
Abstract
Introduction
Competency-based medical education (CBME) requires structured and contextually relevant curriculum reform. In obstetrics and gynecology (OBGYN), aligning undergraduate training with clinical competencies and national health priorities remains a global challenge, particularly in contexts with limited opportunities for procedural experience
Objective
To develop, implement, and evaluate a validated, full life-cycle curriculum reform process for undergraduate OBGYN education aligned with Kern's Six-Step Approach and international best practices
Methods
A comprehensive curriculum review and reform were conducted using a validated full life-cycle process. The process included general and targeted needs assessments, international benchmarking, and a sequence of faculty development mini-workshops. Flipped classrooms, simulation, case-based learning, curriculum mapping, and observable professional activities (OPAs) were integrated. Evaluation involved analysis of student satisfaction, competency attainment, and faculty feedback following implementation.
Results
Lecture hours were reduced and replaced with active, learner-centered strategies. Flipped classroom and simulation-based sessions enhanced engagement, communication, and procedural confidence. Student satisfaction scores improved across domains (mean 3.6-4.2/5), and interest in OBGYN as a career increased from <5% to 34%. Faculty reported improved alignment between learning outcomes, teaching methods, and assessment tools.
Conclusion
Integrating CBME principles with flipped and simulation-based methods, mapped OPAs, and structured evaluation yielded measurable improvements in learner performance, engagement, and professional interest. This validated, full-cycle reform process provides a replicable and sustainable framework for curriculum renewal in OBGYN education within regional and global contexts.
Keywords
Introduction
Curriculum development and reform are fundamental to medical education, ensuring that future physicians are prepared to meet evolving healthcare system needs. In obstetrics and gynecology (OBGYN), undergraduate education has increasingly shifted from knowledge-based instruction toward competency-based, learner-centered models that emphasize observable performance, reflective practice, and patient-centered care.1–3 Traditional medical curricula have relied heavily on passive learning approaches, positioning students primarily as recipients of information rather than active participants in clinical reasoning and skill development. The SPICES model student-centered, problem-based, integrated, community-oriented, elective, and systematic has played a pivotal role in global medical education reform by promoting active learning, integration across disciplines, and alignment between educational outcomes and societal needs. 4 Evidence from multiple educational settings suggests that SPICES-informed curricula enhance learner engagement, clinical reasoning, and readiness for practice, particularly when combined with structured assessment and feedback mechanisms.4,5
Competency-based medical education (CBME) further advances this paradigm by defining training outcomes in terms of demonstrable abilities rather than time-based progression.6,7 CBME frameworks emphasize integration of basic and clinical sciences, workplace-based assessment, and continuous feedback, enabling learners to translate knowledge into effective clinical performance.8,9 In the context of rapidly expanding medical knowledge and changing patient expectations, cyclical curriculum evaluation and renewal have therefore become essential to maintain educational relevance, quality, and accountability. 10
Prior to reform, undergraduate OBGYN education at our college of medicine was characterized by a predominantly lecture-based structure, variability in clinical exposure across training sites, limited opportunities for supervised procedural skills, and inconsistent alignment between learning outcomes, teaching strategies, and assessment tools. Student and faculty feedback highlighted challenges related to learner engagement, equity of learning experiences, and preparedness for core obstetric and gynecologic competencies, underscoring the need for systematic curriculum renewal. In Saudi Arabia, reforming undergraduate OBGYN education is particularly important due to national women's health priorities and cultural considerations affecting intimate examinations. Variability in patient availability and gender-related sensitivities may further limit students’ exposure to essential obstetric and gynecologic procedures. These contextual factors necessitate innovative educational strategies such as simulation-based training and structured case-based learning to ensure competency attainment while maintaining patient dignity and safety.11,12
Although several studies have reported educational innovations in OBGYN teaching, including flipped classrooms and simulation-based modules, the existing literature largely focuses on isolated interventions, short-term electives, or postgraduate training.13,14 Recent work on entrustable professional activities has demonstrated how observable clinical tasks can be integrated into undergraduate curricula to support competency-based assessment and feedback.15,16 However, few studies describe the integration of observable professional activities (OPAs) within a full life-cycle curriculum reform process.
