
Abstract
BACKGROUND
Artificial intelligence (AI) application is increasingly used in all fields, especially, in medicine. However, for the successful incorporation of AI-driven tools into medicine, healthcare professional should be equipped with the necessary knowledge. From that, we aimed to assess the AI readiness among medical students in Jordan.
METHODS
A cross-sectional survey was conducted among medical students across 6 Jordanian universities. Prevalidated Medical Artificial Intelligence Readiness Scale for Medical Students questionnaire was used. The questionnaire was distributed through social media groups of students. SPSS v.27 was used for analysis.
RESULTS
A total of 858 responses were collected. The mean AI readiness score was 64.2%. Students scored more in the ability domain with a mean of 22.57. We found that academic performance (Grade point average) positively associated with overall AI readiness (P = .023), and prior exposure to AI through formal education or experience significantly enhances readiness (P = .009). In contrast, AI readiness levels did not significantly vary across different medical schools in Jordan. Notably, most students (84%) did not receive a formal education about AI from their schools.
CONCLUSION
Incorporation of AI education in medical curricula is crucial to close knowledge gaps and ensure that students are prepared for the use of AI in their future career. Our findings highlight the importance of preparing students to engage with AI technologies, and to be equipped with the necessary knowledge about its aspect.
Introduction
Artificial intelligence (AI) is an interdisciplinary field specialized in the creation of intelligent machines. 1 These machines are capable of problem solving and learning through a lot of methods, including machine learning, neural networks, and natural language processing. 2 It is promising that AI will refine the human decisions and improve overall effectiveness in countless areas. 3
As in the field of medicine, AI often referred to as Artificial Intelligence in Medicine, has revealed its potential, it can classify medical images such as x-rays 3 and offer capabilities for prognosis,4,5 treatment planning,6,7 patient monitoring, 8 and more. A number of AI applications were found to improve different aspects of clinical practices, such as improving medication compliance 9 and reducing outpatient clinic waiting time. 10
However, the application of AI in medicine did not come without challenges. First, there was refusal among physicians is a repeating theme,11,12 even though some studies report an optimistic view. 13 Medical students, too, were found to express concerns about AI incorporation, including time constraint, curriculum, and job prospects.14,15
To be prepared for the incorporation of AI in the medical field, medical students must have a foundational understanding of AI's developing role within medicine. 16 Artificial intelligence readiness in healthcare is explained as the knowledge, attitudes, and skills that prepare healthcare professionals to use AI in their clinical practices and lead to recognizing the principles of AI and any ethical and medicolegal consideration. 17 It is not equal to AI basic knowledge or literacy, although AI literacy with confidence and understanding can have an effect on AI readiness. 18 As AI readiness means the preparedness to adopt and use AI technologies, in this instance, medical practice, whereas knowledge means the level of understanding AI and how it works and its theoretical principals, while attitudes mean personal feelings and beliefs. 19
As for the warning of the World Health Organization that healthcare professionals need to understand how AI operates, 20 it is increasingly likely that AI applications will get hold of a lot of roles and introduce new tasks in medical care. Therefore, medical students and physicians must acquire the base knowledge and skills to navigate this transformative era successfully.
Only a handful of studies have assessed the healthcare personnel's readiness for AI. In Malaysia, they found that around two-thirds of the participants had an average readiness toward AI and scored between 53 and 83 (67.62%).
In contrast, in another study using the same scale in Saudi Arabia, it was reported that the majority of participants were not ready to embrace AI technologies in their careers. 21 A study conducted in Oman revealed that physicians expressed no significant concerns about the impact of AI on their employability. Instead, they demonstrated readiness to embrace AI in their medical practices if it were integrated into international guidelines. 22
In contrast to studies in other countries, Jordanian medical students exhibit unique characteristics that may influence their AI readiness. Jordan's youthful demographic, with a significant proportion of its population under the age of 30, fosters a higher adaptability to new technologies. 23 The country's educational system, renowned for its robust medical and technological education, emphasizes innovative curricula and methods distinct from other countries. 24 Finally, Jordan's significant investment in enhancing digital infrastructure has further supported the integration of advanced technologies in education. 25 These factors collectively underscore the distinctive context of Jordanian medical students in terms of AI readiness.
