while removing IVH are needed to optimize good mRS status, including more frequent use of ipsilateral and dual catheters, and more vigorous dosing pursuing >85% IVH evacuation.
AS21-043
CEREBRAL HAEMORRHAGE 2
Oral
COMBINING MOTOR FUNCTION AND DIFFUSION TENSOR IMAGING DERIVED MEASURES PREDICT MOTOR OUTCOME IN PATIENTS WITH ACUTE INTRACEREBRAL HEMORRHAGE
J. Puig1, G. Blasco1, M. Terceño2, J. Serena2, M. Hernández-Pérez3, P. Daunis-i-Estadella4, V. Cuba1, G. Carbó1, A. Alberich-Bayarri5, G. Schlaug6, B. Menon7, M. Wintermark8, S. Pedraza1 and Y. Silva2
1Institut de Diagnostic per la Imatge Unitat de Recerca- Hospital Dr. Josep Trueta- Institut d'Investigació Biomèdica de Girona IDIBGI, Radiology, Girona, Spain
2Hospital Dr Josep Trueta- Institut d'Investigació Biomèdica de Girona IDIBGI, Neurology- Stroke Unit, Girona, Spain
3Hospital Germans Trias i Pujol University- Universitat Autònoma de Barcelona, Stroke Unit, Badalona, Spain
4Department of Computer Science- Applied Mathematics and Statistics, University of Girona, Girona, Spain
5Biomedical Imaging Research Group- QUIVIM, La Fe Polytechnics and University Hospital, Valencia, Spain
6Neuroimaging & Stroke Recovery Laboratory, Beth Israel Deaconess Medical Center- Harvard Medical School, Boston, USA
7Calgary Stroke Program- Department of Clinical Neurosciences, Hotchkiss Brain Institute- University of Calgary, Calgary, Canada
8Department of Radiology- Neuroradiology Division, Stanford University, Palo Alto California, USA
Abstract
Background: Over half of patients have residual motor deficits 3 months after intracerebral hemorrhage (ICH). We aimed to determine whether combining clinical scores and diffusion tensor imaging (DTI)-derived measures from the first few hours after symptom onset improves prediction of motor outcome in patients with ICH.
Methods: We prospectively studied consecutive patients within 12 hours of onset of primary ICH. Patients underwent multimodal MRI including DTI. We assessed ICH and perihematomal edema location and volume, and corticospinal tract (CST) involvement. We calculated ratios of affected-to-unaffected CST for fractional anisotropy (FA), mean diffusivity, and axial and radial diffusivities (Olea Sphere V.3.0). Paresis was graded by the motor subindex scores of the modified NIHSS (mNIHSS). Motor outcome at 3 months was classified as good (mNIHSS 0–3) or poor (mNIHSS 4–8). Poor functional outcome was defined as mRS >2.
Results: Of 62 consecutive patients, 49 were included in the study (37 men; median age 69.5 years, IQR 59–76). At admission, median NIHSS was 11.5 (IQR5–17), and 25 (71.4%) patients had some motor deficit (median mNIHSS 4 [IQR2–7]). At 3 months, 13 (22.41%) had poor motor outcome. Independent predictors of motor outcome were NIHSS, mNIHSS, rFA of the whole CST, posterior limb of internal capsule (PLIC) involvement by ICH, 72 h-NIHSS, and 72 h-mNIHSS. The sensitivity, specificity, and positive and negative predictive values for poor motor outcome at 3 months by combined mNIHSS > 6 and PLIC-involvement < 12 hours were 84%, 80%, 64%, and 94%, respectively (AUC = 0.91).
Conclusions: Combined assessment of motor function and PLIC damage during hyperacute ICH may predict motor outcome.
AS33-020
CEREBRAL HAEMORRHAGE 2
Oral
SEX DIFFERENCES FOR BLOOD PRESSURE LOWERING AND OUTCOME IN INTRACEREBRAL HAEMORRHAGE: INTERACT2 RESULTS
E.C. Sandset1, X. Wang2, C. Carcel2, S. Shoichiro2, C. Delcourt2, H. Arima2, C. Stapf3, T. Robinson4, P. Lavados5, J. Chalmers2 and C.S. Anderson2
1Oslo Universtiy Hospital, Department of Neurology, Oslo, Norway
2The George Institute for Global Health, University of Sydney, Sydney, Australia
3Université de Montréal, Centre de Recherche du Centre Hospitalier de l'Université de Montréal CRCHUM- Département de Neurosciences, Montreal, Canada
4University of Leicester, Department of Cardiovascular Sciences and NIHR Biomedical Research Unit in Cardiovascular Disease, Leicester, United Kingdom
5Clínica Alemana- Facultad de Medicina Clínica Alemana Universidad del Desarrollo, Unidad de Neurología vascular- Servicio de Neurología- Departamento de Medicina, Santiago, Chile
Abstract
Background: Variable degrees of sex differences have been observed for haematoma location and management of patients with acute intracerebral haemorrhage (ICH). We aimed to investigate potential sex differences in relation to the effect of BP lowering treatment on clinical outcomes among INTERACT2 participants.
Methods: INTERACT2 was an international, open, randomised controlled trial in patients with spontaneous ICH within 6 h of onset and elevated systolic BP (150–220 mmHg) who were allocated intensive (target SBP <140 mmHg within 1 h using intravenous agents) or guideline-recommended (SBP <180 mmHg) BP lowering treatment. We determined the effect of sex difference on haematoma growth at 24 hours and death or major disability at 90 days, and the effect of randomised treatment according to gender.
Results: Among the 2829 participants, 1049 (37%) were female: they were significantly older, had higher National Institutes of Health Stroke Scale scores, but had smaller haematoma volumes at baseline compared to males. SBP reduction over 7 days was larger in women compared to men. There was no significant sex difference on mean haematoma growth at 24 hours or the combined endpoint of death or major disability. Men had higher 3-month mortality (Odds ratio 1.48, 95% confidence interval 1.10–2.00). There was no heterogeneity for the randomised BP lowering treatment effect.
Conclusions: Women with acute ICH were older, had more severe neurological deficits but smaller haematoma volumes at presentation. Achieved SBP was lower in women but there were no gender differences in the treatment effect. Men had significantly higher mortality after ICH.
AS20-044
CEREBRAL HAEMORRHAGE 2
Oral
IDENTIFYING SMALL VESSEL DISEASE HELPS PREDICT THE LIKELIHOOD OF AN UNDERLYING INTRACRANIAL VASCULAR MALFORMATION IN SPONTANEOUS INTRACEREBRAL HAEMORRHAGE
D. Wilson1, A. Ogungbemi1, G. Ambler2, I. Jones1, H.R. Jager3 and D.J. Werring1
1Institute of Neurology, Brain repair and rehabilitation, London, United Kingdom
2University College London, Department of statistical science, London, United Kingdom
3Institute of Neurology, Lysholm Department of Neuroradiology, London, United Kingdom
Abstract
Background: Determining the cause of spontaneous (non-traumatic) intracerebral haemorrhage (ICH) is critical to guide treatment and prognosis. We investigated whether the presence of small vessel disease (SVD) on neuroimaging predicts a low risk of an underlying intracranial vascular malformation.
Methods: We identified patients with acute spontaneous ICH who underwent both acute CT angiography (CTA) and intra-arterial digital subtraction angiography (IADSA) - with or without MRI - at our institution from January 2010-April 2014. SVD was defined as confluent white matter changes (Fazekas scale score ≥2) on CT, or the presence of cerebral microbleeds on MRI. Logistic regression including CTA result, SVD, age, pre morbid hypertension and location of ICH was used to derive a prediction model. ROC curves and bootstrapping were used to internally validate the model.
Results: We included 153 patients (60% males, median age 48) of whom 68 had a vascular malformation on IADSA. CTA had a sensitivity of 82%, absence of SVD 85%, absence of pre-morbid hypertension 79%, non-deep location of ICH 63% and age < 45 years of 46% for identifying a vascular malformation. An algorithm incorporating CTA result, SVD and pre ICH HTN had excellent sensitivity (99%) and acceptable specificity (48%) for the identification of a vascular malformation.
Conclusions: Identifying SVD is associated with a low yield of vascular malformations in patients with spontaneous ICH. A combination of normal CTA and the presence of SVD or pre-ICH hypertension can reliably identify patients at very low risk of an intracranial vascular malformation, reducing the need for IADSA.
AS06-001
EPIDEMIOLOGY OF STROKE
Oral
RECANALIZATION IN CEREBRAL VENOUS THROMBOSIS - A SYSTEMATIC REVIEW AND META-ANALYSIS
D. Aguiar de Sousa1, L. Neto2, P. Canhão1 and J. Ferro1
1Hospital Santa Maria - University of Lisbon, Department of Neurosciences Neurology, Lisbon, Portugal
2Hospital Santa Maria - University of Lisbon, Neuroradiology Service, Lisbon, Portugal
Abstract
Background: The role of recanalization of the occluded dural sinus or veins in the outcome of patients with cerebral venous thrombosis (CVT) is not established. We aimed to systematically review, in patients with CVT, (1) the recanalization rate and its association with (2) clinical outcome and (3) CVT recurrence.
Methods: Systematic search in MEDLINE (from inception to November 2015) and reference lists of included studies and review articles. Search strategy developed in accordance with the clinical questions. We considered observational studies reporting original data on the recanalization rate in adult patients with CVT treated with anticoagulation.
Results: 226 studies were identified and 20 studies were included. A meta-analysis of proportions using a random-effect model and Freeman-Tukey double arcsine transformation was performed. (1)We found report of 676 patients with recanalization amongst 792 cases of CVT. Overall proportion of recanalization in meta-analysis was 0.86 (95%CI 0.81–0.90), I2 = 50%). A secondary analysis including only patients evaluated at least 3 months after diagnosis showed a recanalization rate of 0.83 (95%CI 0.75–0.90), I2 = 65%). (2)Incomplete recovery (mRS > 1) occurred in 319/355 patients achieving recanalization and 42/58 patients without recanalization (RR 2.7; 95%CI 1.6–4.6; p = 0.0002). No recanalization was also associated with death or dependency (mRS > 2): 3/174 vs 9/38 (RR 13.7; 95%CI 3.9–48.4, p < 0.0001). (3)Data regarding recurrence rates according with recanalization status was too scarce.
Conclusions: About 86% of the patients that receive anticoagulation achieve recanalization after CVT. Lack of venous recanalization in the follow-up is associated with worse clinical outcome. There is limited information regarding the association of recanalization with CVT recurrence.
AS16-015
EPIDEMIOLOGY OF STROKE
Oral
SILENT BRAIN INFARCTS, PERIPHERAL VASCULAR DISEASE AND THE RISK OF VASCULAR EVENTS IN A MEDITERRANEAN HYPERTENSIVE COHORT. RESULTS FROM THE ISSYS STUDY
P. Delgado1, I. Riba-Llena1, S. Sánchez-Ballesteros1, F. Orfila2, X. Mundet2, J. Jiménez-Balado1, L. Troya2, C. Violan2 and J. Montaner1
1Institut de Recerca Hospital Vall d'Hebron, Neurovascular Research Lab, Barcelona, Spain
2IDIAP Jordi Gol, Barcelona city Research Suport Unit, Barcelona, Spain
Abstract
Background: Subclinical target organ damage has been associated with the risk of vascular events and might refine risk stratification in hypertensive subjects. We aimed to study its association with the risk and type of events in a Mediterranean cohort.
Methods: Data from the ISSYS study, a prospective cohort of hypertensive individuals, aged 50 to 70 with no prior stroke or dementia. All subjects underwent brain MRI, EKG, blood and urine sampling and vascular testing to assess for markers of target organ damage in the brain (silent brain infarcts-SBI), kidney (microalbuminuria, glomerular filtration rate), heart (left ventricular hypertrophy) and large vessels (ankle to brachial index-ABI). Primary outcome was the presence of any vascular event on follow-up. Secondary outcomes were either cerebral or cardiovascular events assessed separately. Adjusted hazard ratios were obtained by Cox regression.
Results: 976 subjects were followed-up during 3.4 years (median) accounting for a total of 3312 person-years. 49.2% were males. Primary outcome was achieved in 54 subjects and it was independently associated with both the presence of SBI (HR = 2.56, 1.28 to 5.14) and ABI ≤ 0.9 (HR = 4.28, 2.10–8.76). Considering secondary outcome, cerebral events were only associated with the presence of SBIs (HR = 4.54, 1.47 to 14.02) whereas cardiovascular events were only related to low ABI (HR = 5.39, 2.33 to 12.5). Besides those, the most relevant risk factors were male gender and the presence of diabetes.
Conclusions: Among hypertensive subjects, the presence of SBI and low ABI increase the risk of CV events, consequently, both brain imaging and vascular assessments might be useful in risk stratification.
AS20-012
EPIDEMIOLOGY OF STROKE
Oral
CLIMATIC, SEASONAL AND CIRCADIAN CIRCUMSTANCES OF HYPERTENSIVE ICH - AN INTERNATIONAL APPROACH
C. Herweh1, S. Nordlohne1, L. Uhlmann2, S. Thorsten3, B. Martin1 and S. Marek4
1University of Heidelberg, Department of Neuroradiology, Heidelberg, Germany
2University of Heidelberg, Department of Medical Biometry and Informatics, Heidelberg, Germany
3Frankfurt Hoechst Hospital, Department of Neurology-, Frankfurt am Main, Germany
4University of Heidelberg, Department of Neurology, Heidelberg, Germany
Abstract
Background: We investigated associations between presumed etiology of spontaneous intracerebral hemorrhage (ICH) and climatic factors.
Methods: We used data from an international, clinical trial in patients with spontaneous intracerebral (ICH), when meteorological and seasonal data were also available (712 of 841 patients). The recruitment period covered 18 months. Therefore data from uniquely represented months where weighted with factor 2, resulting in 440 additional virtual cases. Climatic data were normalized with regard to the annual mean values for each center. ICH was classified as hypertensive (HT) when located in the basal ganglia and brainstem and as non-hypertensive (NHT) when in a lobar location. We compared these two groups regarding climatic data as well as time of day, week days and seasons and carried out a multifactorial regression analysis.
Results: We compared 956 HT-ICH and 196 NHT-ICH cases. HT-ICH was significantly more frequent in younger patients (63 vs. 69 years; p = 0.002) and occurred on days with higher air pressure (0.07 vs. −0.13; p = 0.01). The regression analysis identified these two factors also as independent predictors of hypertensive ICH (OR = 0.982; p = 0.002 and OR = 1.167; p = 0.018, respectively).
Conclusions: The present analysis of worldwide data strongly suggests an association between the occurrence of hypertensive ICH and air pressure which previously could be shown in local studies, only. As a limitation, the present data do not reflect true ICH incidence but recruitment behavior of a clinical trial and conclusions have to be drawn carefully.
AS13-028
EPIDEMIOLOGY OF STROKE
Oral
TEMPORAL TRENDS (2002-2014) IN SEVERITY AND OUTCOME OF INCIDENT STROKE IN OXFORDSHIRE, UK: EVIDENCE OF IMPACT OF ACUTE STROKE CARE AT THE POPULATION-LEVEL
L. Li1, R. Luengo-Fernandez2, L. Bull1, S. Welch1, S. Gutnikov1, Z. Mehta1, L. Silver1 and P.M. Rothwell On behalf of the Oxford Vascular Study
1
1Stroke Prevention Research Unit, Nuffield Department of Clinical Neurosciences- Oxford University, Oxford, United Kingdom
2Health Economics Research Centre, Nuffield Department of Population Health- Oxford University, Oxford, United Kingdom
Abstract
Background: Acute stroke care improves outcome in eligible patients in randomised trials, but overall impact at the population-level is uncertain.
Methods: Among all incident strokes in a population-based cohort (OXVASC) we studied risk factors, premorbid use of preventive treatments, stroke severity (NIHSS) and outcome (follow-up mRS) from 2002–2014 (in five consecutive 30-month periods) during which acute stroke services were introduced.
Results: Stroke incidence (n = 1821 events) remained stable over time, with 356, 358, 376, 380 and 351 events in each 30-month period, but acute stroke services improved, with the proportion admitted to a stroke unit within 24 h increasing from 0% to 78.6% (ptrend < 0.0001) alongside improved “TIA clinic” services for minor stroke. Acute stroke severity at initial assessment (distribution of baseline NIHSS) did not change over time (ptrend = 0.38). However, stroke outcome improved significantly across the five periods, with less new disability/death at 1-month (n/%: 273/49.0, 168/47.2, 165/46.1, 162/43.1, 148/38.9 and 140/39.9, ptrend = 0.008) and 1-year (284/51.0, 185/52.0, 174/48.7, 172/45.7, 166/43.9 and 140/40.1, ptrend = 0.001). These trends were independent of any changes in age, sex, premorbid disability, risk factors, premorbid preventive treatment and baseline NIHSS (adjusted ORper-period: 1 month - 0.88,95%CI 0.80–0.96, p = 0.006; 1-year - 0.85, 0.77–0.93, p = 0.0003). Results were also consistent in analyses stratified by age, stroke subtypes and major vs. minor stroke.
Conclusions: Despite no temporal trends in stroke incidence or acute stroke severity, substantial improvements in acute stroke services have coincided with improved outcomes at the population level in Oxfordshire over the last 15 years.
AS13-046
EPIDEMIOLOGY OF STROKE
Oral
DIFFERENCES IN THE DISTRIBUTION OF STROKE SUBTYPES IN A UK BLACK STROKE POPULATION; FINAL RESULTS FROM THE SOUTH LONDON ETHNICITY AND STROKE STUDY
L. Rutten-Jacobs1, G. Gulli2, L. Kalra3, A. Rudd4,5, C.D.A. Wolfe4,6 and H. Markus1
1University of Cambridge, Clinical Neurosciences- Stroke Research Group, Cambridge, United Kingdom
2Frimley Park Hospital, Neurology, Surrey, United Kingdom
3Institute of Psychiatry- Psychology and Neurosciences- King's College London, Department of Basic and Clinical Neurosciences, London, United Kingdom
4King's College London, Division of Health and Social Care Research, London, United Kingdom
5St. Thomas' Hospital, Stroke Unit, London, United Kingdom
6St. Thomas' NHS Foundation Trust, National Institute for Health Research NIHR Biomedical Research Centre, London, United Kingdom
Abstract
Background: Stroke incidence is increased in Black individuals but reasons for this are poorly understood. We explored differences in aetiological stroke subtypes, and the extent to which they are explained by traditional risk factors.
Methods: Between 1999- 2010, 1200 black (809 Caribbean and 391 African ethnicity) and 1200 white stroke patients were prospectively recruited from South London in the UK. Stroke subtypes were classified using the TOAST classification. Stroke subtypes were compared between black and white patients and between Black Caribbean and Black African patients using univariable (age, sex, and social deprivation adjusted) and multivariable logistic regression analyses (including traditional vascular risk factors and socio-demographics).
Results: Black patients were younger than white patients (65.1 (SD 13.7) versus 74.8 (SD 13.7) years). Black patients versus white patients more often had small vessel disease stroke (27% vs 12%; OR 2.74 (95% CI 2.19–3.44)), but less frequent large vessel (OR 0.59 (95% CI 0.45–0.78)) and cardioembolic stroke (OR 0.61 (95% CI 0.50–0.74)). These associations remained after controlling for vascular risk factors and socio-demographics. Black Caribbean patients had a risk factor and stroke subtype profile intermediate between that of Black African and white patients. Black Caribbean patients versus Black African patients more often had cardioembolic stroke (OR 1.48 (95% CI 1.04–2.10)), but less intracranial large vessel disease (OR 0.44 (95% CI 0.24–0.83)).
Conclusions: Clear differences exist in stroke subtype distribution between black and white stroke patients, with a marked increase in small vessel stroke. These could not be explained by differences in the assessed traditional risk factors.
AS16-071
EPIDEMIOLOGY OF STROKE
Oral
ASSOCIATION BETWEEN CANCER AND CEREBRAL VENOUS THROMBOSIS
S. Silvis1, S. Hiltunen2, S.M. Zuurbier1, T. Tatlisumak2, A. Dikstaal1, E. Haapaniemi2, S. Middeldorp3, J. Putaala2, S. Cannegieter4 and J. Coutinho1
1Academic Medical Center, Neurology, Amsterdam, Netherlands
2Helsinki University Hospital, Neurology, Helsinki, Finland
3Academic Medical Center, Vascular Medicine, Amsterdam, Netherlands
4Leiden University Medical Center, Department of Clinical Epidemiology, Leiden, Netherlands
Abstract
Background: To assess whether a history of cancer is a risk factor for cerebral venous thrombosis (CVT).
Methods: Case-control study. We assessed consecutive adult patients with CVT admitted to two academic hospitals between 1987 and 2015 (cases) and healthy subjects from the Dutch MEGA study (Multiple Environmental and Genetic Assessment of risk factors for thrombosis; controls). Non-invasive skin malignancy was not scored as cancer. Using logistic regression analysis, we adjusted for age and sex, and stratified for type of cancer (solid vs. haematological) and time since diagnosis of cancer (0–1 year vs. > 1 year).
Results: Out of 453 cases and 6297 controls, we excluded 20 subjects (1 case, 19 controls) because of missing data, leaving 452 cases and 6278 control subjects. 52 cases (11.5%) had a history of cancer compared to 233 (3.7%) controls. Cases were younger (median 41.0 vs. 47.7 years) and more often female (67.3% vs. 53.7%). The risk of CVT was increased in patients with cancer compared to those without (adjusted OR 4.4, 95% CI 3.2–6.2). The association was stronger in the first year after cancer diagnosis (adjusted OR 22.1, 95% CI 12.8–38.4), and in those with haematological malignancies (adjusted OR 24.3, 95% CI 12.5–47.0). The highest risk of CVT was found in subjects with a haematological malignancy within the first year of diagnosis (adjusted OR 122.2, 95% CI 28.2–529.3).
Conclusions: Cancer is a risk factor for CVT, especially haematological malignancies. The risk is the highest in the first year after diagnosis.
AS05-026
EPIDEMIOLOGY OF STROKE
Oral
SYNDROME-SPECIFIC 12-YEAR RISK OF STROKE AFTER TRANSIENT NEUROLOGICAL ATTACK: IMPLICATIONS FOR SECONDARY PREVENTION
M.A. Tuna1, L. Gaziano2, A. Tornada3, L. Li1, S. Gutnikov1, Z. Mehta1 and P. Rothwell1
1Oxford University, Nuffield Department of Clinical Neuroscience, Oxford, United Kingdom
2Washington and Lee University, Biochemistry Department, Lexinghton- Virginia, USA
3Hospital de Cascais, Department of Medicine, Cascais, Portugal
Abstract
Background: TIA patients require intensive long-term secondary prevention of stroke. There are conflicting estimates of the risk of stroke after Transient Neurological Attacks (TNAs).
Methods: In a population-based study of all TNAs and TIAs from 2002–2014 (Oxford vascular study), we prospectively classified all first events as TIA (NINDS criteria) versus TNA. TNAs were subclassified, including: isolated brainstem syndrome (IBS), isolated sensory symptoms (ISS), migraine-like symptoms (MLS), transient confusion (TC), transient unresponsiveness (TU), isolated visual disturbance (IVD), isolated speech disturbance (ISD) and others. Stroke risk on face-to-face follow-up to 12-years was compared with expected age/sex-specific stroke incidence in the underlying population.
Results: Among 674 NINDS-defined TIA (mean/SD age = 73.3/13.4) and 846 TNA (68.3/14.7) 218 had a stroke (105 after a NINDS-defined TIA and 113 after a TNA). As expected, 12-year stroke risk after NINDS-TIA was higher than the underlying population stroke incidence (RR = 4.09, 2.64–6.34, p < 0.001). However, the risk was also higher for the majority of the TNA syndromes: IBS (n = 169, RR = 3.6,1.5–8.7); ISS (108, RR = 6.3,1.7–23.0), MLS (186, RR = 3.6,1.5–9.2), TC (58, RR = 5.3,1.3–20.4), TU (34, RR = 8.9,1.4–17.7), others (151, RR = 4.2, 1.4–13.0). The risk was not significantly increased for IVD (86, RR = 1.9,0.6–6.9) and ISD (54, RR = 3.5, 0.8–15.1). Rates of use of preventive medication at one-month follow-up in TIAs was higher than in TNAs (antithrombotics 97.1% vs 68.6%, statins 71.4% vs 52.6%, and antihypertensives 72.9% vs 62.3%) and declined more rapidly on longer-term follow-up.
Conclusions: The relatively high risk of stroke in patients with TNA appears to justify detailed investigation and higher levels of intensity of secondary prevention.
AS05-028
EPIDEMIOLOGY OF STROKE
Oral
EFFECTS AND INTERACTIONS OF ANTIHYPERTENSIVE DRUG CLASSES ON HOME BP VARIABILITY AFTER TIA OR MINOR STROKE
A. Webb1, N. Lovett1, G. Lau1, R. Wharton1 and R. Peter1
1University of Oxford, Stroke Prevention Research Unit- Department of Clinical Neuroscience, Oxford, United Kingdom
Abstract
Background: Visit-to-visit SBP variability (SBPV) is increased by ACEi and beta-blockers, paralleling effects on stroke risk. Calcium channel blockers (CCB) and diuretics reduce SBPV but it is unclear if their addition limits the effects of ACEi or beta-blockers. Day-to-day home monitoring (HBPM) is a practical method of measuring SBPV to determine effects of antihypertensives and their interactions.
Methods: Consecutive patients were recruited from the Oxford Vascular Study TIA/stroke clinic. They performed Bluetooth-enabled, telemetric HBPM (3 measurements, 3 times daily for ≥1 month), guiding treatment according to guidelines, and ambulatory monitoring at 1 month (ABPM). Mixed linear models identified associations between daily SBP or coefficient of variation over 7 days with antihypertensive classes alone or combined, adjusting for multiple measures, other drugs and demographics.
Results: Across 57721 patient-days in 1118 patients, each drug class was, as expected, associated with a similar reduction in SBP (p < 0.001, figure A). However, day-to-day SBPV was reduced with CCBs and diuretics and increased with ACEi and beta-blockers (figure B-D). CCBs reduced within-day SBPV (HBPM: 7.4vs7.0%, p < 0.001, ABPM: 12.3vs11.7%, p = 0.007). CCBs limited SBPV increases with beta-blockers on waking (p = 0.001) and ACEi in mid-morning (p < 0.001) more than expected.
Conclusions: Antihypertensive effects on day-to-day SBPV were consistent with effects on visit-to-visit SBPV, supporting HBPM-guided treatment of SBPV. Addition of CCBs limits increased SBPV in patients on ACEi or beta-blockers.
AS12-006
EXPERIMENTAL STUDIES IN STROKE
Oral
CEREBRAL COLLATERAL THERAPEUTICS IN EXPERIMENTAL ISCHEMIC STROKE: A RANDOMIZED PRECLINICAL TRIAL OF FOUR MODULATION STRATEGIES
S. Beretta1, A. Versace1, D. Carone1, M. Riva1, V. Dell'Era1, M. Laura1, P. Silvia1, P. Giada1, F. Stiro1, P. Giovanni1, G. Carlo1, C. Ferrarese1 and R. Cai1
1University of Milano Bicocca, Laboratory of Experimental Stroke Research, Monza MB, Italy
Abstract
Background: Cerebral collaterals are dynamically recruited after arterial occlusion, provide residual perfusion to ischemic areas and highly affect tissue outcome in acute ischemic stroke. The present study is a randomized preclinical trial to investigate the efficacy and safety of four pathophysiologically distinct strategies for acute modulation of collateral flow (collateral therapeutics) in experimental ischemic stroke.
Methods: Middle cerebral artery (MCA) was transiently occluded (90 minutes) in adult male Wistar rats (n = 126), followed by 24 hours reperfusion. A composed randomization design was used to randomly assign rats to receive collateral therapeutics or no active treatment, starting 30 minutes after MCA occlusion. Collateral therapeutics used were phenylephrine, polygeline, acetazolamide and 15° head down tilt. The primary outcomes were infarct volume and functional deficit assessed 24 hours after ischemia induction. Changes in cerebral perfusion, physiological variables and treatment-related mortality were assessed as secondary outcomes.
Results: Compared to untreated animals, treatment with collateral therapeutics was associated with a reduction of infarct volume (0.42, p < 0.0001) and neurological deficit (OR 4.56, 95% C.I. 2.07 to 10.08; p = 0.0001). Overall, collateral therapeutics acutely increased cerebral perfusion in cortical ischemic areas (medial and lateral MCA territory), without a significant impact on physiological variables (with the exception of phenylephrine). The highest efficacy and safety profile was observed for head down tilt, while the lowest for phenylephrine.
Conclusions: Our findings suggest that acute modulation of cerebral collaterals is feasible and provide tissue-saving strategies in the hyperacute phase of ischemic stroke prior to recanalization therapy.
AS12-015
EXPERIMENTAL STUDIES IN STROKE
Oral
INHIBITION OF STROKE-ELEVATED ENDOTHELIAL α5β1 INTEGRIN STABILIZIES THE BLOOD-BRAIN BARRIER AND IS NEUROPROTECTIVE
D. Edwards1, J. Roberts1, L. de Hoog2 and G. Bix3
1University of Kentucky, Anatomy and Neurobiology, Lexington, USA
2University of Manchester, Pharmacology, Manchester, United Kingdom
3University of Kentucky, Neurology, Lexington, USA
Abstract
Background: Stroke is a leading cause of death and disability with limited therapeutic options. We recently demonstrated that endothelial cell-selective, α5β1 integrin, (a fibronectin receptor expressed in development, but not adult cerebrovasculature under physiologic conditions) knockout mice are profoundly resistant to changes in blood-brain barrier (BBB) integrity and brain injury after ischemic stroke. Therefore, we hypothesize that α5β1 is acutely upregulated in ischemic penumbral vasculature after stroke, and that blocking α5β1 with ATN-161 could be therapeutic by stabilizing the BBB.
Methods: C57BL6 mice underwent transient middle cerebral artery occlusion and were treated with ATN-161 IV 1 mg/kg on PSD1. Expression determined by immunohistochemistry, and infarct volume by TTC and cresyl violet. Brain endothelial cell monolayers underwent oxygen-glucose deprivation; trans-endothelial electrical resistance and FITC-dextran migration measurements determined permeability.
Results: By post-stroke day (PSD) 2, we noted a significant increase in penumbral α5β1 cerebrovascular expression that exponentially increased until PSD4. Surprisingly, α5β1 was exclusively expressed luminally suggesting a lack of basement membrane interactions and potential ease of access to IV therapeutics. Inhibition of α5β1 with ATN-161 showed lack of brain IgG extravasation on PSD1–3 and infarct volume on PSD3. Finally, in vitro results demonstrated an increased permeability, increased α5β1 expression and decreased cell-surface expression of the tight junction protein claudin-5, and prevented by ATN-161.
Conclusions: Collectively, our results demonstrate that endothelial cell α5β1 expression increases acutely after stroke luminally, may contribute to BBB breakdown and subsequent expansion of brain injury via modulation of tight junction protein function, and could represent a novel therapeutic target for ischemic stroke.
AS12-030
EXPERIMENTAL STUDIES IN STROKE
Oral
GUT MICROBIOTA ALTERATIONS AFTER ISCHEMIC STROKE AFFECT IMMUNE HOMEOSTASIS AND STROKE OUTCOME
V. Singh1, S. Roth1, S. Bärbel2, M. Dichgans1 and A. Liesz1
1Klinikum der Universität München, Institute for Stroke and Dementia Research, Munich, Germany
2Klinikum der Universität München, Max-von-Pettenkofer Institute, Munich, Germany
Abstract
Background: Secondary inflammation after acute brain injury contributes to disease pathophysiology, on the other side brain injury itself also induces perturbations of systemic immune-homeostasis. However, the mechanisms involved in inducing peripheral immunomodulation and priming the (auto-)immune neuroinflammatory reaction are widely unknown. Emerging evidence indicates a central role for gut microbiota in educating immune reactions and maintaining immune homeostasis.
Methods: Experimental stroke was induced either by distal permanent occlusion of the middle cerebral artery (dMCAo) or proximal transient MCA occlusion (pMCAo). We used 16S rRNA sequencing for analysis of mice gut microbiota. Immunohistology and flow cytometry were used for analysis of immune cell subsets. In vivo leukocyte tracking was achieved by dye microinjections in Peyer's patches. Microbiota transplantation studies were performed in germfree (GF) mice.
Results: Microbiota dysbiosis after stroke was associated with reduced intestinal motility and barrier dysfunction. Stroke induced distinct alterations in the intestinal immune compartment. In turn, transfer of post-stroke dysbiotic microbiota in GF recipient mice induced peripheral immune alterations and exacerbated stroke outcome, demonstrating a causality of post-stroke dysbiosis and deleterious immunomodulation. Moreover, we observed migration of T cells from the intestine (PP) to the post-ischemic brain using in vivo cell tracking. Normalization of gut dysbiosis by bacteriotherapy using fecal microbiota transplantation reduced brain lesion volumes.
Conclusions: Our study describes a novel bi-directional interaction along the brain-gut-immune axis in experimental stroke.
AS12-032
EXPERIMENTAL STUDIES IN STROKE
Oral
THE CHOROID PLEXUS IN POST-STROKE CEREBRAL LEUKOCYTE INVASION
G. Llovera1, F. Hellal1, T. Arzberger2, B. Engelhardt3 and A. Liesz1
1Institute for Stroke and Dementia Research, Klinikum der Universität München, Munich, Germany
2Center for Neuropathology and Prion Research, Ludwig-Maximilians-Universität, Munich, Germany
3Theodor Kocher Institute, University of Bern, Bern, Switzerland
Abstract
Background: Invasion of peripheral leukocyte into the ischemic brain is a critical event, which promotes inflammatory tissue damage. The choroid plexus (CP) has been described as an alternative invasion route in autoimmune brain disorders but has so far not been investigated in stroke.
Methods: Leukocyte accumulation after experimental stroke in mice was studied by immunohistology, flow cytometry and 3D-imaging of solvent-cleared whole brains. Human choroid plexus samples of stroke and control patients were analyzed. Microarray analysis was performed for chemokine expression in laser-microdissected samples. Intracerebral leukocyte migration was investigated by in vivo cell tracking. Apoptosis of CP epithelium was characterized by TUNEL staining in different stroke models.
Results: Monocytes equally surround the cortical infarct core while lymphocytes specifically accumulate in the peri-infarct cortex. T-cells were the predominant population in the ipsilateral CP in mice as well as in humans. T-cell migration from CP to the peri-infarct cortex was confirmed by in vivo cell tracking of photo-activated T-cells. Microarray analysis revealed a gradient for ligands of the CCR2 receptor between cortex and CP, which was confirmed in CCL2-reporter mice. Significantly less lymphocytes were observed in stroke models with extensive brain lesions encompassing ischemic lesion also of the ipsilateral CP, in contrast to focal cortical brain lesions.
Conclusions: Our study demonstrates for the first time that the choroid plexus is a key route for post-stroke cerebral T cell invasion. This has to be considered in future studies analyzing neuroinflammatory mechanisms and immunotherapies for stroke.
AS12-044
EXPERIMENTAL STUDIES IN STROKE
Oral
NEOVASCULARIZATION AFTER INTRACEREBRAL HEMORRHAGE IS CONDITIONED BY THE Tp53 ARG72PRO POLYMOSPHISM
C. Rodríguez1,2, T. Sobrino3, J. Agulla1,2, V. Bobo-Jiménez1,2, M.E. Ramos-Araque1,2, J.J. Duarte1, J.C. Gómez-Sánchez1, J.P. Bolaños1,2, J. Castillo3, A. Almeida1,2
1Institute of Biomedical Research of Salamanca IBSAL, University Hospital of Salamanca - University of Salamanca, Salamanca, Spain
2Institute of Functional Biology and Genomics IBFG, University of Salamanca – CSIC, Salamanca, Spain
3Health Research Institute of Santiago de Compostela IDIS, University Clinical Hospital – University of Santiago de Compostela, Santiago de Compostela, Spain
Abstract
Background: Neovascularization following intracerebral hemorrhage (ICH) is an essential compensatory response that mediates brain repair and modulates the clinical outcome of patients. Bone marrow-derived endothelial progenitor cells (EPCs) promote endothelial repair and long-term recovery after stroke. We previously identified the Tp53 Arg72Pro polymorphism as a genetic marker predicting functional outcome after stroke. However, the role of this polymorphism in vascular repair remains unknown.
Methods: The Tp53 Arg72Pro polymorphism was genotyped in 78 patients with non-traumatic ICH included within 12 h of symptoms’ onset. Functional outcome at 3 and 12 months was evaluated by the modified Rankin scale (mRS). Humanized Tp53 Arg72Pro knock-in mouse models were subjected to experimental ICH. Immunohistochemistry analysis was performed to evaluate cell death and vascular density. Serum levels of cytokines and circulating EPCs were measured by ELISA and flow cytometry, respectively.
Results: Patients harboring the Pro allele showed higher levels of circulating EPC at day 7 and better functional outcome at 3 and 12 months following ICH, than those with the homozygous Arg allele. Moreover, levels of the EPC-mobilizing cytokines, vascular endothelial growth factor (VEGF) and stromal-derived factor (SDF)-1a, were also higher in Pro allele-carrying patients. We found that the endothelial cells of the Pro mice brain vessels were more resistant against ICH-induced apoptosis than those of the Arg mice. This allowed increased levels of cytokines and EPC mobilization that promoted neovascularization in the Pro mice.
Conclusions: The Tp53 Arg72Pro polymorphism modulates EPC mobilization and neovascularization, thus determining brain repair and neurological recovery after ICH.
Funded by FEDER and ISCIII (CD11/00348; PI12/0685; INVICTUS RD12/0014/0001, RD12/0014/0007).
AS12-003
GENETICS AND BIOMARKERS
Oral
LEUKOARAIOSIS AND LACUNES ARE ASSOCIATED WITH INFLAMMATION BIOMARKERS IN PATIENTS WITH ISCHAEMIC STROKE TREATED WITH INTRAVENOUS THROMBOLYSIS
F. Arba1, B. Piccardi1, V. Palumbo2, B. Giusti3, A.M. Gori3, M. Nesi2, P. Nencini2, G. Pracucci1, R. Abbate3 and D. Inzitari1
1University of Florence, NEUROFARBA, florence, Italy
2Careggi University Hospital, Stroke Unit and Neurology, Florence, Italy
3University of Florence, Department of Experimental and Clinical Medicine, Florence, Italy
Abstract
Background: Inflammation has been suggested as concurrent mechanism of SVD, although evidence on humans is lacking. In a cohort of acute ischaemic stroke patients treated with intravenous thrombolysis we investigated the relation between: 1-metalloproteinases (MMPs), inhibitors of metalloproteinases (TIMPs) and features of SVD (leukoaraiosis and lacunes); 2-MMPs, TIMPs and clinical outcomes.
Methods: We measured blood levels of MMPs and TIMPs before t-PA treatment and 90 days after the index stroke. We assessed leukoaraiosis and lacunes on CT scan with validated scales. We build up a composite three-point SVD score combining leukoaraiosis and lacunes (absence, mild-moderate and severe SVD). We retained univariate statistically significant MMPs and TIMPs in a multivariate ordinal regression analysis and logistic regression analysis to investigate relation with SVD grade and clinical outcomes, respectively.
Results: We included 262 patients, mean (±SD) age = 68.5 (±12.7) years, 154 (59%) males; 131 had no SVD, 66 (25%) mild-moderate and 65 (25%) severe SVD. Multivariate analysis showed both baseline and 90 days of either MMP-1 (OR = 1.15; 95%CI = 1.01–1.40; OR = 1.20; 95%CI = 1.16–1.42) and TIMP-4 (OR = 1.87; 95%CI = 1.17–2.98; OR = 2.84; 95%CI = 1.62–4.97) independently associated with increasing SVD grade. We found no associations between MMP-1, TIMP-4 and clinical outcomes.
Conclusions: Baseline and 90 days blood levels of MMP-1 and TIMP-4 were associated with increasing severity of SVD at both baseline and 90 days time points. Our results support that in patients with ischaemic stroke increasing degree of SVD sustains higher levels of inflammation.
AS14-001
GENETICS AND BIOMARKERS
Oral
MENDELIAN STROKE GENES AND RISK OF SMALL VESSEL STROKE IN YOUNG INDIVIDUALS
M. Chong1,2,3, M. O'Donnell4, V. Thijs5, A. Dans6, P. Lopex-Jaramillo7, D. Gomez-Arbelaez7, C. Mondo8, A. Członkowska9,10, M. Skowronska9, S. Oveisgharan11, S. Yusuf3,12,13, G. Paré1,3,14
1Population Health Research Institute, Genetic Molecular Epidemiology Lab, Hamilton, Canada
2McMaster University, NA, Hamilton, Canada
3Hamilton Health Sciences Centre, NA, Hamilton, Canada
4National University of Ireland, HRB Clinical Research Facility, Galway, Ireland
6Phillippine General Hospital, Internal Medicine, Manila, Philippines
7Fundación Oftalmológica de Santander FOSCAL, Fundación Oftalmológica de Santander, Desarrollo e Innovación Tecnológica, Colombia
8Uganda Heart Institute, Cardiology, Kampala, Uganda
9Institute of Psychiatry and Neurology, Neurology, Warsaw, Poland
10Warsaw Medical University, Experimental and Clinical Pharmacology, Warsaw, Poland
11Shariati Hospital- Tehran University of Medical Sciences, Neurology, Tehran, Iran
12Population Health Research Institute, NA, Hamilton, Canada
13McMaster University, Medicine, Hamilton, Canada
14McMaster University, Pathology and Molecular Medicine, Hamilton, Canada
Abstract
Background: Mendelian strokes are genetic diseases that are reported to strongly predispose mutation carriers to early-onset stroke. However, mutation penetrance is unknown in patients without clinical suspicion of Mendelian syndrome. To this end, we screened 9 known Mendelian genes within young stroke patients and matched controls.
Methods: Using next-generation sequencing, 9 Mendelian genes were assessed in 742 young cases of unrelated small-vessel stroke (mean age: 50 years), comprising 384 intracerebral hemorrhage (ICH) and 358 small-vessel ischemic stroke (SVIS) cases, along with 742 matched controls selected from INTERSTROKE, a global case-control study of stroke.
Results: Across all Mendelian genes, rare deleterious coding mutations were collectively frequent among cases (29.2%) and controls (24.7%). Overall, mutation carriers were at higher risk of ICH (OR = 1.45; 95% CI, 1.04–2.02; P = 0.01) but not SVIS (OR = 1.10; 95% CI, 0.80–1.51; P = 0.28). Examining individual genes, COL4A1 mutation carriers were at moderately elevated risk of ICH (OR = 2.55; 95% CI, 1.27–5.11; P = 0.004) corresponding to a population attributable risk of 4.08% (95% CI, 2.05–5.66). Similarly, pathogenic mutations, either previously reported to cause stroke or novel mutations strongly resembling reported ones, also posed moderate risk for all stroke (OR = 2.40; 95% CI, 0.85–6.81; P = 0.05) and were found in 12 (1.62%) cases and 5 (0.67%) controls.
Conclusions: Our results confirm the role Mendelian genes in early stroke risk but suggests effects. While causality of Mendelian stroke genes is well-established, our findings point towards low mutation penetrance, and as a corollary, the presence of asymptomatic mutation carriers. Future studies investigating disease modifiers will have important implications for screening, management, and treatment.
AS22-007
GENETICS AND BIOMARKERS
Oral
DIFFERENT TYPES OF WHITE MATTER HYPERINTENSITIES IN CADASIL: INSIGHTS FROM 7-TESLA MRI
F. De Guio1, A. Vignaud2, H. Chabriat3 and E. Jouvent3
1Inserm UMR 1161, Paris, France
2CEA, NeuroSpin, Gif-sur-Yvette, France
3Inserm UMR 1161, Neurology Lariboisière, Paris, France
Abstract
Background: In CADASIL, by contrast to sporadic cerebral small vessel disease, white matter hyperintensities (WMH) are frequently observed in temporal poles, external capsules and superior frontal regions. Whether the mechanisms underlying WMH in these areas (CADASIL-specific WMH - CSWMH) differ from those responsible for WMH outside these regions (non-specific WMH - NSWMH) remains undetermined. The aim of the present study was to determine whether microstructural differences can be detected between CSWMH and NSWMH with the use of quantitative and high-resolution MRI scans.
Methods: Twenty CADASIL patients at the early clinical stages of the disease (MMSE ≥ 24 and modified Rankin’s scale ≤ 1) and 17 age- and sex-matched controls were scanned with a 7-Tesla MRI scanner to obtain quantitative relaxometry maps of T1 and of T2* (T1R and T2*R, respectively) and high-resolution images. CSWMH and NSWMH were compared using region-based and unsupervised voxel-wise analyses of T1R and T2*R.
Results: Significant T1R and T2*R differences were detected between CSWMH and NSWMH with both methods. CSWMH are characterized by longer T1R and T2*R relaxation times than NSWMH (figure). High-resolution images showed numerous dilated perivascular spaces (dPVS) at the cortico-subcortical junction, outside but close to areas of significant differences, confirming that dPVS do not drive these differences.
Conclusions: Our results support the hypothesis that tissue alterations differ between CSWMH and NSWMH and may originate from different mechanisms.
AS14-004
GENETICS AND BIOMARKERS
Oral
A PHARMACOEPIGENETIC STUDY IDENTIFIES AN ALTERED METHYLATION PATTERN ASSOCIATED WITH VASCULAR RECURRENCE IN ASPIRIN TREATED PATIENTS
C. Gallego Fábrega1, C. Carrera2, E. Muiño1, C. Natalia1, A. Pezzini3, P. Fontana4, J.L. Reny- Jean-Luc5, J. Krupinski6, J. Montaner2 and I. Fernandez1
1Fundacio Docencia i Recerca Mutua de Terrassa, Stroke pharmacogenomics and genetics, Terrassa, Spain
2Vall d'Hebron Institute of Research, Neurovascular Research Laboratory, Barcelona, Spain
3Clinica Neurologica- Università degli Studi di Brescia, Dipartimento di Scienze Cliniche e Sperimentali, Brescia, Italy
4Geneva University Hospitals, Division of Angiology and Haemostasis, Geneva, Switzerland
5Trois-Chêne Hospital- University Hospitals of Geneva, Division of Internal Medicine- and Rehabilitation, Geneva, Switzerland
Background: Aspirin is one of the most widely used antiplatelet agents in secondary prevention of stroke. The cumulative risk of vascular recurrence is up to 54% at 10 years. Despite pharmacogenetic studies efforts, the causes of aspirin resistance variability remain unclear. Our aim was to study whether epigenetics could be associated with the risk of vascular recurrence in aspirin treated stroke patients.
Methods: We performed an epigenetic study in 327 patients treated with aspirin. In the discovery study, 450.000 CpG sites were analyzed, using the Infinium Human Methylation 450 Beadchip (Ilumina) in 38 ischemic stroke patients (19 cases and 19 controls). In a second stage, three selected CpGs were analyzed by MassArray EpiTYPER, in 289 new patients from an independent cohort (10% cases). The vascular recurrence was detected by telephone interviews during the first year after ischemic event.
All pre-processing, correction, normalization and analysis steps were implemented using R and Illumina GenomeStudio software package. Mann-Whitney U-test was used to analyze the levels of methylation.
Results: Joint analysis of first and second stage identified an epigenome-wide association of a CpG site with vascular recurrence (p-value = 1.79 × 10−07, which pass FDR correction). This CpG site is located in a gene involved in TGF-β1 signaling and PAI-1 transcription, both proteins directly related with increased risk of ischemic cardiovascular events.
Conclusions: Differential methylation status is associated with vascular recurrence in aspirin-treated stroke patients and may involve the regulation of TGF-β1 signaling and PAI-1 transcription.
AS17-038
GENETICS AND BIOMARKERS
Oral
SHAPE OF THE CENTRAL SULCUS AND DISABILITY AFTER SUBCORTICAL STROKE: A MOTOR RESERVE HYPOTHESIS
E. Jouvent1, Z.Y. Sun2, F. De Guio3, E. Duchesnay4, M. Duering5, S. Ropele6, M. Dichgans5, J.F. Mangin7 and H. Chabriat8
1Hôpital Lariboisière, Neurology, PARIS, France
2NEUROSPIN- CEA- SACLAY, LNAO, SACLAY, France
3INSERM, NEUROLOGY, Paris, France
4NEUROSPIN- CEA, STATISTICS, SACLAY, France
5INSTITUTE FOR STROKE AND DEMENTIA RESEARCH, NEUROLOGY, MUNICH, Germany
6GRAZ UNIVERSITY, NEUROLOGY, GRAZ, Austria
7NEUROSPIN, LNAO, SACLAY, France
8Lariboisière hospital, Neurology, Paris, France
Abstract
Background: Both brain and cognitive reserves modulate the clinical impact of chronic brain diseases. Whether a motor reserve also modulates the relationships between stroke and disability is unknown. We aimed to determine whether the shape of the central sulcus, a marker of the development of underlying motor connections, is independently associated with disability in patients with a positive history of small subcortical ischemic stroke.
Methods: Shapes of central sulci were reconstructed from high-resolution MRI and ordered without supervision according to a validated algorithm in 166 patients with a positive history of small subcortical ischemic stroke caused by CADASIL, a severe monogenic cerebral small vessel disease affecting young patients (figure 1). Ordinal logistic regression modeling was used to test the relationships between modified Rankin scale, a disability scale strongly weighted towards motor disability, and sulcal shape.
Results: Modified Rankin scale was strongly associated with sulcal shape, independent of age, sex and level of education (proportional odds ratio = 1.19, 95%CI = [1.06–1.35], p = 0.002). Results remained significant after further adjustment for brain atrophy, volume of lacunes and volume of white matter hyperintensities of presumed vascular origin.
Conclusions: The severity of disability in patients with a positive history of small subcortical ischemic stroke caused by a severe cerebral small vessel disease is related to the shape of the central sulcus, independently of the main determinants of disability. These results support the concept of a motor reserve that could modulate the clinical severity in patients with a positive history of small subcortical ischemic stroke.
AS16-041
GENETICS AND BIOMARKERS
Oral
ENDOTHELIAL AUTOANTIBODIES AND FUNCTIONAL OUTCOME AFTER STROKE - AN ANALYSIS FROM THE PROSPECTIVE STROKE COHORT WITH INCIDENT STROKE BERLIN (PROSCIS-B)
T. Liman1, P. Heuschmann2, S. Wiedmann2, M.S.V. Elkind3, D. Dragun4 and M. Endres5
1Center for Stroke Research Berlin CSB, Berlin, Germany
2Institute of Clinical Epidemiology and Biometry, Institute of Clinical Epidemiology and Biometry, Würzburg, Germany
3Department of Neurology- College of Physicians and Surgeons- and Department of Epidemiology- Mailman School of Public Health, Columbia University, New York City, USA
4Department of Nephrology, Charité, Berlin, Germany
5Center for Stroke Research Berlin CSB, Neurology, Berlin, Germany
Abstract
Background: Presence of antiendothelial autoantibodies (AEA) is associated with worse outcome in animal models of cerebrovascular diseases and traumatic brain injury. Our aim was to investigate the impact of high levels of AEA on long-term functional outcome after ischemic stroke.
Methods: Data were collected from the Prospective Study with Incident Stroke Berlin (PROSCIS-B; NCT01364168). PROSCIS is a prospective observational hospital-based cohort study investigating the long-term vascular risk after first-ever stroke. Association of baseline levels of AEA targeting vascular receptors such as angiotensin II type 1 (AT1R), Endothelin-1 type A (ETAR), complement factor 3 and 5 (C3aR, C5aR), vascular endothelial growth factor receptor 1, 2 (VEGFR1, 2) as well as VEGF A and B with functional outcome defined as modified Rankin Scale 0–2 vs 3–6 at 1 year after stroke were investigated using multivariate logistic regression analyses.