Guided by Kern's six-step approach, this study introduces a validated, full life-cycle curriculum review and reform process applied to an undergraduate OBGYN clerkship. 6 The novelty of this work lies in the systematic integration of CBME principles, SPICES-aligned educational strategies, OPAs, curriculum mapping, and structured evaluation within a culturally contextualized framework.1,4,8
The objective of this study was to develop, implement, and evaluate this comprehensive curriculum reform process and to examine its impact on student satisfaction, competency development, and interest in OBGYN as a career.
Methods
Curriculum Review Framework
This project was conducted as an educational quality-improvement initiative designed to develop, implement, and evaluate a comprehensive reform of the undergraduate OBGYN clerkship. The reform followed a validated full life-cycle curriculum review process, designed by a medical education consultant (Dr Nehal Khamis) and led by the first author in her role as Department Chair at the time. The process was guided by Kern's six-step approach and aligned with CBME principles.
The curriculum review and reform process were conducted in two sequential phases. Phase I (figure 1) focused on conducting general and targeted needs assessments, completing a curriculum database, and establishing faculty consensus on priority women's health conditions relevant to the Saudi context, in addition to globally relevant healthcare problems. This phase also included a series of structured faculty development mini-workshops and the development of standardized templates for curriculum mapping and evaluation.

Phase I of the validated full-cycle curriculum review process.
Phase II (figure 2) involved defining intended learning outcomes (ILOs), selecting aligned teaching and learning strategies, designing assessment approaches, and establishing mechanisms for continuous evaluation and refinement. This phase was guided by international academic reference standards and best practices in health professions education, including those of the

Phase II of the validated full-cycle curriculum review process.
Setting, Participants, and Study Period
The reformed curriculum was implemented and evaluated during the 2017-2018 academic year at the College of Medicine, King Saud University. Eligible participants included all undergraduate medical students who completed the reformed OBGYN clerkship during the study period, as well as faculty members who were actively involved in teaching or supervising students within the clerkship.
Participants were recruited through the routine end-of-course evaluation process. Participation was voluntary and anonymous for both students and faculty.
Needs Assessment and Benchmarking
A general needs assessment compared the existing curriculum with international programs (United States, Canada, and the United Kingdom) and Saudi NCAAA standards. A targeted needs assessment through faculty, resident, and student feedback identified skill gaps and content redundancies, emphasizing the need for a structured, competency-based, and engaging curriculum that ensures equity in learning experiences across all clinical settings.
Faculty Mini-Workshops
The consultant conducted a sequence of faculty development mini-workshops to operationalize each step of the six-step framework. Workshops covered outcome definition, instructional alignment, and assessment strategy, using standardized templates to ensure coherence and shared understanding among teaching faculty.
Curriculum Mapping
Customized curriculum mapping templates linked outcomes with teaching methods, assessment tools, and OPAs. Mapping ensured horizontal and vertical integration, alignment with national accrediting body domains, and inclusion of cognitive, affective, and psychomotor objectives.
Validation and Refinement
All proposed revisions were reviewed jointly by the consultant and OBGYN faculty. Content validation involved iterative expert review to ensure feasibility, cultural appropriateness, and educational integrity. Revisions balanced foundational knowledge with procedural and communication training.
Implementation and Educational Strategies
Implementation transformed 2 weeks of lectures into flipped classroom modules supported by videos and case-based group discussions. Simulation-based training was integrated for core procedures, including pelvic examinations, deliveries, and emergency management. Curriculum mapping and logbooks linked each session to specific OPAs, facilitating documentation of clinical competence.
