
Abstract
Objective
We developed a curriculum map of the neurology residency program's academic half-day (AHD) at our institution from 2018 to 2024 to assess topic coverage and identify gaps relative to board certification content.
Methods
We cataloged 280 unique AHD lectures over 6 years, recording attributes including title, date, duration, speaker, and subspecialty. These were compared against the American Board of Psychiatry and Neurology (ABPN) certification blueprint using chi-square analysis.
Results
The 280 lectures totaled 358.5 h. We found significant differences across multiple subspecialties. Content categorized as “Questions not associated with a specific neurologic disorder” (4.93%) was overrepresented (P < .05), while topics on metabolic disorders (0.26%), psychiatric disorders (0%), and autonomic nervous system disorders (0%) were underrepresented (P < .05).
Conclusions
Curriculum mapping revealed both strengths and gaps in the current didactic content, underscoring the need for more comprehensive and aligned curricular material. This process offers a data-driven framework for iterative curricular improvement and may serve as a replicable model for other neurology residency programs. Future efforts will focus on building a 2-year curriculum that aligns more closely with ABPN content specifications while considering institutional strengths and resources.
Keywords
Introduction
Curriculum mapping is a systematic educational tool that outlines what is taught (the academic content), how it is taught (teaching methods and resources), when it is taught (the timetable or sequence), and how these elements align with established educational standards and objectives. 1 By visually organizing curricular content, educators can better understand the connections between instructional activities and desired learning outcomes. 2 At a glance, a curriculum map provides a high-level overview of content distribution and progression. Importantly, the curriculum mapping process integrates data collection on the content that is actually delivered and assessed, helping to identify redundancies, gaps, or misalignments. Ensuring alignment between didactic instruction and educational standards brings coherence and intentionality to the learning experience, ultimately strengthening the effectiveness of curricular planning and helping academic programs meet their educational objectives. 3
In the setting of medical education, curriculum mapping has emerged as a valuable tool for improving curricular organization and topic coverage. While more prevalent in undergraduate medical education,2,4 curriculum mapping has been applied to graduate medical education (GME) programs for specialties such as internal medicine. 5 However, there is limited literature on its use in neurology residency programs. Neurology residency training must strike a balance between broad clinical exposure and structured educational content that prepares residents for board certification and clinical practice. As the field of neurology continues to expand in both breadth and complexity and individual residency programs maintain significant autonomy in designing and delivering formal instruction for their trainees, didactic curricula must adapt to reflect these shifts.
Across adult neurology residency programs in the United States, there is substantial variability in how didactic teaching is structured. 6 Many programs employ a daily/noon conference (NC) model, in which brief teaching sessions are held during lunchtime. Others have adopted the academic half-day (AHD) model, which dedicates a half-day each week for protected learning sessions. Supplementary formats such as case-based morning reports and professor's rounds are also common. Despite the varied formats, instruction remains largely lecture-based, and often assembled by program directors, chief residents, or faculty educators.
While this diversity in didactic curricula allows for flexibility and innovation, it also highlights a lack of content standardization. It may be unclear whether the topics covered align with the content domains emphasized in national benchmarks such as the American Board of Psychiatry and Neurology (ABPN) Initial Certification Examination 7 and Residency In-service Training Examination (RITE). 8 In this context, curriculum mapping offers a promising strategy to align neurology residency curricula with national standards, enhancing the clarity, consistency, and impact of educational programming across neurology training programs.
Here, we describe our application of curriculum mapping to the neurology residency program didactic curriculum at our institution based on data from 6 academic years. We examined the breadth and depth of topics covered and compared this distribution with neurology certification content specifications to determine whether the curricula of the prior years adequately represented the diverse aspects of neurology training. Our work offers a replicable evidence-based approach to aligning didactic education with certification standards and real-world practice needs.
Methods
Setting
The UCLA Neurology Residency Program is a 3-year training program comprising postgraduate year (PGY)-2, PGY-3, and PGY-4 residents. A core component of the program's formal curriculum is the AHD, a structured, longitudinal teaching activity that occurs weekly throughout the academic year.
AHD sessions were held every Wednesday morning from 9:00 a.m. to 1:00 p.m. PGY-2 residents had protected educational time to attend these sessions in full. PGY-3 and PGY-4 residents not assigned to inpatient services were also expected to attend. Each AHD session consisted of a didactic lecture delivered by a dedicated faculty member with specialized expertise in a particular area of neurology, with occasional sessions led by fellows or senior residents. Many faculty lecturers returned annually to deliver their sessions, contributing to the continuity and thematic consistency of the curriculum. Some topics were presented only once, while others were included in multiple academic years. The AHD format was established prior to 2018, but consistent digital records of lecture titles and speakers were only available from 2018 onward, which defined the time frame for this study.