Numerous studies worldwide, including those in Jordan, have examined healthcare professionals and medical students’ knowledge and attitudes toward AI. However, very few have investigated AI readiness among medical students. Therefore, do Jordanian medical students have sufficient readiness toward AI tools? As for recently, there are no data or studies conducted in Jordan tackling this subject. Moreover, we do not have enough data and research in Jordan conducted to tackle this problem. This cross-sectional study aims to fill this gap through assessing and evaluating the readiness of Jordanian medical students for AI integration in medical education and practice. The results of this study will help the universities to update their curriculum to suit this developing time, guide policymakers to adapt to the introduction of AI in medicine and provide valuable insights into the readiness level of Jordanian students about AI.
Methods
Study Design
This cross-sectional study surveyed male and female medical students studying at the faculty of medicine at 6 different Jordanian Universities in Jordan. The reporting of this study conforms to the STROBE for cross-sectional statement 26 (Supplemental 1). The curriculum of the faculty of medicine in Jordan follows a 6-year program, the first 3 years represent the preclinical phase and focus mainly on basic sciences. Then, students move to the last 3 clinical years, where they attend lectures, clinical rounds, and tutorials, as well as some surgical procedures.
Participants
For this study, we targeted medical students from years 1 through 6, the study was conducted among 6 universities (the University of Jordan, Al-Balqa Applied University, Hashemite University, and Jordan University of Science and Technology, Mut’ah University, Yarmouk University). We selected medical students from clinical and preclinical phases to ensure a comprehensive representation of different stages in medical education. This range allows us to assess AI readiness across varying levels of exposure to medical training and AI technologies. The universities were chosen based on their representation of major medical schools in Jordan and the 6 chosen universities are all universities that teach medicine in Jordan, ensuring diversity in the student population and the curricula offered. All medical students from the above universities were eligible to participate in the study. According to the Ministry of Higher Education and Unified Research, the number of medical students in Jordan is approximately 20 000 students. Consequently, The sample size was determined using the mathematical equation Z 1-α/2 2P (1-P)/d2, allowing for type I errors at a 5% level of significance (P < .05) and 95% confidence interval, with an expected proportion of 50%. To achieve the study's objective and in order to have sufficient power, a sample size of 385 participants was targeted.
Study Tool
To assess AI readiness, this study used a prevalidated questionnaire that consisted of 29 questions, divided into 2 sections. The first section focused on collecting demographic information, including, inquiries about participants’ age, gender, university, current medical year, awareness of AI usage (yes/no), prior experience with AI in the medical field (yes/no), and Grade point average (GPA), which is going to be self-reported by students.
The remaining 22 questions were drawn from the Medical Artificial Intelligence Readiness Scale for Medical Students questionnaire (MAIRS-MS) 17 which was proven to be valid and reliable.21,27 This questionnaire will be used because it can apply to all medical students around the world. The MAIRS-MS questionnaire is designed to assess students’ readiness and capability to embrace AI across 4 distinct domains: cognition (8 questions), ability (8 questions), vision (3 questions), and ethics (3 questions), each question with a maximum score of 5 and a minimum of 1. The questionnaires will use a 5-point Likert scale, which provides 5 response options, including strongly agree, agree, neutral, disagree and strongly disagree.
Data Collection and Ethical Considerations
The collection of data took place from November 17, 2023, till first, March 2024 using an online Google form, which was distributed among students using different social media platforms. Participation was voluntary, and all answers were self-reported. Participants had the flexibility to answer the form during their free time. At any point, participants had the option to withdraw from the study without any obligations or consequences.
Ethical approval was obtained for the institutional review board at the University of Jordan (IRB) with decision number (111/2023). Before answering the survey, explicit written informed consent was obtained from each participant via the Google form, which included a clear explanation of the purpose of the study, the procedures, the potential risks and benefits, and the assurance that there are anonymity and data confidentiality. The survey was blinded. No identifying information (ID no., emails, names, etc) was collected to ensure the anonymity of the participants. Only the research team had access to the collected data.
Data Analysis
The IBM Statistical Package for Social Sciences (SPSS) version 27.0 (IBM Corporation), and the IBM Analysis of a Moment Structures version 24 were used for analyzing the study data.