Results: From March 2010 to May 2013, 598 patients with first ischemic stroke and baseline data on AEA levels were included. Levels of AEA were positively correlated among each other (r > 0.4, p < 0.01). In multivariate analysis adjusted for age, sex, ischemic stroke subtype, stroke severity, vascular risk factors (hypertension, diabetes mellitus, coronary artery disease), high levels of VEGFB (OR 1.8; 95%CI 1.1–3.1), VEGF2R (OR1.8; 95%CI 1.1–3.0) and C3aR (OR1.9; 95%CI 1.1–3.2) were independently associated with poor outcome (mRS 3–6, quartile 4 vs other).
Conclusions: Our study showed that patients with (pre-stroke) high levels of AEA such as VEGF2R, VEGFB, and C3aR have worse long-term outcome after stroke. However, the underlying pathophysiological mechanisms need further investigation.
AS26-001
GENETICS AND BIOMARKERS
Oral
PERIVASCULAR SPACES ARE INCREASED IN BOTH SPORADIC AND HEREDITARY (DUTCH-TYPE) CEREBRAL AMYLOID ANGIOPATHY
S. Martinez-Ramirez1, S. Van Rooden2, A. Charidimou1, M.E. Gurol1, J. van der Grond2, A. van Opstal2, M. Wermer3, G. Terwindt3, S.M. Greenberg1, M. Van Buchem2 and A. Viswanathan1
1Massachusetts General Hospital, Neurology, Boston- MA, USA
2Leiden University Medical Center, Radiology, Leiden, Netherlands
3Leiden University Medical Center, Neurology, Leiden, Netherlands
Abstract
Background: Increased perivascular spaces in the centrum semiovale(CSO-PVS) have been associated with cerebral amyloid angiopathy(CAA).We aimed to confirm this link in both sporadic and hereditary forms of the disease, and determine whether increased CSO-PVS can predict sporadic CAA even when lobar hemorrhages (micro and macrobleeds) are absent.
Methods: We studied a retrospective hospital-based cohort consisting of 63 individuals aged>55 having brain MRI and pathological assessment of CAA(mean age 73.6 ± 8.5,46% female),and a separate cohort consisting of 27 carriers and 27 age-matched non-carriers of the hereditary cerebral hemorrhage with amyloidosis–Dutch type(HCHWA-D)(mean age 46.7 ± 12.8,61.1% female).CSO-PVS volume was quantified on a single MRI slice using a computer-assisted segmentation method and expressed as the relative volume of the intracranial volume in that particular slice(CSO-PVSrv).We compared CSO-PVSrv between subjects with and without the disease in both cohorts; and non-CAA, CAA without hemorrhage and CAA with hemorrhage cases in the hospital-based cohort. All variables reaching p < 0.1 in bivariate analyses were entered in logistic regression models.
Results: In both hospital and Dutch cohorts, cases with CAA had a significantly higher CSO-PVSrv than cases without(median[IQR] 3.7%[2.5–5.3] vs 1.8%[1.2–2.4],p < 0.0001; 3.8%[0.6–6.2] vs 0.7%[0.4–1.6],p = 0.007, respectively);in regression models, sporadic CAA(p = 0.008) but not HCHWA-D was associated with increasing CSO-PVSrv.In the hospital-based cohort, compared to non-CAA cases, CSO-PVSrv was higher in both CAA cases with hemorrhage(4.4%[2.6–6.1] vs 1.8%[1.2–2.4],p < 0.001)and without(3%[2.4–3.6] vs 1.8%[1.2–2.4],p = 0.005);in regression models, increasing CSO-PVSrv was independently associated with CAA, both when hemorrhage was present(OR[95% CI] = 3.35[0.94–5.76],p = 0.006)and absent(OR[95% CI] = 2.39[0.05–4.72],p = 0.04).
Conclusions: Increased CSO-PVS volume is a consistent MRI marker of cerebrovascular amyloidosis, and a promising diagnostic tool for sporadic CAA without hemorrhagic manifestations.
AS16-063
GENETICS AND BIOMARKERS
Oral
WHAT VASCULAR RISK FACTORS CAUSE LACUNAR STROKE? AN EPIDEMIOLOGICAL AND GENETIC STUDY
L. Rutten-Jacobs1, M. Traylor2, A. Hassan3 and H. Markus1
1University of Cambridge, Clinical Neurosciences- Stroke Research Group, Cambridge, United Kingdom
2King’s College London, Department of Medical & Molecular Genetics, London, United Kingdom
3Leeds General Infirmary- Leeds Teaching Hospitals NHS Trust, Department of Neurology, Leeds, United Kingdom
Abstract
Background: Differing associations of vascular risk factors with lacunar infarct have been reported. A major factor underlying this may be accuracy of diagnosis which has often been based on a clinical lacunar syndrome and CT imaging; MRI based subtyping has been shown to be more accurate. In a MRI-verified cohort of lacunar infarct patients we investigated the association of modifiable risk factors with lacunar infarction and explored the causal nature of these associations using a polygenic risk score approach.
Methods: 1023 patients with lacunar infarction (mean age 56.7 (SD 8.5), range 20–70), were recruited from 72 stroke centres throughout the UK. We compared risk factor profiles (hypertension, diabetes, hyperlipidaemia, smoking, alcohol, body mass index) between patients and 1962 stroke-free population controls of similar age using multivariable logistic regression. Weighted genetic risk scores were constructed for each risk factor by combining genome-wide significant variants from previous association studies. The genetic risk scores were tested for association with lacunar infarction.
Results: Hypertension (OR 2.21 (95% CI 1.85–2.64)), diabetes (OR 2.10 (95% CI 1.61–2.73)), dyslipidaemia (OR 1.74 (95% CI 1.46–2.07)) and smoking (OR 1.65 (95% CI 1.39–1.96)) were associated with lacunar infarct patients compared to healthy controls independent of other risk factors. The genetic risk score for hypertension was significantly associated with lacunar infarction (OR 2.03 (95% CI 1.15–3.57)).
Conclusions: Our data support a role for genetic predisposition to hypertension in the causal pathway of lacunar infarction. Diabetes, dyslipidaemia and smoking were also associated but there was no association of genetic risk scores for these risk factors.
AS28-029
GENETICS AND BIOMARKERS
Oral
CADASIL: MIGRAINE, ENCEPHALOPATHY, STROKE AND THEIR INTER-RELATIONSHIPS
R. Tan1 and H. Markus1
1University of Cambridge, Clinical Neurosciences, Cambridge, United Kingdom
Abstract
Background: CADASIL is the most common monogenic cause of cerebral small vessel disease. Migraine is a common manifestation of CADASIL but its treatment responses are not well described, and its relationship to stroke risk unknown. Encephalopathy is a less common presentation; it has been suggested it is related to migraine. We characterised migraine patterns and treatment responses in CADASIL, and examined associations between migraine and both stroke risk and encephalopathy.
Methods: 300 CADASIL patients were prospectively recruited from a national referral clinic. Migraine was classified according to the International Headache Classification.
Results: Migraine was present in 226(75.3%), and the presenting feature in 203(67.7%). It was usually accompanied by aura (89.8%), and often complicated. Patients showed variable responses to a variety of drugs for migraine. Of 24 given triptans, 45.5% had good or partial responses. None had complications following triptans.
Migraineurs had lower cumulative incidence of stroke than non-migraineurs (HR = 0.46, 95%CI 0.3–0.6, p = 1.6 × 10−6). Thirty-three (11.0%) patients experienced encephalopathy lasting on average 8.1 ± 3.4 days. Patients with migraine with aura had higher odds of encephalopathy (OR = 5.4, 95%CI 1.6–28.4, p = 0.002). Patients with confusional aura had higher odds of encephalopathy than those with other aura types (OR = 2.5, 95%CI 1.0–5.8, p = 0.04).
Conclusions: Migraine with aura is a prominent feature of CADASIL. Treatment responses are similar to those seen in the general migraine population and no complications were observed with triptan use. Migraine with aura was associated with increased risk of encephalopathy suggesting they may share pathophysiological mechanisms. The protective effect of migraine on stroke risk needs confirming in future studies.
AS18-002
HEART AND BRAIN
Oral
TIMING OF INITIATION OF ORAL ANTICOAGULANTS IN PATIENTS WITH ACUTE ISCHEMIC STROKE AND ATRIAL FIBRILLATION - THE OBSERVATIONAL PRE-TIMING STUDY
S. Åsberg1, B. Norrving2, Z. Hijazi3, J. Oldgren3, P. Öhagen3 and T. Andreas1
1Uppsala University, Department of Medical Sciences- Cardiovascular epidemiology, Uppsala, Sweden
2Lund University, Deptartment of Clinical Sciences, Lund, Sweden
3Uppsala University, Uppsala Clinical Research Center, Uppsala, Sweden
Abstract
Background: The optimal time to start secondary stroke prevention with oral anticoagulation (OAC) in patients with atrial fibrillation (AF) and acute ischemic stroke (AIS) is undetermined. We analyzed use of OAC (warfarin or novel OAC) in the acute setting, proportions of recurrent AIS and symptomatic intracerebral hemorrhage (SICH) during hospitalization, and all-cause mortality at 90 days.
Methods: This medical record review study included all consecutive patients with AIS and AF registered in the Swedish Stroke Register during 2014 at Skåne University Hospital, Lund and Uppsala University Hospital.
Results: We identified 294 patients (mean age 80.4 years, 135 (45.9%) women) of whom 45 (15.3%) died during hospitalization. Of the 249 patients discharged alive, 159 (63.9%) received OAC, 116 (46.7%) were OAC-naïve and 43 (17.3%) were OAC-experienced, while 25 (10.0%) discontinued OAC and 65 (26.1%) did not receive OAC neither before nor after AIS. OAC therapy was initiated at 5 days (mean and median) after admission. In all 294 patients, recurrent AIS occurred in 13 (4.4%) and SICH in 9 (3.1%) during hospitalization (mean 16 days). Death at 90 days ranged from 4 (4.3%) in patients on OAC, to 68 (51.1%) in those who discontinued or never received OAC therapy after AIS.
Conclusions: OAC therapy was initiated early after AIS and the proportions of recurrent AIS and SICH was low. The wide range in mortality, based on therapy subgroups, affirmed the difficulties to evaluate efficacy and safety of early OAC therapy in observational studies and put emphasis on the need for randomized trials in this field.
AS28-005
HEART AND BRAIN
Oral
EMBOLIC STROKE OF UNKNOWN SOURCE IN PATIENTS WITH ATRIAL SEPTUM DEFECT AND PATENT FORAMEN OVALE: DIFFERENCE AND SIMILARITIES
C. Delabays1, C. Pamela1, E. Eeckhout2, D. Alain2, E. Ashraf1 and M. Patrik1
Background: Paradoxical embolism from right-to-left shunt through a patent foramen ovale (PFO) is a well-characterized cause of embolic strokes of undetermined source (ESUS). In order to better understand the pathogenic role of atrial septum defects (ASD), we compared them with ESUS of high and low likelihood of being related to PFO.
Methods: In the Acute STroke Registry and Analysis of Lausanne (ASTRAL), we calculated prevalence of PFO and ASD in ESUS patient undergoing echocardiography, and odds ratios (OR) when to compared to non-cryptogenic strokes. Using the Risk of Paradoxical Embolism (RoPE) score, we divided cryptogenic PFO patients in high (HL-PFO, RoPE 8–10) and low-likelihood (LL-PFO, RoPE 0–4) of PFO-related stroke. We then performed univariate comparison of epidemiological, clinical and radiological variables of both group with ESUS ASD patients.
Results: Among all ESUS, prevalence for ASD and PFO were 1.3% and 36.8% respectively. When compared to non-cryptogenic stroke, ASD and PFO were associated with ESUS (OR of 5.2, CI = 1.6–16.6, and 2.8, CI = 2.1–3.8). Compared with HL-PFO, ASD were older, more often female, had more cardiovascular risk factors (CVRF) and silent strokes. Compared with LL-PFO, ASD group was significantly younger, more often female, and had less CVRF. No differences were found for clinical and radiological characteristics and outcome.
Conclusions: In ESUS, ASD seems to be a rare but significant stroke risk factor. Given that characteristics of such patients lie in-between high and low-likelihood paradoxical PFO-stroke, a thorough workup for other stroke mechanisms is warranted in ASD patients before routine ASD closure.
AS18-017
HEART AND BRAIN
Oral
LEFT ATRIAL APPENDAGE OCCLUSION VERSUS STANDARD MEDICAL CARE IN PATIENTS WITH ATRIAL FIBRILLATION AND INTRACEREBRAL HEMORRHAGE: A PROPENSITY SCORE MATCHED FOLLOW-UP STUDY
S.P. Johnsen1, J.E. Nielsen-Kudsk2, M. Rosenqvist3, P. Wester4, D. Damgaard5, J. Lund6, O. De Backer7, S. Pakarinen8, J. Odenstedt9, S. Vikman10, B. Sahlgren3, O. Kongstad11 and D.W. Krieger12
1, Denmark
2Aarhus University Hospital, Department of Cardiology, Aarhus, Denmark
3Karolinska Institute, Department of Cardiology, Stockholm, Sweden
4Umea University, Stroke Center, Umea, Sweden
5Aarhus University Hospital, Department of Neurology, Aarhus, Denmark
6Turku University Hospital, Department of Cardiology, Turku, Finland
7Rigshospitalet, Department of Cardiology, Copenhagen, Denmark
8Helsinki University Hospital, Department of Cardiology, Helsinki, Finland
9Sahlgrenska University Hospital, Department of Cardiology, Gothenburg, Sweden
10Tampere University Hospital, Heart Center, Tampere, Finland
11Skåne University Hospital, Department of Cardiology, Lund, Sweden
12University of Zurich, Comprehensive Stroke Center- Dept. Neurology, Zurich, Switzerland
Abstract
Background: There is no consensus on stroke prevention in patients with atrial fibrillation (AF) sustaining an intracerebral hemorrhage (ICH). These patients have an increased risk for both ischemic stroke and recurrent ICH. Cathether-based Left Atrial Appendage Occlusion (LAAO) represents an alternative treatment for these patients. We aimed to compare the prognosis in patients with AF and ICH having a LAAO versus patients receiving standard medical therapy.
Methods: 127 patients from the Nordic countries with AF and previous ICH who underwent LAAO were retrospectively compared to a propensity score (PS)-matched group of 127 patients receiving standard medical therapy. The control patients were identified from the Danish National Stroke Register among 787 patients with AF and ICH. Patients with LAAO were followed from the implantation date and the patients in the standard care group were followed from day 180 after ICH. The primary endpoint was a composite of mortality, stroke and major bleeding.
Results: The present study suggests a substantial reduction of the combined endpoint (Hazard Ratio 0.26, 95%CI: 0.11–0.63) in the LAAO group as compared to the standard medically treated group. Median length of follow-up was 208 days.
Conclusions: In this propensity score matched study, LAAO was suggested to be of potential clinical benefit in AF patients sustaining an ICH. Due to study design limitations, these results have to be confirmed in a randomized clinical trial.
AS16-039
HEART AND BRAIN
Oral
WHAT MAKES NEW ISCHEMIC LESIONS SYMPTOMATIC AFTER AORTIC VALVE REPLACEMENT?
R. Leker1, S. Messe2, G. Erus3, M. Billelo3, M. Fanning2, M. Acker4, E. Massaro2, T. Floyd5 and S. Kassner2
1, Israel
2University of Pennsylvania, Neurology, Philadelphia, USA
3University of Pennsylvania, Radiology, Philadelphia, USA
4University of Pennsylvania, Cardiothoracic Surgery, Philadelphia, USA
5State University NY, Anesthesiology, New York, USA
Abstract
Background: New diffusion weighted imaging (DWI) lesions indicative of acute cerebral infarction are common after cardiothoracic surgery. However, most of these lesions are asymptomatic and what determines whether a lesion would become symptomatic remains unclear.
Methods: Patients over 65 years undergoing surgical aortic valve replacement (AVR) for calcific stenosis were prospectively recruited (n = 196). All patients underwent neurological evaluation preoperatively and on post-op days 1, 3, and 7, and MRI scans on planned post-op day 5. Among those with new post-operative DWI lesions, we compared baseline characteristics, surgical and imaging data between symptomatic and asymptomatic subjects.
Results: Of the 129 patients who completed a post-surgical MRI, 79 (61%) had new DWI lesions and 17 (21.5%) had new neurological symptoms consistent with acute stroke. In univariate analysis, neurological symptoms were associated with longer bypass times, smaller drops in arterial pressures during surgery, more concomitant procedures, higher number of new DWI lesions and lesion volumes and higher old lesion burden on FLAIR. Symptomatic lesions also more frequently involved the parietal white matter and were more common in right hemispheric lesions. Logistic regression adjusting for lesion volume and number of lesions identified right parietal lesions as positive predictors of symptomatic stroke (OR 9.03 95% CI 1.1.-73.2).
Conclusions: New DWI lesions are common after AVR, but most are asymptomatic. Patients are more likely to have symptoms with right parietal involvement, with larger absolute DWI lesion count and volumes, and with longer bypass durations, complicated surgeries and higher pre-existing lesion burdens.
AS20-026
HEART AND BRAIN
Oral
OPTIMAL TIMING OF INITIATING ANTICOAGULANT TREATMENT FOLLOWING INTRACEREBRAL HAEMORRHAGE IN PATIENTS WITH ATRIAL FIBRILLATION. A NATIONWIDE SWEDISH OBSERVATIONAL STUDY
J. Pennlert1, R. Overholser2, K. Asplund1, B. Carlberg1, B. Van Rompaye2, P.G. Wiklund1 and M. Eriksson3
1Umea University, Public Health and Clinical Medicine, Umeå, Sweden
2Ghent University, Applied Mathematics Computer Science and Statistics, Ghent, Belgium
3Umea University, Department of Statistics - Umeå School of Business and Economics, Umeå, Sweden
Abstract
Background: There is a lack of evidence on the optimal anticoagulant (AC) treatment strategy in patients with atrial fibrillation (AF) who survive intracerebral haemorrhage (ICH). We explored the relationship between the timing of initiating AC treatment and risks of severe thromboembolic events, bleeding events and death by other cause in ICH survivors with AF.
Methods: Patients with AF discharged alive after a first-ever ICH were identified in the Swedish stroke registry, Riksstroke, 2005–2012. Linkage with other national registers to find information on treatment, comorbidity and outcome was performed. The optimal timing of treatment was described through cumulative incidence functions for any event, and for each event type separately.
Results: 2619 ICH survivors with AF, constituting 5759 person-years of follow-up, were included. When AC treatment was started 8–12 weeks after ICH, the 3-year-incidence of severe outcome events was reduced. This was true for men and women with high and low risk profiles. E.g. the incidence of an event within 3 years was 18.0% vs 27.5% (95% CI of difference: 4.5% to 14.3%) starting AC at 10 weeks compared with no treatment for a high-risk woman. Although not statistically significant, initiating AC treatment before week 8 may increase the incidence of severe bleedings. The beneficial time frame of initiating treatment was longer in high-risk patients.
Conclusions: This nationwide observational study suggests that anticoagulant treatment may be initiated between week 8 and 12 following ICH in patients with AF to optimize benefit from treatment and minimize risk.
AS04-009
HEART AND BRAIN
Oral
STROKE SUB-TYPE, TOPOGRAPHY AND MODIFIED RANKIN SCORE (mRS) IN PATIENTS WITH SUB CLINICAL ATRIAL FIBRILLATION: RESULTS FROM THE ASSERT STUDY
K. Perera1, J. Wang2, M. Sharma1, J. Healey3 and S. Connolly3
1McMaster University- Population Health Research Institute, Medicine - Neurology, Hamilton, Canada
2Population Health Research Institute, statistics, Hamilton, Canada
3McMaster University- Population Health Research Institute, Medicine - Cardiology, Hamilton, Canada
Abstract
Background: The relationship between short-lasting, sub-clinical atrial fibrillation (SCAF) and stroke is unclear. Among 2580 participants in the ASSERT trial, SCAF >6 minutes in duration was associated with a 2.5-fold increased risk of stroke; however, fewer than 20% participants suffering stroke during the study had evidence of SCAF in the preceding 30 days, raising the possibility that stroke mechanism may be different than for clinical AF.
Methods: All stroke events in the ASSERT trial were adjudicated by 2 stroke neurologists blinded to SCAF status. Strokes were classified as cortical vs. sub-cortical, and sub-typed using modified TOAST criteria (which did not diagnose cardio-embolic stroke solely on the basis of SCAF or sick sinus syndrome). Stroke severity was measured at 7 and 30 days post-stroke using the mRS.
Results: Of the 44 participants with ischemic strokes 19 had SCAF. No significant differences were noted in stroke subtype, topography or mRS between patients with vs. without SCAF who suffered stroke and patients who had SCAF prior to stroke vs. post stroke.
Conclusions: In the ASSERT trial, stroke severity was similar for patients with and without SCAF. Only 26% of SCAF-related strokes were categorized as cardio-embolic and 26% were lacunar. These data suggest a complex association between SCAF and stroke, with several different stroke mechanisms, some of which may not be prevented with oral anticoagulation.
AS18-035
HEART AND BRAIN
Oral
EARLY START OF NOAC AFTER AN ACUTE CEREBROVASCULAR EVENT - RISK OF INTRACRANIAL HEMORRHAGE AND RECURRENT EVENTS: PROSPECTIVE REAL-LIFE COHORT STUDY FROM THE NOACISP REGISTRY
D. Seiffge1, C. Traenka1, A. Polymeris1, L. Hert1, R. Sutter2, N. Peters1, P. Lyrer1, L. Bonati1, S. Engelter1 and G.M. De Marchis1
1University Hospital Basel- University of Basel, Stroke Center and Neurology, Basel, Switzerland
2University Hospital Basel- University of Basel, Department of Critical Care, Basel, Switzerland
Abstract
Background: Patients with recent ischemic stroke (AIS) were excluded from randomized clinical trials (RCT) assessing NOACs. Real-life clinical practice is different, as NOACs are started after AIS even before the time frames studied in the RCTs (early NOAC-starts). This prospective real-life cohort study sought to assess the (i) the frequency of early NOAC-starts, (ii) the risk of ICH and (iii) recurrent AIS/TIA within 6 months of the index AIS/TIA.
Methods: Prospective cohort study from the single-center registry NOACISP at the University Hospital Basel, Switzerland. Patients with AIS/TIA and nonvalvular atrial fibrillation who received either NOAC (NOACafter) or Vitamin K antagonists (VKAafter) were followed-up for at least 6 month.
Results: 204 patients were included. In the NOACafter cohort, 155 patients received treatment with a median delay of 5 days (IQR 3–11) compared to 49 patients in the VKAafter cohort with a median delay of 4 (IQR 2–8) days. NOAC treatment was started earlier compared to the pivotal RCTs in 81% of patients. During follow-up, 1 ICH occurred in VKAafter; no ICH occurred in the NOACafter cohort. Recurrent AIS occurred in 6 patients (NOACafter n = 4 [3%] and VKAafter n = 2 [4%], P = 0.56).
Conclusions: In a current real-world setting at an academic stroke center, NOAC are started earlier than studied in the RCT in 81%, without an increased ICH risk. Recurrent AIS/TIA were six times more likely than ICH, a fact that need to be considered when choosing the time-point of OAC start after an AIS/TIA.
AS18-045
HEART AND BRAIN
Oral
FREQUENCY AND ASSOCIATIONS OF FAILURE TO ANTICOAGULATE FOR ATRIAL FIBRILLATION PRIOR TO ISCHAEMIC STROKE AND TIA: PROSPECTIVE MULTI CENTRE COHORT STUDY
D. Wilson1, A. Charidimou1, C. Shakeshaft1, G. Ambler2, M. White1, H. Cohen3, T. Yousry4, R. Al-Shahi Salman5, G.Y. Lip6, M.M. Brown1, H.R. Jager4 and D.J. Werring1
1Institute of Neurology, Brain repair and rehabilitation, London, United Kingdom
2University College London, Department of statistical science, London, United Kingdom
3University College London Hospitals NHS Foundation Trust, Haematology, London, United Kingdom
4National Hospital for Neurology and Neurosurgery, Lysholm Department of Neuroradiology, London, United Kingdom
5University of Edinburgh, Division of Clinical Neurosciences- Centre for Clinical Brain Sciences- School of Clinical Sciences, Edinburgh, United Kingdom
6University of Birmingham - City Hospital, Centre for Cardiovascular Sciences, Birmingham, United Kingdom
Abstract
Background: Oral anticoagulation reduces ischaemic stroke risk in patients with atrial fibrillation (AF) and is recommended in current guidelines; by contrast, aspirin is neither effective nor recommended. There are few data on the prevalence, characteristics and antithrombotic treatment of patients with AF-related ischaemic strokes associated with previously-known, but non-anticoagulated AF
Methods: In the CROMIS-2 multicentre prospective cohort study at 79 UK hospitals, we compared baseline demographics and risk factors between acute ischaemic stroke or TIA patients with previously-known but non-anticoagulated AF to those with newly-diagnosed AF. All patients were subsequently anticoagulated. We used t-tests and Chi squared tests for univariate analysis.
Results: Of 1496 patients, 538 (36%) had previously-known AF before their stroke, of whom 469 had an indication for anticoagulation (31% of the whole cohort) yet were not anticoagulated. Compared to those with newly diagnosed AF, patients with previously known AF were more likely to have a history of dementia (4% vs. 2%; p = 0.004) but were otherwise similar. Of note both CHADSVasc (median 2 [IQR 1 to 3] in both cohorts) and HAS-BLED scores were similar (median 2 [IQR 1 to 3] in both cohorts). Both cohorts had a similar prevalence of CHADSVasc ≥ 1 (87% vs.89% p = 0.72).
Conclusions: Over one third of our cohort had known AF prior to their qualifying stroke or TIA, yet were not prescribed anticoagulation despite 87% having an indication according to current guidelines (pre-stroke CHA2DS2-VASc ≥1). Only a history of dementia was associated with non-use of anticoagulation but this only represented a small number of patients.
AS18-046
HEART AND BRAIN
Oral
COMPARISONS OF OUTCOMES IN PATIENTS WITH ATRIAL FIBRILLATION OR REQUIRING CAROTID ENDARTERECTOMY: RESULTS FROM THE TRIPLE ANTIPLATELETS FOR REDUCING DEPENDENCY AFTER ISCHAEMIC STROKE (TARDIS) TRIAL
L. Woodhouse1, J. Appleton1, R. Dineen2, N. Sprigg1 and P. Bath1
1University of Nottingham, Stroke- Division of Clinical Neuroscience, Nottingham, United Kingdom
2University of Nottingham, Radiological Sciences- Division of Clinical Neuroscience, Nottingham, United Kingdom
Abstract
Background: Atrial fibrillation (AF) and carotid stenosis are common antecedents of ischaemic stroke (IS) and TIA, and require anticoagulation and carotid endarterectomy (CEA) respectively to reduce recurrence. Whether these interventions improve outcome is unclear and is examined here using data from the ongoing TARDIS trial.
Methods: TARDIS is assessing the safety and efficacy of intensive vs guideline antiplatelet agents in 4,100 patients with acute non-cardioembolic IS or TIA. Information on AF diagnosis, and CEA need, and recurrent events and functional outcome are assessed centrally with blinding to treatment assignment at day 90. Data are unadjusted odds ratio (OR) or mean difference (MD) with 95% confidence interval (CI) relative to no AF/CEA.
Results: Of 2973 recruited patients, 108 had AF and 81 a CEA. In comparison with others, AF and CEA patients were older (4.5 and 2.3 years respectively) and more likely to have been enrolled with stroke than TIA (p < 0.001, p = 0.029). AF patients were more likely to have a stroke/TIA recurrence (OR 2.7, 95% CI 1.5–4.6; 7 before diagnosis, 9 afterwards), and have a shift to more dependency (modified Rankin Scale, ordinal OR 2.0, 95% CI 1.4–2.8) and disability (Barthel Index, MD −11.3, 95% CI −15.1 to −7.5). CEA patients were more likely to have a recurrent stroke (OR 2.3, 95% CI 1.0–5.1; 5 before and 2 peri- or post-operatively).
Conclusions: Recurrence was more common in patients with AF and those needing CEA than in other TARDIS patients; patients with AF also had worse functional outcomes.
AS21-004
IMAGING
Oral
MULTI-PARAMETER CT PERFUSION IMAGING FOR PREDICTION OF INTRACEREBRAL HEMORRHAGE SECONDARY TO ACUTE ISCHEMIC STROKE
C. Batchelor1,2, C.D. D'Esterre2,3,4, P. Pordeli1,5, C. McDougall2,6, P. Wee2,6, L. Hur2,6, M. Boesen7, F. Alajlan3,4, M. Najm6, J.J. Shankar8, A. Khaw9,10, M. Rubiera11, J. Mandzia12, E. Fainardi13, T. Sajobi3,14, T.Y. Lee4,15, R.I. Aviv16, A.M. Demchuk1,2,3, M. Goyal1,2,3,4, B.K. Menon1,2,3,4,14
1Hotchkiss Brain Institute- University of Calgary- Alberta, Clinical Neurosciences, Calgary, Canada
2Seaman Family MR Centre- Alberta, Neuroscience, Calgary, Canada
3Calgary Stroke Program- Department of Clinical Neurosciences- University of Calgary- AB, Clinical Neurosciences, Calgary, Canada
4Department of Radiology- University of Calgary- Alberta, Clinical Neurosciences, Calgary, Canada
5University of Calgary, Department of Community Health Sciences- University of Calgary, Calgary, Canada
6University of Calgary, Clinical Neurosciences, Calgary, Canada
8Department of Neuroradiology and Diagnostic Imaging- Dalhousie University- Halifx- Canada, Neuroradiology, Halifax, Canada
9Lawson Health Research Institute and Robarts Research Institute- London- Ontario., Neurosciences, London, Canada
10Department of Clinical Neurosciences- University of Western Ontarios, Clinical Neurosciences, Ontario, Canada
11Department of Neurology- Hospital Vall d'Hebron- Ps. Vall d'Hebron- Barcelona- Spain, Neurology, Barcelona, Spain
12Department of Clinical Neurosciences- University of Western Ontario, Clinical Neurosciences, Western Ontario, Canada
13Department of Neurosciences and Rehabilitation- University Hospital- Ferrara- Italy, Neuroscience, Ferrara, Italy
14Department of Community Health Sciences- University of Calgary- Alberta, Health Sciences, Calgary, Canada
15Lawson Health Research Institute and Robarts Research Institute- Ontario, Clinical Neurosciences, London, Canada
16Sunnybrook Health Sciences Centre- Ontario, Clinical Neurosciences, London, Canada
Abstract
Background: Intra-cerebral hemorrhage (ICH) after acute ischemic stroke (AIS) therapy is a major complication. We sought to investigate for any association between various CT perfusion (CTP) parameters and post stroke ICH.
Methods: 291 AIS patients (113 excluded for no tPA) underwent CTP (150s) imaging within 12 hrs of onset. CTP software (GE Healthcare) was used to calculate CBF, CBV, Tmax, and permeability surface-area product (PS) functional maps. Ipsilateral hemisphere volumes (mL), normalized to z-axis coverage, were obtained for: 1) regions of very low CBV (lower 10th, 5th, and 2.5th percentiles) of the contralateral hemisphere (vlCBV10th, 5th, 2.5th), 2) CBF ≤7 ml min−1 (100 g)−1 (vCBF≤7), and 3) Tmax ≥ 16 s (vTmax16s). Mean values were obtained for: 1) PS within a Tmax ≥ 8 s (PSTmax), 2) PS within the total ipsilateral hemisphere (PSIpsi), and 3) Tmax within vTmax16s. The interaction parameter vlCBV10th x PSTmax was also calculated. ICH was determined using ECASS II criteria and assessed on 24–48 hr MRI/CT. Random forest analysis (RFA) was used to rank each parameter in order of importance for hemorrhage prediction.
Results: Figure 1 shows results for RFA and ROC analysis in 104 evaluable out of 178 AIS patients (43 hemorrhage, 61 no hemorrhage). PS within vlCBV and PS within Tmax ≥ 16 s parameters are most important for hemorrhage prediction in WM and GM respectively.
Conclusions: Combining multiple CTP parameters is necessary for robust hemorrhage prediction.
AS15-006
IMAGING
Oral
PULSE WAVE VELOCITY IS ASSOCIATED WITH EARLY CEREBRAL LESION GROWTH IN ISCHEMIC STROKE
D. Gasecki1, M. Kwarciany1, K. Kowalczyk1, T. Nowicki2, E. Szurowska2, P. Boutouyrie3, S. Laurent3, K. Narkiewicz4 and B. Karaszewski1
1Medical University of Gdansk, Department of Adult Neurology, Gdansk, Poland
2Medical University of Gdansk, Department of Radiology, Gdansk, Poland
3Université Paris-Descartes- INSERM U970, Dept. of Pharmacology, Paris, France
4Medical University of Gdansk, Hypertension Unit- Department of Hypertension and Diabetology, Gdansk, Poland
Abstract
Background: Pulse wave analysis (PWV), a marker of aortic stiffness, has independent predictive value for cardiovascular (CV) morbidity and mortality, including stroke, and for clinical and functional stroke prognosis. However, the relationship between aortic stiffness and objective and indirect tissue distraction parameters (neuroimaging) is not known. We measured the relation between aortic stiffness and other central hemodynamic indices and early growth of ischemic lesion.
Methods: We prospectively enrolled 75 patients with acute ischemic stroke, aged 63.4 ± 12.5 years, median National Institutes of Health stroke scale (NIHSS) scored 5 (interquartile range 3–8) at admission.
Carotid-femoral (CF) PWV, central systolic blood pressure (BP) and central augmentation index (cAIx) were measured (Sphygmocor) 5 (±2) days after stroke onset. Lesion growth was estimated semi-automatically (Brain Vision Analyzer) using DWI data obtained at admission and at 5 (±2) days after stroke.
The highest cerebral lesion growth was determined as the highest quintile in a standardized measure of DWI lesion volume increase (marked growth), and was compared with the lowest quintile (small growth) used as the reference group. Data were analysed with multivariate logistic regression.
Results: In univariate analysis, CF-PWV (P = 0.007), but none of central and peripheral BP-derived parameters, was significantly associated with marked cerebral lesion growth. In multivariable regression logistic model, CF-PWV remained significantly associated with marked cerebral lesion growth after adjustment for age, use of rtPA, and peripheral mean blood pressure (OR = 1.96[95%CI,1.00–3.85];P = 0.049.
Conclusions: Increased aortic stiffness is independently associated with cerebral lesion growth in patients with acute ischemic stroke. Its deleterious effect is more important than that of BP.
AS22-013
IMAGING
Oral
LACUNES VARY ALONG A CONTINUUM OF SHAPES DEFINED BY ELONGATION AND PLANARITY AND ALIGN WITH PERFORATING VESSELS
B. Gesierich1, E. Duchesnay2, E. Jouvent3, H. Chabriat3, R. Schmidt4, J.F. Mangin2, M. Duering1, M. Dichgans1,5
1Klinikum der Universität München - Ludwig-Maximilians-Universität LMU, Institute for Stroke and Dementia Research, Munich, Germany
2CEA, Neurospin, Saclay, France
3DHU NeuroVasc- Hopital Lariboisiere- APHP, Department of Neurology, Paris, France
4Medical University of Graz, Department of Neurology, Graz, Austria
5Munich Cluster for Systems Neurology, SyNergy, Munich, Germany
Abstract
Background: Lacunes are a clinically important manifestation of cerebral small vessel disease (SVD). However, their morphological features are still debated. We analyzed incident (i.e. newly appearing) lacunes in patients with cerebral autosomal-dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) thus excluding contamination by other lesions (e.g. perivascular spaces) and ethiologies (e.g. cardioembolism).
Methods: A total of 88 incident lacunes from 57 patients were segmented and three-dimensionally reconstructed. Anatomical distribution, diameter, surface area, volume, and compactness of lacunes were assessed. Shape was analyzed using a size, orientation and position invariant spectral shape descriptor.
Results: Lacunes were most abundant in the centrum semiovale and the basal ganglia. The spectral shape descriptor revealed a continuum of shapes, with no evidence for distinct subgroups or differences between brain regions. The shape continuum was characterized mainly by variations in elongation and planarity of the lacunes. The main axis and plane of lacunes were orientated along the perforating arteries but not along fiber tracts.
Conclusions: We conclude that the development of lacunes is primarily determined by the anatomy of the vascular network and not by that of white-matter.
AS21-024
IMAGING
Oral
DIAGNOSTIC ACCURACY OF CT ANGIOGRAPHY FOR EXTRACRANIAL INTERNAL CAROTID ARTERY PSEUDO-OCCLUSIONS IN ACUTE ISCHEMIC STROKE: A MR CLEAN SUBSTUDY
M. Kappelhof1, H.A. Marquering2, O.A. Berkhemer1, J. Borst1, A. van der Lugt3, W.H. van Zwam4, C.B.L.M. Majoie1 and B. Emmer3
1Academic Medical Center, Radiology, Amsterdam, Netherlands
2Academic Medical Center, Radiology- Biomedical Engineering and Physics, Amsterdam, Netherlands
3Erasmus Medical Center, Radiology, Rotterdam, Netherlands
4Maastricht University Medical Center, Radiology, Maastricht, Netherlands
Abstract
Background: Reperfusion by intra-arterial thrombectomy (IAT) within 6 hours of symptom onset has been proven effective in the treatment of acute ischemic stroke. However, extracranial internal carotid artery (ICA) occlusion can hamper access to the intracranial vasculature, lengthening time to reperfusion. CT angiography (CTA) defines extracranial ICA occlusion by absence of contrast in the vessel. Pseudo-occlusion occurs when sluggish contrast flow mimics an occlusion, while the artery is proven patent on digital subtraction angiography (DSA). As a result, pseudo-occlusions may influence treatment decisions for patients eligible for IAT. The aim of this study was to determine the diagnostic accuracy of CTA-based diagnosis of pseudo-occlusions, compared to DSA, in the MRCLEAN trial population.
Methods: Patients with carotid pathology on CTA and with DSA images available were included. The CTA images were classified by an interventional neuroradiologist into atherosclerotic occlusion or near-occlusion, dissection, or suspected pseudo-occlusion. The same was done for the DSA images after additional blinding. Subsequently, CTA- and DSA-based diagnoses were compared using DSA as gold standard.
Results: In 138 patients, carotid pathology was present on CTA. Patients without DSA images were excluded, leaving 52 patients for analysis. Based on DSA, 18 (34.6%) patients had pseudo-occlusions, 18 (34.6%) atherosclerotic (near-)occlusions, and 16 (30.1%) dissections. T-occlusions occurred more frequently in patients with pseudo-occlusion (82.4% vs. 14.3%, p < 0.001). The sensitivity of CTA for detecting pseudo-occlusions was 82.4% (95% CI 0.59–0.94), the specificity 80.0% (95% CI 0.64–0.90). The Kappa coefficient was 0.588 (p < 0.001).
Conclusions: CTA is accurate in distinguishing extracranial ICA pseudo-occlusions from true occlusions or dissections.
AS21-027
IMAGING
Oral
VARIABLES INFLUENCING THE ASSOCIATION BETWEEN NON-VIABLE TISSUE MEASURED ON PERFUSION CT AND CLINICAL OUTCOME
C. Laredo1, A. Renú1, J.C. Pariente1, L. Oleaga1, X. Urra1, L. San Román1, L. Lull1, S. Rudilosso1, J. Blasco1, V. Obach1, S. Amaro1 and Á. Chamorro1
1Hospital Clinic, Institut Clinic de Neurociències, Barcelona, Spain
Abstract
Background: The objective was to assess the variables that interact on the association between Non-Viable Tissue (NVT) defined in Perfusion-CT (PCT) and Clinical Outcome.
Methods: A prospective cohort of 329 patients with acute stroke due to proximal occlusion in the carotid territory who had whole-brain baseline PCT was analyzed. NVT was computed in PCT Maps (Cerebral Blood Flow < 30% of normal brain), and clinical outcome was evaluated at 90 days using the modified Rankin Scale (mRS) and analyzed as an ordinal variable. The association between NVT and mRS was assessed using ordinal regression models. An interaction term was added to determine whether this association was dependent of baseline variables, and subgroup analyses were performed accordingly. Collateral status and perfusion profile were categorized according to usual definitions.
Results: As shown in the figure, the association between NVT and mRS at day 90 was significantly modified by baseline NIHSS, baseline ASPECTS, collateral status, time from stroke onset to PCT, perfusion profile, and reperfusion-therapy modality. The interaction with other variables such as age, glucose levels or gender was not significant.
Conclusions: Overall, greater volumes of NVT are associated to poor clinical outcome. However, this association is significantly modified by relevant baseline variables and by the type of reperfusion therapy administered in the acute phase. These variables should be taken into account when evaluating PCT data.
AS15-009
IMAGING
Oral
MORPHOLOGIC EVOLUTION AND REMODELING OF INTRACRANIAL ATHEROSCLEROSIS UNDER INTENSIVE RISK FACTOR CONTROL
T.W. Leung1
1The Chinese University of Hong Kong, Hong Kong, Hong Kong- China
Abstract
Background: In SAMMPRIS, the benefit of aggressive medical therapy over stenting persisted throughout the extended follow-up period. It is uncertain how plaques may evolve under this aggressive medical regimen, leading to a diminished rate of stroke relapses.
Methods: In a prospective academic-initiated study, we recruited 40 patients (mean age 63.4 ± 9.0 years) with acute strokes attributed to high-grade (≥70%) intracranial atherosclerotic stenosis for 3D-rotational angiograms before and after intensive medical therapy for 12 months. Treatment targets included low-density lipoprotein <70 mg/dl; HbA1c <6.5%; and systolic blood pressure <140 mmHg. We analyzed the morphologic and geometric evolution of the symptomatic plaques.
Results: Overall, the risk factor control reached the pre-specified goals. Plaque thickness, and hence luminal narrowing, significantly diminished at one year (from 1.50 ± 0.48 to 1.24 ± 0.42 mm; p < 0.001). The site of maximal stenosis shifted significantly towards mid-portion of the plaque (p < 0.001), leading to a diminished upstream angulation. The ulcers noted at baseline (n = 3) had all healed by one year. There was no significant change in terms of plaque length or lesion eccentricity.
Conclusions: Intracranial plaques might regress and positively remodel under intensive risk factor control. The associated morphologic changes might stabilize the plaques, alleviate unfavorable hemodynamics across the steno-occlusion, and hence reduce platelet aggregation or the risk of plaque rupture.
AS05-022
IMAGING
Oral
COMPARISON AND EXTERNAL VALIDATION OF IMAGING BASED SCORES (ABCD2-I AND ABCD3-I) VERSUS ABCD2 FOR STROKE PREDICTION AFTER TIA
A. Merwick1,2, G.W. Albers3, A. Chatzikonstantinou4, G.M. De Marchis5, J. Ferrari6, P.M. George3, M. Katan7, M. Knoflach8, J.S. Kim9, L. Li10, E. Lee9, J.M. Olivot11, F. Purroy12, N. Raposo11, P.M. Rothwell10, V. Sharma13, B. Song14, G. Tsivgoulis15, C. Walsh16 and P.J. Kelly2
1Chelsea and Westminster Hospital NHS Foundation trust, Department of Neurology, London, United Kingdom
2Mater Misericordiae University Hospital/Dublin Academic Medical Centre., Neurovascular Clinical Science Unit- Stroke Service and Department of Neurology, Dublin, Ireland
3Stanford Stroke Centre, Department of Neurology and Neurological Sciences, Palo Alto, USA
4Universitätsmedizin Mannheim- Ruprecht-Karls-Universität Heidelberg, Department of Neurology, Mannheim, Germany
5Department of Neurology, University Hospital of Basel, Basel, Switzerland
6Hospital Barmherzige Brueder, Department of Neurology, Vienna, Austria
7University Hospital of Zurich, Department of Neurology, Zurich, Switzerland
8Medical University of Innsbruck, Department of Neurology, Innsbruck, Austria
9University of Ulsan - Asan Medical Center, Department of Neurology, Seoul, Republic of Korea
10John Radcliffe Hospital, Stroke Prevention Research Unit, Oxford, United Kingdom
11Purpan University Hospital, Stroke Unit- Department of Neurology, Toulouse, France
12Hospitalt Universitari Arnau de Vilanova de Lleida. and Universitat de Lleida- Biomedical research institute of Lleida, Stroke Unit- Department of Neurology, Lleida, Spain
13National University Hospital- Singapore- and YLL School of Medicine- National University of Singapore, Division of Neurology- Department of Medicine, Singapore, Singapore
14the First Affiliated Hospital of Zhengzhou University, Department of Neurology, Zhengzhou, China
15University of Athens- School of Medicine, Second Department of Neurology, Athens, Greece
16University of Limerick, Department of Statistics, Limerick, Ireland
Abstract
Background: Inclusion of brain imaging alone (ABCD2-I) or recent TIA, brain and carotid imaging (ABCD3-I) with ABCD2 may improve stroke risk prediction and prevention after TIA. We aimed to compare and externally validate imaging-based scores versus ABCD2.
Methods: ABCD2, ABCD2-I and ABCD3-I scores were compared using 3535 TIA patients’ individual data. Index TIA was defined clinically as TIA most recently pre-DWI. Early stroke risk was determined prospectively.
Results: 7-day stroke risk increased with ABCD3-I category (p = 0.0005). Compared with ABCD2, both scores showed improved discrimination (c-statistic) for early stroke. However, discrimination was higher for ABCD3-I compared with ABCD2 and ABCD2-I, particularly at 2 and 7 days (p ≤ 0.002). Clinical net risk reclassification index (CNRI) was improved for ABCD3-I but not ABCD2-I (Table 2).
Conclusions: While both imaging-based scores were statistically-valid, ABCD3-I improved risk prediction compared with ABCD2 and ABCD2-I. Further clinical utility studies are needed.
AS21-036
IMAGING
Oral
E-ASPECTS SOFTWARE IS NON-INFERIOR TO NEURORADIOLOGISTS IN APPLYING THE ASPECTS SCORE TO CT SCANS OF ACUTE ISCHEMIC STROKE PATIENTS
S. Nagel1, D. Sinha2, D. Diana3, P. Papanagiotou4, K. Fassbender5, M. Essig6, J. Heidenreich7, A.A. Konstas8, S. Gerry9, C. Roffe10, J. Hampton-Till11 and I.Q. Grunwald12
1University Hospital Heidelberg, Department of Neurology, Heidelberg, Germany
2Southend University Hospital, NHS, Essex, United Kingdom
3Addenbrooke's Hospital, NHS, Cambridge, United Kingdom
4Bremen Hospital, Department of Neuroradiology, Bremen, Germany
5University Hospital Saarland, Department of Neurology, Homburg, Germany
6University of Manitoba, Department of Radiology, Winnipeg, USA
7Dalhousie University, Department of Diagnostic Radiology, Nova Scotia, Canada
8University of California, Dept. of Radiology, Los Angeles, USA
9University of Oxford, Centre for Statistics in Medicine, Oxford, United Kingdom
10North Staffordshire Combined Healthcare NHS Trust, Stroke Research, Stoke on Trent, United Kingdom
11Anglia Ruskin University, Clinical Trials Unit, Chelmsford, United Kingdom
12Anglia Ruskin University, Neuroscience Department, Chelmsford, United Kingdom
Abstract
Background: The Alberta Stroke Program Early CT score (ASPECTS) is an established 10-point quantitative topographic CT scan score to assess early ischemic changes. We performed a non-inferiority trial between e-ASPECTS software and neuroradiologists (NRAD) in scoring ASPECTS on non-contrast enhanced CT images (NECT) of acute ischemic stroke patients.
Methods: In this multicentre study, e-ASPECTS and three independent NRADs retrospectively and blindly assessed baseline NCCTs of 132 patients with acute anterior circulation ischemic stroke. Follow-up scans served as ground truth to determine the definite area of infarction. Sensitivity, specificity and accuracy (SSA) for region based and score based analysis, ROC curves, Bland-Altman plots and Matthews correlation coefficients (MCC) relative to the ground truth were calculated and comparisons were made between NRADs and different prespecified e-ASPECTS operating points. The non-inferiority margin was set to 10% for both sensitivity and specificity on region based analysis.
Results: In total 2640 (132 patients x 20 regions per patient) ASPECTS regions were scored. Mean time from onset to baseline CT was 146+/-124 min and median NIHSS was 11 (6–17, IQR). Median ASPECTS for ground truth on follow-up imaging was 8 (6.5–9, IQR). In the region based analysis, two e-ASPECTS operating points (SSA of 44%, 93%, 87% and 44%, 91%, 85%) were statistically non-inferior to all three NRADs (all p-values < 0.003). Both MCCs for e-ASPECTS were higher (0.36 and 0.34) than those of all NRADs (0.32. 0.31 and 0.3).
Conclusions: e-ASPECTS was non-inferior to three neuroradiologists in scoring ASPECTS on NECTs of acute stroke patients.
AS15-014
IMAGING
Poster
FDG-PET IMAGING OF PLAQUE INFLAMMATION IN RECENTLY SYMPTOMATIC CAROTID STENOSIS HELPS IN RISK STRATIFICATION AND PROGNOSTICATION
V. Sharma1, P. Paliwal1, H.L. Teoh1, B. Chan1, C. Hong1, Y. Chee1, J. Chen1, E. Ting1, H. Zhengdao1, L. Wong1, P. Seow1, B. Chandra1 and A. Sinha1
1National University of Singapore, Neurology, Singapore, Singapore
Abstract
Background: Symptomatic carotid stenosis is associated with an increased risk of stroke recurrence. Currently, therapeutic decisions are largely based on the luminal narrowing, which explains regional hypoperfusion as the underlying mechanism. Plaque inflammation, the initiating event for plaque rupture and thromboembolism (artery-to-artery embolism), is not evaluated routinely in carotid stenosis. Using combined 18F-fluorodeoxyglucose positron-emission tomography (FDG-PET)/computed tomography (CT), we investigated the role of plaque inflammation and stroke recurrence in our cohort of stroke patients with recently symptomatic carotid stenosis.
Methods: This ongoing prospective study aims to include consecutive patients within 30-days of recent stroke and ipsilateral carotid stenosis (≥50%). FDG uptake is quantified as mean standardized uptake values (SUV, g/ml). Patients are followed for stroke recurrence. Embolic potential of the carotid plaque is estimated by presence of spontaneous microembolic signals (MES) on continuous transcranial Doppler monitoring of middle cerebral arteries (MCA) for 40-minutes.
Results: Of the 28 patients included in the study, 6 suffered from recurrent cerebral ischemic event in the same vascular territory within 90-days. In patients with recurrent cerebral ischemia, the mean SUV value in the carotid plaque on the side of symptomatic carotid stenosis was higher (3.46 g/ml) as compared to the patients without stroke recurrence (1.72 g/ml; p = 0.03). MES were noted in 4/6 cases with recurrent cerebral ischemia as compared to 2/22 asymptomatic cases (p = 0.001).
Conclusions: FDG-PET/CT aids in imaging plaque inflammation in carotid stenosis and identifying high-risk patients. We intend to develop a robust prediction model for risk stratification based on luminal stenosis and plaque characteristics for appropriate therapeutic decision-making.
