
Abstract
Challenges during the transition to adulthood affect how adolescents and young adults (AYA) with autism integrate their autism diagnoses into their self-concept. A positive autism identity is crucial for their psychological and social well-being. This study examined the suitability of the Illness Identity Questionnaire (IIQ) for assessing autism identity by assessing its construct validity and internal consistency among 102 autistic AYA (12–25 years). Participants completed the IIQ, which measures four illness identity dimensions: rejection, engulfment, acceptance, and enrichment. We conducted confirmatory factor analysis (CFA) to evaluate the IIQ's factor structure and McDonald's omega coefficients for internal consistency. The CFA demonstrated a good fit between the theoretical model and data, χ²(242) = 257.12, p = .241, comparative-fit index [CFI] = .98, goodness-of-fit index [GFI] = .84, root-mean-square error of approximation [RMSEA] = .02, standardized root-mean-square residual [SRMR] = .09. Internal consistency was high across all dimensions (ω = .85–.90). Acceptance was significantly higher than rejection, engulfment, and enrichment, indicating more adaptive identity integration. The findings support the IIQ as a robust tool for assessing autism identity in AYA. The higher acceptance scores align with previous findings indicating more positive than negative feelings towards autism identity. However, the presence of rejection and engulfment underscores the need to promote more positive perceptions of autism identity. The IIQ offers valuable insights into how autistic AYA integrate their diagnoses into their self-concept. A positive autism identity is essential for improving psychological and social outcomes, making the IIQ valuable for researchers and clinicians.
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental condition characterized by persistent differences in social communication and social interaction across multiple contexts and with restricted, repetitive patterns of behavior, interests, or activities. It can range from mild to severe (American Psychiatric Association, 2013; Huerta et al., 2012). These differences manifest in social interactions, particularly nonverbal communicative behaviors, in social–emotional reciprocity, and in understanding, developing, and maintaining relationships (Lord & Bishop, 2015).
Autistic adolescents and young adults (AYA) face multifaceted challenges as they transition to adulthood, impacting their social, educational, and vocational development. Social isolation and difficulties in developing and keeping relationships are prevalent and can lead to significant feelings of loneliness and exclusion (Cheak-Zamora et al., 2019). The transition from secondary to higher education or employment presents another critical challenge. Many individuals with ASD struggle with the demands of academic and professional environments, necessitating specialized support and accommodations that are frequently inadequate (Hendricks & Wehman, 2009). Achieving independence in daily living skills, such as managing finances, performing household tasks, and self-care, is also a significant challenge for many autistic AYA, affecting their ability to live independently (Richard & Duncan, 2020).
A critical component in this life period is identity development, the process by which individuals integrate various aspects of themselves, including personal characteristics and social roles, into a coherent self-concept that shapes their perception of themselves and their place in society (Erikson, 1968). Identity development is essential for adolescents, as a positive and integrated self-concept supports resilience, emotional stability, autonomy, social functioning, and overall health (Cooper et al., 2022; Jovanović et al., 2024). For autistic AYA, developing a positive autism identity is particularly complex due to the condition's pervasive and multifaceted nature, as well as personal experiences, and environmental context (Shmulsky et al., 2021). Positive autism identity has been linked to better mental health outcomes, including reduced social anxiety and improved psychological well-being (Botha et al., 2020; Cohen et al., 2022; Cooper et al., 2022; Lamash et al., 2024) and better social relationships and more understanding of their differences and strengths (Mogensen & Mason, 2015). Whereas, other studies indicate that autistic individuals face difficulties integrating their autism diagnosis into their self-concept, leading to self-conflicts, camouflaging the diagnosis, and stress the need for acceptance and positive self-identity (e.g., Cage et al., 2017; Cooper et al., 2017; Deguchi et al., 2021; Marion et al., 2023; Mazumder & Thompson-Hodgetts, 2019).
Cooper et al. (2022) examined autism identity primarily through the lens of social identity, emphasizing the importance of a sense of belonging within the autistic community. They found that this sense of belonging is associated with collective self-esteem and reduced anxiety, aligning well with the neurodiversity approach. (Cooper et al., 2022). Indeed, this perspective complements the broader view of autism identity as a natural and valuable variation of human cognition. It allows autistic individuals to embrace autism as a core aspect of their identity rather than a deficit to be corrected (Anderson-Chavarria, 2022; Kapp et al., 2013; Nicolaidis, 2012). Within this framework, autistic people are encouraged to view themselves with pride and self-worth, seeing autism as a unique way of experiencing the world (Chapman, 2019; Kapp et al., 2013).
