
Abstract
Background
Given recent advances in artificial intelligence (AI) in medical education and healthcare, it is essential to examine the perceptions and readiness of medical students. As future medical professionals, their ability to utilize this emerging technology effectively is crucial. Therefore, the present study aimed to examine medical AI knowledge, readiness, and perceptions among medical students in medical education and healthcare, and the risks and disadvantages associated with it in Iran.
Methods
This cross-sectional study was conducted among Iranian medical students in 2025. The questionnaire used in this study consisted of three parts: the first part, socio-demographic characteristics; the second part, basic knowledge and students’ perceptions of medical education, healthcare, and risks and disadvantages of medical AI; and the third part, students’ readiness for medical AI. The data were analyzed using SPSS 22 and Excel 2019 software.
Results
Of the total 280 medical students participating in the present study, 55.4% were female, and 60% were in the preclinical phase. The results showed that respondents demonstrated greater AI readiness in the dimensions of vision and ethics and possessed a high level of knowledge regarding the terms “artificial intelligence,” “neural networks,” and “deep learning.” More than 70% of respondents reported a high perception of medical AI in its three dimensions. A significant relationship exists between the medical AI readiness score and gender, working family/close friends, knowledge of AI, and three dimensions of students’ perceptions of medical AI.
Conclusion
Enhancing students’ knowledge, readiness, and understanding of medical AI can equip professionals with improved medical and decision-making skills. These professionals can make more informed decisions and reduce medical errors with AI tools.
Introduction
Artificial intelligence (AI) is a broad field of computer science that focuses on creating intelligent machines capable of performing activities typically requiring human intelligence. 1 These capabilities enable machines to simulate human cognitive processes and perform tasks that rely on human intelligence. 2 In the 1950s, Marvin Minsky and John McCarthy officially introduced the concept of AI at Dartmouth College in Hanover, New Hampshire, United States. Since then, rapid advancements in AI technology have led to widespread adoption and integration across various industries, transforming problem-solving and decision-making practices. 3 Edward Shortliffe, at Stanford University, developed one of the first AI systems in clinical settings in the early 1970s to aid in identifying blood infections and recommending related treatments. 4
AI in the healthcare sector has garnered significant attention in recent years due to its ability to enhance the delivery of medical services. 5 Incorporating AI into the medical education curriculum can significantly transform teaching and learning methods and educational outcomes. In the future, this may lead to more accurate and precise clinical decision-making. 6 In addition, using AI tools in medical education can provide students with personalized and adaptive learning opportunities.7,8
Research on the use of AI in healthcare is rapidly increasing worldwide, with potential applications in healthcare services, including physical and mental health, such as drug discovery, virtual clinical consultations, disease diagnosis, forecasting, medication management, and health monitoring. 9 With the increasing amounts of data in various medical fields, AI is expected to transform the medical landscape in multiple aspects of clinical care, from patient diagnosis and treatment 10 and biomedical research. Quantum computing in AI holds strong potential to revolutionize healthcare, particularly in disease prediction and personalized therapies. It can thus break down time and space constraints, saving more lives, especially in underserved and less developed areas. 11 Given the vital role of AI in the healthcare sector, it is essential that health education also benefits from advancements in this field. 12 AI holds immense potential for improving treatment planning, disease diagnosis, and patient care.
According to reviews of most previous studies, knowledge, attitude, perception, and readiness regarding medical AI were examined using different tools and questions, especially in perception. For example, in several studies, only the perception of using AI in healthcare was investigated.14,24 In contrast, in the Hammoudi Halat et al’s survey, the readiness and perception of students in education and healthcare were examined. 18 Additionally, a study by Ziapour et al conducted in Iran investigated only students’ readiness. 25 Additionally, in previous studies, it has been shown that although medical students have a positive attitude toward the use of medical AI, they lack sufficient knowledge, awareness, and skills,13,14 and a comprehensive understanding of its computational principles and limitations. 15 Given the advantages of using medical AI and integrating AI into the medical education curriculum, conducting surveys to assess students’ attitudes and perceptions regarding AI content appears essential. 16 By assessing medical students’ readiness, knowledge, and perceptions regarding AI in healthcare, we can take a critical step toward preparing the future workforce to fully harness the potential of AI technologies, thereby enabling the effective integration of AI that ultimately supports patient care and healthcare delivery. Therefore, the present study assessed the level of medical AI knowledge, readiness, and perceptions among medical students in medical education, healthcare, and the risks and disadvantages associated with it at Zahedan University of Medical Sciences in 2025.