AS20-015
INTRACEREBRAL HAEMORRHAGE
Oral
RISK FACTORS FOR SEIZURES AFTER INTRACEREBRAL HEMORRHAGE IN THE ETHNIC/RACIAL VARIATIONS IN INTRACEREBRAL HEMORRHAGE (ERICH) POPULATION
S.Y. Kwon1, A. Obeidat1, P. Sekar1, C.J. Moomaw1, S. Koch2 and D. Woo1
1University of Cincinnati, Neurology, Cincinnati, USA
2University of Miami, Neurology, Miami, USA
Abstract
Background: We aim to identify the risk factors for seizure after intracerebral hemorrhage (ICH) using a multi-ethnic cohort. Furthermore, we set out to validate the prognostic value of the previously reported CAVE score (cortical involvement, age <65, volume >10 mL, and early seizures within 7 days of ICH).
Methods: The ERICH study enrolled 2,505 ICH patients from 2010 to 2015 without a prior history of seizure who survived to discharge. CAVE score (early seizure defined as seizure during hospitalization instead of within 7 days) was calculated for each. Backward elimination (p ≤ 0.05) in a multiple logistic regression model was computed using all variables significant (p < 0.10) in a univariate analysis to identify those risk factors with independent effects in predicting seizure after ICH.
Results: Mean age of ICH cases was 61.3 ± 14.3 years and 41% were female. Seizures developed in 74 patients (2.95%) after discharge within 12 months. Patients with cortical location of ICH, younger age, larger hematoma volume, and surgical evacuation of hematoma had a higher risk of seizure (see Table 1). The CAVE score was highly associated with seizure development (OR 2.5 per unit score increase, 95% CI 2.0–3.0, P < 0.0001). A modified CAVE score including surgical evacuation (CAVES) had a greater predictive value (AUC 0.77 vs 0.73).
Conclusions: We validated the CAVE score in a multi-ethnic population to predict the risk of post-ICH seizure. We also found that including surgical evacuation in the CAVE score improves its predictive ability. No differences by race/ethnicity were observed.
AS20-019
INTRACEREBRAL HAEMORRHAGE
Oral
INTRA-HEMATOMA DIFFUSION CHANGES IN INTRACEREBRAL HEMORRHAGE PATIENTS
R. McCourt1, K. Butcher1, C. Beaulieu2 and L. Sivakumar1
1University of Alberta, Dept of Neurology, Edmonton, Canada
2University of Alberta, Dept of Biomedical Engineering, Edmonton, Canada
Abstract
Background: Changes in hematoma and perihematoma region over time are not well understood in intracerebral hemorrhage (ICH). Fractional Anisotropy (FA) and Average Diffusion Coefficient (ADC) as measured by Diffusion Tensor Imaging (DTI), provide a measure of tissue, and potentially clot, organization. Higher FA values, and lower ADC values, indicate more uniform orientation of surrounding microstructure in hemorrhage.
Methods: Patients with spontanous ICH were serially imaged. Hematoma volume was measured on CT. FA and ADC maps were calculated from DTI source images. Hematoma regions of interest and contralateral homologous regions were drawn on T2-weighted images.
Results: Fourty-six ICH patients (mean age 69 ± 12) were imaged at medians of 1.8(1.1), 8(2.9) and 32(5.1) days. Median hematoma volume was 8.9(23.4)ml, measured at 2.1(3.9)h. Lesion location was: 63%(29) basal ganglia, 33%(15) lobar, and 4%(2) brainstem. Hematoma signal to noise ratio (10.3) was adequate for calculation of FA and ADC.
Hematoma ADC was decreased (0.71 ± 0.02 × 10−3 mm2 /s) compared to ADC in the contralateral region (1.0 ± 0.1 × 10−3 mm2/s; p = 0.032). ADC was 0.69 ± 0.13 × 10−3 mm2/s within 3 days, 0.76 ± 0.15 × 10−3 mm2/s at day 7, and 0.75 ± 0.19 × 10−3 mm2/s at day 30. The change in ADC over time was not significant (p = 0.207).
Mean hematoma FA (0.23 ± 0.05) was lower than contralateral regions (0.31 ± 0.06, p < 0.001). Hematoma FA decreased from 0.26 ± 0.05 (within 3 days) to 0.22 ± 0.04 (day 7) and 0.21 ± 0.19 (day 30; p = 0.001).
Conclusions: It is possible to measure diffusion changes in the hematoma, which reflect the clotting process within injured grey and white matter. Although variable, FA decreases over time with progression of the gliotic process.
AS20-029
INTRACEREBRAL HAEMORRHAGE
Oral
INTRACEREBRAL HEMORRHAGE RELATED TO NON-VKA ORAL ANTICOAGULANTS
J. Purrucker1, K. Haas2, T. Rizos1, S. Khan1, M. Wolf3, S. Poli4, C. Kleinschnitz5, T. Steiner6, P. Heuschmann7 and R. Veltkamp8
7University of Würzburg, Institute of Clinical Epidemiology and Biometry- Comprehensive Heart Failure Center- Clinical Trial Center Würzburg, Würzburg, Germany
8Imperial College London- London, Department of Stroke Medicine, London, United Kingdom
Abstract
Background: In contrast to intracerebral haemorrhage (ICH) associated with vitamin K antagonists (VKA), prospective data about the early clinical course, the acute management, and the outcome of ICH related to non-VKA oral anticoagulants (NOAC-ICH) are lacking.
Methods: This prospective multicentre observational study at 38 stroke units across Germany included consecutive patients with NOAC-ICH admitted from February 2012 to December 2014. All diagnostic and treatment decisions including administration of haemostatic factors (e.g. prothrombin complex concentrate, PCC) were left to the discretion of the treating physicians. We analysed baseline characteristics, early clinical course and management. Functional outcome was determined 90 days after the index event. Haematoma expansion analysis was done in patients with available follow-up brain imaging within 3 to 72 hours after first scan. Substantial haematoma expansion was defined as either relative (≥ 33%) or absolute (≥ 6 ml) volume increase. This study is registered at ClinicalTrials.gov (NCT01850797).
Results: Sixty-one ICH patients were enrolled; 41% were female; mean age was 76.1 years (SD 11.6). On admission, median NIHSS was 10 (IQR 4–18). Mean baseline haematoma volume was 23.7 ml (SD 31.3). In patients with sequential imaging for haematoma expansion analysis (n = 45, 73.8%), substantial haematoma expansion occurred in 38%. Overall mortality was 28% at 3-months, and 65% of survivors had an unfavourable outcome (mRS 3–5). 57% of the patients received PCC with no statistically significant effect on haematoma expansion or outcome.
Conclusions: NOAC-ICH is associated with frequent haematoma enlargement, and high-mortality and unfavourable outcome - as previously reported for VKA.
AS20-030
INTRACEREBRAL HAEMORRHAGE
Oral
INTRACRANIAL HAEMORRHAGE CLINICAL OUTCOMES MAY BE IMPROVED BY EARLY ACCESS TO CRITICAL CARE: OBSERVATIONAL STUDY FROM A UK HYPER-ACUTE STROKE SERVICE
G. Quattrocchi1, D. Austin1, J. Eng2, D. Werring2 and R. Simister2
1University College London, Sobell Department of Movement Disorders and Motor Neuroscience, London, United Kingdom
2University College London Hospital, Hyperacute Stroke Unit, London, United Kingdom
Abstract
Background: Thirty day mortality for intracerebral haemorrhage (ICH) typically approaches 50%. Higher level critical care (HDU/ITU) might improve outcome, and is recommended in international (e.g. AHA/ASA) guidelines. In a UK hyperacute stroke unit (HASU) we implemented a pathway of early transfer to critical care for ICH patients at risk of deterioration for monitoring and management including intensive blood pressure control and access to neurosurgery.
Methods: We analyzed outcomes for all patients between July 2014 and June 2015 using Sentinel Stroke National Audit Program data and six months telephone follow-up collected by a trained researcher.
Results: 1073 patients (age 73.4 + 14.6 years [mean + SD]; 520 [48%] men) were analyzed, of whom 95 (8.9 %) had ICH (age 71.7 + 15.7 years [mean + SD]; 52 [54.7%] men). Mean NIHSS was 6.3 (range 0–36), with 9 (9.5%) patients unresponsive at arrival. The most common mechanisms were hypertensive arteriopathy (35.8%) and amyloid angiopathy (9.5%); cause was documented as undertermined in (41.1%). Thirty-three (34.7%) patients were transferred to ITU/HDU and 6 (6.3%) underwent surgery. The proportion of patients with good outcome (mRS 0–2) in the ITU/HDU and HASU-only groups was 1 (3%) versus 13 (21%) at discharge, and 6 (18.8%) versus 18 (29.5%) at 6 months. Mortality (mRS 6) in the HDU and HASU groups was respectively 5 (15.5%) and 3 (4.9%) at discharge, and 9 (27.7%) and 13 (21.3%) at 6 months.
Conclusions: Mortality and good functional outcome after ICH in our cohort was much lower than expected, which may be explained by early HDU/ITU transfer.
AS20-043
INTRACEREBRAL HAEMORRHAGE
Oral
RISK OF RECURRENT ICH, OTHER VASCULAR EVENTS AND DEATH IN SURVIVIORS OF INTRACEREBRAL HAEMORRHAGE
K.M. van Nieuwenhuizen1, I. Vaartjes2, G.J.E. Rinkel1, L.J. Kappelle1, C.J.M. Klijn1,3
1University Medical Center Utrecht, Department of Neurology and Neurosurgery- Brain Center Rudolf Magnus, Utrecht, Netherlands
2University Medical Center Utrecht, Julius Center for Health Sciences and Primary Care, Utrecht, Netherlands
3Radboud University Medical Center, Department of Neurology- Donders Institute of Brain- Cognition and Behaviour- Center for Neuroscience, Nijmegen, Netherlands
Abstract
Background: Objective: To determine in intracerebral haemorrhage (ICH) survivors, risks of recurrent ICH (rICH), other vascular events, and death, according to age and sex.
Methods: In a hospital-admissions and population-registries linkage study in the Netherlands, we assessed in survivors of ICH between 1998- 2010, cumulative risks of rICH, ischaemic stroke, a composite vascular outcome, and death, according to age and sex, after 1, 2, 5 and 10 years. We compared long-term mortality to the general population.
Results: In 19,444 ICH survivors (52% male, median age 72, IQR 61–79; 78,654 follow-up years), one-year risk of rICH ranged from 1.5% (1.0–2.3; 35–54 years) to 2.4% (2.0–2.9; women 75–94), ten-years risk from 3.7% (2.6–5.1; men 35–54) to 8.1% (6.9–9.4; women 55–74). One-year rICH risk in patients 35–54 years tripled that of ischaemic stroke, and was similar for rICH and ischaemic stroke in older age-groups. Risks of rICH were similar for both sexes at all ages. Ten-year risk of the composite vascular outcome was ∼40% and higher in men (HR:1.23;1.16–1.30). Mortality was higher for ICH survivors than for the general population, ∼15% in those 35–54 and ∼70% in the eldest.
Conclusions: In ICH survivors 35–54 years, risk of rICH is higher than of ischaemic stroke; thereafter risks are similar. Risk of rICH is comparable in men and women in all age-groups. ICH survivors have a high risk of future vascular events and increased risk of death in all age-groups. To improve long-term prognosis tailored, long-term secondary prevention strategies are urgently needed.
AS20-045
INTRACEREBRAL HAEMORRHAGE
Oral
CLINICAL AND RADIOLOGICAL OUTCOME AFTER DIRECT ORAL ANTICOAGULANT INTRACEREBRAL HAEMORRHAGE (DOAC-ICH) COMPARED TO VITAMIN K ANTAGONIST INTRACEREBRAL HAEMORRHAGE (VKA-ICH)
D. Wilson1, D.J. Seiffge2, C. Traenka2, G. Basir3, J.C. Purrucker4, T. Rizos4, R. Al-Shahi Salman5, H.R. Jager6, G. Ambler7, Y. Yakushiji8, P.M.C. Choi9, J. Staals10, C. Cordonnier11, J.S. Jeng12, R. Veltkamp13, D. Dowlatshahi14, S. Engelter15, A.R. Parry-Jones16, A. Meretoja17 and D.J. Werring1
1Institute of Neurology, Brain repair and rehabilitation, London, United Kingdom
2University Hospital Basel- University of Basel, Stroke center and Neurology, Basel, Switzerland
3Ottawa Hospital Research Institute and University of Ottawa, Neurology, Ottawa, Canada
4Heidelberg University Hospital, Department of Neurology, Heidelberg, Germany
5University of Edinburgh, Division of Clinical Neurosciences- Centre for Clinical Brain Sciences- School of Clinical Sciences-, Edinburgh, United Kingdom
6Institute of Neurology, Lysholm Department of Neuroradiology, London, United Kingdom
7Univeristy College London, Dpeartment of statistical science, London, United Kingdom
8Department of Internal Medicine- Saga University Faculty of Medicine, Division of Neurology-, Saga, Japan
9Eastern Health, Department of Neurosciences, Melbourne, Australia
10Maastricht University Medical Centre, Department of Neurology, Maastricht, Netherlands
11University Lille, Degenerative & vascular cognitive disorders, Lille, France
12National Taiwan university Hospital, Stroke Center and Department of Neurology, Taipei, Taiwan
13Imperial College London, Department of Stroke Medicine- Division of Brain Sciences-, London, United Kingdom
14University of Ottawa, Ottawa Hospital Research Institute and University of Ottawa, Ottawa, Canada
15University Hospital Basel, Stroke center and Neurology, Basal, Switzerland
16Salford Royal NHS Foundation Trust, Manchester Academic Health Sciences Centre, Manchester, United Kingdom
17Helsinki University Hospital, Department of Neurology, Helsinki, Finland
Abstract
Background: Without widespread access to antidotes, DOAC-associated intracerebral haemorrhage (DOAC-ICH) might have a poorer clinical outcome, and higher rate of haematoma expansion (HE) than vitamin K antagonist associated ICH (VKA-ICH). In a 13 centre international collaborative multicentre pooled analysis, we compared mortality, functional outcome, ICH volume and HE between DOAC-ICH and VKA-ICH.
Methods: The primary outcome (all-cause mortality within 90 days) for DOAC-ICH and VKA-ICH was compared using a Cox proportional-hazards model, adjusted for: age; gender; baseline GCS, ICH location and log volume; IVH volume; and intracranial surgery. Heterogeneity was addressed using a shared frailty term. Good functional outcome was defined as discharge mRS ≤2 and investigated in multivariable logistic regression. ICH volume was measured by ABC/2 or a semi-automated planimetric method. HE was defined as an ICH volume increase >33% or 6 mL from baseline within 72 hrs.
Results: We included 500 patients (97 DOAC-ICH and 403 VKA-ICH). After adjusting for censoring, all-cause mortality was 31% (adjusted HR for DOAC compared to VKA-ICH 0.93, 95% CI 0.52 to 1.64; p = 0.79). Median baseline ICH volume was 14.4 mL (IQR 3.6 to 38.4) for DOAC-ICH vs 10.6 mL (IQR 4.0 to 27.9) for VKA-ICH, p = 0.78. There were no between-group differences in functional outcome (OR 1.76, 95% CI 0.68 to 4.53; p = 0.24) or the rate of HE (DOAC-ICH 40% (n = 48) vs VKA-ICH 34% (n = 140); p = 0.45).
Conclusions: Mortality, functional outcome, ICH volume, and HE are similar for DOAC-ICH and VKA-ICH, despite the lack of widely-available antidotes for DOAC-ICH.
ESOC6-1431
INTRACEREBRAL HAEMORRHAGE
Poster
EFFECTIVENESS OF DONEPEZIL 5MG IN PATIENTS WITH ANEURYSMAL SUBARACHNOID HEMORRHAGE: A RANDOMIZED, DOUBLE-BLIND, CLINICAL TRIAL
S.D. Yoo1, J. Bark1, L. Jang Bok1, J.S. Koh2 and G.K. Kim2
1Kyung Hee University, Rehabilitation Medicine, Seoul, Republic of Korea
2Kyung Hee University, Neurosurgery, Seoul, Republic of Korea
Abstract
Background: Patients with a ruptured and surgically repaired aneurysm often suffer from long-lasting cognitive deficits, which are associated with functional disability and poor quality of life. The purpose of this study was to evaluate the effects of donepezil in patients with aneurysmal, subarachnoid hemorrhage (SAH).
Methods: A randomized, double-blind, 4-week study was conducted. A total of 243 patients were transferred to rehabilitation department after becoming neurologically stable after aneurysmal SAH. Twenty four patients out of the 243 had spontaneous SAH from the rupture of the solitary aneurysm which was totally excluded by surgically neck clipping, and no major postoperative complication. They were randomized 1:1 to receive donepezil 5 mg/d or control, and memory functions were assessed using mini-mental state examination and computerized neuropsychological test before and after donepezil intake.
Results: There were no differences in age, education, Hunt and Hess grade, Fisher grade, mean initial test time after SAH, and sites of ruptured intracranial aneurysms, between the donepezil group compared to the control group. Compared with the control group, the donepezil group showed a significant improvement in forward digit span (P = 0.03), second, third, fourth trial, recognition in verbal learning test (P < 0.05), and backward visual span (P = 0.02), and first, second, third, fourth trial of the visual learning test (P < 0.05).
Conclusions: Treatment options to improve cognitive impairments after the occurrence of an aneurysm rupture are strongly needed. Patients treated with 5 mg/d donepezil showed significant improvement in cognitive function. Donepezil may improve memory functions in patients suffering from cognitive deficits caused by aneurysmal SAH.
AS17-096
INTRACEREBRAL HAEMORRHAGE
Oral
PROGNOSTIC SIGNIFICANCE OF RENAL FUNCTION IN ACUTE INTRACEREBRAL HAEMORRHAGE
D. Zheng1, S. Sato1, H. Arima2, E. Heeley1, C. Delcourt1, Y. Cao3, J. Chalmers4 and C. Anderson1
1The George Institute for Global Health, Neurology and mental health, Sydney, Australia
2Shiga University of Medical Sciences, Center for Epidemiologic Research in Asia, Otsu, Japan
3The Second Affiliated Hospital of Suzhou University, Neurology department, Suzhou, China
4The George Institute for Global Health, Cardiovascular division, Sydney, Australia
Abstract
Background: Past studies on the effect of renal function on intracerebral hemorrhage (ICH) outcomes have yielded inconsistent findings. We aimed to determine the association between estimated glomerular filtration rate (eGFR) on admission and patient outcomes of the second Intensive Blood Pressure Reduction in Acute Cerebral Haemorrhage Trial (INTERACT2).
Methods: INTERACT2 was an international, randomised controlled trial of patients with spontaneous ICH and elevated systolic BP assigned to intensive (target SBP <140 mmHg) or contemporaneous guideline recommended (SBP < 180 mmHg) BP treatment. We categorised over 2600 participants into 3 groups of eGFR based on the Chronic Kidney Disease Epidemiology Collaboration equation: normal or high (>90 mL/min/1.73m2), mild (60–90 mL/min/1.73m2) and moderate-severe (<60 mL/min/1.73m2) decrease. The effect of admission eGFR on the primary outcome of death or major disability at 90 days (defined by scores of 3 to 6 on the modified Rankin Scale) was analysed using multivariable logistic regression model. The potential effect modification of intensive BP lowering treatment by admission eGFR status was also assessed using interaction terms.
Results: Compared to normal or high eGFR, patients with moderate-severe decrease in eGFR had the greatest risk of death or major disability at 90 days (adjusted odds ratio 1.82, 95% CI 1.28–2.61). The effects of early intensive BP lowering were consistent across different levels of eGFR (P = 0.5 for homogeneity).
Conclusions: Decreased eGFR is an independent predictor of poor outcome in acute ICH. Early intensive BP lowering can provide similar treatment effects in ICH patients with decreased eGFR.
AS26-021
LANGUAGE AND COGNITION
Oral
MRI-VISIBLE PERIVASCULAR SPACE LOCATION DISTINGUISHES ALZHEIMER'S DISEASE FROM SUBCORTICAL VASCULAR COGNITIVE IMPAIRMENT INDEPENDENTLY OF AMYLOID BURDEN
G. Banerjee1, H.J. Kim2, Z. Fox3, H.R. Jäger4, A. Charidimou1, D. Wilson1, H.K. Na2, D.L. Na2, S.W. Seo2 and D. Werring1
1UCL Institute of Neurology, UCL Stroke Research Centre, London, United Kingdom
2Samsung Medical Center- Sungkyunkwan University School of Medicine, Department of Neurology, Seoul, Republic of Korea
3UCL, Biomedical Research Centre, London, United Kingdom
4UCL Institute of Neurology, Neuroradiological Academic Unit- Department of Brain Repair and Rehabilitation, London, United Kingdom
Abstract
Background: MRI-visible perivascular spaces (PVS) are a neuroimaging marker of cerebral small vessel disease. Their location may relate to the type of underlying small vessel pathology: those in the centrum semi-ovale (CSO-PVS) are associated with cerebral amyloid angiopathy, whilst those in the basal ganglia (BG-PVS) are associated with deep perforating artery arteriolosclerosis. We hypothesized that CSO-PVS and BG-PVS would be associated with brain amyloid burden and the clinical diagnosis of cognitive impairment, either Alzheimer’s disease (AD) or subcortical vascular cognitive impairment (SVCI).
Methods: 226 patients (AD n = 110; SVCI n=116) with standardised MRI and PiB-PET imaging were included. PVS were rated using a validated 4-point visual rating scale, and categorised by severity (“none/mild”, “moderate” or “frequent/severe”). Univariable and multivariable regression analyses were then performed.
Results: In adjusted analyses, the severity of CSO-PVS was independently associated with AD (none/mild as reference group: moderate severity, Odds Ratio (OR) 5.40, 95% Confidence Interval (CI) 2.08 to 8.29; frequent/severe, OR 7.69, 95% CI 4.29 to 20.71; p = 0.0003), whereas the severity of BG-PVS negatively predicted AD (none/mild as reference group: moderate severity, OR 0.14, 95% CI 0.04 to 0.26; frequent/severe, OR 0.05, 95% CI 0.01 to 0.47; p = 0.0004). PVS location did not predict amyloid-PET positivity.
Conclusions: These findings support the use of PVS location and amyloid-PET to differentiate between AD and SVCI. This study provides evidence that, in cognitively impaired patients, CSO-PVS are associated with processes that are either not visualised by PiB-PET imaging, or that are amyloid independent.
AS11-001
LANGUAGE AND COGNITION
Oral
SPEECH AND LANGUAGE THERAPY (SLT) FOR APHASIA AFTER STROKE: COCHRANE SYSTEMATIC REVIEW EVIDENCE OF THERAPY REGIMENS, DELIVERY MODELS AND THEORETICAL APPROACHES
M. Brady1, P. Enderby2, H. Kelly3, J. Godwin4 and P. Campbell5
1Glasgow Caledonian University, Nursing- Midwifery and Allied Health Professions Research Unit, Glasgow, United Kingdom
2University of Sheffield, School of Health and Related Research, Sheffield, United Kingdom
3University College Cork, Speech and Hearing Sciences, Cork, Ireland
4Glasgow Caledonian University, Institute for Applied Health, Glasgow, United Kingdom
5Glasgow Caledonian University, NMAHP Research Unit, Glasgow, United Kingdom
Abstract
Background: Aphasia, language impairment affecting expression and understanding of speech, reading and writing impacts a third of stroke survivors. Results from previous reviews of SLT for aphasia were based on limited data. Our 2016 review update sought to synthesise current trial evidence comparing different SLT approaches.
Methods: Systematically searching 12 electronic databases (from inception-September 2015; Cochrane Stroke Group Trials Register, COCHRANE databases, MEDLINE, CINAHL, AMED, EMBASE, LLBA) identified published, unpublished and ongoing randomised controlled trials (RCTs). SLT regimens (intensity, dose, duration) delivery models (e.g. computer-mediated, volunteer) and theoretical approaches (e.g. melodic intonation therapy, constraint induced language therapy (CILT)) were compared to usual SLT. Two reviewers independently assessed quality and extracted data on functional, receptive and expressive language, severity of impairment, psychosocial impact, drop-outs, compliance and economic outcomes. We sought missing data from trialists.
Results: From 11,314 records, we extracted data from 118 papers reporting 37 randomised comparisons (n = 1191) of SLT approaches. Eight compared high with low-intensity therapy. High-intensity SLT (4–15 hours weekly) improved measures of severity (P = 0.02; SMD 0.38, 95%CI 0.07–0.69) but more dropouts from high-intensity groups confounded these results (P = 0.02; OR 1.96, 95%CI 1.10–3.51). Some benefit of high-dose SLT (60–208 hours) was observed. Little evidence of differences between group and one-to-one SLT, computer-facilitated or volunteer-facilitated SLT (under therapist guidance) versus professional SLT were noted. Small numbers of RCTs of popular theoretical approaches (e.g. functional or CILT) did demonstrate evidence of effectiveness over conventional SLT approaches.
Conclusions: Specific SLT approaches may be beneficial but possibly not for all with aphasia.
AS17-021
LANGUAGE AND COGNITION
Oral
RISK PREDICTION OF LONG-TERM COGNITIVE IMPAIRMENT AFTER STROKE
M. Fahey1, G. Emanuel1, A.G. Rudd1,2, C.D.A. Wolfe1,2, A. Douiri1,2
1King’s College London, Division of Health and Social Care Research, London, United Kingdom
2National Institute for Health Research Biomedical Research Centre, Guy’s and St. Thomas’ NHS Foundation Trust, London, United Kingdom
Abstract
Background: Cognitive impairment is a significant outcome of stroke, increasing risk of mortality, disability and depression, impeding recovery and lowering quality of life. We aim to develop and validate a predictive model for monitoring the risk of cognitive impairment after stroke and assess its clinical utility.
Methods: 2,869 patients with first ever stroke from South London Stroke Register between 1995–2004 were included in the development cohort. Cognitive impairment was measured using the Mini Mental State Examination (cut off 24/30) and the Abbreviated Mental test (cut off 8/10) at 3-months and yearly up to 18 years. 2,172 patients from 2005–2014 were included in the validation cohort. Overall predictive trajectories, Receiver operating characteristic and decision curves for 5-years risks were analysed.
Results: Age, stroke type, incontinence, left-hemisphere stroke, diabetes, and atrial fibrillation were identified as strong predictors of cognitive impairment. The overall predictive model showed good precision and accuracy with an R2 of 60% and RMSE of 0.13. Acceptable prognostic accuracy of 5-years risk of cognitive impairment was also observed (AUC: 70%, 95% CI [58–81]). The 5-years accuracy to predict mild cases (MMSE > =27, AMT > =9) was decreased (60% [52–68]); but slightly increased (72% [40–100]) for predicting severe cases (MMSE < 15, AMT < 5). Risk-decision curve analysis to quantify the clinical usefulness showed a large net benefit in the patients classified as being at low-risk of cognitive impairment.
Conclusions: Age, incontinence, left-hemisphere stroke, diabetes, and atrial fibrillation are associated with increased risk of cognitive impairment.The derived prognostic model uses these predictors to accurately predict risk of post-stroke cognitive impairment.
AS26-017
LANGUAGE AND COGNITION
Oral
SMALL VESSEL DISEASE IS ASSOCIATED WITH DELAYED-ONSET DEMENTIA AFTER STROKE/TRANSIENT ISCHEMIC ATTACK: THE STROKE REGISTRY INVESTIGATING COGNITIVE DECLINE (STRIDE) STUDY
V.C.T. Mok1, B.Y.K. Lam1, Z. Wang1, W. Liu1, L.W.C. Au1, W.C.W. Chu2, E.Y.L. Leung3, S. Chen3, A. Chan1, A.Y.L. Lau1, L. Shi2, F. Fan1, S.H. Ma1, V. Ip1, Y.O.Y. Soo1, T.W.H. Leung1, C.L. Ho3, L. Wong1 and A. Wong1
1The Chinese University of Hong Kong, Department of Medicine and Therapeutics, Hong Kong, Hong Kong- China
2The Chinese University of Hong Kong, Department of Imaging and Interventional Radiology, Hong Kong, Hong Kong- China
3Hong Kong Sanatorium and Hospital, Department of Nuclear Medicine, Hong Kong, Hong Kong- China
Abstract
Background: We hypothesised that concurrent cerebral small vessel disease (SVD) and/or Alzheimer’s disease (AD) pathologies predicted delayed-onset dementia after stroke/transient ischemic attack (TIA).
Methods: This 3-year prospective study investigated the prevalence of delayed-onset dementia in patients (n = 919), excluding those who developed dementia 3–6 months after stroke/TIA. Relations between baseline clinical, genetic, imaging measures and recurrent stroke with delayed-onset dementia were tested using binary logistic regression, with adjustment to age, gender and education. In addition, Pittsburg compound B (PiB) positron emission tomography was performed on 31 patients with (n = 10) and without delayed-onset dementia (n = 21).
Results: After 3 years, 40 subjects (4.4%) developed dementia. Presence of ≥ 3 lacunes (OR = 2.6, 95% CI = 1.4–5.0) and severe white matter changes (age-related white matter changes rating of 3/3) (OR = 2.6, 95% CI = 1.3–5.1) independently predicted delayed-onset dementia. Frequency of delayed-onset dementia in subjects with severe SVD (with ≥ 3 lacunes and severe white matter changes) was 12/89 (13.5%) versus 28/830 (3.4%) in those without severe SVD (x2(1) = 19.7, p < 0.0001). Further, severe SVD was shown to be a strong predictor of delayed-onset dementia (OR = 3.5, 95% CI = 1.6–7.3) in logistic regression analysis. Stroke subtypes, recurrent stroke, medial temporal lobe atrophy, and apolipoprotein ɛ4 status were not associated with delayed-onset dementia. Frequency of AD-like PiB retention in delayed-onset dementia patients was low (n = 3/10) and not different from those without dementia (n = 3/21, p = 0.36).
Conclusions: Severe SVD predicts delayed-onset dementia after stroke/TIA. Clinical trial aiming to prevent delayed-onset dementia after stroke/TIA should target subjects with severe SVD.
AS11-014
LANGUAGE AND COGNITION
Oral
LOW ANKLE-BRACHIAL INDEX IS ASSOCIATED WITH POOR COGNITION IN ASYMPTOMATIC HYPERTENSIVE INDIVIDUALS
I. Riba Llena1, J. Jiménez-Baladó1, X. Mundet2, J.L. Fernández3, H. Ostos1, F. Pujadas4, B. Gutiérrez4, J. Montaner5 and P. Delgado1
1Vall Hebron Research Institute. Universitat Autònoma Barcelona, Neurovascular Research Laboratory, Barcelona, Spain
2IDIAP Jordi Gol. Universitat Autònoma Barcelona, Barcelona City Research Suppport Unit-University Reserach Institute, Barcelona, Spain
3Dr Manchon Imaging Center, Neuroradiology, Barcelona, Spain
4Vall Hebron University Hospital, Dementia Unit. Neurology Service, Barcelona, Spain
5Vall Hebron Research Institute. Vall Hebron University Hospital. Universitat Autònoma Barcelona, Neurovascular Research Laboratory. Stroke Unit. Neurology Service., Barcelona, Spain
Abstract
Background: While the association between cognitive function and peripheral vascular disease (PAD) has been reported, the specific mechanisms are not well understood. We aimed to assess whether the association of ankle-brachial index (ABI) is independent of the presence of subclinical brain damage.
Methods: Data came from a Mediterranean cohort of hypertensive individuals without previous stroke or dementia. Participants underwent bilateral ABI testing with a photoplethysmography device and MRI to assess silent brain infarcts, cerebral microbleeds and white matter hyperintensities (WMH, rated with Fazekas scale). Cognitive testing was carried out with the Dementia Rating Scale-2 (DRS-2) and a complete neuropsychological battery when cognitive screening was failed. Mild Cognitive Impairment (MCI) was diagnosed according to previous criteria. Raw cognitive scores were transformed to Z scores and linear and binary logistic regressions were used for analysis.
Results: 782 participants with mean age 62.81(±5.40), 50.7% female and 8 years of median education (IQR = 7,12). Median ABI was 1.09(1.00, 1.17).9.1% (n = 68) had MCI and the rest were cognitively normal. 9.7% had SBI, 6.5% had cerebral microbleeds and median WMH score was 1 (IQR = 0, 2). Lower overall DRS-2 score (β = −0.810, 95%CI = −0.318, −1.302, p-value = 0.001), lower attention (β = −0.853, 95%CI = −0.308, −1.398, p-value = 0.002) and lower executive function (β = −0.773, 95%CI = −0.257, −1.288, p-value = 0.003) scores were associated with lower ABI after adjusting for education, vascular risk factors and MRI markers. However, MCI was not independently associated with ABI.
Conclusions: Our results confirm a relationship between poor cognition and PAD. Remarkably, this association is independent from the presence of subclinical brain lesions.
AS11-018
LANGUAGE AND COGNITION
Oral
EFFECT OF SOCIAL NETWORKS ON COGNITION AFTER STROKE: THE SOUTH LONDON STROKE REGISTER (SLSR)
A. Sahir1, C. McKevitt1, A.G. Rudd1, C.D.A. Wolfe1 and Y. Wang1
1King's College London, Division of health and social care research, London, United Kingdom
Abstract
Background: We aim to assess the effect of social networks on risk of cognitive impairment in patients following stroke.
Methods: 1135 stroke patients from 1995 to 2014 in the South London Stroke Register (SLSR) were included in the study. Cognitive status was assessed by the Mini-Mental State Examination (MMSE) and Abbreviated Mental Test (AMT). Social networks were measured using the social networks questionnaire in SLSR which was further developed into scores for domains of social networks (emotional support, social engagement and instrumental support) and a total social networks score. Multivariate logistic regression models adjusted for socio-demographics, case-mix, acute stroke care and risk factors prior to stroke were used for analysis of the association between social networks and cognitive impairment at 3 months and 1 year after stroke.
Results: Higher levels of social engagement were significantly associated with reduced risk of cognitive impairment at 3 months after stroke (odds ratio (OR): 0.30 to 0.79). On 1 year follow-up, higher levels of social engagement and emotional support were shown significantly associated with reduced risk of cognitive impairment (OR: 0.14 to 0.56, and 0.25 to 0.27, respectively). Also, the total social network score at 1 year was significantly associated with reduced risk of cognitive impairment (OR: 0.87 (95% CI: 0.79–0.97)).
Conclusions: Social engagement is significantly associated with cognitive impairment at both 3 months and 1 year after stroke. Social engagement, emotional support and overall better social networks are associated with reduced risk of cognitive impairment at 1 year after stroke.
AS11-019
LANGUAGE AND COGNITION
Oral
REMOTE STRUCTURAL BRAIN CHANGES ARE ASSOCIATED WITH COGNITIVE DECLINE IN ELDERLY WITH SMALL VESSEL DISEASE
K. Wiegertjes1, E.M.C. van Leijsen1, M. Bergkamp1, I. van Uden1, A.M. Tuladhar1 and F.E. de Leeuw1
Background: Cerebral small vessel disease (SVD) is associated with cognitive decline, but does not explain the whole picture. We hypothesize that apart from SVD, brain atrophy contributes to cognitive decline in patients with SVD.
Methods: 278 Participants with SVD from the RUN DMC study with repeated MRI and neuropsychological assessment at three time points over a 9-year period. Whole-brain atrophy was estimated with SIENA. White matter hyperintensities, lacunar infarcts and microbleeds were assessed. Relations with cognitive performance were assessed with linear regression analysis adjusted for age, education, follow up duration and all SVD characteristics at baseline.
Results: Mean baseline age was 64.1 years (SD 8.4) and 59.2% were male. Mean total brain volume at baseline was 1085.6 ± 71.0 mL, with mean white matter hyperintensity volume of 5.8 ± 9.5 mL. Mean percentage total brain volume change (PBVC) was −4.6% ± 2.0 (annual PBVC of −0.5% ± 0.3). Independent of SVD, each percent of annual PBVC decrease was related to a decline in global cognitive functioning (β = −0.151, p = 0.027), fluency (β = −0.170, p = 0.009) and psychomotor speed (β = −0.147, p = 0.037).
Conclusions: On top of SVD, brain atrophy rate is associated with future cognitive decline. These results indicate that the clinical consequences of SVD are partly explained by changes in remote brain structures.
AS26-004
LANGUAGE AND COGNITION
Oral
PROGRESSION OF DIFFUSION TENSOR IMAGING PREDICTS COGNITIVE DECLINE AND DEMENTIA CONVERSION IN CEREBRAL SMALL VESSEL DISEASE: THE SCANS STUDY
E. Zeestraten1, P. Benjamin1,2, A. Lawrence3, C. Lambert1, A. Mackinnon4, R. Morris5, T. Barrick1 and H. Markus3
1St George's University of London, Cardiovascular and Cell Sciences Research Institute- Neurosciences Research Centre, London, United Kingdom
2Imperial College NHS Trust- Charing Cross Hospital Campus, Department of Radiology, London, United Kingdom
3University of Cambridge, Stroke Research Group- Clinical Neurosciences, Cambridge, United Kingdom
4St George's University Hospitals NHS Foundation Trust, Atkinson Morley Department of Neuroradiology, London, United Kingdom
5King's College Institute of Psychiatry- Psychology and Neuroscience, Department of Psychology, London, United Kingdom
Abstract
Background: Cerebral small vessel disease (SVD) is the major pathology underlying vascular dementia and lesser degrees of vascular cognitive decline (VCI). Cross-sectional studies have shown associations between cognitive impairment and SVD-related MRI markers, including white matter (WM) microstructure quantified using diffusion tensor imaging (DTI). However there is little data from prospective studies determining whether MRI markers predict cognitive decline and dementia.
Methods: 99 patients with lacunar stroke and radiological confluent leukoaraiosis were followed up with annual MRI for 3 years and annual cognitive assessments for 5 years. Progression to dementia was also recorded. The following MRI markers were assessed: lacunes, T2-white matter hyperintensities (WMH), brain volume, microbleeds, and on DTI normalised peak height of mean diffusivity histogram distribution as a marker of WM microstructural damage.
Results: Over the 5 years there was a decline in executive function and processing speed and 18 cases (18.2%) progressed to dementia. All MRI markers also declined. Both the presence of new lacunes (p = 0.007) and rate of increase in DTI WM microstructural damage (p = 0.021) predicted decline in executive function. Both WMH growth (p = 0.013) and deterioration of WM microstructure (p = 0.003) with IQ (p = 0.010) predicted progression to dementia. In a prediction model also including pre-morbid IQ, these 2 MRI parameters predicted dementia with a C-statistic of 0.85.
Conclusions: This longitudinal data demonstrates that change in MRI parameters, and especially DTI, predicts cognitive decline and conversion to dementia. It emphasises the importance of diffuse white matter damage in the pathogenesis of VCI in cerebral SVD.
AS11-020
LANGUAGE AND COGNITION
Oral
ASSOCIATION BETWEEN LESION LOCATION AND COGNITION EARLY AFTER STROKE: A VOXEL-BASED LESION-SYMPTOM MAPPING STUDY IN CHINESE POPULATION
L. Zhao1, J.M. Biesbroek2, L. Shi1, W. Liu1, A. Wong1, H.J. Kuijf3, G.J. Biessels2 and V.C.T. Mok1
1The Chinese University of Hong Kong, Department of Medicine and Therapeutics, NT, Hong Kong- China
2University Medical Center Utrecht, Department of Neurology- Utrecht Stroke Center- Brain Center Rudolf Magnus, Utrecht, Netherlands
3University Medical Center Utrecht, Image Sciences Institute, Utrecht, Netherlands
Abstract
Background: We assessed whether lesion location in key brain regions was associated with post-stroke cognition in Chinese population.
Methods: Voxel-based lesion-symptom mapping (VLSM) and region of interest-based (ROI) analyses were performed to 307 Chinese acute ischemic stroke patients to investigate the spatial relation between the presence of an acute ischemic lesion (AIL) and cognitive functions measured by MoCA at 3 months after stroke.
Results: VLSM identified several clusters of voxels with a significant association between AIL and total MoCA in the left basal ganglia, frontal, parietal and occipital cortex and white matter (WM). The ROI analyses based on linear regression models revealed significant correlations between total MoCA and regional AIL volume within the left basal ganglia, inferior frontal gyrus, angular, cingulate, corpus callosum, corona radiate, and thalamic radiation after adjustment for total AIL volume. Most key regions derived from total MoCA remained significant for memory, language and attention, but some regions were only related to a specific MoCA domain: left angular gyrus, splenium of corpus callosum, and left posterior thalamic radiation were associated with memory; left precentral gyrus, rolandic operculum, and both sides of corona radiata were associated with language; body of the corpus callosum was associated with attention. The left cerebellum AIL was distinctively associated with visuospatial function.
Conclusions: These findings identify lesions in the left basal ganglia, frontal and parieto-occipital WM as common substrates for deficits in memory, language and attention after stroke. However, some regions in the cortex, white matter tracts or cerebellum may have distinctive roles in specific MoCA domains.
ESOC6-1464
LATE BREAKING CLINICAL TRIALS
Oral
24/7 IN-AMBULANCE TELESTROKE: RESULTS FROM THE PRE-HOSPITAL STROKE STUDY AT THE UNIVERSITAIR ZIEKENHUIS BRUSSEL II (PreSSUB II)
R. Brouns1, R.J. Van Hooff1, A. De Smedt1, M. Moens2, A. Valenzuela Espinoza3, D. Lauwaert4, S. Neyrinck4, K. Nieboer5, J. De Mey5, H. Fernandez Tellez3, A. Convents3, R. Van de Casseye3, S. Steurbaut6, P. Cornu6, A. Dupont6, K. Putman7, I. Hubloue4 and J. De Keyser1
6Vrije Universiteit Brussel, Research group Clinical Pharmacology and Clinical Pharmacy, Brussels, Belgium
7Vrije Universiteit Brussel, Interuniversity Center for Health Economics Research, Brussels, Belgium
Abstract
Background: In-ambulance telemedicine is a promising and scalable approach to improve acute stroke care by speeding up key diagnostic processes and by curtailing the number of missed opportunities for specific stroke treatments.
Methods: The Prehospital Stroke Study at the Universitair ziekenhuis Brussel II (PreSSUB II) is an interventional randomized single-center clinical trial comparing standard emergency care with standard emergency care complemented with a 24/7 emergency in-ambulance teleconsultation service provided by stroke experts (ClinicalTrials.gov NCT02270541). The delay between the 112 emergency call and initiation of in-hospital brain imaging (Call-to-Imaging time) was the designated primary efficacy endpoint. Safety analysis included registration of adverse events and all-cause mortality. The proportion of successful in-ambulance teleconsultations was evaluated as a parameter for technical and organizational feasibility.
Results: 140 patients were enrolled between November 2014 and February 2016, of which 103 patients met the inclusion criteria. Brain imaging was performed in 87 patients (43 controls, 44 interventions), with an average reduction in the Call-to-Imaging time of 36.4 minutes (95% CI, 17.5–55.3) in the intervention group compared to controls (50.8 min; 95% CI, 46.3–55.3 vs. 87.1 min; 95% CI, 68.7–105.6; P < 0.001). No telemedicine-related adverse events occurred and mortality was similar in both groups. The proportion of successful in-ambulance telemedicine interventions was 96.2%.
Conclusions: Compared to standard emergency care, the implementation of 24/7 in-ambulance telestroke resulted in significantly decreased delays in key diagnostic processes without increased risk. Technical and organizational feasibility was established. Larger scale studies evaluating the effects on clinical outcomes are needed.
ESOC6-1426
LATE BREAKING CLINICAL TRIALS
Oral
TRIAL OF EARLY ANTICOAGULATION WITH RIVAROXABAN VERSUS WARFARIN IN PATIENTS WITH ATRIAL FIBRILLATION AND ACUTE CEREBRAL ISCHEMIA
K.S. Hong1, J.S. Lee2, Y.J. Kim3, Y.D. Kim4, H.G. Kang5, M.S. Park6, E.G. Kim7, B.W. Yoon8, D.W. Kang9, S.H. Lee9 and S.U. Kwon9
1Ilsan Paik Hospital - Inje University, Neurology, Goyang, Republic of Korea
2Asan Medical Center, Clinical Research Center-, Seoul, Republic of Korea
3Ewha Womans University School of Medicine, Neurology, Seoul, Republic of Korea
4Yonsei University College of Medicine, Neurology, Seoul, Republic of Korea
5Chosun University School of Medicine, Neurology, Gwangju, Republic of Korea
6Chonnam National University Medical School, Neurology, Gwangju, Republic of Korea
7Busan Paik Hospital Inje University, Neurology, Busan, Republic of Korea
8Seoul National University Hospital, Neurology, Seoul, Republic of Korea
9Asan Medical Center- University of Ulsan College of Medicine, Neurology, Seoul, Republic of Korea
Abstract
Background: Patients with atrial fibrillation (AF) and acute cerebral ischemia are at high risk of both recurrent ischemic stroke without anticoagulation and intracranial bleeding with anticoagulation, but the optimal anticoagulation strategy remains unclear.
Methods: This PROBE design trial randomized AF patients deemed eligible for early anticoagulation to either rivaroxaban (10 mg/day for 5 days followed by 15 or 20 mg/day) or dose-adjusted warfarin within 5 days after acute cerebral ischemia. The primary outcome was the composite of symptomatic and asymptomatic lesions of recurrent ischemia or intracranial bleeding seen on 4-week MRI. Secondary outcomes were individual components of composite outcome, clinical major vascular events, major bleeding, and post-randomization hospitalization length.
Results: Of 195 patients randomized, 183 (95 to rivaroxaban and 88 to warfarin) took at least one dose of study medication and completed follow-up MRI: mean age 70.4, median NIHSS score 2, and median CHA2DS2-VASc score 4. The rivaroxaban and warfarin groups did not differ in the primary endpoint (49.5% versus 54.5%, OR [95% CI] 0.82 [0.46–1.46], p = 0.493) and their components (new ischemic lesion: 29.5% versus 35.6%, 0.76 [0.41–1.41], p = 0.375; new hemorrhagic lesion: 31.6% versus 28.7%, 1.15 [0.61–2.16], p = 0.677). All hemorrhagic lesions were asymptomatic, but each group had one clinical ischemic stroke. However, rivaraxaban use was associated with shorter hospitalization (mean [SD], 4.6 ± 3.8 versus 6.5 ± 4.3, p < 0.0001).
Conclusions: In AF patients with acute cerebral ischemia deemed eligible for early anticoagulation, both rivaroxaban and warfarin were equally safe and effective. However, rivaroxaban use may reduce hospitalization due to achieving effective anticoagulation conveniently. (Triple AXEL ClinicalTrials.gov number, NCT02042534).
ESOC6-1462
LATE BREAKING CLINICAL TRIALS
Oral
LEFT ATRIAL APPENDAGE OCCLUSION VERSUS STANDARD MEDICAL CARE IN PATIENTS WITH ATRIAL FIBRILLATION AND INTRACEREBRAL HEMORRHAGE: A PROPENSITY SCORE MATCHED FOLLOW-UP STUDY
S.P. Johnsen1, J.E. Nielsen-Kudsk2, M. Rosenqvist3, P. Wester4, D. Damgaard5, J. Lund6, O. De Backer7, S. Pakarinen8, J. Odenstedt9, S. Vikman10, B. Sahlgren11, O. Kongstad12 and D. Krieger13
1Aarhus University Hospital, Department of Clinical Epidemiology, Aarhus, Denmark
2Aarhus University Hospital, Department of Cardiology, Aarhus, Denmark
3Karolinska Institute- Danderyd, Department of Cardiology, Stockholm, Sweden
4Umea University, Stroke Center, Umea, Sweden
5Aarhus University Hospital, Department of Neurology, Aarhus, Denmark
6Turku University Hospital, Department of Cardiology, Turku, Finland
7Rigshospitalet, Department of Cardiology, Copenhagen, Denmark
8Helsinki University Hospital, Department of Cardiology, Helsinki, Finland
9Sahlgrenska University Hospital, Department of Cardiology, Gothenburg, Sweden
10Tampere University Hospital, Heart Center, Tampere, Finland
11Karolinska Institute- Solna, Department of Cardiology, Stockholm, Sweden
12Skåne University Hospital, Department of Cardiology, Lund, Sweden
13University of Zurich, Department of Neurology, Zurich, Switzerland
Abstract
Background: There is no consensus on stroke prevention in patients with atrial fibrillation (AF) sustaining an intracerebral hemorrhage (ICH). These patients have an increased risk for both ischemic stroke and recurrent ICH. Cathether-based Left Atrial Appendage Occlusion (LAAO) represents an alternative treatment for these patients. We aimed to compare the prognosis in patients with AF and ICH having a LAAO versus patients receiving standard medical therapy.
Methods: 142 patients from the Nordic countries with AF and previous ICH who underwent LAAO (Amplatzer Cardiac Plug/Amplatzer Amulet) were compared to a propensity score matched group of 142 patients receiving standard medical therapy. The control patients were identified from the Danish National Stroke Register among 787 patients with AF and ICH. Patients with LAAO were followed from the implantation date and the patients in the standard care group were followed from day 180 after ICH. The primary endpoint was a composite of all-cause mortality, ischemic stroke and major bleeding.
Results: Patients with AF and a prior ICH treated by LAAO had a lower risk of the composite outcome compared with patients treated by standard care (event rate/1000 years: 50.1, 95% Confidence Interval (CI) 41.9–59.9 vs.190.8, 95% CI 156.8–232.2; Hazard Ratio 0.28, 95% CI 0.11–0.69). A lower risk was also observed for the individual outcomes, although only reaching statistical significance for all-cause mortality and major bleeding.
Conclusions: LAAO was suggested to be of potential clinical benefit in AF patients sustaining an ICH compared with standard medical therapy. These results have to be confirmed in a randomized clinical trial.
AS02-010
LATE BREAKING CLINICAL TRIALS
Oral
RESULTS FROM ACTION: A MULTICENTRE, DOUBLE-BLIND, PLACEBO-CONTROLLED, RANDOMISED PHASE 2 CLINICAL TRIAL OF NATALIZUMAB IN ACUTE ISCHAEMIC STROKE (AIS)
J. Elkins1, M. Elkind2, R. Veltkamp3, J. Montaner4, S.C. Johnston5, A. Singhal6, K. Becker7, M. Lansberg8, I. Chang9, W. Tang9, S. Gheuens10 and L. Mehta11
1Clinical Development, Biogen, Cambridge, USA
2Columbia University, Department of Neurology, New York, USA
3Imperial College London, Department of Medicine, London, United Kingdom
4Vall d’Hebron Research Institute, Neurology, Barcelona, Spain
5University of Texas, Dell Medical School, Austin, USA
6Massachusetts General Hospital, Department of Neurology, Boston, USA
7University of Washington, Department of Neurology, Seattle, USA
8Stanford University Medical, Department of Neurology and Neurological Sciences, Stanford, USA
9Biogen, Biostatistics, Cambridge, USA
10Biogen, Drug Safety and Risk Management, Cambridge, USA
11Biogen, Clinical Development, Cambridge, USA
Abstract
Background: Brain ischaemia triggers an inflammatory reaction that worsens outcomes in experimental stroke models. Here, we evaluate the efficacy/safety of a single dose of natalizumab, an antibody that reduces acute brain inflammation in multiple sclerosis, administered in AIS patients.
Methods: Patients were randomised 1:1 to receive 300-mg IV natalizumab (n = 79) or placebo (n = 82) 0–9 hours from when they were last known normal. The primary endpoint was relative change in infarct volume (baseline to day 5) assessed by MRI. Secondary and exploratory clinical endpoints were also assessed.