The neurodiversity approach to autism identity offers a perspective that can be viewed alongside the framework of chronic 1 illness identity integration. In reference to chronic health conditions, the concept of Illness identity refers to the extent to which individuals integrate their chronic illness into their sense of self, encompassing varying levels of adaptation, ranging from rejection or minimal acknowledgment to full integration and enrichment (Oris et al., 2018; Van Bulck et al., 2018; Yanos et al., 2010). For those with chronic health conditions, cultivating a strong illness identity can lead to better treatment adherence and fewer clinical symptoms, thus improving quality of life and life satisfaction (Oris et al., 2018; Shneider et al., 2024). The illness identity consists of four constructs: (a) engulfment, meaning that individuals feel their illness dominates their identity; (b) rejection, suggesting that the illness is excluded from the self and seen as a threat, often impacting disease management; (c) acceptance, referring to an acknowledgment of the illness as part of one's identity alongside other personal attributes, without overwhelming the self; and (d) enrichment, describing an experience in which the illness is viewed as a source of personal growth and positive life changes. Research across diverse populations with chronic illnesses—such as those with diabetes, mental health conditions, and cardiovascular diseases—supports the role of positive illness identity in improving social participation, quality of life and promoting adaptive coping behaviors (Oris et al., 2018; Van Bulck et al., 2018; Yanos et al., 2010). In adolescents with type 1 diabetes, for instance, a positive illness identity was found to be linked with better clinical outcomes, including improved treatment adherence and psychological resilience (Oris et al., 2018). Similarly, a well-developed illness identity among individuals with chronic mental health conditions, such as schizophrenia, was found to be associated with enhanced self-efficacy, social support, and functional recovery (Yanos et al., 2010). Another example indicated that adolescents with celiac disease exhibited a generally positive illness identity that was correlated with improved social participation and quality of life (Meyer & Lamash, 2021).
Building on the illness identity framework and the neurodiversity perspective, a chronic health self-reported assessment tool was adapted to assess the self-aspects of autism identity. The Illness Identity Questionnaire (IIQ; Oris et al., 2016) is a validated self-report tool designed to measure four dimensions of illness identity: engulfment, rejection, acceptance, and enrichment. The IIQ has been used effectively among populations with diverse chronic conditions, including those with congenital heart disease and type 1 diabetes, to differentiate more and less adaptive identity states (Oris et al., 2018). The IIQ has shown that less adaptive states like engulfment and rejection are associated with poorer psychological outcomes. In contrast, more adaptive states like acceptance and enrichment correlate with better mental health and physical functioning (Van Bulck et al., 2018).
Previous studies showed the potential of the IIQ to be a reliable tool for assessing autism identity perception (Lamash et al., 2024; Lamash & Meyer, 2023). Those studies using the IIQ adapted for autistic adults indicated correlations between autism identity and social participation (Lamash et al., 2024), well-being, and health-related quality of life (Lamash et al., 2024; Lamash & Meyer, 2023). However, a thorough evaluation of its suitability for autistic AYA is crucial for research focused on how this age group perceives their autistic identity. Such understanding will enable further assistance for young individuals in navigating identity-related challenges. Therefore, this study aims to (a) examine the IIQ's construct validity among autistic AYA, (b) examine the IIQ's internal consistency among autistic AYA, and (c) describe the autism identity perception of autistic AYA using the IIQ dimensions.
Methods
Participants
The sample included 102 autistic AYA (89% male; 11% female) aged 12 to 25 years (M = 18.03 years, SD = 2.76) who completed the self-report IIQ in person. Participants were students in the public education system (57%) or in two transition-to-workforce programs (43%). Table 1 presents the participants’ characteristics.
Participants’ characteristics.

ASD: autism spectrum disorder.
Procedure
The [blinded University’] Faculty of Social Welfare & Health Sciences Ethics Committee approved the study (approval #274/19, 25 July 2019). Recruitment was conducted through social media advertising, autism interest groups, educational frameworks for adolescents with ASD, and workforce-transition programs between 2020 and 2023. This cross-sectional study used an anonymous online survey (Google Forms).
