
Abstract
Objective
This study aimed to investigate the evolution of specialty preferences among medical students at Ahvaz Jundishapur University, Iran, with a focus on identifying key factors influencing career decisions, including lifestyle considerations, migration intentions, and familial influences.
Methods
A mixed-methods approach was employed, combining quantitative surveys and qualitative interviews with 169 medical students at different training stages. Data were analyzed to track changes in specialty preferences before and after clinical exposure, with statistical significance assessed using paired t-tests and thematic analysis for qualitative insights.
Results
Findings revealed a significant shift toward lifestyle-oriented specialties during clinical training, with work schedule priority increasing by 133% (P < .001). Additionally, migration intentions rose by 143% (P = .003), highlighting growing concerns over career prospects in Iran. Despite these shifts, familial influences remained a persistent factor in specialty selection.
Conclusion
Clinical experiences substantially reshape medical students’ career priorities, with lifestyle and migration potential becoming increasingly influential. These findings underscore the need for enhanced career counseling programs and policy reforms to address physician maldistribution and brain drain in Iran's healthcare system.
Introduction
The selection of medical specialties in developing healthcare systems like Iran represents a critical juncture. Here, global professional aspirations intersect with local healthcare realities, creating complex tensions that demand scholarly examination. 1 This longitudinal mixed-methods study investigates the dynamic evolution of specialty preferences among Iranian medical students, framed within the theoretical construct of structural dissonance in medical education—the persistent misalignment between institutional training objectives and individual career decision-making in resource-constrained environments. Previous research across Middle Eastern contexts has identified static determinants such as financial remuneration and familial expectations.2,3 Our study captures the temporal transformation of these priorities through clinical training, particularly within Iran's unique healthcare ecosystem. This ecosystem is characterized by paradoxical demographics (62% female medical students vs 28% female surgical specialists), 4 stark urban-rural disparities (2.4 vs 0.7 physicians per 1000 population), 5 and significant brain drain tendencies (18% annual graduate emigration). 6 By employing a dual methodological approach that quantifies preference shifts while elucidating their experiential drivers, we reveal how clinical exposure fundamentally reshapes career aspirations. These changes challenge conventional medical education paradigms and necessitate culturally-grounded policy interventions to address systemic workforce imbalances (Figure 1). 7

Flowchart of specialty preference evolution during clinical training (n = 169).
Methods
Study Design and Setting
We conducted a longitudinal sequential explanatory mixed-methods study at Ahvaz Jundishapur University of Medical Sciences between September 2021 and June 2022. The study received ethical approval from the Ethics Committee of Ahvaz Jundishapur University of Medical Sciences (IR.AJUMS.REC.1400.123) and all participants provided written informed consent. This study utilized a mixed-methods design, incorporating a cross-sectional observational component. Therefore, its reporting adheres to both the Good Reporting of A Mixed Methods Study (GRAMMS) guideline 8 and the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guideline for cross-sectional studies. 9 The completed STROBE checklists are provided as Supplemental File 1.
Participants
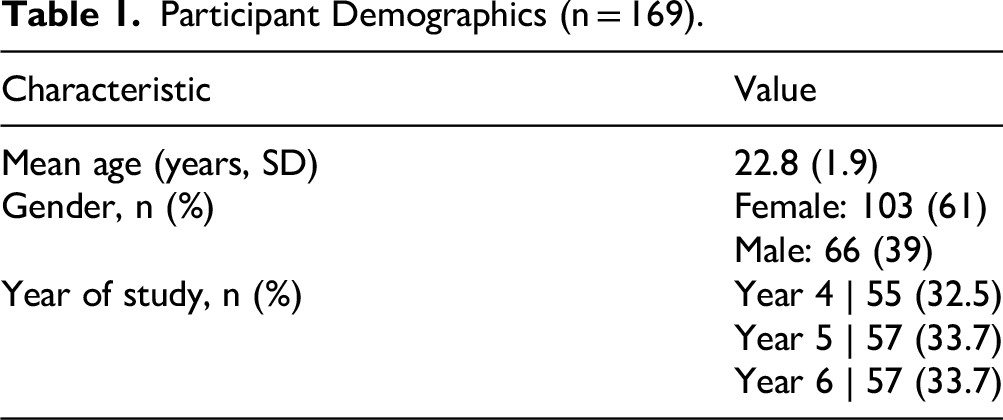
We recruited medical students in years 4–6 of the MD program through convenience sampling. Convenience sampling was used due to accessibility and time constraints in the clinical setting; participants were recruited via class announcements, email invitations, and university online forums to maximize participation. Inclusion criteria required participants to be actively enrolled in clinical rotations and willing to complete both survey and interview components. We excluded students with incomplete questionnaire responses or who withdrew consent during the study. For interviews, purposive sampling was employed to ensure diversity in gender, year of study, and initial specialty preferences, allowing for rich qualitative insights (Table 1).