Results: The median baseline National Institutes of Health Stroke Scale (NIHSS) score was 12 and median time to natalizumab treatment was 6 hours. Natalizumab did not affect infarct volume growth compared with placebo (relative growth ratio: day 5, 1.09 [P = 0.779]; day 30, 1.06 [P = 0.684]). However, more patients on natalizumab than on placebo had an excellent outcome on the modified Rankin Scale (score ≤1 out of 0–6) at days 30 (odds ratio [OR] 2.88; 90% [prespecified] confidence interval [CI] 1.20–6.93) and 90 (OR 1.48; 90% CI 0.74–2.98). More patients on natalizumab than on placebo also had an excellent outcome on the Barthel Index (score ≥95 out of 100) at day 90 (OR 1.91; 90% CI 1.07–3.41). In addition, tertiary clinical endpoints supported improved outcomes with natalizumab. Incidences of adverse events were similar between treatment groups.
Conclusions: Although 300-mg IV natalizumab administered ≤9 hours after stroke onset did not reduce focal infarct volume growth, treatment was associated with functional outcome improvements sustained over 90 days.
ESOC6-1472
LATE BREAKING CLINICAL TRIALS
Oral
STENT-RETRIEVERS VS. MEDICAL THERAPY VS. INTRAVENOUS THROMBOLYSIS IN LARGE VESSEL OCCLUSION STROKES (SMILOS): A POOLED, PATIENT LEVEL COMPARISON STUDY BASED ON HISTORICAL CLINICAL TRIAL DATA
R.G. Nogueira1, R. Macisaac2, J. Saver3, P. Khatri4 and V.E. SMILOS Investigators
5
1Grady Memorial Hospital- Emory University School of Medicine, Neurology, Atlanta, USA
2Glasgow South Glasgow University Hospital, Neurology, Glasgow, United Kingdom
3University of California Los Angeles, Neurology, Los Angeles, USA
4University of Cincinnatti, Neurology, Cincinnatti, USA
5Glasgow University, Neurology, Glasgow, United Kingdom
Abstract
Background: Recent data demonstrated the superiority of thrombectomy versus medical treatment alone in large vessel occlusion strokes (LVOS). A few areas of knowledge gap remain including patients with MCA-M2 occlusion and those who are IV tPA ineligible.
Methods: Pooled comparison of historical data from LVOS prospective trials. Two comparative analyses were performed:
(1) Stent-retrievers + IV tPA (SWIFT, TREVO-2, STAR, and TREVO-EU) vs. IV tPA Alone (IMS-III, EPITHET, DEFUSE, MR Rescue, and SYNTHESIS Expansion);
(2) Stent-retrievers Alone (SWIFT, TREVO-2, STAR, and TREVO-EU) vs Medical Therapy Alone (PROACT-II, EPITHET, and MR Rescue). The primary and secondary endpoints were 90-day mRS shift and 90-day mRS 0–2.
Results: (1) IV tPA treated patient comparison: baseline characteristics were well-balanced in the endovascular (n = 235) and control (n = 145) groups. In agreement with the recent RCTs, there was a strong benefit of thrombectomy for both primary (90-day mRS shift: OR 2.4 95%CI [1.6–3.4], p = 0.001) and secondary (90-day mRS 0–2 54% vs 37.9%; OR 2.1 [1.4–3.3], p = 0.0005) endpoints.
(2) IV tPA ineligible patient comparison: baseline characteristics were well-balanced in the endovascular (n = 153) and control (n = 126) groups. Again, there was a strong benefit of thrombectomy for both primary (OR 2.3 [1.5–3.5], p = 0.021) and secondary (41.2% vs 25.9%; OR 2.4 [1.4–4.0], p = 0.0015) endpoints.
Sensitivity analysis demonstrated a persistent benefit for age ≥ 80 (n = 54, OR 2.3 [1.6–3.5]) and M2 occlusions (n = 85, OR 5.0 [2.1–11.8).
Conclusions: Our study reinforces the benefit of thrombectomy in LVOS patients and provides additional data on patients who are IV tPA ineligible, have M2 occlusions, or are 80 years or older.
ESOC6-1459
LATE BREAKING CLINICAL TRIALS
Oral
EFFECT OF PCC AND FFP ON HEMATOMA EXPANSION IN INTRACRANIAL HAEMORRHAGE RELATED TO VITAMIN-K-ANTAGONISTS AND INFLUENCE OF BLOOD PRESSURE, INCH - A RANDOMIZED CONTROLLED TRIAL
T. Steiner1, J. Hüsing2, S. Poli3, M. Griebe4, J. Hajda5, M. Bendszus6, J. Bösel7, H. Christensen8, C. Dohmen9, A. Freiberger5, J. Kollmer6, H. Stetefeld9, K. Wartenberg10, C. Weimar11, W. Hacke7 and R. Veltkamp12
1Klinikum Frankfurt Höchst and Heidelberg University Hospital, Department of Neurology, Frankfurt and Heidelberg, Germany
2Heidelberg University Hospital- Germany, Coordination center for clinical trials, Heidelberg, Germany
3Hertie Institute for Clinical Brain Research- Tuebingen University Hospital, Department of Neurology & Stroke, Tübingen, Germany
4Mannheim UMM- Heidelberg University, Department of Neurology, Mannheim, Germany
5Heidelberg University Hospital, Coordination center for clinical trials, Heidelberg, Germany
6Heidelberg University Hospital, Department of Neuroradiology, Heidelberg, Germany
7Heidelberg University Hospital, Department of Neurology, Heidelberg, Germany
8Bispebjerg and Frederiksberg Hospital- University of Copenhagen, Department of Neurology, Copenhagen, Germany
9Koeln University Hospital, Department of Neurology, Köln, Germany
10Halle University Hospital, Department of Neurology, Halle, Germany
11Essen University Hospital, Department of Neurology, Essen, Germany
12Imperial College London- United Kingdom and Department of Neurology- Heidelberg University Hospital, Department of Stroke Medicine, London and Heidelberg, Germany
Abstract
Background: Hematoma expansion (HE) predicts mortality in vitamin K antagonist related intracranial hemorrhage (VKA-ICH). We compared the effect of fresh frozen plasma (FFP) and prothrombin complex concentrate (PCC) on early coagulation, HE, and blood pressure
Methods: Prospective, randomized, controlled, open, blinded endpoint (PROBE) design. Adult VKA-ICH patients presenting within 12 hours with an INR ≥ 2.0 received FFP or PCC within 1 hour after initial CCT. Primary endpoint: proportion of patients with INR ≤ 1.2 within 3 hours. Secondary endpoints: HE
Results: The primary endpoint was reached by 2/23 and 18/27 (FFP and PCC respectively): adjusted OR 30·6, 95%-CI: [4·7; 197·9], p = 0·0003. Adjusted difference in HE was significantly smaller in the PCC-group: 16·9 ml (95%-CI: [2·5; 31·3], p = 0·026) at three hours and 16·4 ml (95%-CI: [2·9; 29·9], p = 0·018) at 24 hours. The effect of FFP on mean of systolic and diastolic blood pressure (MAP) at 3 h was 7.6 mmHg, 95%-CI: [-0,8; 16.0], p = 0.075). The influence of MAP on HE was (0.17 ml/mmHg, 95%-CI: [-0,14; 0,48], p = 0,27) and there was no profound change of treatment effect at three hours (15.2 ml, 95%-CI: [0,47; 29.8], p = 0,043) after adjustment for baseline blood pressure differences. Including three hours in lieu of baseline MAP produces similar results (0.28 ml/mmHg, 95%-CI: [-0.24; 0.81], p = 0.28; 15.7 ml, 95%-CI: [1.6; 29.8], p = 0.030)
Conclusions: PCC was significantly more effective in normalizing the INR compared to FFP and reduced the risk of HE. We did not find an association between HE and elevated blood pressure resulting from volume overload in the FFP-group.
ESOC6-1429
LATE BREAKING CLINICAL TRIALS
Oral
LONG TERM OUTCOME AFTER INTRA-ARTERIAL TREATMENT FOR ACUTE ISCHEMIC STROKE - TWO YEAR CLINICAL FOLLOW-UP OF THE MR CLEAN TRIAL
L.A. van den Berg1, M. Dijkgraaf2, O. Berkhemer3, P. Fransen4, D. Beumer5, H. Lingsma6, C. Majoie3, D. Dippel4, A. van der Lugt7, R. van Oostenbrugge5, W.H. van Zwam8 and Y. Roos9
1Academic Medical Center, Neurology, Amsterdam, Netherlands
2Academic Medical Center, Clinical Research Unit, Amsterdam, Netherlands
3Academic Medical Center, Radiology, Amsterdam, Netherlands
4Erasmus MC University Medical Center, Neurology, Rotterdam, Netherlands
5Cardiovascular Research Institute, Neurology, Maastricht, Netherlands
6Erasmus MC University Medical Center, Public Health, Rotterdam, Netherlands
7Erasmus MC University Medical Center, Radiology, Rotterdam, Netherlands
8Cardiovascular Research Institute, Radiology, Maastricht, Netherlands
9Academic Medical Center, Neurologie, Amsterdam, Netherlands
Abstract
Background: MR CLEAN was the first trial to demonstrate clinical efficacy of intra-arterial treatment (IAT) in patients with acute ischemic stroke caused by occlusion in the anterior circulation. In the subsequent months several other trials confirmed that IAT improves clinical outcome at 90 days. However, no data is available on long term clinical outcome and recurrent stroke. We studied clinical outcome at 2 years in patients included in MR CLEAN.
Methods: In MR CLEAN, patients with a proximal arterial occlusion in the anterior cerebral circulation, treatable by IAT within 6 hours after symptom onset, were randomized to IAT plus usual care, or usual care alone. Primary outcome was the modified Rankin Scale (mRS) at 90 days. The current study extended the follow-up period until 2 years after stroke onset, at which the mRS and quality of life (Eq5d),as well as recurrent strokes and other vascular events, were assessed. Treatment effect was estimated with ordinal logistic regression adjusted for prespecified prognostic factors. We estimated the effect of treatment on the occurrence of death and recurrent stroke with Cox proportional hazards model
Results: Five hundred patients were enrolled in the trial between December 2010 and March 2014. After approval for extended follow-up by the local ethics committee in May 2013, 14 patients already passed 2 year follow-up. Ninety-two patients declined consent or could not participate (e.g. living abroad). Thus 394 patients were analyzed for the long term clinical outcome and occurrence of vascular events.
Conclusions: First results will be presented at the conference.
ESOC6-1455
LATE BREAKING CLINICAL TRIALS
Oral
IMATINIB IN ACUTE STROKE STUDY (I-STROKE) OF PATIENTS TREATED WITH INTRAVENOUS THROMBOLYSIS WITHIN 4.5 HOURS AFTER ISCHAEMIC STROKE ONSET – A RANDOMISED CONTROLLED TRIAL
N. Wahlgren1, M. Thorén1, B. Höjeberg2, T.B. Käll3, C. Sjöstrand1, A.C. Laska4, J. Höijer5, H. Almqvist6, S. Holmin6, A. Lilja6, L. Fredriksson7, D. Lawrence8, U. Eriksson9 and N. Ahmed1
1Karolinska Institutet, Clinical Neuroscience, Stockholm, Sweden
2Capio S:t Göran Hospital, Neurology, Stockholm, Sweden
3Södersjukhuset, Internal Medicine, Stockholm, Sweden
4Karolinska Institutet, Clinical Sciences Danderyd Hospital, Stockholm, Sweden
5Karolinska Institutet, Unit of Biostatistics- Institute of Environmental Medicine, Stockholm, Sweden
6Karolinska Institutet, Clinical Neuroscience Neuroradiology, Stockholm, Sweden
7Karolinska Institutet, Medical Biochemistry and Biophysics, Stockholm, Sweden
8University of Michigan Medical School, Internal Medicine Division of Cardiovascular Medicine, Ann Arbor- MI, USA
9Karolinska Institutet, Biochemistry and Biophysics, Stockholm, Sweden
Abstract
Background: Disruption of the blood-brain barrier (BBB) is a critical pathophysiological event following cerebral ischaemia. BBB disruption is blamed for haemorrhagic transformation (HT) and oedema (OED) after treatment with tissue plasminogen activator (tPA), and for increasing the infarct by exposing ischaemia for infiltrating leukocytes, releasing inflammatory mediators such as cytokines, chemokines and reactive oxygen species. Imatinib, a tyrosine kinase inhibitor, has been found to restore BBB integrity by blocking signaling of the platelet-derived growth factor alpha (PDGF-alpha) receptor on perivascular astrocytes. PDGF-alpha receptors open the BBB after tPA-mediated activation of the latent form of PDGF subtype CC (PDGF-CC). Studies in experimental stroke models reveal that treatment with Imatinib lowers risk of HT, OED and reduces infarct size.
Methods: We performed a prospective, randomised, open label, blinded evaluation, dose escalating study of Imatinib at five hospitals in the Stockholm region. Patients, with a baseline NIHSS of 7–25, all had indications for intravenous thrombolysis (IVT) and received IVT < 4.5 h of stroke onset. In a first phase (N = 20), an oral dose of 400 mg daily was evaluated, followed by a second phase (N = 20) with 600 mg and a third (N = 20) of 800 mg. Randomisation was 3:1, to create four groups of equal size (n = 15), including control (total N = 60). All patients were followed until 3 months after stroke.
Results: We have results on safety and tolerability, effect on HT and OED, neurological outcome on NIHSS and functional outcome on mRS.
Conclusions: The study is complete and the results are ready to be presented at ESOC 2016.
ESOC6-1457
LATE BREAKING CLINICAL TRIALS
Oral
DO WAKE-UP STROKES DIFFER FROM OTHER STROKES OF UNKNOWN ONSET? BASELINE VARIABLES AND RESPONSE TO IV ALTEPLASE FROM THE MULTICENTER MR WITNESS TRIAL (NCT01282242)
S. Warach1, O. Wu2, S. Song3, L. Latour4, A. Ford5, A. Hsia4, A. Amuzikansky6, R. Betensky7, M. Lev8, P. Pedro6, G. Boulouis6, G. Harris2, L. Arne6, A. Yoo9 and L. Schwamm6
1Dell Medical School- University of Texas at Austin, Neurology, Austin- TX USA, USA
2Massachusetts General Hospital, Martinos Center, Boston- MA, USA
3Cedars Sinai, Neurology, Los Angeles- CA, USA
4NINDS, Stroke Branch, Bethesda- MD, USA
5Washington University, Neurology, St. Louis- MO, USA
6Massachusetts General Hospital, Neurology, Boston- MA, USA
7Harvard School of Public Health, Statistics, Boston- MA, USA
8Massachusetts General Hospital, Radiology, Boston- MA, USA
9Texas Stroke Institute, Neuroradiology, Plano- TX, USA
Abstract
Background: Many clinical trials in extended time windows include patients with last known well (LKW) time >4.5 hr and unwitnessed stroke onset if there is favorable brain imaging. It is unknown whether patients whose symptoms are discovered at the time of awakening differ from other unwitnessed stroke in baseline features or response to tPA. MR WITNESS primary results found safety of IV tPA in patients with diffusion MRI lesions, and FLAIR MRI signal intensity increases not greater than 15% treated within 4.5 hr of symptom discovery; sICH rate was comparable to that in ECASS3.
Methods: As a secondary analysis, MR WITNESS patients were categorized into two groups: symptom discovery at time of awakening (wake-up) or at a different time (unwitnessed). Four cases could not be classified. Established or hypothesized baseline predictors of clinical outcome in stroke or response to tPA were tested between the groups.Categorical variables compared using two-sided Fisher’s Exact Test; continuous variables using two-sided Wilcoxon rank-sum test. Including patients with pre-stroke mRS > 1 (n = 69), univariate and multivariate logistic regression (odds of mRS 0–1 vs mRS > 1) were calculated.
Results: Of 80 patients enrolled; 57 had symptom discovery at time of wake-up. No differences were observed between the wake-up and non-wake-up groups (Table) on known baseline predictors of clinical outcome or tPA response. Logistic regression confirmed that the wake up vs non-wake up classification did not predict 90d Rankin of 0–1.
Conclusions: In this small sample, we found no difference between patients with symptom discovery at wake-up time vs unwitnessed/unknown onset time.
AS01-001
OFFICIAL WELCOME & LARGE CLINICAL TRIALS
Oral
ULTRASOUND ENHANCED THROMBOLYSIS FOR ISCHEMIC STROKE: RESULTS OF A MULTI-NATIONAL PHASE III TRIAL (CLOTBUSTER)
A.V. Alexandrov1, M. Köhrmann2, L. Soinne3, A.D. Barreto4, A.M. Demchuk5, G. Tsivgoulis6, R. Mikulík7, G. Brandt8, J. Alleman8, J.C. Grotta9, C.A. Molina10, A.W. Alexandrov11 and P.D. Schellinger12
1University of Tennessee Health Science Center, Neurology, Memphis, USA
6University of Athens, 2nd Department of Neurology, Athens, Greece
7St Anne's Hospital, International Research Center, Brno, Czech Republic
8Cerevast Therapeutics- Inc., Clinical Trials Unit, Redmond, USA
9Memorial Hermann Hospital, Mobile Stroke Unit, Houston, USA
10Vall d'Hebron Hosital, Stroke Unit, Barcelona, Spain
11University of Tennessee Health Science Center, School of Nursing, Memphis, USA
12John Wesling Medical Center, Nerology and Neurogeriatry, Minden, Germany
Abstract
Background: Pulsed wave ultrasound at the diagnostic frequency and intensity exposes intracranial thrombus to tissue plasminogen activator (tPA) thereby facilitating early reperfusion and clinical recovery from stroke. Our objective was to determine the efficacy of sonothrombolysis for the treatment of ischemic stroke.
Methods: We conducted a randomized double-blind controlled clinical trial in 70 active North American, European and Australasian centers. All patients with acute ischemic stroke were treated with 0.9 mg/kg intravenous tPA within time frames approved by national authorities. Patients had NIHSS scores 10 or greater and received up to 2 hours of 2 MHz pulsed wave ultrasound (Target group) or sham monitoring (Control) using a novel operator independent therapeutic ultrasound device. Primary global efficacy end-point was ordinal modified Rankin Score shift analysis with intention to treat among patients receiving tPA within 0–4.5 hours of symptom onset. Primary tPA on–label end-point for the United States and Canada included similar analysis in patients treated up to 3 hours.
Results: After the trial was stopped by pre-planned interim analysis at N = 526 for pre-specified futility threshold crossing and no significant increase in sICH, we completed pending 90 day follow-ups of patients recruited in January-March, 2015 that were not included in the interim analysis. A total of 674 patients randomized became available for final analysis that is now being completed and will be presented at ESOC 2016.
Conclusions: Exposure of stroke patients treated with intravenous tPA to low power ultrasound was feasible with no significant clinical benefit in the intention to treat analysis.
AS01-060
OFFICIAL WELCOME & LARGE CLINICAL TRIALS
Oral
ENCHANTED MAIN RESULTS - TRIAL OF LOW-DOSE VERSUS STANDARD-DOSE INTRAVENOUS TISSUE PLASMINOGEN ACTIVATOR IN 3310 PATIENTS WITH ACUTE ISCHEMIC STROKE
C. Anderson1, T. Robinson2, R. Lindley1, P. Lavados3, Y. Huang4, V. Sharma5, X. Chen1, G. Chen6, N. Thang7, T. Lee8, Y. Cao9, M. Parsons10, C. Levi10, V. Olavarría11, A. Demchuk12, P. Bath13 and J. Broderick14
1The George Institute for Global Health, Neurological & Mental Health Division, Sydney, Australia
2University of Leicester, Department of Cardiovascular Sciences and NIHR Biomedical Research Unit, Leicester, United Kingdom
3Clinica Alemana Universidad del Desarrollo, Clinica Alemana de Santiago- Facultad de Medicina-, Santiago, Chile
4Peking University First Hospital, Department of Neurology-, Beijing, China
5National University Hospital and School of Medicine- National University of Singapore, Division of Neurology- Department of Medicine-, Singapore, Singapore
6Xuzhou Central Hospital, Department of Neurology-, Xuzhou, China
7People’s 115 Hospital, Department of Cerebrovascular Disease, Ho Chi Minh, Vietnam
8Linkou Chang Gung Memorial Hospital, Department of Neurology, Taoyuan, China
9The Second Affiliated Hospital of Soochow University, Department of Neurology, Suzhou, China
10John Hunter Hospital- and Hunter Medical Research Institute- University of Newcastle, Neurology Department, Newcastle, Australia
11Facultad de Medicina- Clinica Alemana Universidad del Desarrollo, Clinica Alemana de Santiago, Santiago, Chile
12Radiology Hotchkiss Brain Institute- University of Calgary-, Calgary Stroke Program- Department of Clinical Neurosciences, Calgary, Canada
13University of Nottingham, Stroke Trials Unit- Division of Clinical Neuroscience-, Nottingham, United Kingdom
14University of Cincinnati Neuroscience Institute, Departments of Neurology and Rehabilitation Medicine and Radiology-, Cincinnati, USA
Abstract
Background: A lower dose of tissue plasminogen activator (tPA) may improve outcome with reduced risk of intracerebral hemorrhage (ICH) in acute ischemic stroke (AIS). ENCHANTED uses a partial factorial design to evaluate the effectiveness of (i) low- versus standard-dose intravenous tPA, and (ii) early intensive blood pressure (BP) lowering versus guideline-recommended BP management. We report the main results of the tPA dose arm.
Methods: An investigator-initiated and conducted, international, multicenter clinical trial designed to test for non-inferiority on the primary efficacy outcome of death or disability at 90 days (mRS scores 2–6). The secondary objective was to test for superiority in reducing symptomatic ICH defined by several standard criteria. Main funding is from the National Health and Medical Research Council (NHMRC) of Australia.
Results: From March 2012 through August 2015, 3310 thrombolysis-eligible AIS patients <4.5 hrs of symptom onset were randomized: 1661 to low-dose (0.6 mg/kg) and 1649 to standard-dose (0.9 mg/kg) of tPA from 100+ hospitals in 13 countries. The groups were well balanced for baseline demographic and clinical characteristics of patients, with a median age 67 yrs (iqr 58–76; 14% ≥ 80 yrs), 38% female, and 60% Asian. Median pre-treatment NIHSS was 8 (iqr 5–14) and time from stroke onset to treatment was 170 (iqr 125–219) mins.
Conclusions: The main results are presented at the conference. Low-dose tPA may result in similar efficacy and reduced risk of ICH compared to standard-dose tPA; thus providing a potentially a safer and more affordable treatment in AIS. (ENCHANTED ClinicalTrials.gov number NCT01422616)
ESOC6-1451
OFFICIAL WELCOME & LARGE CLINICAL TRIALS
Oral
EFFICACY OF LOW-DOSE VS STANDARD-DOSE RTPA BETWEEN ASIAN AND NON-ASIAN WITH PARTICULAR EMPHASIS ON STROKE SUBTYPE AND RISK OF INTRACEREBRAL HEMORRHAGE
J. Chalmers1 and C. Anderson2
1The George Institute, professorial division, Sydney, Australia
2The George Institute, Neurological and Mental Health Division, Sydney, Australia
Abstract
Background: Asians are believed to benefit more from a lower dose of alteplase than non-Asians who experience acute ischaemic stroke (AIS), due to ethnic-specific hemostatic and/or cerebrovascular factors. We undertook further examination of an ethnic interaction effect of low-dose versus standard-dose alteplase in the ENCHANTED trial.
Methods: ENCHANTED was an international, multi-centre, open, active-comparison, blinded outcome assessed clinical trial involving 3310 AIS patients (≤4.5 hrs) randomised to low-dose (0.6 mg/kg) vs. standard-dose (0.9 mg/kg) intravenous alteplase. Primary efficacy outcome was death or disability (mRS 2–6) at 90 days. Secondary (safety) outcome was symptomatic intracerebral haemorrhage (sICH). Funding is from the National Health and Medical Research Council of Australia, Stroke Association of the United Kingdom, and others. (ClinicalTrials.gov number NCT01422616)
Results: There were 2079 Asian and 1212 non-Asian with known ethnicity. Non-Asians were older (72 vs 65 years) and more often female (43% vs 35%) with a history of hypertension (66% vs 61%), other heart disease (10% vs 5%), atrial fibrillation (22% vs 18%), hypercholesterolemia (33% vs 8%) but had less prior stroke (16% vs 19%) and tobacco smokers (19% vs 26%). Median (iqr) pretreatment NIHSS was 8 (5 to 13) in non-Asians and 9 (5 to 14) in Asians. Time from stroke onset to treatment was 149 (115 to 198) minutes in non-Asians and 180 (140 to 225) in Asians. The comparative treatment effects will be presented.
Conclusions: Low-dose alteplase may prove a safer and more effective treatment for Asian patients with AIS.
AS04-001
OFFICIAL WELCOME & LARGE CLINICAL TRIALS
Oral
TICAGRELOR VS. ASPIRIN IN ACUTE STROKE OR TRANSIENT ISCHEMIC ATTACK: PRIMARY RESULTS OF THE SOCRATES RANDOMIZED TRIAL
S.C. Johnston1, P. Amarenco2, G.W. Albers3, H. Denison4, J.D. Easton5, S. Evans6, P. Held4, J. Jonasson4, K. Minematsu7, C. Molina8, Y. Wang9 and L. Wong10
1UT Austin, Dell Medical School, Austin, USA
2Bichat University Hospital and Medical School, Department of Neurology and Stroke Center, Paris, France
3Stanford University Medical Center, Stanford Stroke Center, Palo Alto, USA
4AstraZeneca, Clinical Trials, Molndal, Sweden
5University of California San Francisco, Department of Neurology, San Francisco, USA
6Harvard University School of Public Health, Department of Biostatistics, Boston, USA
7National Cerebral and Cardiovascular Center, Research Department, Suita- Osaka, Japan
8Hospital Vall d'Hebron, Stroke Unit, Barcelona, Spain
9Tiantan Hospital, Department of Neurology, Beijing, China
10Chinese University of Hong Kong, Department of Medicine & Therapeutics, Hong Kong, China
Abstract
Background: The risk of stroke and other ischemic events is high after ischemic stroke and transient ischemic attack (TIA), especially in the acute period. Antiplatelet therapy may be particularly effective in this setting.
Methods: SOCRATES was a randomized, double-blind trial (NCT01994720). Participants were randomized to ticagrelor (180-mg loading dose on day 1 followed by 90 mg twice daily for days 2–90) or aspirin (300 mg on day 1 followed by 100 mg daily for days 2–90). Participants were ≥40 years of age with an ischemic stroke (with a National Institutes of Health Stroke Scale score ≤5) or high-risk TIA (defined as an ABCD2 score ≥4). Randomization had to occur within 24 hours of the time last known free of new ischemic symptoms. The primary efficacy end point was the composite of stroke (ischemic or hemorrhagic), myocardial infarction, or death during 90-day follow-up. Major hemorrhage was the primary safety end point.
Results: Overall, 13,198 patients were randomized from 721 sites in 33 countries worldwide. Median age was 66 years and 58.5% were men. The index event was TIA in 27% and ischemic stroke in 73%, and 37% were randomized within 12 hours of symptom onset. Database lock will occur in March 2016. Primary treatment results will be presented.
Conclusions: The SOCRATES trial provides important information about whether the antiplatelet agent, ticagrelor, is superior to aspirin, the current standard of care, in reducing risk of major events acutely after ischemic stroke or TIA.
W. Ziai1, I. Awad2, B. Gregson3, D. Mendelow3, K. Lees4, J. Dawson4, A. Mould1, K. Lane1, N. McBee1, P. Keyl1, J. Betz5, E. Sugar5, G. Yenokyan5, S. Harnof6, M. Rosenblum5, R. Thompson5 and D. Hanley1
1Johns Hopkins University, Neurology, Baltimore, USA
2University of Chicago, Neurosurgery, Chicago, USA
3Newcastle University, Neurosurgery, Newcastle, United Kingdom
4University of Glasgow, Neurology, Glasgow, United Kingdom
5Johns Hopkins University School of Public Health, Biostatistics, Baltimore, USA
6Sheba Medical Center, Neurosurgery, Ramat Gan, Israel
Abstract
Background: Specific therapy to remove intraventricular hemorrhage (IVH) and treat obstructive hydrocephalus may be efficacious in severe IVH. However, concern exists that mortality improvement without functional improvement creates little patient benefit. CLEAR III, a randomized double-blind, placebo-controlled trial, tested if pragmatically employed extraventricular drainage (EVD) plus alteplase improved outcome by removing 80% of IVH clot. We report new 365-day functional outcome and quality of life (QOL) data.
Methods: We randomized 500 subjects from 73 sites (2009–2014), to receive up to 12 doses of alteplase(A) or saline(PCB). Blinded modified Rankin Scale (mRS) scores were assessed at 30, 180 and 365 days.
Results: Mortality was significantly lower in alteplase treated patients over 365 days (p = 0.007). Extent of IVH removal correlated with mortality (p = 0.04) and good outcome (p < 0.001). From 180–365 days, mRS, extended Glasgow Outcome Scale showed ongoing improvement of 3% and 5%, respectively at mRS/eGOS thresholds for functional improvement (0–3; USD-LSD); no statistically significant difference in improvement between A and PCB. Domicile arrangements demonstrated 10% more subjects at home + rehab in the alteplase group (5%-H;5%-R); Long-term care facility was equal 11% in both groups. Stroke Impact Scale, Barthel and EuroQol measures from 30–365 days demonstrated sustained improvement (p < 0.001). SIS showed expected levels of personal satisfaction across each level of mRS/eGOS. Controlled use of alteplase produced 10% lower mortality (NNT = 10) with more efficient and safer care. 365-day QOL was similar for both treatments.
Conclusions: Further investigation of impact of alteplase treatment on functional status of IVH patients is required if this promising therapy is to be adopted.
AS02-016
OFFICIAL WELCOME & LARGE CLINICAL TRIALS
Oral
ANTIHYPERTENSIVE TREATMENT OF ACUTE CEREBRAL HEMORRHAGE PHASE III (ATACH-II) TRIAL PRIMARY RESULTS: ANALYSES BY ASIAN AND NON-ASIAN SUBGROUPS
Y. Palesch1 and A. Qureshi2
1Medical University of South Carolina, Charleston, USA
2University of Minnesota, Neurology, Minneapolis, USA
Abstract
Background: The primary aim of ATACH II Trial was to determine the potential benefit of early intensive systolic blood pressure (SBP) treatment (≤140 mmHg) compared to the standard SBP treatment (≤180 mmHg) in reducing the proportion of ICH subjects with 3-month mRS scores 4–6. Maximum of 1,280 subjects were planned to be randomized to detect an absolute 10% difference in the poor outcome between the treatment groups. Conditional power evaluation at the second interim analysis, using the primary outcome of 850 subjects, resulted in the futility conclusion. The Trial subsequently terminated with 1,000 randomized subjects. The overall study results will be presented separately by the study principal investigator. This presentation will focus on the analysis by Asian vs non-Asian subgroups.
Methods: The Trial involved 110 sites from US (73), Germany (8), Japan (14), China (5), South Korea (2), and Taiwan (8). The Asian sites enrolled 53.7% of the subjects. Therefore, we have added to the statistical analysis plan, subgroup analyses of key efficacy (3-month mRS and EQ-5D; 24-hour hematoma expansion) and safety (SAEs and deaths) outcomes by Asian versus non-Asian sites. A brief demographic distributions are presented below.
Results: The last randomized subject’s visit occurred in December 2015. The trial database will be locked by early March 2016. This abstract will be updated with the results by 20 March.
Conclusions: See Results Section.
Region
N
% Male
Mean (sd) Age
Asian
537
66.7
61.1 (13.0)
Non-Asian
463
56.6
62.8 (13.2)
Overall
1,000
62.0
61.9 (13.1)
AS02-019
OFFICIAL WELCOME & LARGE CLINICAL TRIALS
Oral
ANTIHYPERTENSIVE TREATMENT OF ACUTE CEREBRAL HEMORRHAGE (ATACH) II TRIAL
A. Qureshi1 and Y. Palesch2
1Zeenat Qureshi Stroke Research Center, Neurology, Minneapolis, USA
2Medical University of South Carolina, Department of Public Health Sciences, Charleston, USA
Abstract
Background: There is controversy regarding the most appropriate target for systolic blood pressure reduction in the acute period among patients with intracerebral hemorrhage. Intensive systolic blood pressure treatment may reduce the rate and magnitude of hematoma expansion observed in approximately three fourths of the patients with acute intracerebral hemorrhage.
Methods: The ATACH-II trial was a multicenter, parallel, two-arm study, where eligible subjects with spontaneous intracerebral hemorrhage were randomized to early intensive (goal <140 mm Hg) and standard (goal < 180 mm Hg) systolic blood pressure reduction in a 1:1 ratio within 4.5 hours of symptom onset. Treatment success was defined by reduction and maintenance of hourly minimum systolic blood pressure within goals of allocated treatment arm for 24 hours post symptom onset. The primary outcome of death and disability was defined by modified Rankin scale of 4 to 6, and ascertained at 3-month post randomization by a blinded investigator.
Results: There were 500 subjects randomized to intensive-treatment group and 500 subjects randomized to standard-treatment group. In intent-to-treat analysis, the relative risk of death and disability at 3 months in the intensive and in the standard treatment will be presented after adjusting for initial Glasgow Coma scale, hematoma volume, and presence of intraventricular hemorrhage. The group differences in the rate of serious adverse events will be presented.
Conclusions: Compared with standard systolic blood pressure reduction, the therapeutic effect of intensive systolic blood pressure reduction in patients with intracerebral hemorrhage on adjusted rates of death and disability will be provided.
ESOC6-1434
OFFICIAL WELCOME & LARGE CLINICAL TRIALS
Oral
BENEFITS AND RISKS OF LOW- VERSUS STANDARD-DOSE ALTEPLASE IN PATIENTS ON PRIOR ANTIPLATELET THERAPY: THE ENCHANTED TRIAL
T. Robinson1, R. Lindley2, P. Lavados3, Y. Huang4, V. Sharma5, J.S. Kim6, H. Arima7, N. Thang8, C. Levi9, A. Demchuk10, P. Bath11, J. Broderick12, G. Donnan13, S. Ricci14, X. Wang2, G. Chen15, T.H. Lee16, S. Martins17, J. Chalmers2 and C. Anderson2
1University of Leicester, Department of Cardiovascular Sciences, Leicester, United Kingdom
2The George Institute for Global Health, Neurological and Mental Health Division, Sydney, Australia
3Clinica Alemana Universidad del Desarrollo, Clinica Alemana de Santiago, Santiago, Chile
4Peking University First Hospital, Department of Neurology, Beijing, China
5National University of Singapore, Division of Neurology, Singapore, Singapore
6University of Ulsan, Department of Neurology, Seoul, Republic of Korea
7Fukuoka University, Department of Preventive Medicine and Public Health, Fukuoka, Japan
8People's 115 Hospital, Department of Cerebrovascular Disease, Ho Chi Minh City, Vietnam
9Hunter Medical Research Institute, Neurology Department, Newcastle, Australia
10University of Calgary, Department of Clinical Neurosciences and Radiology, Calgary, Canada
11University of Nottingham, Division of Clinical Neuroscience, Nottingham, United Kingdom
12University of Cincinnati Academic Health Center, Departments of Neurology and Rehabilitation Medicine and Radiology, Cincinnati, USA
13Florey Institute of Neuroscience and Mental Health, Florey Institute of Neuroscience and Mental Health, Parkville, Australia
14USL Umbria 1, UO Neurologica, Branca, Italy
15Xuzhou Central Hospital, Department of Neurology, Jiangsu, China
16Linkou Chang Gung Memorial Hospital, Department of Neurology, Taoyuan, Taiwan
17Hospital de Clinicas de Porto Alegre, Stroke Division of Neurology Service, Porto Alegre, Brazil
Abstract
Background: Higher rates of symptomatic intracerebral haemorrhage (sICH), a disabling and potentially fatal complication of stroke thrombolysis, are seen in patients on prior antiplatelet therapy (APT), who account for ∼1/3 of the thrombolysis population. In a post-hoc analysis of the ENCHANTED trial, interaction effects between low- versus standard-dose alteplase and prior APT in acute ischaemic stroke (AIS) were assessed.
Methods: An international, multi-centre, prospective, randomized, open-label, blinded-endpoint trial. Outcomes included combined endpoint of 90-day death or disability (modified Rankin Scale 2 to 6, 3 to 6, or ordinal shift) and sICH.
Results: There were 3285 thrombolysis-eligible AIS patients (38% female), mean age 67 years (SD 13) included in these analyses, of whom 752 (23%) reported prior aspirin/other APT at time of randomisation <4.5 hours to low- or standard-dose alteplase. Compared to others, prior APT-use patients were older, more often Asian, had greater baseline imaging features of more severe stroke, use of statins and had greater co-morbidity; and they were treated more quickly and with a higher bolus dose of alteplase. All these variables were accounted in adjusted analysis of the treatment effects on key measures of the primary outcome.
Conclusions: These results will accompany those of the main results presented at the ESO Conference. Low-dose alteplase may result in reduced risk of sICH in patients on prior APT, compared to those on standard-dose alteplase, providing a safer alternative treatment for clinicians. (ENCHANTED ClinicalTrials.gov number NCT01422616)
AS03-033
OFFICIAL WELCOME & LARGE CLINICAL TRIALS
Oral
A RANDOMIZED TRIAL OF UNRUPTURED BRAIN AVMS (ARUBA): FINAL OUTCOME RESULTS BY TREATMENT MODALITY
C. Stapf1, J.R. Overbey2, J.P. Mohr3, A.J. Moskowitz2, E. Vicaut4 and M.K. Parides2
1CRCHUM, Neurosciences- Université de Montréal, Montreal, Canada
2InCHOIR, Icahn School of Medicin at Mount Sinai, New York- NY, USA
3Columbia University Medical Center, Stroke Center- The Neurological Institute, New York- NY, USA
4APHP - Hôpital Lariboisière, U.R.C., Paris, France
Abstract
Background: ARUBA is a prospective, multicenter, parallel design, open, randomised controlled clinical trial comparing medical management with interventional therapy inpatients diagnosed with an unruptured brain arteriovenous malformation (AVM). In 2013, patient recruitment had been halted by the NIH/NINDS appointed DSMB as a planned interim analysis had shown a significantly lower risk of death or stroke in patients followed without intervention (HR = 0.27, 95% CI 0.140.54).The DSMB recommended pursuing the planned 5-year follow-up in order to determine if these differences persist over time.
Methods: The primary aim of the trial is to determine whether medical management alone is superior to invasive therapy in averting death (any cause) or stroke (symptomatic hemorrhage or infarction). The secondary aim is to determine whether treatment of unruptured brain AVMs by medical management alone offers a lower risk of death or clinical impairment (modified Rankin Score (mRS) > /= 2) at 5 years post randomization compared to invasive therapy.
Results: Overall, 226 patients (aged ≥18 years, diagnosed with an unruptured brain AVM suitable for curative intervention) have been randomly assigned (1:1) to best possible invasive therapy (medical management plus endovascular, surgical, and/or radiation therapy) versus medical management alone. The final results of the primary (symptomatic stroke or death) and secondary (mRS) endpoints will be presented along with subgroup analysis for specific subgroups and treatment modlaities.
Conclusions: The final results of the trial offer important data on the eventual long-term benefit of non-interventional management of patients diagnosed with an unruptured brain AVM.
Funding: NIH/NINDS cooperative agreements U01NS051483 and U01NS051566.
SEDATION AND AIRWAY DURING ENDOVASCULAR TREATMENT ACUTE ISCHEMIC STROKE TREATMENT: PRIMARY AND SHORT-TERM RESULTS FROM THE RANDOMIZED TRIAL SIESTA (SEDATION VS INTUBATION FOR ENDOVASCULAR STROKE TREATMENT)
S. Schönenberger1, L. Uhlmann2, S. Schieber1, S. Mundiyanapurath1, J. Purrucker1, J. Pfaff3, M. Möhlenbruch3, M. Bendszus3, M. Kieser4, W. Hacke1 and J. Bösel1
2University of Heidelberg, Institute of Biometry and Informatics, Heidelberg, Germany
3University of Heidelberg, Neuroradiology, Heidelberg, Germany
4University of Heidelberg, Institute of Biometrics and Informatics, Heidelberg, Germany
Abstract
Background: An important and controversial issue of peri-interventional management of endovascular stroke treatment (EST) is the management of sedation and airway. According to retrospective data the widely favored intubation and general anesthesia (GA) appears associated with worse functional outcome compared to “conscious sedation” (CS) in the non-intubated state.
Methods: SIESTA is a prospective, monocentric, outcome assessor-blinded, 1:1 randomized, parallel-group interventional study comparing non-intubated vs. intubated patients receiving EST for acute ischemic stroke of the anterior circulation (www.clinicaltrials.gov, NCT 02126085, protocol published**). Primary endpoint is the improvement of the National Institute of Health Stroke Scale (NIHSS) score after 24 hours.
Results: Recruitment has been completed with enrolment of 150 patients, 61 female and 89 male, at a mean age of 72 years, with a median baseline NIHSS score of 17. Of these patients, 64% received pre-procedural rtPA. Of the 78 patients randomized to CS, 11 (8.5%) had to be converted to GA during the procedure. At the meeting, the primary endpoint and selected short-term secondary endpoints will be presented for the first time.
Conclusions: The aim of this study is to elucidate potential advantages of the non-intubated compared to the intubated state in stroke patients receiving EST.
** Ref.: Schönenberger S et al., Sedation vs. Intubation for Endovascular Stroke TreAtment (SIESTA) – a randomized monocentric trial, Protocol, 2015, Int J Stroke, 10; 969–978
AS06-006
PRESIDENTS' SYMPOSIUM: AWARDS AND TRIALS
Oral
FACTOR XA INHIBITORS VERSUS VITAMIN K ANTAGONISTS FOR PREVENTING CEREBRAL OR SYSTEMIC EMBOLISM IN PATIENTS WITH ATRIAL FIBRILLATION: RESULTS FROM AN UPDATED COCHRANE SYSTEMATIC REVIEW
K. Bruins Slot1 and E. Berge1
1Oslo University Hospital, Internal Medicine, Oslo, Norway
Abstract
Background: Anticoagulant treatment with vitamin K antagonists (VKA) is effective in preventing thromboembolic complications in patients with atrial fibrillation (AF). We compared the effectiveness of factor Xa inhibitors (FXaI) with VKAs.
Methods: We performed a systematic review of trials that directly compared long-term treatment with FXaI and VKA for the prevention of cerebral and systemic embolism in patients with AF. We used a fixed-effect model to calculate a weighted estimate of the treatment effect across trials, using odds ratio (OR) with 95% confidence intervals (CI).
Results: We included data from 67,688 participants from 13 trials. These trials compared apixaban, betrixaban, darexaban, edoxaban, idraparinux, idrabiotaparinux or rivaroxaban with dose-adjusted warfarin. Treatment with FXaI significantly decreased the number of strokes and other systemic embolic events (OR 0.87, 95% CI 0.80 to 0.95 - see forest plot). FXaI also reduced the number of major bleedings (OR 0.78, 95% CI 0.73 to 0.84), though statistically significant heterogeneity was observed (I2 = 72%). A pre-specified sensitivity analysis using a random-effects model also showed a statistically significant decrease in the number of major bleedings (OR 0.76, 95% CI 0.60 to 0.96).
Conclusions: FXaIs reduce both the number of strokes and systemic embolic events, and number of major bleedings compared with warfarin in patients with AF. These data support current clinical guidelines that recommend licensed FXaIs in patients with AF.
AS06-017
PRESIDENTS' SYMPOSIUM: AWARDS AND TRIALS
Oral
ANTIPLATELET THERAPY IN PATIENTS WITH CEREBRAL ISCHAEMIA FROM ARTERIAL ORIGIN: NETWORK META-ANALYSIS
J.P. Greving1, H.C. Diener2, L. Csiba3, W. Hacke4, L.J. Kappelle5, P.J. Koudstaal6, D. Leys7, J.L. Mas8, R.L. Sacco9, J. Sivenius10, A. Algra1,5
1University Medical Center Utrecht, Julius Center for Health Sciences and Primary Care, Utrecht, Netherlands
2University Hospital Essen, Department of Neurology, Essen, Germany
3University of Debrecen Medical and Health Science Center, Department of Neurology, Debrecen, Hungary
4University of Heidelberg, Department of Neurology, Heidelberg, Germany
5University Medical Center Utrecht, Department of Neurology and Neurosurgery, Utrecht, Netherlands
6Erasmus Medical Center, Department of Neurology, Rotterdam, Netherlands
7Roger Salengro Hospital, Department of Neurology, Lille, France
8Hôpital Sainte-Anne- Université Paris Descartes, Department of Neurology, Paris, France
9Miller School of Medicine- University of Miami, Department of Neurology, Coral Gables- Florida, USA
10University Hospital of Kuopio and University of Eastern Finland, Department of Neurology, Kuopio, Finland
Abstract
Background: To compare the efficacy and safety of antiplatelet regimens in patients with cerebral ischaemia of arterial origin (CIAO).
Methods: We performed network meta-analyses with individual patient data from six randomized controlled trials (CAPRIE, ESPS-2, MATCH, CHARISMA, ESPRIT and PRoFESS) to compare four antiplatelet regimens in patients with CIAO. Primary outcome was the composite of vascular death, stroke or myocardial infarction (vascular events). We performed a frequentist random-effects network meta-analysis with package netmeta in R.
Results: After a median follow-up of 2.0 years (IQR 1.5–2.7), 5424 of the 43112 patients had experienced a vascular event (5022 ischaemic events). Aspirin + dipyridamole (HR 0.85, 95% credible interval 0.77–0.94), clopidogrel (HR 0.87, 0.79–0.95) and aspirin + clopidogrel (HR 0.82, 0.72–0.93) caused significantly less vascular events than aspirin alone (Table 1). Clopidogrel significantly reduced major bleeding compared with aspirin (HR 0.75, 0.61–0.92). Aspirin + clopidogrel resulted in significantly more major bleedings compared with aspirin, aspirin + dipyridamole and clopidogrel (Table 2). Clopidogrel significantly reduced intracranial haemorrhage compared with aspirin, aspirin + dipyridamole, and aspirin + clopidogrel. Aspirin + dipyridamole (HR 0.87, 0.79–0.95) and clopidogrel (HR 0.88, 0.80–0.96) caused significantly less vascular events plus major bleedings than aspirin alone (Table 3). The results from pairwise comparisons with available head-to-head data closely matched those from the network meta-analysis.
Conclusions: Clopidogrel and aspirin + dipyridamole have a comparable risk-benefit profile for secondary prevention after cerebral ischaemia. Rigorously conducted comparative network meta-analyses of individual patient data are required to fully elucidate the comparative benefits and harms of antiplatelet regimes across various subpopulations.
ESOC6-1453
PRESIDENTS' SYMPOSIUM: AWARDS AND TRIALS
Oral
THE VERTEBRAL ARTERY ISCHAEMIA STENTING TRIAL (VIST) - FIRST RESULTS ON BEHALF OF THE VIST INVESTIGATORS
H. Markus1
1, United Kingdom
Abstract
Background: Prospective observational studies have shown that symptomatic vertebral stenosis is associated with a high rate of early recurrent stroke. Vertebral stenting can be performed with a good technical success rate. Thousands of vertebral stentings have been performed worldwide outside clinical trials but there is little data from clinical trials to assess its therapy compared with best medical therapy. The Vertebral artery Ischaemia Trial (VIST) was set up to answer this question.
Methods: Patients with >50% vertebral stenosis and recent symptoms of posterior circulation stroke or TIA (within the last there months) were randomised to stenting and best medical therapy or best medical therapy alone. Randomisation was stratified for the site of stenosis (extra- versus intracranial)
Results: 182 patients were recruited from 14 centres in the United Kingdom. Three patients dropped out immediately after randomisation before receiving allocated treatment (1 stenting, 2 best medical therapy) leaving 179 (stenting 91; medical therapy alone 88) in the intention to treat analysis. The two groups were well balanced for age, gender and vascular risk factors. The last patient was recruited in February 2015 and follow-up of at least one year for all patients is now complete. Mean (maximum) follow-up is 3.3 (7.3) years; total person-years of follow-up is 593 years. 35% presented with TIA and 64% with stroke.
Conclusions: The first results from VIST will be presented.
AS04-012
PRESIDENTS' SYMPOSIUM: AWARDS AND TRIALS
Oral
PREVENTION OF DEMENTIA BY INTENSIVE VASCULAR CARE (preDIVA) - A CLUSTER-RANDOMIZED TRIAL
E. Richard1,2, E.P. Moll van Charante3, L.S. Eurelings2, J.W. van Dalen2, S.A. Ligthart3, E.F. van Bussel3, M.P. Hoevenaar-Blom2, M. Vermeulen2 and W.A. van Gool2
1Radboud University Medical Centre, Neurology, Nijmegen, Netherlands
2Academic Medical Centre, Neurology, Amsterdam, Netherlands
3Academic Medical Centre, Primary care, Amsterdam, Netherlands
Abstract
Background: Observational studies show that cardiovascular and lifestyle related risk factors are associated with an increased risk of dementia. It is unknown whether targeting these risk factors prevents dementia. In the preDIVA trial we test whether a multicomponent intervention targeting vascular and lifestyle related risk factors could prevent incident dementia.
Methods: In an open cluster-randomized controlled clinical trial in primary care, with blind outcome adjudication, 3526 persons (age 70–78 years) were randomized to nurse-led vascular care (1890 participants) or usual care (1636 participants). The planned intervention and follow-up duration were six years. Primary outcomes were cumulative dementia incidence and disability. Main secondary outcomes were incident cardiovascular disease (CVD), mortality and dementia according to subtype.
Results: Complete data for the primary outcome were obtained for 3454 persons (98%) after a median follow-up of 6.7 years, yielding 21,341 observed person-years. Dementia occurred in 233/3453 participants (6,7%). During the study 578 participants (16,4%) died. Stroke/TIA occurred in 222/2844 participants (7,8%).
Conclusions: PreDIVA is the largest and longest running RCT ever with incident dementia as primary outcome. The pragmatic primary outcome has resulted in a complete follow-up in a very high percentage of participants. The manuscript is under review. Results of the trial will be presented depending on the review process.
ESOC6-1460
PRESIDENTS' SYMPOSIUM: AWARDS AND TRIALS
Oral
EFFECTS OF ALTEPLASE WITHIN 6 HOURS OF ISCHAEMIC STROKE ON SURVIVAL UP TO 3 YEARS: RESULTS FROM THE THIRD INTERNATIONAL STROKE TRIAL
M. Roaldsen1, W. Whiteley2, E. Berge3, G. Cohen2, E. Lundström4, A.S. Rudberg5, J. Forbes6, J. Smith7, K. Bruins Slot3, R. Lindley8, J. Wardlaw2 and P. Sandercock2
1University of Tromsø, Department of Clinical Medicine, Tromsø, Norway
2University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
3Oslo University Hospital, Department of Internal Medicine, Oslo, Norway
4Karolinska Institutet, Department of Clinical Neuroscience, Stockholm, Sweden
5Karolinska Institutet, Department of Clinical Sciences, Stockholm, Sweden
6University of Limerick, Health Research Institute, Limerick, Ireland
7Oxford University, Department of Population Health, Oxford, United Kingdom
8University of Sydney, The George Institute for Global Health, Sydney, Australia
Abstract
Background: An objective of the Third International Stroke Trial (IST-3) was to assess the effect of intravenous alteplase on long-term survival after ischaemic stroke.
Methods: IST-3 was an international, multicentre, randomised-controlled, open-label trial of intravenous alteplase (0·9 mg/kg) plus standard care versus standard care alone within 6 hours of ischaemic stroke. We followed participants in the UK, Sweden and Norway for survival up to 36 months after randomisation, using data from national registries, and compared survival in the two groups with proportional hazards survival analysis, adjusting for key prognostic variables.
