
Abstract
Background
It can be very challenging for practitioners to talk with autistic children, especially when the conversation calls for self-regulation. Self-regulation is inextricably linked to awareness of oneself and others in social contexts. Encouraging the need for autonomy could help increase self-awareness and awareness of others in social events, which in turn could strengthen self-regulation. However, little is known about how autonomy influences competence in reasoning about self and others when regarding social events in which autistic children participate. This study explores the reasoning of self-other awareness on a microlevel timescale using ipsative, dynamic approaches to autism. The central question in this study is: to what extent can autonomy-provided scaffolding (APS) elicit high levels of reasoning about self-others in social events (RSS) over time?
Method
We used video-taped interaction data from three sessions between one autistic child and a practitioner, contextualized by a set of animated DSM-5-based items of social events on which the child was asked to reflect. Interaction variables were the child's level of RSS and the practitioner's level of APS. We coded the real-time interaction.
Results
First, when exploring the dynamics of the microdata, we found contingency over time within sessions. Second, over the sessions, the practitioner showed a stable high level of APS, whereas the child's level of RSS increased. Third, a coupling effect between the level of APS and RSS was found within and over sessions. Salient is that the child and practitioner increasingly adapted to each other over the three sessions, and over time, high-level APS of the practitioner elicited higher levels of RSS of the child.
Discussion
Because the child showed a significant improvement in RSS over time, our research question provides a promising perspective. Contrary to what one might expect in autism, APS supported the performance of the child in reasoning about self-others in social situations. These outcomes underline the importance of giving voice to autistic children. The results may encourage researchers to develop strategies and tools that can help give a voice to children, to gain more insight into the child's reasoning. This may further develop self-other awareness and self-regulation in the social events of autistic children.
Introduction
It can be very challenging for healthcare practitioners and educators to talk with autistic children (Van der Steen et al., 2020). These children often have problems with self-regulation (Barnard-Brak et al., 2014; Laurent & Gorman, 2018; Torrado et al., 2017) and awareness of self and others (Loveland, 2005; St. Clair et al., 2023); their intentions and attempts to interact might be misunderstood by the practitioner (Keen et al., 2005). Self-regulation is a broad concept that can be applied in several contexts and research fields. It can be used to distinguish several types of regulation, like cognition, emotion, and directing attention. Summarizing the use of the term in different research contexts and applications, self-regulation can be defined as “a person's ability to control impulse reactions and manage their behaviour, emotions, and/or attentional capacity” (Williams, 2010). Self-regulation is inextricably linked to awareness of oneself and others in social contexts (Lou, 2012). For autistic people, this awareness is selective or underdeveloped, making self-regulation difficult (Williams, 2010). Self-awareness is, among other skills such as problem solving and, decision making, connected to self-determination (Webster et al., 2022; Wehmeyer et al., 2013). According to Deci and Ryan (2012), self-determination can be fostered when the need for autonomy, competence, and relatedness are met (American Psychiatric Association, 2022; Hesp et al., 2019). In this article, we focus on the interaction between a professional and an autistic child, because for many healthcare practitioners, the interaction with the child is a core activity in therapies and interventions. We explore the reasoning of self-other awareness on a microlevel timescale using ipsative, dynamic approaches to autism spectrum disorder (ASD). Reasoning about self-others can be conceived of as a process that is dynamically formed in real-time interaction between the child and the adult. The theory of complex dynamic systems offers a fruitful framework for analyzing and understanding individual differences in development (=ipsative) in single case studies.
Characteristics of autism
The main characteristics of autism are identified by the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) 5th edition (American Psychiatric Association, 2013). For medical practitioners and policy makers, the DSM-5 is the standard for diagnostic purposes as well as for therapies in ASD (see for an evaluation of the proposed DSM-5; McPartland et al., 2012). According to the DSM-5, ASD encompasses “disorders previously referred to as early infantile autism, childhood autism, Kanner's autism, high-functioning autism, atypical autism, pervasive developmental disorder not otherwise specified [PDD-NOS], childhood disintegrative disorder, and Asperger's disorder” (American Psychiatric Association, 2022). Grzadzinski et al. (2013) reviewed and extended the characteristics of ASD according to the DSM-5 (Table 1). In anticipation of the discussion of the method for the construction of the test items, we used animated items based on criteria A and B (see Method section).
ASD criteria and associated features to be considered when characterizing autistic children.

Note. Proposed diagnostic and statistical manual of mental disorders, 5th edition DSM-5 criteria (left side of the table) and associated features to be considered when characterizing autistic children; reviewed with proposed extension by Grzadzinski et al. (2013) (right side of the table).
ADHD=Attention-deficit/hyperactivity disorder; ASD= autism spectrum disorder; SLI=Specific Language Impairment
Based on their review of the literature, Grzadzinski et al. (2013) expanded (Table 1, right column) the model of the DSM-5 (Table 1, left column) with five additional features that need to be considered when characterizing autistic people: language level, intellectual and adaptive functioning, type of onset, comorbid features, and medical conditions. They paid special attention to language features because their review of the literature revealed rather extreme individual differences in ASD. Idiosyncratic language use is a significant aspect of ASD (Suh et al., 2014). In Table 2, an example of our own experience is presented. However, since the example presents utterances of a child describing a picture, in this case we prefer to use the term “idiosyncratic perception,” since it is neither the grammar nor the vocabulary that are unusual, but the meaning is puzzling. It makes clear that the child does not recognize a person in an image at first sight. The responses of the child may shed interesting light on the affordances of the materials in the ecosystem of the child (Gibson, 1969; Greeno, 1994). According to Bronfenbrenner “the ecological environment is conceived topologically as a nested arrangement of structures, each contained within the next.” The ecosystem consists of both nonphysical (like social-cultural) and physical structures like home, school etc. (Bronfenbrenner, 1977, p. 514).
An example of idiosyncratic perception.

Heterogeneity in autism
Several researchers investigated overlaps between children with Developmental Language Disorder (formerly referred to as Specific Language Impairment [SLI], for an overview see Bishop et al. (2016) and autistic children. Nudel et al. (2020) remarked that the precise nature of this phenotypic overlap has been the subject of debate. In their study, they use a “genome-wide approach to evaluate whether common genetic variants increasing risk of SLI may also be associated with ASD and ADHD” (p. 369). Their results suggest that this is not the case. Later in the discussion, the authors nuanced their results and put them into perspective with respect to the diversity of autistic children: “It should also be noted that the autism spectrum is heterogeneous and includes both children with severely affected language (e.g., children diagnosed with childhood autism) and children with relatively high language skills (e.g., children diagnosed with Asperger syndrome)” (Nudel et al., 2020, p. 376). In this context it is important to recall that autism is very sensitive to comorbidities.
