
Abstract
Introduction
The success of a colonoscopy is highly dependent on the adequacy of bowel preparation. International guidelines recommend good bowel preparation in at least 90% of procedures, as measured by the Boston Bowel Preparation Scale. A quality review at our center revealed 25.7% of colonoscopies had inadequate preparation, which formed the needs basis for our intervention.
Methodology
We implemented a simulation-based educational intervention to improve healthcare workers’ (HCWs) knowledge and confidence regarding colonoscopy preparation. The program included an interactive teaching session covering the essentials of bowel preparation, counseling stations with simulated patients with common clinical presentations, followed by debriefing using the Plus-Delta model. Participants completed pre- and post-intervention tests to assess knowledge improvement and a self-efficacy questionnaire evaluating confidence in key aspects of colonoscopy preparation. A postintervention chart review was conducted to assess the impact of the exercise.
Results
Twenty-eight gastroenterology HCWs participated. The mean pretest score increased from 58.6% to 75.7% (p < .05). Self-efficacy scores improved from 39.1 (71.1%) to 51.0 (92.8%) (p < .05). Qualitative feedback was overwhelmingly positive. A postintervention clinical review after 12 weeks demonstrated significant improvement in bowel preparation quality, with adequate preparation increasing to 92.8%(p < .05).
Conclusion
A simulation-based intervention was successful in an interprofessional healthcare cohort of HCWs in improving counseling skills, participant confidence and quality of clinical care through a measurable improvement in bowel preparation quality.
Introduction
The incidence of colorectal cancer (CRC) has been noted to be increasing in Asia and it is already comparable to that in the West. 1 CRC is preventable and curable, and current studies advocate for colonoscopy as a preferred screening modality for secondary prevention. 2
Colonoscopies can detect and remove precancerous lesions and are also widely used for evaluation of patients presenting with symptoms and other positive CRC screening tests. 3 The success of colonoscopies is associated with the adequacy of preprocedure bowel cleansing. However, up to a quarter of all colonoscopies are reported to have had inadequate bowel preparation. 4
A high-quality colonoscopy is defined as one that has good effectiveness in detecting CRC and its precursors, is safe, and in which the bowel is well prepared so that the operator may detect all pathology 5 . Poor bowel preparation has been linked with indicators of low-quality colonoscopy performance, which include elements such as lower adenoma detection rate, longer and more challenging procedures, increased patient discomfort, increased use of analgesics and hypnotics, lower diagnostic yield, higher burden of CRC incidence and mortality, and a reduction in the interval between subsequent examinations. 6
Adequacy of bowel preparation is one of the most important factors towards the success of a colonoscopy procedure. 7 It is the responsibility of health care professionals to provide patients with instructions for all components of the colonoscopy preparation and emphasis its importance. A patient education program that is administered by healthcare professionals has been shown to increase compliance, improve quality and prevent repeated examinations and costs. 8
The factors that affect bowel preparation can be patient or procedure related. Patient related factors include increased age, male gender, history of constipation or gastroparesis, use of certain medications (eg; tricyclic antidepressants and opioid analgesics) and the presence of comorbidities such as dementia, Parkinson disease, diabetes mellitus, obesity etc.8,9 Procedure related factors include adherence to the bowel preparation instructions, type of cleansing regimen, and timing of the administration of the cleansing regimen. 10
Additionally, with more patients being prescribed newer agents such as direct oral anticoagulants, and an aging population on antiplatelet agents, there may be lack of clarity on the part of medical staff with regards to adjusting doses or stopping these medicines preprocedure. This has important patient safety implications. Current studies show limited information about a standardized way of action and advocate for shared decision making between the patient and multidisciplinary specialists based on the risks versus benefit of holding or adjusting medication doses preprocedure. 11
Other diseases, such as chronic renal failure, diabetes, congestive heart failure, and others require adjustments made to the bowel preparation process as well as specific criteria to be followed for stopping different medications preprocedure. 12 These facts are not known to all staff who counsel patients precolonoscopy, which ultimately affects the safety and quality of the procedure, along with patient and physician satisfaction.
