
Abstract
Background
Motivation is a key determinant of engagement, learning, and well-being for medical students. Guided by Self-Determination Theory, this study examined the intrinsic and extrinsic contributions to motivation across the medical school curriculum using the Work Extrinsic and Intrinsic Motivation Scale (WEIMS).
Methods
This longitudinal study surveyed medical students using the 18-item WEIMS at 5 timepoints: 0 months (matriculation), 12 months, 18 months, 30 months, and 48 months (graduation). Subscales represented 6 motivational types: Intrinsic, Integrated, Identified, Introjected, External, and Amotivation. While the first three subscales reflect forms of autonomous or self-driven motivation, the latter three capture motivation influenced by external pressures or the absence of motivation, altogether. Composite indices included the Work Self-Determination Index (W-SDI), which summarizes how much a person's motivation comes from within themselves versus outside pressures. Reliability was assessed with Cronbach's alpha, and longitudinal differences were evaluated with 1-way analysis of variance and Welch t-test (Holm-corrected).
Results
A total of 1828 surveys were analyzed. Overall, Work Self-Determined Motivation was significantly higher than Work Non-Self-Determined Motivation at all measured timepoints. W-SDI scores were significantly higher at matriculation (mean (SD): 15.387 (5.99)) compared to 18 months (12.13 (6.94), P < .0001), 30 months (12.50 (7.16), P < .0001), and 48 months (13.59 (6.89), P < .01). This decrease in W-SDI arose from significant (P < .0001) increases in external regulation at 18 months (0.52), 30 months (0.54), and 48 months (0.52), as well as a significant increase in amotivation at 18 months (0.32, P < .01) and 30 months (0.29, P = .012).
Conclusions
Medical students’ motivation is dynamic throughout training. Self-determined motivation is higher than non-self-determined motivation at all time points but declined slightly throughout training. These results may help guide the development of curricula that enhance autonomy, competence, and relatedness to sustain intrinsic motivation throughout medical education.
Introduction
Motivation is a critical and dynamic component of medical student learning, well-being, and professional development. 1 Success in medical education demands sustained engagement and self-regulation, particularly in response to negative feedback. 2 Understanding how and why medical students remain motivated throughout their training is essential for fostering success, resilience, and long-term professional fulfillment. 3 Student motivation may be intertwined with professional identity formation (PIF), a developmental process through which learners internalize what it means to be a physician. 4 Self-determined forms of motivation, particularly identified and integrated regulation, align closely with PIF, as they reflect the incorporation of professional goals into one's sense of self.
Grounded in self-determination theory (SDT), motivation is rooted in our innate need for competence, autonomy, and relatedness. Within individual contexts, motivators that support or defy these needs can be conceptualized as intrinsic to the subject or extrinsic, often sociocultural, factors. Self-determination itself can be viewed on a spectrum from the unregulated, or amotivated, to the intrinsically regulated, self-determined learner.5,6 Within this framework, intrinsically regulated behavior in medical students may promote a more biopsychosocial approach to medical care, emphasizing aspects of regulation such as autonomy within the clinician–patient relationship. 7 Furthermore, medical students with highly intrinsic motivational profiles have been shown to achieve a higher GPA and report lower rates of exhaustion compared to status-motivated or low-motivation medical students. 8 In medical training, we suspect that motivation is shaped not only by individual traits, but also by institutional structures such as workload intensity, assessment practices, and grading schemas. These contextual factors may differentially support or constrain autonomy, competence, and relatedness across phases of training.