Results: Of all 3,035 participants in the trial, 1946 were recruited in the UK (1446), Sweden (297) and Norway (203). By 36 months, 453 of 967 alteplase participants (46.8%) and 494 of 979 controls (50.5%) had died. Participants given alteplase had a significantly higher hazard of death during the first 7 days (HR 1.46, 95% CI 1.06–2.01) and a significantly lower hazard in the period 8 days to 36 months (HR 0.78, 95% CI 0.68–0.90). The results did not differ significantly between those aged ≤80 vs. >80 years, with NIHSS score ≤10 vs. >10, or treated ≤3 vs. >3 hours (all p > 0.05).
Conclusions: Among those who survive the first seven days, alteplase given within 6 hours of ischaemic stroke is associated with increased long-term survival. We recommend long-term follow up in new trials of intravenous thrombolytic treatment.
AS02-002
PRESIDENTS' SYMPOSIUM: AWARDS AND TRIALS
Oral
PLATELET TRANSFUSION IN CEREBRAL HAEMORRHAGE (PATCH): A RANDOMISED CONTROLLED CLINICAL TRIAL
M. Baharoglu1, R. Al-Shahi Salman2, C. Cordonnier3 and Y. Roos1
1Academic Medical Center University of Amsterdam, neurology, Amsterdam, Netherlands
2University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
3University of Lille- Inserm- CHU Lille, Degenerative & vascular cognitive disorders, Lille, France
Abstract
Background: Antiplatelet therapy use at the time of intracerebral haemorrhage (ICH) is associated with higher mortality. Reduction of haematoma growth using platelet transfusion might improve outcome. The objective of PATCH was to investigate whether platelet transfusion improves outcome compared to standard care at three months in people with spontaneous ICH taking antiplatelet therapy.
Methods: PATCH was a multicentre prospective, randomised, open, blinded-endpoint (PROBE) parallel group trial, conducted at 60 hospitals in The Netherlands, Scotland and France. We enrolled patients with spontaneous supratentorial ICH aged ≥18 years using antiplatelet therapy for ≥7 days preceding ICH, with Glasgow Coma Scale score ≥8. Participants were randomised (1:1, with a secure web-based system using permuted blocks, stratified by study hospital and type of antiplatelet therapy) to receive either platelet transfusion (intervention) within six hours of start of symptoms and 90 minutes of diagnostic brain imaging, or standard care without platelet transfusion (comparator). The primary outcome (modified Rankin Scale score) was assessed blinded to treatment allocation three months after ICH. PATCH was registered with the Netherlands trial register (NTR1303). Funding: The Netherlands Organization for Health Research and Development (ZON-MW), Sanquin Blood Supply in the Netherlands; Chest Heart and Stroke Scotland in Scotland; and Le programme hospitalier de recherche clinique in France.
Results: 190 participants were randomised to intervention (n = 97, mean age 74.0 ± 10.2 years) or comparator (n = 93, mean age 73.5 ± 11.2 years) between February 2009 and October 2015. Final primary outcome results will be presented at the ESO conference.
Conclusions: not available
AS04-024
PRESIDENTS' SYMPOSIUM: AWARDS AND TRIALS
Poster
A RANDOMIZED COMPARISON OF SYNCHRONOUS CABG AND CAROTID ENDARTERECTOMY VS ISOLATED CABG IN PATIENTS WITH ASYMPTOMATIC HIGH-GRADE CAROTID STENOSIS: THE CABACS TRIAL
C. Weimar1, K. Bilbilis2, J. Rekowski3, F. Beyersdorf4, M. Breuer5, M. Dahm6, A. Diegeler7, A. Kowalski8, S. Martens9, F.W. Mohr10, J. Ondrášek11, B. Reiter12, P. Roth13, R. Seipelt14, M. Siggelkow8, G. Steinhoff15, U. Stock16, M. Wilhelmi.17, G. Wimmer-Greinecker18, S. Knipp19 and CABACS Study group
1Universitätsklinikum Essen, Klinik für Neurologie, Essen, Germany
2Universitätsklinikum Essen, Zentrum für Klinische Studien (ZKSE), Essen, Germany
3Universitätsklinikum Essen, Institut für Medizinische Informatik, Biometrie und Epidemiologie (IMIBE), Essen, Germany
4Universitäts-Herzzentrum Freiburg-Bad Krozingen, Klinik für Herz- und Gefäßchirurgie, Freiburg, Germany
5Universitäts-Herzzentrum Thüringen, Klinik für Herz- und Thoraxchirurgie, Jena, Germany
6Westpfalz-Klinikum, Klinik für Thorax-, Herz- und Gefäßchirurgie, Kaiserslautern, Germany
7Herz- und Gefäßklinik Bad Neustadt/Saale, Klinik für Kardiochirurgie, Bad Neustadt an der Saale, Germany
8Universitätsklinikum Schleswig-Holstein, Klinik für Herz- und Gefäßchirurgie, Kiel, Germany
9Universitätsklinikum Münster, Klinik für Herzchirurgie, Münster, Germany
10HELIOS Herzzentrum Leipzig, Klinik für Herzchirurgie, Leipzig, Germany
11Centrum kardiovaskulární a transplantační chirurgie (Center of cardiovascular surgery and transplantations), Brno, Czech Republic
12Universitäres Herzzentrum Hamburg, Klinik und Poliklinik für Herz- und Gefäßchirurgie, Hamburg, Germany
13Universitätsklinikum Gießen und Marburg, Herz-, Kinderherz- und Gefäßchirurgie, Giessen, Germany
14Universitätsmedizin Göttingen, Abteilung für Thorax-,Herz und Gefäßchirurgie, Göttingen, Germany
15Universität Rostock, Klinik und Poliklinik für Herzchirurgie, Rostock, Germany
16Johann Wolfgang-Goethe-Universität, Klinik für Thorax-,Herz- und thorakale Gefäßchirurgie, Frankfurt, Germany
17Medizinische Hochschule Hannover, Klinik für Herz-, Thorax-, Transplantations- und Gefäßchirurgie, Hannover, Germany
18Herz- und Gefäßzentrum Bad Bevensen, Klinik für Herz-Thorax-Chirurgie, Bad Bevensen, Germany
19Universitätsklinikum Essen, Klinik für Thorax und Kardiovaskuläre Chirurgie, Essen, Germany
Abstract
Background
Rationale: Patients with asymptomatic high-grade carotid artery stenosis undergoing coronary artery bypass graft (CABG) surgery are at high risk of perioperative stroke or death. The benefit of synchronous carotid endarterectomy (CEA) in these patients remains controversial. We therefore compared the safety and efficacy of isolated CABG versus synchronous CABG and CEA in patients with asymptomatic high-grade carotid artery stenosis.
Methods
Design: This was an investigator-initiated, randomized, controlled, open, multicenter, group sequential trial with 2 parallel arms and outcome adjudication by blinded observers. Patients with asymptomatic carotid artery stenosis ≥70% according to NASCET criteria scheduled for elective CABG were randomly assigned to either isolated CABG or synchronous CABG and CEA. The composite primary efficacy endpoint was the number of strokes and deaths from any cause within 30 days after operation.
Results
Results: After inclusion of 129 patients, the trial was terminated early due to lack of funding. Mean age was 69.5 years and 17% were women. In the intention-to-treat analysis, the primary endpoint was reached by 12/65 patients in the combined arm (CEA + CABG) and by 6/62 patients in the isolated arm (CABG only) (rate difference 0.0921, confidence interval −0.0303, 0.2145). Ten perioperative strokes occurred in the combined arm and 4 in the isolated arm. After 1 year, any stroke or vascular death had occurred in 14 patients in the combined arm and 7 in the isolated arm.
Conclusions: Discussion: Although the primary endpoint was not significant due to early termination of the trial, the high rate of perioperative stroke in the combined arm does not seem to justify a combined CEA and CABG intervention in these patients.
AS05-002
PREVENTION
Oral
PRESCRIPTION OF ANTIHYPERTENSIVE MEDICATION AT HOSPITAL DISCHARGE IS ASSOCIATED WITH IMPROVED LONG-TERM SURVIVAL POST-STROKE
N. Andrew1, M.F. Kilkenny1, N.A. Lannin2, C.S. Anderson3, G.A. Donnan4, K. Hill5, S. Middleton6, C. Levi7, S. Faux8, R. Grimley9, A.G. Thrift1, J. Kim1, B. Grabsch4 and D. Cadilhac1
1Monash University, Department of Medicine, Clayton, Australia
2La Trobe University, School of Allied Health, Melbourne, Australia
3The University of Sydney, The George Institute for Global Health, Sydney, Australia
4Florey Institute of Neuroscience and Mental Health, Public Health Division, Heidelberg, Australia
5National Stroke Foundation, Clinical Programs, Melbourne, Australia
6St Vincent’s Health and Australian Catholic University, Nursing Research Institute, Sydney, Australia
7University of Newcastle and Hunter Research Institute, Priority Research Centre for Translational Neurosciences Mental Health Research, Newcastle, Australia
8The University of NSW, Faculty of Medicine, Sydney, Australia
9Queensland Health, Statewide Stroke Clinical Network, Brisbane, Australia
Abstract
Background: Prescription of antihypertensive medication at hospital discharge following stroke is recommended for prevention of recurrent stroke and cardiovascular events. We examined differences in the risk and cause of death between patients discharged to the community or rehabilitation who were and were not prescribe antihypertensive medication, following stroke or transient ischaemic attack (TIA).
Methods: We used data from the Australian Stroke Clinical Registry to identify patients with a diagnosis of stroke or TIA, discharged from 44 acute care hospitals. Date and cause of death were determined for eligible patients from the National Death Register. Cox proportional-hazards regression adjusted for patient factors, clinical factors, year and clustering by hospital was used to compare survival at 180-days post-stroke between those who were and were not prescribed antihypertensive medication at discharge.
Results: Survival status was known for all eligible patients admitted in 2009–2014 (n = 20149, median age 75 years, 45% female, 65% ischaemic). Cause of death up to 180-days was determined for those admitted in 2009–2012 (67% cardiovascular cause). At 180-days following stroke patients prescribed antihypertensive medications at discharge (71%) had an overall reduced risk of death (adjusted Hazard Ratio: 0.58, 95%CI: 0.49–0.67), compared to those not prescribed these agents. For registrants where cause of death was known, those prescribed antihypertensive medication had a reduced risk of cardiovascular death (adjusted Hazard Ratio: 0.67, 95%CI: 0.47–0.94) compared to those not prescribed these agents.
Conclusions: Prescribing antihypertensive medication at hospital discharge is associated with improved early survival, possibly through prevention of cardiovascular events, in patients with stroke or TIA.
AS06-011
PREVENTION
Oral
META-ANALYSIS OF INDIVIDUAL PATIENT DATA FROM 5226 ASYMPTOMATIC PATIENTS IN THE ACST-1, ACAS AND VACS TRIALS: IMMEDIATE CAROTID ENDARTERECTOMY VERSUS MEDICAL THERAPY ALONE
A. Halliday1, R. Bulbulia2, D. Morris2, D. de Waard1, H. Pan2, P. Rothwell3, L. Bonati4, R. Peto2 and On behalf of the ACST- ACAS and VA trial collaborators and the carotid stenosis Trialists' collaboration CSTC
1John Radcliffe Hospital, Nuffield Department of Surgical Sciences, Oxford, United Kingdom
2Clinical Trial Service Unit CTSU, Nuffield Department of Population Health- University of Oxford, Oxford, United Kingdom
3John Radcliffe Hospital, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
4University of Basel, Acute Stroke Unit, Basel, Switzerland
Abstract
ACST-1, ACAS and VACS compared carotid endarterectomy (CEA) plus medical therapy versus medical therapy alone for stroke prevention in patients with tight (usually 70–99%) asymptomatic carotid artery stenosis (ACS). ACST-1 is the largest trial, with 3120 patients and 10-years follow-up and allocation to CEA conferred a 50% relative reduction in net stroke risk, despite 3% peri-procedural stroke rate. ACAS (n = 1662) and VACS (n = 444) showed similar trends, but were somewhat under-powered.
Despite evidence in favour of surgical intervention, currently there is a lack of consensus on the management of ACS, driven by a belief that improvements in medical therapy (mainly lipid-lowering therapy and tighter BP control) have reduced risk of carotid-related stroke to such an extent that CEA is no longer justified.
Planned analyses:
Primary outcomes (analysed separately and together): 30-day peri-procedural stroke and death rates (ie, safety endpoint) Non-peri-operative stroke rates (ie, efficacy endpoint)
Secondary outcomes include:
1. Fatal / disabling stroke or perioperative death
Analyses of primary and secondary outcomes for the following subgroups:
1. Gender
2. Age at entry (years): <65, 65–74, ≥75
3. Percentage of stenosis: <70%, 70–79%, 80–89%, ≥90%
4. Prior disease
5. Prior use of anti-thrombotic, anti-hypertensive and lipid-lowering therapy
This meta-analysis including over 5000 patients allows uniquely reliable assessment of the effects of CEA on stroke risk from asymptomatic carotid disease overall, and may identify certain groups of patients in whom intervention is particularly beneficial.
AS05-018
PREVENTION
Oral
CENTRALLY OBSERVED HOME TELEMETRIC MONITORING OF BLOOD PRESSURE TO MANAGE INTENSIVE TREATMENT (COMMIT) STUDY: FEASIBILITY, SAFETY AND INITIAL CONTROL OF BP
N.G. Lovett1, R. Wharton2, S. Lyons2, B. James2, M. Wilson2, F. Cuthbertson2, L. Silver2, A. Webb2, U. Fischer2, L. Tarassenkco2 and P. Rothwell2
1, Oxford, United Kingdom
2Oxford, Stroke Prevention Research Unit, Oxford, United Kingdom
Abstract
Background: Hypertension is a major modifiable risk factor for recurrent stroke, but control in practice is poor. We determined the feasibility and safety of telemetric home BP-monitoring to facilitate intensive BP-control after TIA/stroke.
Methods: We studied consecutive patients with TIA or non-disabling stroke in a population-based study (Oxford Vascular Study). After prescription of initial antihypertensive medication, patients measured their BP (3 times/day) with a Bluetooth-equipped monitor for 1–3 months, depending on control. Measurements transmitted automatically were checked daily on a secure webpage. If BP was consistently above 130/80 or below 100/60 medication was adjusted. BP was measured in clinic at 1 and 3 months follow-up.
Results: Among 1118 participants (mean/SD age = 68.8/13.2 years; 23% ≥80 y), 1097 (98.1%) monitored for ≥7 days and 1053 (96.0%) for ≥1-month. Mean (SD) SBP/DBP was 149.1(24.1)/84.0(13.7) mmHg at entry, falling to 130.7(18.3)/74.2(11.6) at one-month and 126.9(17.5)/72.3(10.6) at three months. BP-lowering medication was initiated/increased at the pre-monitoring assessment in 448 (40.0%) patients and further initiated/adjusted at least once within the first month of home-monitoring in 535 (47.9%) patients and from 1–3 months in 309 (27.6%). 47 falls occurred during the first month of follow up, of which 9 were deemed secondary to hypotension, and 48 and 6 falls respectively occurred from 1–3 months, but there were no resulting fractures or deaths.
Conclusions: Telemetric home BP-monitoring was feasible in patients with TIA/stroke irrespective of age and informed titration of medication in the majority, allowing intensive treatment with little major fall-related morbidity.
AS06-035
PREVENTION
Oral
DIPEPTIDYL PEPTIDASE-4 INHIBITORS AND PROTECTION AGAINST STROKE: A SYSTEMATIC REVIEW AND META-ANALYSIS
H. Milionis1, F. Barkas1, V. Tsimihodimos1 and M. Elisaf1
1School of Medicine- University of Ioannina, Internal Medicine, Ioannina, Greece
Abstract
Background: Type 2 diabetes mellitus (T2DM) is associated with an increased risk of stroke and a unfavorable outcome following stroke. Apart from pioglitaozone, glucose-lowering modalities have not been shown to protect against stroke. Nonetheless, there is evidence from experimental studies of potential neuroprotective effects with dipeptidyl peptidase-4 (DPP-4) inhibitors, especially if treatment starts before stroke.
Aim: To meta-analyze available evidence regarding the risk of stroke in individuals receiving DPP-4 inhibitors.
Methods: We conducted a meta-analysis of randomized, placebo-controlled trials involving DPP-4 inhibitors published until December 2015. Included trials reported at least one stroke with a recruitment rate of at least 100 subjects with T2DM, and a follow-up of ≥12 weeks.
Results: Three multicenter, prospective double-blinded placebo-controlled randomized, clinical trials (mRCTs) assessing cardiovascular outcomes as primary endpoint (SAVOR TIMI-53, EXAMINE and TECOS) with a total of 36,543 diabetic subjects, along with 19 small RCTs evaluating the efficacy and safety of gliptins (n = 9,047) were meta-analysed separately. The pooled analysis of the small prospective trials showed a trend towards a benefit from DDT-4 inhibitors against stroke (OR: 0.640, 95% CI: 0.348–1.177, p = 0.151). The analysis of mRCTs did not showed any difference in the risk of stroke compared with placebo in T2DM patients [odds ratio (OR): 1.032, 95% confidence interval (CI): 0.890–1.197, p = 0.674)].
Conclusions: The promising data from experimental studies regarding gliptin-associated protective effects against stroke are not supported by available data from clinical trials.
AS04-007
PREVENTION
Oral
RISK OF STROKE OR DEATH OCCURRING ON THE DAY OF PROCEDURE VERSUS DAY 1-30 AFTER PROCEDURE IN ENDARTERECTOMY OR STENTING FOR SYMPTOMATIC CAROTID STENOSIS
M. Müller1, S. Von Felten2, A. Algra3, J.P. Becquemin4, M. Brown5, R. Bulbulia6, D. Calvet7, H.H. Eckstein8, G. Fraedrich9, A. Halliday10, J. Hendrikse11, G. Howard12, O. Jansen13, G.S. Roubin14, J.L. Mas7, T.G. Brott15, P.A. Ringleb16, L.H. Bonati1,5
1University Hospital Basel, Department of Neurology and Stroke Center, Basel, Switzerland
2University Hospital Basel, Clinical Trial Unit, Basel, Switzerland
3University Medical Center Utrecht, Department of Neurology and Neurosurgery, Utrecht, Netherlands
4University of Paris XII- Hôpital Henri Mondor, Vascular Surgery, Paris, France
5University College London, Department of Brain Repair and Rehabilitation, London, United Kingdom
6Oxford University, Clinical Trial Service Unit and Epidemiological Studies Unit, Oxford, United Kingdom
7Université Paris-Descartes- Hôpital Sainte-Anne, Department of Neurology, Paris, France
8Klinikum rechts der Isar der Technischen Universität München, Department of Vascular and Endovascular Surgery- Vascular Center, München, Germany
9Medical University of Innsbruck, Department of Vascular Surgery, Innsbruck, Austria
10John Radcliffe Hospital, Nuffield Department of Surgical Sciences, Oxford, United Kingdom
11University Medical Center Utrecht, Department of Radiology, Utrecht, Netherlands
12UAB School of Public Health, Department of Biostatistics, Birmingham, USA
13UKSH Campus Kiel, Clinic for Radiology and Neuroradiology, Kiel, Germany
14Cardiovascular Associates of the Southeast, Cardiovascular Care, Birmingham, USA
15Mayo Clinic, Department of Neurology, Jacksonville, USA
16University of Heidelberg Medical School, Department of Neurology, Heidelberg, Germany
Abstract
Background: Stenting for symptomatic carotid stenosis (CAS) carries a higher risk of procedural stroke or death than endarterectomy (CEA). It is unclear whether this extra risk is present both on the day of procedure and within 1–30 days thereafter and whether clinical risk factors differ between these periods.
Methods: We analysed procedural risk in 4599 individual patients with symptomatic carotid stenosis who underwent CAS (n = 2327) or CEA (n = 2272) in four randomised trials.
Results: Compared with CEA, patients treated with CAS more often had a stroke or died on the day of procedure (110 versus 41 events, 4.7% versus 1.8%; OR 2.7, 95% CI 1.9–3.9), but not between 1 and 30 days after the procedure (56 versus 46 events, 2.4% versus 2.0%, OR 1.2, 0.8–1.7; interaction p = 0.003). In patients treated with CAS, age increased and smoking history decreased the risk of stroke or death, both occurring on the day of procedure and within 30 days thereafter. In patients treated with CEA, higher level of disability at baseline was associated with stroke or death 1–30 days after the procedure. None of these risk factor associations differed significantly between time periods.
Conclusions: The increased 30-day stroke or death risk associated with CAS compared with CEA was caused by an excess in events occurring on the day of procedure. These events may potentially be prevented by operator skill and technical or medical advances. Higher age increased the risk for both immediate and delayed procedural events in CAS, mechanisms of which remain to be elucidated.
AS06-040
PREVENTION
Oral
A CURRENT ESTIMATION OF THE EARLY RISK OF STROKE AFTER TRANSIENT ISCHEMIC ATTACK: A SYSTEMATIC REVIEW AND META-ANALYSIS OF RECENT INTERVENTION STUDIES
F. Purroy1, J. Valls2, M. Peiro-Chamarra1, S. Cambray1, J. Molina-Seguin2 and I. Benabdelhak2
1Biomedical Research Institute of Lleida, Clinical Neuroscience Group, Lleida, Spain
2Biomedical Research Institute of Lleida, Biostatistics and Epidemiology Unit, Lleida, Spain
Abstract
Background: Recent studies have demonstrated the decrease in the risk of subsequent stroke after transient ischemic attack (TIA) when urgent care (UC) is applied. However no meta-analysis has been developed with contemporaneous TIA studies.
Methods: We searched for studies, without language restriction, from January 2007 to January 2015 according to PRISMA guidelines. We included studies with TIA patients who underwent UC and reported the proportion of stroke recurrence (SR) at 90 days. We performed both fixed and random effects meta-analyses to determine SR and assess sources of heterogeneity.
Results: We selected 14 papers including 10,250 patients. We excluded studies with less than 100 patients and cohorts including both stroke and TIA patients. The pooled stroke risk was 3.13% (95% CI 2.81–3.49) at 90 days and 2.05% 95% CI 1.75–2.39) at 7 days. Although we did not find statistically significant heterogeneity in SR among studies, those with a higher proportion of patients with motor weakness and ABCD2 > 4 had a significantly higher risk of SR. However, TIA clinic management studies showed similar SR to other strategies.
Conclusions: The risk of SR after TIA is low when any urgent care strategy is applied despite the rate of hospitalization
AS04-011
PREVENTION
Oral
FARMALARM: APP FOR MOBILE DEVICES IMPROVES RISK FACTOR CONTROL AFTER STROKE
E. Montiel1, M. Rubiera1, E. Sanjuan1, M. Sanchis1, D. Rodriguez-Luna1, J. Pagola1, S. Boned1, J.M. Juega1, M. Muchada1, C. Molina1 and M. Ribo1
1Hospital Vall d'Hebron, Stroke Unit. Neurology, Barcelona, Spain
Abstract
Background: Risk factor control and treatment compliance the following months after stroke are often poor. We aim to validate an application for smartphones designed to raise awareness about the need to perform healthy lifestyle changes.
Methods: Farmalarm is an app that offers: medication visual alerts and compliance control, chat with medical staff, sharing videos, exercise monitoring… Patients discharged home were screened for participation and divided in two groups: follow Farmalarm program or standard of care follow-up. We determined risk factor control goals at 90 days in all patients.
Results: During 12 months, from 336 patients discharged home, 102(30.4%) were included: Farmalarm n = 52, age:56 ± 12, Control n = 50, age:59 ± 11. There were no significant differences in baseline characteristics between groups. Patients in Farmalarm followed the program for 23,5 ± 5,7 days after discharge. At 90 days, achievement of risk factor control was higher in Farmalarm(table). Rate of patients with ≥2 risk factors under control was higher in Farmalarm (81.6% Vs 42.3%;p = 0.02). The regression model adjusted for age and gender showed that the only variable independently associated with ≥2 risk factors under control at 90 days was the use of Farmalarm (OR: 6.3; 95% CI:2–20; p = 0.02).
Conclusions: In stroke patients discharged home the use of applications to monitor medication compliance and increase stroke awareness is feasible and seems to improve the control of vascular risk factors.
Farmalarm
Control
p
SystolicBP < 120 mmHg
31.1%
24.2%
0.05
DyastolicBP < 75 mmHg
36.6%
15.2%
0.02
Total cholesterol < 175 mg/dl
78%
55.6%
0.04
Non-active smoker
93.6%
68.6%
<0.01
To name 3 risk factors
100%
85.3%
<0.01
Exercise
63.8%
38.2%
0.02
AS06-045
PREVENTION
Oral
PERCUTANEOUS TRANSLUMINAL ANGIOPLASTY AND STENTING FOR SYMPTOMATIC INTRACRANIAL ARTERIAL STENOSIS: A SYSTEMATIC REVIEW AND META-ANALYSIS
A. Katsanos1,2, G. Magoufis3, O. Kargiotis3, A. Safouris1,3, C. Zompola1, G. Papadimitropoulos1, S. Triantafyllou1, E. Stamboulis3, A. Alexandrov4, G. Tsivgoulis1,4
1School of Medicine - University of Athens, Second Department of Neurology, Athens, Greece
2School of Medicine University of Ioannina, Department of Neurology, Ioannina, Greece
3Metropolitan Hospital, Stroke Unit, Piraeus, Greece
4University of Tennessee Health Science Center, Department of Neurology, Memphis, USA
Abstract
Background: The cumulative safety and efficacy measures of percutaneous transluminal angioplasty and stenting (PTAS) for secondary prevention of ischemic stroke (IS) patients with symptomatic intracranial arterial stenosis (SIAS) has not been evaluated using a meta-analytical approach.
Methods: We conducted a systematic review and random effects meta-analysis of all available randomized controlled trials (RCTs) evaluating the safety and efficacy of PTAS (in comparison to medical therapy) for SIAS.
Results: Three RCTs (677 IS patients) were included in the quantitative analysis. PTAS was associated with higher risk of recurrent stroke (ischemic or hemorrhagic) within 30-days and 1 year (Table). PTAS was related to a higher risk of IS in the territory of qualifying artery within 1 year from the index event (Table). The composite outcome of any stroke or death within 1 and 2 years was higher in PTAS than in medical therapy and this association also persisted for posterior circulation SIAS (Table).
Conclusions: PTAS is associated with adverse early and long-term outcomes and should not be recommended in IS patients with SIAS.
AS04-021
PREVENTION
Oral
EFFECT OF BODY MASS INDEX ON RISK OF STROKE AND DEATH AFTER CAROTID REVASCULARIZATION FOR SYMPTOMATIC CAROTID ARTERY STENOSIS
E. Volkers1,2, J. Greving2, J. Hendrikse3, A. Algra1,2, J. Kappelle1, J.P. Becquemin4, T. Brott5, L. Bonati6,7, R. Bulbulia8, D. Calvet9, H.H. Eckstein10, G. Fraedrich11, A. Halliday12, G. Howard13, O. Jansen14, G. Roubin15, J.L. Mas9, M. Brown7 and P.A Ringleb16
1UMC Utrecht, Department of Neurology and Neurosurgery- Brain Centre Rudolf Magnus, Utrecht, Netherlands
2UMC Utrecht, Julius Centre for Health Sciences and Primary Care, Utrecht, Netherlands
3UMC Utrecht, University Department of Radiology, Utrecht, Netherlands
4University of Paris- XII- Hôpital Henri Mondor, Vascular Surgery, Créteil, France
5Mayo Clinic, Department of Neurology, Jacksonville- FL, USA
6University Hospital Basel, Department of Neurology and Stroke Centre, Basel, Switzerland
7UCL Institute of Neurology- University College London, Department of Brain Repair and Rehabilitation, Londen, United Kingdom
8Oxford University, Clinical Trial Service Unit and Epidemiological Studies Unit, Oxford, United Kingdom
9Hôpital Sainte-Anne- Université Paris-Descartes, Department of Neurology, Paris, France
10Klinikum rechts der Isar der Technischen Universität München, Department of Vascular and Endovascular Surgery/Vascular Center, Munich, Germany
11Medical University of Innsbruck, Department of Vascular Surgery, Innsbruck, Austria
12John Radcliffe Hospital, Nuffield Department of Surgical Sciences, Oxford, United Kingdom
13UAB School of Public Health, Department of Biostatistics, Birmingham- AL, USA
14UKSH Campus Kiel, Clinic for Radiology and Neuroradiology, Kiel, Germany
15Cardiovascular Associates of the Southeast, Cardiovascular Associates of the Southeast, Birmingham- AL, USA
16University of Heidelberg Medical School, Department of Neurology, Heidelberg, Germany
Abstract
Background: Overweight or obese patients with symptomatic atherosclerosis had a better prognosis in previous studies. We determined whether the obesity paradox exists in patients who undergo carotid artery stenting (CAS) or carotid endarterectomy (CEA) for symptomatic carotid artery stenosis.
Methods: We combined individual patient data from three randomised trials (EVA-3S, ICSS, and SPACE). Baseline BMI was available for 1969 patients and classified into four groups: <20, 20–25, 25–30, and ≥30 kg/m2. Primary outcome was all strokes or death, investigated separately for the periprocedural and postprocedural period (≤120 days vs. >120 days after randomisation); this outcome was compared between different BMI strata in CAS and CEA patients, and in the total group of patients. We performed intention-to-treat Cox regression analyses with adjustment for vascular risk factors.
Results: Median follow-up was 2.0 years. Stroke or death occurred in 157 patients in the periprocedural period (cumulative risk 8.0%) and in 270 patients in the postprocedureal period (risk rate 4.8/100 person-years). BMI did not affect periprocedural risk of stroke or death for patients assigned to CAS (ptrend = 0.87) or CEA (ptrend = 0.65), nor for the total group (ptrend = 0.62). Within the total group, patients with BMI ≥25 had a lower postprocedural risk of stroke or death than patients with BMI 20–25 (BMI ≥25 vs. BMI 20–25; adjusted Hazard Ratio (HR) 0.73; 95% confidence interval (CI) 0.56–0.93).
Conclusions: BMI is not associated with periprocedural risk of stroke or death; BMI ≥25 is associated with lower postprocedural risk than BMI 20–25. These observations were similar for CEA and CAS.
AS10-003
REHABILITATION
Oral
THE QUALITY OF STROKE CARE AFTER PATIENTS LEAVE HOSPITAL: THE FIRST NATIONAL SURVEY OF REHABILITATION SERVICE AVAILABILITY AND ORGANISATION THROUGHOUT ENGLAND, WALES AND NORTHERN IRELAND
R. Andrews1, G. Cloud2, M. James3, P. Tyrell4, B. Bray5, A. Hoffman1, L. Paley1, M. Kavanagh1, A. Rudd6 and O.B.O. the SSNAP Collaboration
1
1Royal College of Physicians, CEEu, London, United Kingdom
2St George's University Hospitals NHS Foundation Trust, St George's University Hospitals NHS Foundation Trust, London, United Kingdom
3Royal Devon and Exeter NHS Foundation Trust, Royal Devon and Exeter NHS Foundation Trust, Exeter, United Kingdom
4University of Manchester, University of Manchester, Manchester, United Kingdom
5King's College London, Division of Health and Social Care Research, London, United Kingdom
6Guy's and St Thomas NHS Foundation Trust, Guy's and St Thomas NHS Foundation Trust, London, United Kingdom
Abstract
Background: People with stroke report feeling neglected after the acute phase of care, but little is known, in any European country, about the quality and availability of rehabilitation services for stroke patients after they leave hospital. The Sentinel Stroke National Audit Programme (SSNAP) carried out the first national survey to describe the availability of rehabilitation services throughout England, Wales and Northern Ireland.
Methods: 756 services were identified as providing rehabilitation after hospital. Data was collected from 604 (80%) of these between April and May 2015 using a secure web-based tool and audit date of 1st April 2015. Data included location and type of service, waiting times for treatment, staffing, intensity and duration of treatment, and the provision of post stroke reviews.
Results: There is wide variation across the UK in how these services are organised and some important areas for improvement were identified. Psychological support services had median waiting times to treatment of 10 weeks, five times that of physical support services, with a quarter exceeding 20 weeks. 40% of Early Supported Discharge services were not able to treat patients within 24 hours of leaving hospital. Very few nurses (median of 0 per 10 stroke beds) treating stroke patients within community-based hospitals had been trained in swallow screening.
Conclusions: Rehabilitation is a vital, but often neglected, part of the stroke care pathway and is essential in ensuring a good outcome from stroke. Quality improvement in stroke care should focus not just on acute care but on improving the quality and availability of rehabilitation services.
AS03-001
REHABILITATION
Oral
A RANDOMIZED CONTROLLED TRIAL ASSESSING THE EFFECT OF A LONG-TERM FOLLOW-UP PROGRAMME AIMING TO MAINTAIN MOTOR FUNCTION AFTER STROKE: THE LIFE AFTER STROKE (LAST) STUDY
T. Askim1, B. Langhammer2, I.H. Hege3, G. Mari4, L. Stian5 and I. Bent4
1Norwegian University of Science and Technology, Trondheim, Norway
2Oslo and Akershus University College of Applied Science, Department of Physiotherapy, Oslo, Norway
3Vestre Viken- Bærum Hospital, Stroke Unit, Bærum, Norway
4Norwegian University of Science and Technology, Department of Neuroscience, Trondheim, Norway
5Norwegian University of Science and Technology, Regional Centre for Child and Youth Mental Health and Child Welfare, Trondheim, Norway
Abstract
Background: The LAST study intended to prevent functional decline after stroke. Our primary hypothesis was that monthly coaching by a physiotherapist for 18 months in addition to standard care would be superior to standard care only in preventing decline in motor function.
Methods: This was a multi-site RCT with blinded assessment 18 months after inclusion. Main inclusion criteria were; 0–4 points on modified Rankin Scale (mRS), >20 points on Mini-Mental State Examination and community dwelling. Patients were recruited and randomised, 10–16 weeks post stroke, to an intervention group encouraged by a physiotherapist to do at least 30 minutes of daily physical activity and 60 minutes of motor training every week in addition to standard care, or to a control group receiving standard care according to guidelines. The primary outcome was Motor Assessment Scale at 18 months follow-up. Secondary outcomes were among others; adherence, dependency, quality of life and health costs.
Results: Data were collected from October 2012 until December 2015. A total of 1522 patients were screened for inclusion and 384(25%) were included. Out of these, 279(73%) were <80 years and 305(79%) were independent (mRS < 3). A total of 318 patients were assessed at 18 months, 15(4%) patients died while 51(13%) were lost to follow-up. Primary results will be published for the first time at ESOC2016.
Conclusions: This is the first randomised controlled trial to assess the effect of regularly coaching of patients for 18 months after stroke. The results will have impact on future guidelines for individualized rehabilitation of stroke patients.
AS02-003
REHABILITATION
Oral
VERY EARLY STROKE REHABILITATION SAFETY IN THE FIRST 14 DAYS
H. Dewey1, A.G. Thrift2, P. Langhorne3, R.I. Lindley4, P.M. Bath5, C. Bladin6, C.M. Reid7, S. Read8, C. Said9, S. Middleton10, J. Frayne11, V. Srikanth2, L. Churilov12, J.M. Collier13, G.A. Donnan14, J. Bernhardt13 and on behalf of the AVERT Trial Collaboration group
13
1Monash University, Medicine Nursing and Health Sciences, Box Hill, Australia
2Monash University, Medicine, Clayton, Australia
3University of Glasgow, Cardiovascular and Medical Sciences, Glasgow, United Kingdom
4University of Sydney, Westmead Hospital Clinical School, Sydney, Australia
5City Hospital, Stroke Medicine, Nottingham, United Kingdom
6Box Hill Hospital, Medicine, Box Hill, Australia
7Monash University, Clinical Informatics and Data Management Unit, Clayton, Australia
8Royal Brisbane and Womens Hospital, Stroke, Brisbane, Australia
9Austin Health, Physiotherapy Research, Heidelberg, Australia
10St Vincents and Mater Health, Nursing Research Unit, North Sydney, Australia
11Cabrini Hospital, Neurology, Malvern, Australia
12The Florey Institute of Neuroscience & Mental Health, Mathematics and Statistics, Heidelberg, Australia
13The Florey Institute of Neuroscience & Mental Health, Stroke Division, Heidelberg, Australia
14The Florey Institute of Neuroscience & Mental Health, Head, Parkville, Australia
Abstract
Background: In the international trial AVERT (A Very Early Rehabilitation Trial), patients commencing intensive out-of-bed activity within 24 hours of stroke (intervention) showed less favourable outcome (mRS0–2) compared to usual care (UC), but no significant differences in death or serious adverse events (SAEs) at 3 months. We now report the pre-specified safety analysis of deaths and SAEs during the first 14 days (intervention period).
Methods: All deaths and SAEs were independently adjudicated by blinded clinical experts and classified as stroke related, immobility related, falls or other. 14 day outcomes: deaths and numbers of non-fatal SAEs for individual patients adjusted for age and stroke severity, with pre-specified subgroup analyses, and time to death at 14 days were compared using appropriate regression models.
Results: 2104 patients were recruited, 80 died within 14 days. Patients who died were older (age median (IQR): 80.2 (73.0–84.0) v 72.2 (64.6–80.0), p < 0.001) and had more severe strokes (NIHSS median (IQR): 21 (16–24) v 6 (4–11), p < 0.001). More intervention patients (48/1048, 4.5%) died than UC (32/1050, 3.0%); adjusted Odds Ratio [aOR] 1.76, 95% CI 1.06–2.92, p = 0.029) with deaths earlier (aHR 1.59 95% CI 1.01–2.48, p = 0.044). Death was most commonly associated with stroke progression or recurrence (29/48 intervention; 16/32 UC). Intervention patients aged >80 (OR 2.38, 95% CI 1.12–5.08) and with haemorrhagic stroke (OR 4.17, 95% CI 1.06–16.43) had greater odds of death. No significant differences in non-fatal SAEs were found.
Conclusions: Although deaths and SAEs rates were low overall, intervention patients had increased odds of death compared to UC.
AS26-002
REHABILITATION
Oral
SUB-CORTICAL INFARCTS AND THE RISK OF FALLS IN OLDER PEOPLE: COMBINED RESULTS OF TASCOG AND SYDNEY MAS STUDIES
M. Callisaya1,2, V. Srikanth1,2, S. Lord3, J. Close4, H. Brodaty5, P. Sachdev5, P. Thanh2, R. Beare2, J. Troller5, J. Zheng3, W. Wen5 and K. Delbaere3
1University of Tasmania, Menzies Institute of Medical Research, Hobart, Australia
2Monash University, Medicine, Clayton, Australia
3NeuRA Medical Research Unit, Falls and Balance Research Group, Sydney, Australia
4NeuRA Medical Research Unit, Falls and Injury Prevention Group, Sydney, Australia
5University of NSW, School of Psychiatry, Sydney, Australia
Abstract
Background: White matter hyperintensities (WMH) increase the risk of multiple falls, but the effect of sub-cortical infarcts is unknown. We aimed to investigate the association between sub-cortical infarcts and multiple falls and whether this relationship, and that of WMH, is mediated or modified by cognitive or sensorimotor factors.
Methods: Participants from two Australian population-based studies underwent magnetic resonance imaging, cognitive and sensorimotor assessments. Falls were measured over 12 months. Sub-cortical infarcts were detected visually. WMH volume was quantified using automated segmentation. Generalized linear models were used to examine if sub-cortical infarcts and WMH increased falls risk.
Results: The mean age of the sample (n = 655) was 74.5 (SD 6.7) years. Seventeen percent had multiple falls. The majority had no sub-cortical infarcts (n = 491, 75%), 90 had one (14%), 41 had two (6%), and 33 had three or more (5%). The risk of multiple falls was increased in those with 3 or more sub-cortical infarcts (ARR 1.89, 95% CI 1.03, 3.46) and in the highest quarter of WMH volume (ARR 1.46, 95% CI 1.00, 2.13). The effect of sub-cortical infarcts on falls was amplified by poorer vision (P = 0.03). The effect of WMH was amplified by poorer vision (P = 0·008), proprioception (P = 0.03), and muscle strength (P = 0.008).
Conclusions: Increasing burdens of sub-cortical infarcts and WMH are associated with a risk of falling. Interventions targeting sensorimotor factors along with strategies to prevent sub-cortical infarcts and WMH may reduce the risk of falls.
AS24-014
REHABILITATION
Oral
QUALITATIVE FINDINGS FROM A RANDOMIZED CONTROLLED TRIAL OF THE TIMING IT RIGHT STROKE FAMILY SUPPORT PROGRAM
J.I. Cameron1, G. Naglie2, M. Gignac3, M. Bayley4, G. Warner5, T. Green6, M. Huijbregts7, F. Silver8, S. Phillips9, A. Cheung10 and A. Czerwonka1
1University of Toronto, Occupational Science and Occupational Therapy, Toronto, Canada
2Baycrest Health Sciences, Geriatrics, Toronto, Canada
3University of Toronto, Institute of Work and Health, Toronto, Canada
4Toronto Rehabilitation Institute - UHN, Neurology, Toronto, Canada
7Family Service Toronto, Research, Toronto, Canada
8University Health Network, Neurology, Toronto, Canada
9Dalhousie University, Neurology, Halifax, Canada
10University Health Network, Women's Health, Toronto, Canada
Abstract
Background: Family members who provide care to people who have had a stroke need support. We developed the Timing it Right Stroke Family Support Program to address carers changing needs as people with stroke move from acute care, through rehabilitation, and return to community living. The objective of this qualitative study was to explore carers’ experiences with support received.
Methods: In the context of a mixed method multi-site randomized controlled trial, we conducted qualitative interviews with carers in each of three intervention arms, 1) full intervention delivered by a stroke support person; 2) self-directed intervention; and 3) standard care, at the completion of a 12-month follow-up assessment. Interviews explored carers’ needs for support and how the support they received in the context of the study was perceived. Framework analysis was used to compare carers’ support experiences across intervention arms and the influence of time on their needs.
Results: Interviews were completed with 39 carers representing the full (n = 15), self-directed (n = 11), and standard care (n = 13) interventions. Four themes were identified: 1) Variability in personal characteristics influenced carers’ needs for or use of external supports; 2) Variability in carers’ insight informed their engagement in support; 3) Variability in availability and consistency of support; and 4) Experience of intervention delivery not being part of standard care.
Conclusions: Findings suggest situations where carers are more likely to need support and highlight challenges associated with testing a carer intervention in a randomized controlled trial. Future intervention research should target carers in need of support and consider alternate evaluation approaches.
AS06-013
REHABILITATION
Oral
CONTROLLED CLINICAL TRIALS OF CELL THERAPY IN STROKE: META-ANALYSIS AT 6 MONTHS AFTER TREATMENT
O. Detante1, M. Hommel2 and A. Jaillard3
1Grenoble Alpes Hospital, Neurology, GRENOBLE, France
2Grenoble Alpes Hospital, Research Department, GRENOBLE, France
3Grenoble Alpes Hospital, 3T-MRI Research Unit- Department of Neuroradiology, GRENOBLE, France
Abstract
Background: Despite major progresses in stroke care, most of patients are left with disability. In animal studies, cell therapy appears to be beneficial. However, this literature is potentially confounded by poor study quality and publication biases. To evaluate the potential benefit of regenerative cell therapy in humans, we conducted a meta-analysis in trials including a control group and assessed clinically six months after cell administration.
Methods: We checked published reports in English (1995-October 2015) and congress reports. Quality was evaluated using GRADE approach. Quantitative analysis was based on a standardized means difference (SMD) method. Publication biases were assessed with funnel plot and pre-specified explanatory variables were tested with a meta-regression.
Results: Among 21 published trials, nine studies (194 patients and 191 controls) were eligible. The GRADE-quality was evaluated as moderate. Cell therapy had a positive effect on outcome SMD 0.57 (95%CI 0.22–0.92; p = 0.002). Sensitivity analysis showed an upper level of effect size of 0.81 (95%CI 0.34–1.27; p = 0.001) and a lower level effect size of 0.455 (95%CI 0.04–0.87; p = 0.03). The significant heterogeneity test was not explained by publication biases (p = 0.09) and was more likely explained by methodological and quality differences between studies. None of the pre-specified explanatory variable (age, ratio infarction/hemorrhage, delay from stroke, administration route, cell type, randomization, blinded outcome) was significantly correlated to clinical outcome.
Conclusions: Cell therapy may be beneficial after stroke. Due to limited sample sizes, small number of controlled studies and moderate quality of studies, these results should be considered as preliminary. However, they are encouraging for running larger trials.
AS10-044
REHABILITATION
Oral
INCIDENCE OF VISUAL IMPAIRMENT FOLLOWING STROKE
F. Rowe1, L. Hepworth1, K. Hanna1 and C. Howard2
1University of Liverpool, Health Services Research, Liverpool, United Kingdom
2Salford Royal NHS Foundation Trust, Orthoptics, Manchester, United Kingdom
Abstract
Background: Incidence of post-stroke visual impairment is currently unknown. We report our annual incidence of visual impairment in an acute adult stroke population.
Methods: A prospective, epidemiology study was conducted from 1.6.14 to 30.6.15 across 3 stroke units. All stroke admissions were identified by stroke research nurses. Deaths were coded. The orthoptic research team assessed all remaining patients on the stroke unit. Patients who could not be assessed were coded for reasons why. The remaining patients had assessment of visual acuity, visual fields, ocular alignment, ocular motility, visual inattention and visual perception.
Results: There was no significant difference across recruiting sites for general demographics so data were pooled. There were 51% males and 49% females, mean age of 73.4 (SD 13.8) years and 87% ischaemic strokes. 1289 patients were recruited: 144 died before assessment and 148 could never be assessed. Overall we assessed and diagnosed 997 patients. Over half were assessed at baseline. 574 could not be assessed at baseline so were reviewed at visit 1 (median 3 days later). Two thirds were assessed with diagnosis within 1 month and the majority within 2 months. 251/997 (25.2%) had normal eye exams. 746/997 (74.8%) had visual impairment: 63% with impaired central vision, 43.8% with eye movement abnormalities, 28.7% with visual field loss, 27.8% with visual inattention and 3.8% with visual perceptual disorders.
Conclusions: The incidence of post-stroke visual impairment in adult stroke survivors is 75%. This is higher than previous reports, and highlights the need for integration of visual assessment as a core post-stroke assessment.
AS03-028
REHABILITATION
Oral
COGNITIVE, EMOTIONAL AND NEURAL BENEFITS OF MUSIC ON STROKE RECOVERY
T. Särkämö1, V. Leo1, A. Sihvonen1,2, P. Ripollés3,4, A. Rodríguez-Fornells3,4, M. Tervaniemi1,5 and S. Soinila6
1University of Helsinki, Cognitive Brain Research Unit- Institute of Behavioural Sciences, Helsinki, Finland
2University of Turku, Faculty of Medicine, Turku, Finland
3L’Hospitalet de Llobregat, Cognition and Brain Plasticity Group- Bellvitge Biomedical Research Institute, Barcelona, Spain
4University of Barcelona, Department of Basic Psychology, Barcelona, Spain
5University of Helsinki, CICERO Learning Network, Helsinki, Finland
6University of Turku and Turku University Hospital, Department of Neurology, Turku, Finland
Abstract
Background: During the last decade, advances in cognitive neuroscience have shown that music is a rich and versatile stimulus for the human brain, engaging a wide-scale bilateral network of cortical and subcortical regions. By combining cognitive-motor stimulation and enjoyable and rewarding action, music is a highly promising tool for neurological rehabilitation after stroke. We have investigated the cognitive, emotional, and neural efficacy of music listening on stroke recovery in two RCTs, which we will present here.
Methods: The first parallel-group RCT in acute middle cerebral artery stroke patients (N = 60) compared daily music listening to audio book listening and standard care. In a 6-month follow-up, the patients underwent neuropsychological testing, questionnaires, and MEG and MRI measures. Using a similar design with additional fMRI and hormonal measures, the second RCT (N = 50, data collection complete in April 2016) compares daily listening to sung music, instrumental music, and audio books to determine the specific role of singing in music.
Results: In the first RCT, daily music listening during the first two post-stroke months was found to improve the recovery of verbal memory and focused attention and alleviate depressed and confused mood. Using MEG and voxel-based morphometry, these behavioural gains were linked functionally to enhanced early auditory encoding in frontotemporal areas and structurally to increased grey matter volume in perilesional frontolimbic regions. Data analysis of the second RCT is currently in progress, and preliminary results will be presented.
Conclusions: Music listening provides an easily applicable and cost-efficient way to promote stroke recovery with long-term efficacy.
AS03-029
REHABILITATION
Oral
DETERMINANTS OF QUALITY OF LIFE AFTER INTRA-ARTERIAL TREATMENT FOR ACUTE ISCHEMIC STROKE IN THE MR CLEAN TRIAL
J. Schreuders1, L.A. van den Berg2, P.S.S. Fransen1, O.A. Berkhemer3, D. Beumer4, R.J. van Oostenbrugge4, W.H. van Zwam5, C.B.L.M. Majoie3, A. van der Lugt6, P.L.M. de Kort7, Y.B.W.E.M. Roos2 and D.W. Dippel1
1Erasmus University Medical Center, Neurology, Rotterdam, Netherlands
2Academic Medical Center Amsterdam, Neurology, Amsterdam, Netherlands
3Academic Medical Center Amsterdam, Radiology, Amsterdam, Netherlands
4Maastricht University Medical Center, Neurology, Maastricht, Netherlands
5Maastricht University Medical Center, Radiology, Maastricht, Netherlands
6Erasmus University Medical Center, Radiology, Rotterdam, Netherlands
Background: The EuroQol group 5-dimension self-report questionnaire (EQ-5D) is the most often used standardized instrument to assess health-related quality of life in stroke patients. Patient-reported outcome measures may be less sensitive to treatment effects in RCTs. The purpose of this study was to assess and compare the impact of neurological deficits, including those that may not be perceived as a hindrance by patient or proxy on quality of life after stroke and their relation with treatment effect.
Methods: The EQ-5D-3L questionnaire items were reported by the patient or proxy at 3 months after treatment. We used the Dutch tariff to derive a utility value from the 5 category scores. The association of neurological deficits at 1 week with EQ-5D-3L was assessed with multiple linear regression models.
Results: Of the 500 trial patients, 457 (91.4%) completed the EQ-5D-3L questionnaire. The mean EQ-5D-3L score in the 240 controls was 0.41, and 0.48 in the intervention group (p = 0.03). Severe dysarthria was the strongest predictor of the EQ-5D-3L score (−0.47, 95% CI: −0.54 to −0.39, R2 = 0.27), stronger than severe hemiplegia (−0.31, 95% CI: −0.41 to −0.20, R2 = 0.11), severe aphasia (−0.16, 95% CI: −0.26 to −0.06, R2 = 0.12) and hemineglect (−0.22, 95% CI: −0.33 to −0.12, R2 = 0.08). Mild aphasia had a positive association with EQ-5D-3L. There was no interaction with treatment effect.
Conclusions: Neurological impairment involving higher cortical functions does not affect quality of life as much as might be expected. This may be one explanation for a lower sensitivity of EQ-5D to treatment effects in acute ischemic stroke.