Normality assumptions were evaluated, and then descriptive and inferential methods were used to describe students’ AI readiness. The scores of each domain of AI readiness (cognition, ability, vision, ethics) were calculated following a prescribed formula 17 and were represented as means and standard deviations (SDs). Analysis of variance and independent sample t test were used to compare continuous variables among different students according to their demographic variables, any necessary post hoc test was conducted. Continuous variables were presented as mean ± SDs, while categorical variables were presented as frequencies (per cent). In this study, P-values less than or equal to .05 were considered statistically significant.
Results
Reliability
The level of internal consistency for the items of MAIRS-MS was measured using the Cronbach α coefficient, which was 0.966 for AI readiness as a whole, 0.909 for the cognition domain, 0.931 for the ability domain, 0.892 for the vision domain, and 0.909 for the ethics domain. As a Cronbach α coefficient value of >0.7 was considered a desirable reliability estimate, these results indicated a good internal consistency for the tested domains. 28
Regarding assessing data normality, our sample size was larger than 300 individuals. Consequently, Kolmogorov-Smirnov and Shapiro-Wilk's tests might be unreliable. So, both the skew and kurtosis could be analyzed by descriptive statistics. The acceptable values for skewness and kurtosis fell between −3 to +3, and −10 to +10, respectively, when structural equation modeling was introduced. 29 In our study, the skew and kurtosis were less than the absolute value of one for all the domains and the overall scale. Therefore, these results indicated that the data distribution was normal.
Demographics
A total of 858 medical students participated in this study. Table 1 shows a clear demonstration of the sociodemographic characteristics of participants. Participants were classified according to their age into 4 groups, with a mean of 21.01 years old.
Demographic data of medical students among Jordanian universities.
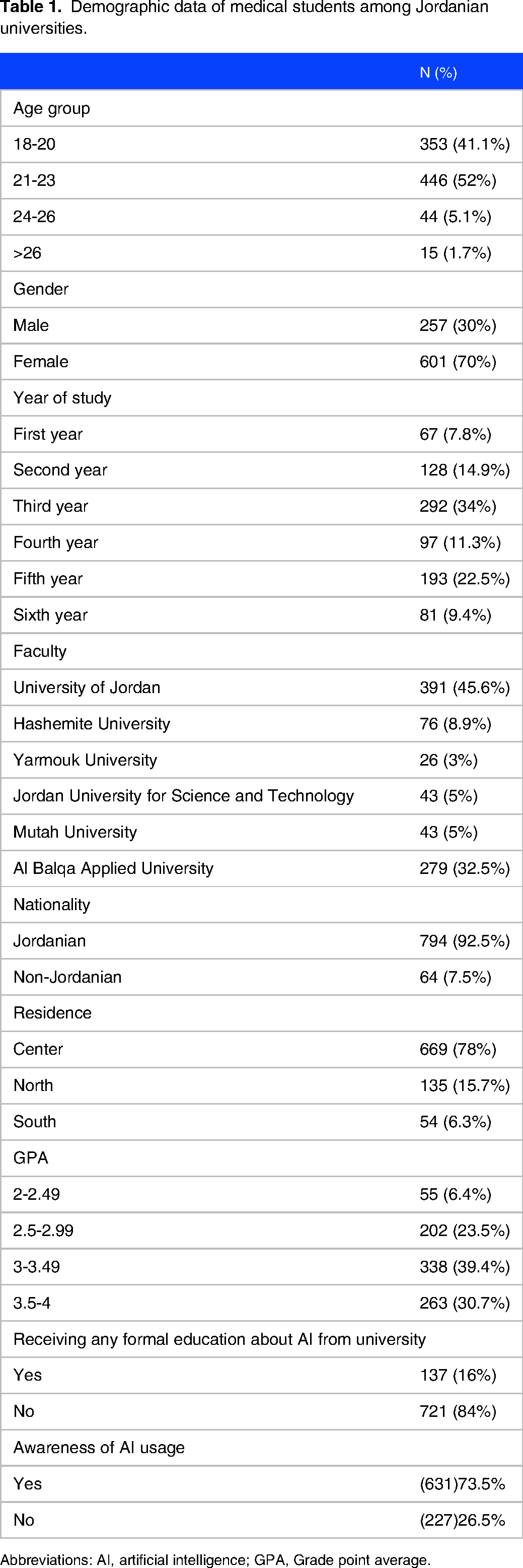
Abbreviations: AI, artificial intelligence; GPA, Grade point average.