Little is known about how the motivation of medical students evolves across the trajectory of their training, from matriculation to the final clinical years. Medical education is characterized by major transitions that reshape students’ motivational profiles, such as the shift from pre-clinical coursework to clinical rotations, and the increased focus on residency preparation and matching successfully in a desired specialty and program. Each phase presents new challenges that may reinforce or challenge students’ sense of autonomy and purpose. 9 This pace of change has accelerated in recent years as shifts toward remote or virtual learning environments require students to adapt to maintain motivation.10,11
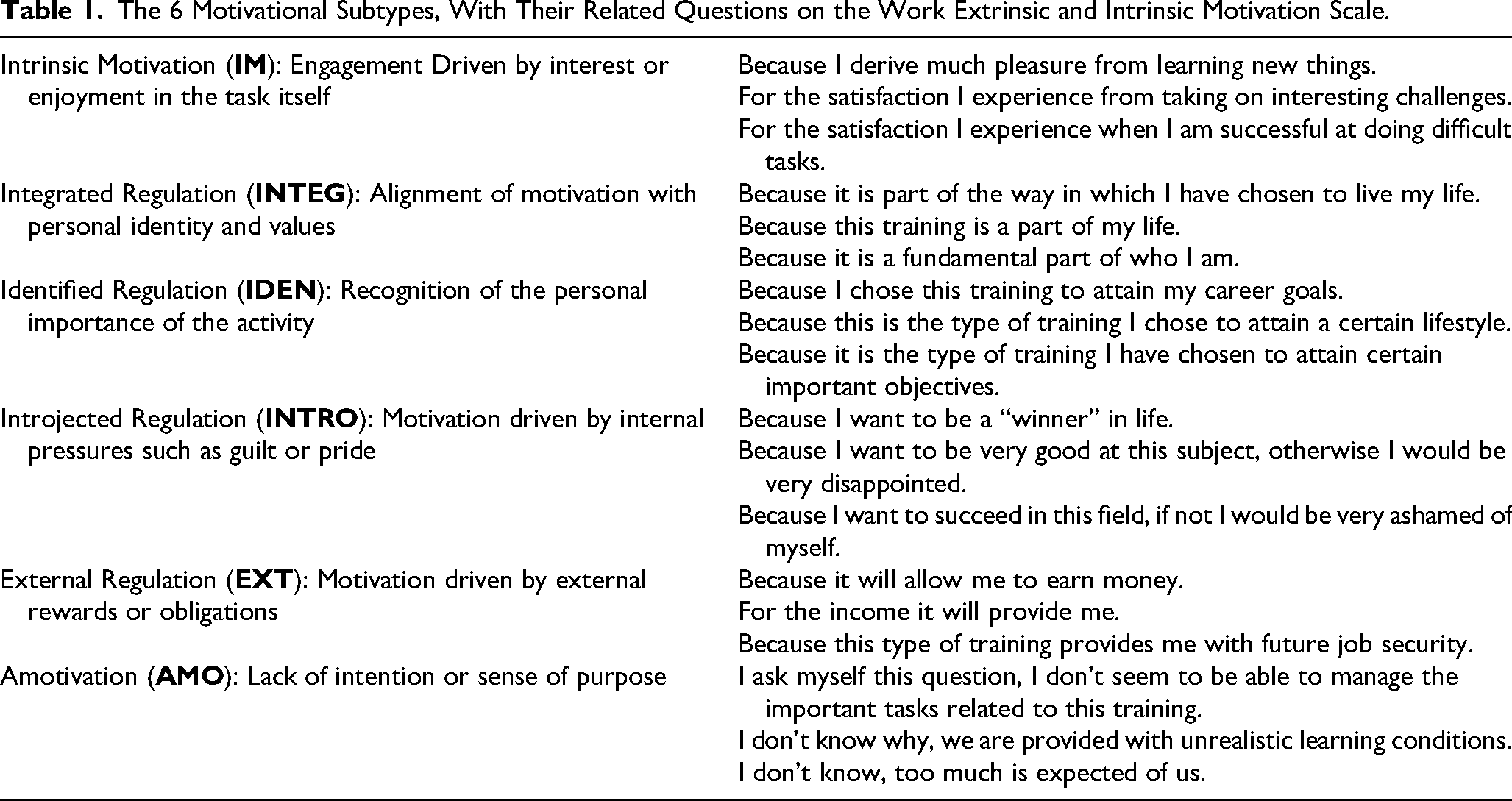
To examine longitudinal changes in motivation across students’ training, this study employed the Work Extrinsic and Intrinsic Motivation Scale (WEIMS). 12 The WEIMS was originally developed for use in occupational settings to assess motivation along the SDT continuum and has demonstrated strong internal structure and construct validity across diverse professional populations. Although not originally designed for medical education, we considered its theoretical grounding well-suited to examine motivation in students whose educational experiences increasingly resemble professional work. This validated tool captures 6 motivational subtypes: Intrinsic Motivation (IM), Integrated Regulation (INTEG), Identified Regulation (IDEN), Introjected Regulation (INTRO), External Regulation (EXT), and Amotivation (AMO). 12 Using responses collected at 5 timepoints, from matriculation through graduation, this analysis explores the primary motivating factors that medical students experience, and how their motivation profiles shift throughout the curriculum. Assessment of both subscale scores and composite indices, such as the Work Self-Determination Index (W-SDI), allowed us to identify periods of motivational decline or growth, and to determine whether certain forms of extrinsic motivation (eg, external vs identified regulation) become more dominant as students progress through training. Insights from this work can inform curricular design and student support interventions aimed at sustaining autonomous motivation, preventing burnout, and fostering PIF during medical school.