The Illness Identity Questionnaire
The IIQ (Oris et al., 2016) is a self-reported instrument comprising 25 items, developed based on a theoretical framework of four identity dimensions (Luyckx et al., 2008): rejection (five items), engulfment (eight items), acceptance (five items), and enrichment (seven items). Respondents rate their agreement with each item on a 5-point Likert scale from 1 (strongly disagree) to 5 (strongly agree). The IIQ yields mean scores for each dimension, with rejection and engulfment reflecting a lack of illness integration, while acceptance and enrichment capture more adaptive illness integration. The IIQ was validated among AYA with various chronic health conditions, with strong construct and factorial discriminant validity. Reliability coefficients ranged from .75 to .95 across populations (Luyckx et al., 2008, 2018; Oris et al., 2016). The Hebrew version of the IIQ was administered in the current study. This version had been previously translated from English to Hebrew using a standardized forward and back-translation process (Meyer & Lamash, 2021). According to its developers’ recommendations and similar adaptations for other chronic health conditions, we replaced the term “illness” with “autism” in both the title and questionnaire items in this study (e.g., Item 3: “I never talk to others about my autism” and Item 21: “Because of my autism, I have become a stronger person”). Face validity was established by consulting with experts in adolescence and autism (n = 6) and autistic AYA (n = 4). They provided feedback on clarity, relevance, and understandability, confirming satisfactory content and comprehension and supporting strong face validity.
Statistical analysis
Descriptive statistics were used for demographic variables and autism identity profiles. We conducted a confirmatory factor analysis (CFA) with AMOS software (Version 28) to evaluate the validity of the IIQ as outlined (Oris et al., 2016). The CFA was designed to verify the factor structure proposed by the original study, assessing how well the observed variables represent the number of factors associated with illness identity: rejection (Items 1–5), acceptance (Items 6–10), engulfment (Items 11–18), and enrichment (Items 19–25). To validate the one-factor solution for each subscale, separate CFAs were conducted for rejection, acceptance, engulfment, and enrichment. Following this, intercorrelations between the four constructs were examined, yielding the highest goodness-of-fit indices (GFIs). The following GFIs were used to evaluate the model: chi-squared (acceptable when the value is insignificant) and the GFI (values > 0.90 indicating a good fit). The comparative-fit index (CFI), the non-normed fit index (adequate values < 0.90, excellent fit < 0.95), and the root-mean-square error of approximation (RMSEA; adequate values > 0.08, excellent fit > 0.06). The standardized root-mean-square residual (SRMR) was also used to assess model fit with values ranging from less than 0.08 (adequate value) to 0.05 or less, considered reasonable (Arbuckle, 2013; Byrne, 2010). Factor loadings were considered acceptable if they exceeded 0.40.
The data were screened before the CFA for missing values and outliers to ensure the appropriateness of the analysis. Maximum-likelihood estimation was used for parameter estimation in the CFA model. McDonald's omega (ω) coefficient analysis was used to assess the internal consistency of the IIQ factors among the autistic AYA. Because the McDonald's omega coefficient accounts for both the number of items and the factor loadings, it provides a more robust measure of internal consistency. McDonald's Omega values above 0.60 were considered adequate items to be included in a factor. McDonald's Omega values are interpreted on a continuum, with values between 0.60–0.69 reflecting marginal reliability, 0.70–0.79 indicating moderate reliability, 0.80–0.89 representing good reliability, and values of 0.90 or higher signifying excellent reliability (McDonald, 2013). Finally, as a secondary analysis, paired sample t-tests were calculated to examine which factor scored higher in comparison with others.