Heterogeneity appears to be the Achilles heel of the DSM-5 definitions of ASD. From this perspective, important criticism comes from philosophers of science like Dehue (2013). Dehue states that a massive corpus of literature on children with a diagnosis in the spectrum of autism provides indirect information on the nature of the disorder. In autism, as in ADHD, a number of features of a disorder are identified as a “thing”, conceptualized as reification (cf. Batstra & Thoutenhooft, 2012; Dehue, 2013). Dehue points out that ADHD is no more than the medical framing of certain undesirable properties, defined in an invalid reasoning in which a property X is valued as disorder Y. However, since the “thing” is a nonexisting artifact of a description, it is important to investigate the individual in finding tailor-made solutions. Another aspect of reification is that labels may give rise to a fixed mindset and get in the way of a growing mindset and developing coping strategies due to its deterministic nature (Yeager & Dweck, 2020). Moreover, these labels may frustrate academic and professional careers, because of misconceptions and prejudices, as in the case of Robin Verstraten: Robin Verstraten was diagnosed with Asperger syndrome as a child. Despite his high marks, he is refused an academic course. The university motivated this decision because the “dynamic environment” of the university could lead to problems for Robin. He is now 23 years old and has, despite of these setbacks, completed two master's degrees (MA Mathematics and MA Fysics). (Zeemeijer, 2020)
A dynamic approach to autism
Since heterogeneity is an essential aspect of autism, this phenomenon needs to be accounted for. Hahamy et al. (2015) argued that there is a growing body of evidence showing that idiosyncrasy, rather than similarity, is one of the defining features of autism (see also Nunes et al., 2019). They stated that the child's process of learning and development was highly idiosyncratic, that is, specific for this particular individual, based on their research into the patterns of connectivity in the brain. Furthermore, they indicate that recent neuropsychological findings show highly individualized alterations in functional connectivity organization in autistic adults. Steenbeek et al. (2018) also found in their study that the child's process of learning and development, specifically about on-task behavior of the child and the number of instructions provided, was highly idiosyncratic, that is, specific for this particular individual. They conclude that “processes of learning and education are very mostly idiosyncratic, that is to say, their properties differ considerably between individuals, and these differences cannot be conceived of as random variation around a common average pattern” (Steenbeek et al., 2018, p. 27).
The theory of complex dynamic system (CDS) offers a fruitful framework for analyzing and understanding individual differences in development (=ipsative) in single case studies (Koopmans, 2016). CDS analyses use models for iterative and reciprocal characteristics of ongoing interactions, including those between a child and its healthcare practitioner (Hesp et al., 2019). Moreover, CDS offers methods and tools for finding relevant information that can improve a better understanding of the idiosyncratic and variable nature of language of autistic children that comes up in the interaction with the healthcare practitioner. An important source of information is (e.g., coded) real-time interaction data.
This study aims to explore ipsative, dynamic approaches to ASD that respect the principle of ergodicity (Molenaar & Campbell, 2009). In ipsative research, data of an individual are compared with the individual itself, not with others, or with other groups. According to the principle of ergodicity “group-to-individual” generalizations are only appropriate if data on individuals (over time) asymptotically follow the same distribution as data across individuals in the population (at any point in time) (Hesp et al., 2019, p. 2). First, according to the principle of ergodicity, a relationship that applies to a sample does not necessarily apply to a process. Second, from a dynamic point of view, autism is not a distinct feature or attribute of a child, but a dynamic developing phenomenon that can be reflected in a multitude of behaviors. Due to idiosyncratic language use and perception, group analysis cannot explain individual trajectories of development. These trajectories are, by definition, nonlinear, and therefore allow for heterogeneous outcomes in understanding development.
A dynamic system consists of intertwined components that can change bidirectionally over time according to an iterative process in a trajectory. Development in such a trajectory can be measured on several timescales. For this research on the interaction between a child and a healthcare practitioner, we used micro as well as meso developmental timescales over several weeks (Steenbeek & van Geert, 2013). At the microlevel, within one session, there is a mutual influence between healthcare practitioner and the autistic child. Because of this coupling of mutual influence, they can adapt to each other's behavior if they find a way to synchronize with each other. The interaction between both actors can lead to a positive (but also to a negative) spiral (see also text below and Figure 1). In such a case, the scaffolding of the healthcare practitioner helps the child to perform a certain task; gradually, the scaffolding stops, while in the end, the child can perform the task independently. In addition, at the meso timescale, or developmental timescale, that is, over several sessions, the coupling effect of the micro timescale may appear. Each microevent (e.g., a conversation or lesson) can be represented as one point on a timescale; drawing several of these points on a timescale, a meso developmental timescale appears, like a week or month, etc. This means that because of the iterative nature of dynamic processes short-time processes affect long-time processes, and vice versa (Steenbeek & van Geert, 2013). Importantly, this implies that even very small steps in the micro timescale matter. A small step can contribute to a significant change in a trajectory, not only for the better but also for the worse.

Scaffolding on an undefined subject on a fictional scale 0–100.
The discovery of this coupling is an important contribution to understanding complex learning trajectories like in ASD, from a dynamic view of development. From a theoretical point of view, this coupling exemplifies that since the learning process is iterative, it is nonlinear by definition. Moreover, it justifies the relevance of dynamic N = 1 case studies that focus on the process characteristics of learning trajectories. By approaching the N = 1 case as a complex system, the principle of ergodicity is not violated.
A second fruitful theoretical framework we use in this article, which deals with motivation and autonomy in health issues, is the self-determination theory (Deci & Ryan, 2008). The relevance of this theory for the present article is that for promoting self-regulation of autistic children, a robust understanding of motivation and autonomy is required.
Self-determination theory in healthcare for autistic children
The self-determination theory (SDT) is a macro theory of human motivation, development, and health (Deci & Ryan, 2008). According to the SDT, motivation is based on three basic needs: competence, relatedness to others, and autonomy. They found that “satisfaction of the needs for competence, autonomy, and relatedness do indeed predict psychological well-being in all cultures” (Deci & Ryan, 2008). Research within the framework of SDT indicates that patients’ autonomy is a critical healthcare outcome in its own right because it promotes improved mental and physical health. An important finding is that when people are autonomously motivated, they experience volition, or self-endorsement of their actions. In short, according to SDT, people are intrinsically motivated when they experience autonomy. Autonomy fulfills one of the (three) basic human needs, competence. In this article, we link the concept of autonomy to Hubers and colleagues’ “to adapt and self-manage” by reasoning that autonomy is the basic need that motivates the development of skills in self-management.