Curriculum Map Development
The curriculum mapping process began by establishing clear goals and identifying the necessary data fields to ensure accurate and complete representation of the residency curriculum. This study was conducted between February 2024 and June 2025, with data analysis completed in March 2025. Didactic curriculum data from 6 academic years (2018-2024) was retroactively collected and included information about lecture titles, dates, duration, speakers, and years covered. This data was compiled into a centralized spreadsheet for ease of access and analysis.
The structure and formatting of the curriculum map were guided by the steps outlined in the AAMC Guidebook to Building a Curriculum Map, 9 which provided a systematic framework for organizing and mapping curricular elements. These steps are illustrated in Figure 1.

To ensure alignment with national standards for board certification, we selected the ABPN Certification Exam Content Blueprint as the primary framework for mapping lecture topics. This blueprint outlines the expected distribution of content areas for board certification and serves as a widely accepted benchmark in neurology education. 7
The curriculum data was organized primarily by subspecialty themes, then further classified according to the ABPN Dimension 1 categories from the Neurology Certification Exam Content Blueprint. 7 Lectures were assigned to one primary ABPN Dimension 1 category based on the title of the lecture and its best fit within a clinical domain as listed in the blueprint. Since detailed information about the specific content and learning objectives of each lecture was limited, we confined the curriculum mapping process to ABPN Dimension 1 categories, which focus on clinical content areas. Dimension 2, which covers Physician Competencies and Mechanisms (eg, diagnostic procedures, systems-based practice, and treatment and management), was not included in the analysis, as it was not feasible to accurately assign lectures to these categories without more granular information on detailed lecture content. Lectures with broad, nonclinical content were excluded from the analysis as they did not clearly fit within a specific clinical domain.
Lectures were also mapped to the RITE Content Blueprint, 8 which uses the same classification system as the ABPN, with the exception that autonomic nervous system disorders is not included as a standalone category in the RITE blueprint.
Total hours spent per ABPN category were calculated by identifying the duration of each individual lecture and multiplying it by the number of academic years in which the lecture appeared in the curriculum. For example, if a lecture lasted 1.5 h and was delivered in 2 different years, it was counted as contributing 3 total hours to the topic's cumulative representation. This approach allowed us to account for recurring lectures and quantify the total instructional time dedicated to each topic across 6 academic years (2018-2024). The resulting distributions were then compared to the ABPN Neurology Certification Exam Content Blueprint recommendations to assess alignment between curricular emphasis and board expectations.
A sample excerpt of the curriculum map structure used for analysis is captured in Figure 2. The curriculum map was organized to allow easy analysis of subspecialty coverage, lecture frequency, and total instructional hours over time, enabling data-driven curriculum review and continuous improvement.

This study involved a comprehensive curriculum mapping of medical education lectures delivered between 2018 and 2024. A total of 280 unique lectures were analyzed, encompassing a wide range of topics and speakers across multiple academic years. Each lecture was treated as a unit of analysis for the purposes of mapping content, themes, and instructional methods. As this study did not involve hypothesis testing or statistical inference, a formal sample size calculation was not applicable. Instead, the study aimed to include the full set of available lectures within the defined time frame, representing the entire curriculum delivered during this period.
Lecture Topic Categories
Lectures were assigned to one primary ABPN Dimension 1 category based on the ABPN Neurology Certification Exam Content Blueprint. Categories included: Headache and Pain Disorders; Epilepsy and Episodic Disorders; Sleep Disorders; Genetics and Developmental Disorders; Vascular Neurology; Neuromuscular Diseases; Movement Disorders; Demyelinating Diseases; Neuroinfectious Diseases; Brain and Spinal Trauma and Spinal Diseases; Neuro-ophthalmologic and Neuro-otologic Disorders; Metabolic, Nutritional, Toxic, and Physical Agent-Related Disorders; Neuro-oncologic Disorders; Behavioral Neurology and Neurocognitive Disorders; Neuroimmunologic and Paraneoplastic CNS Disorders; Autonomic Nervous System Disorders; Psychiatric Disorders; and content not associated with a specific neurologic disorder.
