
Abstract
With the recognition of the problem of child malnutrition in India, the government provides supplementary nutrition under the flagship scheme of Integrated Child Development Services. The scheme has a specific focus on children from geographically and socio-economically disadvantaged groups. In the recent past, although several studies have looked into the access of children to supplementary nutrition services, the effectiveness of the services on children’s nutrition status through the lens of equity has however not drawn adequate attention. This article assesses the nutritional status of children across social groups based on the standard of ‘Nutritive Value of Indian Food’. Data collected from a sample of 286 children across social groups registered under the ICDS scheme covering ten villages in two rural districts of one state; reveals that although the supplementary nutrition meets the protein intake as per the Recommended Dietary Allowances norm, deficiencies are observed in the intakes of nutrients like calorie, calcium and iron. There are notable differentials among children across social groups in the intake of nutrients. The article calls for monitoring of adequacy of supplementary nutrition services for children from disadvantaged groups, and raising nutritional awareness among caregivers.
Introduction
The fundamental right to equality is essentially based on the principle of equity, allowing the state to make special provisions for the advancement of socially and economically weaker sections of Indian society including scheduled castes (SC) and scheduled tribes (ST). Government of India, therefore, implements various schemes/programmes with a special focus on the deprived sections of society (NHRC, 2015). Article 47 of the constitution states that it is the ‘duty of the state to raise the level of nutrition among all people’. As a constitutional obligation government tries to ensure nutrition security in an inclusive manner through various public distribution systems and supplementary food schemes (Sarwal et al., 2022). Ministry of Women and Child Development (MWCD), through its flagship programme of the Integrated Child Development Services (ICDS) provides supplementary nutrition services to children up to six years of age, pregnant women and nursing mothers, with a specific focus on the most vulnerable groups and those who are living in disadvantaged areas like remote rural areas, tribal belts and urban slums. The policy frameworks also prescribe institutional mechanisms through which public resources and services are required to be provided in such a way as to systematically include particular groups of people.
Over the years, the government has accorded the highest priority to combat malnutrition in the county. The ICDS, launched in 1975, is one of the world’s largest and most unique outreach programmes which aims to improve nutritional status of all children. Under the eleventh five-year plan, the universalisation of ICDS expanded the service delivery points (Anganwadi centres) in remote areas to reach out to deprived groups for inclusive growth. However, the intergenerational and multifaceted nature of malnutrition continues to remain a concern. There is a need to further strengthen ICDS based on the lessons learnt from various successful models.
The National Family Health Survey data shows that though the coverage of Anganwadi centres (AWCs) is increasing, the access of eligible children to supplementary nutrition is around 60 per cent (IIPS-ICF, 2021), which means 40 per cent of the children are not accessing the supplementary nutrition from the ICDS centres. Earlier, Meena et al. (2017) found that the mean coverage of ICDS services is around 58 per cent. In a study in Jorhat district of Assam, it is found that although majority of eligible beneficiaries are aware of supplementary nutrition provided by the AWCs many are not satisfied with the services on account of irregular supply of food and poor quality (Burman, 2001). The beneficiaries particularly from disadvantaged sections like SCs are vulnerable to exclusionary behaviours of the dominant caste service providers, affecting equitable access to nutritional services among children (Pal, 2016, 2020). Moreover, the service providers irrespective of their group identity often function under social compulsions, to cause unequal access to nutritional services under the ICDS (Pal, 2022). It is a fact that many children belonging to deprived groups are not privileged enough to have access to adequate food at the household level. The provision of nutrition in AWCs acts as a supplementary source. A recent study (Pradhan & Shete, 2022) based on data from the National Family Health Survey affirms that a sizable proportion of under-five children receiving any ICDS services suffer from undernutrition.
The effectiveness of ICDS services in addressing child malnutrition has been debated on national and subnational platforms. However, despite several evaluation studies focusing on access to nutritional services, the contribution of supplementary nutrition under the ICDS towards children’s nutritional status has not drawn adequate attention. It is expected that if all children access supplementary nutrition under the ICDS, it is more likely to fulfil the unmet need for nutrition among children. However, the persistence of undernutrition among children below six years reveals that the programme has not been effective as expected. So, there is a need to understand to what extent the nutritional services serve the purpose of the ICDS programme. This article makes an attempt to examine the role of supplementary food in meeting the unmet need for nutrients among children belonging to different social groups. It is assumed that, if children belonging to poor households take supplementary food provided by AWCs to supplement the food intake at home, then the nutritional requirement as per the Recommended Dietary Allowances (RDA) norm is more likely to be achieved. An attempt is made to assess the effectiveness of supplementary nutrition provided under ICDS in terms of nutrition intake among children across social groups in rural areas.