Methods
Data Collection
This cross-sectional study was conducted from February to April 2025 on 280 medical students of Zahedan University of Medical Sciences at the clinical and nonclinical levels. Data were collected using online and paper questionnaires. Online questionnaires were sent to clinical students, particularly via social networks, and paper questionnaires were distributed and explained to students on campus. At the beginning of both questionnaire formats, the purpose and necessity of the research, as well as the confidentiality and voluntary nature of participant participation, were explained. Inclusion required participants to be medical students. Students were excluded if they did not respond to the questionnaire. Written informed consent was obtained before the study commenced. Due to time, cost concerns, and participant preference, the ethics committee used and approved oral explanations. The study's purpose was fully explained. Participants were informed that they could leave without incurring any negative consequences. Data confidentiality and security were assured. The questionnaire also stated that it was anonymous and all responses would be kept confidential.
Study Population
From a total of 1333 medical students in medical sciences, the sample size was determined using Cochran’s formula
Questionnaire Information
The self-constructed questionnaire used in this study consists of three parts. The first part is sociodemographic characteristics such as gender, age, study phase (preclinical/clinical), and sources of information on AI (yes/no); the second part is knowledge and perception (a 5-point Likert scale with scores ranging from strongly disagree = 1 to strongly agree = 5 for each question) and it should be mentioned that perception was assessed in three sections: the use of AI in medical education, healthcare, and its potential risks and hazards. The third part assesses readiness for AI; respondents filled out the Medical Artificial Intelligence Readiness Scale for Medical Students (MAIRS-MS). Questionnaire The Persian Readiness Assessment (MAIRS-MS) version consists of four domains: cognition (8 questions), ability (8 questions), vision (3 questions), and ethics (3 questions). A 5-point Likert scale is used for each question, with scores ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). Rezazadeh et al (2023) previously translated and validated the MAIRS-MS in Persian. The scale demonstrated good reliability (Cronbach's alpha = .94) and content validity (content validity index (CVI) = .92, content validity ratio (CVR) = .75). Confirmatory factor analysis supported the hypothesized factor structure. 17
After conducting a thorough literature review, the research team created the initial draft of the questionnaire, focusing on the knowledge and perception section. The questions in this section were designed based on a review of previous studies that examined students’ knowledge and perceptions of medical AI.14,18,19 Next, a panel with eight experts, including two health education specialists, two library science specialists, two health information technology specialists, an epidemiologist, and a psychologist, evaluated the content validity of the questionnaire. Then, the preliminary version of the questionnaire was prepared. Examine the CVI and CVR. In the CVI assessment, item clarity, simplicity, and relevance were measured (acceptable CVIs > .7, Lawshe). 20 CVRs examined the essentiality of items for the specified factors (CVRs > .75 are acceptable, according to Waltz and Bausell). 21 This study’s CVI and Scale CVR were .81 and .85, respectively.
To ensure face validity, 25 medical students who were not involved in the study evaluated the initial draft of the questionnaire. The research team asked for feedback on the questionnaire's clarity and incorporated relevant suggestions into the final version. The reliability of the questionnaire scale was evaluated using internal consistency and test-retest methods. Internal consistency, assessed by Cronbach's alpha in 30 students, was considered satisfactory for alpha values of .70 and above. 22 A questionnaire was administered to students (n = 30) twice, at a two-week interval, to assess test-retest reliability using intraclass correlation coefficients (ICCs). The ICC values demonstrated excellent stability (ICC = 0.9; 95% CI = (0.89 to 0.92)).
Statistical Analysis
Statistical analysis was performed using SPSS 22 and Excel 19 software. Quantitative results were reported as mean ± standard deviation (SD) or frequency (percentage). An Independent Sample t-test is used to see if there is a difference in scores across different subgroups of variables associated with readiness, knowledge, and perceptions. A univariate linear regression analysis was used to investigate the association between student readiness and each sociodemographic characteristic, as well as student perception scores and knowledge. In univariate regression, variables with a probability of less than .2 will be included in multiple linear regression. The significance level in this study will be considered 5%.
The reporting of this study conforms to the STROBE Statement—Checklist of items that should be included in reports of cross-sectional studies (see Supplemental File STROBE Checklist).
Results
A total of 280 people participated in this study. The average age of the respondents was 21.61 ± 2.45 years. 155 (55.4%) were female, and 170 (60.7%) were in the preclinical phase. 249 (89%) of respondents through social media, 255 (91.1%) through friends knew AI, and 22% of medical students had taken AI courses at university. Details are provided in Table 1.
Sociodemographic Characteristics of Respondents (n = 280).

The results of this study show that respondents’ scores were relatively lower in the cognitive and ability domains compared to the vision and ethics domains in MAIRS-MS. In the perception of AI, the average scores for perception in health education were lower than for perception in healthcare, as well as the risks and disadvantages. More details are presented in Table 2.