Quantitative methods, such as the Aronchick Score and the Boston Bowel Preparation Scale (BBPS), have been devised to rate the quality of bowel preparation. The BBPS, which has been found to be both reliable and valid, employs a 9-point score (0-9) where the quality of bowel preparation in 3 segments of the colon is rated after cleansing maneuvers during a colonoscopy. 13
International guidelines recommend that the quality of preparation in colonoscopies, based on the BBPS score, should be above 90% within any individual endoscopy unit. 14 A quality review of the colonoscopies performed in the endoscopy unit at our center between August to October, 2022 showed that up to 25.7% of colonoscopies were reported to have poor bowel preparation. These findings formed the basis of our needs assessment for this interventional study.
Healthcare educators throughout the developing world are increasingly incorporating simulation techniques into their educational models as it offers a safe and controlled environment for training and practicing a particular set of clinical skills. Simulation aims to bridge theoretical medicine through the application of Kolb's experiential learning theory, preparing practitioners for real-life situations. 15 It is immensely beneficial to students and faculty as it provides a realistic environment for participants to grasp key learning objectives, provides opportunity for repeated practice and enables effective learning without it compromising patient safety. 16 We felt this would be the best approach to address the gaps identified at our institution.
Primary and Secondary Objectives
To determine if a simulation-based educational intervention delivered to a group of interprofessional hospital staff is effective in improving the quality of bowel preparation in patients undergoing colonoscopies and whether the delivery of the educational intervention is associated with an improvement in the knowledge and self-efficacy of the participants.
Methodology
Nature of Study
Quasiexperimental, pretest–post-test design. The reporting of this study conforms to the TREND statement for reporting nonrandomized trials. 17
Place
The Center for Innovation in Medical Education at the Aga Khan University (AKU), Karachi, Pakistan.
Period
May 2023
Sample Size
28 (Total staff)
Study Participants
All Hospital staff (gastroenterology trainees, nurses, healthcare assistants and technicians) in the gastroenterology outpatient areas and endoscopic unit who counsel patients for bowel preparation were included (Figure 1). Our clinical practice for patients being scheduled for a colonoscopy includes the gastroenterology consultant explaining the complete procedure to the patient with a brief overview of bowel preparation. This is followed by a more detailed patient counseling session by the trainee physician, nursing or allied health staff who become the main players in educating the patient for correct bowel preparation before colonoscopies.

Division of workshop participants by staff category.
Inclusion Criteria
Aforementioned staff who are involved in the care of patients undergoing colonoscopies at The AKU Hospital, Karachi.
Exclusion Criteria
Not applicable.
Study Procedure
Approval from the Ethical Review Committee of the AKU (Review Reference # 2023-9160-27462) was obtained prior to initiating the study.
Data Collection Tool
Data was collected online by study investigators with the help of a structured google sheet. All records were de-identified and kept confidential, with only the study investigators having access.
Preintervention
EHRs of all patients who underwent a colonoscopy procedure in the specified study period were assessed preintervention. Patient demographics, indication for the colonoscopy, and complications during the procedure were recorded. Qualitative and quantitative assessment of the bowel preparation was also recorded. The qualitative assessment was via the physician's judgment based on their comments within the colonoscopy report, and the quantitative assessment was through the BBPS.
Intervention
We conducted a simulation-based educational intervention through a workshop for hospital staff and healthcare providers. Written informed consent was taken from all participants prior to the commencement of the intervention. Demographics including age, gender, and occupation of all the staff members attending the workshop were recorded. During the workshop, participants were taught about evidence-based colonoscopy preparation best practices. We conducted the workshop in two groups over subsequent days and participants were divided equally to ensure there was no compromise in hospital services.
The Healthcare Simulation Standards of Best Practice® were followed in the construct of the workshop. 16 The workshop consisted of the following steps (Figure 2):

Flowchart of workshop proceedings.
Stage 1
A pretest to gauge the participants existing knowledge regarding the prevalence of CRC, colonoscopy recommendations and preparations, instructions pertaining to diet and drugs modifications patients may have to make, investigations to be done before a routine colonoscopy procedure and the BBPS. It consisted of fourteen multiple-choice questions of the single-best-answer type.
An interactive teaching session addressing colonoscopy indications, recommendations, practices, bowel preparation regimens, counseling components and special population groups with reference to comorbidities and regular medications. The course content was designed by a content expert, a practicing gastroenterologist with more than a decade of experience, in conjunction with the head nurse of the endoscopy unit. The session was conducted by members of the research team, with ample opportunity for participants to ask questions and clarify concepts.