Statistical Analysis
We used a chi-square goodness-of-fit test to evaluate whether the observed distribution of lecture topics across ABPN Dimension 1 categories significantly differed from the proportions recommended in the ABPN Neurology Certification Examination Content Blueprint. The expected frequencies for each category were calculated by multiplying the total instructional hours across all categories by the corresponding recommended percentage from the ABPN blueprint.
For each ABPN category, we compared the observed total instructional hours (aggregated across all academic years) with the expected hours derived from the ABPN blueprint proportions. The ABPN provides a recommended range of percentages for each subspecialty theme on the certification exam blueprint; to facilitate comparison, we calculated the average of each recommended range and used this value as the expected proportion for our analysis.
In addition to the global chi-square test, we conducted individual z-tests for proportions to compare observed and expected proportions for each subspecialty category. Given the number of comparisons (24 categories), we applied a false discovery rate (FDR) correction using the Benjamini–Hochberg procedure to adjust for multiple comparisons. We also calculated effect sizes, defined as the difference between the observed and expected proportions (Obs – Exp), along with 95% confidence intervals to quantify the magnitude and precision of the differences.
Categories with observed hours significantly higher or lower than expected were interpreted as areas of curricular overrepresentation or underrepresentation, respectively. We conducted separate analyses excluding categories not present in the RITE blueprint (eg, autonomic nervous system disorders) for comparison. Categories with zero lectures were retained in the analysis to preserve the overall distribution.
Statistical significance was defined as P < .05. All analyses were performed using SAS 9.4 (Cary, NC).
Reporting Standards
The reporting of this curriculum mapping study conforms to the SQUIRE-EDU guidelines for quality improvement reporting in education. 10 A completed SQUIRE-EDU checklist is included as a supplementary file (see Supplemental File 1).
Ethics Approval
This curriculum mapping project was conducted as part of a quality improvement initiative and did not involve human subjects research, patient data, or identifiable personal information and was therefore exempt from IRB review under UCLA policy. According to UCLA OHRPP guidance, IRB review is not required for activities that do not meet the federal definition of research involving human subjects.
Results
Curriculum Content Overview
From 2018 to 2024, a total of 280 unique lectures were delivered (total 358.5 h of instruction), covering a broad range of neurology subspecialties. A side-by-side comparison of the percentage of total lecture hours dedicated to each subspecialty theme with ABPN recommendations is shown in Table 1. Analysis of the lecture distribution revealed that the majority of AHD content was concentrated in five major subspecialty areas: Movement Disorders (16.6%) Epilepsy and Episodic Disorders (13.0%), Vascular Neurology (11.5%), Neuromuscular Diseases (10.6%), Headache and Pain Disorders (8.8%). These five topics alone accounted for over 60% of total didactic time, reflecting strong emphasis on foundational clinical areas commonly encountered in both residency training and board certification. Several other subspecialties were also represented, though to a lesser degree. The overall distribution of instructional hours by subspecialty is visualized in Figure 3.

This table displays the percentage of total lecture hours dedicated to each ABPN subspecialty theme in the UCLA neurology residency didactic curriculum compared to the corresponding recommended percentages outlined by the ABPN Neurology Certification Exam Content Blueprint. The ABPN provides recommended percentage ranges for each content area; the average of each range was used as the comparison benchmark in this analysis. This side-by-side comparison highlights areas of alignment as well as under- or overrepresentation within the curriculum.