Assessment and Evaluation
A comprehensive assessment blueprint was developed to align learning outcomes with teaching strategies and assessment methods. The evaluation of the reformed clerkship incorporated both quantitative and qualitative approaches, including student and faculty satisfaction surveys, faculty feedback, supplement file 1&2, and review of competency documentation through logbooks.
Student and Faculty Evaluation Surveys
Student perceptions of the reformed OBGYN course were assessed using a locally developed 36-item questionnaire rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). 17 The survey evaluated key clerkship domains, including clarity of learning objectives, teaching organization, effectiveness of educational strategies (flipped classrooms, case-based discussions, and simulation), clinical exposure, feedback, learning environment, and overall satisfaction. Content validity was established through expert review, and the instrument was piloted for clarity prior to use. Formal psychometric validation was not undertaken, as the tool was intended for educational quality-improvement purposes.
Faculty perceptions were assessed using a 10-item structured questionnaire, also rated on a 5-point Likert scale, 17 covering course organization, teaching methods, student engagement, assessment strategies, balance between clinical settings, and workload feasibility. The instrument underwent expert review for content relevance, and mean scores were calculated to identify strengths and areas for improvement.
Response Rate
A total of 267 undergraduate medical students were eligible to participate, and 267 completed the post-course evaluation questionnaire, yielding a 100% response rate. Faculty feedback questionnaires were completed by all faculty members involved in the clerkship during the study period.
Ethical Considerations
This educational quality-improvement project was reviewed and approved by the Institutional Review Board no. E-22-7348. Participation was voluntary and anonymous, and no identifiable data were collected. Written informed consent was obtained in accordance with COPE guidelines, with retrospective consent accepted for this educational initiative.
Statistical Analysis
Descriptive statistics were used to summarize student and faculty evaluation data. Likert scale responses were reported as means and standard deviations for individual items and domains. No inferential statistical analyses were performed, as this project was conducted as an educational quality-improvement initiative and was not designed for hypothesis testing or comparative comparisons.
This study was conducted as an educational quality-improvement initiative and is reported in accordance with the SQUIRE 2.0 (Standards for Quality Improvement Reporting Excellence) guidelines. Specifically, reporting was aligned with the SQUIRE-EDU extension, and the completed checklist is provided as Supplementary File 3. 18
Results
Table 1 summarizes key differences in curriculum structure, educational strategies, and assessment approaches before and after implementation of the reformed OBGYN curriculum.