Participant Demographics (n = 169).
Data Collection
For the quantitative component, we administered the validated Medical Career Decision-Making Questionnaire (MCDMQ, α=0.82) at the beginning and end of core clinical rotations. The MCDMQ was adapted from validated instruments used in similar developing country contexts10,11 and was pilot-tested on 20 students not included in the main study to ensure cultural appropriateness and comprehension. Content validity was confirmed by five medical education experts, with minor revisions made. Factor analysis was not performed due to the adapted nature of the tool, but reliability was high in the pilot (α=0.85). English Version of the Study Questionnaire is provided as Supplemental File 2. The qualitative component involved semi-structured interviews (30-45 min) with purposively selected participants, continuing until thematic saturation was achieved (n = 30). Example interview questions included: “How have your specialty preferences changed since starting clinical rotations?” “What factors, such as lifestyle or family, influence your decisions?” and “How has clinical exposure affected your migration intentions?” No duplicate responses occurred, as unique participant IDs were assigned during data collection.
Missing data were handled by excluding incomplete questionnaires; there were no missing values in the analyzed dataset.
Statistical Analysis
Statistical Analysis
Quantitative data were analyzed using paired t-tests for continuous variables and McNemar's test for categorical changes. We calculated effect sizes using Cohen's d. Qualitative data underwent thematic analysis using Braun and Clarke's framework, with dual independent coding (Krippendorff's α > 0.80) managed in NVivo 12 software. To ensure rigor, codes were developed inductively from initial transcript readings. Thematic saturation was defined as no new themes emerging from three consecutive interviews. Disagreements between coders were resolved through discussion and consultation with a third researcher if needed. Sample size was calculated using G*Power software for paired t-tests, assuming a medium effect size (d = 0.5), alpha=0.05, and power=0.80, yielding a minimum n = 34. We oversampled to 169 to accommodate qualitative components and potential attrition.
Study Design and Setting
Our longitudinal analysis revealed significant transformations in specialty selection priorities, quantitatively captured in Table 2 and qualitatively elaborated below:
Evolution of Specialty Selection Factors (n = 169).

These dramatic percentage changes (eg, + 133% and +143%) highlight the rapid recalibration of priorities triggered by clinical realities, with large effect sizes (Cohen's d > 0.8 for key factors).
Three dominant patterns emerged from the data:
The Lifestyle Priority Surge: Practical considerations like work schedule flexibility underwent the most dramatic transformation, escalating from a secondary concern for 18% of pre-clinical students to a primary decision factor for 42% of clinical trainees (OR = 3.1, P < .001). This shift was particularly acute among students who had completed surgical rotations, where 68% reported the specialty's demanding schedule as “prohibitively stressful” in follow-up interviews. Illustrative quote: “The long hours in surgery made me realize I want a specialty that allows family time” (Female, year 5). The Tertiary Center Migration Effect: Intentions to pursue international training more than doubled during clinical years (14% to 34%, P = .003), with a striking exposure gradient—students rotating through tertiary care centers demonstrated 2.8× higher emigration odds (95% CI 1.7-4.6) than those at community hospitals. Qualitative data revealed this stemmed from: (a) unfavorable comparisons with international standards, and (b) mentorship by foreign-trained faculty. Illustrative quote: “Professors trained abroad showed us better techniques—I now plan to migrate for advanced training” (Male, year 6). Cultural Anchoring of Family Influence: While Western studies show family impact declining by 19–26% during training,
12
Iranian students maintained stable familial consideration (Δ-3%, P = .752). This cultural persistence manifested differently by gender—female students increasingly selected “family-compatible” lifestyle specialties (82% vs male 48%, P < .01), while males more often reported “continuing family medical traditions” (67% vs female 29%). Illustrative quote: “My family wanted a traditional specialty, but I negotiated for one with better balance” (Female, year 4) (Table 3).
Joint Display Integrating Quantitative and Qualitative Findings.