Mean Readiness, Knowledge, and Perception Scores of Respondents Toward Medical AI.

Table 3 and Figure 1 show the respondents’ knowledge of AI. Most participants reported having a high level of knowledge regarding the terms “artificial intelligence,” “neural networks,” and “deep learning.”

Chart of the respondents’ knowledge of AI.
Respondents’ knowledge of AI.

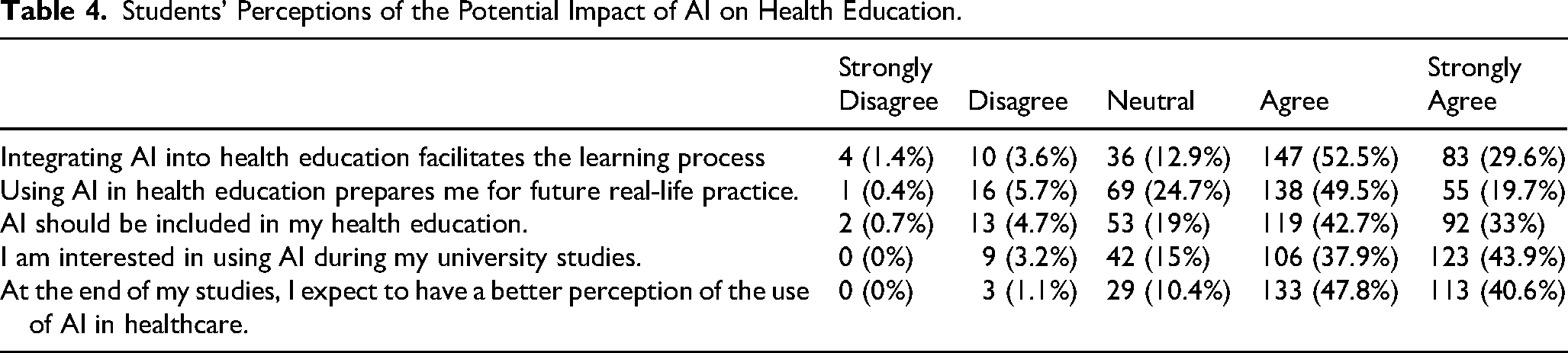
In examining students’ perceptions of the potential impact of AI on medical education, the majority of respondents agreed with the items asked, with the most agreement related to the items “At the end of my studies, I expect to have a better perception of the use of AI in healthcare” and “The integration of AI into health education facilitates the learning process.” More details are provided in Table 4 and Figure 2.

Chart of the students’ perceptions of the potential impact of artificial intelligence on health education.
Students' Perceptions of the Potential Impact of AI on Health Education.
In examining students’ perceptions of the potential impact of medical AI on healthcare, most respondents agreed with all the items asked, with the lowest agreement related to items such as “AI increases patient trust in healthcare” and “AI reduces healthcare.” Details are provided in Table 5 and Figure 3.
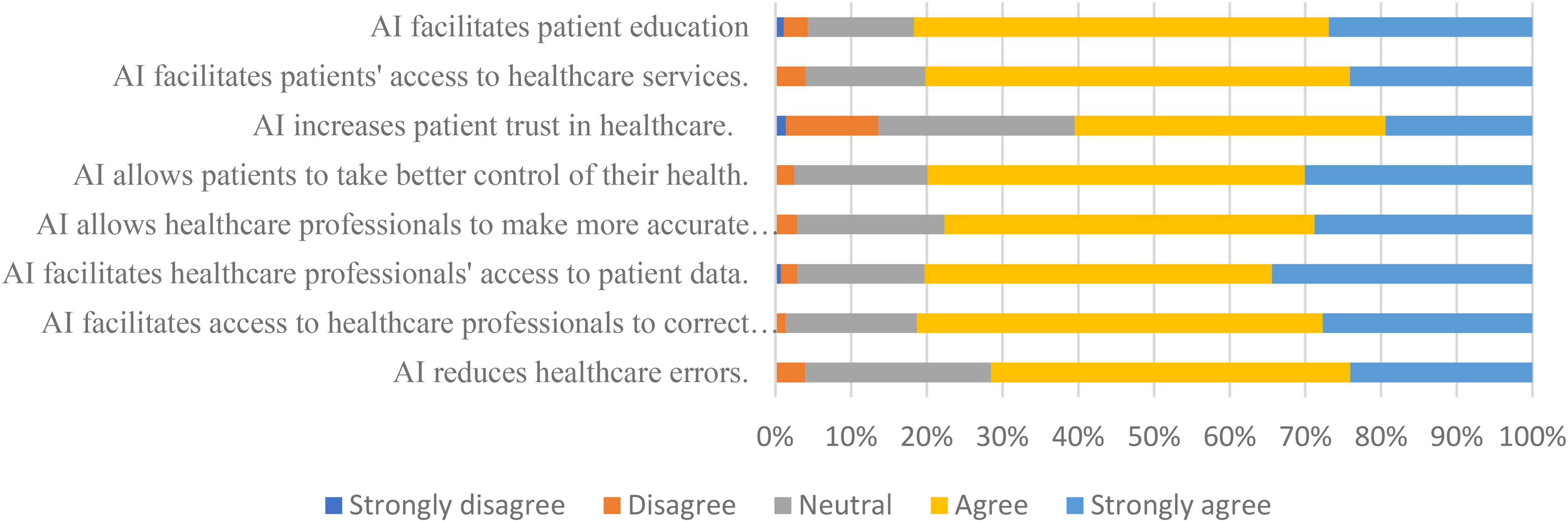
Chart of the students’ perceptions of the potential impact of artificial intelligence in healthcare.