Comparison of Undergraduate OBGYN Curriculum Before and After Reform.
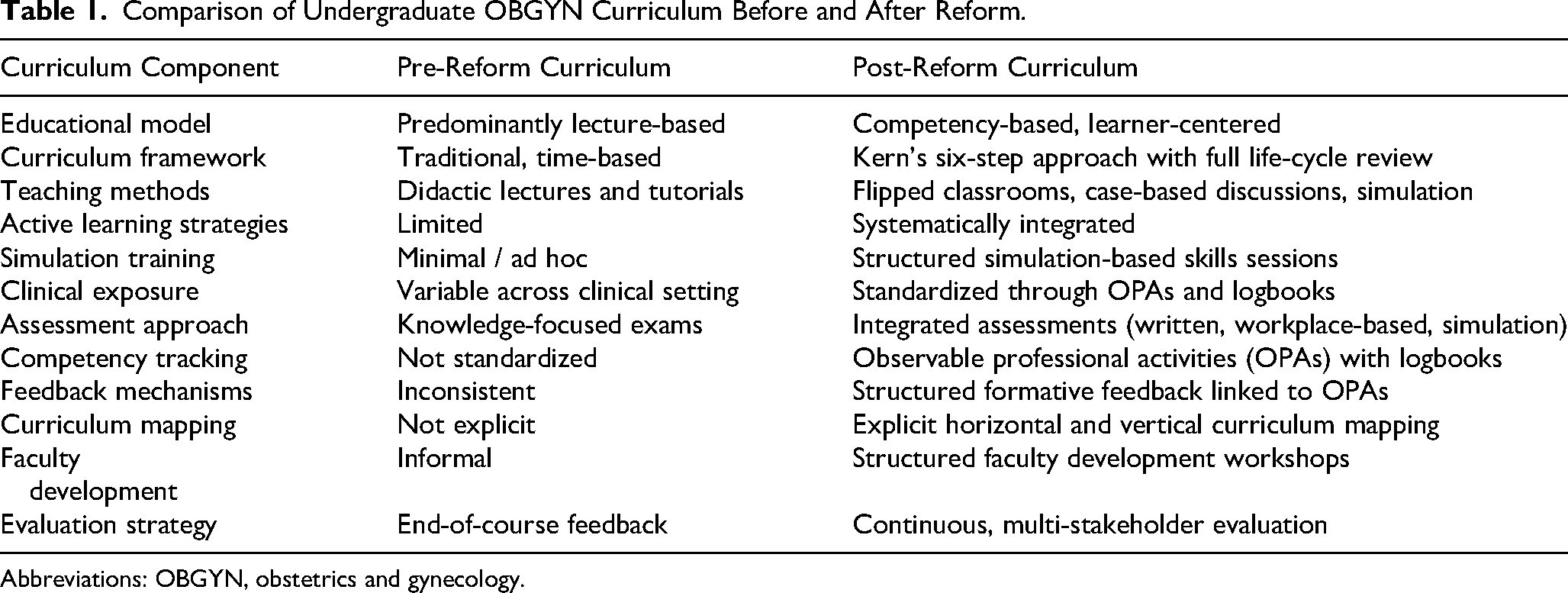
Abbreviations: OBGYN, obstetrics and gynecology.
Participant Characteristics
A total of 267 undergraduate medical students completed the OBGYN clerkship during the study period and were included in the analysis. All participants were enrolled in the same undergraduate medical program and completed the clerkship under a standardized curriculum structure. No individual demographic data were collected, as the evaluation focused on course-level educational outcomes.
Targeted Needs Assessment Finding
Prior to curriculum reform, the undergraduate OBGYN course consisted of 2 weeks of lectures and tutorials, followed by clinical rotations in which students were assigned to small groups attached to consultants, registrars, and interns. Clinical activities included outpatient clinics, ward rounds, and operating room sessions. Feedback collected from students and faculty identified several challenges, including variation in teaching methods, inconsistency in the number and type of clinical cases encountered, unequal exposure to surgical procedures, and limited integration between OBGYN clinical activities. Inconsistent student attendance and variable levels of interest in the course were also reported.
Curricular Structure Following Reform
Following implementation of the reform process, the undergraduate OBGYN curriculum was restructured in alignment with national accreditation requirements and international academic standards, including benchmarks from the APGO.
Key structural features of the revised curriculum included:
Alignment of student and faculty guides, course specifications, assessment blueprints, and required clinical encounter lists Curriculum mapping to ensure horizontal and vertical alignment between ILOs, teaching methods, and assessment tools
The traditional 2-week lecture block was replaced with a diversified instructional model comprising:
17 focused lectures 28 video-assisted and case-based discussion sessions 5 simulation-based skills laboratory sessions 2 interactive case seminars
Observable Professional Activities and Logbook Documentation
Twelve OPAs were introduced to operationalize competency-based training (Table 2). Each OPA represented a core professional task contextualized to the local clinical environment and aligned with internationally benchmarked learning outcomes. Student participation in OPAs was documented using a structured logbook, with completion verified by supervising faculty signatures. Faculty used the logbook to document exposure to required clinical activities and to provide formative feedback. Aggregated logbook data indicated that a proportion of students completed all required OPAs, with higher participation recorded for labor and vaginal delivery experiences and lower participation observed for assisting in gynecologic surgical procedures.
Observable Professional Activities (OPAs) and Required Clinical Encounters in the Revised OBGYN Clerkship.

Abbreviations: OBGYN, obstetrics and gynecology.