AS13-015
RISK FACTORS FOR STROKE
Oral
MEASURES OF WHITE MATTER INTEGRITY IMPROVE PREDICTION OF STROKE IN THE GENERAL POPULATION
T. Evans1,2,3, M. O'Sullivan2, M. de Groot3,4,5, W. Niessen3,4,6, A. Hofman1, G. Krestin3, A. van der Lugt3, M. Portegies1,5, P. Koudstaal5, D. Bos1,3, M. Vernooij1,3, A. Ikram1,5
1Erasmus MC, Department of Epidemiology, Rotterdam, Netherlands
2Kings College London, Department of Basic and Clinical Neuroscience, London, United Kingdom
3Erasmus MC, Department of Radiology, Rotterdam, Netherlands
4Erasmus MC, Department of Medical informatics, Rotterdam, Netherlands
5Erasmus MC, Department of Neurology, Rotterdam, Netherlands
6Delft University of Technology, Imaging Science and Technology, Delft, Netherlands
Abstract
Background: The presence of subclinical vascular brain disease, including white matter lesions and lacunar infarcts, substantially increases the risk of clinical stroke. White matter microstructural integrity is considered an earlier and potentially better marker of the total burden of vascular brain disease. Yet, its association with risk of stroke remains unknown.
Methods: From the population-based Rotterdam Study, 4,259 stroke-free participants (mean age 63.6 years, 55.6 % women) underwent brain MRI between 2006 and 2011 to quantify markers of white matter microstructural integrity (fractional anisotropy (FA) and mean diffusivity (MD)). Next, all participants were followed for occurrence of stroke until 2013. We used Cox proportional hazards models to associate markers of white matter microstructural integrity with risk of stroke. Finally, we assessed the predictive value of markers of white matter microstructural integrity for stroke beyond the predictors in the Framingham Stroke Risk Profile.
Results: During 18,476 person-years of follow-up, 58 persons suffered a stroke. We found that both FA and MD increased risk of stroke, independent of age, sex, cardiovascular risk factors, white matter lesion volume, and presence of lacunar infarcts [hazard ratio (HR) per SD increase in FA: 0.75(95% confidence interval (CI): 0.57–0.98), and HR per SD increase in MD: 1.50 (95%CI:1.08–2.09)]. MD improved stroke prediction beyond the Framingham Stroke Risk Profile [Continuous net reclassification improvement: 0.52 (95%CI: 0.24–0.81)].
Conclusions: Our findings suggest that worse white matter microstructural integrity increases the risk of stroke and yields unique information with regard to prediction of stroke in addition to the Framingham Stroke Risk Profile.
AS16-023
RISK FACTORS FOR STROKE
Oral
PARACETAMOL, IBUPROFEN, AND RECURRENT MAJOR CARDIOVASCULAR AND MAJOR BLEEDING EVENTS IN 19,120 PATIENTS WITH RECENT ISCHAEMIC STROKE
J. Gonzalez-Valcarcel1, L. Sissani2, J. Labreuche3, M.G. Bousser4, A. Chamorro5, M. Fisher6, I. Ford7, K.M. Fox8, M.G. Hennerici9, H.P. Mattle10, P.M. Rothwell11, P.G. Steg12, E. Vicaut13 and P. Amarenco2
1Foch Hospital, Neurology, Suresnes, France
2Hopital Bichat- APHP, Neurology, Paris, France
3Université de Lille, Santé publique: épidémiologie et qualité des soins, Lille, France
4Hopital Lariboisiere- APHP, Neurology, Paris, France
5Hospital Clinic, Neurology, Barcelona, Spain
6Harvard University- Brigham and Women hospital, Neurology, Boston- MA, USA
7University of Glasgow, Robertson Centre for Biostatistics, Glasgow, United Kingdom
8NHLI Imperial College- ICMS- Royal Brompton Hospital, Cardiology, London, United Kingdom
9University of Heidelberg, Neurology, Mannheim, Germany
11University of Oxford, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
12Hopital Bichat- APHP, Cardiology, Paris, France
13Hôpital Fernand Widal- APHP, Biostatistics, Paris, France
Abstract
Background: Paracetamol safety in high cardiovascular risk patients has been questioned. We sought to determine whether paracetamol or ibuprofen use is associated with major cardiovascular events or major bleeding in patients with recent ischaemic stroke or transient ischaemic attack (TIA).
Methods: Using the PERFORM trial database, we performed two nested case-control analysis (2153 cases with a major cardiovascular event and 4306 controls matched on ESSEN score; a second with 809 cases with a major bleeding matched with 1616 controls). A separate time-varying analysis was performed.
Results: 11·2% of the study population were prescribed paracetamol and 2·5% ibuprofen. Paracetamol was associated with increased risk of a major cardiovascular event (OR 1·21, 95% CI 1·04–1·42) or a major bleeding (OR 1·60, 95% CI 1·26–2·03), with no impact of daily dose and duration of treatment. There was no increased risk of major cardiovascular events (OR 1·03, 95% CI 0·73–1·34) or major bleeding with ibuprofen and no significant association with duration or dose. Time-varying analysis found an increased risk of major cardiovascular events with both paracetamol (OR 1·22, 95% CI1·05–1·43) and ibuprofen (OR 1·47, 95% CI 1·06–2·03) and of major bleeding with paracetamol (OR 1·95, 95% CI 1·45–2·62).
Conclusions: There was a weak and inconsistent signal for association between paracetamol or ibuprofen and major cardiovascular events or major bleeding, which may be related to either a genuine but modest effect of these drugs, or to residual confounding. Given the widespread use of paracetamol and ibuprofen, their safety among patients with stroke/TIA should be investigated in randomised studies.
AS16-027
RISK FACTORS FOR STROKE
Oral
SYSTOLIC VISIT-TO-VISIT BLOOD PRESSURE VARIABILITY INCREASES RISK OF ISCHAEMIC STROKE IN PATIENTS WITH HYPERTENSION AND HIGH RISK OF CARDIOVASCULAR EVENTS. RESULTS FROM THE VALUE TRIAL
M. H Mehlum1, K. Liestøl2, S. Julius3, S.E. Kjeldsen4, T.A. Hua5, P.M. Rothwell6, G. Mancia7, G. Parati8, M.A. Weber9 and E. Berge10
1Institute of Clinical Medicine, Department of Geriatric Medicine and Department of Internal Medicine, Oslo, Norway
2University of Oslo, Department of Informatics, Oslo, Norway
3University of Michigan, Divison of Cardiovascular Medicine, Ann Arbour- Michigan, USA
4Faculty of Medicine, Department of Cardiology- Oslo Unviersity Hospital Ullevaal, Oslo, Norway
5Novartis, Novartis Pharmaceuticals Corporation, East Hanover- NJ, USA
6Stroke Prevenetion Research Unit- University of Oxford, Nuffield Department of Clinical Neuroscience- John Radcliffe Hospital, Oxford, United Kingdom
7University of Milano-Bicocca, St Gerardo Hospital, Monza, Italy
8Instituto Auxologico Italiano- University of Milano-Bicocca, Department of Cardiology S. Luca Hospital- Department of Health Sciences, Milan, Italy
9Downstate College of Medicine- State University of New York, Department of Cardiovascular Medicine, New York, USA
10Oslo University Hospital Ullevaal, Department of Cardiology, Oslo, Norway
Abstract
Background: We have studied whether increased visit-to-visit variability in systolic blood pressure increases the risk of ischaemic and haemorrhagic stroke in the VALUE trial population.
Methods: VALUE trial was a randomised-controlled, double-masked investigation of valsartan versus amlodipine in patients ≥50 years with hypertension and high risk of cardiovascular events. Mean follow-up time was 4.2 years. We calculated standard deviation (SD) of mean systolic blood pressure from 6 months onward, excluding patients with <3 visits, or stroke or cardiac events during the first 6 months. We grouped SD in quintiles and compared risk of ischaemic and haemorrhagic stroke in the highest and lowest quintile, using Cox regression, adjusting for prognostic variables, including randomised treatment and mean systolic blood pressure.
Results: Of 13.803 patients included, 359 (2.6%) experienced ischaemic and 42 (0.3%) experienced hemorrhagic stroke. Compared to patients with the lowest variability, those in the highest quintile had an increased risk of ischemic stroke (HR 1.9, 95% CI 1.3–2.7, p < 0.0001, Figure). There were too few haemorrhagic strokes for the same analysis.
Conclusions: Visit-to-visit systolic blood pressure variability predicts ischaemic stroke in high risk hypertensive patients receiving valsartan or amlodipine, independent of mean systolic blood pressure. We could not analyse the effect on haemorrhagic stroke, due to few events.
AS13-020
RISK FACTORS FOR STROKE
Oral
HIGH BODY MASS INDEX IN CHILDHOOD INCREASES THE RISK OF EARLY ADULT ISCHEMIC STROKE INDEPENDENTLY OF BIRTH WEIGHT
L.K. Haugaard1, M. Gamborg2, T. Truelsen3, T.I.A. Sørensen1 and J.L. Baker2
1Novo Nordisk Foundation Center for Basic Metabolic Research, Section of Metabolic Genetics, Copenhagen, Denmark
2Institute of Preventive Medicine, Bispebjerg and Frederiksberg Hospitals, a part of Copenhagen University Hospital, The Capital Region, Copenhagen, Denmark
3Department of Neurology, Rigshospitalet, University of Copenhagen, Denmark
Abstract
Background: We aimed to investigate if childhood body mass index (BMI), independently of birth weight, affects the risk of early and late adult ischemic stroke.
Methods: We studied a cohort of 307,677 Danish school children born from 1930 to 1987 who had weight and height measurements at age 7, 10, or 13 years. BMI was calculated (kg/m2) and transformed to z-scores. We ascertained ischemic stroke (IS) events by linkage to national registers and categorized them as early (25 – 55 years) or late (>55 years) events. We used restricted cubic splines to model non-linear effects of childhood BMI on early and late adult IS and estimated hazard ratios (HR) with 95% confidence intervals (CIs) by Cox proportional hazards regressions.
Results: During 8,128,058 person-years of follow-up, 3,529 women and 5,370 men had an IS. Both men and women with a childhood BMI z-score above average had an increased risk of early, but not late, IS. The pattern of the associations with early IS was similar at all ages in childhood, but strongest at age 13 years, where a BMI z-score of 1 was associated with a HR of 1.26 (95% CI: 1.11, 1.43) in women and 1.21 (95% CI: 1.10, 1.33) in men. Adjusting for birth weight did not affect the associations.
Conclusions: In this large prospective study we found that having a BMI above average in childhood increases the risk of early, but not late, adult IS. Future research should address the potential influence of other risk factors such as diabetes and hypertension.
AS16-038
RISK FACTORS FOR STROKE
Oral
THE RELATIONSHIP BETWEEN SLEEP-DISORDERED BREATHING AND BLOOD PRESSURE PARAMETERS IN CEREBROVASCULAR EVENTS: THE EVOLUTION FROM ACUTE TO SUBACUTE PHASE
T. Horvath1, L. Korostovtseva2, U. Fischer3, S. Ott4, M. Manconi5, C. Bernasconi6, C. Cereda5, G. Moschovitis7 and C. Bassetti6
1Bern University Hospital, Department of Neurology, Bern, Switzerland
2 V.A. Almazov Federal North-West Medical Research Centre / Bern University Hospital, Department for Hypertension / Neurology Department, St. Petersburg / Bern, Russia
3Bern University Hospital, Neurology Clinic, Bern, Switzerland
4Bern University Hospital, Department for Pulmonology, Bern, Switzerland
5Neurocenter of Southern Switzerland- Ospedale Regionale di Lugano, Neurology Department, Lugano, Switzerland
6Bern University Hospital, Neurology Department, Bern, Switzerland
7Neurocenter of Southern Switzerland- Ospedale Regionale di Lugano, Cardiology Department, Lugano, Switzerland
Abstract
Background: The objective is to assess the evolution of blood pressure (BP) parameters with regard to sleep-disordered breathing (SDB) in post-stroke patients and its impact on outcome within a multicenter prospective study (SAS-CARE1).
Methods: We enrolled 131 patients (101 males, mean age 61.8 ± 9.5years) with acute stroke (NIHSS 2(0;25)). At baseline (within 7 days from stroke onset) and at 3-month follow-up, all patients underwent full video-polysomnography, and 24-hour BP monitoring (24hBPM) with assessment of BP variability (standard deviation/SD, range, coefficient of variance/CV) and daily profile (mean nighttime/daytime BP).
Results: At baseline, SDB was diagnosed (apnea-hypopnea index, AHI > 5/h) in 113(87%) patients, at 3 months – in 82(83.7%) with an average AHI 17.1(0;73) and 13.8(0.2;79.2)/h, respectively (p = 0.11). AHI positively correlated with 24hBPM both at baseline and follow-up, in particular with systolic BP, and with nighttime BP at 3 months (Table). However, in regression analysis BP was not independently correlated with SDB. SDB evolution (AHI_3_months-AHIbaseline) positively correlated with BP variability change (SD_systolic_BP: ρ = 0.27, p = 0.033; CV_diastolic_BP: ρ = 0.26, p = 0.034; CV_systolic_BP: ρ = 0.23, p = 0.07). Mean systolic_BP at baseline (p = 0.02) was associated with NIHSS change (model: R2 = 0.93, p < 0.0001).
Conclusions: In stroke patients, SDB severity decreases from acute to subacute phase and is associated with 24hBPM parameters at both time points. SDB evolution may play a predictive role for BP variability changes by 3 months, while mean systolic BP at baseline is associated with functional post-stroke outcome.
AS13-027
RISK FACTORS FOR STROKE
Oral
30-YEAR TRENDS IN 28-DAY FUNCTIONAL OUTCOMES: FINDINGS FROM THE AUCKLAND REGIONAL COMMUNITY STROKE STUDIES, 1981-2011
R. Krishnamurthi1, V. Parag2, P. Parmar1, P.A. Barber3 and V. Feigin1
1National Institute for Stroke and Applied Neurosciences, Faculty of Health and Envioronmental Sciences, Auckland, New Zealand
2The University of Auckland, The National Institute for Health Innovation- School of Population Health, Auckland, New Zealand
3The University of Auckland, Centre for Brain Research, Auckland, New Zealand
Abstract
Background: There is a paucity of reliable data on longitudinal trends in functional outcome following stroke. However it is crucial to evaluate these trends in global outcomes of disability to assess the level of success of healthcare interventions and future plans for post-stroke services. We aimed to describe temporal trends over 3 decades in 28-day outcomes for disability following first-ever stroke using data from the Auckland Regional Community Stroke Studies (ARCOS I-IV), conducted in 1981, 1991, 2002, and 2010.
Methods: Disability at 28-days post stroke was assessed using the modified Rankin scale (mRS), dichotomised into good (mRS 0–2) and poor (mRS 3–5) outcomes. The temporal trend in the proportion of stroke survivors with good vs poor outcome across the 4 studies was analysed using the Cochran-Armitage trend test in a sample of 3956 first-ever strokes.
Results: The 28-day case fatality was 31.6%, 23.1%, 19% and 17.8% in 1981, 1991, 2002, and 2011 respectively. Of the survivors, the proportion of people with good outcome was 67.6%, 65.5%, 62.6% and 79.6% in 1981, 1991, 2002, and 2011 respectively. There was an overall significant increase in the proportion of stroke survivors with good outcome over the 3 decades (p < 0.001). Further analysis is currently underway, and analysis of trends by age, sex and ethnicity will be presented.
Conclusions: The proportion of stroke survivors with good outcome increased in the last 3 decades, which may be a result of improved healthcare and management of risk factors.
AS06-032
RISK FACTORS FOR STROKE
Oral
EARLY LIFE RISK FACTORS AND STROKE IN LATER LIFE: SYSTEMATIC REVIEW AND META-ANALYSIS
C.A. McHutchison1, E.V. Backhouse1, S.D. Shenkin2, V. Cvoro1 and J.M. Wardlaw1
1University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
2University of Edinburgh, Department of Clinical and Surgical Sciences, Edinburgh, United Kingdom
Abstract
Background: Risk factors emerging in midlife, like hypertension, diabetes and smoking explain some but not all stroke risk. Some evidence suggests that early life factors such as childhood, IQ, socioeconomic status (SES), and education may also affect later life stroke risk. We meta-analysed all available evidence on early life factors and risk of stroke in later life.
Methods: We searched Medline, PsychINFO and EMBASE electronically and hand-searched the previous 5 years of Stroke, Neurology and International Journal of Epidemiology. Two reviewers screened all abstracts and full texts independently, and extracted data on stroke incidence by IQ, fathers’ occupation/education and years of education. Hazard ratios (HR), odds ratios (OR), relative risks (RR) and mean differences were used to compute the overall effect using a random-effects model.
Results: We found 99 studies examining early life factors and risk of stroke (80, education; 10 SES; nine IQ) including 137,689 stroke and 2,695,705 non-stroke participants. Meta-analysis adjusted for vascular risk factors showed that lower education (OR = 1.40, 95% CI = 1.28–1.53), childhood IQ (HR = 1.17, 95% CI = 1.00–1.37) and SES (OR = 1.28, 95% CI = 1.12–1.46) were each significantly associated with increased stroke risk. Heterogeneity was high ranging from 55–96%.
Conclusions: Early life factors including fewer years of education, lower IQ and SES are related to increased stroke risk in later life. Education and childhood SES are both potentially modifiable have significant implications for public policy and offer routes to ameliorate stroke rates.
AS16-061
RISK FACTORS FOR STROKE
Oral
SELECTIVE SEROTONIN REUPTAKE INHIBITORS AND THE RISK OF INTRACEREBRAL HAEMORRHAGE: A POPULATION-BASED COHORT STUDY
C. Renoux1, S. Vahey2, S. Dell'Aniello2 and J.F. Boivin3
1Jewish General Hospital - McGill University, Neurology- Epidemiology and Biostatistics, Montreal, Canada
2Jewish General Hospital - Lady Davis Research Institute, Centre for clinical epidemiology, Montreal, Canada
3Jewish General Hospital - McGill University, Epidemiology and Biostatistics, Montreal, Canada
Abstract
Background: Selective serotonin reuptake inhibitors (SSRIs) may increase the risk of intracerebral haemorrhage through inhibition of platelet aggregation. However, this risk is not well quantified, and the impact of concomitant use of antithrombotic agents is unknown.
Methods: We used the UK Clinical Practice Research Datalink (CPRD) to form a cohort of all new users of antidepressants, 18 years or older, between 1995 and 2014. Using a nested case-control approach, each case of first intracerebral haemorrhage identified during follow-up was matched with up to 30 controls selected among the cohort members in the risk sets defined by the case and matched on age, sex, calendar time, and duration of follow-up. Incidence rate ratios (RR) of intracerebral haemorrhage associated with current use of SSRIs compared with tricyclic antidepressants (TCAs) were estimated using conditional logistic regression, adjusted for potential confounders.
Results: Among a cohort of 1,363,990 incident users of antidepressants, 3,036 cases of intracerebral haemorrhages were identified during follow-up and matched to 89,702 controls. Current SSRI use was associated with an increased risk of intracerebral haemorrhage (RR = 1.17, 95% CI 1.02–1.35) relative to TCAs, highest during the first month of use (RR = 1.42, 95% CI 1.04–1.93). Concomitant use of anticoagulants increased the risk 3-fold although the result did not reach statistical significance (RR = 3.08, 95% CI 0.89–10.63). Conversely, SSRI use along with antiplatelets did not increase the risk of haemorrhage.
Conclusions: The use of SSRIs is associated with an increased risk of intracerebral haemorrhage, particularly when taken together with oral anticoagulants.
AS06-048
RISK FACTORS FOR STROKE
Oral
AMBIENT TEMPERATURE AND STROKE OCCURRENCE: SYSTEMATIC REVIEW AND META-ANALYSIS
X. Wang1, D. Hong2, Z. Danni3, T.H. Leong3, S. Richtering3, E.C. Sandset3, Y. Cao3, C. Anderson3 and M. Hackett3
1The George Institute for Global Health, Sydney, Australia
2The George Institute for Global Health, Renal & Metabolic Divisions, Sydney, Australia
3The George Institute for Global Health, Neurological & Mental Health Division, Sydney, Australia
Abstract
Background: Biologically plausible associations exist between climatic conditions and stroke risk, but the results of studies are inconsistent. We aimed to summarize current evidence on ambient temperature and stroke occurrence.
Methods: We performed a comprehensive literature search across Medline, Embase, PsycINFO, Cinahl, Web of Science, and Geobase from inception to the 16th October 2015 to identify all population-based observational studies examining the relationship between ambient temperature and admission to hospital for stroke. Two authors independently screened articles and conducted data extraction based on pre-defined inclusion criteria. Odds ratios (OR) with corresponding 95% confidence intervals (CI) were pooled by means of the random effects method.
Results: We included 21 studies with a total of 476,511 patients. Pooled ORs (95% CI) associated with every 1 degree Celsius increase in ambient temperature were 1.00 (0.99–1.00) for ischemic stroke (IS), 0.96 (0.93–1.00) intracerebral haemorrhage (ICH), and 1.00 (0.98–1.01) for subarachnoid haemorrhage (SAH). For IS, 5 of 6 studies found statistically significant associations in women; 3 of 3 studies identified significant associations in the elderly; and 3 of 7 reported significant associations with larger variations in ambient temperature. For ICH, significant associations were found for the elderly; and 5 of 8 studies found significant associations with larger variation in ambient temperature.
Conclusions: Larger variations in temperature appear to be associated with higher rates of stroke occurrence, especially in the elderly population.
AS17-008
SMALL VESSEL DISEASE
Oral
THE RISK OF PARKINSONISM IN PATIENTS WITH SMALL VESSEL DISEASE. RESULTS OF 9-YEAR FOLLOW-UP IN THE RUN DMC STUDY
M.I. Bergkamp1, H.M. van der Holst1, E.M.C. van Leijsen1, A.M. Tuladhar1, I.W.M. van Uden1, K.F. de Laat2, A.G.W. van Norden3, E.J. van Dijk1, R.A.J. Esselink1 and F.E. de Leeuw1
1Radboudumc, Neurology, Nijmegen, Netherlands
2Hagaziekenhuis, Neurology, The Hague, Netherlands
3AmphiaZiekenhuis, Neurology, Breda, Netherlands
Abstract
Background: Motor symptoms of patients with comparable cerebral small vessel disease (SVD) are variable, ranging from no symptoms to parkinsonism. We investigated if a difference in SVD location and/or in remote brain volumes plays a role in this variability.
Methods: The RUNDMC study is a prospective cohort study (baseline 2006) of 503 individuals with SVD. Incident parkinsonism was diagnosed according to the UKPDS brain bank criteria during follow-up in 2011 and 2015. The diagnosis was based on motor examination during the follow-up visits and through review of medical records. All participants underwent T1, T2*and FLAIR scanning. To assess the association between SVD, remote brain volumes and incident parkinsonism, Kaplan-Meier curves were calculated and Cox regression analysis was used.
Results: Baseline mean age was 65.6 year (±SD 8.8), 56.8% were male and mean White Matter Hyperintensities (WMH) volume was 9 mL (SD 12). 32 Participants developed parkinsonism, resulting in a 9-year cumulative risk of 6.8%. WMH volume (HR 1.53 per SD 95%CI 1.23–1.91) and presence of lacunes (HR 1.4 95%CI 1.15–1.59), independent of their location, were significant predictors of parkinsonism. A higher total brain volume was associated with a lower risk of incident parkinsonism (HR 0.35 per SD; 95%CI 0.18–0.65). Grey matter volume explained most of the variance.
Conclusions: The degree, rather than the location of WMH and lacunes, is important in the prediction of parkinsonism. Difference in total brain volume partially explained the variable risk of incident parkinsonism in patients with equal SVD severity.
AS26-011
SMALL VESSEL DISEASE
Oral
SMALL VESSEL DISEASE AND COGNITION IN FIRST EVER STROKE PATIENTS: RESULTS FROM THE TABASCO STUDY
E. Kliper1, J. Molad1, E. Ben Assayag1, L. Shopin1, A. Korczyn2, N. Bornstein1 and E. Auriel1
1Tel Aviv Sourasky Medical Center, Neurology, Tel-Aviv, Israel
2Tel Aviv University, Neurology, Tel Aviv, Israel
Abstract
Background: Small vessel disease (SVD) is known to be important cause of cognitive impairment and dementia. Recently, a new score, "SVD burden", was suggested to provide an estimation of the impact of SVD on the brain in relation to cognitive impairment.
Methods: SVD burden is an ordinal scale from 0 to 4, including sum of the following MRI features: white matter hyperintensities (WMH), lacunes, microbleeds, perivascular spaces. In this study (TABASCO, Tel Aviv acute brain stroke cohort), we investigated, for the first time, the predictive role of SVD burden on cognitive state one year after first-ever ischemic stroke or TIA.
Results: Included were 230 consecutive patients. Significant main effect was observed for Framingham Stroke Risk Profile score across SVD burden partitioning (p < 0.001). Also, there were significant differences in the frequencies of SVD burden between patients with DWI positive and those without (main effect p = 0.001). Negative correlations between SVD burden and cognitive scores were observed for global cognitive, memory and visual spatial scores after one year (all p < 0.05). However, adjustment for age and education kept significance only for the memory score. Fazekas WMH score significantly correlated with different cognitive scores following an adjustment for age and education.
Conclusions: To the best of our knowledge, this study is the first to examine the predictive role of SVD burden score on cognitive state one year after first-ever stroke or TIA. The results suggest that WMH score may be a better predictor of cognitive state than SVD burden.
AS16-040
SMALL VESSEL DISEASE
Oral
AGE-SPECIFIC ROLE OF PREMORBID BLOOD PRESSURE IN PATIENTS WITH SMALL VESSEL TIA AND STROKE: A POPULATION-BASED STUDY
L. Li1, L. Bull1, S. Welch1 and P.M. Rothwell On behalf of the Oxford Vascular Study
1
1Stroke Prevention Research Unit, Nuffield Department of Clinical Neurosciences- Oxford University, Oxford, United Kingdom
Abstract
Background: There is conflicting evidence of the role of blood pressure (BP) in the aetiology of small vessel (SVD) events at different ages.
Methods: In a population-based study of acute TIA/stroke (OXVASC), we compared 15-year pre-morbid BP readings from primary care records in patients with SVD vs. non-SVD events (TOAST) stratified by age (<65 y vs.≥65 y).
Results: Of 2081 patients (1249-stroke/832-TIA/>45,000 pre-morbid BP readings), 308 had SVD events and 491 were aged < 65 y. Prevalence of diagnosed hypertension did not differ between SVD vs. non-SVD events, but 15-year mean/SD premorbid BP (mmHg) was higher in SVD events in patients aged < 65 y (SBP-138.5/16.5 vs. 133.4/15.0, p = 0.004; DBP-84.2/8.8 vs. 80.9/5.4, p = 0.001). Moreover, this difference increased (p-trend < 0.001) with BP measured closer to the index event (figure) (<30d pre-event-SBP 152.7/16.1 vs. 135.3/23.1, p = 0.009; DBP 87.9/9.4 vs. 80.8/12.8, p = 0.05; mean BP in 1-year pre-event - 146.1/22.0 vs. 134.7/16.1, p = 0.0004; 86.1/10.7 vs. 80.4/9.8, p < 0.0001), particularly in patients on premorbid antihypertensive treatment (figure). However, no similar differences in BP were observed in patients aged≥65 y, due partly to a J-shape association at BP < 110/70.
Conclusions: Recent premorbid BP control is strongly related to acute SVD events at younger ages, particularly in patients on antihypertensive drugs, highlighting the importance of consistent control of BP. The BP associations at older ages were more complex, with some evidence of a J-shape.
AS26-043
SMALL VESSEL DISEASE
Oral
TOPOGRAPHIC DISTRIBUTION OF LACUNES IN CEREBRAL AMYLOID ANGIOPATHY AND HYPERTENSIVE DEEP INTRACEREBRAL HEMORRHAGE
M. Pasi1,2, G. Boulouis2, A. Charidimou2, A. Eitan3, K. Haley2, A. Ayres2, K.M. Schwab2, J. Rosand4, A. Viswanathan2, L. Pantoni1 and S.M. Greenberg2
1University of Florence, NEUROFARBA Department, Florence, Italy
2Massachusetts General Hospital Stroke Research Center- Harvard Medical School- Boston, Hemorrhagic Stroke Research Program- Department of Neurology, Boston, USA
3Sourasky Medical Center, Neurology Department, Tel Aviv, Israel
4Massachusetts General Hospital- Harvard Medical School, Division of Neurocritical Care and Emergency Neurology, Boston, USA
Abstract
Background: To evaluate whether lacunes in lobar (LL) and deep (DL) locations, defined similarly to microbleed distribution, would differ between intracerebral hemorrhage patients (ICH) with definite/probable CAA (CAA) and hypertensive deep-ICH (HTN-ICH).
Methods: We compared presence/absence of LL and DL between CAA and HTN-ICH patients. Their associations with both markers of SVD severity [white matter hyperintensity (WMH) volume and microbleed counts] and small vessel disease (SVD) type [perivascular spaces (PVS), and WMH patterns] were assessed using multivariate models.
Results: In our cohort of 316 ICH patients, lacunes were frequent (30.4%) with similar rates in 191 CAA and 125 HTN-ICH (29.3% vs 32%, p = 0.62). Higher creatinine, WMH volume, and the diagnosis of HTN-ICH (all p < 0.05) but not microbleed counts were associated with lacune counts. LLs were more commonly present in CAA (23% vs 7.2% in HTN-ICH, p < 0.001) while DLs more frequent in HTN-ICH (16.8% vs 3.1%, p < 0.001). In multivariate model, LLs were associated with CAA diagnosis (p < 0.001), older age (p = 0.018), and presence of centrum-semiovale PVS (p = 0.033). Conversely, diagnosis of HTN-ICH (p = 0.001), higher WMH volume (p = 0.012), presence of peri-basal ganglia WMH pattern (p = 0.019) were predictors of DLs.
Conclusions: Distinguishing CAA from HTN-SVD is important as they are associated with significantly different ICH risk. LL appears to be a marker of CAA whereas DL of HTN-SVD, they can thus be clinically useful in the appropriate context.
AS20-025
SMALL VESSEL DISEASE
Oral
PATIENTS WITH MIXED LOCATION (DEEP AND LOBAR) CEREBRAL MACROBLEEDS AND MICROBLEEDS: BASELINE CHARACTERISTICS AND FOLLOW UP DATA
M. Pasi1,2, A. Charidimou2, G. Boulouis2, E. Auriel3, K. Haley2, A. Ayres2, K.M. Schwab2, J. Rosand4, A. Viswanathan2, L. Pantoni1, S.M. Greenberg2 and E. Gurol2
1University of Florence, NEUROFARBA Department, Florence, Italy
2Massachusetts General Hospital- Harvard Medical School, Hemorrhagic Stroke Research Program- Department of Neurology, Boston, USA
3Sourasky Medical Center, Department of Neurology, Tel Aviv, Israel
4Neurocritical Care and Emergency Neurology, Massachusetts General Hospital- Harvard Medical School, Boston, USA
Abstract
Background: The predominant type of cerebral small vessel disease (SVD) and clinical outcomes of patients who present with a combination of lobar and deep intracerebral hemorrhage (ICH)/microbleed (MB) locations (Mixed-ICH, FIGURE) is unknown.
Methods: Demographics, clinical/laboratory features, and SVD neuroimaging markers of 75 patients with Mixed-ICH were compared to 191 probable Cerebral Amyloid Angiopathy (CAA-ICH) and 125 Hypertensive deep-ICH (HTN-ICH) patients. ICH-recurrence, ischemic stroke (IS)-occurrence and case-fatality on follow up were analyzed.
Results: Mixed-ICH patients had a higher prevalence of hypertension, diabetes, left ventricular hypertrophy rates, and higher creatinine values (all p < 0.05) than CAA-ICH, while no significant differences were found when compared to HTN-ICH. In multivariable models, Mixed-ICH was associated with higher creatinine, more lacunes and basal ganglia perivascular spaces (PVS), than CAA-ICH (all p < 0.05). When compared to HTN-ICH, Mixed-ICH patients were older and had more lacunes and MBs in multivariable models (all p < 0.05). Among 90-day survivors, adjusted case fatality rates were similar for all 3 categories. Annual risk of ICH-recurrence was 5.1% for Mixed-ICH, higher compared to HTN-ICH but lower than CAA-ICH (1.6% and 10.4% respectively). IS-occurrence for Mixed-ICH was similar to HTN-ICH but higher than CAA-ICH.
Conclusions: Mixed-ICH, commonly seen when MRI obtained during etiologic workup, appears to be mostly driven by vascular risk factors similar to HTN-ICH, but demonstrates more severe parenchymal damage and higher ICH-recurrence risk.
AS26-029
SMALL VESSEL DISEASE
Oral
RECENT SMALL SUBCORTICAL INFARCTS ARE RELATED WITH PROGRESSION OF CEREBRAL SMALL VESSEL DISEASE: A NINE YEARS FOLLOW-UP STUDY
A. ter Telgte1, A. Tuladhar1, P. Barbosa Oliveira1, R. Maas1, M. Bergkamp1, H.M. van der Holst1, E. van Leijsen1, I.W.M. van Uden1, M. Ghafoorian2, B. Platel2, D. Norris3, E.J. van Dijk1 and F.E. de Leeuw1
1Radboud University Medical Centre- Donders Institute for Brain- Cognition and Behaviour- Centre for Neuroscience, Neurology, Nijmegen, Netherlands
2Radboud University Medical Centre, Radiology and Nuclear Medicine- Diagnostic Image Analysis Group, Nijmegen, Netherlands
3Radboud University Nijmegen, Donders Institute for Brain- Cognition and Behaviour- Centre for Cognitive Neuroimaging, Nijmegen, Netherlands
Abstract
Background: Recent findings suggest a causal role for recent small subcortical infarcts (RSSIs) in cerebral small vessel disease (SVD). However, the relationship between RSSIs in SVD and progression of white matter hyperintensities (WMH) and presence of lacunes and microbleeds during a long-term follow-up has never been investigated.
Methods: 503 subjects with SVD (mean age 65.7 [SD8.8] years, 56.4% male) were obtained from the RUNDMC study, with neuroimaging in 2006, 2011 and 2015. Diffusion-weighted images were checked for RSSIs and its prevalence was calculated. Progression of WMH volume and presence of microbleeds and lacunes were compared between RSSI+ and RSSI- subjects.
Results: Prevalence of RSSIs was 2.6% (2006), 1.7% (2011) and 2.1% (2015). At each time point, RSSI+ subjects had increased WMH volume compared to RSSI- subjects (mean difference: 12.5 ml, p < .001 [2006]; 6.7 ml, p = .040 [2011]; 19.7 ml, p = .011 [2015]). The annual WMH progression was increased across RSSI+ subjects (mean difference 0.79 ml, p = .002) compared to RSSI- subjects. Furthermore, presence of lacunes was increased in RSSI+ subjects in 2006 (RSSI+ vs. RSSI-: 85% vs. 26%, p < .001) and 2011 (83% vs. 33%, p = .019), though non-significantly in 2015 (50% vs. 32%, p = .391). Similarly, presence of microbleeds was increased in RSSI+ subjects in 2006 (62% vs. 15%, p < .001), but non-significantly in 2011 (50% vs. 22%, p = .133) and 2015 (50% vs. 25%, p = .172).
Conclusions: These results suggest a common pathology underlying the SVD spectrum. Remarkably, acute cerebral ischemia is related to progression of WMH, traditionally believed to have a chronic ischemic cause.
AS22-046
SMALL VESSEL DISEASE
Oral
WHITE MATTER ATROPHY AND LOSS OF WHITE MATTER INTEGRITY ARE ASSOCIATED WITH GAIT DECLINE IN OLDER ADULTS WITH CEREBRAL SMALL VESSEL DISEASE
E. van der Holst1, A. Tuladhar1, I.W.M. van Uden1, K. de Laat2, E. van Leijsen1, M. Ghafoorian3, B. Platel3, M. Bergkamp1, A.G.W. van Norden4, D. Norris5, E.J. van Dijk1 and F.E. de Leeuw1
1Radboud university medical center, Neurology, Nijmegen, Netherlands
2HagaZiekenhuis Den Haag, Neurology, Den Haag, Netherlands
3Radboud university medical center, Radiology, Nijmegen, Netherlands
4Amphia ziekenhuis, Neurology, Breda, Netherlands
5Radboud University- Donders Institute for Brain- Cognition and Behaviour, Center for Cognitive Neuroimaging, Nijmegen, Netherlands
Abstract
Background: The relation between progression of cerebral small vessel disease (SVD) and gait decline is uncertain and diffusion tensor imaging (DTI) studies on gait decline are lacking. We therefore investigated the associations between (micro)structural brain changes and gait decline in SVD.
Methods: 269 participants from the RUN DMC cohort, a prospective cohort of participants with SVD ≥ 50years, were included. Gait was assessed quantitatively during baseline (2006–2007) and follow-up (2011–2012). Linear regression analysis was used to investigate the association between changes in MRI and DTI measures and gait decline. Tract-based spatial statistics (TBSS) was used to investigate region-specific associations between changes in white matter integrity and gait decline.
Results: 56.1% were male, mean age was 62.9 y (SD8.3), follow-up duration was 5.4 y (SD0.2) and mean gait speed decline was −0.2 m/s. Stride length decline was associated with white matter atrophy (β = .16, p = 0.003) and white matter radial diffusivity (β = −.15, p = 0.004), independent of age, sex, height, follow-up duration and baseline stride length. TBSS analysis showed significant associations between stride length decline and fractional anisotropy decrease and mean diffusivity increase (primarily explained by radial diffusivity increase) in multiple white matter tracts, with the strongest associations found in the corpus callosum, independent of conventional SVD markers (see figure).
Conclusions: White matter atrophy and loss of white matter integrity are associated with gait decline in adults with SVD.
AS13-056
SMALL VESSEL DISEASE
Oral
THE RISE AND FALL OF CEREBRAL SMALL VESSEL DISEASE - THE RUN DMC STUDY
E. van Leijsen1, I.W.M. van Uden1, M. Ghafoorian2, M. Bergkamp1, V. Lohner3, E. Kooijmans1, H.M. van der Holst1, R. Arntz1, A. Tuladhar1, D. Norris4, E.J. van Dijk1, K. Klijn1, B. Platel2 and F.E. de Leeuw1
1Radboudumc- Donders Institute for Brain- Cognition and Behaviour, Department of Neurology, Nijmegen, Netherlands
2Radboudumc, Department of Radiology and Nuclear Medicine- Diagnostic Image Analysis Group, Nijmegen, Netherlands
3University of Cambridge, Department of Clinical Neurosciences- Neurology Unit, Cambridge, United Kingdom
4Donders Institute for Brain- Cognition and Behaviour, Centre for Cognitive Neuroimaging, Nijmegen, Netherlands
Abstract
Background: Cerebral small vessel disease (SVD) and its progression is increasingly recognized as the most important vascular contributor to dementia. However, understanding of who experiences progression in SVD remains elusive. Remarkably, recently not only progression, but also SVD regression was noted. However, systematic research on the magnitude of SVD disappearance is lacking. We therefore investigated both progression and regression of the whole SVD spectrum over time, thereby taking baseline SVD severity into account.
Methods: From 276 participants of the RUN DMC cohort study SVD characteristics were assessed at 3 time points, with a follow-up of almost 9 years. WMH volume was rated by semi-automatic segmentation. Lacunes and microbleeds were counted manually.
Results: Mean age was 62.5 (SD 7.7) years and 59.1% was male. Mean WMH progression was 4.7 ml (IQR 0.95 – 5.5 ml) over 9 years (0.54 ml/yr), 25.0% had incident lacunes (2.9%/yr) and 18.9% had incident microbleeds (2.2%/yr). Progression of WMH was predominantly seen in participants with moderate or severe WMH at baseline, whereas those with only mild WMH barely progressed (Figure). Interestingly, WMH declined in 1.4% of the participants and in 5.7% and 1.1% of the participants microbleeds and lacunes disappeared.
Conclusions: Progression of SVD is highly differential, suggesting heterogeneity in etiology of mild versus severe SVD. Remarkably, some patients even showed vanishing SVD.
AS18-044
SMALL VESSEL DISEASE
Oral
PREVALENCE AND ASSOCIATIONS OF MRI MARKERS OF SMALL VESSEL DISEASE IN ISCHAEMIC STROKE AND TIA ASSOCIATED ATRIAL FIBRILLATION: BASELINE CHARACTERISTICS OF THE CROMIS-2 STUDY
D. Wilson1, A. Charidimou1, G. Ambler2, C. Shakeshaft1, M. White1, R. Al-Shahi Salman3, H. Cohen4, T. Yousry5, G.Y.H. Lip6, M.M. Brown1, H.R. Jager5 and D.J. Werring1
1Institute of Neurology, Brain repair and rehabilitation, London, United Kingdom
2University College London, Department of Statistical Science, London, United Kingdom
3School of Clinical Sciences- University of Edinburgh, Division of Clinical Neurosciences- Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
4University College London Hospitals NHS Foundation Trust, Haematology, London, United Kingdom
5National Hospital for Neurology and Neurosurgery, Lysholm Department of Neuroradiology-, London, United Kingdom
6University of Birmingham, Centre for Cardiovascular Sciences- City Hospital, Birmingham, United Kingdom
Abstract
Background: Imaging markers of small vessel disease (SVD) (Cerebral microbleeds (CMBs), white matter hyperintensities of presumed vascular origin (WMH) and cortical superficial siderosis (cSS)) have potential value in predicting the risk of oral anticoagulant (OAC)-related intracerebral haemorrhage (ICH). We investigated their prevalence within CROMIS-2. We hypothesised that CMBs are common and associated with other markers of SVD, age and hypertension.
Methods: CROMIS-2 is a prospective, multicentre, inception cohort study of adults with AF started on OAC after recent ischaemic stroke (IS) or TIA with followed up planned for up to 2 years. All participants have standardized brain MRI at baseline. One trained observer rated CMBs and WMHs using validated scales, and cSS (disseminated or focal) according to consensus criteria.
Results: We included 1496 patients. The prevalence of ≥1 CMBs was 22%, severe WMH (≥2 Fazekas scale in periventricular or deep white matter) 28%, and cSS 0.7%. In univariate analyses, CMBs were associated with age (OR 1.02 per year; 95% CI 1.01 to 1.04), hypertension (OR 1.40; 95% CI 1.06 to 1.84), previous IS (OR 1.99; 95% CI 1.29 to 3.08) and severe WMH (OR 1.81; 95% CI 1.39 to 2.37), but not with cSS (focal or disseminated). In multivariable logistic regression, age, severe WMH and thrombolysis were associated with CMBs.
Conclusions: CMBs are common, but cSS is very rare in patients with ischaemic stroke or TIA associated with atrial fibrillation. CMBs are associated with increasing age, WMHs and thrombolysis.
AS16-001
STROKE IN THE YOUNG
Oral
TO WHAT EXTENT DO ESTABLISHED RISK FACTORS EXPLAIN STROKE IN THE YOUNG? A CASE-CONTROL STUDY
A. Aigner1, U. Grittner2,3, A. Rolfs4, B. Norrving5, B. Siegerink2 and M. Busch6
1University Medical Center Hamburg-Eppendorf, Institute for Medical Biometry and Epidemiology, Hamburg, Germany
2Charité–Universitätsmedizin Berlin, Center for Stroke Research, Berlin, Germany
3Charité–Universitätsmedizin Berlin, Department for Biostatistics and Clinical Epidemiology, Berlin, Germany
4Medical Faculty- University of Rostock, Albrecht Kossel Institute for Neuroregeneration, Rostock, Germany
5Lund University Hospital, Department of Neurology, Lund, Sweden
6Robert Koch Institute, Department of Epidemiology and Health Monitoring, Berlin, Germany
Abstract
Background: The INTERSTROKE study showed that 10 risk factors are associated with 90% of stroke risk in all age groups, but corresponding data for young stroke are not available. This study aims at closing this research gap.
Methods: We performed a case-control study based on 3308 stroke patients aged 18 to 55 years of the Stroke In Young Fabry Patients (SIFAP1) study in 26 German centers, who were matched to controls from the nationwide population-based study German Health Update (GEDA), and calculated adjusted population attributable risks (PARs) of established risk factors and their combinations for all stroke and ischemic and hemorrhagic stroke separately. Additional analyses were carried out for age groups (<35,35–44,>44) and etiological subtypes of ischemic stroke.
Results: We included 2125 cases (95% ischemic) and 8500 controls. Hypertension and physical inactivity were the most important risk factors, in combination accounted for 52.9% (95%-CI: 47.9–57.8), 51.6% (47.2–56.0) and 73.7% (58.0–89.4) of all, ischemic and hemorrhagic strokes, respectively. All included risk factors accounted for 59.3% (53.7–65.0) of all strokes. Smoking (PAR: 14.9%, 10.0–19.7) and diabetes (PAR: 4.9%, 3.1–6.8) were additional important risk factor for ischemic stroke. PARs of most important risk factors were fairly consistently higher in older age groups. For ischemic stroke, PARs were higher for stroke caused by large-artery artherosclerosis and small-vessel occlusion, compared to cardioembolism.
Conclusions: Risk factors previously established for older age account for a large part of stroke in younger age. Targeted population-based risk factor interventions may also have a substantial effect in reducing stroke in the young.
AS28-003
STROKE IN THE YOUNG
Oral
COST UTILITY ANALYSIS OF ROUTINE HYPERCOAGULABLE TESTING IN YOUNG PATIENTS WITH ISCHEMIC STROKE
N. Cheng1, M. Freedman2 and A. Kim1
1UCSF, Neurology, San Francisco, USA
2UCSF, School of Medicine, San Francisco, USA
Abstract
Background: Although the causes of stroke in the young are diverse and tests to evaluate for rare hypercoagulable disorders are commonly performed, it is uncertain whether this routine testing is preferred over presumptive antiplatelet therapy.
Methods: We created a decision-analytic model to compare a strategy of routine hypercoagulable panel testing and long-term anticoagulation if positive with a strategy of no testing and empiric antiplatelet therapy for secondary stroke prevention in young ischemic stroke patients. Clinical event rates, stroke outcomes, healthcare costs, and utilities were drawn primarily from the Healthcare Cost and Utilization Project, the Evaluation of Dutch Integrated Stroke Service Experiments, and the Bernese stroke registry. A Markov model was used to estimate ongoing costs and utilities for recurrent stroke, major and minor hemorrhage, ongoing disability, and death from a societal perspective over 20 years. We used a Monte-Carlo simulation as a sensitivity analysis to account for input uncertainty.
Results: Routine hypercoagulable testing resulted in similar benefits (9.6 [8.7–10.5] vs. 9.7 [8.7–10.5] QALYs) at slightly higher costs ($82,600 [95% CI $70,300–$104,000]) vs. $79,900 [95% CI $67,000–$101,900)] compared to the no test/aspirin strategy. Results were most sensitive to ongoing annual costs of disability and one time costs of hemorrhage and stroke outcomes. In the probabilistic sensitivity analysis, the no-test/aspirin strategy was preferred in 95% of iterations.
Conclusions: Based on currently available evidence, routine testing for hypercoagulable states and long-term anticoagulation may not be preferred over presumptive antiplatelet therapy for young stroke patients.
AS16-037
STROKE IN THE YOUNG
Oral
RISK FACTORS FOR EARLY-ONSET ISCHEMIC STROKE: CASE-CONTROL STUDY
R. Kivioja1,2, A. Pietilä3, N. Martinez-Majander1,2, A.S. Havulinna3, V. Salomaa3, D. Gordin4,5,6,7, M. Kaste1,2, T. Tatlisumak8,9, J. Putaala1,2
1Helsinki University Hospital, Department of Neurology, Helsinki, Finland
2University of Helsinki, Clinical Neurosciences- Neurology, Helsinki, Finland
3National Institute for Health and Welfare, Health Monitoring Unit- Department of Health, Helsinki, Finland
4Helsinki University Central Hospital, Abdominal Center Nephrology, Helsinki, Finland
5University of Helsinki, Abdominal Center Nephrology, Helsinki, Finland
6University of Helsinki, Research Programs Unit- Diabetes and Obesity, Helsinki, Finland
7Folkhälsan Research Center, Folkhälsan Institute of Genetics, Helsinki, Finland
8Sahlgrenska Academy at the University of Gothenburg, Institute of Neuroscience and Physiology, Gothenburg, Sweden
9Sahlgrenska University Hospital, Department of Neurology, Gothenburg, Sweden
Abstract
Background: Recent studies have shown a high prevalence of vascular risk factors in young adults with ischemic stroke (IS). However, the strength of association of such risk factors for the early-onset IS has not been established.
Methods: Patients with first-ever ischemic stroke at age of 25–49 years (n = 961) were compared with sex- and age-matched (5-year bands) stroke-free controls (n = 1403) from a population-based cohort (FINRISK). Risk factors assessed were: family history of stroke, dyslipidemia (LDL-cholesterol ≥3.0 mmol/L, HDL-cholesterol <1.0 mmol/L, or triglycerides ≥2.0 mmol/L), current smoking, hypertension, cardiovascular disease (any of coronary heart disease, history of myocardial infarction, heart failure, or peripheral arterial disease), atrial fibrillation (AF), type 1 (T1D) and type 2 diabetes mellitus (T2D), and active malignancy. Sex, age group, and each risk factor with significant association in univariate comparison were entered in a logistic regression model.
Results: In multivariate-adjusted logistic regression, significant risk factors for IS in order of strength of the association were: AF (odds ratio 39.48, 95% confidence interval 5.26–296.19), cardiovascular disease (18.39, 7.30–46.29), T1D (5.91, 2.70–12.93), T2D (3.08, 1.77–5.36), active malignancy (2.90, 1.02–8.24), current smoking (1.79, 1.48–2.17), low HDL-cholesterol (1.78, 1.30–2.43), family history of stroke (1.45, 1.08–1.94), and hypertension (1.41, 1.15–1.74).
Conclusions: Our study showed stronger associations than expected for AF, cardiovascular disease and both types of diabetes. This may indicate that these comorbidities represent more aggressive forms of diseases predisposing to severe vascular endpoint early in life.
AS28-024
STROKE IN THE YOUNG
Oral
TEMPORAL TRENDS IN STROKE INCIDENCE IN YOUNG PEOPLE: A SYSTEMATIC REVIEW
C. Scott1, R. Wharton1, Z. Mehta1 and P. Rothwell1
1Stroke Prevention Research Unit, Nuffield Department of Clinical Neurosciences Clinical Neurology, Oxford, United Kingdom
Abstract
Background: In recent decades, overall stroke incidence has fallen in high-income countries, but it is uncertain whether this has occurred in younger age groups. We aimed to determine temporal trends in stroke incidence at younger ages (<60 years) in high income countries.
Methods: We searched to 2015 (Pubmed/Medline/Google/bibliographies/abstracts) for studies in high income settings, that reported stroke incidence (or requisite raw numbers) stratified by age, over a period of several years after 1970 (continuously or periodically) in the same population. Relative temporal change in incidence in younger vs older age groups (temporal rate ratio) was calculated within study and meta-analysed (fixed/random effects models).
Results: Our search (figure 1) identified 17 population-based time-trend studies and 17 eligible administrative data studies. On pooled analysis, incidence of stroke at younger ages increased over the last few decades (<45 years - annual increment/100,000 = 0.19, 0.07–0.30, p = 0.0008; 16 studies), whereas incidence declined in older age groups. The age-difference in temporal trend was best reflected in the relative temporal rate ratio (<55 vs ≥55: 1.40, 1.27–1.55, p < 0.0001; 17 studies).
Conclusions: That incidence of “young stroke” in high-income countries is not declining in the same way as stroke in older age groups should inform projections of future stroke incidence and research into aetiology of “young stroke” as well as possible age-related investigation/ascertainment biases.