The main idea of SDT and its concept of autonomy in particular can be found in discussions on social innovation. An example is the initiative of Huber et al. (2011). These researchers propose to renew the World Health Organization (WHO) definition of health as “complete wellbeing” to “the ability to adapt and self-manage” in the face of social, physical, and emotional challenges (Huber et al., 2011). “Several dimensions of health can be identified in the social domain, including people's capacity to fulfil their potential and obligations, the ability to manage their life with some degree of independence despite a medical condition, and the ability to participate in social activities, including work. Health in this domain can be regarded as a dynamic balance between opportunities and limitations, shifting through life and affected by external conditions such as social and environmental challenges. By successfully adapting to an illness, people are able to work or to participate in social activities and feel healthy despite limitations.” (Huber et al., 2011, p. 2)
Scaffolding reasoning about the self and others
Self-regulation occurs in relation to our own personal standards as well as to broader, more contextual, and socially accepted standards (cf. Bandura, 1991; Jahromi et al., 2013). In this article, we explicitly add the social constructive and cognitive nature of self-regulation by introducing the concept of reasoning about self-others in social events (RSS). In the present article we define RSS as an active and social constructive cognitive process in which the child reflects on the social processes of (and between) the self and the other. This definition makes explicit that reasoning about social events can be influenced by interaction with healthcare practitioners.
Scaffolding techniques may be used by healthcare practitioners in interactions with children to support RSS skills. Scaffolding helps children to reach a next or higher level of achievement by giving the student some “external” support and by discarding this support after learning has taken place (Ensing et al., 2014; Steenbeek et al., 2012; Van Geert & Steenbeek, 2005). Scaffolding provides temporary support when a child is performing a task that he or she has not yet mastered. After the task is completed, the support can be gradually toned down (Granott et al., 2002; Van de Pol et al., 2010; Wood et al., 1976). Scaffolding has several important aspects. First, scaffolding implies a coupling between the performance level of the student and the level of teaching content of the teacher (Van Geert & Steenbeek, 2005). There is an optimal distance between the two when the level of the healthcare practitioner always stays slightly ahead of the current level of the student. This optimal distance is not fixed but can vary among students and change over time (Kupers et al., 2017).
Scaffolding can be considered a typical dynamic concept because it is based on the iterative nature of interaction. It is about changes over time in which the child and the healthcare practitioner mutually influence each other as in a complex intertwined system of two components (Steenbeek & van Geert, 2013). In Figure 1, the dynamic coupling of a positive spiral is shown.
In healthcare, scaffolding can be used as a technique to improve the health literacy of the child (Veenker & Paans, 2016). Health literacy is the ability of, for example, patients to obtain, understand, and use medical information to benefit their health and to navigate through the healthcare system. In the present study, we investigate the dynamic relationship between APS (autonomy-provided scaffolding) of the healthcare practitioner and RSS of the child on different timescales.
This study
The key question of this article is: To what extent can APS of the healthcare practitioner increase the level of RSS of the autistic child over time? In studying this question, we will focus on the relationship between APS of the healthcare practitioner and RSS of the child.
Question 1: To what extent are RSS of the child and APS of the adult “on the same page” on the micro timescale (within sessions)?
For scaffolding to be effective, it is important that the healthcare practitioner and the child are “on the same page,” in other words that they synchronize with each other and have a mutual agreement of what, for example, the object or subject of joint attention is. Considering the issue of idiosyncrasy, the question of synchronization can be asked: to what degree are dyadic discussion partners sufficiently capable of co-regulating mutual interaction? Fogel (1993, p. 16) describes dyadic synchronous or co-regulated interaction as “matching action that is partly the partner's and partly your own action reflected back to you.” Within this concept, synchrony involves dynamic adaptation on the part of both partners. Dyadic synchrony has been found to play an important role in secure attachment, early self-regulation and autonomy development, and the development of social skills (Kupers et al., 2015; Van der Steen, 2019). In summary, question 1 is to study dyadic synchrony in terms of autonomy in real-time interactions between healthcare practitioner and child. If the child and the healthcare practitioner are indeed synchronizing an important condition for creating a learning situation has been met.
Question 2: To what extent is the level of RSS of the child and the level of APS of the adult related on the meso timescale (over sessions)?
At the meso timescale, we would like to know whether there is a trend indicating an increase in the proportion of RSS. If so, this may indicate that RSS of autistic children is subject to influence from the APS of the healthcare practitioner.
Question 3: How are RSS of the child and APS of the adult dynamically related?
Unlike questions 1 and 2, this third question specifically refers to the iterative sequencing of the utterances of interactions. Since we are fundamentally interested in the dynamics of the interaction, we would like to know whether it can be observed that the health practitioner and the autistic child are to some degree sensitive to each other's utterances that carry respectively information on supporting and performing self-reflecting reasonings. For instance, if both partners collaborate, to what degree can it be established that the child's level of RSS and practitioner's level of APS are dynamically related which can be seen both within the sessions and over sessions. And if so, to what degree can the coupling effects of successions of utterances be perceived?
Methods
Participants
The healthcare practitioner in this study was a scholar of the research group Diversity and Learning Behaviour of the Hanze University of Applied Sciences. The scholar was experienced in using open strategies to evoke reasoning in students in educational primary school settings. She was trained in applying Pivotal Response Treatment and experienced in interviewing autistic children. The student, Ivan 1 was a boy aged 13.7 years with a diagnosis of ASD (diagnosed with PDD-NOS in 2012, DSM-4 criteria were used), IQ 69 (V64; P80). Ivan attended special education. Intellectual disability is common among autistic individuals (Mefford et al., 2012; Moss & Howlin, 2009). Assessment of intellectual ability may be complicated by social-communication and behavior deficits inherent to ASD, which may interfere with understanding and complying with test procedures. “Appropriate assessment of intellectual functioning in ASD is essential, with reassessment across the developmental period, because IQ scores in ASD may be unstable, particularly in early childhood” (American Psychiatric Association, 2013, p. 40). The student participated in an adjacent study that involved a professional development program for teachers about autism. He was asked by his teacher if he wanted to participate in this research. Active written (parental) consent was requested for this research.