Student and Faculty Evaluation Findings
All 267 eligible students completed the post-clerkship evaluation questionnaire, yielding a 100% response rate. Evaluation findings are presented descriptively. Mean student satisfaction scores across evaluated domains ranged from 3.5 to 4.2 out of 5 (Table 3). Mean scores for flipped classroom activities and case-based discussions ranged from 3.8 to 4.0, while mean scores related to clinical exposure and feedback ranged from 3.5 to 3.8. Faculty feedback surveys demonstrated mean scores of approximately 4.0 for clarity of course objectives and perceived effectiveness of flipped classroom activities. Mean scores related to workload manageability and structure of patient care teaching ranged from 3.6 to 3.7. At the end of the clerkship, 34% of students indicated interest in pursuing OBGYN as a future career.
Summary of Quantitative Findings Following Curriculum Reform.

Abbreviations: OBGYN, obstetrics and gynecology.
Design Intent and Program Outcomes
The revised curriculum incorporated structured educational strategies, OPAs, and logbook documentation to support standardization of learning activities and documentation of clinical
Discussion
Medical education is a continuously evolving discipline that requires systematic renewal to remain responsive to learner needs and community expectations. This study describes the application of a validated, multidisciplinary, full life-cycle curriculum review and reform process in an undergraduate OBGYN clerkship, guided by Kern's six-step approach and informed by CBME principles.
Interpretation of the findings should be considered in light of several important limitations. The study was conducted at a single institution, employed a descriptive design, and relied primarily on self-reported student and faculty evaluations, which may be subject to response bias. In addition, objective pre- and post-reform measures of competency attainment and longitudinal outcome, and comparative analyses were not assessed. As this was a whole-cohort educational intervention, no a priori sample size calculation was performed.
Within these constraints, the descriptive findings demonstrate the feasibility and acceptability of implementing an integrated CBME-aligned curriculum reform within a culturally contextualized undergraduate setting. The reform aligns with international efforts to better prepare undergraduate learners for competency expectations encountered in postgraduate training. Prior work by Morgan et al described a milestone-based pilot curriculum incorporating flipped classrooms and simulation to support early residency readiness among senior medical students. 19 In contrast to this short elective model, the present study implemented a comprehensive, clerkship-wide reform, integrating OPAs, curriculum mapping, and structured evaluation across all learners. This broader scope enabled standardized documentation of required clinical activities and improved alignment between learning outcomes, instructional strategies, and assessment tools.
The instructional restructuring specifically, the replacement of an intensive lecture block with flipped classroom sessions, case-based discussions, and simulation-based training is consistent with active learning approaches reported in undergraduate clinical education. Student evaluation data demonstrated moderate to high satisfaction with these strategies, supporting their acceptability within a time-limited OBGYN clerkship. While these findings do not permit conclusions regarding educational effectiveness or superiority, they suggest that learner-centered strategies can be incorporated without compromising curricular structure or content coverage.
Integration of CBME principles through OPAs operationalized expected competencies into observable clinical tasks. The use of structured logbooks facilitated documentation of student participation in core activities and supported formative feedback. 20 Although conclusions regarding competency acquisition cannot be drawn, these findings demonstrate the feasibility of OPA-based documentation as a structured approach to monitoring clinical exposure in undergraduate training.
Sustainability of curriculum reform is a critical consideration, particularly in clinical disciplines with high service demands and resource-intensive educational strategies. In this initiative, sustainability was supported through phased implementation, use of standardized teaching and assessment templates, and targeted faculty development workshops that promoted shared understanding of educational goals and methods. Although simulation-based training requires dedicated facilities and faculty time, its integration was limited to core competencies and aligned with existing institutional resources, minimizing additional workload. Faculty feedback indicated that the revised curriculum was manageable within existing clinical responsibilities, suggesting that the model is feasible for continued implementation and potential adaptation in similar educational contexts.