A detailed pre-brief in keeping with best practices, with particular emphasis on clarifying expectations, psychological safety, attention to logistic details, and establishing a fiction contract. 18
Stage 2
The participants then moved to counseling stations with simulated patients (SPs) where they were given a supervised opportunity to practice what they had learned. The sessions involved interaction with SP`s who played the role of patients scheduled to undergo a colonoscopy, Participants were expected to counsel the patients regarding the procedure, cover the points as per the checklist for each case (appendix 1), and address any queries the patient may have. The following scenarios were created for the SP interactions:
Patient with no known comorbid conditions undergoing a routine screening colonoscopy. Patient on antihypertensive and anticoagulation (due to atrial fibrillation) undergoing a colonoscopy due to bleeding per rectum. Patient with diabetes and chronic kidney disease with poor glycemic control undergoing a colonoscopy due to generalized weakness. Patient with ischemic heart disease and history of a percutaneous coronary intervention 5 years ago and currently on dual antiplatelet therapy undergoing a routine colonoscopy.
All scenarios were developed by experienced and qualified simulationists, in collaboration with content experts. All participants rotated through all the stations with active participation. Debriefing with the participants was done after each station using the Plus-Delta and 3-phase debriefing techniques by study investigators.
20
All debriefers were trained and experienced prior to the intervention.
Stage 3
A post-test to determine the change in knowledge of participants regarding colonoscopy best practices and components.
A self-efficacy questionnaire to judge their confidence in 11 aspects of the colonoscopy counseling and preparation procedure before and after the workshop.
Postintervention
EHRs of all patients who underwent a colonoscopy procedure in the specified study period post-intervention were assessed, to determine if the intervention was successful. Patient demographics, indication for the colonoscopy, and complications during the procedure were recorded. Qualitative and quantitative assessment of the bowel preparation was also recorded. The qualitative assessment was via the physician's judgment based on their comments within the colonoscopy report, and the quantitative assessment was through the BBPS.
Statistical Analysis
Statistical analysis was performed using SPSS version 22.0. Participant demographics were defined using frequencies. Normality was tested using Shapiro–Wilk test. Median test as well as SEQ scores were calculated along with their differences. The significance of the difference in scores for both groups was tested using dependent t-test.
Results