Methods
This study is situated in a rural context. For the purpose of this study, data is collected from 300 households with children aged 35–71 months from two rural districts, namely, Mayurphanj and Koraput of Odisha, one of the states in the eastern part of the country with a relatively higher proportion of both SC and ST population. Both districts have the highest concentration of ST population in the state. In the Mayurbhanj district, a higher proportion of ST population lives in plain area whereas in Koraput district a higher proportion of ST lives in hilly area. Sample households were selected from two blocks, one each from two districts. Like the sample district, the selection of blocks was based on concentration of SC and ST population in the districts. A total of 10 villages were identified for field survey, of which six villages were from Mayurbhanj district and four villages from Koraput district. Village selections were mainly based on the village size and households from different social groups. Out of six villages in Mayurbhanj district, three were relatively large/medium-sized villages with higher concentrations of SC and ST population (above 60%) and three villages with medium concentrations of SC and ST population (40%–60%). Similarly, in Koraput district, two villages had a higher concentration of SC and ST population, and in another two villages, there was a medium concentration. The sample households were selected from these sample villages based on the proportion of social groups in the villages. An informed consent was obtained from all the selected households before enlisting children for the purpose of study.
A total of 286 children constituted the sample of children. These children were from the families who showed their willingness to extend support for the study. Mothers of these children however constituted the actual respondents. For the assessment of nutritional status of the children who were enrolled in AWCs, permission was obtained from Anganwadi functionaries. The actual sample size was calculated based on the prevalence studies formula mentioned below.

Where, n = required sample size; z = confidence level at 95 per cent (standard value of 1.96); p = estimated proportion with the attribute; d = margin of error at 5 per cent (standard value of 0.05); and total sample size (N) = 286. Interviews were conducted with the caregivers (mothers) by the researchers with the help of a few trained enumerators using a research tool (interview schedule) specifically designed and pre-tested for the study purpose. The data was collected electronically using tablets with Open Data Kit software. This enabled researchers to transfer data from CSPro files to the statistical software packages for further analysis.
For dietary assessment, dietary recall methods were used to estimate the amount of each food consumed by the children. The intakes of total protein and energy were estimated based on the 24-hour dietary recall data. In other words, caregivers were interviewed to report on food intake of their children during prior 24 hours (defined as the time the child woke up on the previous day and the time the child woke up the day of the interview). Pre-exercises were conducted before actual dietary data collection. Measuring food cups were used to measure the weight of the food consumed as well as the ingredients used in food preparation. The caregivers were asked to report everything that their children had consumed during the 24 hours. The opening questions were like: ‘After you got up this morning/yesterday morning, at what time you give something to eat or drink to your child?’; ‘What did your child eat or drink at that time?’; and ‘Did the child eat or drink anything else?’ These questions were repeatedly asked until the caregiver recalled all the food and drink items consumed by a child over the specified period. The first pass ended with the question ‘Can you remember any other times you had given something to eat or drink to your child?’ In the second pass, caregivers were asked to provide additional detailed information about each item of food and drink consumed by the children. This included the name of the food items, where they had eaten it, cooking methods, amounts served, and amount consumed. For homemade dishes, the caregivers were asked for the recipes and ingredients. The final pass reviewed all previously recalled information to confirm the accuracy of the record. The enumerators had to prompt for information about foods and drinks not mentioned that were considered to be easy to forget, which enumerators had to read from a list. The assessment involved mean daily food intake of cereals, pulses, green leafy vegetables, other vegetables, roots and tubers, milk products, meat, fish, egg, fats and oils, sugar and fruits, and so on. Then protein and calorie values of different items were calculated on the basis of the nutritive value of Indian foods as provided in the standard text ‘Nutritive Value of Indian Foods’ of the National Institute of Nutrition (NIN) (NIN, 2017).
Findings
Child undernutrition and micronutrient deficiencies in India are the highest in the world and worse than many poorer countries (Galvin, 2012; NIN, 2017). Protein-energy malnutrition is the most important factor for high rate of undernourishment of children in India. Itis more common among the children under six years. Protein energy deficiency creates health hazards among children resulting in overall depletion of immunity, and thus opening the gates of plethora of illnesses. However, proportion of children with protein deficiency declines whereas energy deficiency continues. Relative risk of morbidity is higher and is seen consistently in children with energy deficiency, which is manifested in wasting, low BMI for age or in the small group of children who are stunted and wasted (Ramachandran, 2009). Further, it is accelerated due to inability to access adequate food among children specifically belonging to deprived groups. Children belonging to different social groups have access to supplementary nutrition under ICDS. However, there is a difference in access to nutrition among children belonging to different social groups owing to family economic status.