Methods
Study Design and Participants
This study employed a prospective, repeated-measures observational design to assess motivation profiles among medical students across a 4-year curriculum. The reporting of this study conforms to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement and the completed checklist is provided as a Supplemental file. 13
The study design was reviewed by the University of North Carolina at Chapel Hill Institutional Review Board (IRB) (#25-0419), which found it to be exempt. Participants included all students enrolled in a single, large medical school in the Southeastern United States between August 2022 and August 2025. Requirement for written informed consent was waived by the University of North Carolina at Chapel Hill IRB, as this survey's inclusion in the standard student surveys was considered part of normal program or curricular assessment for which students consent to participate at the outset of their enrollment in the program. There were no exclusion criteria. Because all students were targeted with the survey, sample size calculations were not completed.
Surveys were administered electronically at 5 standardized timepoints representing key phases of medical training: 0 months (matriculation), 12 months, 18 months (conclusion of foundational science coursework), 30 months (following 12 months of clinical rotations), and 48 months (completion of medical school). Participation was voluntary, and responses were de-identified prior to analysis. The study protocol was reviewed and deemed exempt by the University's Institutional Review Board (#25-0419).
Work Extrinsic and Intrinsic Motivation Scale
Motivation was assessed using the WEIMS, a validated 18-item instrument. 4 The WEIMS was selected as part of an institutional effort to better understand longitudinal motivational patterns across the medical curriculum and to inform curricular reflections. It was modified slightly to relate to medical training as opposed to professional work. For example, “training” was substituted for “work,” where applicable. This linguistic substitution was made to improve face validity for medical students while preserving the theoretical structures of the scale. Each item was rated on a 7-point Likert scale ranging from 1 (does not correspond at all) to 7 (corresponds exactly) for the following statement: “Please indicate to what extent each of the following items corresponds to reasons why you are presently involved in your [training].” Items measure 6 motivational subtypes, which are summarized in Table 1 with their respective items. 12
The 6 Motivational Subtypes, With Their Related Questions on the Work Extrinsic and Intrinsic Motivation Scale.
Analysis of WEIMS includes subscale composites of Work Self-Determined Motivation (W-SDM) and Work Non-Self-Determined Motivation (W-NSDM). Each subscale score was computed as the mean of its three constituent items and required at least 2 valid responses to generate a score. The reliability of subscales was evaluated using Cronbach's alpha. The three composite indices below were adopted from the publication by Tremblay et al.
12
See Table 1 for a description of the terms.
W-SDM = IM + INTEG + IDEN W-NSDM = INTRO + EXT + AMO W-SDI = (3×IM + 2×INTEG + 1×IDEN − 1×INTRO − 2×EXT − 3×AMO)
Higher W-SDI scores reflect greater overall self-determination, whereas lower values indicate predominance of controlled or amotivated regulation.
Data Management and Statistical Analysis
Data were imported from Microsoft Excel into Python (v3.11) for analysis. Descriptive statistics (mean, standard deviation (SD), and percent missing) were computed for each subscale and composite index at all 5 timepoints. Reliability coefficients (Cronbach's alpha) were calculated to assess internal consistency.
To evaluate changes in motivation across the curriculum, 1-way analysis of variance (ANOVA) was conducted separately for each subscale and for the W-SDI composite. Because sample sizes and variances differed across training stages, we used Welch's t-test for pairwise comparisons of mean WEIMS scores. To control for multiple comparisons across subscales and timepoints, we applied the Holm–Bonferroni method.
Results
Participant Responses
A total of 1828 surveys were analyzed. Response rates per timepoint were as follows: matriculation (73.29%), 12 months (53.5%), 18 months (56.84%), 30 months (57.54%), and 48 months (64.74%). An error in the administration of the survey led to the following statement, part of the INTEG scale, not being included in years 2022 through 2024: “Because it is a fundamental part of who I am.” We decided to continue with the analysis despite this error, given that 2 of the 3 constituent INTEG items were still queried. Item-level missingness was low across all other items, with less than 2% missing responses per item.
Internal Consistency
Cronbach's alpha coefficients indicated acceptable internal consistency for most WEIMS subscales. Reliability was highest for Amotivation (α = 0.843) and External Motivation (α = 0.839), followed by Intrinsic Motivation (α = 0.756), Introjected Regulation (α = 0.746) and Integrated Regulation (α = 0.729). Lower, but still moderate, reliability was observed for Identified Regulation (α = 0.521).