AS28-025
STROKE IN THE YOUNG
Oral
CANNABIS USE AND ISCHEMIC STROKE IN YOUNG SUBJECTS: A PROSPECTIVE STUDY OF 114 PATIENTS
C. Séchet1, F. Toulgoat2 and M. Sévin1
1CHU de Nantes, Neurology, Nantes, France
2CHU de Nantes, Neuroradiology, Nantes, France
Abstract
Background: Etiology of ischemic stroke (IS) in young adults often remains undetermined. Recent data suggest that cannabis consumption could trigger multiple intracranial vasospasm and may be a risk factor for stroke.
Methods: A systematic urine screening and structured interview for recent cannabis use were performed in 114 consecutive patients aged 15 to 55 years, admitted for acute IS. Other investigation included complete cardiac work-up and intracranial vessel imaging. All patients were followed at 3 months post-stroke.
Results: Median age was 44 years, and 32% were female. Recent cannabis consumption before IS was found in 18 of 114 cases (16%). Most of the cannabis-positive cases were chronic cannabis users. Cannabis-positive patients were significantly younger, more frequent tobacco smokers and illicit drugs users, compared with cannabis-negative patients. Other stroke characteristics and etiological distribution did not differ between the two groups. According to Naranjo scale, a causal link between cannabis and IS was definite or probable in 50% of cases. Multiple intracranial stenosis were present in 2 of 18 cannabis-positive cases. At follow-up, 53% of positive cases still smoked cannabis. Three-month rate of stroke recurrence was higher in cannabis-positive cases than in negative patients (22% vs 1%, p 0,002)
Conclusions: Cannabis use is frequent in young patients with IS, and may be associated with worse outcome. Several etiological mechanisms seem to be involved. Systematic cannabis screening and appropriate addictologic care should be performed early in all young patients with IS. Further research is needed to better determine the frequency and pathophysiology of IS linked to cannabis use.
AS28-031
STROKE IN THE YOUNG
Oral
CANNABIS AND STROKE FAMILY HISTORY ARE PREDICTIVE FACTORS FOR STROKE IN A CASE-CONTROL STUDY THE GENESYS STUDY: GENOMIC STUDY IN YOUNG PATIENTS WITH ISCHEMIC STROKE
S. Timsit1, S. Redon2, T. Ronziere3, F. Rouhart4, C. Breuilly5, B. Guillon6, F.M. Merrien4, V. Golfier7, C. Veduva7, G. Taurin8, S. Debiais9, G. Marc10, A. Tirel4, P. Goas4, I. Viakhireva-Dovganyuk4 and C. Ferec2
1CHRU Brest- Inserm 1078, Neurology & Stroke Unit, Brest, France
2Inserm 1078, Genetic, Brest, France
3CHRU Rennes, Neurology & Stroke Unit, Rennes, France
4CHRU Brest, Neurology & Stroke Unit, Brest, France
5CHIC Quimper, Neurology, Quimper, France
6CHU Nantes, Neurology, Nantes, France
7CH Saint-Brieuc, Neurology & Stroke Unit, Saint-Brieuc, France
8CH Saint-Malo, Neurology & Stroke Unit, Saint-Malo, France
9CHU Tours, Neurology & Stroke Unit, Tours, France
10CHU Angers, Neurology & Stroke Unit, Angers, France
Abstract
Background: The weight of environmental and genetic factors in young patients with ischemic stroke (IS) is not well characterized. The goal of this study was to identify potential non-genetic and genetic risk factors by studying personal and family (first degree) medical history as well as genomic copy number variations (CNV). In this study, we will only present non-genetic data.
Methods: In this multicenter (Brest, Rennes, Quimper, Nantes, Saint-Brieuc, Saint Malo, Tours, Angers) case-control study, patients under 40 year-old with ischemic stroke were compared to controls. Data were collected prospectively from 2009 to 2014 for demographics, clinical presentation, vascular risk factors and exposition to alcohol and drugs. IS were compared to controls by univariate and multivariate analyzes (p < 0.05).
Results: 300 IS and 302 controls were collected. Diagnostic work-up for the index stroke included cerebral imaging, EKG, cardiac imaging, neck vessel and intracerebral vessel studies. Univariate analysis showed that age, smoking, migraine with aura, hypertension, hypercholesterolemia, cannabis, combined pill in women, stroke and myocardial infarction family history where higher in the IS group while alcohol was higher in controls. Controlling for age and sex, multivariate analysis showed that predictors of IS were: age (OR = 1.53 for 5-year increment; 95% CI [1.32–1.78]); smoking (2.91; [1.91–4.45]); cannabis (1.73; [1.09–2.76], p = 0.020); stroke family history (2.38; [1.04–5.42]), migraine with aura (10.73; [4.25–27.10]), hypertension (8.13;[1.81–36.50]). On the contrary, alcohol was a predictor of controls (0.36; [0.22–0.61]).
Conclusions: This study provides new evidences for the importance of cannabis consumption, and family history of stroke in young patients with stroke.
AS28-033
STROKE IN THE YOUNG
Oral
THE VERY LONG-TERM RISK AND PREDICTORS OF RECURRENT ISCHEMIC EVENTS AFTER A STROKE AT YOUNG AGE: THE FUTURE-STUDY
M. van Alebeek1, R. Arntz1, N. Synhaeve2, J. van Pamelen2, N. Maaijwee1, H. Schoonderwaldt1, M. van der Vlugt3, E.J. van Dijk1, L. Rutten-Jacobs4 and F.E. de Leeuw1
1Radboud university medical center, Neurology, Nijmegen, Netherlands
2St. Elisabeth Hospital, Neurologie, Tilburg, Netherlands
3Radboud university medical center, Cardiology, Nijmegen, Netherlands
4University of Cambridge, Clinical Neurosciences, Cambridge, United Kingdom
Abstract
Background: Patients with a stroke at young age remain at risk of recurrent vascular events. However, information on this and their risk factors is unavailable.
Methods: Prospective cohort study among 656 patients with a first-ever ischemic stroke or TIA, aged 18–50, who visited the RadboudUMC between 1980- 2010 (Follow-up in 2015). Outcomes included cerebral ischemia and other arterial events. Kaplan-Meier analysis quantified the cumulative risks. Prediction model was made to assess baseline risk factors associated with recurrent ischemic events, using cox proportional hazard analyses.
Results: Mean follow-up was 12.4 (SD 8.2) years; 11.1% had a follow-up over 25 years. 25-Years cumulative risk of any ischemic event was 45.4% (95%CI 39.4–51.5), 30.1% (95%CI 24.8–35.4) for cerebral ischemia and 27.0% (95% CI 21.1–33.0) for other arterial events. Patients with large artery (61.4%, 95%CI 51.1–71.8) or cardio-embolic stroke (62.7%, 95%CI 38.6–86.7) had a higher cumulative risk of any ischemic event compared to undetermined cause (33.8%, 95%CI 24.3–43.2) (Log-rank p < 0.001 and p = 0.001 respectively). Risk factors associated with any ischemic event were smoking (HR 1.35, 95%CI 1.04–1.74), poor kidney function (HR 2.10, 95%CI 1.32–3.35), history of peripheral arterial disease (HR 2.10, 95%CI 1.08–3.76) and history of cardiac disease (HR 1.84, 95%CI 1.06–3.18). C-statistics of the model was 0.59 (95%CI 0.55–0.64).
Conclusions: Young stroke patients remain at risk for recurrent vascular events, even decades after their initial stroke. Among those with “old age vascular risk factors” the level of suspicion of their treating physicians should be raised as they are at the highest risk for future vascular events.
AS28-034
STROKE IN THE YOUNG
Oral
MRI-VISIBLE PERIVASCULAR SPACES AS A NEUROIMAGING BIOMARKER IN FABRY DISEASE: CASE CONTROL STUDY
D. Lyndon1, D. Wilson1, I. Davagnanam1, F. Jichi2, A. Merwick1, F. Bolsover3, H.R. Jäger4, L. Cipolotti5, C.A. Gandini Wheeler-Kingshott6, E. Murphy3, R. Lachmann3 and D.J. Werring1
1Institute of Neurology, Brain repair and rehabilitation, London, United Kingdom
2University College London, Department of biostatistics, London, United Kingdom
3National Hospital for Neurology and Neurosurgery, Charles Dent Metabolic Unit, London, United Kingdom
4Institute of Neurology, Neuroradiological academic unit- Department of Brain repair and rehabilitation, London, United Kingdom
5National Hospital for Neurology and Neurosurgery- Queen Square-, Department of Neuropsychology, London, United Kingdom
6University College of London Institute of Neurology, Department of Neuroinflammation Queen Square MS Centre-, London, United Kingdom
Abstract
Background: Fabry disease (FD) is an X-linked lysosomal storage disorder resulting in vascular glycosphingolipid accumulation and increased stroke risk. Established MRI findings include white matter hyperintensities (WMH) and cerebral microbleeds (CMBs) but the underlying mechanisms remain uncertain. MRI-visible perivascular spaces (PVS) are a promising marker of small vessel disease presence and mechanism. We investigate whether PVS (in addition to CMBs, lacunes and WMHs) are associated with FD.
Methods: We compared genetically-proven FD patients to healthy controls. PVS, WMH, lacunes and CMBs were rated on standardized sequences using validated criteria and scales, blinded to diagnosis. Basal ganglia (BG) and centrum semiovale PVS scores were dichotomized into mild (0 – 1) or severe (2 – 4) and analysed using logistic regression; ordered logistic regression was used for total PVS (composite of all PVS scores) and WMH scores.
Results: We included 33 FD patients (median age 44, 55.9% female) and 20 controls (median age 33.5, 50% female). Adjusting for age and sex, FD was associated with severe BG-PVS (OR 5.80, 95% CI 1.03–32.70, p = 0.046) and total PVS score (OR 4.03, 95% CI 1.37–11.89, p = 0.01). WMH scores were higher in FD (OR 4.19, 95%CI 1.22–14.40, p = 0.02). CMBs were present in 15% of the FD patients but none of the controls (p = 0.04). Lacunes were present in 18% of FD patients and 2.0% of controls (p = 0.23).
Conclusions: BG and total PVS scores are more severe in FD than control subjects, and may have value for diagnosis and understanding disease mechanisms.
AS28-035
STROKE IN THE YOUNG
Oral
CANNABIS USE AS A RISK OF STROKE IN YOUNG MEN LESS THAN 45 YEARS IN A 40-YEAR COHORT STUDY
V. Wolff1, D. Falkstedt2, A.K. Danielsson2 and P. Allebeck2
1Hôpital de Hautepierre CHU de Strasbourg, neurology, STRASBOURG Cedex, France
2Karolinska Institutet, Department of Public Health Sciences, Stockholm, Sweden
Abstract
Background: Stroke among the young is a real challenge for neurologists to search for risk factors and etiologies. Cannabis has recently been identified as a possible risk factor for stroke.
Methods: The aim of our study was to assess the risk of stroke among cannabis users in a population-based cohort study of Swedish men (n = 45,528) aged 18–20 years conscripted and examined for compulsory military training in 1969–1970. Participants were followed until 2009, and stroke occurrence was assessed by linkage to the national inpatient register.
Results: There were 5156 (10.5%) lifetime cannabis users and 831 (1.7%) heavy cannabis users at the baseline conscription assessment. In the whole cohort, 1160 (2.5%) participants developed a stroke (∼40% ischemic, ∼20% hemorrhagic) over the 40-year follow-up period. Among these stroke patients, 105 (0.2%) occurred before age of 45, and 9 of them were cannabis users. Use of cannabis >10 times was positively associated with increased risk of stroke under 45 years [10 to 50 times: odds ratio = 1.30 (0.32–5.28); use of cannabis more than more than 50 times: odds ratio = 1.83 (0.58–5.79)], however this association was reduced when controlling for tobacco smoking [more than 50 times: odds ratio = 1.07 (0.33–3.43)].
Conclusions: With reservation for large confidence intervals, use of cannabis in adolescence was associated with increased risk of stroke under 45 years in a longitudinal cohort of young men, but this association was not independent of tobacco use. In clinical practice, it is necessary to ask young stroke patients about their frequency of lifestyle risk factors use including tobacco and cannabis.
AS07-014
STROKE PROGNOSIS
Oral
ONE-MONTH MODIFIED RANKIN SCORE (mRS) PREDICTS FIVE-YEAR DISABILITY, DEATH, AND HEALTHCARE COSTS IN ISCHAEMIC STROKE: IMPLICATIONS FOR OUTCOME MEASUREMENT IN HYPERACUTE STROKE TRIALS
A. Ganesh1,2, R. Luengo-Fernandez3, R.M. Wharton1, S.A. Gutnikov1, L.E. Silver1, Z. Mehta1, P.M. Rothwell1 and O.B.O. the Oxford Vascular Study
1
1University of Oxford, Stroke Prevention Research Unit- Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
2University of Calgary, Department of Clinical Neurosciences, Calgary, Canada
3University of Oxford, Health Economics Research Centre- Department of Public Health, Oxford, United Kingdom
Abstract
Background: Outcome in hyperacute stroke trials is often based on short-term mRS. However, there are few data from high-quality population-based studies on how short-term functional status translates into long-term outcomes. We evaluated the relationship between 1-month mRS and 5-year disability, death, and healthcare cost in a population-based prospective cohort study.
Methods: In 3-month survivors of ischaemic stroke in the Oxford Vascular Study (2002–2014), we performed logistic regression to determine predictors of 5-year disability and death, including mRS score at 1 month, age, and sex. Hospital resource use data up to 31 August 2015 were collected; a general gamma linear model was used with the 1-month mRS controlling for age, gender, and cardiovascular comorbidities.
Results: Among 1,409 3-month survivors, mRS score was a strong independent predictor (p < 0.0001) of disability or death at 5 years, gaining additional predictive value with each increment of the scale: mRS = 0 (reference); mRS = 1 adjusted OR: 2.15, 95%CI 1.39–3.31; mRS = 2: 2.65,1.67–4.18; mRS = 3: 14.82,7.61–28.85; mRS = 4: 16.42,7.76–34.72, mRS = 5: 86.82,11.63–647.97. Predictive values were similar for 5-year mortality alone (p < 0.0001). mRS level was the only significant independent predictor of 5-year healthcare costs (p < 0.001) aside from age, with a major step-change again between mRS 2 and 3.
Conclusions: Our results reaffirm the current practice in hyperacute trials of using the short-term mRS as the primary outcome measure, with strong associations for 5-year disability, death and healthcare costs. The step-change between mRS 2 and 3 supports the standard dichotomy, although it does not fully account for overall predictive value.
AS17-028
STROKE PROGNOSIS
Oral
DEVELOPMENT OF A PREDICTION MODEL FOR MAJOR BLEEDING IN PATIENTS WITH CEREBRAL ISCHAEMIA
N. Hilkens1, A. Algra2, H.C. Diener3, L. Csiba4, W. Hacke5, J. Kappelle6, P. Koudstaal7, D. Leys8, J.L. Mas9, R. Sacco10, J. Sivenius11 and J. Greving1
1University Medical Center Utrecht, Julius Center for Health Sciences and Primary Care, Utrecht, Netherlands
2University Medical Center Utrecht, Julius Center for Health Sciences and Primary Care- Department of Neurology and Neurosurgery- Brain Center Rudolf Magnus, Utrecht, Netherlands
3University Hospital Essen, Department of Neurology, Essen, Germany
4University of Debrecen Medical and Health Science Center, Department of Neurology, Debrecen, Hungary
5University of Heidelberg, Department of Neurology, Heidelberg, Germany
6University Medical Center Utrecht, Department of Neurology and Neurosurgery- Brain Center Rudolf Magnus, Utrecht, Netherlands
7Erasmus Medical Center, Department of Neurology, Rotterdam, Netherlands
8Roger Salengro Hospital, Department of Neurology, Lille, France
9Hôpital Sainte-Anne- Université Paris Descartes, Department of Neurology, Paris, France
10Miller School of Medicine, Department of Neurology, Coral Gables, USA
11University Hospital of Kuopio and University of Eastern Finland, Department of Neurology, Kuopio, Finland
Abstract
Background: Antiplatelet therapy is widely used in secondary prevention after cerebral ischaemia, but leads to an increased bleeding risk. Our aim was to develop a prediction model to estimate 1-year risk of major bleeding in patients with cerebral ischaemia.
Methods: We combined individual patient data from six randomised clinical trials (CAPRIE, ESPS-2, MATCH, CHARISMA, ESPRIT and PRoFESS) investigating antiplatelet therapy after cerebral ischaemia. Patients with likely cardio-embolic stroke were excluded from the development population, as well as patients randomised to placebo or dipyridamole alone, leaving 43,112 patients for the analyses. Major bleeding was defined as bleeding that was fatal, intracranial, requiring hospital admission or led to significant disability. A Cox regression model was fit to predict 1-year risk of major bleeding. Performance of the model was assessed with the c-statistic and calibration plots.
Results: Major bleeding occurred in 1521 patients during 93,847 person years of follow-up. The observed 1-year risk of major bleeding was 1.8% (95%CI 1.7–1.9). Predictors for major bleeding were age, male sex, Asian ethnicity, lower BMI, current smoking, modified Rankin score ≥3, hypertension, prior stroke, diabetes, and type of antiplatelet agents. A model that combined these ten predictors had a c-statistic of 0.63 (0.61–0.64) and showed good calibration. The estimated 1-year major bleeding risk ranged from 0.5% to 12%.
Conclusions: This prediction model can be used to estimate one year major bleeding risk in patients with cerebral ischaemia, based on easily available patient characteristics. The model may be improved by identifying stronger predictors for major bleeding.
AS07-024
STROKE PROGNOSIS
Oral
PREDICTIVE VALUE OF ABCD2 AND ABCD3-I SCORES IN TIA AND MINOR STROKE IN THE STROKE UNIT SETTING
M. Knoflach1, W. Lang2, L. Seyfang3, F. Elisabeth4, S. Oberndorfer5, G. Daniel6, T. Seifert-Held7, M. Brainin8, S. Krebs2, B. Matosevic1, T. Toell1, S. Kiechl1, J. Willeit1 and J. Ferrari2
1Medical University of Innsbruck, Neurology, Innsbruck, Austria
2Hospital Barmherzige Brueder, Neurology, Vienna, Austria
3Danube University Krems and Gesundheit Österreich GmbH/BIQG, Vienna, Austria
4Hospital Rudolfstiftung, Neurology, Vienna, Austria
5University Clinic St Pölten- KLPU, Neurology, St. Poelten, Austria
6Hospital Wilhelminenspital, Neurology, Vienna, Austria
7Medical University of Graz, Neurology, Graz, Austria
8Danube University Krems, Clinical Neurosciences and Preventive Medicine, Krems, Austria
Abstract
Background: It is not clear whether risk scores for early stroke recurrence after TIA that have been mainly established in out-patient and emergency department settings are valid on the background of highly specialized stroke unit care.
Methods: ABCD2 and ABCD3-I-scores have been prospectively documented in a cohort of patients admitted on Austrian stroke units within 24 hours of symptom onset with TIA or minor stroke (NHISS score <4).
Results: 5237 TIA and minor stroke patients met inclusion criteria with 3 month follow-up data available on 2557. Early and 3-month stroke were observed in 2.4% and 4.2% of the study population. The probability of early stroke during the stroke unit stay (median 2 (interquartile range 1 – 3) days) steadily increased from 0% to 4.8% and 0% to 16.7% with increasing ABCD2 and ABCD3-I-score points, respectively. On 3-month follow-up, stroke risk increased from 0% to 8.0% and 0% to 23.8% with increasing ABCD2 and ABCD3-I-score points, respectively. Of the individual score components, age, blood pressure and diabetes were not related to early or 3-month stroke, whereas clinical presentation (C), symptom duration (D) and cerebral as well as carotid imaging (I) were. A simplified ‘CDI-score’ performed similarly well in the risk prediction of stroke as the full ABCD3-I-score.
Conclusions: Standard ABCD2 and ABCD3-I-scores and a simplified CDI-score are useful instruments to estimate the probability of early and 3-month stroke in TIA and minor stroke patients treated at specialized stroke units.
AS17-062
STROKE PROGNOSIS
Oral
ASTRAL PROGNOSTIC SCORE HAS A HIGH PROGNOSTIC ACCURACY IN DIFFERENT ISCHAEMIC STROKE MECHANISMS
V. Papavasileiou1,2, G. Ntaios3, C. Weimar4, K.R. Lees5, N. Kakaletsis6, K. Vemmos7, E. Manios7, D. Strbian8, T. Tatlisumak8, J.H. Heo9, T.J. Song9,10, D.J.I.J. Seiffge11, J. Ferrari12, S. Moulin13, B. Yan14, B.J. Weder15, C.W. Cereda6,16, E. Mori17, M. Kurniawan18 and P. Michel6
1Leeds Teaching Hospitals NHS Trust, Department of Neurosciences, Leeds, United Kingdom
2Leeds Institute of Biomedical and Clinical Sciences- Faculty of Medicines and Health- University of Leeds, School of Medicine, Leeds, United Kingdom
3Larissa University Hospital- School of Medicine- University of Thessaly, Department of Medicine, Larissa, Greece
4University Hospital of Essen, Stroke Unit and Department of Neurology, Essen, Germany
5Institute of Cardiovascular & Medical Sciences- University of Glasgow, BHF Cardiovascular Research Centre, Glasgow, United Kingdom
6Centre Hospitalier Universitaire Vaudois and University of Lausanne, Neurology Service, Lausanne, Switzerland
7Medical School of Athens- Alexandra Hospital, Department of Clinical Therapeutics, Athens, Greece
8Helsinki University Central Hospital, Department of Neurology, Helsinki, Finland
9Severance Hospital- Yonsei University- College of Medicine, Department of Neurology, Seoul, United Kingdom
10Ewha Womans University, School of Medicine, Korea, United Kingdom
11University Hospital Basel- University of Basel, Stroke Center and Depatment of Neurology, Basel, Switzerland
12St. John´s of God Hospital, Department of Neurology, Vienna, Austria
13University of Lille- Roger Salengro Hospital, Stroke Unit- Department of Neurology, Lille, France
14University of Melbourne- Royal Melbourne Hospital, Melbourne Brain Centre- Department of Neurology, Melbourne, Australia
15Kantonsspital St.Gallen, Stroke Center- Department of Neurology, St Gallen, Switzerland
16Neurocenter of Southern Switzerland, Stroke Center- Neurology Department, Lugano, Switzerland
17Tohoku University Graduate School of Medicine, Department of Behavioral Neurology and Cognitive Neuroscience, Sendai, Japan
18Cipto Mangunkusumo National Hospital- Faculty of Medicine- University of Indonesia, Stroke Unit- Department of Neurology, Jakarta, Indonesia
Abstract
Background: The ASTRAL prognostic score reliably predicts unfavourable functional outcome (mRS > 2) at 3 months after an acute ischemic stroke. The aim of the present study was to assess ASTRAL score’s accuracy in TOAST (Trial of Org 10172 in Acute Stroke Treatment) classification subgroups.
Methods: Stroke databases from multiple countries and the Virtual International Stroke Trials Archive (VISTA) recording the 6 variables of ASTRAL prognostic score [Age, Severity (NIHSS), Time delay from symptom onset to admission, Range of visual field defect, Acute glucose, Level of consciousness] and 3-month outcome were identified. ASTRAL score’s discriminatory power for the 3-month unfavourable outcome (mRS > 2), in the different TOAST subgroups, was assessed by the area under the receiver operating characteristic curve (AUC) and the calculation of the 95% Confidence Interval (95%CI). All data were handled in an anonymized way and approval of the local ethics committee was available for all participating databases.
Results: A total of 11,763 patients from 8 European databases, 3 Asians and 1 from Australia along with the VISTA participated in the study. The mean age was 68.4 ± 13.4years and the median NIHSS was 9 (IQR:4–15). As per TOAST classification, the predictive accuracy of ASTRAL score for the 3-month unfavourable outcome was AUC:0.817 (95%CI: 0.798–0.836) in the large-vessel (n = 1912), AUC:0.815 (0.802–0.828) in cardioembolic (n = 4000), AUC:0.862 (0.842–0.882) in lacunar (n = 1622), AUC:0.799 (0.762–0.836) in other determined aetiology (n = 582), and AUC:0.830 (0.816–0.843) in the undetermined aetiology strokes (n = 3598).
Conclusions: ASTRAL score shows a high accuracy in predicting 3-month unfavourable outcome in all TOAST classification subgroups.
AS17-063
STROKE PROGNOSIS
Oral
ASTRAL PROGNOSTIC SCORE HAS A HIGH PROGNOSTIC ACCURACY IN BOTH THROMBOLYZED AND NON-THROMBOLYZED PATIENTS WITH ACUTE ISCHAEMIC STROKE
V. Papavasileiou1,2, G. Ntaios3, C. Weimar4, K.R. Lees5, A. Eskandari6, K. Vemmos7, E. Manios7, D. Strbian8, T. Tatlisumak8, J.H. Heo9, T.J. Song9,10, D.J. Seiffge11, J. Ferrari12, S. Moulin13, B. Yan14, B.J. Weder15, C.W. Cereda6,16, E. Mori17, M. Kurniawan18 and P. Michel6
1Leeds Teaching Hospitals NHS Trust, Department of Neurosciences, Leeds, United Kingdom
2Leeds Institute of Biomedical and Clinical Sciences- Faculty of Medicines and Health- University of Leeds, School of Medicine, Leeds, United Kingdom
3Larissa University Hospital- School of Medicine- University of Thessaly, Department of Medicine, Larissa, Greece
4University Hospital of Essen, Stroke Unit and Department of Neurology, Essen, Germany
5Institute of Cardiovascular & Medical Sciences- University of Glasgow, BHF Cardiovascular Research Centre, Glasgow, United Kingdom
6Centre Hospitalier Universitaire Vaudois and University of Lausanne, Neurology Service, Lausanne, Switzerland
7Medical School of Athens- Alexandra Hospital, Department of Clinical Therapeutics, Athens, Greece
8Helsinki University Central Hospital, Department of Neurology, Helsinki, Finland
9Severance Hospital- Yonsei University- College of Medicine, Department of Neurology, Seoul, United Kingdom
10Ewha Womans University, School of Medicine, Seoul, United Kingdom
11University Hospital Basel- University of Basel, Stroke Center and Department of Neurology, Basel, Switzerland
12St. John´s of God Hospital, Department of Neurology, Vienna, Austria
13University of Lille- Roger Salengro Hospital, Stroke Unit- Department of Neurology, Lille, France
14University of Melbourne- Royal Melbourne Hospital, Melbourne Brain Centre- Department of Neurology, Melbourne, Australia
15Kantonsspital St.Gallen, Stroke Center- Department of Neurology, St GAllen, Switzerland
16Neurocenter of Southern Switzerland, Stroke Center- Neurology Department, Lugano, Switzerland
17Tohoku University Graduate School of Medicine, Department of Behavioral Neurology and Cognitive Neuroscience, Sendai, Japan
18Cipto Mangunkusumo National Hospital- Faculty of Medicine- University of Indonesia, Stroke Unit- Department of Neurology, Jakarta, Indonesia
Abstract
Background: The ASTRAL prognostic score, developed in a general acute ischemic stroke (AIS) population (including both thrombolyzed and non-thrombolyzed patients), reliably predicts unfavourable functional outcome. The aim of the present study was to assess ASTRAL score’s accuracy separately in thrombolyzed and non-thrombolyzed AIS populations from multiple AIS databases.
Methods: Patients from 12 AIS databases from different countries, and the Virtual International Stroke Trials Archive (VISTA) were used if they had all 6 variables of the ASTRAL score recorded [Age, Severity (NIHSS), Time delay from symptom onset to admission, Range of visual field defect, Acute glucose, Level of consciousness] and if their 3-month outcome was available. Unfavourable outcome was defined as a modified Rankin Scale (mRS) >2. ASTRAL score’s discriminatory power was assessed by the area under the receiver operating characteristic curve (AUC) in the thrombolyzed patients and those who did not receive any specific recanalization treatment. Patients with acute endovascular treatment were excluded from this analysis.
Results: A population of 13,353 patients [5,447 thrombolyzed, mean age 68.0 ± 13.4years, median NIHSS 12(IQR:7–17) versus 7,906 non-thrombolyzed, mean age 68.7 ± 13.3 years, median NIHSS 7(IQR:3–13)] from 12 databases and the VISTA participated in the analysis. The AUC in the non-thrombolyzed and the thrombolyzed population was 0.848 (95%CI:0.839–0.857) and 0.789 (95%CI:0.778–0.801) respectively (p < 0.001).
Conclusions: ASTRAL score shows a high accuracy in predicting 3-month unfavourable outcome both in thrombolyzed and non-thrombolyzed acute ischemic stroke patients. The higher accuracy in the non-thrombolyzed group could be due to the higher proportion of such patients in the original development cohort of the ASTRAL score.
AS17-057
STROKE PROGNOSIS
Oral
ASTRAL, DRAGON & SEDAN SCORES PREDICT STROKE OUTCOME MORE ACCURATELY THAN PHYSICIANS
G. Ntaios1, F. Gioulekas2, V. Papavasileiou3, D. Strbian4 and P. Michel5
1University of Thessaly, Department of Medicine, Larissa, Greece
2General University Hospital of Larissa, Sub-Directorate of Informatics, Larissa, Greece
3Salford Royal NHS Foundation Trust- Manchester Academic Health Sciences Centre- Salford Royal Foundation Trust, Comprehensive Stroke Centre, Manchester, United Kingdom
4Helsinki University Central Hospital, Department of Neurology, Helsinki, Finland
5Centre Hospitalier Universitaire Vaudois and University of Lausanne, Stroke Center- Neurology Service, Lausanne, Switzerland
Abstract
Background: ASTRAL, SEDAN and DRAGON scores are three well-validated scores for prediction of stroke outcome. We investigated whether these scores predict stroke outcome more accurately compared with physicians interested in stroke.
Methods: Physicians interested in stroke were invited to an online anonymous survey to provide estimates of outcome in randomly-allocated structured scenarios of recent real stroke patients. Their estimates were compared to predictions based on the scores in the same scenarios. An estimate was considered accurate if within 95% confidence intervals (CI) of actual outcome.
Results: There were 244 responses by participants from 32 different countries assessing 720 real scenarios and 2636 outcomes. The majority of physicians’ estimates fell outside the 95%CI of actual outcome (1422/2636, 53.9%).
400 (56.8%) of physicians’ estimates about the %probability of 3-month modified-Rankin-score (mRS) > 2 fell within 95%CI of actual outcomes compared with 609 (86.5%) estimates by ASTRAL score (p < 0.0001).
394 (61.2%) of physicians’ estimates about %probability of post-thrombolysis sICH fell within 95%CI of actual outcomes compared with 583 (90.5%) estimates by SEDAN score (p < 0.0001) (upper panel). 160 (24.8%) of physicians’ estimates about post-thrombolysis 3-month %probability of mRS:0–2 fell within the 95%CI of actual outcomes compared with 240 (37.3%) estimates by DRAGON score (p < 0.0001) (middle panel). 260 (40.4%) of physicians’ estimates about the %probability of post-thrombolysis mRS:5–6 fell within 95%CI of actual outcomes compared with 518 (80.4%) estimates by DRAGON (p < 0.0001) (lowerpanel).
Conclusions: ASTRAL, DRAGON and SEDAN scores predict outcome of acute ischemic stroke patients with higher accuracy compared to physicians interested in stroke.
AS23-007
STROKE PROGNOSIS
Oral
PROGNOSTIC IMPORTANCE OF THE ECHOGRAPHIC RISK INDEX OF CAROTID ATHEROSCLEROTSIS (ERICA): A MULTICENTER SWISS STUDY ON ASYMPTOMATIC 60-80% OR SYMPTOMATIC 50-69% CAROTID STENOSES
R. Sztajzel1, H. Muller1, S. Engelter2, L. Bonati2, P. Lyrer2, G. Kägi3, M. Kapauer3, M.L. Mono4, K. Nedeltchev5, R. Baumgartner6, L. Hirt7 and C. Bonvin8
1Geneva University Hospital, Neurology, Geneva 14, Switzerland
Background: To determine the prognostic value of a Risk index (RI) combining degree of stenosis and carotid plaque echogenicity
Methods: Consecutive patients with 60–80% asymptomatic or 50–69% symptomatic carotid stenoses were included. Degree of stenosis was assessed on longitudinal colour-Duplex imaging sections. A semi-automated grey-scale based colour mapping (red, yellow and green) of the whole plaque and of its surface was achieved. Risk index (RI) was based upon a combination of degree of stenosis and the predominance of the red colour (reflecting low echogenicity) on the surface of the plaque. Ultrasound was performed every 6 months.
Results: Overall 199 patients with 207 carotid stenosis were included. Of these 182 were asymptomatic and 25 symptomatic. RI as well as predominance of the red colour at the surface were increased among patients with symptomatic stenosis at baseline (respectively p < 0.001 and p < 0.0001). Follow-up (mean 23.9 months) could be performed upon 147 patients during which 15 experienced a stroke or TIA. Kaplan-Meyer curves showed that RI (>0.2) as well as predominance of the red colour on the surface (>75%) predicted stroke or TIA occurrence (respectively p < 0.03 and p < 0.004, sensitivity and specificity of 80% and 52% and 93% and 52% respectively).
Conclusions: In our cohort of patients low echogenicity of plaque surface whether combined to degree of stenosis or not resulted to be an accurate predictor of stroke or TIA occurrence. Ultrasound evaluation of plaque surface may be therefore a valuable tool to assess the clinical risk of the carotid plaque.
AS17-084
STROKE PROGNOSIS
Oral
THE 12-YEAR RISK OF STROKE AND CORONARY EVENTS AFTER FOCAL AND NON-FOCAL TRANSIENT NEUROLOGICAL ATTACKS: A POPULATION-BASED STUDY
M.A. Tuna1, L. Li1, A. Tornada2, L. Gaziano3, S. Gutnikov1, Z. Mehta1 and P. Rothwell1
1Oxford University, Nuffield Department of Clinical Neuroscience, Oxford, United Kingdom
2Hospital de Cascais, Department of Medicine, Cascais, Portugal
3Washington and Lee University, Biochemistry Department, Lexinghton- Virginia, USA
Abstract
Background: Since patients with TIA require intensive long-term secondary prevention, the distinction between a TIA and a transient neurological attack (TNA – a TIA-like event not satisfying the NINDS Criteria) has important implications for clinical practice, but there are conflicting estimates of the prognosis of TNA.
Methods: In a population-based study of all TNAs with duration <24 hours and TIAs from 2002–2014 (Oxford Vascular Study), we prospectively classified all first events as TIA (NINDS criteria) or TNA, excluding other TIA-mimics of known non-vascular cause. TNAs were subclassified as focal (e.g. positive sensory symptoms, isolated dysarthria, isolated vertigo etc), non-focal (e.g. isolated confusion, bilateral visual disturbance, bilateral sensory disturbance etc) or mixed. Prognosis (risks of stroke/MI/sudden-cardiac-death-SCD) was compared on regular face-to-face follow-up to 12-years and in relation to the expected age/sex-specific stroke incidence in the underlying population.
Results: Among 1520 patients, 674 had NINDS-defined TIA (mean/SD age = 73.3/13.4) and 846 had TNA (68.3/14.7), of which 381 were focal (67.0/14.9), 228 non-focal (70.9/14.4) and 237 mixed (67.9/14.4). Focal-TNAs had a lower 12-year risk of stroke than NINDS-defined TIA (RR = 0.65, 0.46–0.92, p = 0.01) whereas non-focal (1.05, 0.73–1.51) and mixed (0.71, 0.47–1.07) TNAs had similar risks. However, for all groups of TNA, the risk was higher (all p < 0.001) than the expected underlying population stroke incidence: focal (RR = 3.4, 1.9–6.4); non-focal (4.4, 2.1–9.3) and mixed (5.0, 2.0–12.2). The pattern of relative risks of MI/SCD was similar.
Conclusions: The long-term prognosis of TNAs, especially those with non-focal symptoms, is not dissimilar to that after definite TIA.
AS09-043
STROKE PROGNOSIS
Oral
BETA-BLOCKERS, INFECTION AND OUTCOME IN ACUTE STROKE
W. Westendorp1, J.D. Vermeij1, M. Brouwer1, Y. Roos1, P. Nederkoorn1 and D. van de Beek1
1Academic Medical Center University of Amsterdam, Neurology, Amsterdam, Netherlands
Abstract
Background: Stroke-associated infections occur frequently and are associated with unfavorable outcome. Previous cohort studies suggest a protective effect of beta-blockers against infections. A sympathetic drive may increase immune suppression and infections. We report the association between beta-blocker treatment and post-stroke infection in the Preventive Antibiotics in Stroke Study, a prospective clinical trial.
Methods: In PASS, 2538 patients with acute phase of stroke (24 hours after onset) were randomized to ceftriaxone (intravenous, 2 g per day for 4 days) in addition to stroke unit care, or standard stroke unit care without preventive antibiotic treatment. All clinical data including use of beta-blockers was prospectively collected. Infection was diagnosed by the physician and by a blinded expert panel. Multivariate analysis was performed to investigate associations between beta-blocker treatment and infection rate.
Results: Infection as defined by the physician occurred in 348 of 2538 patients (14%). Multivariable analysis showed that use of beta-blockers at baseline was associated with development of infection during clinical course (aOR 1.61; 95%CI 1.19–2.18; p < 0.01). Beta-blocker use at baseline was also associated with development of pneumonia (aOR 1.56 95%CI 1.05–2.30; p = 0.03). Baseline beta-blocker use was not associated to mortality (aOR 1.14; 95%CI 0.84–1.53; p = 0.41) or unfavourable outcome at 3 months (aOR 1.10; 95%CI 0.89–1.35; p = 0.39).
Conclusions: Pre-stroke use of beta-blockers is not associated with lower infection rates, but with higher rate of infection and pneumonia.
AS01-005
THROMBOLYSIS: IMPROVING EFFICACY
Oral
TIME TO TREATMENT EFFECTS WITH ULTRA-EARLY INTRAVENOUS THROMBOLYSIS ON OUTCOME IN ACUTE ISCHEMIC STROKETHE STROKE EMERGENCY MOBILE (STEMO) WRITING GROUP
H. Audebert1, A. Kunz1, C. Nolte1, H. Erdur1, J. Fiebach1, G. Frederik1, M. Rozanski1, J. Scheitz1, K. Villringer1, C. Waldschmidt1, J. Weber1, M. Wendt1, B. Winter1, K. Zieschang1, U. Grittner1, S. Kaczmarek2, M. Endres1 and M. Ebinger1
1Center for Stroke Research- Charité Universitätsmedizin Berlin, Department of Neurology, Berlin, Germany
2Berliner Feuerwehr, Research, Berlin, Germany
Abstract
Background: Effects of intravenous thrombolysis (IVT) in ischemic stroke are time-sensitive. Because virtually no patients received IVT within 60 min of onset in randomized controlled trials, the impact of such early treatment on 3-month outcomes remains unknown. Pre-hospital thrombolysis on specialized CT-equipped ambulances offers the opportunity of treating patients within this time window.
Methods: We analyzed data from two registries of pre-hospital and in-hospital thrombolysis both operated by the Charité University Hospital Berlin. The study population consisted of patients who had lived at home without assistance pre-stroke, had witnessed time of onset and were admitted via conventional ambulance or STEMO. We tested the effects of onset-to-treatment time (OTT) on 3-month modified Rankin Scale (mRS) ≤ 1 and 3-month mortality in the first three 60 min OTT-intervals as compared to the OTT between 181 and 270 min. Outcomes were adjusted in multivariable regression for demographics, co-morbidities and stroke severity according to the National Institutes of Health Stroke Scale.
Results: From February 5, 2011 to March 5, 2015, 629 patients received IVT and had complete documentation (42% treated on STEMO, mean age 70.2 y, 42% female, median OTT: 90 min). Numbers of patients who received IVT were 134 within 60 min, 302 within 61–120 min, 111 within 121–180 min and 82 within 181–270 min. Odds ratios (OR) for mRS ≤ 1 were higher when treated earlier with OR 1.89 (95%CI: 1.01–3.55) for 0–60 min, 1.14 (0.66–1.95) for 61–180 min and 1.14 (0.62–2.12) for 121–180 min, while ORs for mortality were lower with OR: 0.26 (0.08–0.88), 0.42 (0.15–1.22), 0.91 (0.29–2.84) respectively.
Conclusions: Ultra-early intravenous thrombolysis was related to improved clinical outcomes.
AS08-006
THROMBOLYSIS: IMPROVING EFFICACY
Oral
THE INTERACTION OF AGE AND NIHSS PREDICTS DOOR-TO-NEEDLE TIMES IN A TELE-NEUROLOGY STROKE NETWORK
L. Birnbaum1, C. Topel2, J. Cornell3, M. Goros3 and J. Rodriguez1
1University of Texas Health Science Center, Neurosurgery, San Antonio, USA
2University of Texas Health Science Center, Neurology, San Antonio, USA
3University of Texas Health Science Center, Epidemiology and Biostatistics, San Antonio, USA
Abstract
Background: Timesaving variables within our tele-neurology IV tPA cohort were examined to improve our Door-to-Needle (DTN) times.
Methods: A retrospective review of GWTG database was performed for a 5-hospital, tele-neurology stroke network between 2010 and 2015. All acute ischemic stroke patients that were triaged in the ED and received IV tPA were included. Good DTN time was defined as <60 minutes. Logistic regression was performed with clinical variables associated with DTN. Age and NIHSS were categorized based on clinically significant cut-offs.
Results: Of 674 eligible patients, 652 (51% women, 46% White, 45% Hispanic, and 8% Black) were included. The average age was 70 years (range 29–98). Of the variables included, only Arrival Mode, Initial NIHSS, and interaction of Age:Initial NIHSS were significant (Table 1). DTN > =60 minutes was most common in patients >80 years with NIHSS >10 (Figure 1).
Conclusions: Arrival by EMS is critical to reduce DTN times. The cause of DTN delay for older patients with higher NIHSS is less clear and may include unstable medical conditions or complicated medical histories. Further study of this subgroup is important to reduce overall DTN times.
AS01-026
THROMBOLYSIS: IMPROVING EFFICACY
Oral
MRI IS NOT AS FAST AS CT BUT INCREASES THE PHYSICIAN'S CERTAINTY OF PRESCRIBING THROMBOLYTIC THERAPY
C.K. Hansen1, A. Christensen2, I. Havsteen2 and H. Christensen1
1Bispebjerg University Hospital, Department of Neurology, Copenhagen K, Denmark
2Bispebjerg University Hospital, Department of Radiology, Copenhagen K, Denmark
Abstract
Background: CT-based door-to-needle-times of 20 minutes are feasible, but the more time-consuming
MRI-based-evaluation is superior in detecting acute ischaemia and stroke-mimicking pathology; hypothetically adding relevant information on patients with a dubious clinical presentation. As the efficacy of thrombolysis decreases with time to treatment, one must ask if use of MRI is merely of academic interest or does indeed ensure a higher level of decision support for the physician on call?
The aim of this study was to compare door-to-needle-times and the physician’s certainty of prescribing thrombolytic therapy to stroke patients randomized to CT versus MRI prior to prescription of iv-tPA.
Methods: Four-hundred-forty-five consecutive patients admitted with symptoms of stroke within 4.5 hours from symptom-onset were quasi-randomized to CT or MRI and treated with iv-tPA if eligible.
Door-to-needle-times for patients, allocated to CT and MRI, were compared.
The level of decision support of the imaging and the physician’s certainty of prescribing thrombolytic therapy were documented with use of visual analog scales.
Results: Door-to-needle-times for CT evaluated patients (median 23 min) were significantly faster than for MRI-examined patients (median 32 min), p = 0.002.
The tPA-prescribing stroke physicians indicated significantly higher levels of decision support in patients having MRI compared to CT-imaging (p = 0.011) as well as significantly higher levels of certainty in prescribing iv-tPA to MRI-examined patients (p = 0.039).
Conclusions: CT-based evaluation prior to iv-tPA-treatment is faster but MRI contributes with higher levels of decision support and increases the physician certainty of prescribing or refraining from thrombolytic therapy.
AS25-005
THROMBOLYSIS: IMPROVING EFFICACY
Oral
PREHOSPITAL AARHUS STROKE SEVERITY SCALE TO PREDICT LARGE ARTERY OCCLUSION: DESIGN AND COMPARISON WITH OTHER SCALES
S. Hastrup1, D. Damgaard1, S.P. Johnsen2 and G. Andersen1
1Aarhus University Hospital, Department of Neurology, Aarhus C, Denmark
2Aarhus University, Department of Clinical Epidemiology, Aarhus N, Denmark
Abstract
Background: Prehospital identification of emergent large vessel occlusion (ELVO) is of importance. We designed and validated a simple prehospital stroke scale to identify ELVO in patients with acute ischemic stroke and compared it to other published scales predicting ELVO.
Methods: A national historical test cohort of 3127 patients with information on intracranial vessel status (angiography) before reperfusion therapy was identified. National Institutes of Health Stroke Scale (NIHSS) items with the highest predictive value of occlusion of a large intracranial artery were identified and the most optimal combination meeting pre-defined criteria to ensure usefulness in the prehospital phase was determined. The predictive performance of Prehospital Aarhus Stroke Severity (PASS) scale was compared with other published scales for ELVO.
Results: The PASS scale was composed of 3 NIHSS scores: level of consciousness (month/age) (1 point > 0); gaze palsy/deviation (1 point > 0) and arm weakness (1 point > 0). In derivation of PASS 2/3 of the test cohort was used and showed accuracy (Area Under Curve) of 0.76 for detecting large artery occlusion. Optimal cut point ≥ 2 abnormal scores showed: sensitivity 0.66 (95%CI 0.62–0.69); specificity 0.83 (0.81–0.85) and AUC 0.74 (0.72–0.76). Validation on 1/3 of the test cohort showed similar performance. Patients with a large artery occlusion on angiography with PASS ≥ 2 had a median NIHSS of 17 (IQR = 6) as opposed to PASS < 2 with a median NIHSS of 6 (IQR = 5). The PASS scale showed equal performance although more simple when compared to other scales predicting ELVO.
Conclusions: The PASS scale is simple and has promising accuracy for prediction of ELVO in the field.
AS08-040
THROMBOLYSIS: IMPROVING EFFICACY
Oral
PRE-HOSPITAL START OF INTRAVENOUS THROMBOLYSIS IN ACUTE ISCHEMIC STROKE - EFFECT ON OUTCOME IN PATIENTS WITH PRE-STROKE NEED OF ASSISTANCE
C. Nolte1, A. Kunz1, H. Erdur1, J. Fiebach2, F. Geisler1, M. Rozanski1, J.F. Scheitz1, K. Villringer2, C. Waldschmidt1, J. Weber3, M. Wendt1, B. Winter1, K. Zieschang1, U. Gritttner4, M. Ebinger5 and H. Audebert1
1Charité - Campus Benjamin Franklin, Neurology, Berlin, Germany
2Charité - Campus Benjamin Franklin, Neuroradiology, Berlin, Germany
3Charité - Campus Benjamin Franklin, Berlin Insitute of Health, Berlin, Germany
4Center for Stroke Research, Clinical Epidemiology and Health Services Research in Stroke, Berlin, Germany
Background: There is an ongoing debate on whether ischemic stroke patients with pre-stroke need of assistance (dependent, i.e. with private or professional care at home or institution) should be treated with intravenous thrombolysis (IVT) because they were excluded in some randomized trials. We analyzed the effect of IVT on patients with and without pre-stroke dependency with a focus on pre-hospital IVT in a specialized ambulance.
Methods: We pooled data from a pre-hospital and an in-hospital thrombolysis register operated by the Charité University-Hospital Berlin. We stratified study populations into patients needing assistance (dependent) or living at home without assistance (independent) pre-stroke. We tested the effects of pre-hospital start of IVT within the STEMO concept on 3-month modified Rankin Scale (mRS) ≤3 and mortality in both groups. Outcomes were adjusted in multivariable regression for demographics, co-morbidities, stroke severity (National Institutes of Health Stroke Scale (NIHSS)) and pre-stroke level of care.
Results: From 2011 to 2015, 268 dependent and 661 independent patients received IVT. Dependent patients were older (85 ± 8 versus 71 ± 12 years), more often female (68% versus 42%) and had higher median NIHSS (11 versus 7) (all p < 0.01). In unadjusted analysis, 3 month mRS of pre-stroke dependent patients was ≤ 3 in 31% (versus 78%, p < 0.01) and mortality was 35% (versus 8%, p < 0.01). However, pre-hospital IVT (with shorter mean OTT) had similar favorable effects in both groups: Adjusted OR for mRS ≤ 3: 2.03 (95%-CI:1.03–4.00) and 1.97 (1.38–2.82) and OR for death: 0.64 (0.35–1.17) versus 0.53 (0.34–0.82), respectively.
Conclusions: Pre-hospital IVT seems beneficial in patients with and without pre-stroke dependency.
AS17-072
THROMBOLYSIS: IMPROVING EFFICACY
Oral
THROMBUS PERMEABILITY ESTIMATED FROM BASELINE CT IMAGING IS ASSOCIATED WITH IMPROVED IV-RTPA TREATMENT SUCCESS AND FUNCTIONAL OUTCOME IN PATIENTS WITH ACUTE ISCHEMIC STROKE
E. Santos1,2, J.W. Dankbaar3, K. Treurniet4, W. Niessen2, C. Majoie4, B. Velthuis3 and H. Marquering1
1AMC - Academic Medical Center- University of Amsterdam-, Biomedical Engineering and Physics and Radiology, Amsterdam, Netherlands
2Erasmus MC University Medical Center, Medical Informatics, Rotterdam, Netherlands
3University Medical Center Utrecht, Radiology, Utrecht, Netherlands
4AMC - Academic Medical Center- University of Amsterdam-, Radiology, Amsterdam, Netherlands
Abstract
Background: Predicting recanalization success of intravenously administered recombinant tissue plasminogen activator (IV-rtPA) and patient functional outcome from baseline imaging would be a strong improvement in acute ischemic stroke management. Pre-clinical studies have shown that thrombus permeability may improve rtPA efficiency. We hypothesize that thrombus permeability estimated from baseline radiological imaging is associated with IV-rtPA treatment success.
Methods: All patients with proven proximal occlusion of the anterior and posterior circulation, without intra-arterial treatment and good quality baseline imaging from the DUST study were included. Thrombus permeability was gauged using the manual measurement of the attenuation increase (Δ) between co-registered admission NCCT and CTA for 278 patients. Subsequently, associations between Δ and both complete recanalization (for IV-rtPA and no IV-rtPA patients separately) and favorable outcome (mRS ≤ 2 at 90 days) were investigated.
Results: The median Δ was 20.1 (IQR: −31.7, 224.0) HU. Using a TG-ROC analysis, thrombi with an attenuation increase Δ above 23.0 HU were considered pervious and were significantly associated with successful complete IV-rTPA recanalization: OR = 2.7 (95%CI:1.2–5.9, p = 0.01, n = 177). However, without IV-rTPA, perviousness was negatively correlated with recanalization, OR = 0.6 (95%CI:0.2–1.8, p = 0.35, n = 101). A pervious thrombus was also associated with improved functional outcome independently from the recanalization status and treatment (p = 0.001).
Conclusions: We showed that thrombus perviousness measured on admission imaging is strongly associated with IV-rTPA treatment success and functional outcome. This suggests that this measure is an excellent candidate for AIS patient stratification in acute clinical diagnosis settings.