Procedure
A set of three conversations was conducted. The main topics were: deficits in social communication and social interaction and restricted repetitive, patterns of behavior, interests, or activities (American Psychiatric Association, 2013). The topics of the conversations were guided by eight animated items that are closely related to the DSM-5 characteristics, see Instrument 2 section. The items consisted of a prototype of an eHealth application of an animated questionnaire. 2 During the three sessions the healthcare practitioner used a simple semistructured interview protocol (see Supplemental Appendix A), comparable with typical conversations that healthcare professionals have or tend to have when talking with autistic children. Our protocol prescribed an introduction in which the practitioner explained the aim and procedure of the interview. After the introduction the student started the application, and the healthcare practitioner used APS techniques to guide the conversation about the task. Each time a new item started, the student was asked first to describe the animation, second to think out loud about the meaning of the animation, third to make self-reflective reasonings, and fourth to indicate the frame that resembles the student's feelings/behavior in the last 24 h and to explain the score (e.g., “And now for yourself”). At this final point the child was invited to motivate the selection of a final score on the respective animated item of DSM-5, a skill that calls on its self-reflective capacity and RSS. When the student and practitioner completed all eight items of the application, the practitioner concluded the session.
The data comprised video recordings of conversations during three sessions between the scholar/healthcare practitioner and the student. All three sessions were recorded with video and transcribed by line. This resulted in 441 (first session), 422 (second session), and 573 lines (third session). Each line was coded both with scales for APS and RSS (Instrument 1 and 2 sections) and at the level of a micro timescale. This type of coding can be used for dynamic analyses.
Instrument 1
To measure the RSS of the child, we used a scale based on skill theory (Fischer & Bidell, 2006). The original scale (Van der Steen et al., 2012) consisted of 10 levels, grouped into three tiers, and built in complexity of skills, starting with a tier on sensorimotor skills and ending with a tier on abstractions, like general rules or laws. Taking the age and capacities of the child in our research into account, we adapted the first and second tiers of the skill theory and moderated it into the scale to gain insight in RSS (Table 3—A). This procedure is also common in research in Science, Technology and Mathematics (STEM) (Meindertsma, 2014; Van der Steen, 2014). We coded each utterance of the child by assigning a level of RSS to the event. We then clustered the levels in high-level or low-level RSS. Levels 1–2 of RSS are considered low-level reasoning, and levels 3–4 are considered high-level reasoning (see Table 3).
Coding student's level of RSS (A) and level of APS (B).

Note. APS=autonomy-provided scaffolding; RSS=reasoning about self-others in social events.
To measure APS, we used a scale based on the Openness Scale of Meindertsma (2014), aimed at measuring the level of autonomy support (or “openness”) the adult provides (Table 3—B). Children show more productive, complex, and elaborative reasoning when the adult uses open questions and encouragements (Chin, 2006; Geveke et al., 2016). The scale on APS has seven levels (0–6) on which utterances of the practitioner can be scored, starting from giving restrictions and directions on the lowest levels, and ending with more open utterances to facilitate student's autonomy in the conversation. We coded each utterance of the healthcare practitioner by assigning a level of APS to the event. We then clustered the levels in high-level or low-level APS. Levels 1–3 of APS are considered as low-level APS and 4–6 as high-level APS (see Table 3).
Independent transcriptions of the observed data were used to calculate interobserver reliability. Matching agreements, were calculated using the proportion reliability method (cf. Steenbeek et al., 2011), for child's RSS of 85% (p < .001) for all levels and 85% (p < .001) for high-low levels was achieved. For APS of the practitioner, agreements of 78% (p < .001) for all levels and 92% (p < .001) for high-low levels were achieved. Finally, all data used in this study were checked by the second rater for consistency.
Instrument 2
A prototype of an eHealth application with animated items related to autism was used to gain insight into how a student perceives and reflects on his/her own disorder. This application consisted of eight graphical, animated digital items related to the DSM-5 features of autism (American Psychiatric Association, 2013): stimulus sensory sensitivity hyper-reactivity or hyporeactivity to sensory input in the environment, looking at other people, understanding feelings; focusing on hobby; difficulty with change; suffering from tics; playing together; and getting nervous. Each item consisted of an animation made of a set of scaled images that moved from, for example, feeling very distressed to feeling very happy (see Figure 2) on the screen. By moving a sliding button, the child could intuitively score on the scale by selecting the most adequate image in the animation. In each session, the same set of eight items was used.

Examples of three stills of animated items on “stimulus sensory sensitivity.”
Data analyses
Q1: To what extent are RSS of the child and APS of the adult “on the same page” on the micro timescale (within sessions)? For this question, we used the Loess smoothing technique (Simonoff, 1996) to visualize the timeseries of the coded data. Smoothed data makes it easier to interpret the data when the data points are very dense, as was the case in this present study. The smoothed timeseries of the level of the student's RSS and the level of the practitioner's APS were plotted for each of the three sessions. We inspected the graphs for patterns of increase or decrease and the extent to which the timeseries of the child and adult went up and down at the same time. For each session, the correlation between the healthcare practitioner's timeseries and the child's timeseries was calculated, using the Pearson correlation method.
Q2: To what extent is the level of RSS of the child and the level of APS of the adult related on the meso timescale (over sessions)? For this issue, we calculated the proportions of the utterance levels of the healthcare practitioner and the child. We also measured the differences within these levels between the three sessions. To estimate the probability that a difference between the sessions was caused by chance alone, a Monte Carlo analysis (Good, 2001) was used. This nonparametric permutation test has good statistical validity in the case of small samples and is used in combination with Excel and Poptools (Hood, 2010). The software also helps with the analysis of the simulation of stochastic processes. After calculating the differences in levels of both RSS and APS (separately) between sessions 1 and 2, 2 and 3, and 1 and 3, the second step was to shuffle the empirical data randomly per level over both sessions that were being compared and again calculate the differences in the proportions of levels between the sessions. The shuffling resulted in randomly assigned data to the sessions. This outcome corresponded to a null hypothesis, which stated that there would be no differences between the two sessions being compared. The third step was to test, using the Monte Carlo simulations, whether the differences in the levels between sessions were larger than the differences in the randomly permuted data (expressed in a p-value). The Monte Carlo simulation technique was used to examine whether the successions were reliable and not caused by change. Therefore, we shuffled the empirical data randomly, which resulted in randomly assigned data to successions. We considered a reliable difference in increase or decrease of a level if the p-value was under .05.