Students’ Perceptions of the Potential Impact of Medical AI in Healthcare.

Table 5 and Figure 3 show students’ perceptions of the potential impact of AI in healthcare.
More than half of the students, respectively, agreed with the “In the future, some healthcare professions may be replaced by AI,” “It diminishes the human aspect of the medical profession,” and “AI in medicine brings new medical errors and ethical challenges.” More details are provided in Table 6 and Figure 4.
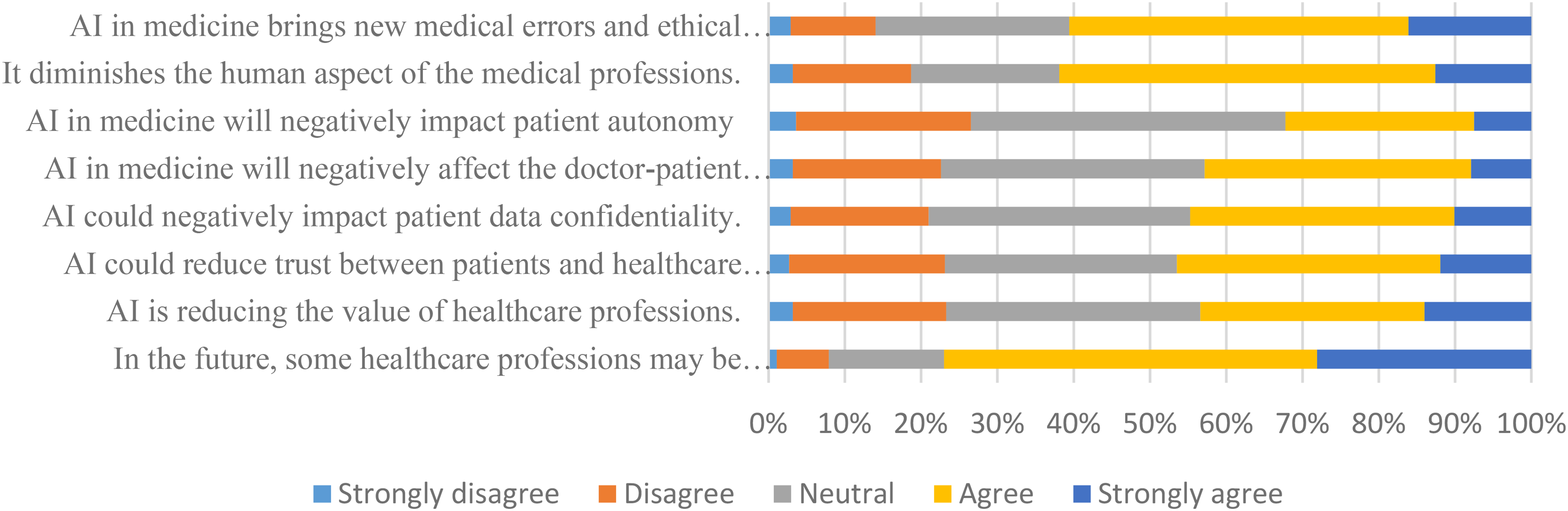
Chart of the students’ perceptions of the possible risks and disadvantages of artificial intelligence.
Students’ perceptions of the possible risks/disadvantages of medical AI.

Table 7 shows factors associated with respondents’ readiness for AI. In the domains of cognitive ability and vision, the average score of men was significantly higher. Having family or close friends in AI had a significant impact on cognitive ability, vision, and ethics. Knowing about AI from social media had a significant impact on the dimensions of ability, ethics, and knowledge about AI compared to television. Taking AI courses at the university had a significant impact on the cognitive dimension.
Factors Associated with Respondents’ Readiness Toward Medical AI (t-Test Analysis).

*Sig. < .05.