A total of 28 hospital staff members from the gastroenterology section were part of our study. They consisted of registered nurses (n = 11; 39.3%), critical care technicians (n = 6; 21.4%), healthcare assistants (n = 5; 17.9%), residents and fellow medical officers (n = 4; 14.3%) and endoscopy lead technicians (n = 2; 7.1%).
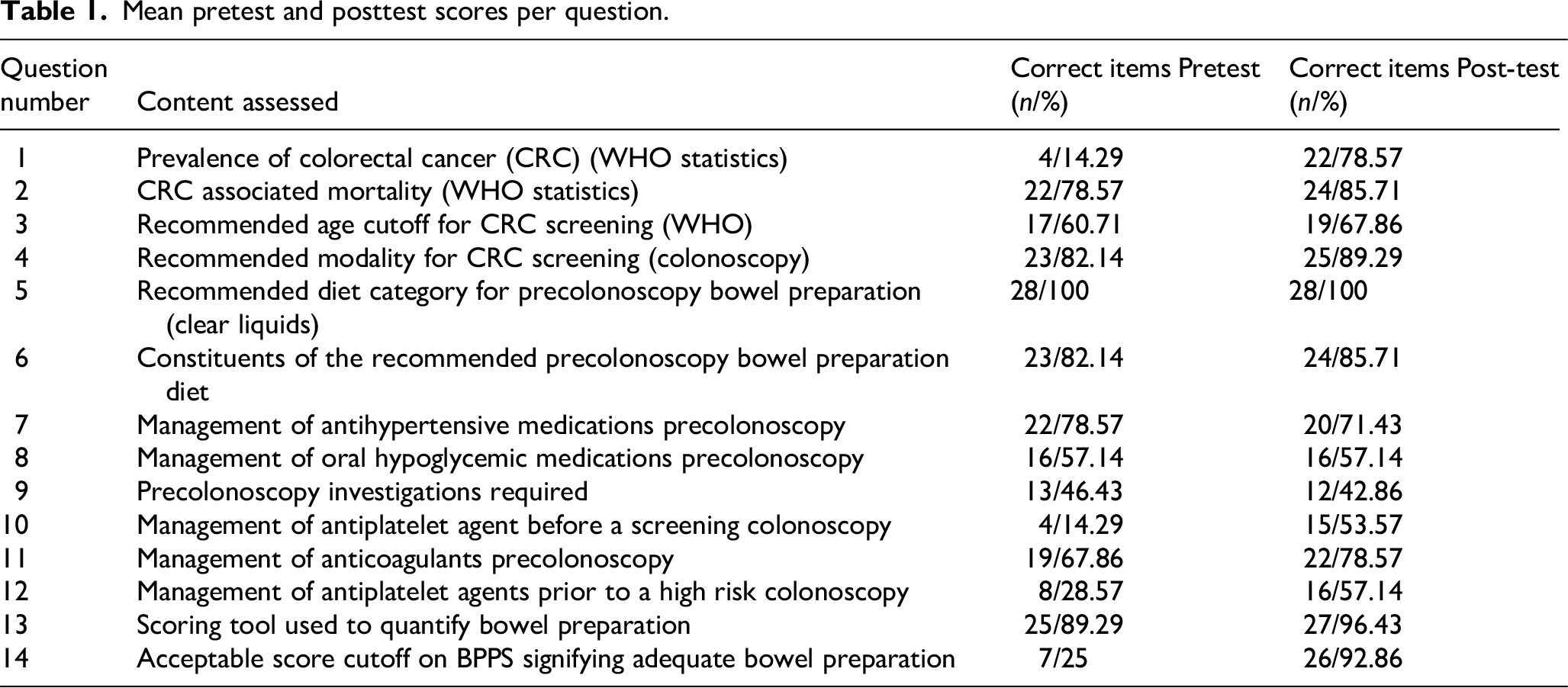
The mean total score in the pretest was 8.25 (58.9%) out of a total of 14. This increased to 10.57 (75.5%) in the posttest. The p-value for this difference was statistically significant (p < .05). The change in the number and percentage of participants who got each question correct is summarized in Table 1.0. The greatest increase in percentage (67.9%) of participants answering a question correctly was seen in question 14 which asked for the minimum BBPS required to label a procedure as having good bowel preparation. Only 25.0% (n = 7) participants answered correctly in the pretest and the number increased to 92.9% (n = 25) in the post-test (Table 1).
Mean pretest and posttest scores per question.
The mean total self-efficacy score across 11 objectives prior to the intervention was 39.1 (71.1%), and increased to 51.0 (92.8%) postintervention. The p-value for this difference in means was 0.000000854 which was also statistically significant (p < .05). The individual objective score changes, displayed in Table 1.0, also showed a significant increase after our intervention with a p value of 0.012 (p < .05).
Qualitative data obtained through participant comments showed an unopposed positive response due to the “patient-centric” and “engaging” nature of the workshop. Additionally, many participants expressed enthusiasm for similar workshops in the future which focused on addressing more skills based learning. Following are some of the comments received: “I learnt a few things that I can implement in my daily practices. Can differentiate now between (the characteristics of) low risk and high risk procedure and patient.” “Excellent way of teaching, this was very effective for me today” “Encountering different simulated patients with different scenarios helped us learn how to answer questions appropriately” “We suggest recording a teaching video and sharing it with staff from other departments as well.”
Discussion
Our study was effective in revealing gaps in knowledge and practices regarding colonoscopy practices at our institution and was successful in bridging these gaps through a multidisciplinary simulation-based intervention.
A similar study conducted at the University of California used an online education module for nurses. 21 They covered the instructions nurses are required to give to patients before starting colonoscopy preparation and used a pretest and post-test to gauge the change in knowledge of the practitioners. Their study demonstrated a significant increase in the knowledge levels following their intervention. However, this study only targeted nursing staff and did not evaluate the practical outcome of the teachings.