Results
Confirmatory factor analysis
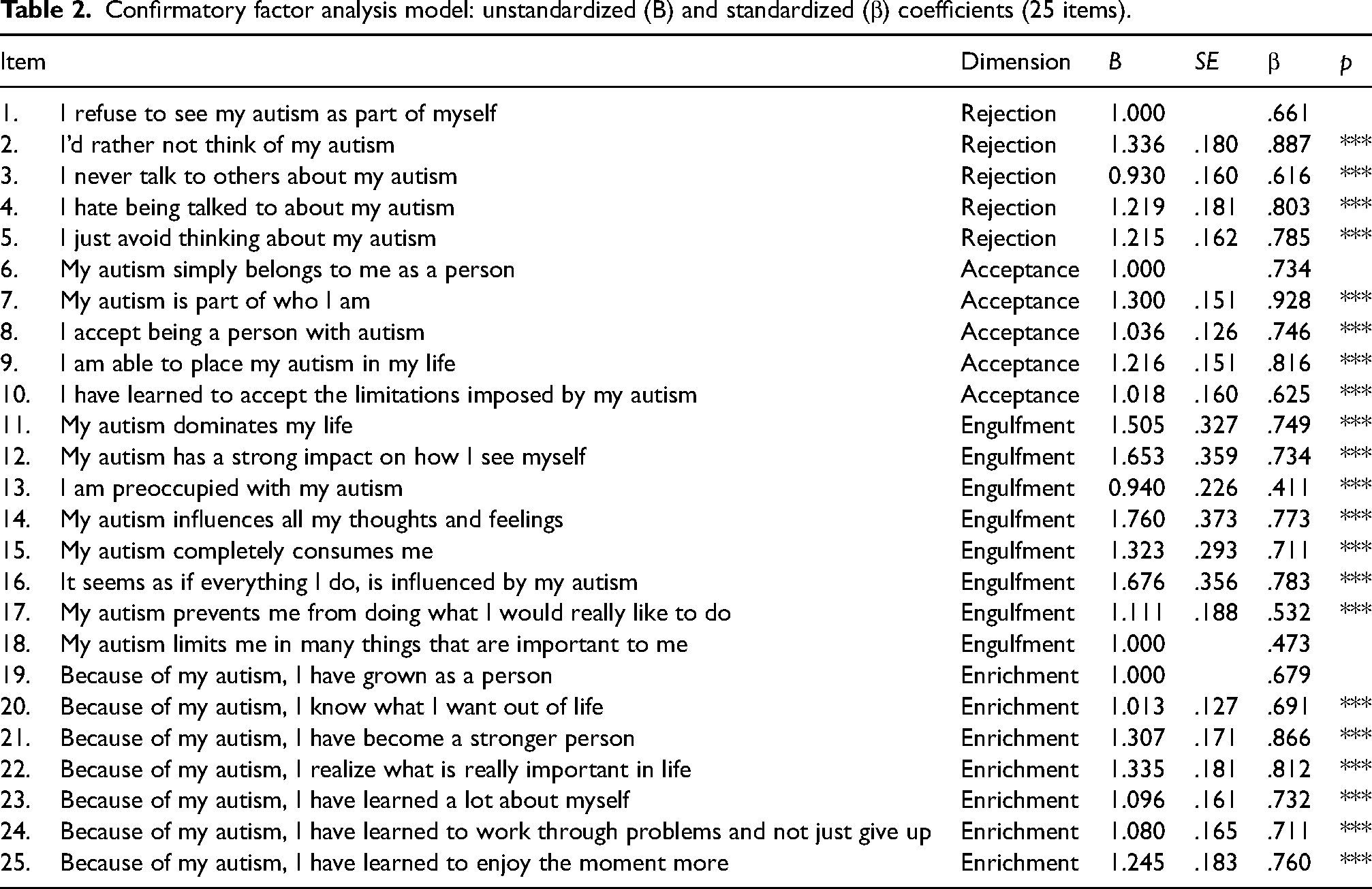
The CFA model showed acceptable fit, χ²(242) = 257.12, p = .241, CFI = .98, GFI = .84, RMSEA = .02, SRMR = .09. All indices except GFI reached the required values. Despite the small sample size, this pattern shows a good fit between the theoretical model and the data. Item loadings on each hypothesized factor, according to the expected structure, were high and significant (Table 2). Specifically, item loading was high on rejection (.61 < β < .89), acceptance (.62 < β < .93), engulfment (.41 < β < .78), and enrichment (.68 < β < .87). As for the engulfment factor, two items showed relatively low loadings (Item 18 [.47] and Item 13 [.41]).
Confirmatory factor analysis model: unstandardized (B) and standardized (β) coefficients (25 items).
Due to the two items with low loadings on the engulfment factor, we performed a second CFA model after omitting Items 13 and 18. The new CFA model also showed an acceptable fit, similar to the 25-item model, χ²(202) = 209.23, p = .349, CFI = .99, GFI = .86, RMSEA = .02, SRMR = .09. Consequently, the initial set of 25 items was retained. Examining intercorrelations between the factors, we found that acceptance was negatively related to rejection (r = −.37, p < .001), positively related to enrichment (r = .49, p < .001), and not significantly related to engulfment (r = .01, p = NS). Rejection had a marginally significant correlation with engulfment (r = .19, p = .05) and was not significantly related to enrichment (r = −.17, p = NS). Enrichment was positively related to engulfment (r = .27, p < .01).