Discussion
This study reveals a fundamental paradox in Iranian medical education. Clinical training—designed to cultivate specialty commitment—instead accelerates preferences for lifestyle-oriented specialties and emigration intentions. This phenomenon is driven by two key mechanisms: selective disillusionment and a training paradox. Selective disillusionment involves waning enthusiasm upon facing practice realities, supported by data (eg, 68% reporting stress in interviews) and literature on socialization in medicine. 13 The training paradox occurs when advanced exposure highlights local deficiencies, fueling migration, as seen in similar Middle Eastern studies. 14
Our findings align with patterns in other developing nations, such as high family influence in Pakistan 2 and gender-based lifestyle shifts in Saudi Arabia, 15 but show more pronounced migration increases, possibly due to Iran's socioeconomic factors. 16
Remarkably, familial influence persists as a stabilizing counterweight, with students employing nuanced negotiation strategies to reconcile personal aspirations with cultural expectations. These include opting for socially approved lifestyle specialties, framing potential migration as temporary skill acquisition, and engaging in generational bargaining to align family expectations with individual goals. These findings suggest that specialty selection should be reconceptualized as an ongoing dialectic between global professional norms and local healthcare imperatives, rather than a static decision point.
The implications for medical education are profound. Current career counseling models appear inadequate in addressing the complex identity work required to navigate these tensions. A multi-tiered intervention framework is needed, combining structural reforms (such as service-linked scholarships and improved working conditions), pedagogical innovations (including critical media literacy and realistic specialty previews), and cultural bridges (such as family engagement programs and mentorship networks). Specifically, family engagement programs could include workshops for parents on specialty impacts on work-life balance. Mentorship programs might pair students with local physicians for ongoing guidance, as implemented in similar Iranian initiatives. 17 Such interventions could help align individual career aspirations with national healthcare needs while mitigating brain drain. 18
However, several limitations must be acknowledged. The single-center design and convenience sampling may limit generalizability, while introducing potential selection bias (eg, more motivated students participating). No formal pre-study sample size calculation was done, relying on post-hoc power, which is a limitation. The adapted questionnaire, though validated, may not fully capture cultural nuances in career decision-making. Additionally, the study's nature (longitudinal within clinical years but not full career follow-up) precludes causal inferences, and the lack of longitudinal follow-up means actual career outcomes remain unknown. The timing of data collection during the COVID-19 pandemic may have also influenced responses, particularly regarding migration intentions. Future research should employ multi-center longitudinal designs, incorporate culturally sensitive measures, and explore intersectional factors shaping specialty choices.
Despite these limitations, the study underscores the need for medical education systems in resource-constrained settings to address the growing tension between individual career aspirations and systemic healthcare demands. By fostering more realistic expectations, creating supportive training environments, and engaging families in career discussions, institutions can better prepare students to navigate the complexities of specialty selection in an era of globalized medical labor markets. Ultimately, this research contributes to broader conversations about physician workforce development, offering insights applicable not only to Iran but to other healthcare systems facing similar challenges of professional identity formation and brain drain.
Conclusion
This study provides compelling evidence that medical students’ specialty preferences undergo significant transformation during clinical training, with important implications for healthcare workforce planning. The findings underscore the need for developmental career counseling that evolves alongside students’ changing priorities. By implementing targeted interventions that acknowledge both global trends and local cultural realities, medical educators can better support students through this critical decision-making process while addressing systemic healthcare needs.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251407764 - Supplemental material for The Dynamics of Medical Specialty Selection Among Iranian Medical Students: A Comprehensive Analysis
Supplemental material, sj-docx-1-mde-10.1177_23821205251407764 for The Dynamics of Medical Specialty Selection Among Iranian Medical Students: A Comprehensive Analysis by Elham Rajaei, Samaneh Yazdi Baghbanzadeh and Mehdi Sayyah in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205251407764 - Supplemental material for The Dynamics of Medical Specialty Selection Among Iranian Medical Students: A Comprehensive Analysis
Supplemental material, sj-docx-2-mde-10.1177_23821205251407764 for The Dynamics of Medical Specialty Selection Among Iranian Medical Students: A Comprehensive Analysis by Elham Rajaei, Samaneh Yazdi Baghbanzadeh and Mehdi Sayyah in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The work was conducted while the corresponding author was a Master's student at the Medical Ethics and History of Medicine Research Center, Tehran University of Medical Sciences, Tehran, Iran.
Ethics Approval
The study was approved by the Ethics Committee of Ahvaz Jundishapur University of Medical Sciences (IR.AJUMS.REC.1400.123).
Informed Consent
Written informed consent was obtained from all participants.
Author Contributions
ER: data collection, analysis, writing—original draft. SY: data collection, writing—review & editing. MS: conceptualization, supervision, writing—review & editing, project administration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.