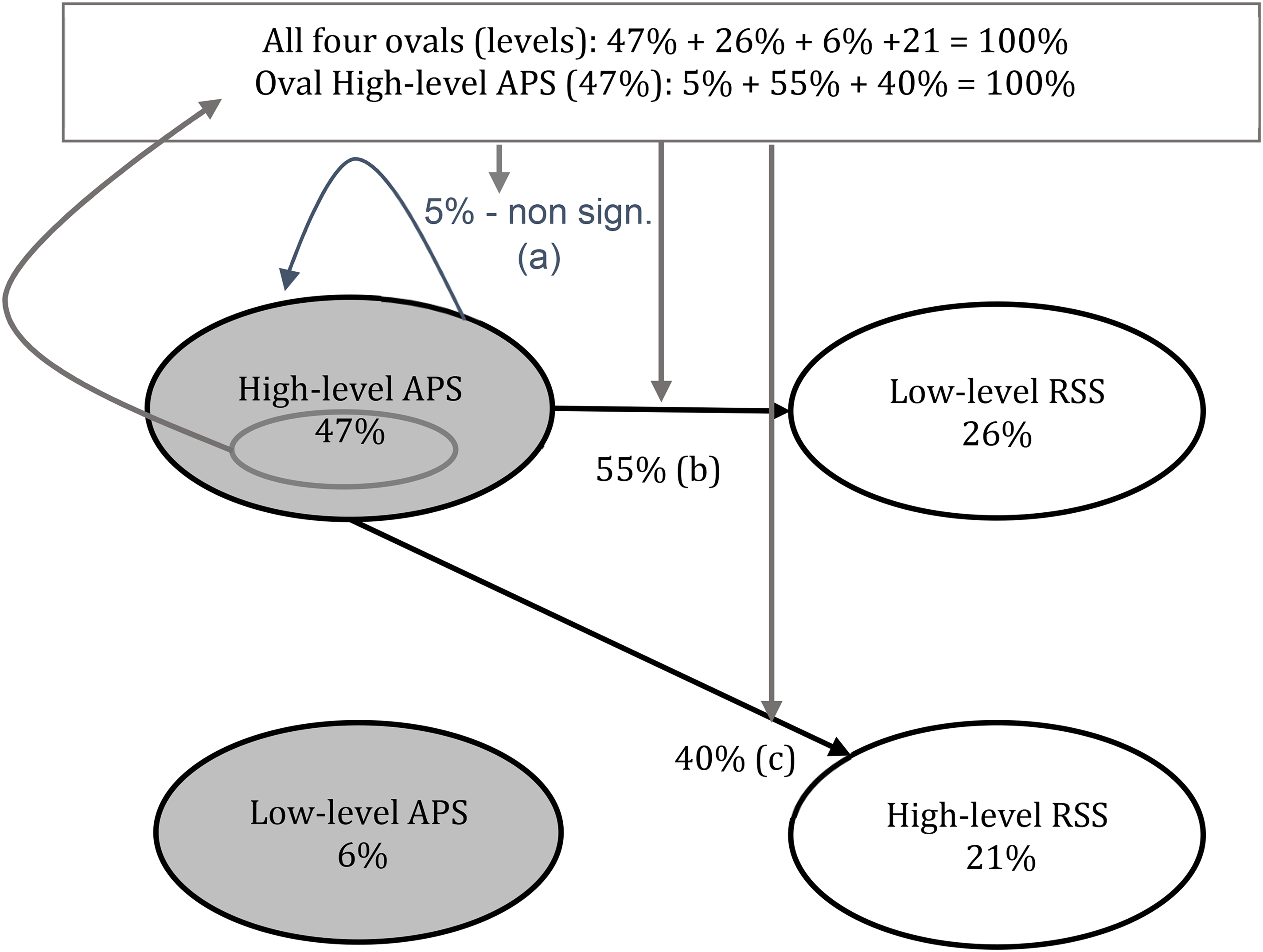
Q3: How are RSS of the child and APS of the adult dynamically related? To investigate Q3 we analyzed successions of utterances in the dyads and analyzed these dyads with quantitative sequential analyses and we visualized the action-reaction patterns with a transition diagram (Guevara Guerrero, 2015; Steenbeek et al., 2012; Van Vondel et al., 2016). We used successions of utterances within a session using the data of the clustered levels of RSS and APS (see Table 3). A transition diagram visualizes the successions of variables using the transition matrix technique. A transition matrix consists of a cross table in which all possible combinations of utterances and their relative proportion of occurrences are listed. By doing so, significant relationships between action–reaction patterns can be found. In this study we were interested in the successions of interactions (two utterances that follow-up on each other) within one session between the practitioner and child.
Figure 3 shows an example of a transition diagram. The utterances of the adult (gray ovals) and child (white ovals) total to 100% (47% + 26% + 6% + 21%). The upper gray oval represents the proportion of utterances coded as high-level APS (levels 4–6) which is 47% in this example. The succession can be found by following the arrows connected to high-level APS. In this example, high-level APS is followed in 55% of cases by an utterance of the child, which is coded as low-level RSS (levels 1–2) (b). In 40% of the cases, high-level APS is followed by an utterance that is coded as high-level RSS (levels 3–4) (c). These two successions are significant (p-value <.05), which means that these successions are substantially present in the interaction. And 5% of the high-level APS utterances are followed by another high-level APS utterance, however this succession is not significant (a). All successions add up to 100%. For clarity, only the significant successions were presented in the transition diagrams in this study. Also, level 0 (off topic; unintelligible; impossible to score) was not included in the results; only content-based successions were considered.
Example of a transition diagram.
Results
Question 1: To what extent are RSS of the child and APS of the adult “on the same page” on the micro timescale (within sessions)?