In the domain perception of AI in healthcare, men's average score was significantly higher. Preclinical participants scored higher in AI knowledge and Risk Perception. Working family or close friends in AI significantly impacts knowledge and perception in health education AI. Knowing AI from friends significantly affected the Perception of AI in health education. Knowing about AI through social media significantly impacted knowledge and perception of AI in health education and healthcare. Knowing about AI from television had a significant impact on the dimensions of AI knowledge and perception of the potential disadvantages and risks associated with medical AI. Taking courses at the university, however, significantly improved knowledge of AI. Details are provided in Table 8.
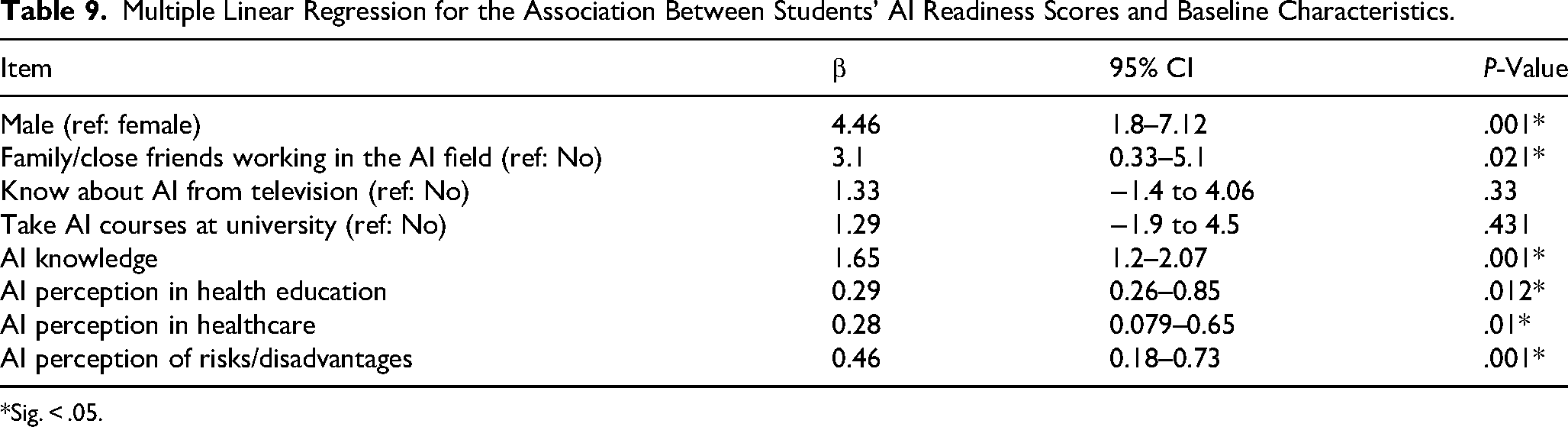
Multiple Linear Regression for the Association Between Students‘ AI Readiness Scores and Baseline Characteristics.

*Sig. < .05.
To examine the correlation between Sociodemographic characteristics, knowledge, and perception toward medical AI and scores of readiness, we initially used univariate linear regression analysis. There was a strong positive correlation between scores of medical AI readiness in the male gender (P = .001), as the AI readiness score was higher in men than in women.
Knowledge, perception of risks/disadvantages (P = .001), health education, and healthcare regarding medical AI (P = .006) have a direct correlation with the AI readiness score, so that, with the increased knowledge and perception of the risks and disadvantages of health education and healthcare related to medical AI, the AI readiness score improves.
Knowledge of AI from television (P = .043) and taking AI courses at university (P = .016) are directly related to the AI readiness score. Thus, acquiring knowledge about AI from TV and university enhances the AI readiness score. The overall model was statistically significant and explained 58% of the variability in readiness scores (R2 = .58%, P < .001). This indicates that independent variables explain 58% of the variance in AI readiness scores. Moreover, the R2 effect size is 1.38, indicating a large effect. Details are provided in Table 9.
Multiple Linear Regression for the Association Between Students’ AI Readiness Scores and Baseline Characteristics.
*Sig. < .05.
Discussion
Participants’ AI Knowledge
The results indicated that most participants reported having a high level of knowledge regarding the terms “AI,” “neural networks,” and “deep learning.” In contrast, their understanding of “algorithm” and “machine learning” was relatively limited. Previous studies have shown that medical students possess a high level of knowledge regarding the term “AI,” it has been demonstrated that medical students reported basic knowledge of medical AI.14,18,23 Given that medical students likely have a limited understanding of complex concepts such as algorithms and machine learning, and considering the importance of using advanced technologies like AI in healthcare, it seems necessary to design and implement appropriate and structured educational interventions to improve the knowledge and skills of future physicians through various platforms, especially the medical curriculum.