Descriptive and internal consistency of the Illness Identity Questionnaire among autistic adolescents and young adults
Table 3 presents the descriptives and internal consistency for the IIQ among autistic AYA. The internal consistency of the four factors, assessed using McDonald's Omega (ω), demonstrated strong reliability across the scale dimensions. The rejection subscale achieved a high-reliability score (ω = .87), while the acceptance and engulfment subscales also exhibited strong reliability (ω = .85 and ω = .86, respectively). The highest reliability was observed in the enrichment subscale (ω = .90), indicating excellent internal consistency. All coefficients exceeded the commonly accepted threshold of 0.60, reflecting good to excellent reliability across the subscales. These results confirm the robustness of the subscales in measuring distinct yet related constructs, supporting their validity within the overall measure.
Descriptive and internal consistency of the illness identity questionnaire among autistic adolescents and young adults.

Examining the differences between the IIQ dimensions revealed that acceptance was significantly higher than rejection, t(101) = −5.46, p < .001, d = .54; engulfment, t(101) = 10.65, p < .001, d = 1.05; and enrichment, t(101) = 7.52, p < .001, d = .74. In addition, engulfment was significantly lower than rejection, t(101) = 3.66, p < .001, d = .36, and enrichment, t(101) = −5.21, p < .001, d = .72 (Figure 1).

Differences between the Illness Identity Questionnaire dimensions.
Discussion
The Illness Identity Questionnaire validation for autistic adolescents and young adults
This study assessed the construct validity and internal consistency of the IIQ among autistic AYA, demonstrating that it is a robust tool for evaluating how individuals integrate their autism diagnosis into their self-concept. By assessing dimensions such as acceptance, rejection, engulfment, and enrichment, the IIQ offers insights into how autistic individuals perceive and integrate their diagnosis into their self-concept.
The CFA results demonstrate an overall good fit between the IIQ's theoretical model and the data collected from autistic AYA. The initial CFA model, which included all 25 items, showed acceptable fit indices. Although the GFI value was slightly below the recommended threshold, the other fit indices indicated a good model fit (Arbuckle, 2013). This suggests that the IIQ adequately captures the IIQ's four dimensions among autistic AYA. The high and significant item loadings on their respective factors further support the IIQ's construct validity (Byrne, 2010). The limitation that the GFI did not meet the commonly accepted cut-off for adequate model fit, could be attributed to several factors, including the small sample size, the complexity of the model, and the potential for cross-loadings, where certain items may load onto multiple factors. A smaller sample size can reduce the power of the analysis, making it difficult to achieve strong fit indices. Additionally, a more complex model with numerous parameters increases the risk of overfitting and may struggle to capture the underlying data structure adequately, further affecting the GFI. The issue of cross-loadings also deserves consideration, as items that load on multiple factors can introduce ambiguity in the measurement model, complicating the interpretation of the fit indices. These challenges might have contributed to the lower GFI value observed in our analysis. While we aimed to minimize these issues through careful model specification and evaluation, we acknowledge that the results should be interpreted with caution. Future research should consider using larger samples and refining the model to reduce complexity and minimize cross-loadings, thereby improving the likelihood of achieving acceptable fit indices.
Another limitation of our study is the relatively small sample size (N = 102), which may affect the stability and reliability of the CFA results. Common guidelines for CFA suggest having at least 5–10 participants per estimated parameter to ensure robust and accurate estimates. Given our sample size, there is a heightened risk of underpowered analysis, which may result in biased parameter estimates and less reliable fit indices. This limitation implies that the findings should be interpreted with caution, as the reduced sample size could impact the validity of the factor structure. We acknowledge that without a larger sample, our ability to detect true model fit and achieve stable estimates is constrained. Future studies should aim to include a larger sample size to enhance the robustness and generalizability of the CFA results. Despite these limitations, our study provides preliminary evidence that contributes to understanding the factor structure and lays the groundwork for subsequent research with more robust sample sizes.
The IIQ's internal consistency ranged from .85 to .90 across the four dimensions. These coefficients indicate a high level of reliability, comparable to those reported with other chronic illness populations (Oris et al., 2018). Specifically, the acceptance and enrichment dimensions showed the highest internal consistency, aligning with previous research.