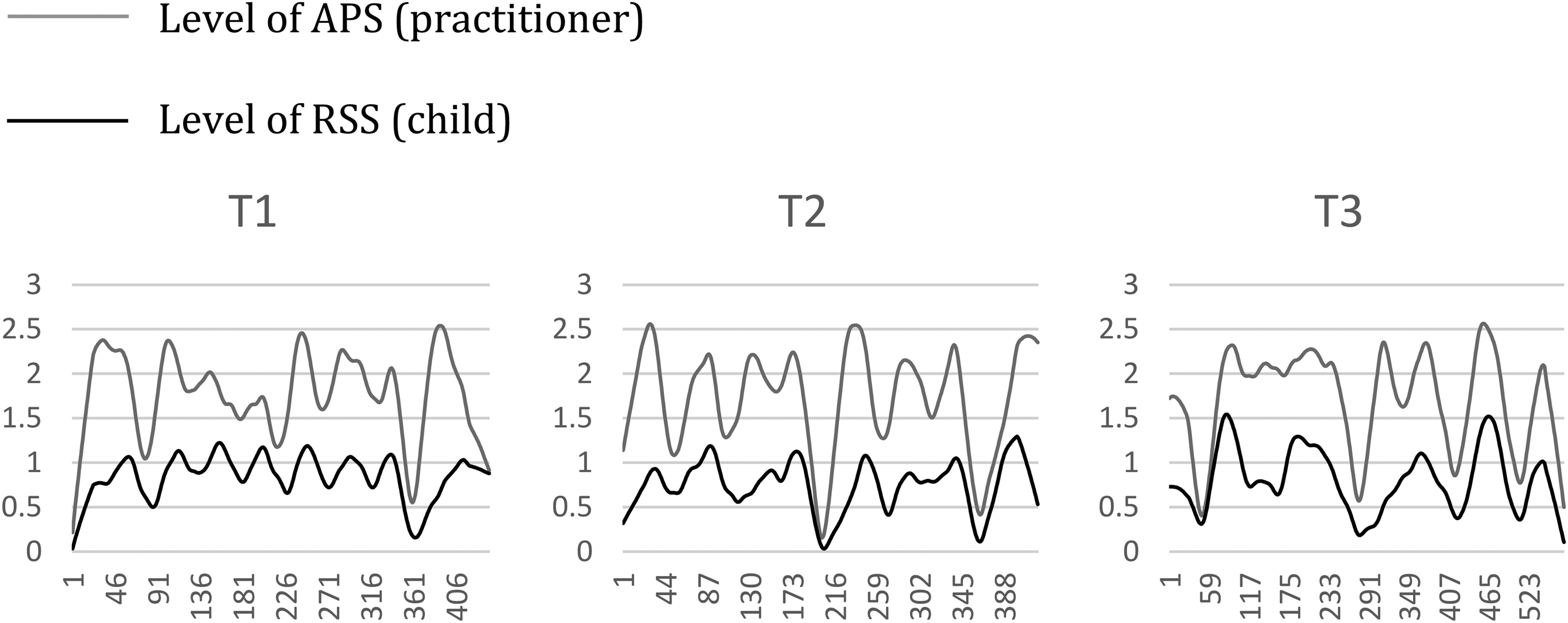
To investigate Q1, we plotted the coded timeseries of the child's RSS (black) and the timeseries of the practitioner's APS (gray) of the three sessions (see Figure 4). The y-axis shows the level of APS/level of RSS, and the x-axis shows the number of consecutive utterances. These are smoothed timeseries, which means that the numbers on the y-axis do not correspond in a 1-1 matter to the levels but are the result of the local regression technique.
Relation practitioner's level of APS and child's level of RSS over time.
Figure 4 reveals synchrony, a dynamic adaptation of both child and adult (cf. Kupers, 2014), in the interactions in all sessions. The interactions follow the same pattern with the correlating lines. Salient is that the child and practitioner increasingly become adapted to each other over sessions, as correlations reveal r = .54 (p < .001) in T1, r = .70 (p < .001) in T2, and r = .79 (p < .001) in T3. This also indicates that on the microlevel, APS and RSS are indeed increasingly related, which shows that child and adult (practitioner) were indeed “on the same page.”
Question 2: To what extent is the level of RSS of the child and the level of APS of the adult related on the meso timescale (over sessions)?
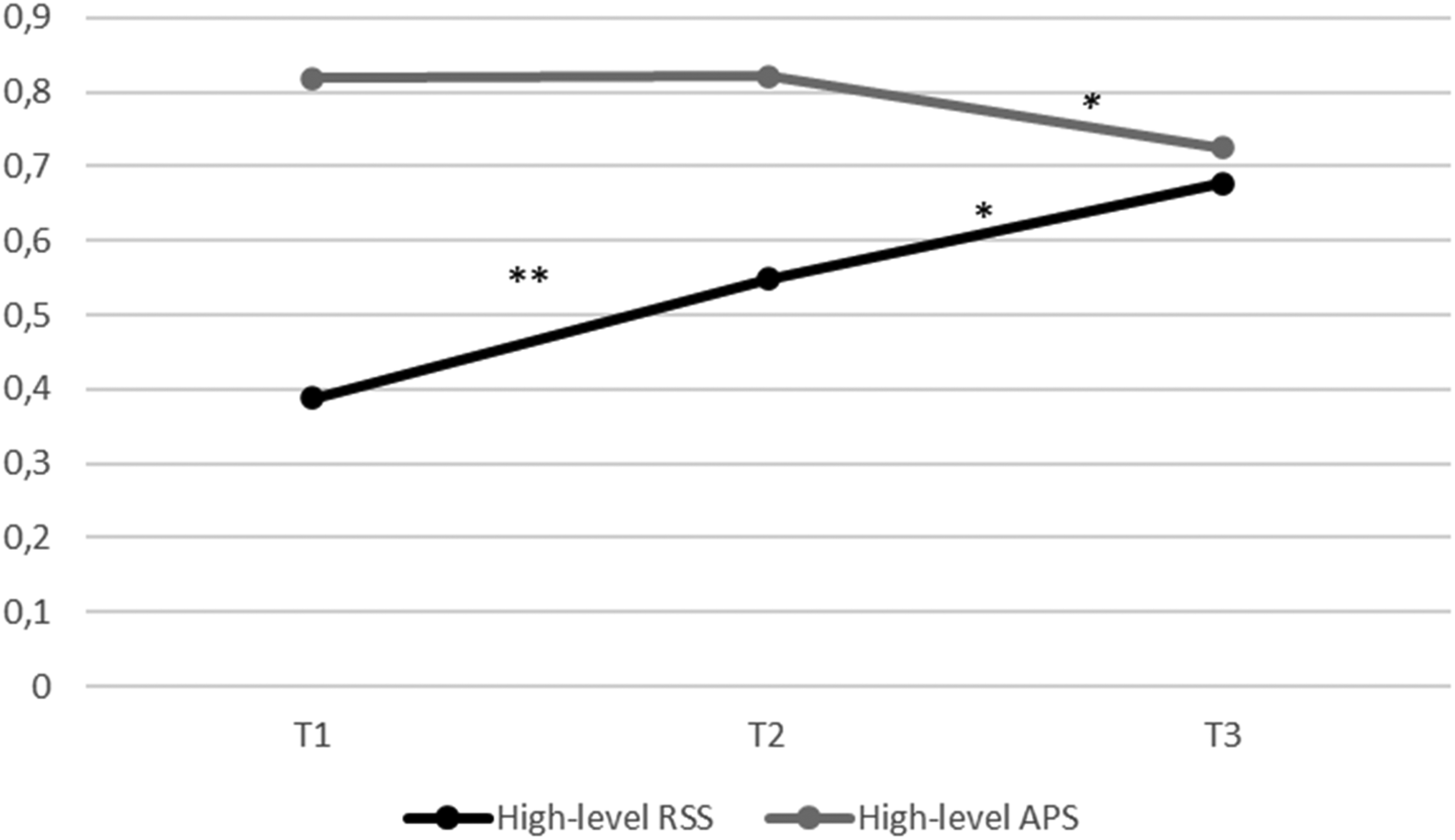
Figure 5 displays the change in the proportions of high-level RSS of the child (black) and high-level APS of the practioner (gray) of the sessions T1, T2, and T3.