Participants’ AI Readiness
The overall readiness score toward AI among the respondents was reported as 74 out of 110, and the respondents’ readiness was assessed in four dimensions, with the highest level of readiness related to ethics and vision. In the study by Lugito et al and Tung and Dong, the overall readiness score for AI in medicine among students was 73 and 67, respectively.14,24 Previous studies reported the highest level of student readiness for medical AI in the dimensions of ethics and vision.14,18,24–26 In the present study, students scored highest in the ethics dimension, which is significant considering the ethical challenges that the use of AI in healthcare can pose, as well as the lack of consistent ethical and legal regulations governing the use of AI in healthcare, and highlights the high readiness of medical students to adhere to moral norms when using this technology. 27 Moreover, the participants exhibit a high level of vision, which refers to the students’ readiness regarding the capabilities, limitations, opportunities, and threats of AI and indicates the readiness of medical students to optimally leverage the capabilities of medical AI while being mindful of its limitations and the associated threats to its use in healthcare. It should be noted that due to the potential capabilities of using medical AI in education and health care, the Ministry of Health of Iran has recently held programs in the form of webinars and online workshops at the level of medical universities in an integrated manner to improve the knowledge and skills of faculty members and medical students. In addition, medical universities at the domestic level are required to hold AI workshops for students, which can significantly impact the readiness of Iranian students to use medical AI in line with developed countries.
Participants’ AI Perception
In the present study, medical students’ perceptions regarding AI were evaluated in three dimensions: health education, healthcare, and potential risks and disadvantages. In terms of students’ perception of the impact of AI on health education, more than 70% of students agreed or strongly agreed with all items. The most excellent agreement was related to the question, “At the end of my studies, I expect to have a better perception of the use of AI in healthcare,” which indicates the students’ high perception of the importance of AI education to utilize the high potential of this technology in healthcare. In previous studies, students also positively perceived AI training in health education.18,19 Despite the importance of AI education, especially in the medical field, the lack of AI training as part of the educational curriculum is felt in Iran and most countries.19,28,29 When teaching AI through the medical curriculum, all aspects of the application of medical AI, including its limitations and potential risks, should be considered scientifically, and optimistic and superficial information should be avoided. 28 On the other hand, given that AI focuses on existing phenomena and data and lacks the necessary capacity to address the context, process, or development of applications in the real environment, AI education should be considered beyond technical education and should focus on recognizing the philosophical and ethical foundations of using AI, and especially the application of critical thinking for the responsible and thoughtful implementation of AI, in particular. In sensitive health care situations, it is vital to make safe and ethical decisions that are impartial, justified, and reasonable. 30
The results showed that more than 70% of medical students’ perceptions were in agreement with all items of AI in health care, including patient education, access to health care, patient control of their health, accurate decisions, access to patient data, correction of medical information, and reduction of errors, except “increases patient trust in healthcare.” In the study by Lugito et al, medical students also demonstrated confidence in the ability of AI to assist in performing healthcare tasks such as diagnostic imaging, disease prediction, and documentation. 14 In the study by Hammoudi Halat et al, dental students found that AI would benefit by providing accurate health information, facilitating precise decision-making, and reducing medical errors. This finding is consistent with the present study. 18 In the study by Nong and Plat, the results also showed that most patients had little trust in the responsible use of AI tools. 31 The use of advances in AI, such as quantum computing, requires a strong understanding of these capabilities by medical professionals to be able to effectively translate into tailored care plans and timely implementation, in addition to acquiring the necessary skills to manage and coordinate with these advanced technologies, and to ensure that the safety and quality of patient care continue to be a priority. 32 Therefore, training healthcare professionals and increasing public awareness of this new technology seems necessary to improve health outcomes and make appropriate health decisions. Subsequently, these capabilities will increase patients’ trust in physicians and medical centers that utilize AI tools to diagnose, treat, and monitor their conditions.
In the section on students’ perception of the potential risks and disadvantages of medical AI, results showed that Iranian medical students have concerns about the risks of using AI in healthcare, particularly regarding the replacement of healthcare professionals, diminishing the human aspect of the medical profession, and bringing new medical errors and ethical challenges. Previous studies have also reported these concerns about AI's potential risks and disadvantages.18,33,34 In a study, Al Hadithy et al showed that medical students were hesitant about the ability of AI to replace or surpass healthcare workers. 23 Although the integration of AI in healthcare is receiving significant attention, concerns about risks, potential biases, and the ethical and legal considerations of AI cannot be ignored.33,35 On the one hand, the limitations of AI in providing emotional support and empathy should be considered. For example, in the field of psychiatry, consulting requires human interaction. Thus, it cannot replace humans but can support healthcare providers.36,37 In addition, using AI systems to make predictions or decisions without critical thinking can cause serious problems for the community's well-being and patient safety. 38 Therefore, paying special attention to the promotion of critical thinking skills along with teaching the use of medical AI tools in the educational curriculum can significantly improve the biases and potential risks of using AI, such as human errors, trust, and the doctor–patient relationship, and the human aspect of the medical profession.