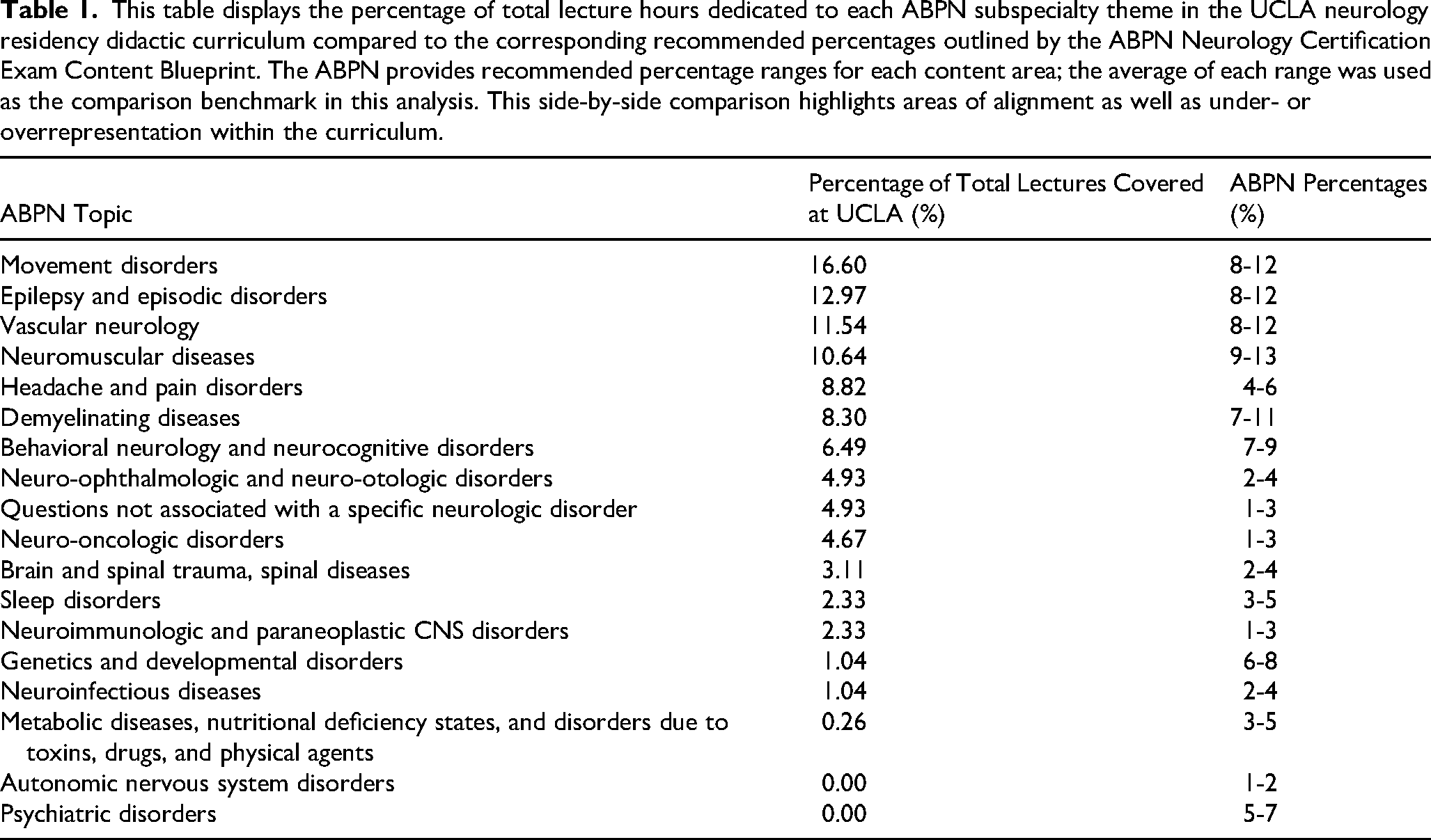
Other content areas were notably underrepresented or entirely absent: Metabolic, Nutritional, Toxic, and Physical Agent-Related Disorders (0.3%), Autonomic Nervous System Disorders (0.0%), Psychiatric Disorders (0.0%).
Statistical Significance
Chi-square goodness-of-fit testing was used to compare the overall distribution of total instructional hours by ABPN content category against the expected distribution based on the ABPN Neurology Certification Examination Content Blueprint. The global chi-square test demonstrated a significant difference between the observed and expected curricular distributions (P < .05), indicating overall misalignment with the ABPN blueprint.
To further identify which subspecialties contributed to this misalignment, we conducted individual z-tests for proportions comparing observed and expected lecture hours across 24 ABPN categories. An FDR correction using the Benjamini–Hochberg procedure was then applied to adjust for multiple comparisons. After adjustment, only the “Questions Not Associated with a Specific Neurologic Disorder” category remained statistically significant.
Instructional content within this category (eg, “Brainstem Anatomy,” “Spine and Spinal Cord Imaging”) accounted for 4.93% of total hours compared with 2% expected (P < .05, FDR-adjusted), reflecting a meaningful overrepresentation. In contrast, three categories—Autonomic Nervous System Disorders (0% vs. 1.5%, P < .05), Metabolic, Nutritional, Toxic, and Physical Agent-Related Disorders (0.26% vs. 4%, P < .05), and Psychiatric Disorders (0% vs. 6%, P < .05)—showed relative underrepresentation, though these differences were no longer statistically significant after FDR adjustment. Figure 4 shows the observed versus expected instructional hours across ABPN content categories.