Change in proportion of high-level RSS and high-level APS over time.
Figure 5 shows large proportions of high-level APS of the practitioner in all sessions (T1: 0.82; T2: 0.82; T3: 0.72). The proportion of high-level RSS is relatively low (0.39) in T1 but increases in T2 (0.55) and further increases in T3 (0.68). On the one hand, the level RSS of the child does increase over time; on the other hand, the level of APS of the healthcare practitioner shows another pattern with no change between T1 and T2 and a significant decrease T2 and T3. An explanation may be that because the level of APS of the healthcare practitioner is very high from the beginning, she may have reached a ceiling level that is close to an optimum.
Question 3: How are RSS of the child and APS of the adult dynamically related?
For Q3, we displayed the successions of utterances within sessions using a transition diagram. Figure 6 shows the transitions within sessions T1, T2, and T3. Gray ovals show the proportions of utterances verbalized by the practitioner (high-level and low-level APS), and the white ovals show the proportions of utterances of the child (low-level and high-level RSS). Figure 6 shows the selection of only the significant (p < .05) (coupling) arrows. Moreover, bold arrows, as in T2 and T3, represent a significant change between the session and the previous session. For instance, at T2, the bold arrows between high APS–low RSS and high APS–high RSS (resp. 36% and 56%) differ significantly from the same coupling at T1 (resp. 59% and 36%).

Transition diagrams of session 1 (T1), session 2 (T2), and session 3 (T3).
Figure 6 shows the successions within the sessions and over sessions. In session 1 (T1), high-level of APS were followed by utterances of the child coded as high-level RSS (36% of the cases) and low-level RSS (59% of the cases). The other way around: utterances coded as low-level RSS were followed by high-level APS of the adult (73% of the cases), and high-level RSS utterances were followed by high-level APS utterances (71% of the cases). Finally, utterances coded as high-level RSS were also followed by utterances coded as low-level of APS (19% of the cases). In session 2 (T2), almost the same patterns are found. In this session, low-level RSS utterances were also followed by low-level APS utterances (18% of the cases), and the other way around: low-level APS utterances were followed by low-level RSS utterances (43% of the cases). No significant successions were found between high-level RSS and low-level APS in T2. In the last session (T3), a similar pattern as in session 1 was found. In this session, low-level APS utterances were also followed by low-level RSS (21% of the cases).
In summary, if we look at high APS at T1, T2, and T3 a decrease of low RSS (31%–22%–14%) and an increase of high RSS (18%–26%–30%) can be observed.
Over all sessions, the pattern of couplings between high-level APS and high-level RSS, and high-level APS and low-level RSS that is found within the sessions repeats over sessions. Some of these interactions seem to shape the pattern in T2 and T3: the proportion of successions of high-level APS and low-level RSS decreased over sessions (decrease of 23% in T2; p < .001; another decrease of 14% in T3; p = .009), whereas the successions of high-level APS and high-level RSS significantly increased in T2 (increase of 20%; p = .02) and stabilizes in T3 (increase of 4%; not significant).
In sum, it can be concluded that there is a dynamic relationship between APS and RSS which is reflected in a coupling effect between APS and RSS. This is found within and over sessions. These results indicate that, over time, high-level APS have elicited higher levels of RSS.
Discussion
In the introduction, we described the meaning of self-regulation and autonomy in the discussion of social innovation in healthcare (Huber et al., 2011; Deci & Ryan, 2008). In this article, we introduce RSS as an active and socially constructive cognitive process in which the child reflects on social processes of (and between) himself and the other, to elaborate on these concepts. Thus, we express that self-regulation and autonomy should be understood as relational concepts that transcend the individual's knowledge of himself.
The central question of this article is To what extent can APS elicit high levels of RSS over time? The healthcare practitioner used autonomy-providing strategies within a semicontrolled protocol in an interview that was guided by prototyped animated items related to aspects of ASD according to the DSM-5 definitions.
Question 1. It was shown that during the three sessions, the child and the healthcare practitioner were “on the same page.” In other words, the practitioner and child synchronize with each other through dynamic adaptation of both partners, such as mutual alignment on the topic of conversation or an aligned common focus on the topic or object. In this single case study, we found that the degree of autonomy provided by the practitioner is synchronized with the degree of reasoning about the self and others in social events, as evidenced by elevated correlated timeseries of the learner and practitioner showing a pattern of simultaneous peaks over time. Although autistic children have idiosyncratic perceptions, this study shows that these children can certainly come into synchrony when interacting with someone who is specifically focused on APS. Attunement to the child's reasoning is fundamental to shared knowledge construction and the mutual construction of RSS in dialogs.
Question 2. The results of Q3 indicate that there may exist an optimal (ceiling) level for high level of APS, which nevertheless keeps on motivating the child to continue using higher levels of RSS.
Question 3. Furthermore, while the two partners were on the same page in their talks, the coupling of high-level APS and high-level RSS increased over time with a maximum at T2. At the same time, the coupling of high-level APS and low-level RSS decreased. This means that overall (T1, T2, and T3), a significant improvement in coupling between high-level APS and high-level RSS occurred, both at the micro and meso developmental timescales. The practitioner predominantly responded with high-level APS to any utterance of the child in all sessions, and it seems that the child is increasingly profiting from APS over time in terms of high-level reasoning.
In summary, the main result of this article is that high levels of APS can elicit the autistic child to use higher levels of RSS. In addition, protocoled scaffolding strategies as we used in this article appear to have a strong potential to elicit RSS.