Factors Associated with Respondents’ Readiness, Knowledge, and Perception Toward Medical AI
The present study's findings revealed a significant relationship between gender and readiness and perception of AI use in healthcare, and male students had a higher mean score in the domains of cognitive, vision, ability, and perception of AI in healthcare. In a study conducted on Iranian students, contrary to the results of the present study, the results showed that female students had higher readiness for AI. 25 In the study by Lugito et al, the findings indicated that male students had higher readiness in the domains of cognition, ability, and vision. 14 The study by Sarwar et al also showed that male respondents showed greater trust and readiness to use medical AI. 39 Given the rapid introduction of AI into health education and healthcare, male students participating in the present study were likely to have a greater desire and interest in this technology.
The present study's findings showed a positive and significant relationship between taking an AI training course and medical students’ cognitive domain and knowledge. The survey by Boillat et al showed that medical students who had completed AI training reported a statistically higher level of familiarity with medical AI. 40 Previous studies have shown that students with prior training in coding and programming can develop a deeper understanding and a broader vision of complex concepts like AI.14,23 Considering that it is possible to change the educational curriculum by 20% in Iranian universities of medical sciences, it is suggested that in some fundamental and clinical courses, such as surgery, gynecology, radiology, etc, topics related to the use of medical AI tools should be included in teaching-learning. The optimal implementation of this process, prerequisites such as the development of technological infrastructures, the empowerment of basic and clinical science professors, and the design of valid and reliable educational content should be on the agenda, should be placed. Regarding the technological infrastructure in some countries, such as Iran, there may be some restrictions on the part of AI tool providers and policymakers, which is essential due to the importance of open access to information, providing access to AI tools for all medical professionals in healthcare in all countries, regardless of political issues.
Medical students whose family or close friends work in AI scored highly in all four readiness domains. They also reported higher knowledge and perception of medical AI, similar to the results of Lugito et al's study. 14 Exposing students to peers and family who work with AI can provide an opportunity for deep learning and improving individuals’ knowledge in AI in a friendly and informal setting. 26 It can affect people’s readiness and perception of the optimal use of this technology in their educational and professional paths.
In examining the sources of medical AI information, students who used social media and television reported more readiness in ability/ethics and cognitive, respectively, and reported higher knowledge of AI. In addition, obtaining information from relatives has increased the perception of healthcare. The use of social media has also increased the perception of medical education and healthcare. Furthermore, television has increased the perception of the disadvantages and risks associated with AI. The results showed that acquiring AI information from various contexts, especially social media, can affect students’ readiness, knowledge, and perception. In the study by Logito et al, the results also showed that medical students exposed to AI through friends, television, and internet blogs had higher AI readiness in cognitive, and higher AI knowledge. 14 Due to the level of awareness, knowledge and skills of medical students in the field of AI and inadequate formal training on the one hand, and the existence of advertising, news and false information in the media and the Internet on the other hand, medical schools and universities should play a more active role in empowering medical students to detect false information and educate this emerging technology to ensure that doctors use medical AI appropriately.
The findings of this study revealed a significant relationship between students’ study phase and their knowledge and perception of the risks and disadvantages associated with medical AI. Preclinical students had higher knowledge and a more positive perception. This may be because preclinical students do not face the same pressure and stress of working in a clinical setting, allowing them to spend more time in a university setting, where they have more opportunities to learn about AI through various platforms, such as in-person and online workshops, social media, and interactions with friends and peers. Additionally, they may be encouraged to utilize AI tools to complete educational assignments. Contrary to the results of this study, Lugito et al found that clinical students had higher knowledge and perception of medical AI, which could be attributed to their increased exposure to AI technology in hospitals. 14 Paranjape et al recommend that medical AI training can occur at several stages. Before starting medical school, mathematical concepts related to AI should be taught. In the preclinical stage, students should familiarize themselves with the basic concepts, ethical and legal aspects of using medical AI, and the introduction of clinical AI tools and advanced concepts should continue in the clinical stage. 41
The present study’s findings revealed a strong positive statistical relationship between medical AI readiness and the perception of AI use in education and healthcare. These results indicate that students who had a positive perception of using medical AI in education and healthcare were more prepared to accept AI, consistent with the results of Hammoudi Halat et al 18 In addition, the findings showed a strong relationship between students’ perceptions of potential risks and disadvantages of medical AI and their readiness. Previous studies have also reported concerns about medical AI's disadvantages and ethical aspects.14,19,40 In an editorial, Park et al discussed the transformation of nursing practices with AI, emphasizing training in the ethical use of AI and bias detection. It is also important to note that although AI-based tools such as CDSS make good suggestions for complex scenarios, nurses need to combine AI insights with their clinical expertise and ethical judgment to get better results, which not only highlights the need to teach AI tools but also to use critical thinking among healthcare professionals. 32 Integrating AI ethics education into the medical curriculum 19 Providing well-structured regulations and laws with an in-depth understanding of the potential risks, disadvantages, and ethical aspects of using medical AI can increase readiness and reduce concerns among medical professionals regarding the use of AI. In addition, AI can be highly effective in medical education and healthcare. The optimal use of AI can act as a tool to enhance the capabilities of healthcare providers and reduce human errors, thereby promoting professional and clinical skills rather than replacing medical professionals.