We also calculated effect sizes, defined as the difference between observed and expected proportions (Obs – Exp), and corresponding 95% confidence intervals to contextualize the magnitude and precision of these findings. The effect size for the “Questions Not Associated with a Specific Neurologic Disorder” category was 0.079, with a 95% CI [0.052, 0.107], indicating a practically meaningful deviation. Complete results, including effect sizes and 95% CIs for all subspecialties, are presented in Supplemental Table 2.
These findings highlight areas where the current curriculum may diverge from board examination emphasis, suggesting potential targets for curricular enhancement.
Discussion
This project demonstrates the value of curriculum mapping in evaluating neurology residency didactics. Over a 6-year period, we found strong representation of subspecialties such as vascular neurology/stroke and movement disorders as well as underrepresentation of several ABPN-relevant topics. Institutional factors, such as the involvement of specific subspecialists in lecture planning, likely contributed to the overrepresentation of some content areas. This highlights the importance of systematic curriculum mapping to detect such discrepancies.
Strengths in Core Topics
Overall, the curriculum demonstrated a strong alignment with ABPN certification standards. The majority of subspecialty topic areas did not show statistically significant deviations from the ABPN-recommended proportions, indicating a balanced distribution across much of the didactic curriculum. The AHD curriculum covered a wide array of neurologic conditions and domains. Fourteen out of 16 ABPN-relevant subspecialty categories were represented (88%), underscoring the diversity of the curriculum over the 6-year period. The breadth of content across diverse areas—from Epilepsy and Neuromuscular Disorders to Neuroimmunology and Neurobehavioral Disorders—demonstrates a broad-based approach to training that supports resident development across the full spectrum of neurological practice.
These strengths form a solid base upon which targeted improvements can be made, ensuring the curriculum continues to evolve in alignment with national standards and resident needs.
Gaps and Underrepresented Areas
Our mapping revealed that critical topics like Metabolic Disorders, Autonomic Disorders, and Psychiatric Disorders were consistently underemphasized. These areas not only appear on the ABPN blueprint but are highly relevant to clinical neurology. The low frequency of lectures in these areas may be due to logistical barriers, such as limited faculty with subspecialty expertise, limited connections to faculty in the Department of Psychiatry, or difficulty integrating these topics into a lecture schedule that is often adapted from prior years. Nonetheless, they represent important facets of neurologic care, particularly in consultative or multidisciplinary settings.
Without structured planning, these omissions can persist across residency cycles, potentially affecting board performance and clinical readiness. Curriculum mapping allows educators to visualize and correct these blind spots, creating a more equitable and comprehensive training experience.
Comparisons to Other Training Programs
Our findings align with those from other residency and fellowship programs that have used curriculum mapping to assess educational alignment. For example, a curriculum mapping project conducted within an internal medicine residency program found that only 29% of scheduled lecture hours addressed content previously covered on ACP-ASIM examinations, underscoring the presence of significant gaps in didactic coverage. 5 Similarly, our analysis identified underrepresented subspecialty areas despite their inclusion on the ABPN Content Blueprint, demonstrating that even well-structured curricula can unintentionally omit key topics.
Curriculum mapping has also been successfully applied in nonclinical fellowship training programs to ensure that educational content is aligned with defined competencies. 11 These studies support our conclusion that curriculum mapping serves as a valuable tool to systematically uncover gaps, realign instructional priorities, and ultimately strengthen educational outcomes. Our work contributes to this growing body of evidence, particularly within the context of neurology residency training, where published applications of curriculum mapping remain limited.
Generalizability
While this project focused on a single neurology residency program, the methodology and findings are broadly applicable across GME. Many programs, regardless of specialty, are challenged with ensuring didactic content is comprehensive, balanced, and aligned with board certification requirements. Our approach—using publicly available exam blueprints and mapping tools—provides a scalable model that can be adapted by other institutions. Although individual institutions may vary in their ability to offer representation of all content areas, curriculum mapping can first highlight areas for adjustment, which can lead to potential interdisciplinary or cross-institutional collaboration. Programs with a daily/NC model for their didactics may also find this framework useful and adapt a similar approach for evaluating existing educational offerings and identifying gaps. By aligning instructional content with defined clinical competencies, residents can also better understand how individual sessions contribute to their overall professional development and board preparation.
We have created a spreadsheet template to allow readers to easily replicate curriculum mapping for their own needs. The template can be found at this link: https://bit.ly/curricmapping.