In addition to assessing the impact on knowledge, we also tested for the change in self-efficacy of healthcare workers towards essential parts of the counseling procedure. Resultantly, we saw a significant improvement in the confidence of healthcare workers to carry out the expected tasks. This is another important factor to ensure better outcomes.
Similarly, another study aimed to investigate and teach colonoscopy best practices to multidisciplinary inpatient care teams. 22 Their teaching technique was multipronged and consisted of interactive lectures as well as visual posters and handouts. They followed this with evaluating for the change in the bowel preparation quality and they found that they were successful in increasing the quality of bowel preparation. Our study, however, used SPs to target the outpatient interaction which specifically honed the skills of the participants and also helped identify errors in the counseling conversation which were subsequently corrected due to the standardized nature of our checklists.
A study from Korea investigated the impact of a ward nurse educational intervention to improve the bowel preparation quality and they found it to be successful in improving the preparation. 23 However, this study focused only on inpatient procedures and was directed towards assessing bowel preparation and the resultant colonoscopy outcomes. In contrast, in our study, we quantified and analyzed the change in knowledge and self-efficacy of healthcare workers with regard to the counseling procedure in itself also.
Our study is among the first to demonstrate the effectiveness of a simulation-based intervention towards outpatient colonoscopies in a multidisciplinary cohort of healthcare workers. The experiential nature of simulation adds an additional layer to the knowledge and skills gained and thus results in improved outcomes.
While the aforementioned studies showed successful outcomes, all of them primarily assessed inpatient colonoscopy procedures. As a result, they primarily focused on teaching the methodology of preparation. In our intervention, we focused on patient counseling which is more important in the outpatient setting due to a high reliance on patient adherence to instructions.
Investigators have tried different innovative techniques to improve out-patient bowel preparation. Preprocedure video tutorials have not met with much success, 24 but the use of mobile apps by patients did yield favorable results. 25 However, most of these interventions were targeting the patient and their individual procedure, while we wanted to induce a system change through staff upskilling. The multipronged nature of our study focused on assessing the improvement in knowledge, self-efficacy, and bowel preparation using simulation, which resulted in statistically significant outcomes in all the aforementioned aspects.
While our study showed promising results, our intervention was a single event which we aim to conduct as a recurring workshop in future for sustainable results. Perhaps, one way could be to introduce a similar module for all new staff members who are inducted and follow it up with a refresher video resource available for participants who were part of the present study, in addition to patient information reading material.
Our study had several limitations. The sample size, while all-inclusive, was small to generalize findings. Its single-center design, and short follow-up duration are other limiting factors. Another limitation was that the scenarios, while scientifically sound, were not validated in a similar cohort of participants. And finally, we acknowledge that the cost of training and recruiting SP's may be prohibitive in some contexts. 26 Nevertheless, we feel that the results are promising enough to warrant further study.
Conclusion
Simulation based education is effective in significantly increasing the quality of precolonoscopy bowel preparation, knowledge, and perceived self-efficacy in an interprofessional cohort of healthcare workers. The intervention received excellent participant feedback regarding the mode of instruction and was objectively impactful in improving the status of bowel preparation. We propose that such educational interventions should be held regularly to meet the targeted needs of staff in endoscopy centers to enable them to maintain international standards of quality and safety.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251398936 - Supplemental material for Colonoscopy with Attention, Reliability and Excellence—The CARE Project
Supplemental material, sj-docx-1-mde-10.1177_23821205251398936 for Colonoscopy with Attention, Reliability and Excellence—The CARE Project by Umar Tariq, Maha Inam, Masood M Karim, Zanish Hajani and Faisal Wasim Ismail in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-2-mde-10.1177_23821205251398936 - Supplemental material for Colonoscopy with Attention, Reliability and Excellence—The CARE Project
Supplemental material, sj-pdf-2-mde-10.1177_23821205251398936 for Colonoscopy with Attention, Reliability and Excellence—The CARE Project by Umar Tariq, Maha Inam, Masood M Karim, Zanish Hajani and Faisal Wasim Ismail in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
We acknowledge the support staff for simulation at the Center for Innovation in Medical Education of the AKU Karachi for providing assistance with all the logistics involved in executing this study.
Ethics
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the institutional review board (Application # # 2023-9160-27462).
Consent
All participants provided written informed consent prior to enrollment in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.