Based on the results of past studies and the conduct of this research, firstly, workshop sessions were held for professors and students to familiarize them with different areas of AI. Then, according to the instructions of the Deputy Director of Education, some AI-related topics were placed in related courses, allowing changes to 20% of approved educational programs (curriculum). And in some cases, optional courses were included in the approved curriculum. Then, a committee was formed at the universities consisting of seven subgroups: AI, simulation, blockchain, mobile learning, metaverse, empowering and training people related to AI, and the Specialized Committee for Developing Standards for Accreditation of Smart Education and Evaluation of Educational Technologies.
Conclusion
Overall, the use of AI in education is increasing. These conditions require fundamental actions, and these actions will serve as a model that can be applied and used everywhere with minor changes for two reasons: Generation Z students worldwide have similar tastes and interests. In addition, social networks have facilitated communication between people. Therefore, several approaches are suggested: firstly, empowering students and professors, changing curriculum and educational programs, creating specialized committees, and involving policymakers to implement planned action.
Limitation
Our first limitation was that our access to clinical students was limited due to our presence in hospitals. Questionnaires were designed online and shared with these students through social media to address this limitation. The second limitation of the present study is that the data were collected through self-reporting, and the participants’ statements, particularly regarding their knowledge and readiness to use medical AI, may be influenced by selective memory and exaggeration, which could differ from their actual abilities and skills in using AI tools in a clinical setting. Therefore, a practical assessment of the knowledge and readiness of Iranian medical students in medical AI is recommended to confirm the present study's findings. The third limitation of the study is that exploratory and confirmatory factor analysis were conducted for the MARIS questionnaire in the survey by Karaca et al. 42 However, it is suggested that the self-made questionnaire be examined as a separate study.
Supplemental Material
sj-docx-2-mde-10.1177_23821205251407758 - Supplemental material for Knowledge, Readiness, and Perception of Medical Students Toward Medical Artificial Intelligence: A Cross-Sectional Study
Supplemental material, sj-docx-2-mde-10.1177_23821205251407758 for Knowledge, Readiness, and Perception of Medical Students Toward Medical Artificial Intelligence: A Cross-Sectional Study by Zahra Arab-Borzu, Leila Keikha and Azita Shahraki-Mohammadi in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205251407758 - Supplemental material for Knowledge, Readiness, and Perception of Medical Students Toward Medical Artificial Intelligence: A Cross-Sectional Study
Supplemental material, sj-docx-3-mde-10.1177_23821205251407758 for Knowledge, Readiness, and Perception of Medical Students Toward Medical Artificial Intelligence: A Cross-Sectional Study by Zahra Arab-Borzu, Leila Keikha and Azita Shahraki-Mohammadi in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-4-mde-10.1177_23821205251407758 - Supplemental material for Knowledge, Readiness, and Perception of Medical Students Toward Medical Artificial Intelligence: A Cross-Sectional Study
Supplemental material, sj-docx-4-mde-10.1177_23821205251407758 for Knowledge, Readiness, and Perception of Medical Students Toward Medical Artificial Intelligence: A Cross-Sectional Study by Zahra Arab-Borzu, Leila Keikha and Azita Shahraki-Mohammadi in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The research team sincerely thanks all Zahedan University of Medical Sciences medical students for participating in this study.
Ethical Approval and Consent to Participate
The Zahedan University of Medical Sciences ethically approved this study with the ethics code IR.ZAUMS.REC.1403.440. The respondents in this study gave their consent to participate
Author Contributions
Conceptualizing the study: ASH. Writing—original draft: ASH and AAB. Writing—review and editing: ASH and LK. Methodology/formal analysis: AAB. Project administration: ASH. All authors reviewed the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
Data are provided within the manuscript or supplementary information files.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.