Limitations
Despite the structured approach, several challenges emerged during the curriculum mapping process. We limited mapping to ABPN Dimension 1 categories. Although we initially attempted to map lectures to Dimension 2 as well, this was ultimately not possible without understanding the detailed content of each individual lecture as domains of Dimension 2 included topics such as clinical aspects of neurologic disease and diagnostic procedures, of which multiple may be covered in a single lecture. As we were unable to confidently and accurately quantify these elements, we decided to omit this from the approach. Additionally, some lectures addressed interdisciplinary or non-disease-specific themes (eg, diversity, leadership skills, wellness), which did not align neatly with ABPN categories and were therefore excluded. However, we recognize that these align with certain ACGME milestones, and so continue to have value. These limitations underscore the importance of accurate curriculum tracking over time.
This study did not include a formal sample size calculation, as it was designed to document and analyze the full set of lectures delivered over a 6-year period rather than to test a specific hypothesis. While comprehensive, the findings may not generalize beyond the curriculum and institutional context studied.
Implementing Change
Based on the findings from our curriculum mapping project, the UCLA Neurology Residency Program Leadership plans to implement a structured 2- to 3-year longitudinal curriculum that more closely reflects ABPN blueprint percentages and would span multiple years of a trainee's time in residency. This would allow for a more balanced distribution of content across training years and help prevent unintentional over- or underrepresentation of certain topics.
To address persistent gaps, particularly in areas like Psychiatric Disorders and Autonomic Disorders, we intend to build collaborations with other departments such as Psychiatry and Internal Medicine. This may include inviting guest lecturers with relevant expertise, integrating interdisciplinary modules, and using shared faculty resources to enhance cross-disciplinary teaching and expand faculty involvement.
We aim to make annual curriculum mapping a standard part of our planning process, supported by resident feedback and faculty input. Although resident perceptions were not formally analyzed in this study, their input will be incorporated in future iterations of curriculum evaluation. This will allow for ongoing evaluation and adjustment, helping to ensure the curriculum remains both comprehensive and adaptable to evolving educational needs.
Ultimately, we hope that implementing a structured 2-year didactic curriculum will improve residents’ exposure to previously underrepresented ABPN content areas. As the curriculum evolves, future evaluations may examine whether these changes lead to improved performance on the RITE exam in these domains, serving as a potential proxy for enhanced knowledge acquisition and retention.
Conclusions
This curriculum mapping project identified key strengths and gaps within the UCLA Neurology Residency AHD curriculum by comparing lecture content to the ABPN blueprint. The analysis revealed areas of overrepresentation and underemphasized topics. By highlighting these disparities, the project provides a foundation for targeted improvements aimed at aligning educational content with board competencies and ensuring comprehensive, equitable training.
This approach offers a practical, data-driven framework for residency programs seeking to optimize their curricula and better prepare residents for board exams and diverse clinical practice. Curriculum mapping can also guide content review, support more balanced topic distribution, and inform long-term curricular planning aligned with institutional goals.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251405155 - Supplemental material for A Different Kind of Brain Mapping: Curriculum Mapping in Neurology Residency Education
Supplemental material, sj-docx-1-mde-10.1177_23821205251405155 for A Different Kind of Brain Mapping: Curriculum Mapping in Neurology Residency Education by Saatvika Nair, Hayoung E. Ahn, Myung Shin Sim and Katherine A. Fu in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205251405155 - Supplemental material for A Different Kind of Brain Mapping: Curriculum Mapping in Neurology Residency Education
Supplemental material, sj-docx-2-mde-10.1177_23821205251405155 for A Different Kind of Brain Mapping: Curriculum Mapping in Neurology Residency Education by Saatvika Nair, Hayoung E. Ahn, Myung Shin Sim and Katherine A. Fu in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
We would like to acknowledge Adrienne M. Keener, MD, for her support in the didactic curriculum of the residency program.
Author Contributions
SN was involved in study design, data collection, data analysis, data interpretation, and manuscript review and writing; HA was involved in data analysis, data interpretation, and manuscript review and writing; MS was involved in data analysis, data interpretation, and manuscript review and writing; KF was involved in study design, data collection, data analysis, data interpretation, and manuscript review and writing.
Financial Disclosure
Katherine Fu, MD, has received financial compensation for serving as the Neurology® Resident and Fellow Section, Section Editor as well as prior grant funding from the American Academy of Neurology. All remaining authors do not have any financial disclosures related to this work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Center for Advancing Translational Science of the National Institutes of Health under the UCLA Clinical and Translational Science Institute (Grant No. UL1TR001881).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.