Among the participants, 601 (70%) were females. When evaluating the years of study among participated, 487 (56%) of the total participants were in their basic years of study, whereas the rest 371 (44%) were in their clinical years.
The greatest proportion of participants were from the University of Jordan 391 (45.6%), followed by Al-Balqa Applied University 279 (32.5%), Hashemite University 76(8.9%), and lastly Yarmouk University 26 (3%). More than 90% of participants were Jordanian, 64 (7.5%) were from other nationalities. The majority (78%) are residents in the center of Jordan. Grade point average of medical students was also assessed, 39.4% had a GPA between (3-3.49).
From the table, it is clear that 73% (631) are aware of the use of AI in the medical field, whereas 26.5% (227) are still unaware. Moreover, the majority of participants (84%) did not receive any formal education about AI in the medical field.
Artificial Intelligence Readiness
Table 2 presented the different domains of AI readiness among medical students in different domains. The ability domain had the highest mean 23.38 (SD: 7.16), followed by the cognitive domain (mean: 22.57, SD: 6.67), ethics (mean: 9.29, SD: 3.06), and vision domains (mean: 9.02, SD: 2.99), respectively. Furthermore, the mean score of AI readiness was 64.26 out of 110.
Subscale of AI readiness among medical students.

Abbreviations: AI, artificial intelligence; SD, standard deviation.
Factors Affecting AI Readiness
Table 3 reveals the association between the demographic characteristics of participants, the previous AI experience and training, and the AI readiness among medical students in Jordan.
The association between sociodemographic characteristics, previous AI experience, and AI readiness.

Abbreviations: AI, artificial intelligence; GPA, Grade point average; SD, standard deviation.
It is clearly demonstrated that the GPA is significantly associated with cognition (P = .020), vision (P = .009), and AI readiness overall (P = .023). As students with higher GPAs tend to score more in these domains. Also, receiving formal education about AI from a university is also associated with higher ethics domain (P = .009). Furthermore, having any prior experience (training, course) with AI in medicine is clearly associated with cognition (P = .002), ability (P = .024), and overall AI readiness (P = .027).
Discussion
This study aimed to assess AI readiness among medical students in Jordan and its associated factors. Our sample size was big enough to reach sufficient power as we collected 858 and added trustworthiness to our findings, as we collected double the target sample size, which is 385. Previous studies in different countries and universities focused on knowledge and attitudes without assessing AI readiness specifically. These studies revealed low levels of AI knowledge among medical doctors and students, particularly in the Middle East.30,31
We found that students who performed well academically tended to be far better in understanding AI concepts and ethical considerations. Interestingly, those who had prior exposure to AI, either through formal education or practical experience, showed higher levels of readiness across the board. However, it was noted that readiness levels did not vary much between different medical schools in Jordan.
Our findings showed that students with higher GPA are significantly associated with higher cognition, ethics, ability, vision, and overall medical AI preparation, indicating a relationship between academic achievement and preparedness in these areas. Furthermore, participants with prior experience in AI in medicine exhibited significantly higher scores across all evaluated domains, indicating the significance of practical exposure in enhancing readiness among students. Our study showed that there was a significant association between previous training and medical AI readiness, in a previous study, similar findings were observed, in which Students who received previous training in AI demonstrated higher readiness levels and were more eager to involve AI technology in medical practice. Additionally, they were more likely to identify the limitations, advantages, and disadvantages of AI and its role in healthcare. 27 Moreover, it was shown that receiving formal teaching of AI in university greatly improves students’ readiness. However, no significant difference in readiness was observed across medical schools in Jordan, different age groups or study years.