Motivational Subscales
Intrinsic Motivation (IM), Integrated Regulation (INTEG), and Identified Regulation (IDEN) demonstrated the highest mean values. By contrast, Introjected (INTRO) and External Regulation (EXT) scores were moderate, and Amotivation (AMO) remained low (Table 2).
Motivation Subscale and Composite Scores by Timepoint Aligned to Months Since Matriculation.

Each individual scale is on a 7-point Likert Scale (N = number, µ = mean, SD = standard deviation).
ANOVA tests indicated statistically significant differences for several domains across training. External Regulation (EXT) increased significantly from matriculation (mean (SD): 3.68 (1.31)) to 18 months (4.20 (1.42), P < .0001), 30 months (4.22 (1.45), P < .0001), and 48 months (4.20 (1.46), P < .0001). Furthermore, there were statistically significant increases in the amotivation subscale noted from matriculation (mean (SD): 1.93 (0.96)) to 18 months (2.25 (1.34), P < .01) and 30 months (2.22 (1.34), P = .012). A statistically significant decrease in mean integrated regulation subscale score was noted from matriculation to 18 months (mean (SD): 5.13 (1.26) vs 4.82 (1.29), P < .01). Other subscales, including introjected and identified regulation scales, remained relatively stable across measured timepoints (P > .05). Mean subscale scores on WEIMS are shown in Figure 1.

WEIMS motivation continuum (means) across timepoints aligned to months since matriculation (* denotes statistical significance with P < .05).
W-SDM and W-NSDM
Overall, W-SDM was significantly higher than W-NSDM at all time points measured (Figure 2). At matriculation (0 months), mean (SD) W-SDM was 5.30 (0.81) compared to 3.2 (0.89) for W-NSDM. This difference remained significant (P < .05) at 12 months (5.2 (0.93) vs 3.2 (0.95)), 18 months (5.1 (0.85) vs 3.4 (1.0)), 30 months (5.1 (0.87) vs 3.4 (1.0)), and 48 months (5.2 (0.87) vs 3.4 (0.98)).

Work Self-Determined Motivation (W-SDM) and Work Non-Self-Determined Motivation (W-NSDM).
Work Self-Determination Index
The composite W-SDI demonstrated a modest but significant overall difference across the 5 timepoints. Post-hoc Welch t-test (Holm-corrected) comparisons revealed that W-SDI scores were significantly higher at matriculation (mean (SD): 15.387 (5.99)) compared to 18 months (12.13 (6.94), P < .0001), 30 months (12.50 (7.16), P < .0001), and 48 months (13.59 (6.89), P < .01) indicating a decline in overall self-determined motivation. Mean W-SDI scores (±95% CI) are plotted across the 5 timepoints of medical training in Figure 3.

Work Self-Determination Index (W-SDI) by months since matriculation (* denotes statistical significance with P < .05).
Discussion
This longitudinal study examined the sources of medical students’ motivation and how it evolved throughout their training using the WEIMS. While the WEIMS was developed for employed workers, medical students occupy a hybrid role that combines structured learning with increasing professional responsibility. Therefore, this study extends prior WEIMS applications to this new population. Findings revealed that overall, W-SDM far outweighed W-NSDM during all phases of medical training. There were small but statistically significant changes in motivational profiles across the curriculum, characterized by an early decline in self-determined motivation during the pre-clinical and early clinical months, followed by a modest rebound near graduation. Months 18-30 represent a particularly challenging transition period, coinciding with the conclusion of foundational science coursework and the first year of full-time clinical rotations. During this phase, students encounter increased workload intensity, frequent high-stakes evaluations, unfamiliar clinical environments, and growing pressure related to residency competitiveness, all of which may constrain perceived autonomy and competence. Although overall motivation remained autonomous, the pattern suggests a shift toward more externally regulated forms as students progress through medical school.