There is a shortage of food at home among the children belonging to scheduled tribes followed by children belonging to SC, other backward classes (OBC) and ‘others’ (upper caste), respectively. The field survey data revealed that the shortage of calories is more than 300-kcal per day among children belonging to scheduled castes and scheduled tribes, while there are around 200-kcal calories and 50-kcal calorie shortages among children belonging to OBC and others respectively (findings from field survey data). A detailed analysis of access to nutrients among children from home supplementary nutrition under ICDS is discussed through the lens of equity approach in the following sections.
Differentials in Nutrient Intake Among Children by Social Groups
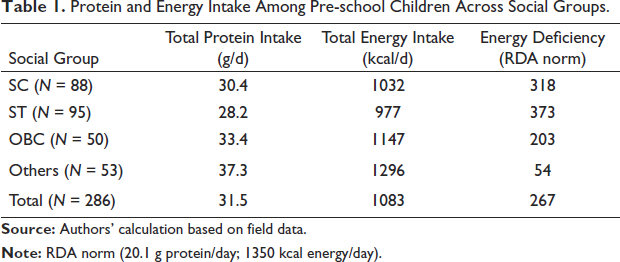
As mentioned, access to food is different for children belonging to different social groups. Understandably, most of the children belonging to SC and ST are deprived of adequate food at the household level for various reasons. Along with the access to food at the household level, the food provided through supplementary nutrition determines the nutritional status of children. Supplementary nutrition is served to these children through the AWCs at the community level. Here the nutritive value of total food consumed in a day is calculated. Table 1 shows that the average intake of protein across social groups is 31.5g per day, which is adequate as per the RDA norm. However, the average energy (calorie) intake among children is found deficient. The average daily energy intake of 1083 kcal is considerably lower than the RDA norm of 1350 kcal. Reversely, the shortage in average daily energy intake is 267 kcal. The deficiency or shortage in energy intake is the highest for ST (373 kcal), followed by SC (318 kcal), OBC (203 kcal), and it is considerably low for ‘others’ (54 kcal).
Protein and Energy Intake Among Pre-school Children Across Social Groups.
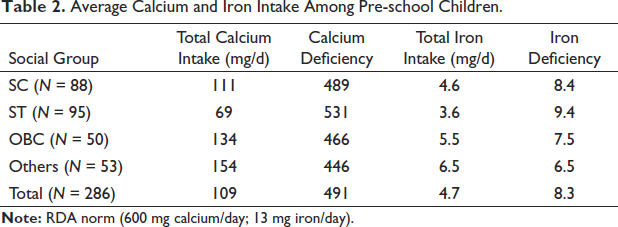
Further, with calorie deficiency, on average a child takes calcium and iron less than the RDA norm (Table 2). While the recommended norm for calcium is 600 mg per day, child takes only 109 mg per day. Similarly, there is also a huge iron deficiency among children across all social groups. On an average, a child takes 4.7 mg of iron against the recommended norm of 13 mg per day. Thus, there is a remarkable difference between the actual intake of calcium and iron and recommended norm for children across social groups.
Average Calcium and Iron Intake Among Pre-school Children.
Differentials in Nutrient Intake from Home Food and Supplementary Nutrition Across Social Groups
Children’s consumption of nutrients from the home food and supplementary nutrition under ICDS provided by AWCs differs significantly. A calculation of protein and energy intake is made based on food consumption at the home and AWCs separately. As per data, children on average get 7.8g of protein from the supplementary nutrition and 23.7g of protein from the home food. The protein intake from supplementary nutrition is notably lower than the ICDS norm of 12–15g of protein per day. The average protein intake by children from home food is adequate. Further, the protein intake of children across social groups does not show remarkable differences.
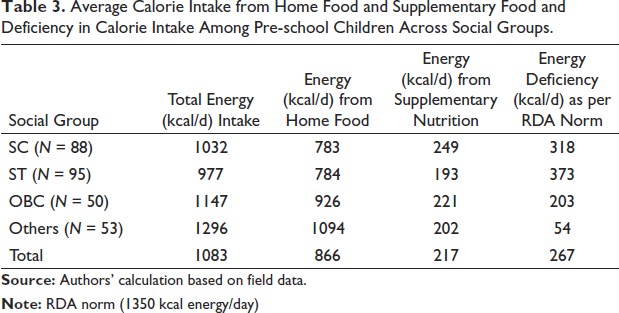
The calculation of energy intake shows that on average, a child gets 217 kcal of energy from the supplementary nutrition and 866 kcal of energy from the home food (Table 3) against the ICDS norm of 500 kcal of energy per day from the supplementary nutrition. Thus, around one-fifth of the total calorie intake per day is received by children from the supplementary nutrition and there is a huge shortage of calorie intake as per the RDA norm even after getting calorie from both the home food and supplementary nutrition. Children belonging to ST have considerably lower amounts of calorie intake from supplementary nutrition as compared to other social groups, with the highest gap even between ST and SC. The variations across social groups in overall calorie intake are seen from the data on energy deficiency in reference to the RDA norm, indicating the highest deficiency among ST (373 kcal) followed by SC (318 kcal), OBC (203 kcal) and others (54 kcal).