The results of this study are consistent with previous research, which has demonstrated a positive relationship between academic achievement and preparedness for cognitive tasks linked to AI as well as ethical issues. This alignment underscores the importance of interactions with AI for students’ academic success to not only have technological literacy but also by ethical grounding. Through recognizing and enhancing these connections, educational institutions can better prepare students for a future where proficiency in AI is increasingly intertwined with academic achievement. 32
Additionally, our results are consistent with studies confirming the importance of practical experience in AI applications for healthcare professionals. A survey was carried out among members of the European Society of Radiology to assess the present hands-on clinical familiarity of radiologists with AI-driven tools, the practical experience mentioned in the study refers to direct engagement with AI technologies in real-world healthcare environments. This hands-on experience enables healthcare professionals to gain insights and skills necessary for effectively utilizing AI tools in clinical practice. Practitioners can learn how to understand AI-generated insights, incorporate them into decision-making, and refine patient care processes by interacting directly with AI systems. This first-hand experience is vital for ensuring the successful implementation and employment of AI solutions in healthcare settings. 33
According to a prior Malaysian study on undergraduate medical students’ preparedness for AI, it was found that age and study year significantly correlated with the ability, vision, and ethics domains of medical AI readiness. Furthermore, compared to our study in Jordan, Malaysian students’ overall mean score for AI preparedness was noticeably higher. This might be a result of Malaysia having a higher standard of formal education as well as more medical students participating in AI learning campaigns and courses. 27 However, in Saudi Arabia, the readiness was lower, possibly reflecting differences in educational emphasis and exposure. These findings underscore the importance of tailored AI education strategies to understand global trends in AI readiness among medical students and to take into consideration the difference between educational levels and cultural backgrounds. 21
The findings of our study, which revealed no appreciable variations in AI readiness among study years, different universities, and age groups, could have been caused by a number of things, including the homogeneity of curricula in educational institutions. Also, there may be a shared expectation across different study years to stay updated with emerging technologies like AI. This requirement could lead to similar levels of AI readiness across age groups. Furthermore, self-directed learning opportunities and integration of AI concepts into medicine strengthen students’ understanding of AI regardless of their study year, contributing to the overall consistency in AI knowledge among medical students. Alternative explanations for the observed patterns and relationships could include individual differences in learning styles and variations in educational backgrounds. It is necessary to conduct additional research to fully understand these findings.
This study found that gender was not a significant factor in determining AI readiness, consistent with previous studies on elementary students in China and medical students in Malaysia,18,27 which showed no gender differences in AI readiness and knowledge. This suggests that if both genders receive equal education and exposure to AI concepts, they will show similar readiness levels. To address this, educational interventions must focus on providing a uniform AI curriculum and equal opportunities for practical experience while also addressing confidence gaps to ensure that all students, regardless of gender, are adequately prepared for AI integration in medicine. However, previous research conducted in Germany on undergraduate medical students has shown that males tended to be more confident about the impact of technology and AI on radiology and medicine. Also, they expressed more interest in AI being part of medical training and teaching. 34
The integration of AI into various medical fields has gained significant attention due to its potential to enhance diagnostic accuracy, optimize treatment plans, and revolutionize the educational landscape. As a result, assessing AI readiness among medical students is crucial as AI is becoming an integral part of modern healthcare. In Jordan, where there is a significant investment in digital infrastructure and a youthful population adept at new technologies, understanding AI readiness among medical students helps in preparing future medical professionals to use AI in enhancing patient care. This assessment also provides insights into how medical education can evolve to incorporate AI, ensuring that graduates are well prepared to utilize AI tools efficiently in their practice.35–37
To adequately rise the level of AI readiness among Jordanian medical students, it is necessary to integrate AI education into medical curricula among all universities. According to Keng Siau's earlier research, “Artificial Intelligence Impacts on Higher Education,” it is crucial to include AI in curricula in a variety of fields, including medicine. According to recommendations from earlier research, 21 this would entail offering specific courses and modules addressing AI's essential components and its applications in medicine. Additionally, drawing from successful approaches in other regions, we suggest hands-on training sessions, workshops, and collaborations with AI experts to provide practical exposure. 38 Also, it is essential to introduce AI fundamentals in the education system as early as possible as it was shown in our study that having prior formal teaching and experience in AI (training, course) is strongly associated with a higher level of AI readiness. This is extremely important because our study showed that the majority of participants (84%) did not receive any formal teaching about AI in the medical field. However, 73% of students are aware of the use of AI in the medical field, and they develop positive attitudes toward learning more about this field. On the other hand, conducting educational programs for university students is critical to raise awareness about the positive and negative impacts of AI to avoid its harmful effects and blind use. These actions would provide future medical professionals with the required knowledge to effectively utilize AI technologies in their practice.