The observed decrease in W-SDI was primarily driven by increases in External Regulation, which may reflect the growing external pressures encountered during medical training. As students advance, their focus may shift from curiosity and learning for its own sake to external demands such as performance evaluations, licensing exams, and residency placement. These extrinsic stressors may undermine perceived autonomy, replacing intrinsic motivation with more controlled forms of regulation. Partial recovery of W-SDI near graduation suggests a re-emergence of autonomous motivation, perhaps as students reconnect their learning to patient care and their professional identities as physicians. Clinical experiences and increasing self-efficacy may help restore a sense of purpose and internalized motivation. 14
These findings underscore the importance of designing curricula that support autonomy, competence, and relatedness throughout all phases of training. During the pre-clinical phase, motivation may be strengthened by increasing perceived relevance of basic science content, incorporating early clinical exposure, and offering more opportunities for self-directed and collaborative learning. 15 In the clinical years, low intrinsic motivation and high amotivation are associated with higher burnout and lower academic performance. 3 Regular assessment of motivational profiles could also serve as an early indicator of disengagement or burnout risk. 16 Integrating brief, evidence-based interventions may help students maintain intrinsic motivation and connect their learning to enduring professional values. 16
Limitations
This study's strengths include its longitudinal design, large data set, repeated WEIMS measurement at 5 distinct timepoints, and use of a validated framework grounded in SDT. However, given that this study was conducted at a single institution with a structured pre-clinical curriculum followed by graded clinical rotations, results should be interpreted considering several limitations. Evaluation practices and academic culture at this institution may influence motivational profiles and findings may differ in settings with alternative grading systems or curricular structures. The set-up of this study precluded individual-level tracking, thus preventing within-person analysis of motivational change, which may be of interest in future studies. Furthermore, participation rates varied across timepoints, potentially introducing response bias. Sample size justifications were not performed a priori given that all students at the university were targeted with the survey. As previously mentioned, one question related to INTEG was inadvertently omitted from the survey, which may have attenuated our ability to fully characterize motivation profiles. While WEIMS captures broad motivational constructs, it does not account for contextual factors such as learning climate, faculty feedback, or assessment stress, which likely influence motivation dynamically. 17 Institutions that employ pass/fail or narrative-based assessment systems may observe different motivational trajectories, as reduced emphasis on comparative grading and ranking could attenuate external regulation and preserve autonomous motivation.
Future Directions
Future research should employ within-subject longitudinal designs to track how individual motivational trajectories evolve and identify predictors of resilience or vulnerability. Qualitative studies, including semi-structured follow-up interviews, could complement these quantitative findings by exploring the underlying “why” behind observed motivational shifts, particularly how students experience external pressures, PIF, and autonomy across training phases. Interventions targeting motivational support, such as curriculum redesign, autonomy-supportive teaching strategies, or peer mentorship programs, could then be evaluated for their impact on self-determination and well-being. In addition, continuing the study to include physicians during and after residency training would provide a broader view of the arc of motivational shifts throughout physicians’ training and careers.
Conclusion
Motivation in medical students is dynamic throughout training. While autonomous motivation dominates throughout medical school, external regulation increases over time. By intentionally designing educational environments that nurture autonomy, competence, and relatedness, medical schools may help students sustain the intrinsic drive that underpins both effective learning and compassionate clinical practice.
Supplemental Material
sj-docx-1-mde-10.1177_23821205261431557 - Supplemental material for Sources and Changes in Medical Student Motivation: A Longitudinal Self-Determination Theory Analysis
Supplemental material, sj-docx-1-mde-10.1177_23821205261431557 for Sources and Changes in Medical Student Motivation: A Longitudinal Self-Determination Theory Analysis by James Jones, Jessica Fuller, Seth Alexander and Christina Shenvi in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-2-mde-10.1177_23821205261431557 - Supplemental material for Sources and Changes in Medical Student Motivation: A Longitudinal Self-Determination Theory Analysis
Supplemental material, sj-pdf-2-mde-10.1177_23821205261431557 for Sources and Changes in Medical Student Motivation: A Longitudinal Self-Determination Theory Analysis by James Jones, Jessica Fuller, Seth Alexander and Christina Shenvi in Journal of Medical Education and Curricular Development
Footnotes
Ethical Considerations/Approval
This study was reviewed by the University of North Carolina at Chapel Hill IRB (#25-0419) and determined to be exempt.
Consent to Participate
Consent to participate was implied upon completion of the survey, a process approved by the University of North Carolina at Chapel Hill IRB. The requirement for written informed consent was waived by the IRB (#25-0419).
Consent to Publish Findings
Consent to publish findings was included as part of the survey delivery, a process approved by the University of North Carolina at Chapel Hill IRB.
Author Contributions
Authors CS and SA planned the study, author JJ performed the statistical analysis and was primary contributor to the manuscript. All authors jointly reviewed the literature and data, and contributed to the manuscript
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Generative AI Statement
Generative AI was not used in the preparation/writing of this manuscript.
Data Availability
Data is available upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.