Average Calorie Intake from Home Food and Supplementary Food and Deficiency in Calorie Intake Among Pre-school Children Across Social Groups.
It is clear that, though the average total protein intake of children belonging to different social groups is adequate, calorie efficiency still prevails. Children belonging to SC and ST have more deficiency in nutrient intake in terms of calorie deficiency in particular. So, the SC and ST children need more supplementary food than the others. Further, there is a need for effective counselling on nutrition through the AWCs for these children to meet their nutrition requirements as many households have adequate staple food. It is a fact that more SC children attain AWCs than other groups in mixed-caste villages (Pal, 2016). On the other hand, most of the SC &ST children attain AWCs on a daily basis in remote villages. In such a situation, special focus can be given towards AWCs in SC &ST dominated villages as the provision of supplementary nutrition has not been adequate to bring changes in the energy intake of deprived children who have already low energy intake from home food.
An analysis of variance was carried out to assess whether there is any significant difference in calorie intake among children across social groups.
Analysis of Variance (ANOVA) of Calories Intake Among Children by Social Groups.
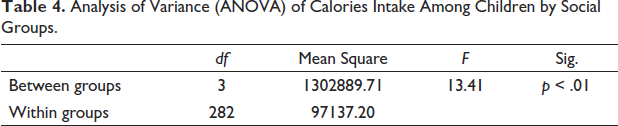
There is significant variation in calorie intake among children belonging to different social groups. This clearly replicates the social group disparity in access to food is exists in rural areas. Though, there are programmes to give priority in distribution of supplementary food to deprived groups, but still these programmes are not able to bring equity in access to calorie consumption among different social groups.
As per the capability approach (Sen, 2000) every child should get adequate nutrient intake as per the need to achieve equality in cognitive development and productivity, and avoid intergenerational disparities. Saxena (2014) opines that SC and ST children have a higher demand for supplementary nutrition services. This is corroborated by the Supreme Court order that more number of AWCs should be opened in the areas with higher concentrations of deprived sections of population. Given that nutrition and health status of children are interrelated, it is argued that healthcare access among economically vulnerable groups needs more curative care (Acharya, 2018) to bridge the gap in health status across social groups.
Protein and Energy Deficiency Among Children Against RDA Norms
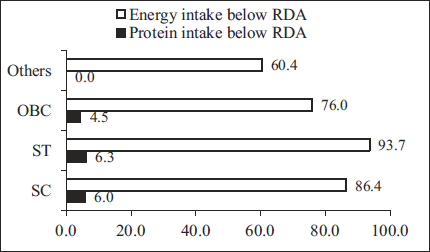
As evident, though the average intake of protein is adequate, there are about 5 per cent children (four to six years) who do not get the protein as per the RDA norm (Figure 1). However the major concern is that the majority of children have energy or calorie deficiency. In both cases, SC and ST children are in disadvantaged positions. As seen, while around 6 per cent of SC and ST children get protein below RDA norm as compared to 4.5 per cent of OBC children. But no child from ‘other’ castes gets protein below the RDA norm. Average energy intake is found a concern for children across social groups. While on average 82 per cent of children have energy below the RDA norm, it is significantly higher for ST children (93.7%), followed by children from SC (86.4%), OBC (76%) and others (60.4%). Besides, the field data also reveals that a large majority of children across social groups have calcium and iron below the RDA norm.
A multivariate analysis was carried out to examine the differences in energy (calorie) intake among children after controlling other background factors (Table 5). The result shows that on an average ST children take 959 kcal of energy, whereas SC children take 1068 kcal of energy. This is comparatively higher for OBC (1135 kcal) and other children (1273 kcal). It reveals that children from socio-economically disadvantaged families take less calories as compared to children from better-off social groups after controlling their other background factors.
Multiple Classification Analysis of Calorie (kcal) Intake Among Children by Background Variables.