An additional descriptive observation was the proportion of students expressing interest in OBGYN as a future career at the end of the clerkship. While causality cannot be inferred, this finding is consistent with previous literature suggesting that structured, supportive, and engaging undergraduate learning environments may positively influence specialty perceptions and career decision-making.21,22 Further longitudinal studies are needed to determine whether such interest translates into residency selection or long-term career outcomes.
Few published studies describe a comprehensive, validated, and iterative curriculum reform process spanning needs assessment, benchmarking, implementation, and evaluation at the undergraduate level. The integration of Kern's framework, CBME principles, OPAs, simulation-based strategies, and curriculum mapping within a culturally contextualized structure distinguishes this work as a transferable model for clinical disciplines facing similar educational and contextual constraints.6,14,15,20 Future research should focus on multi-institutional implementation, longitudinal outcome assessment, and objective measures of competency attainment. As this study was conducted as a whole-cohort educational quality-improvement initiative and analyzed descriptively rather than as a hypothesis testing study, an a priori sample size calculation was not performed.
Conclusion
This study demonstrates the feasibility of a competency-based, full life-cycle curriculum reform within an undergraduate OBGYN clerkship. Based on the descriptive findings, institutions seeking similar reforms may consider integrating flipped classroom and simulation-based learning to enhance engagement and address variable clinical exposure, and implementing OPAs with structured logbooks and curriculum mapping to support alignment between learning outcomes, teaching strategies, and assessment methods. These approaches offer a practical and adaptable framework for undergraduate OBGYN curriculum renewal
Supplemental Material
sj-docx-1-mde-10.1177_23821205261445332 - Supplemental material for Developing Tomorrow's Obstetrics and Gynecology Physicians: A Holistic Approach to Undergraduate Curriculum Transformation
Supplemental material, sj-docx-1-mde-10.1177_23821205261445332 for Developing Tomorrow's Obstetrics and Gynecology Physicians: A Holistic Approach to Undergraduate Curriculum Transformation by Lateefa Othman Aldhakil, Salwa Neyazi, Malak M. Alhakeem, Ahmed Abdulwahab Abdulkarim and Nehal Khamis in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205261445332 - Supplemental material for Developing Tomorrow's Obstetrics and Gynecology Physicians: A Holistic Approach to Undergraduate Curriculum Transformation
Supplemental material, sj-docx-2-mde-10.1177_23821205261445332 for Developing Tomorrow's Obstetrics and Gynecology Physicians: A Holistic Approach to Undergraduate Curriculum Transformation by Lateefa Othman Aldhakil, Salwa Neyazi, Malak M. Alhakeem, Ahmed Abdulwahab Abdulkarim and Nehal Khamis in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205261445332 - Supplemental material for Developing Tomorrow's Obstetrics and Gynecology Physicians: A Holistic Approach to Undergraduate Curriculum Transformation
Supplemental material, sj-docx-3-mde-10.1177_23821205261445332 for Developing Tomorrow's Obstetrics and Gynecology Physicians: A Holistic Approach to Undergraduate Curriculum Transformation by Lateefa Othman Aldhakil, Salwa Neyazi, Malak M. Alhakeem, Ahmed Abdulwahab Abdulkarim and Nehal Khamis in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The authors thank all faculty members and students of the Department of Obstetrics and Gynecology for their collaboration, as well as the medical education department, and Prof. Mona Soliman for ongoing support throughout the reform process.
Author Contributions
LOA conceived and led the curriculum reform project, supervised all phases of design, implementation, and evaluation, and drafted the initial manuscript. SN and MMA contributed to curriculum development, faculty coordination, data collection, and manuscript review. AAA participated in curriculum implementation, data acquisition, and critical revision of the manuscript. NK provided expert guidance in medical education, designed the full life-cycle curriculum review framework, led faculty development workshops, and contributed to study design and critical manuscript revision. All authors reviewed and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Human and Animal Welfare Statement
This study did not involve experiments on humans or animals. All procedures were conducted in accordance with ethical standards and institutional guidelines where applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.