AS25-047
THROMBOLYSIS: IMPROVING EFFICACY
Oral
THE “HELSINKI MODEL” ORGANIZATION OF ACUTE STROKE CARE REDUCES DELAYS IN THROMBOLYSIS IN PATIENTS WITH ISCHEMIC STROKE
N. Shamalov1, G. Ivanova1 and L. Stakhovskaya1
1Pirogov Russian National Research Medical University, Stroke Institute, Moscow, Russia
Abstract
Background: In stroke patients any delays during hospitalization should be avoided for decreasing of the time from symptoms onset to treatment (including thrombolysis). The aim of our study was to assess the effectiveness of “Helsinki model” (Meretoja A., Kaste M. et al) of organization of stroke units (HMOSU) on onset-to-door time (ODT), door-to-CT time (DCTT), door-to-needle time (DNT), safety and efficacy of IV rt-PA in stroke units (SUs) in Russia.
Methods: Due to State Stroke Program in Russia 505 SUs with 20,843 dedicated stroke beds were created from 2008 to 2013. The HMOSU has been realized in 309 SUs. We enrolled all patients treated with IV rt-PA in SUs in routing clinical practice that were registered in web-based Federal Hospital Registry (01Jan 2014–31Dec 2015). Median ODT, DCTT, DNT, mortality rate as well as number of patients with good outcome (mRs score 0–1) in 30-day were calculated in SUs with and without HMOSU.
Results: In 2015 8,132 patients received IV rt-PA in Russia (2.4% of all ischemic strokes). Significantly reduced DCTT (17 min vs 45 min, p < 0.001) and DNT (55 min vs 68 min, p = 0.001) were observed in HMOSU. There were no changes in ODT. The mortality rate were similar (11.7% vs 12.8%) and the good outcome rate was higher in HMOSU (37.4% vs 31.2%; p = 0.038).
Conclusions: These data suggest that the HMOSU–like system can significantly reduce time delays in hospitals for IV thrombolysis and provide additional possibilities for good functional outcome in rt-PA treated patients.
AS07-041
THROMBOLYSIS: IMPROVING EFFICACY
Oral
MOBILE STROKE AMBULANCE: HIGH RECANALIZATION RATES AND EXCELLENT OUTCOMES AFTER EARLY INTRAVENOUS TPA ADMINISTRATION IN PATIENTS WITH ACUTE LARGE VESSEL OCCLUSION
G. Toth1, A. Taqui1, R. Cerejo1, S. John1, M. Donohue1, K. Uchino1 and M.S. Hussain1
1Neurological Institute, Cerebrovascular Center, Cleveland, USA
Abstract
Background: The Mobile Stroke Unit (MSTU) is a novel concept bringing stroke care to the patient in an ambulance. It carries the promise of significant improvement in tPA delivery times/rates, and patient outcomes.
Methods: The Cleveland MSTU is an ambulance equipped with a portable CT/CTA scanner, point-of-care testing, and telemedicine. Our database, a prospectively maintained registry of patients evaluated in the MSTU, was reviewed to identify “hyperacute” patients assessed within 60 minutes of their symptom onset. We analyzed information on demographics, presentation, imaging, vessel status, tPA times, and short-term clinical follow-up.
Results: Among the first 100 patients evaluated in the MSTU, 95 presented with known time of onset, and 25 (26.3%) were within 60 minutes of symptom onset at a median of 39 minutes (interquartile range (IQR) = 27–46). After applying standard exclusion criteria, 9/25 (36%) patients received IV t-PA at a median time of 51 min (IQR 46–56). On initial CTA 6/25 (24%) patients had large vessel occlusion (LVO). Recanalization was seen in 5 of 6 (83.3%) patients on follow-up imaging after tPA bolus at a median time of 88 min (IQR 84–96). Median NIHSS at presentation was 16 (IQR 16–19), which improved by 6–17 points at 24 hours after tPA. By the time of discharge, 2 patients further improved resulting in a low median NIHSS of 3 (IQR 0–3) in the group.
Conclusions: Early tPA administration in stroke patients with acute LVO in our MSTU resulted in high recanalization rates and excellent clinical outcomes. Further study in a larger cohort is warranted.
AS13-058
THROMBOLYSIS: IMPROVING EFFICACY
Oral
EMERGENCY MEDICAL DISPATCHERS RECOGNIZE 66% OF ACUTE STROKE DURING EMERGENCY CALLS
S. Viereck1, T.P. Møller1, H.K. Iversen2, H. Christensen3 and F. Lippert1
1Emergency Medical Services Copenhagen University of Copenhagen, Research Unit, Ballerup, Denmark
2Copenhagen University Hospital Rigshospitalet - Glostrup, Stroke Unit Department of Neurology, Glostrup, Denmark
3Copenhagen University Hospital Bispebjerg, Stroke Unit Department of Neurology, Copenhagen, Denmark
Abstract
Background: Immediate recognition of stroke symptoms is crucial to ensure timely access to revascularization therapy. Medical dispatchers can ensure fast admission to stroke facilities. Data on medical dispatchers’ ability to recognize symptoms of acute stroke are therefore valuable in organizing emergency stroke care.
We aimed at describing the sensitivity and positive predictive value of stroke recognition during emergency calls and to identify factors associated with recognition.
Methods: This was an observational study of 2,653 consecutive unselected patients with a final diagnosis of stroke or transient ischemic attack (TIA), admitted through the Emergency Medical Services Copenhagen, during a two-year period (2012–2014). Final diagnoses were matched with dispatch codes from the Emergency Medical Dispatch Center. Sensitivity and positive predictive value were calculated. The effect of age, gender, and time-of-day was analyzed using multivariate logistic regression.
Results: This study showed a sensitivity of 66.2% (95% CI: 64.4%-68.0%), and a positive predictive value of 30.2% (95% CI: 29.1%-31.4%) for stroke recognition during emergency calls, see Table 1. The multivariate logistic regression analysis showed that stroke recognition was better during daytime, OR 1.38 (95% CI: 1.02–1.87).
Conclusions: We report an overall high recognition of stroke by medical dispatchers, however recognition was significantly improved during day-time. Emergency medical dispatchers may play an important role in ensuring a fast-track for stroke treatment which is likely to promote timely acute therapy.
AS08-012
THROMBOLYSIS: OUTCOMES AND COMPLICATIONS
Oral
CEREBRAL WHITE MATTER LESIONS AND POST-THROMBOLYTIC REMOTE PARENCHYMAL HEMORRHAGE
S. Curtze1, J. Putaala1, G. Sibolt1, S. Melkas1, S. Mustanoja1, E. Haapaniemi1, T. Sairanen1, M. Tiainen1, T. Tatlisumak1 and D. Strbian1
1Helsinki University Central Hospital, Neurology, Helsinki, Finland
Abstract
Background: Intracranial hemorrhage following intravenous thrombolysis (IVT) may occur within the ischemic area (PH) or as a remote hemorrhage (rPH). The latter may partly relate to cerebral amyloid angiopathy (CAA), which belongs to the continuum of cerebral small vessel disease. Because cerebral white matter lesions (WML) represent an imaging surrogate of small vessel disease, we hypothesized that they are associated with higher rates of rPH.
Methods: We analyzed 2485 consecutive patients treated with IVT at the Helsinki University Central Hospital. Severe WMLs were defined as 5–6 points on the Blennow rating scale from all baseline CT head scans. Remote PH (rPH) was defined as hemorrhages that appear in brain regions without visible ischemic damage. The association of severe WMLs with pure rPH, pure PH, and rPH versus PH were adjusted in multivariate logistic regression models for all in univariate analyzes associated (p < 0.1) covariates.
Results: After adjustments, severe WMLs were associated with pure rPH compared with pure PH (OR 5.5; 95% CI 1.69–17.86). When comparing rPH with patients without any PH (no rPH and no PH), severe WMLs (OR 6.48; 95% CI 2.82–14.89) and age (OR 1.06; 95% CI 1.01–1.10) were associated with rPH. Severe WMLs were not associated with the occurrence of pure PH after adjustment for associated factors in univariate analyzes.
Conclusions: Severe cerebral WMLs are associated with post-thrombolytic rPH but not with PH within the ischemic area. Our findings strengthens the hypothesis that CAA is the leading underlying pathology in rPH.
AS06-020
THROMBOLYSIS: OUTCOMES AND COMPLICATIONS
Oral
LEUKOARAIOSIS ASSOCIATED SYMPTOMATIC INTRACEREBRAL HAEMORRHAGE AND FUNCTIONAL OUTCOME AFTER THROMBOLYSIS FOR ACUTE ISCHAEMIC STROKE: SYSTEMATIC REVIEW AND META-ANALYSIS
K. Kongbunkiat1, D. Wilson1, F. Jichi2, V. Palumbo3, M.D. Hill4, A.M. Buchan5, S. Jung6, H.P. Mattle6, N. Henninger7 and D.J. Werring1
1UCL Institute of Neurology, UCL Stroke Research Centre, London, United Kingdom
2UCL School of Life & Medical Sciences, Medical Statistician, London, United Kingdom
3Careggi University Hospital, Department of Neurology, Florence, Italy
4Hotchkiss Brain Institute- University of Calgary, Cumming School of Medicine, Calgary- Alberta, Canada
5University of Oxford- John Radcliffe Hospital, Radcliffe Department of Medicine, Oxford, United Kingdom
6Inselspital- University of Bern, Department of Neurology, Bern, Switzerland
7University of Massachusetts Medical School, Departments of Neurology and Psychiatry, Worcester, USA
Abstract
Background: Leukoaraiosis, a neuroimaging marker of small vessel disease, may be associated with an increased risk of symptomatic intracerebral haemorrhage (sICH) and poor clinical outcome following thrombolysis for acute ischaemic stroke, but previous studies have been inconclusive. We performed a systematic review and meta-analysis of published aggregate data.
Methods: We included studies of patients with acute ischaemic stroke treated with intravenous/intra-arterial thrombolysis, which assessed functional outcome (3-month mRS) or sICH in relation to leukoaraiosis on pretreatment scans (CT or MRI). We used fixed-effects models to calculate pooled relative risks (RR) of sICH and poor functional outcome (mRS > 2) for any vs. no leukoaraiosis (using any rating scale) and for none-to-mild vs. moderate-to-severe leukoaraiosis (using the Van Swieten or Fazekas Schmidt scale). We confirmed the results using random-effects models.
Results: We identified 13 studies (total n = 6901). Not all leukoaraiosis measures or outcomes were available from all studies, so different numbers of participants contributed to each analysis. The RR for sICH (n = 5454) was 1.66 for any leukoaraiosis vs. none (95%CI 1.31–2.09; p = 0.001). The RR for sICH (n = 4095) was 2.42 for moderate-to-severe vs none-to-mild leukoaraiosis (95%CI 1.84–3.17; p = 0.001). The RR of poor functional outcome (n = 3304) was 1.26 for any leukoaraiosis vs none (95% CI 1.19–1.34; p = 0.001). The RR for poor functional outcome (n = 3562) was 1.30 for moderate-to-severe vs none-to-mild leukoaraiosis (95%CI 1.23–1.37; p = 0.001). No statistical heterogeneity was noted for any of the analyses.
Conclusions: Leukoaraiosis presence and severity are consistently associated with sICH and poor functional outcome after intravenous/intra-arterial thrombolysis for acute ischaemic stroke.
AS08-023
THROMBOLYSIS: OUTCOMES AND COMPLICATIONS
Oral
DOES THE PROPORTION OF SINGLE-CHAIN RTPA INFLUENCE OUTCOMES IN PATIENTS WITH CEREBRAL ISCHEMIA?
D. Leys1, I. Sibon2, J.L. Mas3, T. Moulin4, M. Giroud5, R. Bordet6 and D. Vivien7
1University Lille 2- INSERM U 1171- CHU Lille, Neurology, Lille, France
2University of Bordeaux, Neurology, Bordeaux, France
3Ste Anne Hospital, Neurology, Paris, France
4University of Franche Comté, Neurology, Besançon, France
5University of Burgundy, Neurology, Dijon, France
6University Lille 2- INSERM U 1171- CHU Lille, Pharmacology, Lille, France
7Inserm UMR-S 919- University of Caen Basse-Normandie, GIP CYCERON, Caen, France
Abstract
Background: The 2 forms of tissue plasminogen activator (tPA), single- (sc-tPA) and 2-chain (tc-tPA) have similar thrombolytic activities, but neurotoxicity is specific to sc-tPA. The proportion of sc- and tc-forms of recombinant tPA (rtPA) being different between blisters, patients who receive higher proportions of the sc-form might have worse outcomes. The objective of OPHELIE was to determine whether the sc/(sc + tc) rtPA ratio influences the proportion of patients without handicap 3 months after cerebral ischemia, and to identify its influence on (i) dependency, (ii) survival, and (iii) symptomatic intracerebral hemorrhage (s-ICH).
Methods: We prospectively included consecutive stroke patients treated with i.v. rtPA in 13 French centers, and determined the sc/(sc + tc) ratio in the treatment administered for each patient. Samples were frozen at −20°C and analyzed by densitometry. We studied the association between sc/(sc + tc) ratios and the 4 outcome measures. OPHELIE was registered under ClinicalTrials.gov Identifier n° NCT01614080.
Results: We recruited 1,004 patients (515 men, median age 75 years, median onset-to-needle time 170 minutes, median national institutes of health stroke scale score 10). The sc/(sc + tc) ratios ranged from 51% to 91% (median 71%). There was no statistical association between sc/(sc + tc) ratios and handicap, dependency or death at 3 months. Patients with s-ICH had significantly lower ratios (median 69%, IQR 67%-72% vs. 72%, 68%-76%; adjusted p = 0.003).
Conclusions: The neurotoxicity of rtPA does not influence functional outcomes and mortality in patients with cerebral ischemia. Higher proportions of sc-rtPA are even associated with lower risks of s-ICH.
AS08-024
THROMBOLYSIS: OUTCOMES AND COMPLICATIONS
Oral
OROLINGUAL ANGIOEDEMA DURING THROMBOLYSIS FOR CEREBRAL ISCHEMIA
F. Myslimi1, F. Caparros2, N. Dequatre-Ponchelle3, S. Moulin4, G. Sophie4, P. Girardie5, C. Cordonnier4, R. Bordet6 and D. Leys4
1University of Medicine of Tirana- Albania, Neurology, Tirana, Albania
2University of Lille., Neurology, Lille, France
3CHU Lille, Neurology, Lille, France
4University of Lille. INSERM U 1171. CHU Lille., Neurology, Lille, France
5CHU Lille, Intensive care medicine, Lille, France
6University of Lille. INSERM U 1171. CHU Lille., Pharmacology, Lille, France
Abstract
Background: Most studies on orolingual angioedema (OLAE) reported isolated cases, and did not evaluate its influence on the 3-month outcome. Our objective was to compare baseline characteristics and outcomes in a large cohort of patients with and without OLAE associated with thrombolysis, and to perform a systematic review of the literature.
Methods: We prospectively included consecutive patients who received i.v. thrombolysis for cerebral ischemia at the Lille University Hospital. We evaluated the 3-month outcome (modified Rankin scale, mRS). We examined tongue/lips every 15 minutes up to 30 minutes after thrombolysis. We determined the proportion of patients with OLAE, and compared their characteristics and outcomes with those of patients without. We performed a systematic literature search.
Results: Of 923 consecutive patients, 20 (2.2%) developed OLAE. None of them needed intubation. They were more likely to be under angiotensin converting enzyme inhibitors (ACE-I) (adjusted odds ratio [OR]: 3.9; 95% confidence interval [CI]: 1.6 to 9.7), to have total insular infarcts (OR: 5.0; 95%CI: 1.5–16.5), and to develop symptomatic intracerebral hemorrhages (OR: 3.2; 95%CI: 1.2 to 8.5). The long-term outcome was not influenced by OLAE. In the meta-analysis, on-going treatment with ACE-I was strongly associated with OLAE (OR 8.6; 95%CI: 5.5–13.5).
Conclusions: OLAE occurs in 1 out of 50 patients treated by i.v. thrombolysis for cerebral ischemia, and this increases to 1 out 6–12 if they are under ACE-inhibitors, and 1 out of 10 if they have a total insular infarct. Their long-term outcome is not influenced. This risk should not prevent the prescription of rt-PA.
AS08-034
THROMBOLYSIS: OUTCOMES AND COMPLICATIONS
Oral
CHANGES IN EUROPEAN LABEL AND GUIDELINE ADHERENCE IN THE SITS REGISTRY FOLLOWING UPDATED RECOMMENDATIONS FOR STROKE THROMBOLYSIS
T. Moreira1, M. Mazya1, N. Anani2, O. Bill3, R. Chen2, S. Koch2, N. Ahmed1 and N. Wahlgren1
1Karolinska University Hospital, Department of Neurology, Stockholm, Sweden
2Karolinska Institute, Department of Health Informatics, Stockholm, Sweden
3Centre Hospitalier Universitaire Vaudois - CHUV, Department of Neurology, Lausanne, Switzerland
Abstract
Background: In acute ischemic stroke, label and guideline contraindications for intravenous thrombolysis (IVT) are checked before treatment initiation. The current EU label and ESO guidelines are however frequently in conflict. The aims of the present study were to compare non-adherence to label versus guideline contraindications following the European guideline update in 2008/09 and to determine if hospital patient volumes influence non-adherence.
Methods: Data was collected from hospitals enrolling patients in the SITS registry both before (2006/07; n = 6354) and after (2010/11; n = 12046) the guidelines’ update.
Results: Label non-adherence increased from 23.6% in 2006/07 to 51.1% in 2010/11.Non-adherence to stroke onset >3 h increased from 8.2% to 27.9% and to age >80 years from 8.9% to 17.2% (both p < 0.001). Slightly higher label non-adherence was also detected for the contraindications severe stroke (from 1.1 to 1.7%), stroke onset >4.5 hours (from 0.9 to 1.8%), systolic/diastolic blood pressure >185/110 mm Hg (from 2.5%/0.8% to 5.4%/2.1 %), and ongoing oral anticoagulation (from 2.4 to 3.1%; all P ≤ 0.001). Higher hospital volumes of IVT patients were associated with higher non-adherence.
Conclusions: Clinicians promptly adopted the new European guideline recommendations. Label non-adherence increased, particularly in high volume centers. With mounting evidence on the safety and efficacy of IVT in patients with various label contraindications, and over 50% of all patients in our material treated off-label, there is a strong impetus on an update of the European alteplase label.
AS08-047
THROMBOLYSIS: OUTCOMES AND COMPLICATIONS
Oral
RISK FACTORS FOR DEEP AND LOBAR REMOTE HEMORRHAGES AFTER INTRAVENOUS THROMBOLYSIS ARE DIFFERENT
L. Prats-Sánchez1, J. Sotoca-Fernández1, A. Martínez-Domeño1, P. Camps-Renom1, R. Delgado-Mederos1, R. Marin1, L. Dorado2, J. Codas3, A. Gómez-González4, F. Purroy5, M. Gómez-Choco6, D. Canovas7, D. Cocho8, M. Garces9, S. Abilleira10 and J. Martí-Fàbregas1
1Hospital de la Santa Creu i Sant Pau, Neurology, Barcelona, Spain
2Hospital Universitari Germans Trias i Pujol, Neurology, Badalona, Spain
3Hospital Clínic i Provincial, Neurology, Barcelona, Spain
4Hospital del Mar, Neurology, Barcelona, Spain
5Hospital Universitari Arnau de vilanova, Neurology, Lleida, Spain
7Hospital Universitari de Sabadell-Corporació Sanitària Parc Taulí, Neurology, Sabadell, Spain
8Hospital General Universitari de Granollers, Neurology, Granollers, Spain
9Hospital de Tortosa Verge de la Cinta, Neurology, Tortosa, Spain
10Stroke Programme Catalan Agency for Health Information Assessment and Quality CAHIAQ, Neurology, Barcelona, Spain
Abstract
Background: The pathophysiology of remote parenchymal hemorrhage (rPH) after intravenous thrombolysis (IV-tPA) is uncertain. We hypothesized that rPH may have different risk factors according to the bleeding localization. We analyzed the risk factors for deep and lobar rPH.
Methods: We studied prospectively consecutive patients with ischemic stroke who were treated with IV-tPA and were included in a multicenter prospective registry. rPH was defined as any extra-ischemic hemorrhage detected in the follow-up CT. We collected demographic, clinical, laboratory and radiological (presence and localization of any parenchymal bleeding in the follow-up CT) data. In patients who underwent a MRI examination, we evaluated the distribution of microbleeds (MB), cortical superficial siderosis, leukoaraiosis and recent silent ischemia (RSI). We compared patients with deep or lobar rPH with those without any parenchymal bleeding. Bivariate and multivariable logistic regression analyses were performed.
Results: We studied 992 patients (mean age 73.7 ± 13.4 years, 52.9% were men) and 408 (41.1%) underwent a MRI examination. We observed rPH in 34 patients (3.4%), 9 were deep and 25 lobar. Deep rPH were associated with hypertensive episodes during IV-tPA (OR 7.4; 95%CI 1.8–27.0, p = 0.005) whereas lobar rPH were associated with lobar MB (OR 13.3; 95%CI 4.08–62.5, P < 0.001), RSI (OR 4.4; 95%CI 1.2–15.8, p = 0.022) and atrial fibrillation (OR 5.8; 95%CI 1.4–23.2, p = 0.012).
Conclusions: Deep and lobar rPH after IV-rtPA may have different pathophysiology. Blood Pressure control may be important to avoid deep rPH, whereas lobar rPH may be related to amyloid deposition and recent ischemic damage.
AS13-052
THROMBOLYSIS: OUTCOMES AND COMPLICATIONS
Oral
LONG TERM COST-EFFECTIVENESS OF THROMBECTOMY FOR ACUTE ISCHAEMIC STROKE IN REAL LIFE: AN ANALYSIS BASED ON DATA FROM THE SWEDISH STROKE REGISTER (RIKSSTROKE)
K. Steen Carlsson1, G. Andsberg2, J. Petersson2 and B. Norrving2
1Lund University, Department of Clinical Sciences- Malmö: Health Economics Unit, Lund, Sweden
2Lund University, Department of Clinical Medicine- Lund, Lund, Sweden
Abstract
Background: Recent randomized controlled trials (RCTs) have demonstrated substantial benefit of thrombectomy in patients with proximal anterior circulation arterial occlusion. Cost effectiveness estimates of thrombectomy need to include not only effects on the health care system, but also a societal perspective (social services and nursing home care).
Methods: A Markov state transition cohort model was constructed to estimate costs and outcomes in a 25-year perspective. Treatment outcome was based on pooled modified Rankin Scale (mRS) data at 3 months from five published RCTs, and recent age-specific survival data from Riksstroke grouped by mRS score. Resource use for the post-acute care, rehabilitation, social services and nursing home care was linked to mRS and data from Riksstroke for a sample of 710 patients with NIHSS > 7 treated with thrombolysis during 2014. A 3% discount rate was applied on future costs and benefits.
Results: While thrombectomy can be expected to increase the health care cost per patient (+ SEK 117 000) (EUR 1 = SEK 9.35) mainly because of intervention costs, the reduced burden on the social services including home help services (¬−SEK 169 000) and nursing home care (−SEK 331 000) implies cost savings at the societal level. The average patient gain was 1.0 QALY with higher gains for younger age groups.
Conclusions: Based on real world data from Riksstroke, thrombectomy therapy in patients matching those in recent RCTs, may lead to substantial cost savings in the social service sector, more than 3 times the increase in health care costs.
AS06-044
THROMBOLYSIS: OUTCOMES AND COMPLICATIONS
Oral
MECHANICAL THROMBECTOMY IMPROVES FUNCTIONAL OUTCOMES INDEPENDENT OF PRETREATMENT WITH INTRAVENOUS THROMBOLYSIS: A SYSTEMATIC REVIEW AND META-ANALYSIS
G. Tsivgoulis1,2, A. Katsanos1,3, G. Magoufis4, A. Safouris1,4, O. Kargiotis4, C. Liantinioti1,4, M. Chondrogianni1, A. Papa1, A. Roussopoulou1,5, A. Arhtur2 and A. Alexandrov2
1School of Medicine - University of Athens, Second Department of Neurology, Athens, Greece
2University of Tennessee Health Science Center, Department of Neurology, Memphis, USA
3School of Medicine University of Ioannina, Department of Neurology, Ioannina, Greece
4Metropolitan Hospital, Stroke Unit, Piraeus, Greece
5“Evangelismos” General Hospital, Department of Neurology, Athens, Greece
Abstract
Background: Endovascular reperfusion therapies (ERTs) improve functional outcome (FO) in patients with emergent large vessel occlusion (ELVO), but there are contradictory data regarding ERT efficacy in ELVO patients without pretreatment with intravenous thrombolysis (IVT). We conducted a systematic review and meta-analysis of all available randomized controlled trials (RCTs) that included patients with ELVO pretreated with IVT prior to ERT.
Methods: We performed a random effects pooled subgroup analysis of the adjusted common odds ratios (acOR) of the association of ET (vs. standard therapy) with three-month FO, stratified by pretreatment with IVT.
Results: Three RCTs (MR CLEAN, ESCAPE and REVASCAT; n = 1021) included both subgroups with (n = 833) and without (n = 188) pretreatment with IVT. In the subgroup analysis, ET was associated with a higher likelihood of better three-month FO in both the subgroup of patients with (OR = 1.85, 95%CI: 1.37–2.49; p < 0.001) and without (OR = 2.48, 95%CI: 1.43–4.30; p = 0.001) IVT pretreatment. We documented no significant difference between these two subgroups (p = 0.360) on the association of ELVO with three-month FO. There was no evidence of heterogeneity (I2 < 30%), while the risk of bias was considered to be generally low in the qualitative assessment of included trials.
Conclusions: Our findings provide further reassurance to stroke clinicians regarding the efficacy of ERT in ELVO independent of pretreatment with IVT. These data, however, do not indicate ineffectiveness of IVT nor should be used to withhold IVT in appropriate candidates.
AS33-001
WOMEN AND STROKE
Oral
SAFETY OF PREGNANCY FOLLOWING CEREBRAL VENOUS THROMBOSIS (ISCVT2 - PREGNANCY)
D. Aguiar de Sousa1, P. Canhão1, I. Crassard2, J.M. Coutinho3, A. Arauz4, A. Conforto5, M. Giroud6, J.M. Ferro1 and The ISCVT investigators
7
1Hospital Santa Maria - University of Lisbon, Department of Neurosciences Neurology, Lisbon, Portugal
2Hôpital Lariboisière, Deparment of Neurology, Paris, France
3Academic Medical Center, Department of Neurology, Amsterdam, Netherlands
4Instituto Nacional de Neurologia y Neurocirurgia, Deparment of Neurology, Mexico City, Mexico
5Hospital das Clínicas- São Paulo University, Stroke Unit, São Paulo, Brazil
6University Hospital and Medical School of Dijon- University of Burgundy, Stroke Unit, Dijon, France
7-, -, -, Portugal
Abstract
Background: Pregnancy is associated with an increased risk of venous thrombotic events (VT), including cerebral venous thrombosis (CVT). Data regarding the prognosis of pregnancy following CVT and the most appropriate preventive strategy are scarce. We aimed to study the course of subsequent pregnancies in women with previous CVT.
Methods: Women of childbearing age (<45 years) included in the International Study of Cerebral Vein and Dural Sinus Thrombosis (ISCVT, 1998 to 2001) were eligible. Patients were interviewed (consultation or phone contact) to assess rate of VT recurrence, outcomes of subsequent pregnancies and antithrombotic prophylaxis regimen.
Results: 32/74 centers agreed to participate. Follow-up was obtained in 119/193 eligible women from participating centers (median follow-up 169 ± 10 months). There were 82 new pregnancies in 47 women. In the 3rd trimester, 71% of women used low molecular weight heparin (LMWH) (52% in prophylactic dosage and 19% in therapeutic dosage). Four VT recurrences (in three patients) occurred during pregnancy or puerperium, including one CVT. Two of these three women were on prophylactic LMWH at the time of recurrence. Outcome of pregnancies was as follows: 51 full-term newborns, 9 preterm births, 2 stillbirths, 14 spontaneous and 6 induced abortions. The incidence of spontaneous abortion was lower in women receiving heparin and/or antiplatelets compared with women without antithrombotic prophylaxis (2/42 vs 8/24); RR 0.14, 95%CI 0.03–0.62; p = 0.009).
Conclusions: The absolute risk of pregnancy related VT in women with previous CVT was low. Antithrombotic therapy was associated with lower miscarriage rates in women with previous CVT.
AS33-002
WOMEN AND STROKE
Poster
SEX-RELATED DIFFERENCES IN RISK FACTORS, TYPE OF TREATMENT RECEIVED AND OUTCOMES IN PATIENTS WITH ATRIAL FIBRILLATION AND ACUTE STROKE: RESULTS FROM THE RAF-STUDY
K. Antonenko1, V. Caso2 and on behalf of the RAF study
1Bogomolets National Medical University, Neurology, Kiev, Ukraine
2University of Perugia, Stroke Unit and Division of Cardiovascular Medicine, Perugia, Italy
Abstract
Background: Atrial fibrillation (AF) is an independent risk factor of thromboembolism. Women with AF are at a higher overall risk for stroke compared to men with AF. The aim of this study was to evaluate for sex-differences in patients with acute stroke and AF, regarding risk factors, treatments received and outcomes.
Methods: Data were analysed from the RAF study, a prospective, multicenter, international study including only patients with acute stroke and AF. Patients were followed-up for 90 days.
Results: Of the 1,029 patients enrolled, 561 were women (54.5%) (p< 0.001), younger (p < 0.001) compared to men. In patients with known AF, women were less likely to receive oral anticoagulants before index stroke (p = 0.026) and were less likely to receive anticoagulants after stroke (28.8% versus 21.6%, p = 0.009). There was no observed sex difference regarding the time of starting anticoagulant therapy between two groups. Men presented with more severe strokes at onset (mean NIHSS 9.2 ± 6.9 versus 8.1 ± 7.5, p < 0.001). Within 90 days, women had 46 (8.2%) recurrent ischemic events (stroke/TIA/systemic embolism) and 19 (3.4%) symptomatic cerebral bleedings compared to 30 (6.4%) and 18 (3.8%) in men (p = 0.28 and p = 0.74). At 90 days 57.7% of women were disabled or deceased, compared to 41.1% of the men (p < 0.001). Multivariate analysis did not confirm this significance.
Conclusions: Women with AF were less likely to receive oral anticoagulants prior to and after stroke compared to men with AF. Despite their younger age and slightly milder stroke severity on admission, women displayed similar rates of recurrent ischemic event, bleedings and functional outcome.
AS33-004
WOMEN AND STROKE
Oral
RISK OF FIRST STROKE IN AND AFTER PREGNANCY: A POPULATION-BASED COHORT STUDY FROM SWEDEN
L. Ban1,2, A. Abdul Sultan1, O. Stephansson3, L.J. Tata1, N. Sprigg4, C. Nelson-Piercy5, P.M. Bath4 and J.F. Ludvigsson6
1University of Nottingham, Division of Epidemiology & Public Health, Nottingham, United Kingdom
2University of Nottingham, Division of Rheumatology- Orthopaedics and Dermatology, Nottingham, United Kingdom
3Karolinska Institutet, Department of Medicine, Stockholm, Sweden
4University of Nottingham, Division of Neuroscience, Nottingham, United Kingdom
5Guy’s and St. Thomas’ NHS Foundation Trust, Women’s Health Academic Centre, London, United Kingdom
6Karolinska Institutet, Department of Medical Epidemiology and Biostatistics, Stockholm, Sweden
Abstract
Background: We aimed to quantify the risks of ischaemic, intracerebral haemorrhagic and subarachnoid haemorrhagic stroke in and after pregnancy compared with the baseline risk in women of childbearing age.
Methods: All women aged 15–49 years with live birth or stillbirth in 1992–2011 were identified from the Swedish Medical Birth Registry linked with the National Patient Registry. First stroke coded either as a primary or first of two secondary diagnoses during the study period was identified. Incidence rates per 100,000 person-years with 95% confidence intervals (95%CIs) were calculated for pregnancy (conception until 3 days before delivery), around delivery (2 days before to 1 day after delivery), postpartum (2 days after delivery until the end of 12 weeks postpartum) divided into early (first 6 weeks) and late (second 6 weeks) postpartum, and all other available follow-up time, including time before pregnancy and after postpartum. Incidence rate ratios (IRRs) were calculated using the Poisson regression with adjustment for age, education attainment and calendar time.
Results: Of 1,124,664 women, 3,105 had first stroke, about half having ischaemic stroke. The risk of stroke was 15.0 per 100,000 person-years (95%CI 14.5–15.6) in women of childbearing age. The risk was lower in pregnancy (7.3, 6.0–8.9; IRR = 0.7, 0.5–0.8) but higher around delivery (366.0, 293.2–467.0; IRR = 31.8, 25.4–40.0) and early postpartum (64.0, 54.1–75.7; IRR = 3.2, 2.7–3.7). The increased risk around delivery was more evident for haemorrhagic compared to ischaemic stroke.
Conclusions: Although the overall risk of stroke was low in women of childbearing age, the risk rose dramatically around the time of delivery.
AS06-008
WOMEN AND STROKE
Oral
ISCHEMIC STROKE IN WOMEN USING CONTRACEPTIVES: CAUSES, CHARACTERISTICS AND OUTCOME
P. Correia1, S. Machado2, A. Eskandari1 and P. Michel1
1Centre Hospitalier Universitaire Vaudois, Department of Neurology, Lausanne, Switzerland
2Hospital Professor Doutor Fernando Fonseca, Department of Neurology, Amadora, Portugal
Abstract
Background: Oral contraceptive usage may increase stroke risk in young women. We aimed at assessing characteristics and outcome of acute ischemic stroke (AIS) in women below age of 50 while on oral contraceptives.
Methods: We used consecutive AIS between 2003 and 2015 from the ASTRAL registry with detailed determined demographics, risk factors, clinical, radiological and prognostic data. We compared female patients <50 years with and without contraceptive usage in a multiple logistic regression model, with contraceptive use as the dependent variable.
Results: Of the young 179 women identified, 57 used contraceptives: oestrogen and progesterone (n = 43), progesterone only (n = 10), and unknown (n = 4). Stroke in contraceptive users occurred at a significantly younger age and in women with significantly lower history of hypertension or previous psychosis or depression. Initial stroke severity was similar, but a significantly higher proportion of contraceptive users had unknown stroke (TOAST) mechanism. PFO prevalence was similar, 17.54% in contraceptive users vs. 14.75% to non-users. These patients had significantly less intra and extracranial stenoses and occlusions and more often positive CT perfusion studies. Adjusted functional outcome was similar at 3 months and more favourable at 12 months in contraceptive users with significantly fewer stroke recurrences.
Conclusions: Women using contraceptives have strokes at a young age, with less arterial pathology, and less identified stroke mechanisms. Together with a lower recurrence rates after discontinuing contraceptives, an important causative role of contraceptives in stroke is suggested. The stroke mechanism being often unexplained, a prothrombotic state or hitherto unrecognized mechanisms may be responsible.
AS33-008
WOMEN AND STROKE
Oral
SEX DIFFERENCES IN THROMBOLYSED STROKE PATIENTS: WISE-GROUP INITIATIVE
M.R. Heldner1, R. Kurmann1, R. Balasubramaniam1, M.L. Mono1, F. Pult2, K. Hsieh2, S. Jung3, P. Mordasini2, J. Gralla2, M. Arnold1 and U. Fischer1
1Inselspital- University of Bern- Switzerland, Department of Neurology, Bern, Switzerland
2Inselspital- University of Bern- Switzerland, Institute of Diagnostic and Interventional Neuroradiology, Bern, Switzerland
3Inselspital- University of Bern- Switzerland, Department of Neurology and Institute of Diagnostic and Interventional Neuroradiology, Bern, Switzerland
Abstract
Background: To assess gender differences in clinical characteristics, treatment and outcome in thrombolysed stroke patients.
Methods: From January 2010–2015 1211 patients (n = 524[43.3%] women) were thrombolysed at the Bernese Stroke Center.
Results: Thrombolysed women were older than men (median 77.4 vs. 71 years; p < 0.0001), and median NIHSS score on admission was higher (median 13 vs. 11; p = 0.023) as well as premorbid disability (mRS < 2: 12.2% vs. 6.7%;p = 0.001). Women had less frequently hypercholesterolemia (54.8% vs. 61.7%;p = 0.017) and coronary artery disease (14.8% vs. 28.1%;p < 0.0001). Stroke etiology was more often cardioembolic (49.0% vs. 39.6%;p = 0.001) and less frequently caused by large artery disease (6.7% vs. 13.4%;p < 0.0001) and women had more often atrial fibrillation (47.2% vs. 34.7%;p < 0.0001). There was a longer time delay from admission to imaging in women (median 36 vs. 33 min.;p = 0.009) and women had more often an occlusion of the main stem of the middle cerebral artery (34.5% vs. 25.8%;p < 0.0001) and less frequently vertebral artery occlusions (0.4 vs. 1.6%;p = 0.041). Women were less frequently thrombolysed with rtPA (29.4% vs. 39.4%;p < 0.0001), but were more often treated with mechanical thrombectomy (29% vs. 19.9%;p < 0.0001). Women had less favorable outcome at 3 months (mRS ≤ 2: 39.4% vs. 53.6%;p < 0.0001, fatality: 26.5% vs. 21.2%;p = 0.042). In multivariate logistic regression analysis female sex was a predictor of unfavorable outcome (mRS ≥ 3; OR 1.427; p = 0.045).
Conclusions: Clinical characteristics, stroke etiology, treatment modalities and outcome differ between female and male patients thrombolysed for an acute ischemic stroke. Future research should focus on improvement of outcome in female stroke patients.
AS33-021
WOMEN AND STROKE
Oral
DIFFERENCE IN OUTCOME AND RESOURCE UTILIZATION BETWEEN MEN AND WOMEN WITH HEMORRHAGIC STROKE
C. Willers1, I. Lekander2, H. Pessah-Rasmussen3 and M. von Euler4
1Karolinska institutet, Department of Clinical Science and Education and Ivbar Institute AB, Stockholm, Sweden
2Karolinska institutet, Medical Management Centre/LIME and Ivbar Institute AB, Stockholm, Sweden
3Lund university, Dept. Health Sciences and Department of Neurology and Rehabilitation medicine at Skåne University Hospital, Lund, Sweden
4Karolinska institutet, Department of Clinical Science and Education and Karolinska Institutet Stroke research Network at Södersjukhuset, Stockholm, Sweden
Abstract
Background: Differences in stroke care between men and women have been explained by men on average being younger at time of stroke onset. To explore this, achieved health outcomes at one year and received care in Swedish men and women with hemorrhagic stroke were analyzed.
Methods: Patients with registered diagnosis of hemorrhagic stroke (ICD-10 code I61) within regional administrative systems and the Swedish Stroke Register during the years 2010–2011 were included and followed for one year after stroke. Through personal identification numbers, data linkage to multiple other data sources on individual level was performed. Case-mix factors such as age, socioeconomic factors, living arrangements, dependency for activities of daily life (ADL) and severity of stroke were used for univariate and multivariate regression analyses of health outcomes and dimensions of received care (resource utilization).
Results: Population: 1,560 women (47.6 %) and 1,716 men (52.4 %). Performing univariate regression analyses, women showed a lower proportion with good functioning (mRS < 2) at one year compared to men, more net days of sick leave and a higher proportion moving to care home during the year after stroke. In multivariate regression analyses, adjusting for all of the aforementioned case-mix factors, women with hemorrhagic stroke showed higher one-year survival and shorter initial inpatient stay.
Conclusions: After case-mix adjustments for age, stroke severity and socioeconomic factors, living arrangements and ADL we found women to have better survival rate and shorter initial inpatient stay in hospital after hemorrhagic stroke.
AS29-009
YOUNG STROKE PHYSICIANS AND RESEARCHERS
Oral
REPERFUSION INJURY AFTER STROKE STUDY (RISKS STUDY)
B. Piccardi1, M. Nesi2, F. Arba1, V. Palumbo2, P. Nencini2, B. Giusti3, A.M. Gori3, D. Gadda4, S. Nannoni1, G. Pracucci1, A. Fanelli5, S. Mangiafico6, S. Vanni7, L. Pantoni1, C. Sarti2, M. Lamassa2, A. Poggesi1, F. Pescini2, R. Abbate3 and D. Inzitari1
1University of Florence, Department of Neurosciences- Psychology- Drug Research and Child Health, Florence, Italy
2Careggi University Hospital, Stroke Unit, Florence, Italy
3Careggi University Hospital, Department of Experimental and Clinical Medicine- Atherothrombotic Diseases Center, Florence, Italy
4Careggi University Hospital, Department of Neuroradiology, Florence, Italy
5Careggi University Hospital, Central Laboratory, Florence, Italy
6Careggi University Hospital, Interventional Neuroradiology Unit, Florence, Italy
7Careggi University Hospital, Department of Emergency Medicine, Florence, Italy
Abstract
Background: Stroke is a major cause of death and disability. Revascularization techniques are able to re-open occluded vessels, salvaging the ischemic tissue from death. However, recanalization may cause blood brain barrier (BBB) disruption due to activation of molecular pathways eventually determining reperfusion injury and hemorrhagic transformation of an ischemic lesion. Preliminary data show that BBB disruption can be traced in vivo by perfusion CT (CTP). Our aim is to evaluate relative effects of biomarkers (circulating factors versus imaging) in relation to clinical outcomes after revascularization in patients with acute ischemic stroke.
Methods: Consecutive acute stroke patients candidates to intravenous thrombolysis or to endovascular treatment are currently being enrolled in our hospital. Circulating levels of pro-, anti-inflammatory, immunomodulatory factors, metalloproteinases and their inductors/inhibitors, factors of endothelial dysfunction and fibrin resistance to lysis (measured in blood samples of each patients pre-thrombolysis and 24 hours after thrombolysis) will be determined in relation to in vivo measurement of BBB permeability assessed by CTP, symptomatic hemorrhagic transformation and 3 months functional outcome.
Results: Enrollment started on October 2015. As of January 11th 2016, 11 patients have been included. Results are expected by the end of 2017 with an estimated sample size of 120 patients.
Conclusions: Using a definite protocol, a prospective collection of data, and an adequate number of patients assuring statistically powered data, this study will integrate clinical information about biological factors involved in reperfusion injury after cerebral ischemia. Data obtained may help design of randomized control trials to test putative therapeutic strategies in contrasting reperfusion injury.
AS29-010
YOUNG STROKE PHYSICIANS AND RESEARCHERS
Poster
CRYPTOGENIC STROKE IN ATRIAL FIBRILLATION - THE NORDIC ATRIAL FIBRILLATION AND STROKE STUDY (NOR-FIB)
B. Ratajczak-tretel1, A.H. Aamodt2, H. Johansen2, D. Atar3, B. Halvorsen4, E.C. Sandset5, H. Naess6, H. Tobro7, W. Ghanima8, T. Idicula9, T.C. Truelsen10 and D. Russell11
1Østfold Hospital Trust HF, Department of Neurology, Kalnes, Norway
2Oslo University Hospital, Department of Neurology, Oslo, Norway
3Oslo University Hospital, Department of Cardiology, Oslo, Norway
4University of Oslo, Research Institute of Internal Medicine- Institute of Clinical Medicine, Oslo, Norway
5The George Institute, The George Institute, Sydney, Australia
6Haukeland University Hospital, Neurology, Bergen, Norway
11University of Oslo, Institute of Clinical Medicine, Oslo, Norway
Abstract
Background: Different studies with real-life data and randomized controlled trials have shown a detection rate of paroxysmal atrial fibrillation (AF) of 10–20% in patients with cryptogenic stroke using insertable continuous cardiac monitoring for 6 months. More studies are needed, however, to identify factors which can be used to select the patients where the possibility of detecting AF with prolonged rhythm monitoring is highest, to evaluate the best duration of rhythm monitoring, to determine the optimal definition of short-term AF that warrants intervention and to evaluate whether intervention results in improved clinical outcomes.
Methods: The NOR-FIB study is a multi-centre prospective observational trial, designed to evaluate the detection of AF in cryptogenic stroke and transient ischemic attack (TIA). Patients admitted with cryptogenic stroke or TIA in stroke units in the Nordic countries, aged 18–80 years are included and have the Reveal LINQ® Insertable cardiac monitor system implanted for 12 months for the purpose of AF detection. Biomarkers that may identify patients, who could derive the most clinical benefit from the detection of AF by prolonged monitoring, are being studied.
Results: The results will be published in 3 years.
Conclusions: This NOR-FIB study will increase our knowledge regarding occurrence of AF in patients with cryptogenic stroke and TIA that potentially can improve secondary prevention. The study will provide information on biomarkers that may be used to select cryptogenic TIA and stroke patients for long-term monitoring as well as information on the significance of short-term AF and optimal duration of cardiac rhythm monitoring.
AS29-016
YOUNG STROKE PHYSICIANS AND RESEARCHERS
Oral
THE ASPHALT PROJECT: RATIONALE AND DESIGN OF A RANDOMIZED CONTROLLED TRIAL EVALUATING THE COST-UTILITY OF A MOBILE STROKE UNIT IN THE ERA OF BRIDGING THERAPY
G. Turc1, C. Cordonnier2, A. Ricard-Hibon3, S. Dubourdieu4, C. Oppenheim5, H. Chabriat6, O. Naggara5, R. Poll7, S. Descombes8, I. Girard-Buttaz9, Y. Samson10, S. Alamowitch11, P. Amarenco12, X. Leclerc13, M. Obadia14, P. Goldstein15, G. Chatellier16, I. Durand-Zaleski17, J.L. Mas18 and B. Vivien19
1Hopital Sainte-Anne & Université Paris Descartes- Sorbonne Paris Cité & INSERM UMR 894, Neurology- DHU NeuroVasc, Paris, France
2Centre Hospitalier Régional Universitaire de Lille - Hôpital B, Neurology, Lille, France
3Centre Hospitalier René Dubos, SAMU 95, Pontoise, France
4Brigade des Sapeurs Pompiers de Paris, Bureau medical d’urgence, Paris, France
5Hopital Sainte-Anne & Université Paris Descartes- Sorbonne Paris Cité & INSERM UMR 894, Radiology - DHU NeuroVasc, Paris, France
6Hopital Lariboisiere, Neurology - DHU Neurovasc, Paris, France
7Centre Hospitalier René Dubos, Neurology, Pontoise, France
8Centre Hospitalier de Gonesse, Neurology, Gonesse, France
9Centre hospitalier de Valenciennes, Neurology, Valenciennes, France
10Groupe Hospitalier Pitie-Salpetriere, Neurology, Paris, France
11Hopital Saint-Antoine, Neurology, Paris, France
12Hopital Bichat, Neurology, Paris, France
13Centre Hospitalier Régional Universitaire de Lille, Radiology, Lille, France
14Fondation Ophtalmologique Rothschild, Neurology, Paris, France
15Centre Hospitalier Régional Universitaire de Lille, SAMU 59, Lille, France
16Hopital Europeen Georges Pompidou, Methodology & IT, Paris, France
17Hopital Hotel Dieu, URC Eco, Paris, France
18Hopital Sainte-Anne & Université Paris Descartes- Sorbonne Paris Cité & INSERM UMR 894, Neurology - DHU NeuroVasc, Paris, France
19Hopital Necker Enfants Malades, SAMU 75, Paris, France
Abstract
Background: Rationale: Recent trials showed that ambulances equipped with a computed tomography scanner, point-of-care laboratory and telemedicine support (Mobile Stroke Units, MSUs) reduce the onset-to-thrombolysis time and increase the rate of thrombolysis by 50%, as compared to usual stroke care. However, those studies were conducted before the demonstration of the benefit of thrombectomy/bridging therapy, and proof of improved long-term outcome after MSU deployment is currently lacking. Besides, whether MSU represents a viable innovation in health-economic dimensions is still uncertain.
Methods: Aims: We hypothesized that compared to usual care, the deployment of a MSU would result in an incremental cost-utility ratio (ICUR) ≤50,000 euros per QALY in the lifetime horizon.
Results: Design: ASPHALT (Acute Stroke: Prehospital versus in-HospitAL initiation of recanalization Therapy) is an academic-driven, multicenter, open-label randomized controlled trial of MSU deployment versus standard care, with blinded assessment of efficacy endpoints. Randomization will be performed on an individual patient basis. Three distinct geographic areas in France will be alternatively involved, over 6-month periods. 450 acute ischemic stroke patients (emergency call ≤5 hours after onset) will be recruited over a 3-year period, and followed one year. Costs and clinical outcomes including utilities will be collected prospectively during the study period and extrapolated over a lifetime horizon using a Markov model.
Conclusions: Study outcomes: The primary endpoint is the ICUR, based on extrapolated results of the mRS and incremental costs at one year. Secondary endpoints include 3-month and 6-month mRS, ICUR at one and five years, proportion of patients undergoing reperfusion therapies, onset-to-treatment and alarm-to-treatment times.
AS29-017
YOUNG STROKE PHYSICIANS AND RESEARCHERS
Oral
PREHOSPITAL HEART RATE VARIABILITY IN PATIENTS WITH SUSPICION OF ACUTE STROKE: PREDICTIVE AND DIAGNOSTIC VALUE
L. Yperzeele1,2, R.J. van Hooff2,3, P. Vanacker4,5,6, K. Monsieurs7,8, I. Hubloue9,10, P. Cras1,11,12, R. Brouns2,3
1Antwerp University Hospital, Department of Neurology, Antwerp, Belgium
2Vrije Universiteit Brussel, Center for Neurosciences, Brussels, Belgium
3Universitair Ziekenhuis Brussel, Department of Neurology, Brussels, Belgium
4Antwerp University Hospital, Department of Neurology, Bruges, Belgium
5Centre Hospitalier Universitaire Vaudois, Department of Neurology, Lausanne, Switzerland
6AZ Sint-Lucas, Department of Neurology, Antwerp, Belgium
7Antwerp University Hospital, Department of Emergency Medicine, Antwerp, Belgium
8University of Antwerp, Department of Emergency Medicine, Antwerp, Belgium
9Universitair Ziekenhuis Brussel, Department of Emergency Medicine, Brussels, Belgium
10Vrije Universiteit Brussel, Research Group on Emergency and Disaster Medicine, Brussels, Belgium
11University of Antwerp, Research group on Translational Neurosciences, Antwerp, Belgium
12University of Antwerp, Institute Born-Bunge, Antwerp, Belgium
Abstract
Background: Autonomic nervous system (ANS) dysfunction is common in acute stroke and is believed to influence outcome through increased blood pressure variability, impaired cerebral autoregulation, cardiovascular complications and secondary brain injury due to inflammation, hyperglycemia and blood brain barrier dysfunction. Heart rate variability (HRV) has been investigated as a parameter of ANS and a reduction has been reported in association with stroke severity, early and late complications, dependency and mortality. In acute stroke, prehospital diagnosis of reduced HRV may have diagnostic and possibly therapeutic value. Our research group has previously demonstrated the feasibility and reliability of in-ambulance HRV acquisition in an explorative study and demonstrated the correlation between prehospital frequency domain parameters and stroke outcome.
Methods: The objective of this study is to evaluate the predictive and diagnostic value of prehospital HRV in patients with suspicion of acute stroke in an observational, prospective, multi-center clinical trial. HRV will be registered during transportation by emergency medical services of patients with prehospital suspicion of acute stroke, using a non-invasive, 2 lead ECG registration device. Assessment will included time domain, frequency domain, nonlinear and time-frequency analysis. Patients will be included within 24 hours of symptom onset. Patients with pacemaker activity or non-sinus rhythm during registration will be excluded. Recordings with presence of ectopic beats and/or noise in over 25% of the fragment will also be excluded from further analysis.
Results: Not available.
Conclusions: This observational, prospective, multi-center clinical trial will assess the predictive and diagnostic value of HRV in patients with pre-hospital suspicion of acute stroke.