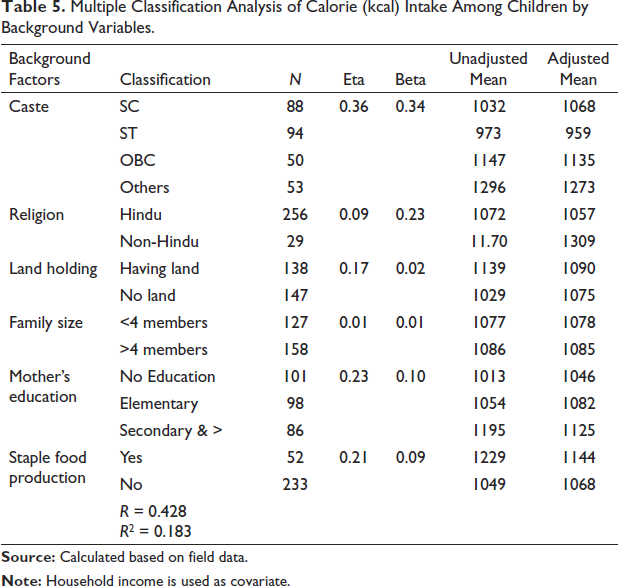
Further, Table 5 shows the factor summary eta, which is the unadjusted correlation ratio and beta-adjusted correlation coefficient. The factor summary shows eta between calorie intake and caste of children, education level of mother and staple food production at household level found to be high, whereas type of family size, religion and land holding of households were found to be relatively low level. Moreover, the eta value shows there is a high association between calorie intake and caste of children as compared to education level of mother and staple food production at the household level. This indicates caste plays a prominent role in access to calories among children. After controlling for the factors and covariates, correlation between children ever born and all selected categorical variables particularly caste of children, education level of mother and staple food production at household level reduced.
Conclusions
Results clearly indicate that children belonging to poor households have low unmet need of protein from home food. To an extent it is met by the provision of supplementary nutrition under ICDS. But shortage of calorie cannot be addressed adequately by the supplementary nutrition. It is evident that if the diet does not contain adequate carbohydrates to provide energy, then dietary protein may be broken down and converted to energy (Gopalan et al., 1989). Children should take adequate calories so that the proteins in the diet are most economically used. One compelling issue is that children in better-off families also have a high unmet need for calorie intake. Although there is no food shortage in these families, still a considerable proportion of children take calories below the RDA norm.
The result shows that protein deficiency prevails among a few children, whereas calorie deficiency prevails among the majority of the children. Only 5 per cent of children are with protein deficiency. However, more than 80 per cent of children are with calorie deficiency. Thus, it is concluded that the average shortage of protein intake among children is low, whereas the shortage of calories is substantially high. Further, children belonging to the scheduled tribe are getting the lowest calories as compared to children belonging to other social groups. During field visits, it is observed that in the tribal areas, children take their dinner in the early evening, and breakfast in the late morning of the next day. Thus, the time gap is more than 12 hours. So, this creates a problem for high-calorie deficiency among children belonging to scheduled tribes. Though there are many programmes that address the nutrition safety of children, it is not well reflected in the conditions of the nutrition status of children. Gopalan (2010) rightly points out that it is important to ensure proper monitoring of the performance of the programme on a continual basis. Martin et al. (2021) view that child nutrition status can be improved through the involvement of family members in maternal and child nutrition guidance campaigns.
There are also program gaps in coverage of supplementary nutrition to rural area, particularly its irregular supply to the beneficiaries (Singh & Gupta, 2016). A review of the functioning of AWCs (NITI Aayog, 2015) shows that 31 per cent AWCs are not intervening in children’s malnutrition. Despite substantial funding for early childhood development programmes, with a large supplementary feeding component, malnutrition among children continues. According to Dutta and Ghosh (2017), the programmes can break the intractable barriers of child stunting not only when the child successfully receives supplementary feeding but also when caregivers collect crucial information on the nutritional awareness and growth trajectory of the child.
Anganwadi workers should give more focus on the nutritional improvement of children through nutrition education, and this should be strengthened in rural and tribal areas through the ICDS and National Health Mission (NHM), as almost all children have calorie intake below the recommended norm. This has been observed over time. Sukhatme (1978) pointed out that Indians get adequate protein from their diet but there is a huge shortage of calories, which is also observed at present time. A recent study conducted in the district of Palghar, India revealed that women had high levels of energy deficiency because of insufficient dietary energy intake (Rajpal et al., 2021). Children belonging to SC and ST groups take much fewer calories as compared to children from other social groups. So, the idea of equity in the nutritional status of children belonging to different social groups through ICDS needs serious attention.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from ICSSR, India for the research and publication of this article.