The autism identity perception
The sample's autism identity characteristics elucidate that autistic AYA expresses higher feelings of autism acceptance than other dimensions. This finding reflects more adaptive illness integration, meaning they accept their autism as part of their identity alongside other social roles without being overwhelmed by it (Luyckx et al., 2023; Oris et al., 2016). Some research has underscored the importance and protective role of a positive autism identity. For example, autism social identification was positively associated with lower depression and anxiety and higher self-esteem (Cooper et al., 2017). Similarly, Cooper et al. (2022) demonstrated that young autistic people with higher satisfaction with their autism social identity and solidarity with the autistic community had better psychological and social well-being and lower social anxiety (see also Lamash & Meyer, 2023; Mogensen & Mason, 2015). This suggests that the link between autism identity acceptance and improved psychological and social outcomes may also extend to illness identity. An accepting illness identity could similarly foster resilience and adaptive functioning by integrating the illness into one's broader sense of self. Exploring this potential connection highlights the importance of addressing illness identity as a critical factor in promoting well-being, particularly during adolescence. Developing self-identity during adolescence is crucial because it lays the foundation for future psychological well-being and social functioning (Erikson, 1968; Jovanović et al., 2024). Referring to this, Riccio et al. (2020) found that adolescents whose parents voluntarily disclosed their autism diagnosis described both autism and themselves more positively. This outcome indicates that early and positive framing of the diagnosis can facilitate healthier identity development. Notably, a significant portion of participants in this study still experienced negative feelings related to their autism identity. Their relatively high scores on the rejection and engulfment dimensions indicate that negative perceptions of autism persist for many individuals. They can lead to increased psychological distress and social isolation, negatively affecting collective self-esteem and overall well-being (Cooper et al., 2022).
The significant correlations between the four IIQ dimensions strengthen the IIQ's content validity for use in the autism population. Most of these correlations align with findings in other populations (e.g., Luyckx et al., 2018; Oris et al., 2016; Sematlane et al., 2022). Interestingly, we also found a positive correlation between engulfment and enrichment, which contradicts previous studies. This surprising result may be explained by the unique context of autism, where individuals who experience a higher degree of engulfment might also perceive their intense focus and deep involvement in their condition as a source of personal growth and enrichment (Tedeschi & Calhoun, 2004). Specifically, for individuals with autism, the deep immersion in understanding and managing their condition might lead to greater self-awareness and personal development; hence, the observed correlation between these seemingly opposing dimensions. Moreover, the unique coping mechanisms and resilience that individuals with autism develop might contribute to this positive outlook, reinforcing the interconnectedness of engulfment and enrichment (Berkovits et al., 2019; Hobson et al., 2006).
It is also important to consider the gender distribution of the sample, which was predominantly male. While autism is more commonly diagnosed in males, growing evidence suggests that females with autism are often underdiagnosed or misdiagnosed, and the actual gender ratio may be more balanced than previously thought. Women and girls with autism have reported feeling less accepted within the autism community due to not fitting stereotypical ideas about autism (Harmens et al., 2022; Kelly et al., 2024; Seers & Hogg, 2021). These unique experiences may influence how autistic women respond to the IIQ, potentially leading to different patterns compared to males. Future research should explore these gender-related differences to ensure the measure is inclusive and representative of all individuals on the autism spectrum.
The findings of this study highlight the importance of early and supportive discussions about autism and the role of community solidarity in fostering a positive identity. Promoting a supportive environment that encourages positive perceptions of autism can lead to improved mental health and social outcomes, underscoring the need for targeted interventions to address the negative aspects of autism identity (Tan, 2018). Interventions aimed at reducing stigma and enhancing positive self-identity are crucial for improving the quality of life of autistic individuals.
Implications
This study highlights the IIQ's suitability for assessing autism identity among AYA. By providing a reliable and valid measure of how autistic individuals perceive and integrate their diagnosis into their self-concept, the IIQ can inform tailored interventions to promote positive identity development. This is particularly important for autistic AYA, who face significant challenges during the transition to adulthood. Interventions that foster acceptance and enrichment could help mitigate the negative effects of rejection and engulfment, thereby improving psychological and social outcomes (Mazumder & Thompson-Hodgetts, 2019).
Conclusion
This study demonstrated the construct validity and internal consistency of the IIQ among autistic AYA. The findings highlight the value of incorporating the IIQ as a reliable tool for assessing how autistic individuals integrate their autism diagnosis into their self-concept. Furthermore, the results emphasize the IIQ's potential to offer valuable insights into autism identity integration and its influence on various well-being outcomes.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
The University of Haifa, Faculty of Social Welfare & Health Sciences Ethics Committee approved the study (approval #274/19, 25 July 2019).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient consent statement
All participants were required to sign an online consent in order to proceed to the anonymous online survey.