The need for longitudinal studies was brought out in another Saudi Arabian study, highlighting the importance of tracking the long-term impact of medical AI readiness levels. 21 In terms of future research, these longitudinal studies must address the effect of AI readiness among medical students on improving the healthcare system and the quality of education. Additionally, research needs to look into various approaches for giving medical students a sufficient foundation in AI and monitoring their progress toward AI readiness during the course of medical school. In addition, investigating other cultural and socioeconomic factors that affect students’ AI medical readiness is essential for a comprehensive understanding of the issue. Therefore, qualitative analysis through interviews could complement quantitative findings, providing an understanding of the factors influencing students’ readiness toward AI.
There were some limitations in the current study. These include the unproportional distribution of participants from different regions of Jordan, the use of a self-reported questionnaire, and the use of convenience sampling to collect data. These limitations may have influenced the study findings by potentially introducing biases and limiting the generalizability of the results.
In contrast, this is the first study to measure AI readiness among medical students in Jordan comprehensively addressing all regions inside the country. Furthermore, by studying factors such as academic performance, prior experience in AI and, we can better understand what helps students become more prepared and engaged in this field. Also, the study calls for more research to track how students’ AI readiness changes over time. Overall, this research contributes to making sure that future doctors are prepared to integrate technology and AI in their medical practice for better outcomes. In addition, the results of this study will help universities and schools to update their curriculum to suit this developing time of increasing demand for integrating AI in the medical field and guide policymakers to adapt to the introduction of AI in medicine.
Conclusion
In our study, we evaluated how prepared medical students in Jordan are for the world of AI and what factors shape this readiness. Our results revealed that the majority of participants did not receive formal AI teaching in the medical field. However, most of them are aware of the use of AI in the medical field and they develop positive attitudes toward learning more about integrating AI in medicine. It became evident that the inclusion of AI education in medical curricula is essential for filling in knowledge gaps and guaranteeing that every student is suitably equipped for the future of medicine. Additionally, higher academic performance and prior exposure to AI were significantly associated with greater AI readiness levels. Although gender appeared to have minimal impact on preparedness, ongoing monitoring of how students’ preparedness develops and the examination of cultural and economic factors affecting their AI outlook is needed. This study underscores the importance of preparing future healthcare professionals to engage AI technologies in the medical teaching process for the benefit of patient care.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241281648 - Supplemental material for Artificial Intelligence Readiness Among Jordanian Medical Students: Using Medical Artificial Intelligence Readiness Scale For Medical Students (MAIRS-MS)
Supplemental material, sj-docx-1-mde-10.1177_23821205241281648 for Artificial Intelligence Readiness Among Jordanian Medical Students: Using Medical Artificial Intelligence Readiness Scale For Medical Students (MAIRS-MS) by Mohammad Hamad, Fares Qtaishat, Enjood Mhairat and Ahmad AL-Qunbar, Maha Jaradat, Abdullah Mousa, Baha'eddin Faidi, Sireen Alkhaldi in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
Special thanks to our collaborator Shahd Aktham Etoom. Thanks to Ghada Sami Alzyadat and Wisam Al Safadi or helping in collecting data for the study and for all the students who participated in the study.
Authors’ Note
Ethics: This study was done according to the ethical guidelines in the University of Jordan. And was approved by the Institutional review board at the University. Consent: Written informed consent was obtained from participants prior to completing the form.
Author Contributions
MH: conceptualization, study design, writing, data analysis, project management, and reference management. FQ: writing, data collection, project management, and literature search. EM: writing, data collection, and tables figure creation. AAQ: writing, data collection, and interpretation of results. MJ: writing, data collection, and instrument building. AM: writing, data collection. BF: writing, data collection. SA: editing and critical revision, supervision of the project.
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.