We started this article with the problem of healthcare practitioners on how to talk with autistic children when the conversation calls for self-regulation. In line with Huber et al. (2011) and theories on motivation (SDT) (Deci & Ryan, 2008) we were looking for an approach to “give the child a voice.” A short review of the literature on interaction shows that most studies on interaction in ASD focus on talking about children instead of talking with children (cf. Supplemental Appendix B). Exceptions are researchers that start from the motivation of children, like Koegel and Koegel (2006) and Bruinsma and Stockmann (2008). In this article, the autistic child could articulate his voice in self-regulated reasoning, supported by APS based scaffolding techniques. This result is even more remarkable considering the cognitive limitations of the child studied.
DSM-5 and the dynamic approach
In the introduction, we promoted a dynamic instead of a static approach to autism. At the same time, we used the DSM-5 criteria for selecting items for RSS. We would like to make the point that the DSM-5 criteria of features are not static properties of a person but are dynamic and can be influenced over time by being part of a dynamic system. Therefore, it is important that children with a diagnosis in DSM-5 features also develop a growth mindset (Yeager & Dweck, 2020) and that they are being challenged in their RSS by using APS scaffolding techniques. At the same time also healthcare practitioners can use a growth mindset in their own ability to evoke RSS in autistic children. Such a growth mindset is fundamental for achieving robust, durable results in RSS.
Our approach of APS fits especially within approaches or interventions that (also) include nonspecific therapy factors such as a good relationship and interaction between healthcare practitioner and child. The extent to which all this can be influenced depends on the various components and their mutual relationships in the system.
The use of dynamic analyses of microdata of utterances proved to be a solid base for an ipsative approach in a case study. In particular, coding utterances at the microlevel makes the iterative character of for instance coupling between RSS of child and APS of healthcare practitioner possible. The microdata facilitates researchers to closely examine the process of the interaction itself, which gives access to the idiosyncratic nature of development.
Nevertheless, there are also some major drawbacks to this type of research. First it is labor-intensive. It requires the development of accurate transcriptions and adequate scales for coding; supplementary it requires an inter-reliability study on a certain proportion of the data. Second, many such case studies are needed to obtain a good picture of the spectrum of diversity of these types of interactions. A third limitation of this present research is that we used only three sessions for analyses.
Idiosyncrasy
The theory of Gibson about affordances (Gibson, 1969; Greeno, 1994) is fundamentally dynamic in its view of the dynamic relationship between perception and action. In the protocol, the healthcare practitioner explicitly asked the child what he sees. In this step of the conversation, it proved very productive to distinguish according to the neo-Piagetian scale (cf. Table 3). Each level occurred in the responses of the child and facilitated the healthcare practitioner in obtaining a deeper understanding of what the child meant. It also helped the healthcare practitioner to take him seriously and communicate with him as a fully fledged discussion partner. The openness of the healthcare practitioner gives the child the opportunity to talk about his focus of perception. This is information for the healthcare practitioner who can further explore this with the child.
It is not clear whether the responses were merely due to a language problem or whether the child experiences an idiosyncratic perception. For the sake of consistency, we would like to introduce the term “idiosyncratic perception,” meaning “specific for this particular individual.” Since it cannot always be established whether a cryptic verbalization goes back to a language- or a perception-related issue, both options need to be considered.
A suggestion for further research is to elaborate on the linguistic aspect of dynamic interactions in autism that evoke responses, in particular, what verbal and nonverbal iterations evoke context-adequate, meaningful reasonings about self and others.
Scales for the healthcare practitioner and the child
The scale for the healthcare practitioner to support autonomy proved to be a very useful tool for directing reflective conversations in ASD. The scale for the child on reasoning proved to be a very useful tool for eliciting affordances and social reflection. Moreover, the tool proved adequate in measuring the verbal performances of the child.
The scales were designed for use in this research project. Similar scales though were formerly implemented in educational contexts, like primary schools, in the field of Science and Technology (SET) [cf. Geveke, 2017]. We expect that the scales used in the present research can be adjusted for implementation in practices of healthcare practitioners like teachers and practitioners who work with autistic children by means of special coaching trajectories.
The scales may also contribute to the development of health literacy curricula for medical and healthcare practitioners, focusing on patient-oriented skills in “making sense” and “to adapt and self-manage.” The scales can be used by trainees in internships and as tools in research projects for healthcare students. In such projects, scales can be further developed for specific, tailor-made contexts.
In this study, we used the CDS approach as a theoretical framework for developing a better understanding of autism as a developmental process. An important characteristic of dynamical systems is that they change iteratively and therefore nonlinearly in time on micro, macro, and meso timescales. It also follows from the iterative nature that dynamic processes have no direction. Applied to autism as a developmental process, the course of the “autism profile” changes iteratively. If CDS is applied to developmental problems and disorders, including autism, predicting its course is problematic. This also makes it problematic to measure the effectiveness of interventions based on linear measurements using linear research methods in groups. For further research on the development of children with ASD and what healthcare professionals can do to support them, we recommend the use of CDS analyses with models for iterative and reciprocal features of ongoing interactions, including those between child and healthcare practitioner (Hesp et al., 2019).
Supplemental Material
sj-docx-1-dli-10.1177_23969415241268192 - Supplemental material for Reasoning about self and others: A dynamic process
Supplemental material, sj-docx-1-dli-10.1177_23969415241268192 for Reasoning about self and others: A dynamic process by C H Geveke, H J J M Veenker and H W Steenbeek in Autism & Developmental Language Impairments
Supplemental Material
sj-docx-2-dli-10.1177_23969415241268192 - Supplemental material for Reasoning about self and others: A dynamic process
Supplemental material, sj-docx-2-dli-10.1177_23969415241268192 for Reasoning about self and others: A dynamic process by C H Geveke, H J J M Veenker and H W Steenbeek in Autism & Developmental Language Impairments
Footnotes
Acknowledgments
We are grateful to OCRN Youth Care and Madlogic. We owe our special thanks to dr. F. Withaar and G. Dekker. We thank prof. dr. P.L.C. van Geertfor the feedback with regard to the analyses.
Ethics approval and consent to participate
The present paper is solely based on a review of papers published in international scientific journals. The Ethics Advisory Committee of the Hanze University of Applied Sciences (HEAC) stated that research relevant to this article has been exempted from ethical testing (case number 210917). Active (parental) consent was requested for this research in accordance with the guidelines of the ethical committee of the University of Groningen in 2017 when the data was gathered. Furthermore, the Dutch national legislation on medical research (Wet op Medisch Onderzoek) is not applicable. The paper meets the ethics standards of the Dutch NIP (National Institute of Psychologists; code of national professional standards).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported, in part, by a grant from Samenwerkingsverband Noord-Nederland (SNN), supported by the European Union.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.